Surgical Management of the Neck for Minor SalivaryGland Malignancies
The Role of Radiation Therapy in the Management ofMinor Salivary Gland Malignancies
The Role of Chemotherapy in the Management of MinorSalivary Gland Malignancies
SummaryReferences
Introduction
The evaluation, diagnosis, and treatment of apatient with a mass occupying the territory ofminor salivary gland tissue in the palate, buccalmucosa, or lips, represent intellectually stimulatingdisciplines. This statement is clearly derived fromthe relative paucity of lesions in these anatomicareas. Salivary gland tumors in general are quiterare, accounting for only 0.2–6.6% of all human
tumors (Chidzonga, et al. 1995). Both geographicand racial factors may explain the relative paucityof these tumors (Ansari 2007). The average annualincidence of salivary gland tumors per 100,000population is 4.7 for benign tumors and 0.9 formalignant tumors (Ansari 2007). Both neoplas-tic and non-neoplastic entities are diagnosed inthe salivary glands, including the minor salivaryglands, thereby adding to the stimulating nature ofthe differential diagnosis, microscopic diagnosis,and treatment of minor salivary gland tumors. Dataregarding the incidence of salivary gland tumorsin general may be difficult to obtain. This is notonly due to the rarity of these tumors, but alsoto the previous non-routine nature of reporting ofthese diagnoses to hospital tumor registries, andthe occasional treatment of these lesions in officesettings (Melrose 1994). It has been estimated thatminor salivary gland tumors account for only 2–5%of all head and neck tumors, with malignant minorsalivary gland tumors accounting for only 2–4%of all head and neck cancers (MacIntosh 1995). In1985, Regezi, et al. reported on 238 minor salivarygland tumors amongst 72,282 (0.33%) total oralbiopsy specimens diagnosed over a 19-year period(Regezi, et al. 1985). Similarly, Rivera-Bastidas,et al. reported 62 minor salivary gland tumorsfrom a total of 9000 oral biopsies (0.7%) during a24-year period (1996). A review of 40,000 head andneck tumors over a 40-year period of time revealed196 (0.5%) minor salivary gland tumors. Approx-imately 10% of all salivary gland tumors arisein the minor glands (Ord 1994). Of these minorsalivary gland tumors, 70% occur in the oral cavity,25% in the nasal cavity/sinuses/nasopharynx, and3% occur in the larynx (MacIntosh 1995). Of theoral minor salivary gland tumors, at least 50%have been diagnosed in the palate, according to
281
�
� �
�
282 Chapter 11
most large series (Eveson and Cawson 1985; Spiro1986). In addition to relatively low numbers ofminor salivary gland tumor diagnoses, there arecontroversies regarding the precise microscopicdiagnosis of these tumors. In Waldron et al.’sreview of 426 oral minor salivary gland tumors(Waldron, et al. 1988), each of these cases werereviewed by the three authors and complete con-currence of the microscopic diagnoses was reachedin 346 cases (81.2%). In 49 cases, there were minordisagreements as to the diagnoses, mainly relatedto the subclassification of the tumors. Significantdisagreement, regarding a benign versus malignantdiagnosis of the neoplasm, was noted in 21 cases(5%). Moreover, following the authors’ review,their diagnoses were compared to those of thecontributing pathologists. There was completeagreement in 374 cases (87.8%). These statisticsexemplify the complex nature of intraoral minorsalivary gland tumors, thereby questioning theexact incidence of these neoplasms as a whole aswell as specific diagnoses in particular.
Minor salivary gland tumors occur not onlyas benign and malignant entities, but also as aspectrum of cell types within these glands (Carlson1998). The frequency of benign versus malignanttumors occurring throughout the minor glands inthe oral cavity is one feature that distinguishesthese tumors from their counterparts in the majorglands. One series reported 15% of parotid glandtumors and 37% of submandibular gland tumorsto be malignant (Eveson and Cawson 1985). Ingeneral terms, published series record that approx-imately 20–70% of minor salivary gland tumorsare malignant (Ord 1994; Epker and Henny 1969)(Table 11.1). It seems that the center that reportsthe incidence of benign versus malignant minorsalivary gland tumors of the oral cavity is theprimary bias in these reports. For example, tertiarycare referral centers with a cancer initiative maybe preferentially referred patients with malignantdiagnoses. Spiro’s report of his 35 year experiencewith salivary gland neoplasia at Memorial SloanKettering Cancer Center is a case in point. Hereported on 2807 patients, 607 of whom had minorsalivary gland tumors. The frequency of malig-nant tumors in this report was 87%. The ArmedForces Institute of Pathology reported 2945 cases ofminor salivary gland tumors in 1991. By contrast,49% of these cases were malignant. Numerousother series have reported similar figures, suchthat it has become reasonably well acceptedthat approximately 50% of minor salivary gland
tumors of the oral cavity are benign and 50% aremalignant.
Etiology of Minor Salivary GlandTumors
Risk factors for salivary gland tumors have beenstudied extensively. Carcinoma of the majorsalivary glands, for example, has identified arelationship with prior radiation therapy and pre-vious skin cancer (Spitz, et al. 1984). Anotherstudy reported 31 patients who had both a newlydiagnosed salivary gland tumor and a history ofradiation therapy to the head and neck region(Katz and Preston-Martin 1984). Radiation therapyhad been administered with a range of 11–66years prior to the development of the salivarygland tumors. No course of radiation therapy wasadministered for a malignant condition, but ratherfor acne, hypertrophied tonsils, keloids, and otherbenign conditions. As such, it is reasonable toassume that a low dose of radiation therapy wasadministered. Only three cases of minor salivarygland tumors were identified among these 31 cases,including two adenoid cystic carcinomas and onemucoepidermoid carcinoma. One of the tumorswas located in the palate and two were located inthe cheek/retromolar region.
Benign and malignant salivary gland tumorshave also been linked to exposure to ionizing radi-ation related to the atomic bombings in Hiroshimaand Nagasaki during World War II. One hundredand forty-five salivary gland tumors have beenstudied in survivors of these bombings (Saku,et al. 1997). One hundred and nineteen majorgland tumors (27 malignant tumors, 82 benigntumors, 10 undetermined tumors) and 26 minorgland tumors (14 malignant tumors, 12 benigntumors) were identified. Among the 41 malignanttumors, the frequency of mucoepidermoid carci-noma was disproportionately high, and among the94 benign tumors, the frequency of the Warthintumor was high.
The association between first primary benignand malignant neoplasms of the salivary glandsand the subsequent development of breast cancerhas also been investigated (Abbey, et al. 1984).This study identified a fourfold to fivefold increasedrisk of a second primary breast cancer subsequentto the first salivary gland tumor. Of note is thatall of the primary salivary gland tumors were ofthe major glands and three of the four patients
�
� �
�
Minor Salivary Gland Tumors 283
Table 11.1. Incidence of minor salivary gland tumors
Authors Year Location Number of Cases Histology
AFIP (Ellis and Auclair 1991a) 1991 USA 2945 Benign 51%Malignant 49%
Ansari 2007 Iran 18 Benign 11.1%Malignant 88.9%
Chau and Radden 1986 Australia 98 Benign 62%Malignant 38%
Chidzonga, et al. 1995 Zimbabwe 282 Benign 80%Malignant 20%
Dhanuthai, et al. 2009 Thailand 311 Benign 47.3%Malignant 52.7%
Eveson and Cawson 1985 England 336 Benign 54%Malignant 46%
Isacsson and Shear 1983 Sweden 201 Benign 28%Malignant 72%
Ito, et al. 2005 Brazil 113 Benign 37%Malignant 63%
Jabar 2006 Libya 75 Benign 39%Malignant 61%
Lopes, et al. 1999 Brazil 196 Benign 35%Malignant 65%
Potdar and Paymaster 1969 India 110 Benign 49%Malignant 51%
Regezi, et al. 1985 USA 238 Benign 65%Malignant 35%
Rivera-Bastidas, et al. 1996 Venezuela 62 Benign 55%Malignant 45%
Satko, et al. 2000 Slovakia 31 Benign 48%Malignant 52%
Spiro 1986 USA 607 Benign 13%Malignant 87%
Stuteville and Corley 1967 USA 80 Benign 10%Malignant 90%
Toida, et al. 2005 Japan 82 Benign 67%Malignant 33%
Waldron, et al. 1988 USA 426 Benign 58%Malignant 42%
described had benign salivary gland tumors. Whileno association between minor salivary gland neo-plasia and breast cancer was established, the studynonetheless attempted to develop a relationshipbetween salivary gland neoplasia and breast can-cer. Moreover, the study investigated subsequent
breast cancer in patients with a history of salivarygland neoplasia, rather than vice versa. As such,a risk factor for salivary gland tumor developmentwould not be established in patients with breastcancer. In addition, minor salivary gland neoplasiawas not represented in this cohort of patients.
�
� �
�
284 Chapter 11
In the final analysis, there is some evidence toidentify risk factors for the development of minorsalivary gland tumors, yet not as much evidence asexists for the development of major salivary glandtumors.
Diagnosis of Minor Salivary GlandTumors
The diagnosis of a minor salivary gland tumorbegins with the establishment of a differentialdiagnosis. This differential diagnosis should beclassified categorically and in order of decreas-ing likelihood (Carlson 1998). The evaluationof a lesion of the palate, lip, or buccal mucosamight suggest inflammatory, neoplastic, andnon-neoplastic entities. Ultimately, the differen-tial diagnosis is based on the patient’s history,physical examination, and the anatomic locationof the pathologic entity under scrutiny. Generallyspeaking, benign and malignant minor salivarygland tumors present as painless, slowly enlargingintraoral masses. When present, ulceration predictsa malignant diagnosis, although many minor sali-vary gland malignancies do not create ulcerationof the oral mucosa. Pain is an ominous sign andis associated with perineural invasion, typically byadenoid cystic carcinoma. A painful enlargementof the minor salivary glands is malignant untilproved otherwise. The presence or absence of paintherefore represents an important element of thepatient’s history. Special imaging studies may beobtained prior to performing the biopsy, if requiredat all, or they may be obtained after the establish-ment of a diagnosis based on incisional biopsy.Experience shows, however, that their purpose isto anatomically delineate the extent of the tumorrather than to assist in the establishment of thediagnosis. The experienced salivary gland surgeonmay detect nuances on imaging studies that favorvarious diagnoses on the differential diagnosis.While fine needle aspiration biopsy is an essentialpart of the diagnosis of parotid neoplasms, it hasno practical role in the diagnosis of minor salivarygland neoplasms. Rather, an incisional biopsyshould be routinely performed, for example, whenplanning treatment of palatal tumors due to thediverse nature of possible histopathologic diag-noses, as well as the diverse nature of surgicaltreatment plans based on these diagnoses.
Other minor salivary gland tumor sites, suchas the buccal mucosa and upper lip require greaterattention to the differential diagnosis in order todetermine whether incisional or excisional biopsybest serves the needs of the patient. In manyinstances, the differential diagnosis may stronglysupport a benign neoplasm such that proceedingdirectly to excision is the most appropriate therapy.For example, a tumor in the upper lip that is freelymoveable and associated with normal overlyingmucosa indicates that an excisional biopsy maybe performed in most instances due to the highlikelihood of a benign tumor. A minor salivarygland tumor of the buccal mucosa, similar to thepalate, has a diverse number of possibilities on thedifferential diagnosis such that an incisional biopsyshould be considered to establish the diagnosis(Table 11.2). There are instances, however, wherea freely moveable buccal mucosal tumor maybe excised without preceding incisional biopsy,similar to the upper lip tumor previously described.
Treatment of Minor Salivary GlandTumors
GENERAL PRINCIPLES OF SURGERY FORMINOR SALIVARY GLAND TUMORS
The treatment of minor salivary gland tumors isdistinctly surgical. The specific type of surgeryis a function of the anatomic site of the tumor,the invasion of surrounding structures, and thehistopathologic diagnosis provided that an inci-sional biopsy has been performed. In general terms,a palatal minor salivary gland tumor requires anincisional biopsy so as to definitively establishthe histopathologic diagnosis prior to the tumorsurgery. This biopsy should be performed in thecenter of the mass so as to not seed the surround-ing normal tissue (Freedman and Jones 1994). Thedecision as to whether to perform an incisionalbiopsy of buccal mucosal and lip masses thought torepresent minor salivary gland tumors rests on thesurgeon’s intuition as to the benign versus malig-nant nature of the mass. Smooth, freely moveablesubmucosal masses without fixation to the overly-ing mucosa are likely benign and may be treatedwith excisional biopsies without first performingan incisional biopsy due to the high likelihood of abenign process. By contrast, sizeable masses withmucosal fixation in these areas should probably
�
� �
�
Minor Salivary Gland Tumors 285
Table 11.2. Incidence of benign and malignant minor salivary gland tumors at various sites
be subjected to incisional biopsy so as to establishthe diagnosis due to the concern for malignant dis-ease. As with tumor surgery for other diagnoses,minor salivary gland tumor surgery requires apre-operative assessment of the anatomic barriers.Physical examination and imaging studies serveto delineate invasion of surrounding anatomicbarriers by the tumor. In the palate, for example,it is important to determine whether the palatalbone has been invaded by the tumor. Benigntumors typically do not invade bone, but may “cupit out.” In such situations, it is not necessary toresect bone. Malignant tumors of the palate displayvariable involvement of the palatal bone. Imaging
studies, particularly coronal bone windows, mustbe obtained so as to assess the involvement of theanatomic barrier of palatal bone. Minor salivarygland tumors of the upper lip and buccal mucosaexhibit different behavior regarding their invasionof the anatomic barrier of the surrounding mucosa.In general terms, it is appropriate to preserve themucosa surrounding a benign minor salivary glandtumor of these sites, while a malignant tumorsurgery in these sites requires sacrifice of thesurrounding mucosa (Table 11.3).
Treatment of minor salivary gland tumorsbecomes predicated on the histopathologic diagno-sis, which largely translates to the known biologic
�
� �
�
286 Chapter 11
Table 11.3. Management of the anatomic barriers in minor salivary gland tumor surgery
Site
Histology Palate Lip Buccal mucosa
Benign – Mucosal sacrificing– Periosteal sacrificing– Bone sparing
– Mucosal sparing– Muscle sparing– Skin sparing
– Mucosal sparing– Muscle sparing– Skin sparing
Malignant – Mucosal sacrificing– Periosteal sacrificing– Bone sacrificing (variable)
behavior of the neoplasm. Descriptive surgicalterms may describe the sacrifice of surroundingsoft and hard tissues as a matter of convenience(Carlson 1998). For example, surgical managementof palatal tumors may be as straight forward asa periosteal sacrificing, bone sparing wide localexcision with split thickness dissection of the softpalate. This specific surgical procedure is the mainprocedure performed for benign palatal tumorsand also has a role to play in some low-grademalignancies (Carlson 1998). The bone sparing,periosteally sacrificing wide local excision withfull thickness sacrifice of the soft palate is reservedfor deeply infiltrative low-grade malignancies ofthe palate. The most aggressive surgery for palatalminor salivary gland tumors is the maxillectomy,specifically reserved for the highly aggressiveminor salivary gland malignancies of the palate.
SURGICAL TREATMENT OF BENIGNMINOR SALIVARY GLAND TUMORS
The treatment of benign tumors of the minorsalivary glands centers on the pleomorphic ade-noma, with a brief discussion of the surgery forthe canalicular adenoma. The three most commonminor salivary gland anatomic sites will be consid-ered, including the palate, the lip, and the buccalmucosa.
Pleomorphic AdenomaThe terms pleomorphic adenoma and mixed tumorare equally satisfactory and interchangeable whendescribing this common minor salivary glandtumor. The designation mixed is based on thetumor’s mixtures of neoplastic elements such that
each mixed tumor has unique features (Melrose1994). It has also been pointed out that the designa-tion refers to the tumor showing combined featuresof epithelioid and connective tissue-like growth(Waldron 1991). There is universal agreement thatthe pleomorphic adenoma is the most commonsalivary gland tumor. The Armed Forces Instituteof Pathology data of 13,749 salivary gland tumorsshowed 6880 cases of pleomorphic adenoma ofwhich 4359 were located in the parotid gland and1277 were located in minor salivary gland tissue(Auclair, et al. 1991). The palate accounted for711 of these 6880 cases of pleomorphic adenoma(10.3%) and was the second most common sitefor this tumor in the AFIP data. The 711 cases inthe palate represent 56% of cases located in theminor salivary glands. Interestingly, the AFIP datasubclassified palatal pleomorphic adenomas intothose occurring on the hard palate (118 cases)and those occurring in the soft palate (110 cases).There were 483 cases that were not specified asto location in the palate. The subclassification ofspecific anatomic location in the palate is of signif-icance when working up these cases and planningsurgical treatment for these patients. Those pleo-morphic adenomas located primarily in the softpalate require investigation as to involvement ofthe parapharyngeal space.
Treatment of the palatal pleomorphic ade-noma is based on the realization that this tumordoes not possess a capsule. This notwithstand-ing, the tumor does exhibit a “pseudocapsule”represented by a loose fibrillar network surround-ing the tumor. In addition, the periosteum onthe superior aspect of the tumor does serve asa very competent anatomic barrier such thatpalatal bone may be preserved in this tumor
�
� �
�
Minor Salivary Gland Tumors 287
surgery, even when the bone has been “cuppedout” clinically and radiographically. Under suchcircumstances, the pleomorphic adenoma doesnot invade bone histologically such that boneresection is not warranted. In fact, it is reasonableto proceed with surgery without obtaining CTscans pre-operatively. A periosteally sacrificingwide local excision is performed, observing at leasta 5 mm linear margin surrounding the clinicallyapparent tumor (Figure 11.1). While these tumorsare submucosal in nature, the mucosa must besacrificed with the tumor due to the close proxim-ity of the tumor and the overlying mucosa (Yih,et al. 2005). The most appropriate linear marginof uninvolved soft tissue included at the peripheryof the tumor seems to be a source of controversy(Carlson 1998; Ord 1994; Pogrel 1994). The softpalate musculature is dissected in a split thicknessfashion so as to prevent an oral-nasal communi-cation. A preoperatively fabricated palatal stentprotects the exposed bone in the postoperativeperiod until granulation tissue appears on the bonesurface of the palate. There is no need to providereconstruction of this exposed bone surface, asmucosalization ultimately occurs predictably. Neg-ative soft tissue margins in the specimen predict acurative surgery without recurrence of the tumor(Beckhardt, et al. 1995).
As previously mentioned, the pleomorphicadenoma that develops in the soft palate may bedifferent from the pleomorphic adenoma of thehard palate, in so far as its anatomic progression isconcerned. Tumors located on the hard palate willgrow into the oral cavity (Figure 11.2), whereastumors of the soft palate (Figure 11.3) may descendinto the parapharyngeal space (Carlson 1998).As such, when considering the surgical treatmentfor a pleomorphic adenoma of the soft palate,the surgeon should obtain CT scans preopera-tively so as to determine possible involvementof the parapharyngeal space. When dissection ofthe parapharyngeal space by the tumor is noted,a combined transoral/transcutaneous approachto tumor extirpation is indicated. A mandibularosteotomy for effective dissection of the tumor bedand protection of the great vessels in the neck maybe indicated.
Pleomorphic adenomas are known to occurin other minor salivary gland sites, includingthe lip, buccal mucosa, and tongue. Lip tumorsaccounted for 297 cases in the AFIP files, of whicha majority occurred in the upper lip. Lower lip
pleomorphic adenomas are very rare. The buccalmucosa accounted for 126 cases in the AFIP series.The surgery required for removal of pleomorphicadenomas in the lip and buccal mucosa involvesan excision of the tumor and associated minorsalivary gland tissue. The plane of dissection is“peri-pseudocapsular” in nature. This ensures ananatomic barrier of fascia surrounding the tumor.These tumor surgeries are curative as long astumor spillage does not occur intraoperatively.Subtherapeutic ablation of these tumors in theform of an enucleation will certainly predisposethe patient to persistent disease. Such recurrenceswere noted to be multifocal in nature as originallydescribed in the major salivary glands (Foote andFrazell 1953).
Malignant pleomorphic adenomas of sali-vary gland origin are uncommon neoplasms. Thebroad heading, malignant mixed tumor, includesthree different clinical and pathologic entities:carcinoma ex. pleomorphic adenoma, carcinosar-coma, and metastasizing pleomorphic adenoma.Carcinoma ex.pleomorphic adenoma, perhaps themost commonly referenced malignant pleomorphicadenoma, is a pleomorphic adenoma in which asecond neoplasm develops from the epithelialcomponent that fulfills the criteria for malignancy.These features include invasiveness, destructionof normal tissues, cellular anaplasia, cellularpleomorphism, atypical mitoses, and abnormalarchitectural patterns (Gnepp and Wenig 1991).The Armed Forces Institute of Pathology datashowed 326 cases of carcinoma ex-pleomorphicadenoma which accounted for 2.4% of their 13,749cases. A significant majority of these tumors werelocated in the parotid gland (64.4%); however,these malignancies occurred in the minor salivaryglands, as well. The palate accounted for 36 of57 cases in the minor glands, with the upper lip(6 cases), tongue (4 cases), and cheek (4 cases)also represented. A review of this tumor showsthat preoperative duration of a benign pleomorphicadenoma is the main determining factor regard-ing malignant transformation. Specifically, theincidence of malignancy progressively increasesfrom 1.6% for tumors present for less than 5 yearsto 9.4% for tumors present for periods longerthan 15 years (Auclair, et al. 1991). The otherpredisposing condition for the development of thismalignancy is recurrence of a benign pleomorphicadenoma. This fact supports a curative approachto the pleomorphic adenoma from the outset, with
�
� �
�
288 Chapter 11
(a) (b)
(c) (d)
(e) (f)
Figure 11.1. The clinical appearance of a pleomorphic adenoma of the palate (a). An incisional biopsy was performed,and showed an acanthomatous variant of this tumor (b). A periosteal sacrificing, bone sparing wide local excision withsplit thickness sacrifice of the soft palate was performed with a 5–10 mm linear mucosal margins (c). In so doing, theperiosteum serves as the superior anatomic barrier on the specimen (d, e). The cut specimen (f) shows the characteristicappearance of a pleomorphic adenoma. The histopathology of the tumor specimen (g) shows the tumor approaching, butwell contained within the pseudocapsule. The remaining tissue bed (h) is covered with a surgical stent and allowed to healwith tertiary intention. No tissue coverage of the palate is required. The tissue bed is noted at 3 months (i) and 12 months(j) postoperatively. Effective mucosalization of the exposed bone surface of the hard palate and exposed muscle surface ofthe soft palate has occurred.
�
� �
�
Minor Salivary Gland Tumors 289
(g) (h)
(i) (j)
Figure 11.1. (Continued)
abandonment of the subtherapeutic enucleation ofthese tumors in the parotid gland or minor salivarygland tissues. The prognosis for this malignancy isgenerally considered dismal, with 71% of patientsexhibiting metastatic disease during the course oftheir disease.
Carcinosarcoma, also known as true malig-nant pleomorphic adenoma, is a tumor definedby histologic evidence of malignancy in both theepithelial and stromal elements of the tumor.These tumors are rarer than the carcinoma ex.pleomorphic adenoma, accounting for only eightcases in the AFIP registry, and none occurred in
the minor salivary glands. Other cases presentedin the literature do identify the existence of thisdiagnosis in the minor salivary glands.
Metastasizing mixed tumor is a histologicallybenign pleomorphic adenoma, but located in dis-tant sites. The pleomorphic adenomas are knownto arise in major as well as minor salivary glands,and the metastatic foci have been identified in thecervical lymph nodes, spine and liver (Auclair,et al. 1991). Data on the interval from removalof the primary tumor to the identification of thefirst metastasis is 1.5–51 years, with an average of16.6 years.
�
� �
�
290 Chapter 11
Figure 11.2. A large pleomorphic adenoma that is pri-marily located over the hard palate. As such, it is permit-ted to grow in an exophytic fashion, with cupping out ofthe palatal bone, but no involvement of the parapharyn-geal space. Reprinted with permission from: Carlson ER:Salivary gland pathology – Clinical perspectives and dif-ferential diagnosis, In: The Comprehensive Managementof Salivary Gland Pathology, Oral and Maxillofacial SurgeryClinics of North America 7, 361–386, WB Saunders Co.,1995.
Canalicular AdenomaThe canalicular adenoma is a benign tumor thathas a significant predilection for the upper lip(Figure 11.4). In the past, this tumor was morecommonly referred to as a monomorphic adenoma.Gardner recommended that the term monomorphicadenoma be used as a nosologic group of epithelialsalivary gland tumors that are not pleomorphic ade-nomas (Gardner and Daley 1983). The canalicularadenoma and basal cell adenoma identify specificforms of monomorphic adenomas (Daley, et al.1984). The canalicular adenoma classically occursin the upper lip in elderly women (Kratochvil 1991).In fact, canalicular adenomas typically affect anolder population compared to pleomorphic ade-nomas (Ord 1994). The canalicular adenoma istypically an asymptomatic, slow-growing, andfreely moveable mass that uncommonly exceeds2 cm in widest diameter. They may resemblemucoceles which are uncommonly located in theupper lip. Of the 121 canalicular adenomas in theAFIP files, 89 of them occurred in the upper lip.The second most common site was the buccalmucosa (Auclair, et al. 1991). The tumor is encap-sulated such that an excision of the tumor in anyanatomic site in a pericapsular fashion represents
a curative surgery provided that tumor spillagedoes not occur (Figure 11.5). The canalicular ade-noma is multifocal in 20% of cases (Ord 1994). Ifrecurrence is believed to have occurred, it mightactually represent a new primary tumor (Melrose1994).
SURGICAL TREATMENT OF MALIGNANTMINOR SALIVARY GLAND TUMORS
The malignant diagnoses in the minor salivaryglands are more diverse than their benign counter-parts. These malignant diagnoses may be low-gradeor high-grade, and most represent histopathologicdiagnostic challenges. As with the benign minorsalivary gland tumors, surgery represents thehallmark of therapy for malignant minor salivarygland tumors, and the principles of surgery havenot changed significantly over the past severaldecades (Bell, et al. 2005). In addition to eradi-cation of the primary malignancy, considerationshould be given for neck dissection in very specificcircumstances, as well as postoperative radiationtherapy in this cohort of patients.
Mucoepidermoid CarcinomaThe mucoepidermoid carcinoma is the secondmost common tumor of the salivary glands overall,the most common salivary gland malignancy over-all, and the most common minor salivary glandmalignancy (Auclair and Ellis 1991). During thegreater than 70 years since its first description, thisneoplasm has generated significant debate regard-ing the possible existence of a benign variant, theoptimal number of grades, and the proper treat-ment for certain minor salivary gland lesions. Theterm mucoepidermoid tumor was first introducedby Stewart, Foote, and Becker in 1945 in their pub-lication of 45 cases (Stewart, et al. 1945). In thisreport, only two grades were utilized, including rel-atively favorable (benign) and highly unfavorable(malignant) tumors. The authors indicated that theadjective benign was rarely ever applicable in anabsolute sense and as used in their report did notimply innocent behavior. It did indicate, however,that the authors had not observed metastasis fromthese tumors. The designation malignant indicateda histologic structure that was associated with theability to produce regional lymph node and distantmetastases. This notwithstanding, the authors
�
� �
�
Minor Salivary Gland Tumors 291
(a) (b)
(c) (d)
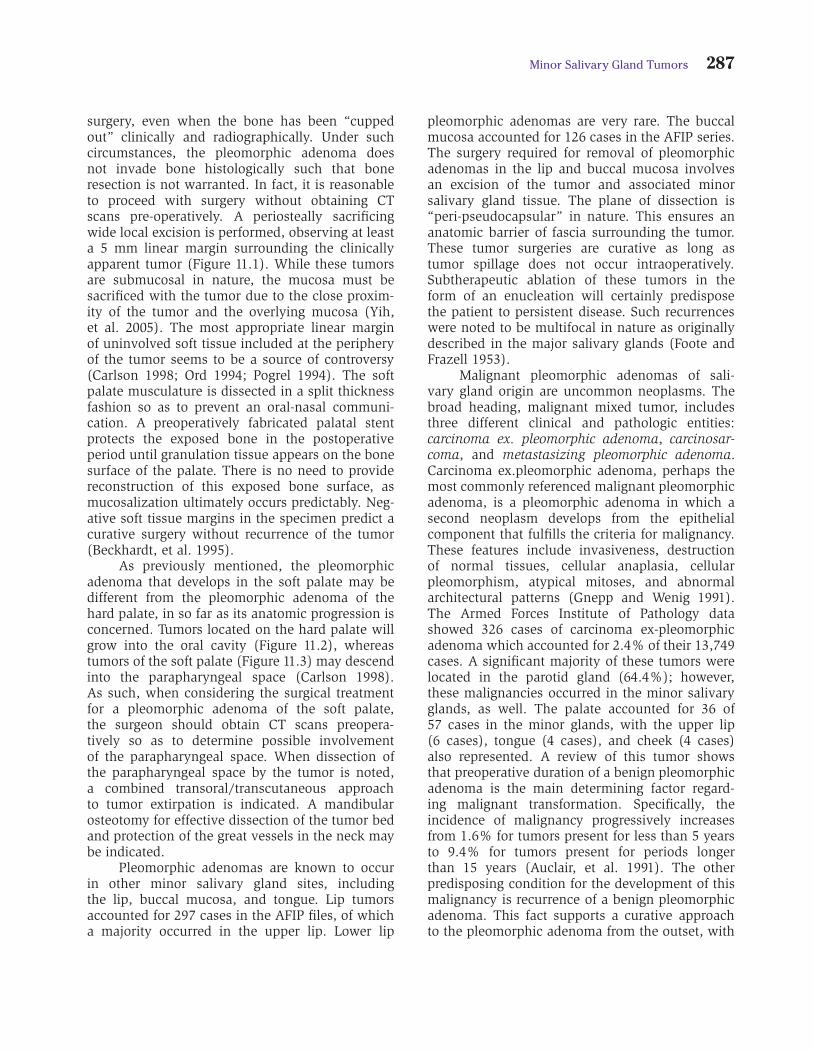
Figure 11.3. The clinical appearance of a pleomorphic adenoma that is located primarily in the soft palate (a). Its chronicgrowth permitted entry into the parapharyngeal space, as noted on CT scans (b, c). Due to the relative inability to dissectthis tumor bed entirely transorally, a decision was made to perform a combined transcutaneous and transoral approachto the tumor ablation with an Attia double osteotomy of the mandible. Wide transcutaneous access was accomplished forthis tumor surgery (d). Dissection of the mandible was performed in a subperiosteal fashion, while maintaining as muchperiosteum and muscle as possible on the lateral surface of the mandible (e). Bone plates were placed on the mandiblein preparation for the osteotomy (f). The plates were then removed and an Attia double osteotomy of the mandible wasperformed that involved a horizontal resection of the mandible superior to the mandibular foramen and a vertical resectionof the mandible anterior to the mental foramen. Superior reflection of the mandibular segment was then able to be accom-plished (g). Reflection of the medial surface of the medial pterygoid muscle permitted entry into the parapharyngeal spacewith identification of the tumor (h). With the great vessels of the neck protected, the tumor ablation continued intraorally withdevelopment of the tumor dissection surrounding the pseudocapsule (i). The combination of transcutaneous access andtransoral access permitted safe delivery of the specimen (j). Histopathology identified a pleomorphic adenoma with tumorpresent in the pseudocapsule, but with negative margins (k). Following delivery of the specimen, the plates are replacedon the mandible and closure occurred (l). The 6-month postoperative view of the palate is noted (m). This surgery providedcurative surgery for this patient’s tumor. Reprinted with permission from: Carlson ER, Schimmele SR: The management ofminor salivary gland tumors of the oral cavity, In: Surgical Management of Salivary Gland Disease, The Atlas of the Oral andMaxillofacial Surgery Clinics of North America 6:75–98, WB Saunders Co., 1998.
�
� �
�
292 Chapter 11
(i) (j)
(g) (h)
(e) (f)
Figure 11.3. (Continued)
�
� �
�
Minor Salivary Gland Tumors 293
(l) (m)
(k)
Figure 11.3. (Continued)
explicitly referred to and separated the benign andmalignant tumors in their series of 45 cases in thisreport, of which there were 26 “benign” tumorsand 19 “malignant” tumors. In 1953 this gradingscheme was modified to include three grades dueto the development of metastases related to tumorspreviously referred to as benign (Foote and Frazell1953). These investigators accepted all of thesetumors as malignant, and clinical and pathologiccorrelation suggested that separation into low,intermediate, and high grade malignant subgroupsmight be useful, mainly due to histologically over-lapping qualities. The designation of intermediategrade was recognized as behaving more like thelow-grade tumors than the high-grade tumors.Interestingly, despite the authors’ recognition thatall of these tumors were malignant, the designationmucoepidermoid tumor persisted throughout their
paper. Subsequent studies were undertaken tomore objectively determine if a benign variantexisted. One such study investigated 23 mucoepi-dermoid carcinomas with a malignant course,such as evidence of local extension of tumor out-side the capsule, local recurrences, histologicallyverified metastases, or death due to the tumor(Eneroth, et al. 1972). Fifteen patients showedlocal recurrences, 13 showed histologically verifiedmetastases, and 22 patients died of their disease.In 7 of the 23 cases the histology revealed highlyor moderately differentiated structures, and in 3of these cases the primary tumor as well as thelymph node metastases were highly differentiated.Six of the 23 patients had tumors in the palatewith 2 of these patients developing recurrences, 1with lymph node metastases, and 5 of the patientsdied due to their disease. The authors concluded
�
� �
�
294 Chapter 11
(a) (b)
(c)
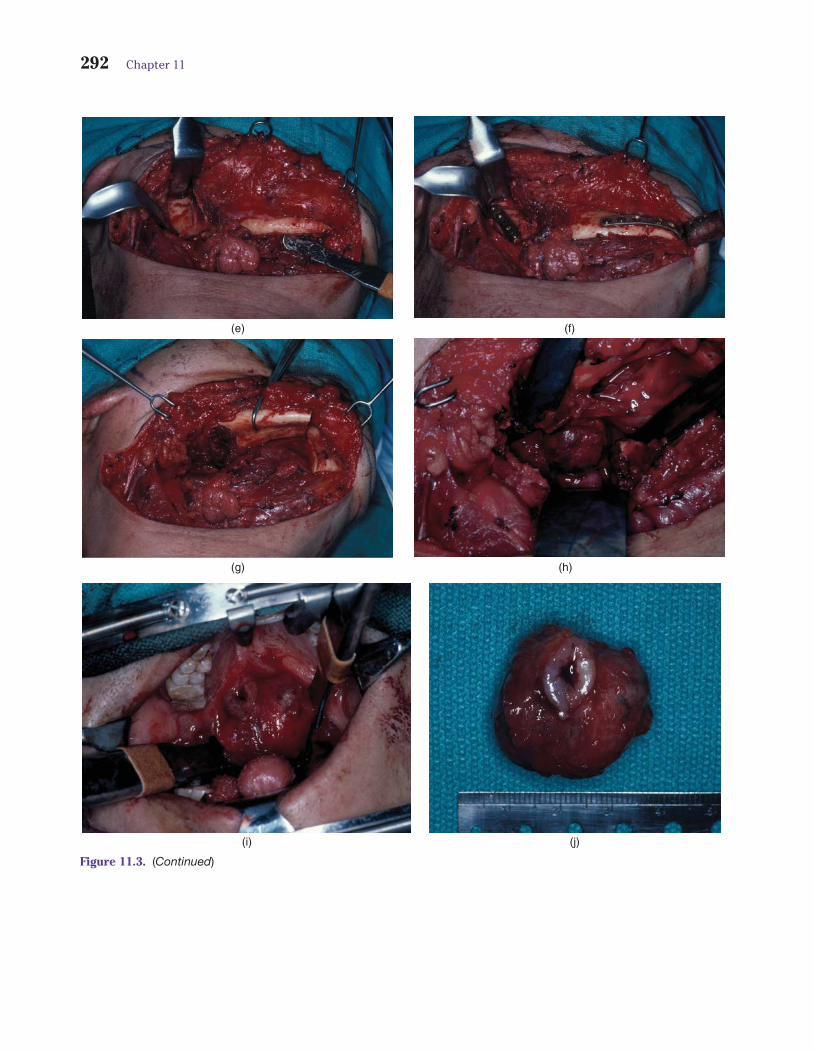
Figure 11.4. A freely moveable, indurated, submucosal mass of the upper lip in an elderly woman, highly suggestive ofa canalicular adenoma (a). Based on this assumption, an incisional biopsy is not required. A pericapsular dissection ofthis mass was performed in association with surrounding minor salivary gland tissue, thereby allowing for delivery of thespecimen (b). The histopathology of the specimen confirms the clinical impression of canalicular adenoma (c). Reprintedwith permission from: Carlson ER, Schimmele SR: The management of minor salivary gland tumors of the oral cavity, In:Surgical Management of Salivary Gland Disease, The Atlas of the Oral and Maxillofacial Surgery Clinics of North America6:75–98, WB Saunders Co., 1998.
by stating that well differentiated metastases incases with a malignant course contradicted theexistence of a benign variety of mucoepidermoidcarcinoma, such that all of these neoplasms shouldbe considered cancers (Eneroth, et al. 1972).
Of the 712 mucoepidermoid carcinomasoccurring in the minor salivary glands in the AFIPregistry, 305 (43%) of these tumors were located inthe palate, 93 (13%) in the buccal mucosa, and 58(8%) in the lip, with 37 specifically designated asthe upper lip and 12 specifically designated as thelower lip (Auclair, et al. 1991). While the AFIP datais generally recognized as being representative of
the incidence of most salivary gland tumors, someauthors have identified the mucoepidermoid carci-noma to be more common in minor salivary glandsites than in major salivary gland sites (Plambeck,et al. 1996).
Histologic grading of mucoepidermoid carci-nomas is an important exercise. Histologic gradeconnotes biologic aggressiveness, prognosis, andalso provides the surgeon with important informa-tion with which to plan surgical treatment (Evans1984; Brandwein, et al. 2001). Mucoepidermoidcarcinomas are composed of three cell types:mucous secreting, epidermoid, and intermediate.
�
� �
�
Minor Salivary Gland Tumors 295
(a) (b)
(c) (d)
Figure 11.5. A freely moveable, indurated, submucosal mass of the buccal mucosa is noted in this patient (a). The CT scans(b, c) show a well circumscribed mass of this region. A benign neoplastic process occupies a high position on the differentialdiagnosis such that a mucosal sparing excision of the mass with transoral access is able to be performed without firstobtaining an incisional biopsy (d). A pericapsular dissection is performed (e), thereby permitting delivery of the specimen(f). Stenson duct was intimately attached to the tumor and therefore sacrificed with the tumor. Histopathology identifiedcanalicular adenoma (g) with an uninvolved capsule (h). The appearance of the site is noted to be well healed at 9 monthspostop (i). Reprinted with permission from: Carlson, ER, Salivary gland pathology – Clinical Perspectives and DifferentialDiagnosis, In: The Comprehensive Management of Salivary Gland Pathology, Oral and Maxillofacial Surgery Clinics of NorthAmerica 7, 361–386, WB Saunders Co., 1995.
The intermediate cell is appropriately namedbecause it is likely the progenitor of the two othercells (Batsakis and Luna 1990). Three gradingschemes have found general acceptance amongpathologists, and differences in biologic behaviorcould be demonstrated as a function of grade, even
though the clinical stage has also been consideredan important prognosticator. Indeed, Brandwein,et al. found that only 5% of low-grade mucoepi-dermoid carcinomas of the major glands, and only2.5% of low-grade mucoepidermoid carcinomas ofthe minor glands metastasized to regional lymph
�
� �
�
296 Chapter 11
(g) (h)
(i)
(e) (f)
Figure 11.5. (Continued)
nodes or resulted in death. Spiro indicated thatsurvival of patients with minor salivary glandcarcinoma is significantly influenced by the clinicalstage and the histologic grade, but the applicabilityof grading to survival was limited to patients withmucoepidermoid carcinoma or adenocarcinoma in
their study (Spiro, et al. 1991). They determinedthat staging was important in all patients regardlessof the histologic diagnosis.
The mucoepidermoid carcinoma is the mostcommon salivary gland malignancy in children(Auclair, et al. 1991; Luna, et al. 1991; Ord 1994;
�
� �
�
Minor Salivary Gland Tumors 297
Rogerson 1995). Although most of these tumorsare noted in the parotid gland, the palate is thesecond most common site of involvement. Mostappear to occur in teenagers and the majorityare of low-grade or intermediate-grade histology.Mucoepidermoid carcinoma in children appears tofollow a more favorable course with cure rates of98–100% (Ord 1994).
Surgical treatment of the mucoepidermoidcarcinoma of minor salivary gland origin is primar-ily a function of the anatomic site of the tumor andits histologic grade. Those arising in the palate arenot only the most common, but also the most vari-able in so far as surgical treatment is concerned. Itis the histologic grade that is of utmost importancewhen determining treatment in the palate. Largeseries show that the low grade cancer is mostcommon in this anatomic site (Pires, et al. 2007).Incisional biopsy is clearly essential to establish thehistopathologic diagnosis, as previously described.Computerized tomograms are essential in planningsurgical treatment of palatal mucoepidermoidcarcinomas as they assess the involvement of theunderlying palatal bone. When the palatal bonedoes not appear to be involved by the cancer,a bone sparing, periosteal sacrificing wide localexcision with split thickness sacrifice of the softpalate musculature is the surgical treatment ofchoice (Figure 11.6). Similar to the surgery forthe palatal pleomorphic adenoma, the periosteumserves as the anatomic barrier on the superioraspect of the tumor specimen, and tumor-freeperiosteal frozen and permanent sections shouldbe obtained so as to confirm this concept. Whenthe periosteum has not been invaded by the cancerand all radial soft tissue margins are free of tumor,this surgery has a high frequency of cure. Whenthe palatal bone is noted to be invaded by tumoron preoperative CT scans, however, its sacrificeis indicated as part of a traditional partial max-illectomy (Figure 11.7). Ord and Salama (2012)reviewed their series of 18 mucoepidermoid carci-nomas of the palate, 17 of which were low-grade.Sixteen patients underwent soft tissue excisiononly of their tumors with periosteum serving asthe deep anatomic barrier on the specimen dueto the absence of bone erosion on preoperativelyobtained CT scans. One patient required bonesacrifice due to intraoperative suspicion for boneerosion and one patient underwent bone sacrificedue to preoperative CT suspicion for bone erosion.Interestingly, only the patient with CT evidence
of bone erosion demonstrated microscopic evi-dence of bone invasion by the tumor. No localrecurrences were identified in these 18 patientswith a mean follow-up period of 44 months. Theauthors concluded that the periosteum representsan effective anatomic barrier margin for palatalmucoepidermoid carcinomas.
The designation of an intermediate mucoepi-dermoid carcinoma of the palate may change therecommended surgical treatment of the tumorin this, and other anatomic sites, with a moreaggressive surgical procedure required for curativeintent (Figure 11.8). This is particularly true ifthe designation of intermediate grade is madeby the pathologist based on the worst micro-scopic pattern observed in the tumor. For example,a mucoepidermoid carcinoma that is predomi-nantly low grade, but that shows a componentof intermediate-grade cancer, will likely be desig-nated intermediate grade. This notwithstanding,the behavior of such a tumor is likely to be lowgrade in nature. This scenario is different from acancer that is designated intermediate-grade thatshows a predominantly intermediate grade patternwith intermixed low-grade cancer. The surgeonmay wish to offer more aggressive surgical ther-apy in the form of a partial maxillectomy for themucoepidermoid carcinoma of the palate that ispredominantly intermediate grade on microscopicsections. While rare, a high grade mucoepidermoidcarcinoma of the palate would require a partialmaxillectomy, and prophylactic surgical removalof the cervical lymph nodes in the case of an N0neck, or a therapeutic neck dissection in the caseof an N+ neck. Postoperative radiation therapywould also be administered in such circumstances.
Mucoepidermoid carcinoma of the buccalmucosa is the second most common minor sali-vary gland site affected. In contrast to benignneoplasms of this anatomic site, a mucosal sacri-ficing tumor surgery is required, with attention tothe sacrifice of surrounding submucosal anatomicbarriers. The same is true of the lip (Figure 11.9).
Survival of patients with mucoepidermoidcarcinomas of the minor salivary glands is clearlyrelated to grade. Five-year survival rates have beenestimated at 90% and 15-year survival rates havebeen estimated at 82% for low-grade mucoepi-dermoid carcinomas (Ord 1994). In their study of37 patients with mucoepidermoid carcinoma ofthe palate, Li, et al. (2012) identified an overallsurvival of 84.4% at 5 years and 10 years.
�
� �
�
298 Chapter 11
(a) (b)
(c) (d)
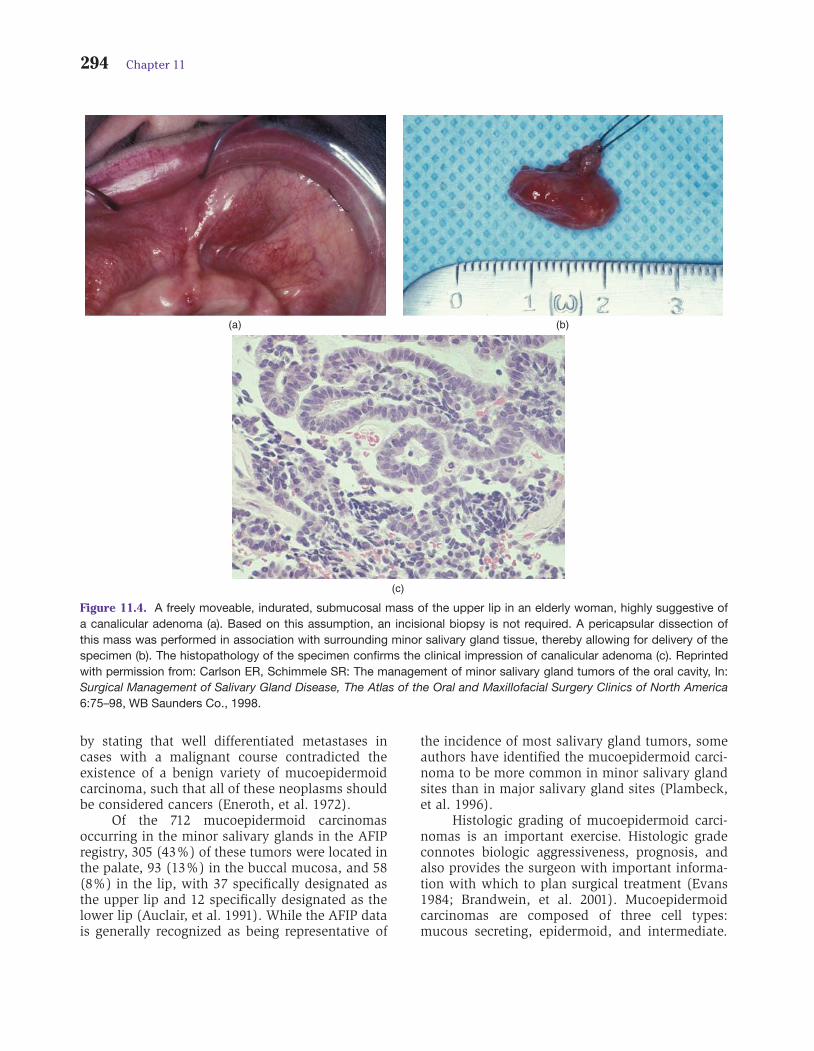
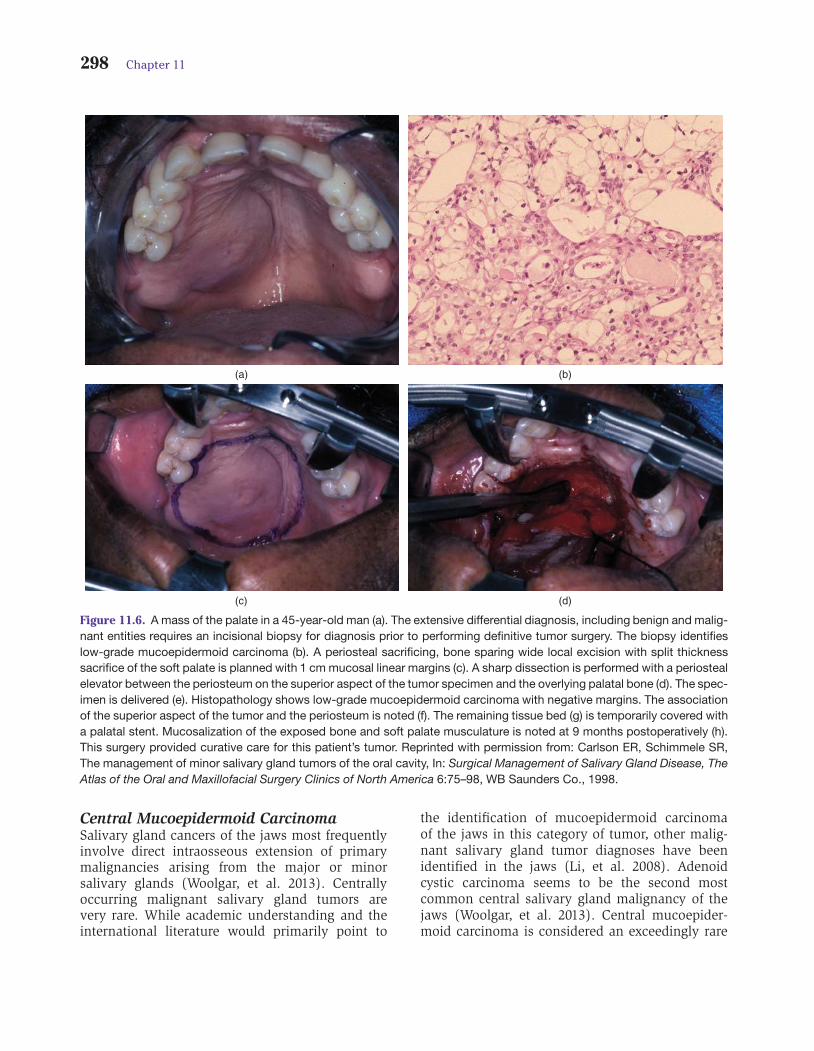
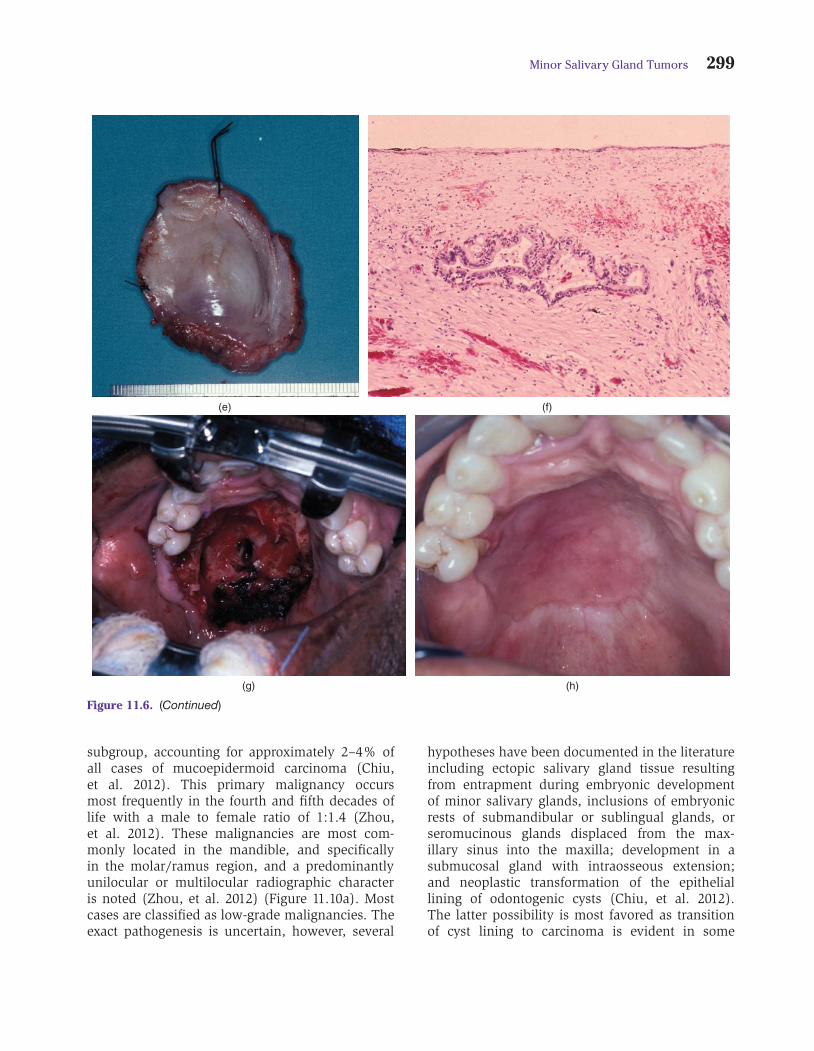
Figure 11.6. A mass of the palate in a 45-year-old man (a). The extensive differential diagnosis, including benign and malig-nant entities requires an incisional biopsy for diagnosis prior to performing definitive tumor surgery. The biopsy identifieslow-grade mucoepidermoid carcinoma (b). A periosteal sacrificing, bone sparing wide local excision with split thicknesssacrifice of the soft palate is planned with 1 cm mucosal linear margins (c). A sharp dissection is performed with a periostealelevator between the periosteum on the superior aspect of the tumor specimen and the overlying palatal bone (d). The spec-imen is delivered (e). Histopathology shows low-grade mucoepidermoid carcinoma with negative margins. The associationof the superior aspect of the tumor and the periosteum is noted (f). The remaining tissue bed (g) is temporarily covered witha palatal stent. Mucosalization of the exposed bone and soft palate musculature is noted at 9 months postoperatively (h).This surgery provided curative care for this patient’s tumor. Reprinted with permission from: Carlson ER, Schimmele SR,The management of minor salivary gland tumors of the oral cavity, In: Surgical Management of Salivary Gland Disease, TheAtlas of the Oral and Maxillofacial Surgery Clinics of North America 6:75–98, WB Saunders Co., 1998.
Central Mucoepidermoid CarcinomaSalivary gland cancers of the jaws most frequentlyinvolve direct intraosseous extension of primarymalignancies arising from the major or minorsalivary glands (Woolgar, et al. 2013). Centrallyoccurring malignant salivary gland tumors arevery rare. While academic understanding and theinternational literature would primarily point to
the identification of mucoepidermoid carcinomaof the jaws in this category of tumor, other malig-nant salivary gland tumor diagnoses have beenidentified in the jaws (Li, et al. 2008). Adenoidcystic carcinoma seems to be the second mostcommon central salivary gland malignancy of thejaws (Woolgar, et al. 2013). Central mucoepider-moid carcinoma is considered an exceedingly rare
�
� �
�
Minor Salivary Gland Tumors 299
(g) (h)
(e) (f)
Figure 11.6. (Continued)
subgroup, accounting for approximately 2–4% ofall cases of mucoepidermoid carcinoma (Chiu,et al. 2012). This primary malignancy occursmost frequently in the fourth and fifth decades oflife with a male to female ratio of 1:1.4 (Zhou,et al. 2012). These malignancies are most com-monly located in the mandible, and specificallyin the molar/ramus region, and a predominantlyunilocular or multilocular radiographic characteris noted (Zhou, et al. 2012) (Figure 11.10a). Mostcases are classified as low-grade malignancies. Theexact pathogenesis is uncertain, however, several
hypotheses have been documented in the literatureincluding ectopic salivary gland tissue resultingfrom entrapment during embryonic developmentof minor salivary glands, inclusions of embryonicrests of submandibular or sublingual glands, orseromucinous glands displaced from the max-illary sinus into the maxilla; development in asubmucosal gland with intraosseous extension;and neoplastic transformation of the epitheliallining of odontogenic cysts (Chiu, et al. 2012).The latter possibility is most favored as transitionof cyst lining to carcinoma is evident in some
�
� �
�
300 Chapter 11
(a) (b)
(c) (d)
Figure 11.7. A mass of the left palate (a) that demonstrated low-grade mucoepidermoid carcinoma on incisional biopsy.Axial (b) and coronal (c) CT scans demonstrated bone invasion by the tumor such that a partial maxillectomy was planned.One centimeter linear margins in bone and soft tissue were included at the periphery of the resection (d and e). Decalcifiedhistopathologic sections (f – hematoxylin and eosin, original magnification ×140) confirmed the destruction of bone by thetumor. The defect (g) underwent obturation and showed no evidence of disease at 2 years postoperatively (h).
cases (Zhou, et al. 2012; Spoorthi, et al. 2013).Preferred treatment is radical resection of thetumor (Figure 11.10). The value of neck dissectionfor N0 disease is debatable as cervical lymphnode metastases seem to occur in fewer than 10%of cases (Chiu, et al. 2012; Takano, et al. 2012).Patients require therapeutic neck dissections whencervical lymph node metastases are apparent onclinical examination and or on imaging studies
(Figure 11.10). Distant metastasis is rare but hasbeen reported in the lungs, brain and clavicle(Chiu, et al. 2012; Zhou, et al. 2012).
Adenoid Cystic CarcinomaLike the mucoepidermoid carcinoma, the adenoidcystic carcinoma is a very diverse tumor with threehistologic variants. These have been described