AbstractBackground: The minimum clinically important difference (MCID)attempts to define the patient’s experience of treatment outcomes. Effortsat calculating the MCID have yielded multiple and inconsistent MCIDvalues. The purposes of this reviewwere to describe the usage of theMCIDin the most recent orthopaedic literature, to explain the limitations of itscurrent uses, and to clarify the underpinnings of MCID calculation.Subsequently, we hope that the information presented here will helppractitioners to better understand the MCID and to serve as a guide forfuture efforts to calculate the MCID. The first part of this review focuses onthe upper-extremity orthopaedic literature. Part II will focus on the lower-extremity orthopaedic literature.
Methods: A reviewwas conducted of the 2014 to 2016 publications in TheJournal of Arthroplasty, The Journal of Bone & Joint Surgery, The AmericanJournal of SportsMedicine, Foot&Ankle International, Journal ofOrthopaedicTrauma, Journal of Pediatric Orthopaedics, and Journal of Shoulder andElbow Surgery. Only clinical science articles utilizing patient-reportedoutcomemeasure (PROM) scores were included in the analysis. A keywordsearch was then performed to identify articles that calculated orreferenced the MCID. Articles were then further categorized into upper-extremity and lower-extremity publications. MCID utilization in theselected articles was subsequently characterized and recorded.
Results: The MCID was referenced in 129 (7.5%) of 1,709 clinical sciencearticles that utilized PROMs: 52 (40.3%) of 129 were related to the upperextremity, 5 (9.6%) of 52 independently calculated MCID values, and 47(90.4%) of 52 used previously published MCID values as a gauge of theirown results.MCIDvalueswere consideredor calculated for 16PROMs; 12ofthese were specific to the upper extremity. Six different methods wereused to calculate the MCID. Calculated MCIDs had a wide range of valuesfor the same PROM (e.g., 8 to 36 points for Constant-Murley scores and 6.4to 17 points for American Shoulder and Elbow Surgeons [ASES] scores).
Conclusions: Determining useful MCID values remains elusive and iscompounded by the proliferation of PROMs in the field of orthopaedics.The fundamentals of MCID calculation methods should be criticallyevaluated. If necessary, thesemethods shouldbe corrected or abandoned.
Disclosure: There was no source of external funding for this study. On the Disclosure of Potential
Conflicts of Interest forms, which are provided with the online version of the article, one or more of the
authors checked “yes” to indicate that the author had a relevant financial relationship in the
biomedical arena outside the submitted work (http://links.lww.com/JBJSREV/A377).
Furthermore, the type of change intended to bemeasured should beclarified: beneficial, detrimental, or small or large changes. Thereshould also be assurance that the calculation method actuallymeasures the intended change. Finally, the measurement errorshould consistently be reported.
Clinical Relevance: The MCID is increasingly used as a measure ofpatients’ improvement. However, the MCID does not yet adequatelycapture the clinical importance of patients’ improvement.
Ashealth-care reimburse-ment becomes increasinglydependent on the quality ofvalue-based care, patient
engagement plays an increasingly largerrole in the evaluation of treatmentoutcomes in the United States1. Con-sequently, the utilization of patient-reported outcome measures (PROMs)has become commonplace. The adventof PROMshas been an attempt to fill thevoid that exists from the inability ofmore objective measures to quantifypatients’ experiences of treatment out-comes. Despite these useful metrics,there are several shortcomings withregard to the usage of PROMs that areworth noting. First, accumulating evi-dence demonstrates that a wide range ofreported improvementsmay result usingthe same PROM to assess the sametreatment even within similar patientpopulations. Second, many studies inthe literature have shown mean scoreimprovements ofwhole patient samples,which fundamentally fail to capture theindividual patient’s experience. Third,many PROM scores lack intuitive clin-ical relevance; for example, one cannotdefinitively saywhether a pain reductionof 2 of 10will improve a patient’s qualityof life. Although efforts to better definethe clinical importance of PROM scoreshave been ongoing, currently, to ourknowledge, none have yet yielded con-sistent and valid results.
The minimum clinically impor-tant difference (MCID) is the product ofone attempt to define patients’ experi-ences. The term MCID was coined in1989 by Jaeschke et al. as “the smallestdifference in score in the domain ofinterest which patients perceive as ben-
eficial.”2 In other words, the MCIDis a calculated minimum thresholdvalue in an outcome of interest thatpatients perceive as clinically meaning-ful. Although both improvement andclinical decline can be defined in thisway, the calculation of the former hasbeen the primary focus in the literature.The definition of the MCID appearsuniversally accepted, but, unfortunately,there has been extreme variability in bothits measurement and applications.
Two broad categories of calculat-ing the MCID include anchor-basedmethods anddistribution-basedmethods.Furthermore, there are many subcate-gories of methods within these 2 generalgroups. Confusingly, this has yieldeda countless number of ways that theMCID can be calculated, each com-monly resulting in a different value ofthe MCID.
In the most commonly usedanchor-based approach of calculatingthe MCID, patient-reported outcomesare paired or anchored to another sub-jective scale, usually some form of aglobal rating scale. Changes in scores onthe patient-reported outcome are com-pared with a change in a specified globalrating scale, and then various statisticaltools are applied to determine theMCID.However, the use of a subjectiveanchor and the inconsistent manner inwhich global rating scales are formu-lated and utilized or relative changes inpatient-reported outcome scores areclustered raise concerns with regard tothe validity of anchor-based MCIDs.
Distribution-based methods con-sider that some measurement of varia-bility in PROM scores, such as thestandard deviation or the effect size, is
indicative of the MCID. Two com-monly implemented distribution-basedmethods of calculating the MCID arethe standard error of measurement(SEM) and the minimum (or smallest)detectable change (MDC). The SEMrepresents the underlying chance forerror in a measured score due to the testitself (i.e., due to randomvariation).TheMDC is a variation of the SEM thatestimates the smallest amount of changein a score that is not due to chance. Afrequently cited flaw of the distribution-based methods is that, because they areprimarily statistically based, they do notadequately address patient-perceivedclinical importance, the underlyingtenet of the MCID.
Unfortunately, there is no consensuson the optimal method of calculating theMCID. Consequently, calculated valuesof the MCID in the literature vary quitedrastically for the same patient-reportedoutcomes. This variability in MCIDvalues has been shown to be related to amultitude of factors, including thepatient population being studied, treat-ment modality, follow-up intervals, andmethod used to calculate the MCID.The wide spectrum of MCID calcula-tionmethods and its implications for theresultant MCID values have previouslybeen reviewed3,4.
The consequent existence of mul-tiple and inconsistent MCID values hascontributed to confusion among prac-titioners and scientists. Thus, the pur-pose of this review was to describe theusage of the MCID in the most recentorthopaedic literature, to explain thelimitations of its current uses, and toclarify the underpinnings of the MCIDcalculation. Ultimately, we hope thatour review will help practitioners tobetter understand the MCID. BecausePROMs are joint-specific, this review isdivided into 2 parts. In this current part,we will first address the upper-extremityliterature. In Part II5, the lower-extremityliterature will be discussed. In this part,Part I, we will discuss the multiplicityof the MCID values and the followingconcepts as they relate to MCID: thedirection of measured change and the
| MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y
measurement error. The lower-extremitydiscussion will address equation confu-sion and the fundamentally flawed usagesof the MCID for power analyses and as abenchmark for group means.
Material and MethodsArticles published from 2014 to 2016 ina sampling of 7 major orthopaedicjournals were reviewed: the Journal ofArthroplasty, The Journal of Bone & JointSurgery, The American Journal of SportsMedicine, Foot & Ankle International,Journal of Orthopaedic Trauma, Journalof Pediatric Orthopaedics, and Journalof Shoulder and Elbow Surgery. Webelieve that our sampling of generaland specialty-specific journals is broadlyrepresentative of upper-extremity andlower-extremity subspecialties and ac-complishes the task of identifying arandom sampling of the orthopaedicliterature that utilizes the MCID.Additionally, spine-related publicationswere not included in either part of thisreview as they have been previously re-viewed in a separate article4. Clinicalstudies utilizing PROMs were identi-fied. A keyword searchwas performed in
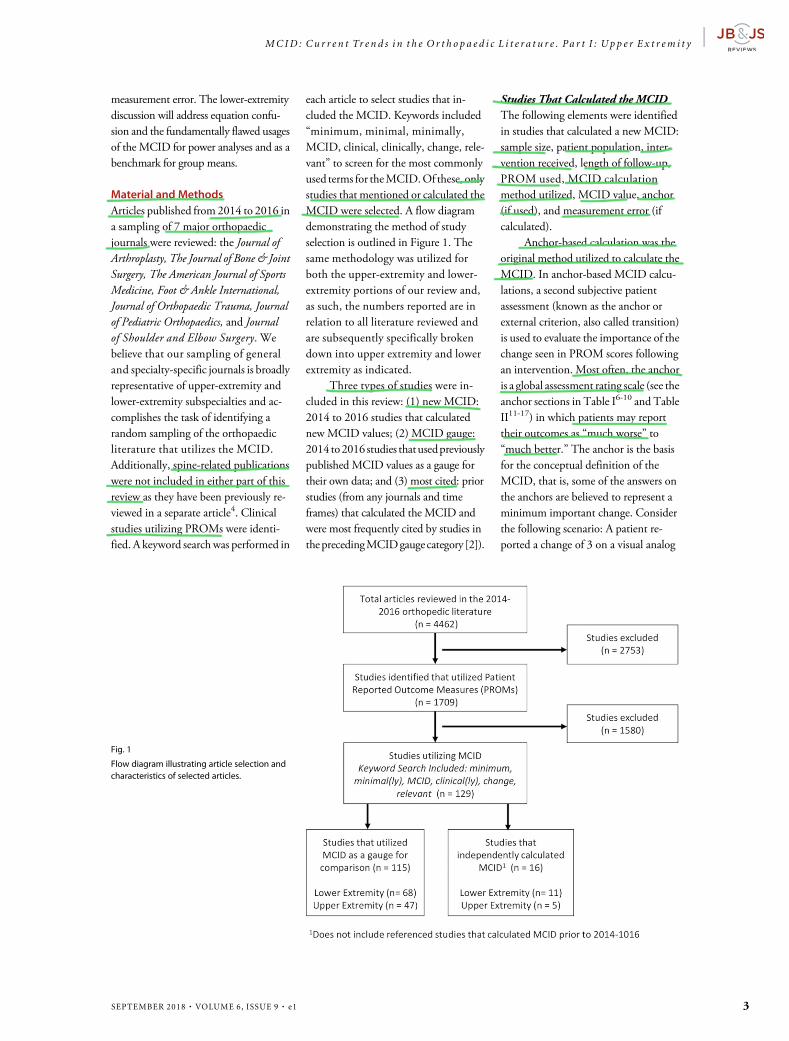
each article to select studies that in-cluded the MCID. Keywords included“minimum, minimal, minimally,MCID, clinical, clinically, change, rele-vant” to screen for the most commonlyused terms for theMCID.Of these, onlystudies that mentioned or calculated theMCID were selected. A flow diagramdemonstrating the method of studyselection is outlined in Figure 1. Thesame methodology was utilized forboth the upper-extremity and lower-extremity portions of our review and,as such, the numbers reported are inrelation to all literature reviewed andare subsequently specifically brokendown into upper extremity and lowerextremity as indicated.
Three types of studies were in-cluded in this review: (1) new MCID:2014 to 2016 studies that calculatednew MCID values; (2) MCID gauge:2014 to2016 studies thatusedpreviouslypublished MCID values as a gauge fortheir own data; and (3) most cited: priorstudies (from any journals and timeframes) that calculated the MCID andwere most frequently cited by studies intheprecedingMCIDgaugecategory [2]).
Studies That Calculated the MCIDThe following elements were identifiedin studies that calculated a new MCID:sample size, patient population, inter-vention received, length of follow-up,PROM used, MCID calculationmethod utilized, MCID value, anchor(if used), and measurement error (ifcalculated).
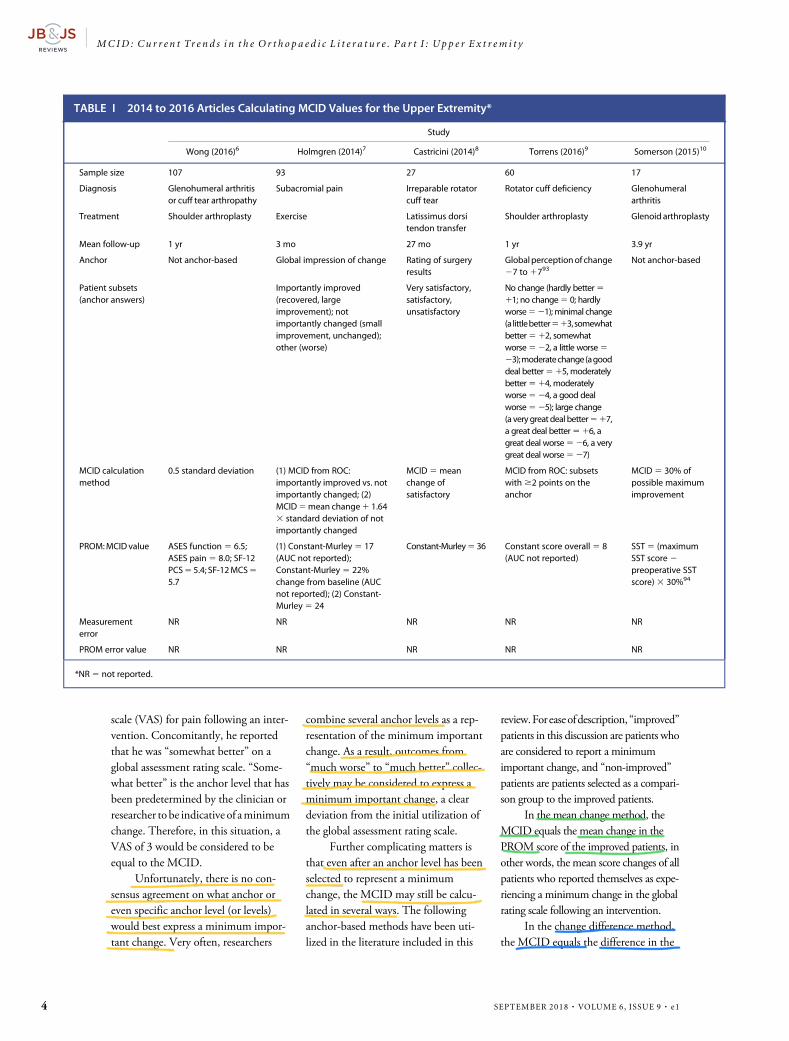
Anchor-based calculation was theoriginal method utilized to calculate theMCID. In anchor-based MCID calcu-lations, a second subjective patientassessment (known as the anchor orexternal criterion, also called transition)is used to evaluate the importance of thechange seen in PROM scores followingan intervention. Most often, the anchoris a global assessment rating scale (see theanchor sections in Table I6-10 and TableII11-17) in which patients may reporttheir outcomes as “much worse” to“much better.” The anchor is the basisfor the conceptual definition of theMCID, that is, some of the answers onthe anchors are believed to represent aminimum important change. Considerthe following scenario: A patient re-ported a change of 3 on a visual analog
Fig. 1
Flow diagram illustrating article selection andcharacteristics of selected articles.
MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y |
SEPTEMBER 2018 · VOLUME 6, ISSUE 9 · e1 3
scale (VAS) for pain following an inter-vention. Concomitantly, he reportedthat he was “somewhat better” on aglobal assessment rating scale. “Some-what better” is the anchor level that hasbeen predetermined by the clinician orresearcher tobe indicative of aminimumchange. Therefore, in this situation, aVAS of 3 would be considered to beequal to the MCID.
Unfortunately, there is no con-sensus agreement on what anchor oreven specific anchor level (or levels)would best express a minimum impor-tant change. Very often, researchers
combine several anchor levels as a rep-resentation of the minimum importantchange. As a result, outcomes from“much worse” to “much better” collec-tively may be considered to express aminimum important change, a cleardeviation from the initial utilization ofthe global assessment rating scale.
Further complicating matters isthat even after an anchor level has beenselected to represent a minimumchange, the MCID may still be calcu-lated in several ways. The followinganchor-based methods have been uti-lized in the literature included in this
review.For easeofdescription,“improved”patients in this discussion are patients whoare considered to report a minimumimportant change, and “non-improved”patients are patients selected as a compari-son group to the improved patients.
In the mean change method, theMCID equals the mean change in thePROM score of the improved patients, inother words, the mean score changes of allpatients who reported themselves as expe-riencing a minimum change in the globalrating scale following an intervention.
In the change difference method,the MCID equals the difference in the
TABLE I 2014 to 2016 Articles Calculating MCID Values for the Upper Extremity*
Study
Wong (2016)6 Holmgren (2014)7 Castricini (2014)8 Torrens (2016)9 Somerson (2015)10
No change (hardly better511; no change5 0; hardlyworse521);minimal change(alittlebetter513,somewhatbetter512, somewhatworse522, a little worse523);moderatechange(agooddeal better515, moderatelybetter514, moderatelyworse524, a good dealworse525); large change(a very great deal better517,a great deal better516, agreat deal worse526, a verygreat deal worse527)
MCID calculationmethod
0.5 standard deviation (1) MCID from ROC:importantly improved vs. notimportantly changed; (2)MCID5mean change1 1.643 standard deviation of notimportantly changed
MCID5meanchange ofsatisfactory
MCID from ROC: subsetswith$2 points on theanchor
MCID5 30% ofpossible maximumimprovement
PROM:MCID value ASES function5 6.5;ASES pain5 8.0; SF-12PCS55.4; SF-12MCS55.7
(1) Constant-Murley5 17(AUC not reported);Constant-Murley5 22%change from baseline (AUCnot reported); (2) Constant-Murley5 24
Constant-Murley5 36 Constant score overall5 8(AUC not reported)
| MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y
4 SEPTEMBER 2018 · VOLUME 6, ISSUE 9 · e1
mean change in the PROM score be-tween the improved and non-improvedpatients, in other words, the mean scorechange of all patients who reportedthemselves as experiencing a minimumchange in the global rating scale minusthe mean score change of all patientswho did not report themselves as expe-riencing a minimum change.
In the receiver operating char-acteristic (ROC) curve method, theMCID equals the cutoff score betweenimproved and non-improved patientsdetermined by an ROC curve. TheROC curve is another modality thatidentifies a change in a PROM thatdiscriminates between the improved andnon-improved patients. It relies on the
area under the curve (AUC) to deter-mine how often the score change cor-rectly discriminates between 2 patients.For instance, if the AUC equals 0.80, aspecific change in score correctly iden-tifies improved and non-improvedpatients 80% of the time. AUC valuesapproaching 1.0 represent excellentdiscrimination.
In the mean change limit method,the MCID equals the mean change (asabove, but of non-improved patients)11.645 times the standard deviation ofthe non-improved patients’ reportedscore18.
Distribution-based MCID calcu-lations compare the change in PROMscores with some measure of variability
such as the standard deviation or effectsize.Distribution-basedmethods do notconceptuallydefine theminimumchange(in contrast to anchor-based calculationmethods). The following distribution-based methods were utilized in the liter-ature included in this review.
In the 0.5 standard deviationmethod, the MCID value is equal tohalf of the standard deviation of themeasured change in PROM scores19.
In the percentage from baselinemethod, the MCID equals a specific per-centage of improvement from the baselinescore, for instance, an improvement of30% from before the intervention.
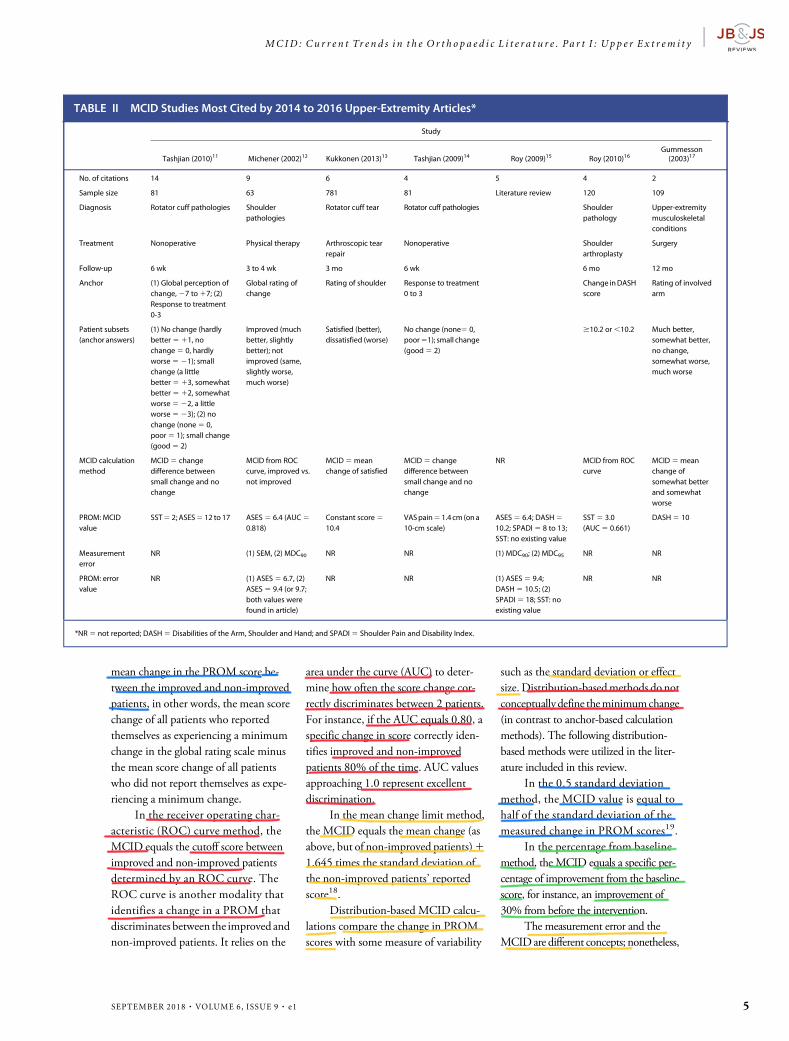
The measurement error and theMCIDare different concepts; nonetheless,
TABLE II MCID Studies Most Cited by 2014 to 2016 Upper-Extremity Articles*
Study
Tashjian (2010)11 Michener (2002)12 Kukkonen (2013)13 Tashjian (2009)14 Roy (2009)15 Roy (2010)16Gummesson(2003)17
No. of citations 14 9 6 4 5 4 2
Sample size 81 63 781 81 Literature review 120 109
NR (1) SEM, (2) MDC90 NR NR (1) MDC90; (2) MDC95 NR NR
PROM: errorvalue
NR (1) ASES5 6.7, (2)ASES5 9.4 (or 9.7;both values werefound in article)
NR NR (1) ASES5 9.4;DASH5 10.5; (2)SPADI5 18; SST: noexisting value
NR NR
*NR5 not reported; DASH5 Disabilities of the Arm, Shoulder and Hand; and SPADI5 Shoulder Pain and Disability Index.
MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y |
SEPTEMBER 2018 · VOLUME 6, ISSUE 9 · e1 5
the calculation of MCID values for aPROM should take measurement error(i.e., the imprecision of that PROM) intoaccount. The SEM has traditionally beenutilized as a representation of the randomvariation in a data set of recorded scores.Hence, a change in a score that is smallerthan the calculated SEM is likely to occurbecause of measurement error and is lesslikely to represent a true change. Anothermeasure ofmeasurement error, theMDC,is the smallest change that can be consid-ered to exceed themeasurement error withagiven levelofconfidence(usuallyata95%level of confidence; sometimes, 90%).Ultimately, if the value calculated for theMCID is smaller than that of the mea-surement error, the PROMmay not beresponsive enough to detect an improve-ment that is deemed meaningful to theindividual patient20.
The SEMandMDCare calculatedas follows21:� SEM 5 SD
ffiffiffiffiffiffiffiffiffiffi
12 rp
(SD: stan-dard deviation of baseline scores,r: test-retest reliability coefficient)
� MDC90 5 1:65ffiffiffi
2p
SEM(hence, MDC90 5 2.33 SEM)
� MDC95 5 1:96ffiffiffi
2p
SEM(hence, MDC95 5 2.77 SEM)
Tables I and II include the fol-lowing information: the anchor type(for anchor-based calculations) withthe anchor answers; the combinationof anchor answers to form subsets ofimproved and non-improved patients,the MCID calculation method uti-lized, and the measurement error (ifapplicable).
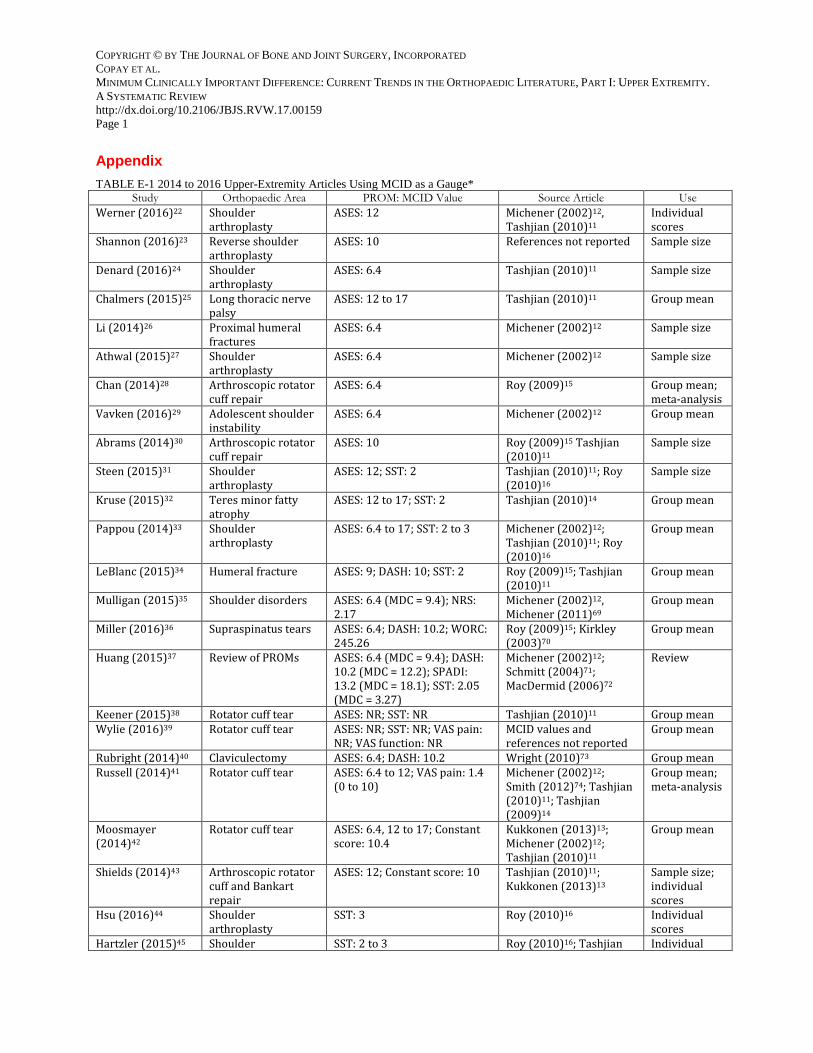
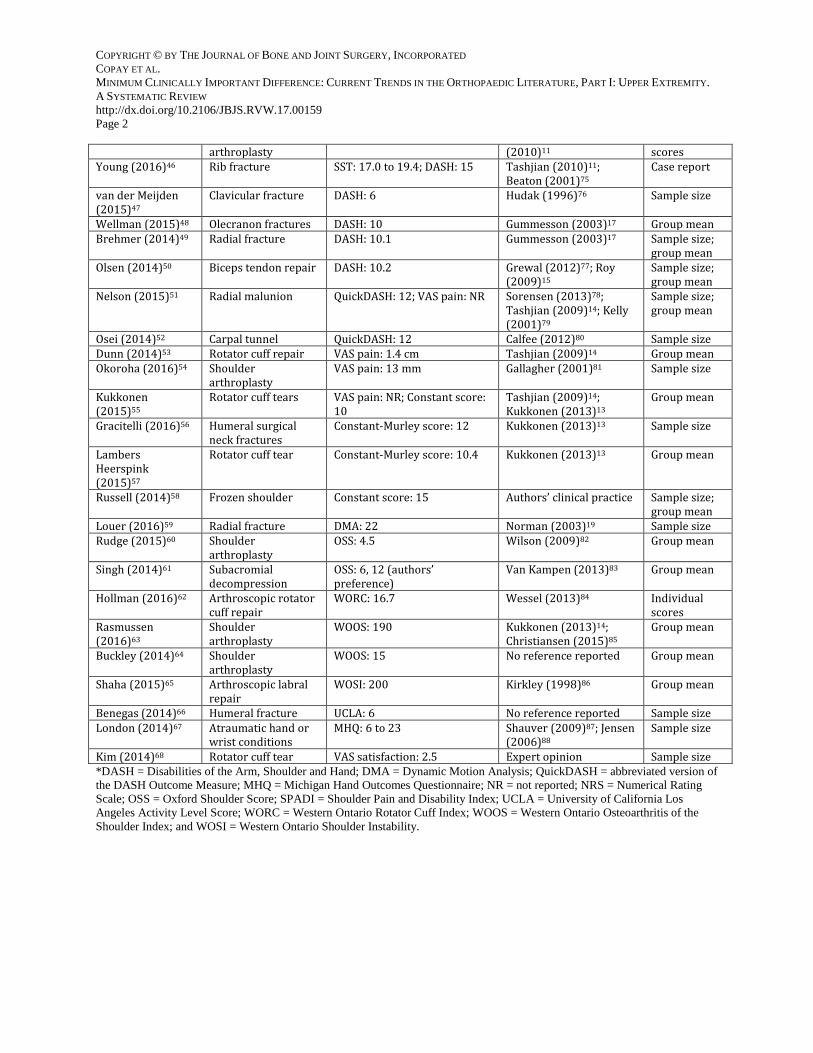
Studies That Used Published MCIDValues as a GaugeFor studies that used a previously pub-lished MCID value as a gauge for theirown data, the following elements of thatstudy were reported: the orthopaedicsubspecialty, thePROMused, theMCIDvalue and the corresponding article(s)referenced, and how theMCID was usedin the study. The MCID had 3 possibleuses: (1) sample size: studies based theirpower analysis on previously reportedMCID values to determine the sample
size required to detect a change in scoreor a difference between groups equal totheMCIDvalue; (2)groupmeans: studiescompared the mean score improvementin their sample to the previously reportedMCID; and (3) individual scores: studiescalculated the proportion of patientswhose score improvement reached apreviously reported MCID.
Studies That Were Most FrequentlyReferencedPreviously published studies were citedas references by the studies using theMCID as a gauge. The most frequentlycited of these studies were analyzedsimilarly to the studies calculating theMCID and the following elements wereidentified: sample size, patient popula-tion, length of follow-up, PROM used,MCID calculation method utilized,MCID value, potential anchor, andmeasurement error.
ResultsIn total, 4,462 articles were reviewed.Ofthese, 1,709were clinical science articlesthat utilized PROMs as part of theirstudy design. A total of 129 (7.5%) ofthe 1,709 studies used or referenced theMCID to some extent; 52 (40.3%) of129 were related to the upper extremity(Fig.1).Five studies calculatednewMCIDvalues (TableI),47studiesusedtheMCIDas a gauge (see Appendix22-68, with anumberof source articles11-17,19,69-88), and7 studies were the most frequently cited inthe reviewed literature (Table II). Alto-gether, 11 studies calculated the MCID(5 studies calculated a newMCID and 6of the most frequently cited studies alsocalculated theMCID). These 11 studiesused a total of 6 different methods; theROC curve was the most frequentlyused method of MCID calculation.Only 2 studies showed estimates of themeasurement error; in both cases, theMCID was within the measurementerror12,15.MCID values were calculatedfor the Constant-Murley score, SimpleShoulder Test (SST), American Shoul-der and Elbow Surgeons (ASES) score,Short Form-12 (SF-12) items, and VASfor pain. Multiple calculations for the
same questionnaire yielded a wide rangeof MCID values, for example, 8 to 36points for the Constant-Murley scoreand 6.4 to 17 points for the ASES score.The reported MCID values used as agauge also varied noticeably. Altogether,MCID values were considered or werecalculated for 16 PROMs; 12 of thesewere joint-specific PROMs for theupper extremity.
When the MCID was used as agauge, 55.3% of studies compared themean score change between preoperativeand postoperative PROMscoreswith theMCID, 40.4% used the MCID to de-termine their sample size, and 10.6%showed theproportionofpatients in theirstudies who improved to the level oftheMCIDafter the studied intervention.A total of 28 different studies were citedas references for the MCID; of those,only 7 were cited more than once(Table II).
DiscussionThe current climate regarding theMCID is limited by disorganization anda general lack of a consensus agreementon its appropriate usage. This can cer-tainly be expected given themultitude offactors that contribute to variability inMCID values and what seems to be awidespread misunderstanding with re-gard to the fundamentals of MCIDusage. Further, the multiplicity ofPROMs, heterogeneity of publishedMCID values, and inconsistency in thecalculation of MCID have made inter-pretation and effective utilization of thispotentially powerful metric increasinglydifficult. Despite these obvious flaws,there nonetheless appears to be interestin this potentially powerful metric. Itcan be anticipated that this interest maypotentially grow given the current pro-gressive shift toward value-based care inour current health-care economy.
Based on our review, we identifiednumerous factors that further underminethe utility of the MCID and contributeto the general confusion that underliesMCID utilization. We will elaborate on 3of these concepts in this part of our 2-partdiscussion.
| MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y
6 SEPTEMBER 2018 · VOLUME 6, ISSUE 9 · e1
The first concept is MCID multi-plicity. Several factors are known tocontribute to themultiplicity ofMCIDs.First, the MCID is always PROM-specific. As such, as more PROMs aredeveloped to evaluate treatment results,the number of potential MCID valueswill likely increase. Second, for the samePROM, different calculation methodsyield variable MCIDs that may have upto a tenfold difference in values89. Fur-thermore, even the same calculationmethod may result in variable MCIDvalues depending on the characteristicsof the sample population, the underly-ing pathology being addressed, and thetreatment being studied4. Hence, theMCID should be calculated with asample that is sufficiently large to mini-mize the influence of atypical patients.Additionally, when theMCID is used asa gauge, the pathology or treatmentunder study should be similar to thepathology or treatment that was initiallyused to calculate the cited MCID value.
The second concept is beneficialcompared with detrimental change. Intheir seminal article, Jaeschke et al.2
defined theMCIDas a beneficial changebut proceeded to measure the MCID asany small change, be it improvement ordeterioration. A change of 1 to 3 pointsin either direction was considered aminimal change. The authors onlyconsidered themagnitude of the PROMscore change, without the direction ofthe change, so that negative changes didnot nullify positive changes in the meanPROM score change. A proportion ofMCID studies continue to incorporateworsening as part of the change to bemeasured but fail to take into accountthe direction of the change in theircalculation of the MCID9,11,12. Forinstance, themost citedMCID value forthe ASES score (6.4 points) is the dis-criminating value between patients whoimprove and those who get worse12 and,for that reason, fundamentally is not ameasure of beneficial change. Futurestudies should take care to incorporateonly beneficial changes into their cal-culation of the MCID. Readers shouldadditionally be mindful of this subtle
flawwhen deciding onwhether to utilizea previously published MCID.
The third concept is meaningfulcompared with random change. Mea-surement error is typically calculated asthe SEM; MDC90 5 2.33 SEM andMDC955 2.77 SEM. Some of the earlyMCID research set the MCID equal to1 SEM90,91. Since then, two schools ofthought have considered how theMCIDand the measurement error should relate.Oneopinion is that ameasurement error,such as the MDC, a statistically basedcalculation, is fundamentally differentfrom theMCIDand, as such, should notbe used as a measure of the MCID. Thelogic for this argument is as follows:although a calculated value of theMCIDmay be inside the range of measurementerror, this value may not necessarilyreflect a change that is unimportant tothe patient12,18,92. Yet another belief isthat MCID values should not be lowerthan the measurement error. This is alsoour current belief. The rationale for thisbelief is that it would be impossible todiscriminate between random andmeaningful change if theMCID value islower than the measurement error12.
Given the confusion, most authorscontinue to disregard the issue alto-gether. In our review, the measurementerror was not reported in 10 of the 12orthopaedic studies (Tables I and II).Although the relationship between theMCID and the measurement error hasnot been fully defined92, it is our rec-ommendation that a measure of themeasurement error nonetheless be re-ported in conjunction with the MCID.
In conclusion, a meaningful inter-est in the utility of the MCID has beendemonstrated in the upper-extremityorthopaedic literature. As mentionedpreviously, MCID values may varysubstantially on the basis of numerousfactors, including the underlying patientpopulation being studied, treatmentmodality, follow-up intervals, andmethod used to calculate the MCID.Unfortunately, the recent proliferationof both PROMs andMCID calculationmethods has created a climate of con-fusion. Consequently, although the
MCID, in theory, is certainly a poten-tially powerful metric, it seems asalthough an improved understanding ofthe fundamentals of the MCID iswarranted.
Additionally, numerous method-ological errors in the utilization of theMCID need to be addressed. Thesemethods should either be corrected orabandoned. Further, the type of changebeing measured should be clarified,whether beneficial or detrimental.Finally, until the ideal method of cal-culating the MCID is identified, werecommend that readers and cliniciansutilize the 4 following questions whencritically evaluating MCID values. (1)Is the measured change a true change? IftheMCIDvalue is less than theMDC95,the change in PROM score is likely arandom change. If the MDC95 is notreported, it is not possible to assesswhether the MCID represents a truechange. (2) Is the measured changeminimal? If MCID is calculated for pa-tients who report being much better orlargely improved, it is unlikely that theMCID represents a minimal change. (3)Is themeasured change important? If theMCID is calculated for patients whoreport no change, it is unlikely that thechange is important. Furthermore, ifpatients who report being worse areincluded in the calculation, the MCIDno longer represents a desirable change.(4) Is the sample used for calculating theMCID large and representative of aspecific pathology or treatment?
Furthermore, it has been our rec-ommendation that the MDC95 be re-ported in conjunction with the MCIDor utilized as a surrogate for the MCID.This, at the very least, ensures that thecalculated MCID value is at least free ofmeasurement error (i.e., it is not simplydue to random variation).
AppendixA table showing 2014 to 2016 upper-extremity articles using the MCID asa gauge is available with the onlineversion of this article as a data sup-plement at jbjs.org (http://links.lww.com/JBJSREV/A378).
MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y |
ORCID iD for A.G. Copay:0000-0002-3179-2587ORCID iD for A.S. Chung:0000-0003-3942-9595ORCID iD for B. Eyberg:0000-0002-9361-1964ORCID iD for N. Olmscheid:0000-0002-3970-7850ORCID iD for N. Chutkan:0000-0001-7751-9095ORCID iD for M.J. Spangehl:0000-0003-1090-9165
References1. Centers for Medicare & Medicaid Services.CMS quality measure development plan:supporting the transition to the Merit-basedIncentive Payment System (MIPS) and Alterna-tive Payment Models (APMs). 2016 May 2.https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/MACRA-MIPS-and-APMs/Final-MDP.pdf. Accessed 2018 Feb 16.
2. Jaeschke R, Singer J, Guyatt GH.Measurement of health status. Ascertaining theminimal clinically important difference. ControlClin Trials. 1989 Dec;10(4):407-15.
3.CopayAG, SubachBR,GlassmanSD,PollyDWJr, Schuler TC. Understanding the minimumclinically important difference: a review ofconcepts and methods. Spine J. 2007 Sep-Oct;7(5):541-6. Epub 2007 Apr 2.
4.ChungAS, CopayAG,OlmscheidN, CampbellD, Walker JB, Chutkan N. Minimum clinicallyimportant difference: Current trends in thespine literature. Spine (Phila Pa 1976). 2017 Jul15;42(14):1096-105.
5. Copay AG, Eyberg B, Chung AS, Zurcher KS,Chutkan N, Spangehl MG. Minimal clinicallyimportant difference: current trends in theorthopaedic literature, part II: lower extremity.Asystematic review. JBJS Rev. 2018 Sept;6(9):e2.
6.WongSE, ZhangAL, Berliner JL,MaCB, FeeleyBT. Preoperative patient-reported scores canpredict postoperative outcomes after shoulder
7. Holmgren T, Oberg B, Adolfsson L, BjornssonHallgren H, Johansson K. Minimal importantchanges in the Constant-Murley score inpatients with subacromial pain. J ShoulderElbow Surg. 2014 Aug;23(8):1083-90. Epub2014 Apr 13.
8. Castricini R, Longo UG, De Benedetto M,Loppini M, Zini R, Maffulli N, Denaro V.Arthroscopic-assisted latissimus dorsi transferfor the management of irreparable rotator cufftears: short-term results. J Bone Joint Surg Am.2014 Jul 16;96(14):e119.
9. Torrens C, Guirro P, Santana F. The minimalclinically important difference for function andstrength in patients undergoing reverseshoulder arthroplasty. J Shoulder Elbow Surg.2016 Feb;25(2):262-8. Epub 2015 Sep 28.
10. Somerson JS, Wirth MA. Self-assessed andradiographic outcomes of humeral headreplacement with nonprosthetic glenoidarthroplasty. J Shoulder Elbow Surg. 2015 Jul;24(7):1041-8. Epub 2015 Jan 1.
11. Tashjian RZ, Deloach J, Green A, PorucznikCA, Powell AP. Minimal clinically importantdifferences in ASES and simple shoulder testscores after nonoperative treatment of rotatorcuff disease. J Bone Joint Surg Am. 2010 Feb;92(2):296-303.
13. Kukkonen J, Kauko T, Vahlberg T, JoukainenA, Aarimaa V. Investigating minimal clinicallyimportant difference for Constant score inpatients undergoing rotator cuff surgery. JShoulder Elbow Surg. 2013 Dec;22(12):1650-5.Epub 2013 Jul 12.
14. TashjianRZ,Deloach J, PorucznikCA, PowellAP. Minimal clinically important differences(MCID) and patient acceptable symptomaticstate (PASS) for visual analog scales (VAS)measuring pain in patients treated for rotatorcuff disease. J Shoulder Elbow Surg. 2009 Nov-Dec;18(6):927-32. Epub 2009 Jun 16.
15. Roy JS, MacDermid JC, Woodhouse LJ.Measuring shoulder function: a systematicreview of four questionnaires. Arthritis Rheum.2009 May 15;61(5):623-32.
16. Roy JS, Macdermid JC, Faber KJ,Drosdowech DS, Athwal GS. The simpleshoulder test is responsive in assessing changefollowing shoulder arthroplasty. J OrthopSports Phys Ther. 2010 Jul;40(7):413-21.
17. Gummesson C, Atroshi I, Ekdahl C. Thedisabilities of the arm, shoulder and hand(DASH) outcome questionnaire: longitudinalconstruct validity and measuring self-ratedhealth change after surgery. BMC Muscu-loskelet Disord. 2003 Jun 16;4:11. Epub 2003Jun 16.
18. de Vet HC, Ostelo RW, Terwee CB, van derRoer N, Knol DL, Beckerman H, Boers M, BouterLM. Minimally important change determinedby a visual method integrating an anchor-based and a distribution-based approach. QualLife Res. 2007 Feb;16(1):131-42. Epub 2006 Oct11.
19. Norman GR, Sloan JA, Wyrwich KW.Interpretation of changes in health-relatedqualityof life: the remarkableuniversalityofhalf
a standarddeviation.MedCare. 2003May;41(5):582-92.
20. Hagg O, Fritzell P, Nordwall A; SwedishLumbar Spine Study Group. The clinicalimportance of changes in outcome scores aftertreatment for chronic lowbackpain. Eur Spine J.2003 Feb;12(1):12-20. Epub 2002 Oct 24.
21. Beaton DE. Understanding the relevance ofmeasured change through studies ofresponsiveness. Spine (Phila Pa 1976). 2000Dec15;25(24):3192-9.
23. Shannon SF, Wagner ER, Houdek MT, CrossWW 3rd, Sanchez-Sotelo J. Reverse shoulderarthroplasty for proximal humeral fractures:outcomes comparing primary reversearthroplasty for fracture versus reversearthroplasty after failed osteosynthesis. JShoulder Elbow Surg. 2016 Oct;25(10):1655-60.Epub 2016 Apr 18.
24.Denard PJ, LadermannA. Immediate versusdelayedpassive rangeofmotion following totalshoulder arthroplasty. J Shoulder Elbow Surg.2016 Dec;25(12):1918-24. Epub 2016 Oct 7.
25. Chalmers PN, Saltzman BM, Feldheim TF,Mascarenhas R, Mellano C, Cole BJ, Romeo AA,Nicholson GP. A comprehensive analysis ofpectoralismajor transfer for long thoracic nervepalsy. J Shoulder Elbow Surg. 2015 Jul;24(7):1028-35. Epub 2015 Feb 2.
26. Li F, Zhu Y, Lu Y, Liu X, Wu G, Jiang C.Hemiarthroplasty for the treatment of complexproximal humeral fractures: does a trabecularmetal prosthesis make a difference? Aprospective, comparative study with aminimum 3-year follow-up. J Shoulder ElbowSurg. 2014 Oct;23(10):1437-43.
27. Athwal GS, MacDermid JC, Reddy KM,Marsh JP, Faber KJ, Drosdowech D. Does bonyincreased-offset reverse shoulder arthroplastydecrease scapular notching? J Shoulder ElbowSurg. 2015Mar;24(3):468-73. Epub 2014 Oct 22.
28.ChanK,MacDermid JC,HoppeDJ,AyeniOR,Bhandari M, Foote CJ, Athwal GS. Delayedversus early motion after arthroscopic rotatorcuff repair: a meta-analysis. J Shoulder ElbowSurg. 2014 Nov;23(11):1631-9. Epub 2014Aug 13.
29. Vavken P, Tepolt FA, Kocher MS. Openinferior capsular shift for multidirectionalshoulder instability in adolescents withgeneralized ligamentous hyperlaxity or Ehlers-Danlos syndrome. J Shoulder Elbow Surg. 2016Jun;25(6):907-12. Epub 2016 Jan 14.
30.AbramsGD,GuptaAK,HusseyKE, Tetteh ES,Karas V, Bach BR Jr, Cole BJ, Romeo AA, VermaNN. Arthroscopic repair of full-thickness rotatorcuff tears with and without acromioplasty:randomized prospective trial with 2-year fol-low-up. Am J Sports Med. 2014 Jun;42(6):1296-303. Epub 2014 Apr 14.
31. Steen BM, Cabezas AF, Santoni BG, HusseyMM, Cusick MC, Kumar AG, Frankle MA.Outcome and value of reverse shoulderarthroplasty for treatment of glenohumeralosteoarthritis: a matched cohort. J ShoulderElbowSurg. 2015 Sep;24(9):1433-41. Epub 2015Mar 11.
32. Kruse LM, Yamaguchi K, Keener JD,Chamberlain AM. Clinical outcomes afterdecompression of the nerve to the teres minor
| MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y
in patients with idiopathic isolated teres minorfatty atrophy. J Shoulder Elbow Surg. 2015 Apr;24(4):628-33. Epub 2014 Oct 29.
33. Pappou I, Virani NA, Clark R, Cottrell BJ,Frankle MA. Outcomes and costs of reverseshoulder arthroplasty in the morbidly obese: acase control study. J Bone Joint Surg Am. 2014Jul 16;96(14):1169-76.
34. LeBlanc JE, MacDermid JC, Faber KJ,Drosdowech DS, Athwal GS. Outcomes afterhemiarthroplasty for proximal humerusfracture are significantly affected by handdominance. J Orthop Trauma. 2015 Aug;29(8):379-83.
36. Miller RM, Popchak A, Vyas D, Tashman S,Irrgang JJ, Musahl V, Debski RE. Effects ofexercise therapy for the treatment ofsymptomatic full-thickness supraspinatus tearson in vivo glenohumeral kinematics. J ShoulderElbow Surg. 2016 Apr;25(4):641-9. Epub 2015Nov 24.
37. Huang H, Grant JA, Miller BS, Mirza FM,Gagnier JJ. A systematic review of thepsychometric properties of patient-reportedoutcome instruments for use in patients withrotator cuff disease. Am J Sports Med. 2015 Oct;43(10):2572-82. Epub 2015 Jan 26.
38. Keener JD, Galatz LM, Teefey SA, MiddletonWD, Steger-May K, Stobbs-Cucchi G, Patton R,Yamaguchi K. A prospective evaluation ofsurvivorship of asymptomatic degenerativerotator cuff tears. J Bone Joint Surg Am. 2015Jan 21;97(2):89-98.
39.Wylie JD, Suter T, Potter MQ, Granger EK,Tashjian RZ. Mental health has a strongerassociation with patient-reported shoulderpain and function than tear size in patients withfull-thickness rotator cuff tears. J Bone JointSurg Am. 2016 Feb 17;98(4):251-6.
40. Rubright J, Kelleher P, Beardsley C, Paller D,Shackford S, Beynnon B, Shafritz A. Long-termclinical outcomes, motion, strength, andfunction after total claviculectomy. J ShoulderElbow Surg. 2014 Feb;23(2):236-44. Epub 2013Aug 12.
41. Russell RD, Knight JR, Mulligan E, KhazzamMS. Structural integrity after rotator cuff repairdoes not correlate with patient function andpain: a meta-analysis. J Bone Joint Surg Am.2014 Feb 19;96(4):265-71.
42. Moosmayer S, Lund G, Seljom US,Haldorsen B, Svege IC, Hennig T, Pripp AH,Smith HJ. Tendon repair compared withphysiotherapy in the treatment of rotator cufftears: a randomized controlled study in 103cases with a five-year follow-up. J Bone JointSurg Am. 2014 Sep 17;96(18):1504-14.
43. Shields E, Mirabelli M, Amsdell S, ThorsnessR, Goldblatt J, MaloneyM, Voloshin I. Functionaland imaging outcomes of arthroscopicsimultaneous rotator cuff repair and bankartrepair after shoulder dislocations. Am J SportsMed. 2014 Nov;42(11):2614-20. Epub 2014Sep 26.
44. Hsu JE, Gorbaty JD, Whitney IJ, Matsen FA3rd. Single-stage revision is effective for failedshoulder arthroplasty with positive cultures forPropionibacterium. J Bone Joint Surg Am. 2016Dec 21;98(24):2047-51.
45. Hartzler RU, Steen BM, Hussey MM, CusickMC, Cottrell BJ, Clark RE, Frankle MA. Reverse
shoulder arthroplasty for massive rotator cufftear: risk factors for poor functionalimprovement. J Shoulder Elbow Surg. 2015Nov;24(11):1698-706. Epub 2015 Jul 11.
46. Young BL, Watson SL, Meyer RD, Ponce BA.Nonunion of first rib fracture in a softball player:case report of a rare cause of thoracic outletsyndrome. J Shoulder Elbow Surg. 2016 Nov;25(11):e353-7.
47. van der Meijden OA, Houwert RM,Hulsmans M, Wijdicks FJ, Dijkgraaf MG,Meylaerts SA, Hammacher ER, Verhofstad MH,Verleisdonk EJ. Operative treatment ofdislocatedmidshaft clavicular fractures:plateorintramedullary nail fixation? A randomizedcontrolled trial. J Bone Joint Surg Am. 2015 Apr15;97(8):613-9.
48.Wellman DS, Lazaro LE, Cymerman RM,Axelrad TW, Leu D, Helfet DL, Lorich DG.Treatment of olecranon fractures with 2.4- and2.7-mm plating techniques. J Orthop Trauma.2015 Jan;29(1):36-43.
49. Brehmer JL, Husband JB. Acceleratedrehabilitation compared with a standardprotocol after distal radial fractures treatedwithvolar open reduction and internal fixation: aprospective, randomized, controlled study. JBone Joint Surg Am. 2014Oct 1;96(19):1621-30.
50. Olsen JR, Shields E, Williams RB, Miller R,MaloneyM, Voloshin I. A comparison of corticalbutton with interference screw versus sutureanchor techniques for distal biceps brachiitendon repairs. J Shoulder Elbow Surg. 2014Nov;23(11):1607-11. Epub 2014 Sep 11.
51. Nelson GN, Stepan JG, Osei DA, Calfee RP.The impact of patient activity level on wristdisability after distal radius malunion in olderadults. J Orthop Trauma. 2015 Apr;29(4):195-200.
52. Osei DA, Calfee RP, Stepan JG, Boyer MI,Goldfarb CA, Gelberman RH. Simultaneousbilateral or unilateral carpal tunnel release? Aprospective cohort studyofearly outcomes andlimitations. J Bone Joint Surg Am. 2014 Jun 4;96(11):889-96. Epub 2014 Jun 4.
53. Dunn WR, Kuhn JE, Sanders R, An Q,Baumgarten KM, Bishop JY, Brophy RH, Carey JL,Holloway GB, Jones GL, Ma CB, Marx RG, McCartyEC, Poddar SK, Smith MV, Spencer EE, Vidal AF,Wolf BR, Wright RW. Symptoms of pain do notcorrelate with rotator cuff tear severity: a cross-sectional study of 393 patients with a sympto-matic atraumatic full-thickness rotator cuff tear. JBone Joint SurgAm. 2014May21;96(10):793-800.
54. Okoroha KR, Lynch JR, Keller RA, Korona J,Amato C, Rill B, Kolowich PA,Muh SJ. Liposomalbupivacaine versus interscalene nerveblock forpain control after shoulder arthroplasty: aprospective randomized trial. J Shoulder ElbowSurg. 2016Nov;25(11):1742-8. Epub2016 Jul 14.
55.Kukkonen J, JoukainenA, LehtinenJ,MattilaKT, Tuominen EK, Kauko T, Aarimaa V.Treatment of nontraumatic rotator cuff tears: arandomized controlled trial with two years ofclinical and imaging follow-up. J Bone JointSurg Am. 2015 Nov 4;97(21):1729-37.
56. Gracitelli ME, Malavolta EA, Assunção JH,KojimaKE, dosReis PR, Silva JS, FerreiraNetoAA,Hernandez AJ. Locking intramedullary nailscompared with locking plates for two- andthree-part proximal humeral surgical neckfractures: a randomized controlled trial. JShoulder Elbow Surg. 2016 May;25(5):695-703.
57. Lambers Heerspink FO, van Raay JJ,Koorevaar RC, van Eerden PJ, Westerbeek RE,van ’t Riet E, van den Akker-Scheek I, Diercks RL.
Comparing surgical repair with conservativetreatment for degenerative rotator cuff tears: arandomized controlled trial. J Shoulder ElbowSurg. 2015 Aug;24(8):1274-81.
58. Russell S, Jariwala A, Conlon R, Selfe J,Richards J, Walton M. A blinded, randomized,controlled trial assessing conservativemanagement strategies for frozen shoulder. JShoulder Elbow Surg. 2014 Apr;23(4):500-7.
59. Louer CR, Boone SL, Guthrie AK, Motley JR,Calfee RP, Wall LB. Postural stability in olderadults with a distal radial fracture. J Bone JointSurg Am. 2016 Jul 20;98(14):1176-82.
60. Rudge WB, Sewell MD, Al-Hadithy N,Wallace CN, Lambert SM. Shoulder linkedarthroplasty in patients with obstetricbrachial plexus palsy can improve quality oflife and function at short-term follow-up. JShoulder Elbow Surg. 2015 Sep;24(9):1473-80. Epub 2015 May 7.
61. Singh HP, Mehta SS, Pandey R. Apreoperative scoring system to select patientsfor arthroscopic subacromial decompression. JShoulder Elbow Surg. 2014 Sep;23(9):1251-6.
62. Hollman F, Wessel RN, Wolterbeek N.Response shift of the Western Ontario RotatorCuff index in patients undergoing arthroscopicrotator cuff repair. J Shoulder Elbow Surg. 2016Dec;25(12):2011-8. Epub 2016 Jul 14.
63. Rasmussen JV, Olsen BS, Al-Hamdani A,Brorson S. Outcome of revision shoulderarthroplasty after resurfacing hemiarthroplastyin patients with glenohumeral osteoarthritis. JBone Joint Surg Am. 2016 Oct 5;98(19):1631-7.
64. Buckley T, Miller R, Nicandri G, Lewis R,Voloshin I. Analysis of subscapularis integrityand function after lesser tuberosity osteotomyversus subscapularis tenotomy in totalshoulder arthroplasty using ultrasound andvalidated clinical outcome measures. JShoulder Elbow Surg. 2014 Sep;23(9):1309-17.Epub 2014 Mar 4.
65. Shaha JS, Cook JB, Song DJ, Rowles DJ,Bottoni CR, Shaha SH, Tokish JM. Redefining“critical” bone loss in shoulder instability:functional outcomes worsen with “subcritical”bone loss. Am J Sports Med. 2015 Jul;43(7):1719-25. Epub 2015 Apr 16.
66. Benegas E, Ferreira Neto AA, Gracitelli ME,Malavolta EA, Assunção JH, Prada FdeS, BolligerNeto R, Mattar R Jr. Shoulder function aftersurgical treatment of displaced fractures of thehumeral shaft: a randomized trial comparingantegrade intramedullary nailing withminimally invasive plate osteosynthesis. JShoulder Elbow Surg. 2014 Jun;23(6):767-74.Epub 2014 Apr 24.
67. LondonDA,StepanJG,BoyerMI,CalfeeRP.Theimpactofdepressionandpaincatastrophizationoninitial presentation and treatment outcomes foratraumatic hand conditions. J Bone Joint Surg Am.2014 May 21;96(10):806-14.
68. Kim HM, Caldwell JM, Buza JA, Fink LA,Ahmad CS, Bigliani LU, Levine WN. Factorsaffecting satisfaction and shoulder function inpatients with a recurrent rotator cuff tear. JBone Joint Surg Am. 2014 Jan 15;96(2):106-12.
69. Michener LA, Snyder AR, Leggin BG.Responsiveness of the numeric pain ratingscale in patients with shoulder pain and theeffect of surgical status. J Sport Rehabil. 2011Feb;20(1):115-28.
70.KirkleyA,Griffin S,DaintyK. Scoring systemsfor the functional assessment of the shoulder.Arthroscopy. 2003 Dec;19(10):1109-20.
MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y |
SEPTEMBER 2018 · VOLUME 6, ISSUE 9 · e1 9
71. Schmitt JS,Di Fabio RP. Reliable changeandminimum important difference (MID)proportions facilitated group responsivenesscomparisonsusing individual threshold criteria.J Clin Epidemiol. 2004 Oct;57(10):1008-18.
72. MacDermid JC, Drosdowech D, Faber K.Responsiveness of self-report scales in patientsrecovering from rotator cuff surgery. J ShoulderElbow Surg. 2006 Jul-Aug;15(4):407-14.
73.Wright RW, Baumgarten KM. Shoulderoutcomes measures. J Am Acad Orthop Surg.2010 Jul;18(7):436-44.
74. Smith MV, Calfee RP, Baumgarten KM,Brophy RH, Wright RW. Upper extremity-specific measures of disability and outcomes inorthopaedic surgery. J Bone Joint Surg Am.2012 Feb 1;94(3):277-85.
75. Beaton DE, Katz JN, Fossel AH, Wright JG,Tarasuk V, Bombardier C. Measuring the wholeor the parts? Validity, reliability, andresponsiveness of the Disabilities of the Arm,Shoulder and Hand outcome measure indifferent regions of the upper extremity. J HandTher. 2001 Apr-Jun;14(2):128-46.
76. Hudak PL, Amadio PC, Bombardier C; TheUpper Extremity Collaborative Group (UECG).Development of an upper extremity outcomemeasure: the DASH (disabilities of the arm,shoulder and hand) [corrected] [corrected]. AmJ Ind Med. 1996 Jun;29(6):602-8.
77. Grewal R, Athwal GS, MacDermid JC, FaberKJ, DrosdowechDS, El-Hawary R, KingGJ. Singleversus double-incision technique for the repairof acute distal biceps tendon ruptures: a ran-domized clinical trial. J Bone Joint Surg Am.2012 Jul 3;94(13):1166-74.
78. Sorensen AA, Howard D, Tan WH,Ketchersid J, Calfee RP. Minimal clinicallyimportant differences of 3 patient-rated out-comes instruments. J Hand Surg Am. 2013 Apr;38(4):641-9. Epub 2013 Mar 6.
79.KellyAM.Theminimumclinically significantdifference in visual analogue scale pain scoredoesnot differwith severity of pain. EmergMedJ. 2001 May;18(3):205-7.
80. Calfee RP, Adams AA. Clinical research andpatient-rated outcome measures in hand sur-gery. J Hand Surg Am. 2012 Apr;37(4):851-5.
81. Gallagher EJ, Liebman M, Bijur PE.Prospective validation of clinically importantchanges in pain severity measured on a visualanalog scale. Ann Emerg Med. 2001 Dec;38(6):633-8.
82.Wilson J, Baker P, Rangan A. Is retrospectiveapplication of the Oxford Shoulder Score valid?J Shoulder Elbow Surg. 2009 Jul-Aug;18(4):577-80. Epub 2009 May 7.
83. van Kampen DA,WillemsWJ, van Beers LW,Castelein RM, Scholtes VA, Terwee CB.Determination and comparison of the smallestdetectable change (SDC) and the minimalimportant change (MIC) of four-shoulderpatient-reportedoutcomemeasures (PROMs). JOrthop Surg Res. 2013 Nov 14;8:40.
86. Kirkley A, Griffin S, McLintock H, Ng L. Thedevelopment and evaluation of a disease-specific quality of life measurement tool forshoulder instability. The Western OntarioShoulder Instability Index (WOSI). Am J SportsMed. 1998 Nov-Dec;26(6):764-72.
87. Shauver MJ, Chung KC. The minimalclinically important difference of the Michiganhandoutcomes questionnaire. J Hand SurgAm.2009 Mar;34(3):509-14.
88. Jensen MP, Gammaitoni AR, Olaleye DO,Oleka N, Nalamachu SR, Galer BS. The painquality assessment scale: assessment of painquality in carpal tunnel syndrome. J Pain. 2006Nov;7(11):823-32.
89. Copay AG, Glassman SD, Subach BR, BervenS, Schuler TC, Carreon LY. Minimum clinicallyimportant difference in lumbar spine surgerypatients: a choice of methods using theOswestry Disability Index, Medical OutcomesStudy questionnaire Short Form 36, and painscales. Spine J. 2008 Nov-Dec;8(6):968-74. Epub2008 Jan 16.
90.Wyrwich KW, Nienaber NA, Tierney WM,Wolinsky FD. Linking clinical relevance andstatistical significance in evaluating intra-individual changes in health-related quality oflife. Med Care. 1999 May;37(5):469-78.
91.Wyrwich KW, Tierney WM, Wolinsky FD.Further evidence supporting an SEM-basedcriterion for identifying meaningful intra-individual changes in health-related quality oflife. J Clin Epidemiol. 1999 Sep;52(9):861-73.
92. de Vet HC, Terwee CB. The minimaldetectable change should not replace theminimal important difference. J Clin Epidemiol.2010 Jul;63(7):804-5, author reply :806.
93. Juniper EF, Guyatt GH, Willan A, Griffith LE.Determining a minimal important change in adisease-specific Quality of Life Questionnaire. JClin Epidemiol. 1994 Jan;47(1):81-7.
94. Gilmer BB, Comstock BA, Jette JL, WarmeWJ, Jackins SE, Matsen FA. The prognosis forimprovement in comfort and function after theream-and-run arthroplasty for glenohumeralarthritis: an analysis of 176 consecutive cases. JBone Joint Surg Am. 2012 Jul 18;94(14):e102.
| MC ID : Cu r r e n t Tr e n d s i n t h e O r t h o p a e d i c L i t e r a t u r e . Pa r t I : Up p e r E x t r em i t y
Benegas (2014)66 Humeral fracture UCLA: 6 No reference reported Sample size London (2014)67 Atraumatic hand or
wrist conditions MHQ: 6 to 23 Shauver (2009)87; Jensen
(2006)88 Sample size
Kim (2014)68 Rotator cuff tear VAS satisfaction: 2.5 Expert opinion Sample size *DASH = Disabilities of the Arm, Shoulder and Hand; DMA = Dynamic Motion Analysis; QuickDASH = abbreviated version of the DASH Outcome Measure; MHQ = Michigan Hand Outcomes Questionnaire; NR = not reported; NRS = Numerical Rating Scale; OSS = Oxford Shoulder Score; SPADI = Shoulder Pain and Disability Index; UCLA = University of California Los Angeles Activity Level Score; WORC = Western Ontario Rotator Cuff Index; WOOS = Western Ontario Osteoarthritis of the Shoulder Index; and WOSI = Western Ontario Shoulder Instability.