26
Minimizing Growth Suppression in Children with Steroid- sensitive Nephrotic Syndrome Alex Constantinescu, MD Director, Pediatric Nephrology Joe DiMaggio Children’s Hospital
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | shoshana-benjamin |
| View: | 44 times |
| Download: | 9 times |

Minimizing Growth Suppression in Children with Steroid-sensitive Nephrotic Syndrome
Alex Constantinescu, MD
Director, Pediatric Nephrology
Joe DiMaggio Children’s Hospital
Hollywood, Florida

Outline
• Define steroid-sensitive nephrotic syndrome
• Disease course – relapse pattern
• Side effects of steroids
• Growth suppression data
• Strategies to prevent growth-suppression

Definition
• “Nephrotic Syndrome = clinical entity having multiple causes, characterized by high glomerular membrane permeability, manifested by massive proteinuria and lipiduria, …in the absence of depressed GFR.” (G. Schreiner, 1963)
• Upr excretion rates are usually >40 mg/m2/hr in children, or >1 g protein/g creatinine (random sample)

Childhood Nephrotic Syndrome (NS)
• Most common cause: minimal change disease (MCD)
• First line of therapy: corticosteroids – daily followed by alternate day
• Many protocols ISKDC – 1978, 1981

Types of Nephrotic Syndrome
• Based on steroid sensitivity:– steroid-responsive (protein-free)
• Infrequent relapsers (<2 in a year)• Frequent relapsers (2 in 6 months, or >3 in a year)• Steroid-dependent (within 1 month after steroids
stopped or while on alternate day therapy)
– steroid-resistant (no response after 4-6 weeks)

Systems Affected by Steroid Therapy
• Gastro-intestinal (gastritis)
• Cardio-vascular (hypertension)
• Hematological (leukocytosis, immunosuppression)
• Neuro-psychological (psychosis, depression)
• Bone metabolism (osteoporosis)
• Skin and Eye (striae, cataracts)
• Glucose metabolism (diabetes, cushingoid body habitus)
• Growth – suppression, leading to short stature
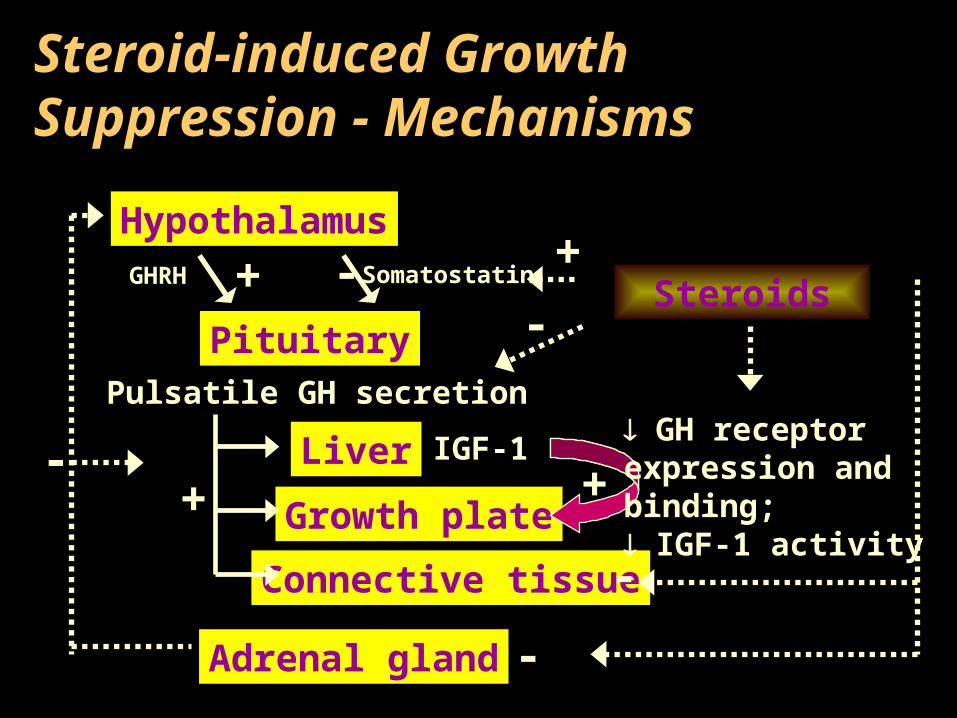
Steroid-induced Growth Suppression - Mechanisms
Hypothalamus
Pituitary
Liver
Growth plate
Connective tissue
Adrenal gland
GHRH Somatostatin+ -
Pulsatile GH secretion
+IGF-1
+ GH receptorexpression andbinding; IGF-1 activity
Steroids+
-
-
-
-

Impact of Short Stature
• Body image
• Psychosocial adaptation
• Bone metabolism
• Pubertal development

• Single center - Robert Wood Johnson Medical School, New Brunswick, NJ• We sought to identify:
– Degree of growth suppression caused by steroid therapy in children with NS, presumed to have MCD
– Moment of “maximum impact”– Frequency of this adverse effect – Is this long-lasting?
• Patients with focal segmental sclerosis on biopsy, as well as those with other steroid-resistant forms of NS were excluded
• Data entered in GrowTrack v 1.0.6 Software (Genentech, Inc.)• Standard deviation scores (SDS) for Ht (HtSDS) and GR (GRSDS), were
calculated and compared with normal values for age and gender
Growth in Children with Nephrotic Syndrome
Cederbaum N, Constantinescu A. J Investigative Medicine 50:187, 2002.

Results
• 69 children with complete growth data
• 44 boys, 25 girls, M:F=1.8:1
• Age range 1-17.8 years
• Younger than 6 yrs of age 75.4%
• Older than 6 yrs of age 24.6%

Ht SDS in Children with Nephrotic Syndrome
-4
-3
-2
-1
0
1
2
3
4
Time
Ht
SD
S
3m 6m 1y 2y 3y 4y 5y 6y 7y 8y 9y 10y 11y
-1.8 SD

HtSDS in Children with Nephrotic Syndrome
-3-2-10123456
HtS
DS
HtSDS in M<6y (n=31)
HtSDS in F<6y (n=21)
HtSDS in M>6y (n=13)
HtSDS in F>6y (n=4)
3 mos 6 mos 12 mos

Growth Rate SDS in Children with Nephrotic Syndrome
-8
-6
-4
-2
0
2
4
6
8
10
12
Time
Gro
wth
Rat
e S
DS
3m 6m 1y 2y 3y 4y 5y 6y 7y 8y 9y 10y 11y 12y

Growth Velocity Rate (GVR) in Children with NS
0.0
5.0
10.0
15.0
20.0
p=0.029
3 m 6 m 12 m
GVR for 3-6-12 mo.
0.0
5.0
10.0
15.0
20.0
3 m 6 m 12 m
MF
M F M F
GVR - M vs. F <6 yrs.
p=0.0190.0
5.0
10.0
15.0
20.0
3 m 6 m 12 m
MF
M
FM
GVR - M vs. F >6 yrs.

Long-term Linear Growth in Children with SD or FR Nephrotic Syndrome
Emma F, et al. Pediatr Nephrol 18:783-8, 2003
• 56 children (37 M, 19 F) followed-up for 10.5±3.1 yrs• SD = 42, FR = 14• Average growth loss was 0.66±0.89 SD• 2 patients fell below -2SD• 23 reached final height with loss of:
• 0.92±0.8 HtSDS from the onset of disease (p=0.001)• 0.68±0.7 HtSDS from predicted target height (p=0.001)
• Correlated with steroid dose – higher risk if more than 6 months• Growth velocity rate lower in younger children, <4 yrs

So far …
• Reviewed the impact of steroids on growth
• How can we minimize exposure to steroids?– Lower the frequency of relapse– Lower the initial dose of steroids
• Can we tailor the therapy?

Tailor Therapy
• Arbeitsgemanschaft für Pädiatrische Nephrologie published in 1998, in Lancet, the finding that 6 weeks of daily steroids + 6 weeks of alternate day steroids appear to reduce the relapse rate – larger cumulative steroid dose
• Niaudet and Habib in 1994 introduced cyclosporine in the treatment of NS, as steroid-sparing agent.
• No sustained remission, additional side effects
• Segregate according to “days to remission” ?

Predictors of Frequent Relapses in NS
• Mishra et al. J Trop Pediatr 2013; 59:343-349– 60% relapse (150 – 1 year) – young age and longer time to
remission predicts frequent relapsing course
• Harambat et al. Pediatr Nephrol 2013; 28:631-638– 70% FR/SD (120 – 6.7 years) – longer time to remission
predicts use of steroid-sparing agents
• Sureshkumar et al. Pediatr Nephrol 2014; 29:1039–1046– 66% relapse (129 – 1 year) – male, young age, short time to
first relapse predicts FR
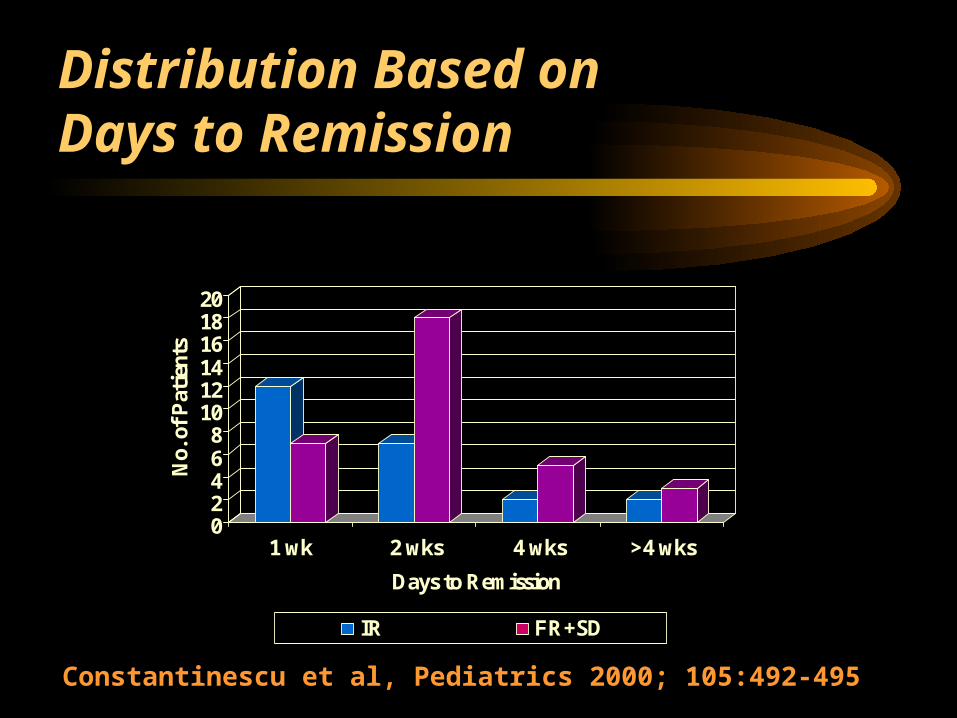
Distribution Based on Days to Remission
02468
101214161820
No.
of
Pat
ient
s
1 wk 2 wks 4 wks >4 wks
Days to Remission
IR FR+SD
Constantinescu et al, Pediatrics 2000; 105:492-495

Disease Course in Patientswith Hematuria
0
5
10Nr.
patients with
hematuria
Relapse pattern vs. Days to remission
0-7 >7 IR
FR+SD
Constantinescu et al, Pediatrics 2000; 105:492-495

Disease Course in Patients without Hematuria
02468
10
1214
16
Nr. Patients without
hematuria
Relapse Pattern vs. Days to remission
0-7
>7
IRFR+SD
Constantinescu et al, Pediatrics 2000; 105:492-495
*
Predictsinfrequent
relapsing course
* p<0.05

MDR-1 Gene Polymorphism
• MDR-1 encodes for P-glycoprotein-170, a biological barrier
• Up-regulated MDR-1 gene expression correlates with a poor response to steroids
• MDR-1 polymorphism studies – in NS, TT genotype associated with a delayed response to steroids and a FR course
Wasilewska, A, et al. Pediatr Nephrol 22:44-51, 2007

Our Approach to Minimize Exposure to Steroids
• Establish the diagnosis of nephrotic syndrome• Determine if hematuria is present at the onset• Start steroid therapy• Parents call first day urine is protein-free• With hematuria, steroids 6 wks QD + 6 wks QOD• Without hematuria AND response in >1 wk, therapy for 6 wks QD
+ 6 wks QOD • Without hematuria AND response in <1 wk, therapy only for 4
wks QD + 4 wks QOD• No response in 4 wks - kidney biopsy

Our Data
• 2006 – present: 60 children with steroid-sensitive NS• 26 with complete growth records• 34 – either recently diagnosed, incomplete records, or lost
to follow-up• Relapse pattern noted (IR, FR/SD)• Initial steroid course (4+4 or 6+6)• Ht SDS at the last visit

Ht SDS - A Function of Relapse Pattern and Steroid Dose
Ht SDS in Children with NS
-1.6
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
Ht
SD
S
IR 4+4 IR 6+6 FR/SD 6+6(pre-SSA)
FR/SD 6+6(on SSA, last)
SSA = patient receiving steroid-sparing agent (tacrolimus or cyclosporine)* p = 0.039 between IR 4+4 and pre-SSA# p = 0.0000133 between pre-SSA and last visit on SSA¶ p = 0.29 between IR 4+4 and FR/SD 6+6 at last visit on SSA
5 11 10*
10#,¶

Conclusions
• Steroids have growth-suppression potential• Attempts needed to minimize the exposure• Change in daily dose is not recommended • Cumulative dose can be decreased by predicting
the infrequent relapsing pattern based on:– response within one week and,
– the absence of hematuria.
• Prospective studies needed

















