Post-dural puncture headache: Post-dural puncture headache: an update an update Mike Paech Department of Anaesthesia and Pain Medicine King Edward Memorial Hospital, Perth, Western Australia
Transcript
Post-dural puncture headache: Post-dural puncture headache: an updatean update
Mike Paech Department of Anaesthesia and Pain Medicine King Edward Memorial Hospital, Perth, Western Australia
Disclosures
Learning objectivesLearning objectives
• Update on pathophysiology, aetiology & risk factors of PDPH in the obstetric population
• Pain management. What is current evidence for? –– intrathecal catheter insertion versus epidural catheter re-siting– prophylactic epidural blood patch (EBP) if we re-site– other therapies
• Epidural blood patch: new data
• Is PDPH also a persistent pain issue?
Pathophysiology of PDPH: Why does it happen?
PDPHPDPH- a curious definition?- a curious definition?
Description:
Headache occurring within 5 days of a lumbar puncture, caused by cerebrospinal fluid (CSF) leakage
through the dural puncture. It is usually accompanied by neck stiffness and/or subjective hearing symptoms. It remits spontaneously after 2 weeks, or after sealing of the leak with autologous epidural lumbar patch.
Diagnostic criteria:A.Any headache fulfi lling criterion CB.Dural puncture has been performedC.Headache has developed within 5 days of the dural punctureD.Not better accounted for by another ICHD-3 diagnosis
ICHD-3 = The International Headache Society’s Classification of Headache Disorders, 2013
5% atypicalLoures et al. IJOA 2014
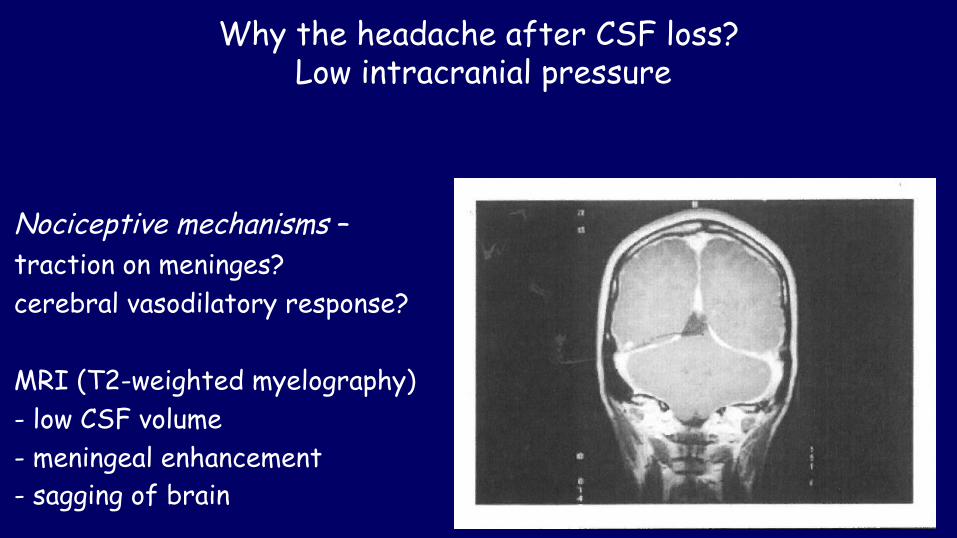
Why the headache after CSF loss? Low intracranial pressure
Nociceptive mechanisms – traction on meninges? cerebral vasodilatory response?
Why the headache after CSF loss? Monroe-Kellie principle
Impaired autoregulation: cerebral vasodilationVadhera et al IJOA 2017
Boezaart. RAPM 2001 MCA Doppler pre- & post-EBP
Why do only 50-80% of pregnant women get a headache after accidental dural puncture?
Anatomical reasons?–characteristics of the hole, the meningeal structure & the closure: volume & duration of CSF loss?–pressure differentials (pushing in labour; body habitus)?
Why do only 50-80% of pregnant women get a headache after accidental dural puncture?
Incidence & severity of PDPHIncidence & severity of PDPH
•Lower in older adults (> 60 years) & children (< 12 years)Lower in older adults (> 60 years) & children (< 12 years)
•Lower in malesLower in males
•Less commonly moderate to severe with post-spinal headache vsLess commonly moderate to severe with post-spinal headache vs
‘ ‘dural tap’dural tap’
•Lower severity in morbidly obeseLower severity in morbidly obese
The patient’s risk factors
1. Does a history of migraine increase the risk? No van Oosterhout et al. Neurology 2013
2. Do smokers have a reduced risk? Perhaps Dodge et al. Pain Physician 2013
3. Does high body mass index reduce the risk? Originally suggested in 1994
– higher intraabdominal or epidural pressure?– lower lumbosacral CSF volume?– different cerebrovascular response?
Miu et al. IJOA 2014 BMI > 35 vs < 35 no differencePeralta et al. Anesth Analg 2015 BMI > 32 7-26% reduction Song et al. IJOA 2017 BMI > 40 vs < 30 no differenceFranz et al. J Clin Anesth 2017 BMI > 50 vs < 30 OR 0.33 (0.13-0.85)
Probably lower risk in super-obesity
Situational risk factorsSituational risk factors1. The operator’s choice of needle1. The operator’s choice of needle
16 G epidural16 G epidural 60-80%60-80%18 G epidural18 G epidural 50-70%50-70%
22 G Quincke22 G Quincke 30-50%30-50%24 G Sprotte24 G Sprotte 2% 2%25 G Whitacre25 G Whitacre 2 – 5% 2 – 5%26 G Quincke26 G Quincke 5% 5%27 G Whitacre27 G Whitacre 0.5% 0.5%
Risk 2.5-3x with ‘traumatic’ needles Risk 2.5-3x with ‘traumatic’ needles Arevalo-Rodriguez a et al. Cochrane 2017 & Xu et al. Medicine (Baltimore) Arevalo-Rodriguez a et al. Cochrane 2017 & Xu et al. Medicine (Baltimore) 20172017
Reina MA et al. RAPM 2017
Lesions produced by different small gauge spinal needles were not markedly different. Ultimately the size and character of the arachnoid hole is what matters
Situational risk factors 2. Does pushing in labour increase the risk?
Older studies unclear. Two new studies suggest it does.
Peralta et al. Anesth Analg 2015- retrospective, n=518
Franz et al. J Clin Anesth 2017- retrospective, n=190
Should we encourage our obstetric colleagues to restrict pushing after dural tap in labour?
Pushing Not pushing OR (CI)
54% 33% 2.4 (1.2-3.9)
75% 59% 2.1 (1.1-4.0)
3. Does placing the epidural catheter intrathecally reduce the risk?
Original studies very positive. More recently…..
Negative studies
Peralta et al. Anesth Analg 2015 retrospective, n=177
Tien et al. Curr Med Res Opin 2016 retrospective, n=109
Russell et al. IJOA 2012 quasi-RCT, n=97
PDPH 72% IT catheter vs 62% re-sited epidural catheter
Do IT catheters reduce the risk?
Positive studies
Bolden et al. RAPM 2016- retrospective, n=218
Verstraete et al. AA Scand 2014- retrospective, n=128
Meta-analysisDeng J et al PlosOne 2017 13 studies, n=1044
RR PDPH 0.8 / EBP 0.6
Intrathecal insertion of the epidural catheter probably has a moderate effect, mainly by reducing severity
4. Does a prophylactic EBP through a re-inserted epidural catheter reduce the risk?
Scavone et al. Anesthesiology 2004 Stein et al. Anaesthesia 2014 - D-B RCT, n=64 - S-B RCT, n=116
Some modest effect…or not??
PDPH Mod or severe PDPH
EBP
Scavone 56% vs 56% 34% vs 47%
Stein 18% vs 80% 15% vs 73% 10% vs 73%
Treatment of PDPH: What therapies help?
What is the natural history of PDPH? What is the natural history of PDPH?
We aren’t sure, esp. after dural tap!We aren’t sure, esp. after dural tap!Post-spinal PDPHs resolve in 1-12 days (mean 4) but for younger patients or
from large needles, 80% DO NOT RESOLVE by 1 week & 10% persist for weeks
What are the consequences of symptomatic treatment and What are the consequences of symptomatic treatment and waiting for resolution?waiting for resolution?
1. Greater suffering & increased length of hospital stay1. Greater suffering & increased length of hospital stay
2. Increased anaesthetic workload due to visits for evaluation & 2. Increased anaesthetic workload due to visits for evaluation & treatmenttreatment
3. A higher risk of serious complications??3. A higher risk of serious complications??
Therapies that don’t help
• Posture / bed rest Cochrane review 2016• Fluid therapy Cochrane review 2016• Opioids & adjuncts No studies• Triptans Small non-randomised trials• Epidural saline Small non-randomised trials
Therapies that might help some
• Caffeine > 300 mg/day (2-4 h reduction in severity)• Epidural morphine• IV aminophylline 250 mg / theophylline 200 mg (duration 1-2 h)
Ergun et al. Acta Neurol Belg 2016
• IV hydrocortisone 200-400 mg daily in divided doses (better than caffeine)Ergun et al. Acta Neurol Belg 2016
• IV ACTH (cosyntropin) 500 mcg in 1 L over 1 h Hanling et al. Pain Med 2016 RCT [vs EBP, n=28]
• IV ondansetron 0.15 mg/kg Fattahi et al. J Anesth [RCT post-spinal, n=210: PDPH 4% vs 20%]
• Oral gabapentinoidsOral gabapentinoids
Short to medium duration relief?
Oral gabapentin or pregabalinOral gabapentin or pregabalin
Erol. Acute Pain 2006Nofal et al. Saudi J Anaesth 2014Mahoori et al. Saudi J Anaesth 2014
Wagner et al. Anaesth Intens Care 2012: n=19 case series after ‘dural tap’n=19 case series after ‘dural tap’
Other ‘miracle cures’…….ha (no controlled studies)!
• Hyperbaric oxygen therapy (for pneumocephalus)
• IV mannitol (onset > 8 h)
• Acupuncture
• Occipital nerve blocks
• Sphenopalatine ganglion block (SPGB)
SPGB with 4% lidocaineCohen et al. RAPM 2014Cohen et al. RAPM 2014Kent et al. J Clin Anesth 2016 Kent et al. J Clin Anesth 2016 Patel. Unpublished retrospective, n=72 vs EBPPatel. Unpublished retrospective, n=72 vs EBP• at 60 min 64% recovered (vs 31%)• at 24 h, 48 h & 1 week, as effective as EBP
ProsPros• Long history of use for migraine & facial painLong history of use for migraine & facial pain• Familiar to pain specialistsFamiliar to pain specialists• Easy to do with cotton-tip applicatorEasy to do with cotton-tip applicator
Cons• Physiological plausibility (PNS block prevents vasodilation?)• No scientific validation
Epidural blood patch (EBP): Anything new?
Efficacy: best for post-spinal PDPHN=151
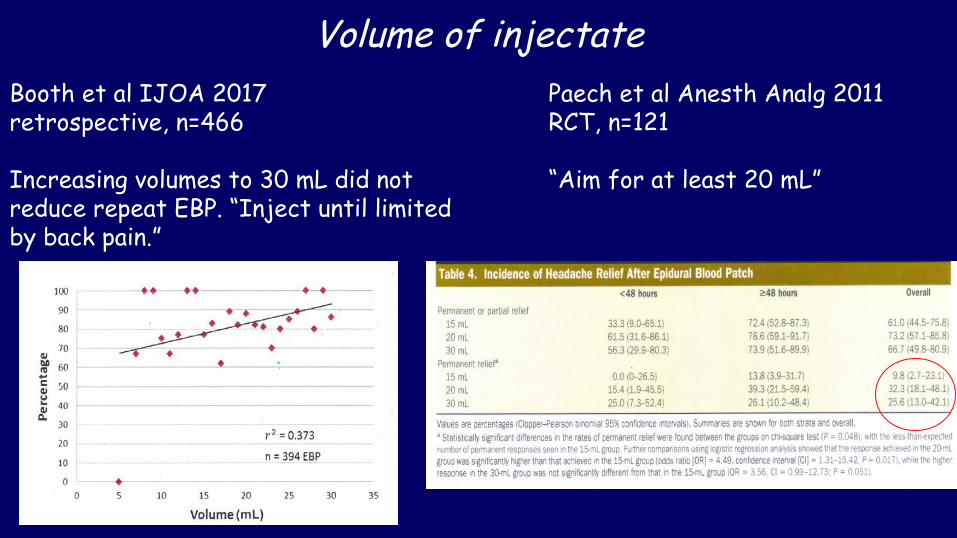
Volume of injectateBooth et al IJOA 2017 retrospective, n=466
Increasing volumes to 30 mL did not reduce repeat EBP. “Inject until limited by back pain.”
Paech et al Anesth Analg 2011RCT, n=121
“Aim for at least 20 mL”
Timing Relieve suffering and repeat prn….. or delay for better first time success?
Kokki et al. IJOA 2013 Booth et al. IJOA 2017 Scavone. IJOA 2017
Targeting the CSF leak site3D optical coherence tomography
Kuo et al. Plos One 2017
Digital subtraction myelography Schievink et al J Neurosurg Spine 2017
Other things associated with PDPH
Don’t forget other possible consequences of CSF loss!1. Cranial nerve palsies 1. Cranial nerve palsies Chambers et al. IJOA 2017 Chambers et al. IJOA 2017
2. Subdural haematoma 2. Subdural haematoma Lim et al. RAPM 2016Lim et al. RAPM 2016
•incidence 1:4,000 [1:90 after ‘dural tap’?]incidence 1:4,000 [1:90 after ‘dural tap’?]
3. Chronic headache, backache and auditory symptoms3. Chronic headache, backache and auditory symptoms
Does acute headache lead to chronic headache?
Jeskins et al IJOA 2001 case control n=192Webb et al. Anesth Analg 2012 case-control study n=40Ranganathan et al. J Clin Anesth 2015 n=308 & 50 controlsTan et al. unpublished retrospective, n=62
- incidence 28%- most with postural elements
Summary: Key points
• New insights into pathophysiology & individual variability
• Needle size, patient age and body mass index remain the only major predictors of risk
• Weak evidence for a modest benefit from IT catheterisation and detriment from pushing in the second stage of labour
• Conflicting evidence for PEBP so still unpopular….
• Interest in some symptomatic therapies, including gabapentinoids & sphenopalatine ganglion block, requires study
EBP•arguments about optimal timing persist•use at least 20 mL or a volume determined by patient tolerance•imaging techniques can determine the site of CSF leak, if necessary
Be aware of potential cranial nerve palsies & cranial subdural haematoma - image and get neurological opinions when in doubt
Weak evidence suggests PDPH confers a substantial risk of persisting symptoms up to years later