Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Wednesday 29 th April 2015 1. Welcome, opening comments Dr. Kem Kharki (MOHP focal point for International Teams) and Dr. Ian Norton (WHO coordinator for Foreign Medical Teams, FMT) opened meeting. The meeting intent is an operationally focussed daily Coordination meeting for teams providing medical and health related care to the population affected by the Earthquake. 2. Introductions/attendees Partner name Capability Comments Rescue Net Type 1 Norway Red Cross Type 2 60 beds Canadian Red Cross Type 2 40 beds +MCH component Japan Red Cross Type 1 15-20 beds Qatar Red Crescent Type 1 10-15 beds Americares Type 1 (two teams) IOM Nil Camp management UK Govt/Save the Children Type 2 without facility Italy Type 2 Rubicon/Amercian Nepal foundation Type 1 mobile Ways for water Nil Provides WASH JICA (Japanese Govt) Type 2 Handicap International Specialist rehab services Physiotherapists etc working in national hospitals Israel Defence Force Type 3 Humedica (Germany) Type 1 with light surgical capacity Lands AID (Germany) Type 1 mobile IMC Type 1, but can become 2 if needed MdM Spain Ortho-plastics specialist team To work in national hospital NATAN (Israel) Type 1 Nick Simmons Institute Nil Curative services in Nepal hospitals programme WHO MOHP UNDAC-UNOCHA 3. Operational briefing Overview of impact on health system, numbers of casualties and current known FMTs deployed was shared. Up to 90% of primary health care structures in the 11
Transcript
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Wednesday 29th April 2015
1. Welcome, opening comments Dr. Kem Kharki (MOHP focal point for International Teams) and Dr. Ian Norton (WHO coordinator for Foreign Medical Teams, FMT) opened meeting. The meeting intent is an operationally focussed daily Coordination meeting for teams providing medical and health related care to the population affected by the Earthquake. 2. Introductions/attendees Partner name Capability Comments Rescue Net Type 1 Norway Red Cross Type 2 60 beds Canadian Red Cross Type 2 40 beds +MCH component Japan Red Cross Type 1 15-20 beds Qatar Red Crescent Type 1 10-15 beds Americares Type 1 (two teams) IOM Nil Camp management UK Govt/Save the Children
Type 2 without facility
Italy Type 2 Rubicon/Amercian Nepal foundation
Type 1 mobile
Ways for water Nil Provides WASH JICA (Japanese Govt) Type 2 Handicap International Specialist rehab services Physiotherapists etc
working in national hospitals
Israel Defence Force Type 3 Humedica (Germany) Type 1 with light surgical
capacity
Lands AID (Germany) Type 1 mobile IMC Type 1, but can become 2
if needed
MdM Spain Ortho-plastics specialist team
To work in national hospital
NATAN (Israel) Type 1 Nick Simmons Institute Nil Curative services in Nepal
hospitals programme WHO MOHP UNDAC-UNOCHA 3. Operational briefing Overview of impact on health system, numbers of casualties and current known FMTs deployed was shared. Up to 90% of primary health care structures in the 11
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Wednesday 29th April 2015
most affected districts have been damaged or destroyed. 3 district hospitals have been damaged and are not usable, requiring Field Hospital substitution.
The ministry decided to institute a “hub and spoke” approach to placement of large teams in strategic locations based on previously existing hospitals and health care facilities, and with extra placement according trauma load. From each “hub” mobile teams, or smaller type 1 facilities will be dispatched to the remoter areas, to allow remaining trauma cases to be either treated or referred to the next level of care, including back to tertiary level care at the Kathmandu hospitals. Large numbers (over 10) military field hospitals have been deployed from the armies of India, China, Israel, Pakistan, Bangladesh, Sri Lanka, Singapore and Bhutan.
4. Information for partners
FMTs were asked to register using the following process;
• Register with either the WHO prior to arrival in Nepal, or with the Reception and Departure Centre (RDC) at the airport.
• Proceed to the Ministry of Health headquarters for certification procedures and tasking, bringing a copy of the registration form.
a. Present a letter from your organisation with a short summary of your organisation type, and intent while in Nepal. The letter must include a complete list of all health practioners on the team, and their licence to practice certificates.
b. Teams should show proof of the licence to practice/registration, ideally in a photocopy form that can be left with the application
c. Teams will then be certified as licenced to practice medicine for a time limited period, and as a functional team, for the purposes of the response and relief effort for the earthquake.
d. Teams can expect a formal letter from the ministry attesting o their certification, as well as a tasking to proceed to a specified area to undertake tasks in support of a specific district under the district health director.
• Teams were informed of some key clinical and management issues to be aware of during their mission in Nepal.
a. Documentation of all patient care. In particular, detailed patient records of those requiring difficult procedures such as amputations, and cases that require follow-up and rehabilitation. Notes must explain the reasons requiring the procedures carried out, and copies given to the patient, the Ministry of Health and retained by the FMT.
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Wednesday 29th April 2015
b. Reporting to the MoH must occur at least weekly. A form for surveillance for Public Health issues and critical diseases, as well as numbers of trauma cases was described to the teams, with the final copy to be available tomorrow.
c. Teams asked about medical waste management and were directed to both the FMT minimum standards technical document to which they had all agreed to comply, and to the Nepal ministry protocols for waste management. Sharps and contaminated waste are to be disposed of to a standard expected in the FMTs country of origin, and pose no threat to the local population.
d. Protocols for the management of patients that die in a health facility were discussed. Unidentified patients are to be seen by the police who will take forensic samples and proceed from there. Those who die with family in attendance should have death certificate and police identification carried out according to local district protocols and handed over to the family.
e. Teams were asked to comply with the Nepalese trauma standard guidelines which will be sent to all teams by email.
f. Drug donations are to be only if on the essential drug list for Nepal, and in English or Nepali, and in date. All other drugs must be destroyed properly or taken home by the teams.
Coordination meetings will occur every day at 15.00 for at least the first week of the response and until all teams have a primary tasking.
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Thursday 30th April 2015
1. Welcome, opening comments Dr. Kem Kharki (MOHP focal point for International Teams) Lt. Col. Dr. Naiban Bhakta Shakya (medical team coordinator for military response) and Dr. Ian Norton (WHO coordinator for Foreign Medical Teams, FMT) opened meeting. This meeting is an operationally focussed daily Coordination meeting for teams providing medical and health related care to the population affected by the Earthquake. 2. Updates from the ministry and military The military medical operational leader briefed FMTs on the current deployment of up to 12 military teams and large field hospitals. He stressed the collaboration of military and civilian teams with the same goal of relief of suffering and saving lives. Both Lt. Col. Dr. Naidan and Dr. Kharki agreed with the proposal for a hub and spoke model of larger teams at strategic and district focal points, and smaller teams both fixed and mobile fanning out from these points. Referral would then be to the district hospital if the case was manageable at that level or to the tertiary care facilities in Kathmandu. 3. Updates from partners A discussion on the capacities of Urban Search and Rescue (USAR) and rescue
affiliated medical teams was held. The Search and Rescue phase has been declared
over on day 5, with a concentration on body recovery by some teams. Medical
details from these teams (3-6 members often) are now free to respond in other ways.
A brief discussion was held, and while some USAR medical personnel must depart
in a few days, others could be reconfigured and strengthened to form mobile teams
for difficult access area response in distant areas, for 2 weeks or more. In particular
UK ISAR, UMKE Turkey and Norway SAR offered to respond, and will be available
for tasking to this role tomorrow. Action: Teams available have been placed on a
tasking list at the end of the meeting, and will be tasked tomorrow morning to
districts with critical needs.
The need for water, food and shelter as well as health care was highlighted, when
teams described mobile units being asked for these essentials while they attempted
to care for injuries and illnesses in remote clinics yesterday. Action: this will be
raised at the Health cluster 1st May.
Transport into remote areas has been difficult, and helicopter access has been
difficult. Please note, those teams requiring helicopter access to be dropped at their
agreed location will go through the logistics cluster focal point for requests. Recon
missions via helicopter should be done sparingly, as all sectors have already been
assessed, and needs are known and helicopters are vitally needed to transport food
and shelter to those cut off from roads. Those who are going are asked to be exact
in their manifests and persons travelling and be early for any scheduled departure.
Failure to comply has resulted in loss of flights as pressure on air time is very high.
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Thursday 30th April 2015
Surveillance and reporting were highlighted as a key requirement for all FMTs using
the Ministry endorsed form. Action: this was made available to all partners after
the meeting in hard copy and will be sent in digital copy within 24 hours
Difficulty to discharge patients from the major hospitals of Kathmandu was
highlighted, with over 500 patients who have no homes to go to, waiting in hospitals
for discharge. Action: continue to explore options with ministry and the Camp
cluster/IOM.
Review of comments from yesterday’s meetings for those not present included
affirming the need for patient records, and the patients right to have a copy, the need
for referral of cases when a team do not have the capacity to manage, and their
access to rehabilitation and repatriation when they have been transported far from
home.
Participants will receive meeting minutes daily. Teams requiring tasking were asked
to stay behind and have their details captured for tasking early 1st May. All
participants were given surveillance forms to fill.
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Friday 8th May 2015
1. Welcome, opening comments Dr. Kem Kharki (MOHP focal point for International Teams) and Dr. Ian Norton (WHO coordinator for Foreign Medical Teams, FMT) opened meeting. This aims to be an operationally focussed Coordination meeting for teams providing medical and health related care to the population affected by the Earthquake. 2. Updates from the Ministry of Health and Population Dr Karki reminded participants that it is now 2 weeks into the worst disaster in our lifetime in Nepal and thanked everyone for their moral support at this critical time. Dr Ian Norton visited some of the worst hit districts and FMTs over the last two days and the scale of destruction is evident. The ministry is planning for handover and takeover process so FMTs are requested to provide an exact date of exit and coordinate with the FMT coordination team. Dr Karki added that there is intention to create an earthquake book surrounding the disaster and would like to capture everyone’s contributions and thoughts about their time here. (Provide information to [email protected] labelled clearly). Dr Norton informed that the humanitarian hubs are established in Gorkha ([email protected], Tel: 9824125560, OCHA office at the Hotel Gorkha Inn) and Chautara ([email protected] , Sat Phone: +881 641436757). There are 7759 confirmed deaths and 16 434 are injured. More than 121 FMTs have been deployed, and two teams have departed. 3. Rehabilitation working group (Presentation by Brian) A rehabilitation network headed by Dr Bachchu KC (MOHP) has been formed. He is supported by Dr Guna Raj Lohani (MOHP) and Dr Khem Karki (NHRC). Alice Harvey and Peter Skelton from UK EMT is supporting is coordination. It is collaboration of WHO, IOM, Government and non-Government health facilities, NGOs and FMTs There are more than 1000 patients requiring ongoing care and 700-800 will need accommodated care mostly orthopaedic. Also there are more than 200 patients with spinal injury many with neurological deficit. Patients need to be accommodated in step down hospitals. Some existing facilities can be utilized and some needs to be built. Up to four facilities are required in Kathmandu valley. Collation of Information on which patients need step-down care and rehabilitation is handled by co-ordination team – MoHP and UK-EMT. A hotline
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Friday 8th May 2015
will be established by HI for information, and for referral, as well as an email, that is already active (see below). Physical rehabilitation needs, assistance devices needs, psychosocial needs, shelter / ongoing accommodation needs and transport needs are to be identified. FMTs are requested to notify suitable cases to co-ordination team and advise capacity to receive suitable patients into district facilities. Contact: [email protected] 4. Logistics support for medical teams Reminder that all registered teams need to be self-sufficient for first 2 weeks; if requiring additional stocks contact: Mr.Purushottam (Puru) DHAKAL Ministry of health Tel. 9843493101 Email : [email protected] Do not proceed with vaccination programmes without consultation as MoHP have existing programs. 5. Medical Evacuation In case of emergency for team members, medical evacuation by private helicopters is available but be aware it needs to be self-funded or by the insurance company of your team. Contact details are below: SHREE AIRLINES [email protected], Tel: 9851020639, 9851026197 6. Update from an FMT – Israel IDF medical corps (Presentation by COL. Tarif Bader –Commander) A Type 3 FMT, IDF has 129 Medical personnel with 45 medical officers. It has treated 1299 patients in the period of 4/29/2015 to 5/8/2015. Out of 104 procedures, two thirds are orthopaedic surgeries. EQ related patients are decreasing to less than 10%. It is being demobilised from 9th May at 1200 and will refer patients to nearby facilities in Kathmandu. However there are issues with 4 patients still intubated, with the receiving ICU unable to provide the required hardware so if any teams have
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Friday 8th May 2015
spare ventilators, please advise, and they will be returned directly after the patients have been weaned (4-7 days). The team also demonstrated an electronic medical record system where all patient information is captured digitally and available for display at once, or printed out for patient discharge. There may be application for future responses where FMTs can share such information between each other and report to the Ministry in almost real time. 7. Updates on hospitals Ramechapp (MdM Spain) is returning to normal capacity and can take referrals but no C-section or major surgery, as this did not exist prior. Chautara, Sindulpalchowk (IFRC) can take referrals (including C-section and emergency surgery). Dhunche, Rasuwa (IFRC) can take referrals (including C-section and emergency surgery). Bidur, Nuwakot (Bhutanese army) will be demobilising but currently can take referrals (including C-section and emergency surgery). Dr. Karki and Dr. Norton will report on their field visit to the site and meeting with partners at the next FMT coordination meeting. MSF France in Aarughat FMT is up and can take referrals. Canadian RC in Tatopani are providing basic health care from yesterday for three weeks. JICA (Japan Govt) Type 2 is open in Bharabise (Sinduhpolchowk), as is the Type 2 of the Italian Govt in Betrawati (Nuwakot) Langtang has suffered massive destruction due to avalanche and will not require an FMT because any survivors are no longer in the village. 8. Standing items Gender issues: NTR Security updates: Communities are reported to be very appreciative of the FMT services. FMT coordination team will provide an aftershock map. Please be cautious when using damaged buildings for sleeping or other activities.
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Friday 8th May 2015
Environmental issues: NTR Coordination and reporting: Reporting from about half the teams is still missing. Please be mindful it is a requirement for recognition, surveillance and capturing patient records. Be in email group of the FMT coordination cell ([email protected]) and you will be provided a cover note, reporting form and exit form. FMTs should provide daily surveillance reports to the FMT email account by 1600hrs using provided form.
Medical team exit process: FMTs need to coordinate with the District Health Office (DHO) and WHO field coordinator for the exit process. Advance notice of withdrawal is required and much appreciated. FMTs need to submit service related data to the DHO first. In case of inpatients and operated cases, detail case profiles need to be submitted. The medical team then receives a brief acknowledgement letter from the DHO. Along with this letter an exit report needs to be submitted to the FMT coordination cell (FMT CC) at Ministry of Health and Population. The FMT CC verifies the information and HEOC will issue letter of appreciation to the medical team. The procedures at the MOHP will be rapid, but please leave at least an hour and a half for the processing of this appreciation letter. In case of donation, the teams should submit a list of equipment and tents to be handed over to the DHO or Logistics Management Division (LMD) and get a receipt so this can also be reflected in the letter of appreciation. (See attached detail process of exit and FMT exit report form for use) Access: Road to Tatopani is open. Potential for landslides with monsoon rains but already considered by GoN. Dr. Norton provided detail on an aerial recon flight over the road north of Dhunche to the border, there are two blockages being worked on within 1km of the town, byt then the road is relatively clear to Syaphru. The road north to the border from there has been completely lost, or covered in deep avalanche in at least 15 places and is very unlikely to be cleared soon. The final avalanche at the border itself is estimated over 50M high and several hundred metres wide AOB/Questions; Some hospitals are reported to ask money with the patients. Dr. Khem said this is against the directive issued and the government will take action. Participants will receive meeting minutes after each meeting. Meetings to be conducted Mondays, Wednesdays and Fridays.
Nepal Earthquake 2015 Foreign Medical Team Coordination Meeting Minutes Friday 8th May 2015
Next meeting 11th May 15.00 Ministry of Health Meeting adjourned 16.05 All enquiries to; FMT Coordination Team WHO / UNDAC / MOHP Operations Cell at MOHP Conference room, 1st floor [email protected] + 977 9801083421
FMT Meeting Minutes from the 14th May 2015lead by Dr. Khem Karki (MoHP), Major General Prof. Dr. Kishore Rana (Nepalese Military), Dr. Ian Norton (WHO).Time: 3:00 PM 4:00 PM
1. Updates
1.1. Update from the WHO
Dr. Ian Norton introduced Flavio Salio as his replacement for WHO Coordinator for Foreign Medical Teams. He provided updates on the second earthquake on 12th May, 2015 with epicenter in Dolakha which has resulted in reported 80 deaths and 1961 injuries. Level 2 civilian and military Indian and Nepali teams have been attending the victims in Charikot at a field hospital and have seen at least 114 casualties. There has been conflicting numbers on the number of casualties. At present there are no gaps to be addressed by FMT deployment. However, gaps still exist in hospital tents and maternity tents in the affected areas.
He informed that 72 FMTs currently deployed. Although the total numbers are fluctuating, we know of at least 49 FMTs which have left or are leaving in the next day or so.
1.2. Update from the MoHP
Dr. Karki informed that the second earthquake which caused major destruction in Dolakha was quite manageable.
NHRC is conducting a threeday training course to the local health workers working in surveillance with the help of the Chinese Medical team. It also includes management of reproductive health in crisis. There are around 30 local participants, who, on completion of the training will be competent in field investigation, postdisaster surveillance and management of reproductive health in crisis.
Cuban team has almost established hospital at Kirtipur and will have rehabilitation facilities. They will work with Ayurveda hospital and Phect hospital and will have a total of 150 beds.
Furthermore, he emphasized that reconstructing health facilities is a prime issue. MoHP has started formal discussions with external development partners and will be continued.
Psychosocial cluster is also working together and we will need updates from them too.
He inquired about difficulties in the field, especially in Tatopani and Barabise. Also asked the FMTs to use new account [email protected] for sending their reports and any other communication as required.
1.2. Update from the Military
Director General of Medical services of Nepal Army Dr.Rana provided the following updates:
Death toll has reached 8219 as of today. Nepal Army is involved mainly in Search And Rescue, the operation resumed after the second quake especially in Charikot area where most houses have collapsed, and also in the valley. Almost 80 people have died from the second quake; most of these deaths are in Dolakha i.e. 37. There were 1299 injuries. 27000 houses in Kathmandu has been destroyed beyond repair. Nepal army rescued 175 and US army rescued 42 from Langtang after the second quake. However, the rescue has been stopped due to difficult geographic conditions.
The Nepalese Army had 15 foreign medical teams in the country. To this date there are 5 teams still continuing their service in the deployed area. A combined Indian Nepali Level 2 team has been deployed at Charikot to deal with surge. It has provided triage/ primary trauma care to 114 patients. Canadan Military, Pakistan Military and Indian Military teams have been deployed in Sukute, Bhaktapur and Sinamangal respectively. These teams were asked to hold their departure due the second quake but are likely to leave soon due to low severity of new quake.
Indonesian military team has left (and been replaced by civilain team), Half of the Bhutan team has left and the second half leaves by Sunday.
Estimated 600 medical facilities have been destroyed and concern is rebuilding them.In Kathmandu valley most hospitals are fully functionning. Army hospital has been destroyed, however it is providing services from the tents outside the building. Other hospitals like Bir Hospital and Om Hospital are paritially damaged but are doing the same.
The major issue is the safety of own teams and patients after the major aftershock. Everyone is advised not to use buildings to sleep in, especially if they appear damaged. Thankfully on the check with all FMTs, no casualties has been reported.Lanslide risk will increase with the coming rainy season.
3.2. Gender Issues
NTR
3.2. Environmental Issues
One Landslide blocked a road in the Tatopani region now unblocked again there is a serious risk for landslides. Sunkoshi dam is the name FYI.
Dr. Karki reminded the FMTs to seek help of Grande Hospital for hospital waste Management if required.
The Chinese Medical team in coordination with Epidemiology and Disease Control Division (EDCD) and National Public Health Laboratory (NPHL) has collected 232 samples 180 water, 40 stool and 56 stool swap, and will submit the report formally tomorrow on 15th May . 2 stool samples are found positive for V. cholera and 1 positive for Shigella from Kathmandu valley. The positive news is there is no indication of outbreak from anywhere.
3.2. Coordination and reporting
Many teams are exiting but only a handful have submitted an exit report. FMTs are requested to provide the exit report as this is crucially important for the Ministry for further use.
Surveillance forms are not coming in very often; we implore you to report back on a daily basis using [email protected] gmail account. We lost 1224 hours of surveillance because of failing gmail account. Please resend any forms you think may have been lost in this time.
All reporting forms can be accessed through: www.humanitarianresponse.info (http://www.humanitarianresponse.info/en/operations/nepal/foreignmedicalteamwg )
3.2. Remote Area Access
http://logcluster.org/ops/nepa provides updates to road access.
Tatopani - Canadian Red Cross working there had to be evacuated due to the destruction caused by the second earthquake. According to the team, there are lot of damage and it is very unsafe. Their equipment are still there, taken care by a local security guard. Re-deployment is under discussion.
According to the Japanese team working in Barhabise, road is blocked around field hosptial. There are no casualties in the region. JICA team has been evacuated because of landslides and are now working in Dhulikhel Hospital Emergency department until May 18, 2015.
MSF working in Dolakha rediverted medical teams to region and evacuated 6 people to KTM. 5 causalties in the field.
3.2. District Hospital Status and updates from the teams
Ramechhap: MDM Spain is supporting district hospital in Ramechhap. 7 patients were injured; no reports of deaths. They will start psychosocial support program soon.
Chautara (IFRC): There were 80 disaster related casualties after the second earthquake. Psycological first aid also being provided. The hospital is functioning well. National Red Cross Society has been set up near the hospital to provide some first aid.
Nuwakot: Post exit plan in Bidur exists. District hospital has prepared ground. Italian team has donated a tent. Unicef and Save the Children also donated tents. By next week district hospital will be functional.Tents will be used for indoor patients. Govt doctors, Italian team and Red Cross led by Nepali doctors will work there. On 12th 116 paitents visited Italian team. Ambulatory part has been donated to Trishuli hospital as well as old equipments has been transferred.
Dhunche: No issue after the major aftershock.
Gorkha : 3 minor injuries
Arughat: Patients are low 9 patients, half are injury cases. Small outreach teams are working as well. No new injuries from the new quake.
Samaritans Purse 3 small teams are deployed in Dolakha for initial assessment and WASH. Health facilities at Simigaon has been completely destroyed. No casualties due to the earthquake. Only 30 tents have arrived from Government and they are asking for tents for health post and medicines/matress.
Medical team in Pangtang: French team doing 6070 consultations a day. The team is coming back tomorrow on 15 May
Team Rubicon: 16 patietns in Barwa area after earthquake. No evacuation was needed.
Japanese team in Melamchi are fine continuing to work from tents. Few casualties, one death, one head injury and some small injuries.
Czech Receving 23 casualties per day
Thailand team working in Sipaghat: Have splitted into 3 groups to respond at health post. It is handling minor surgical cases as well and mobile teams went up and saw 40 cases
regular disease. Disease prevention team is teaching how to care for themselves and health promotion. Next team is coming tomorrow. Departure date is not sure yet.
Chautara (South korean): Mobile teams in different areas of Chautara.
Humedica, Jalbire One seriously injured flown to Kathmandu. Road is blocked. Received 6 minor cases from Ghatlang after the second quake. Left Jalbire due to bad wheater.
Cuban team: Arrived yesterday and are in Kirtipur. The hospital will be inside the Ayurvdea Center and camping out as residence. OPD starts from 15 May and embedded some Nepali team to increase capacity. Right now there are 20 beds, basic surgery will start from day after tomorrow. Ready to deploy mobiles from 15 May and ready for rehabilitation work in 23 days.
Rehabilitation: There are 60 beds for spinal injury patients in Anandaban Hospital and Green Pastures and the hospitals are running out of capacity. Spinal center is increasing its capacity to take more patients. Handicap International is setting up a focal point outside Bir hospital to address the demand for rehab prosthesis and assistance. If anyone requires equipment, please contact them.
Rehab cluster group is working for the same and is assessing Dolakha facility to see if there is any need there. Next meeting of Rehab cluster is at 9 am tomorrow morning at NHRC Hall.
The medical rehab team from Royal Melbourne University Australia treated over 300 spinal injuries in the past 5 days. They worked with Handicap International on community based rehab and referrals. There has been 30% increase in pressure sores in spinal injury patients. The hosptital currently has 88 paraplegics, and 50 more are coming in tonight.
Army hospital Dr Rana provided update on status of Army hospital. It is paritally destoyed after the first quake. ICU patients were inside the hospital but everything was shifted outside after the second quake. It may take 6 months for the entire hospital to be reconstructed. It is 490 bedded tertiary level hospital , now catering to 125 casualty patients.At present it is only taking emergency and trauma cases, OPD cases will open in a few days. Army to be contacted for any evacuations.
Bir hospital is also functioning outside. Almost all of IPD department is damaged. Patan hospital is partially damaged. Civil hospital is okay. Orthopedic hospital only OPD is fine. B and B is alright. Most part of Grande Hospital, Om Hospital and Medicare are unusable. All together, 700 bed have been decreased within the valley and with reduced capacity should any new crisis arise.
4. Any other business:
Contact Rajib Pokharel at Airport Custom 9841272138 in case of any inconveniece regarding to custom clearence.
Tents: Americares has 5 tents 45 by 45 feet coming from India and 5 more from USA and Amersterdam each (25 beds) . Global medics from canada 16 by 16 sized 9 tents, and eureka 32 by 20 2 tents.
5. Meeting practicabilities
Participants will receive meeting minutes after each meeting.
Meeting closed at 16:00 hrs.
Next meeting on Monday, 18th May, 2015 15:00 hrs at Ministry of Health and Population Conference Room, 1st Floor.
All enquiries to;FMT Coordination TeamWHO / UNDAC / MOHP Operation Cell at Research Section, 1st floorNepal Health Research Council (NHRC)[email protected] + 977 9801083421
FMT Meeting Minutes from the 18th May 2015 Chaired by Dr. Khem Karki (MoHP), Col. Dr. Arun Neupane (Nepalese Military), Dr. Flavio Salio (WHO) Time: 3:00 PM 4:00 PM
Flavio welcomed all FMTs to the meeting and introduced Col. Dr. Arun Neupane from the Nepalese Army in the absence of Maj. General Prof. Kishore Rana.
1. Updates
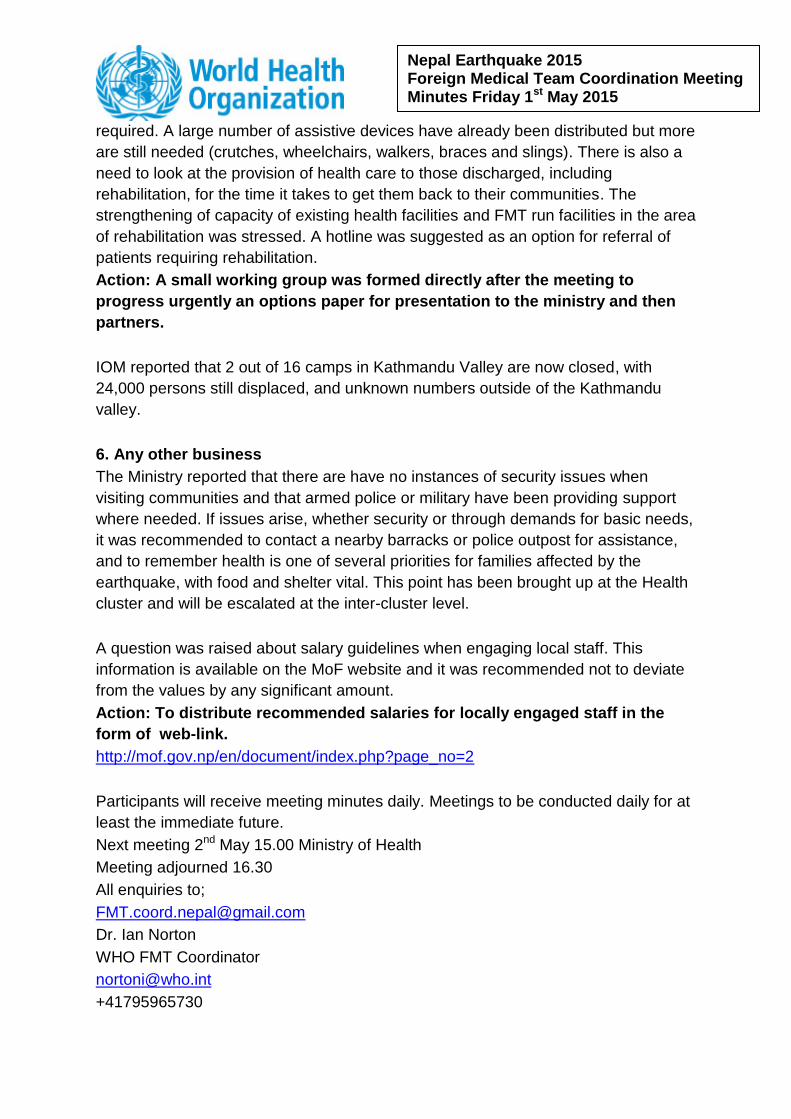
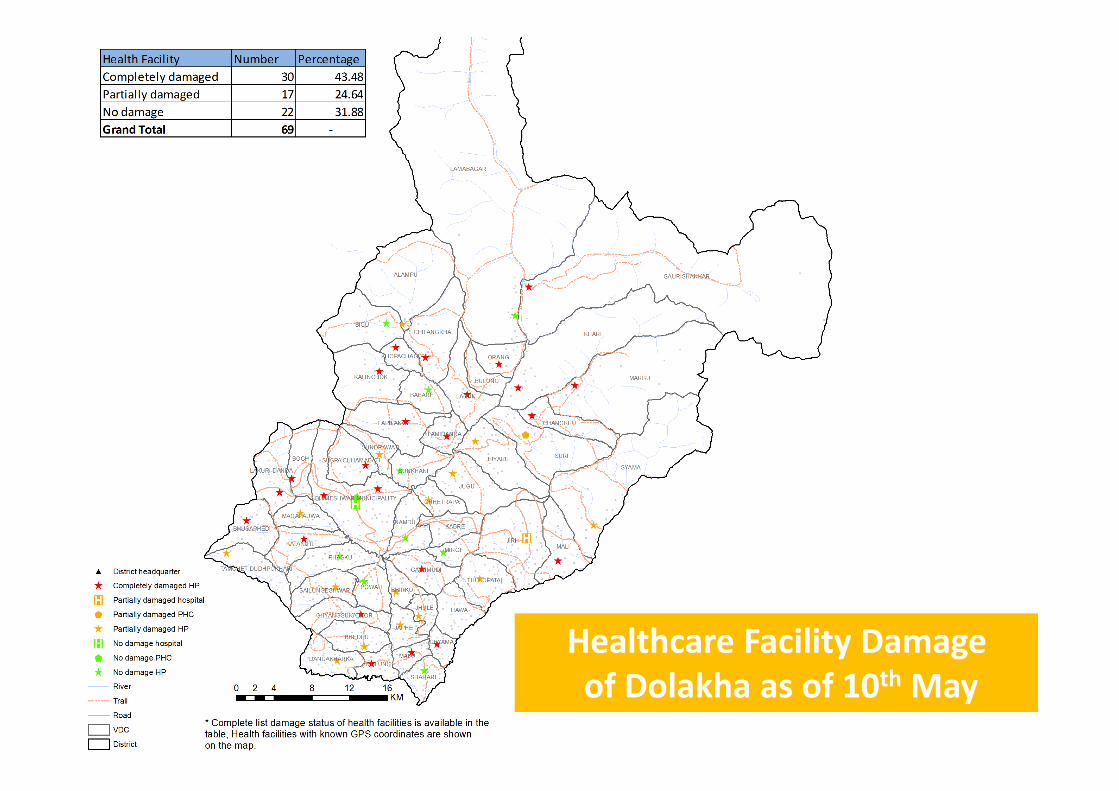
1.1. Update from the WHO Flavio highlighted the issue of retasking, and raised daily surveillance reports as an issue. He discussed medical needs. Medical needs in affected areas still include maternity and hospital tents. There is the need for psychological support, which has been further exacerbated by the 12th May aftershock. There seems to be no requirement of further medical teams from outside Nepal, though redistribution in Sindhupalchowk may be required. Flexibility of teams is needed in regards to tasking. E.g. level 2 team may be tasked as a level 1 based on the needs communicated by district and MoHP. Flavio presented maps of districts severely affected by the aftershocks of 12th of May. He also presented a map depicting health care facility damages in Dolakha as of 10th May, as well as a graph of FMTs deployed in Dolakha as of 17th May. He mentioned that discussions are ongoing regarding deployment in Dolakha, and that he will ask some FMTs to provide information on their movements, in particular International Federation of the Red Cross and MSF. On the topic of reporting, Flavio stressed the fact that the number of FMT daily reports received is still low. 56 FMTs are deployed at present, and the highest number of reports received so far has been less than 20 a day. He asked FMTs why they are not sending the reports. This information will be used to retask the teams. Only 45 teams have submitted at least one daily report, and only 17 have submitted exit reports. From a project management side, Oliver asked the teams to fill in date, district, FMT name, location and date, while they send their daily surveillance forms. Without this information, surveillance is not possible. He also requested that teams update their contact information and departure dates in order to facilitate planning structured handovers. A letter of recommendation from the District Health Officer is required to get the letter of appreciation from MoHP, along with exit form. He said that the FMT coordination team will send out the
daily surveillance form in an Excel sheet format as of tomorrow for teams to fill out instead of word document of the form, which will make life much easier for FMT coord team moving forward. A snapshot was shown of total cases treated by FMTs: 28,372 OPD cases, 1499 IPD cases, 440 major surgeries, 158 cases referred from FMTs to hospitals, 6073 trauma cases, 2,793 ARI cases and 308 deaths reported.
1.2. Update from the MoHP Dr. Khem B Karki provided an update from the MoHP. He thanked all FMTs for their support and tireless efforts in the field, as well as for attending this meeting. He apologized for not being able to use the MoHP meeting hall: following damage sustained on the May 12th earthquake, engineers have assessed the building and deemed it unsafe. As the UNICEF tent is too noisy, the meeting is being held in NHRC meeting hall. He added that Italy Civil Protection and JICA will be leaving by tomorrow two huge groups that we are farewelling fondly. This morning the Bidur office was contacted by Dr. Karki. Operations have already been handed over to the district hospital there, which is now supplied with Italian commodities and a tent. Other teams including MSF and an Israeli group are working there. Qatar Red Crescent was not. Bidur has need of medical doctors and nurses, but the government of Nepal has plans to recruit Nepalese doctors and nurses in the very near future to fill these gaps. Dr. Karki described his and Flavio’s visit to Melamchi. They went there yesterday to meet with medical teams on the ground: the Czech Medical Team and Japanese Red Cross, and spoke with the private health care workers. There is very good work going on and cooperation between teams. The Czech team have a good generator, while the Japanese team have an Xray, which are being shared synergistically. A young doctor recruited as medical officer is in command and is doing a surprisingly good job. In a very short period of time, an exit plan was developed, meaning primary health care services in Melamchi can take over. The Czech team is leaving within 2 weeks, while the Japanese team is staying for 3 months to conduct activities including WASH, nutrition etc. He also shared a tale of improper practice in the field which should be avoided. In Dubachor, near Melamchi, unknown medical team(s) treated wounds without cleaning/sterilisation, approximately 48 hours after the earthquake. These patients’ wounds are now all infected. The team(s) went there directly and started work without being deployed. This case must be followed up to identify the medical team(s) responsible. The avoidance of situations such as this is the reason coordination and regular communication is critical. Dr. Karki added that it is important to maintain a global list of FMTs, detailing with their strengths and performance history. This can be referred to times of disaster anywhere in the world, and the best teams can be dispatched. Not all teams are necessarily desirable or able to be useful. For example, a team of 19 people recently approached him asking for
deployment instructions. However, the team was not selfsustainable. They were without medical supplies, appropriate staff, water and related necessities for effective operation. This is another reason for requirement of FMT registration and surveillance. There is a greater need to have effective information systems. Flavio added that the WHO is preparing such a recording system for global disaster responses. It is likely the process will be active as of the second half of 2016. Dr. Karki reiterated the numbers of FMTs and their various statuses. There have been 140 teams from 38 countries. Of these, 56 FMTs are still deployed, 70 have left, 9 teams have unknown status and the rest either left after assessment or were not applicable. These unknown teams came and registered, then deployed by themselves rather than returning the next day for instructions, so they’re now lost. Generally we do not have contact details for them. It’s possible that they’ve done good work, but it is not recorded anywhere or known.
1.2. Update from the Military Dr. Neupane gave an update from the military. He said as far as military support is concerned, from day zero till now there have been a good service. Military teams have all departed bar one, which will depart next week. All gaps will be filled by MoHP and national military teams, which are getting organised quite well. He has seen that the health cluster is doing a great job. Activities are much more organised, which should be commended. One issue is the small amount of medical support that’s been able to reach remote locations, so the Nepalese Army Medical Corps is going to these thus far unreached locations to fill in the gaps. There are two more mobile field hospitals being set up, and vehiclemounted field hospitals which were meant to arrive a long time ago and have finally arrived in Kathmandu and will be deployed shortly. There are two epidemic prevention teams from the Chinese government (civil and military), specialising in assessing water sources and toilets, and monitoring sanitation. The civil team tested water sources and the military team had subsequently sanitised any problem areas, and they’ve played a very significant role in preventing the spread of communicable diseases. Nepalese military air assets can be used when required and requested through the proper channels. They evacuated a newborn baby with respiratory distress from Dhunchhe IFRC Hospital, which made the front page news in The Kathmandu Post a couple of days ago. Villages are very scattered so health access is a challenge. VDCs are broken into 9 wards, potentially spread across 4 mountains. As such, it may appear a small area on the map, but in fact be very large on the ground and difficult for people to move around. Large FMTs are therefore requested to send satellite teams to service the wider area. This is more effective than staying in one location.
3. Other
3.1. Safety and Security Issues The Nepalese Army is distributed in 567 places in earthquake affected areas, as well as permanent camps in villages. If you have any safety or security issues, please report to them. Bob from Team Rubicon raised a security issue faced by his team. A female burn victim in the Surmitan area came to their camp and was treated. The local army was called to provide evacuation, and advised that this couldn’t happen until the morning, when they would send transport. However, Nepali police forces showed up in the morning. It turned out that the patient was a domestic abuse victim, and locals accused Team Rubicon of calling them. Luckily the situation was defused, but there is much grief and stress in affected populations, and sensitivity is paramount. Counseling and training of locals is important, and it is critical to have a local translator working with all FMTs. Sam Taylor from MSF shared another security issue. While assessing small communities in Dolakha yesterday by helicopter, landing was not possible in several instances because of the danger of the helicopter being swarmed. Some villages have not been seen for more than 3 weeks, so there is anger, stress and impatience. MSF is flying with experienced Nepali pilots who are making judgements about when it’s safe to land.
3.2. Gender Issues NTR
3.2. Environmental Issues Flavio stressed that it is the responsibility of FMTs to handle medical waste management. It is advised FMTs ensure they have the capacity to treat waste onsite. If not, they should coordinate with Nepali military forces near the service area. The MoHP has requested the military support anybody who approaches with hospital waste. Medical teams who can’t manage medical waste can also contact the Grandee Hospital, who have an extensive waste management system and can accommodate FMT waste as well. A meeting participant suggested that FMTs with mobile clinics in camps should go beyond providing clinical assistance, to also stressing hygiene and health education to locals.
3.2. Coordination and reporting IOM is facilitating stepdown and relocation of patients. They requested that departing FMTs provide them at least 23 days notice for any patients that require transportation or stepdown. Calling on the morning of their departure is not acceptable.
Flavio reminded all FMTs with departure dates to work on their exit plans. Also take stocks of all assets being left behind so that distribution can be coordinated according to the needs communicated to WHO/HEOC. Dr. Karki showed a graph of FMT departure dates. This information is important for MoHP to have in order to plan takeover of health services that were being provided.
3.2. Remote Area Access Dr. Karki said that there was a request for support from Dolakha District Health Office. Following that, MSF has committed to providing logistics and health materials for 3 months, so that even in the face of monsoon season and potential landslides they will have stocks to continue their services there. He thanked MSF for taking on that challenge. Sam Taylor from MSF said that they will work in 13 VDCs listed as affected by the DHOs. MSF will be stocking most damaged health posts with 34 months of drugs, and taking shelter materials to the worst damaged areas. They have access to a number of small helicopters and 300 tonnes of material that they’d like to distribute. They have conducted assessments and know where it needs to go, but are having difficulty getting heavy lifting helicopters, and instead are flying up to 20 rotations per day with small lifting helicopters which is suboptimal. He added that UN civil military has not given any clear answers about what assets may be available to them. It is now a race against time and has already been 23 weeks. Dr. Neupane suggested MSF would need heavy lifting helicopters to Charikot, and they could take smaller helicopters from there. He informed that Army HQ has a brief every morning with OCHA and that there is a system in place for actioning requests that come, including medical relief. MSF should come through Dr. Karki or OCHA. Sam said he’d already tried those channels and action was not being taken fast enough. Sam was requested to give Dr. Karki a load table which representatives from the Nepalese Army could assess. Dr. Khem suggested sending materials by truck to Charikot and using helicopters from there, but Dr. Neupane updated that road access is not possible. Dr. Khem added that most requests are covered by MSF in Dolakha. Singati is the hardest hit village, which the Canadian Red Cross and some other group have been asked to support. Dr. Mausam from Nepal Red Cross confirmed that needs look fair as most health posts are not functional. The Canadian Red Cross is planning to establish a base there in the next few days.
3.2. District Hospital Status and updates from the teams Ramechhap (MDM Spain): No representative from MDM spain present. Dr. Karki mentioned an issue recently took place. Some members of a mobile team went into the community and talked about religious issues, which angered the locals. It is not a time to discuss anything publicly except medical needs.
Sindhupalchok/Chautara (IFRC): The Red Cross there is offering surgical care and mobile clinics, as well as taking referrals from another team. Nuwakot (Civil Protection Team): The Italian Civil Protection Team is departing tomorrow. The meeting representative would like to thank everyone, especially the central government. There was very good coordination between central and local government he said, which facilitated the Italian FMT’s actions. He met the MoHP representative who visited their camp and the local DHO. The MoHP visit was very important psychologically for the local people and the team. He added that they were supported by WHO to fill the famous exit form. It is an important form for exit customs as it provides proof of work done here. The Italian team added another appendix to the two existing ones “material on arrival minus material donated”, i.e. material returning to Italy. He also made a note on selfsufficiency. Their team was selfsufficient, but they made a waste management agreement with the local hospital and an agreement with the municipality for providing water. He stressed that it is important for FMTs to be selfsufficient, and for the government to support them in whatever activities needed. Another important factor was the population in Nuwakot, who he described as fantastic. They assisted the FMT in everything, offered dinner to the Italian staff, and cried on the last day, saying “Don’t forget Nepal”. The Italian FMT members cried too. He concluded that it was a good mission for the Italian FMT because the state was with them. He thanked his colleagues, especially his officer who coordinated operations. Arughat (MSF): The hospital is up and running but receiving quite low patient numbers not sure why, though possibly patients are unaware of its existence and are instead going to Gorkha. Sam said that the team is going to do community radio to announce the presence of the hospital. Dr. Khem informed everyone that he would be visiting Arughat tomorrow. A lady from IOM updated that IOM has been requested to provide psychosocial support in Gorkha. Barhabise (JICA): JICA had been working in Barhabise. They saw 56 patients in May 11th and 12th, and after that went to Dhulikhel to help coordinate. They spent 5 days there, and are returning Japan tomorrow. Flavio thanked the JICA team greatly for their flexibility and for supporting the FMT Coord Cell here at NHRC with staff. Dr. Khem added that Barabise was a very difficult situation as no land space exists to establish even a tent, let alone a larger health clinic. He informed that he has started talking with political leaders to seek means to resume primary health service. They have doctors, nurses and supplies there. A local woman named Sam (owner of the the Last Resort), in Listikot VDC above Barhabise, says that the health posts in Marming, Chankhu and lower villages have all collapsed. The local appointed doctor has left for Kathmandu, and Hindi health post has collapsed. Her groups is working with a local health worker in Thengthali (a village in Marming VDC). Many local villages have been evacuated and people have arrived in their
clinic, but they don’t have necessary health facilities. The nearest facility is Dhulikhel, but road conditions to get there are very bad. Flavio said that he and his team discussed this with MoHP yesterday. Dr. Khem asked to discuss this with them further after the meeting. Cuban team: Hospital has been operational since yesterday, and they have performed first 4 surgeries. He provided lots of details about operations carried out in Lalitpur and Bhaktapur. They are ready to tackle more complicated surgery patients and are in contact with the Nepalese Military. All their facilities are ready, although there are some shortages with chemicals, though these can be discussed bilaterally. Dr. Khem said that some requested supplies have already arrived, but the representative from the team insisted that oxygen and medical gasses have not arrived. International Medical Corps: They are providing medical teams in Gorkha and Dhading two teams in both locations. Additionally they are also providing WASH facilities, shelter, protection and running assessments on gender issues. Also they are discussing establishing rehab facilities in both locations to help with stepdown. MSF: It is going to sign a MOU with the Nepalese Orthopaedic hospital, which is hoping to increase their capacity with various activities UK International rehab subcluster: There is quite a lot of support within Kathmandu. The Nepal rehab cluster is able to direct to services such as physio etc when contacted. The cluster visited Gorkha district hospital yesterday and is going into partnership with IMC. Dr. Khem asked to make sure to get rehab information as well from DHO to determine where priority areas are and also coordinate with MoHP. IOM have a patient transport number, so they can be called if you have trouble discharging or relocating patients. Flavio said that daily surveillance reports are being read too, so FMTs can report any assistance or materials required in there. Thailand team: They are a 3rd rotation team which started on May 11th. Their treated cases numbered 1200 up until yesterday. They’re sending out mobile teams and doortodoor searching. During the last week they were able to find one earthquake victim who was unable to walk to the hospital. They assisted in his infected open foot injury. He was referred to Dhulikhel local hospital where he was operated on.
4. Any other business Handicap International can be contacted for assistance with Rehab operations: +977 1437 2794
Further discussions to be held now with JICA, the Cuban team and anyone else with issues requiring urgent actioning
5. Meeting practicalities Participants will receive meeting minutes after each meeting. Meeting closed at 16:00 hrs. Next meeting is on Thursday, 21st May, 2015 15:00 hrs at Nepal Health Research Council (Behind MoHP Building) Meeting Room , Top Floor. All enquiries to; FMT Coordination Team WHO / UNDAC / MoHP Operation Cell at Research Section, 1st floor Nepal Health Research Council (NHRC) [email protected] + 977 9801083421




































































![jf:Yo, kf]if0f tyf hg; +Vof ^=@=! k[i7e ldnepalpolicynet.com/images/documents/publichealth/research/MoHP... · ^=@ :jf:Yo, kf]if0f tyf hg; +Vof ^=@=! k[i7e "ld g]kfnsf ] cGtl/d ;](https://static.documents.pub/doc/80x56/5b19b5ca7f8b9a1e258cf347/jfyo-kfif0f-tyf-hg-vof-ki7e-jfyo-kfif0f-tyf-hg-vof-.jpg)





