Page 1
DOI 10.1378/chest.08-2784; Prepublished online March 2, 2009;Chest
Scott D. Halpern and Darren B. Taichman End-Diastolic PressurePressure Rather Than Left-Ventricularto Reliance on Pulmonary Capillary Wedge Misclassification of Pulmonary Hypertension Due
http://www.chestjournal.org/content/early/2009/02/20/chest.08-2784
services can be found online on the World Wide Web at: The online version of this article, along with updated information and
) ISSN:0012-3692http://www.chestjournal.org/site/misc/reprints.xhtml(without the prior written permission of the copyright holder.
distributedrights reserved. No part of this article or PDF may be reproduced or College of Chest Physicians, 3300 Dundee Road, Northbrook IL 60062. Allhas been published monthly since 1935. Copyright 2007 by the American CHEST is the official journal of the American College of Chest Physicians. It
initial publication. online articles must include the digital object identifier (DOIs) and date ofare indexed by PubMed from initial publication. Citations to Advance Advance online articles are citable and establish publication priority; theyversions may be posted when available prior to final publication).
typesetpublication but have not yet appeared in the paper journal (edited, Advance online articles have been peer reviewed and accepted for
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 2
1
WORD COUNT: 2,858 1
ABSTRACT WORD COUNT: 250 2
3
4
5
6
MISCLASSIFICATION OF PULMONARY HYPERTENSION DUE TO RELIANCE ON PULMONARY 7
CAPILLARY WEDGE PRESSURE RATHER THAN LEFT-VENTRICULAR END-DIASTOLIC 8
PRESSURE 9
10
Scott D. Halpern, M.D., Ph.D.1,2,3
11
Darren B. Taichman, M.D., Ph.D.1 12
1Division of Pulmonary, Allergy and Critical Care Medicine;
2Center for Clinical Epidemiology 13
and Biostatistics; and 3Leonard Davis Institute of Health Economics; 14
University of Pennsylvania School of Medicine 15
16
17
18
19
ADDRESS CORRESPONDENCE AND REQUESTS FOR REPRINTS TO: 20
Scott D. Halpern 21
Center for Clinical Epidemiology and Biostatistics 22
724 Blockley Hall 23
423 Guardian Drive 24
Philadelphia, PA 19104-6021 25
Phone: (215) 898-1462 26
Fax: (215) 573-5325 27
Email: [email protected] 28
29
SUPPORT and DISCLOSURE: This work was supported by an American Thoracic Society 30
Fellows Career Development Award to Dr. Halpern. Drs. Halpern and Taichman have each 31
received support from Actelion Pharmaceuticals to conduct other research related to pulmonary 32
hypertension. The authors have no other involvement with organizations with a financial interest 33
in the subject matter.34
Page 1 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 3
2
Abstract 35
36
Background: Pulmonary arterial hypertension is typically distinguished from pulmonary venous 37
hypertension by documenting a pulmonary capillary wedge pressure (PCWP) ≤ 15mmHg. 38
However, PCWP has uncertain utility in establishing pulmonary venous hypertension. We 39
sought to determine the calibration, discrimination, and diagnostic accuracy of PCWP, using 40
simultaneously measured left-ventricular end-diastolic pressure (LVEDP) as the gold standard. 41
42
Methods: We examined hemodynamic data from the 11,523 unique patients undergoing 43
simultaneous right- and left-heart catheterization at a large academic center from 1998 – 2007. 44
45
Results: Among 4,320 patients (37.5%) with pulmonary hypertension (mean pulmonary artery 46
pressure ≥ 25mmHg), hemodynamic data were complete for 3,926 (90.9%). Of these, 580 47
(14.8%) met criteria for pulmonary arterial hypertension with a PCWP ≤ 15mmHg, but 310 48
(53.5%) of these patients had an LVEDP > 15mmHg. Such discrepancies remained common 49
among patients with a pulmonary vascular resistance > 3 Wood units and those being 50
catheterized specifically to evaluate pulmonary hypertension. PCWP provided moderate 51
discrimination between patients with high vs. normal LVEDP (area under the receiver-operating 52
characteristic curve = 0.84, 95% confidence interval = 0.81 – 0.86) but was poorly calibrated to 53
LVEDP (Bland-Altman limits of agreement: – 15.2mmHg to 9.5mmHg; Hosmer-Lemeshow 54
goodness-of-fit χ2
statistic: 155.4, p < 0.0001). 55
56
Page 2 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 4
3
Conclusions: Roughly half of patients presumed to have pulmonary arterial hypertension based 57
on PCWP may be found to have pulmonary venous hypertension based on LVEDP. Reliance on 58
PCWP may result in the dangerous or cost-ineffective use of pulmonary vasodilators for patients 59
with left-heart disease. Furthermore, without assessing LVEDP, investigators may include 60
patients with left-heart disease in therapeutic trials of PAH drugs, thereby limiting their ability to 61
detect beneficial drug effects. 62
Page 3 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 5
4
KEY WORDS: pulmonary hypertension, left-heart disease, pulmonary capillary wedge pressure, 63
hemodynamic assessment, cardiac catheterization 64
Page 4 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 6
5
ABBREVIATION LIST 65
66
AUROC, area under the receiver-operating characteristic curve 67
LVEDP, left-ventricular end-diastolic pressure 68
mPAP, mean pulmonary artery pressure 69
PAH, pulmonary arterial hypertension 70
PCWP, pulmonary capillary wedge pressure 71
PVH, pulmonary venous hypertension 72
PVR, pulmonary vascular resistance 73
TPG, transpulmonary gradient 74
WHO, World Health Organization 75
Page 5 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 7
6
Introduction 76
In approaching a patient with pulmonary hypertension, it is crucial to distinguish between 77
pulmonary arterial hypertension (PAH) and other causes of elevated pulmonary pressures, 78
including pulmonary venous hypertension (PVH) due to left-sided heart disease. The World 79
Health Organization (WHO) emphasizes the importance of such a differentiation in its 80
classification system that separates PAH (Group 1) from other forms of pulmonary hypertension 81
(e.g., Group 2 patients with left heart dysfunction).1-3
Patients with PAH may benefit from 82
recently approved prostacyclin analogues, endothelin receptor-antagonists, or phosphodiesterase 83
inhibitors.4 By contrast, in patients with PVH these same therapies are not indicated, may be 84
harmful, and initial management is best focused on amelioration of left-heart dysfunction.5, 6
85
86
Differentiation of PAH from PVH is most commonly accomplished by documenting a 87
pulmonary capillary wedge pressure (PCWP) of ≤ 15mmHg at the time of diagnostic right-heart 88
catheterization.7, 8
This diagnostic approach is predicated on the assumption that a normal 89
PCWP measurement adequately excludes left atrial hypertension. Indeed, rather than having 90
intrinsic value, the utility of the PCWP resides primarily in its ability to rule in or out disease 91
states characterized by an elevated left-ventricular end-diastolic pressure (LVEDP). 92
93
Although the assumption that PCWP is a useful surrogate marker for LVEDP has both strong 94
historical roots and substantial face validity,9 there is scant evidence regarding the abilty of 95
PCWP to establish the presence or absence of left-sided heart disease among patients with 96
pulmonary hypertension. Thus, when both PCWP and LVEDP are available in a patient with 97
pulmonary hypertension, the LVEDP is generally considered to be the gold standard. 98
Page 6 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 8
7
99
In a preliminary report of a study involving 131 patients with pulmonary hypertension, Soto and 100
colleagues found that PCWP has poor operating characteristics when tested against the standard 101
of LVEDP.10
Given the potential importance of such findings to the management of pulmonary 102
hypertension patients, we sought to determine the calibration, discrimination, and accuracy of 103
mean PCWP compared with the gold standard of LVEDP among a large cohort of patients with 104
pulmonary hypertension. 105
106
Methods 107
Patients 108
All patients undergoing right-heart catheterization at Penn-Presbyterian Medical Center – a large, 109
community-based, academic hospital and regional referral center for pulmonary vascular disease 110
affiliated with the University of Pennsylvania Health System – from January 1, 1998 – 111
December 31, 2007 were included. This study was deemed exempt from review by the 112
University of Pennsylvania Institutional Review Board because it used previously collected, de-113
identified data. 114
115
Patients were considered ineligible for the study if they had a diagnosis of mitral stenosis 116
(identified by an International Classification of Diseases – 9 code between 394.0 and 396.8 on 117
the catheterization record) or if tachycardia (>130 beats per minute) was present during 118
catheterization because these phenomena are known to cause discrepancies between PCWP and 119
LVEDP.12
Among the 2,763 patients who underwent multiple catheterizations during the study 120
period, only the first catheterization was included. 121
Page 7 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 9
8
122
Eligible patients were grouped according to whether they had a combined right- and left-heart 123
catheterization (the “combined catheterizations” group) or a right-heart catheterization alone. 124
Because patients in whom physicians order combined catheterizations may differ from those in 125
whom only right-heart catheterization is ordered, hemodynamic measurements were compared 126
between these groups to determine whether selection bias may have influenced the results. 127
128
In both groups, patients were considered to have pulmonary hypertension (PH) if their mean 129
pulmonary artery pressure (mPAP) (calculated as 2/3 pulmonary artery diastolic pressure + 1/3 130
pulmonary artery systolic pressure) was ≥ 25mmHg at rest.1 Patients were excluded if data were 131
missing for mPAP, PCWP, or LVEDP (among patients undergoing combined catheterization) 132
(Figure 1). 133
134
Hemodynamic Measurements 135
Catheterizations were performed by 10 interventional cardiologists, all of whom were board-136
certified and members of the University of Pennsylvania faculty. Hemodynamic parameters were 137
recorded directly into electronic spreadsheets and stored in a computerized database. 138
139
Physicians performing the catheterizations followed standard protocols for measuring 140
hemodynamic values. Hemodynamic values from both right- and left-heart catheterizations were 141
obtained prior to the injection of contrast for left ventriculography or coronary angiography. For 142
PCWP, values for the A-wave pressure, V-wave pressure, and mean pressure were recorded at 143
end-expiration. The mean PCWP was used for analyses. Among patients who underwent left-144
Page 8 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 10
9
heart catheterization, LVEDP was recorded simultaneously with PCWP using a pigtail catheter 145
placed in the left ventricle. 146
147
Pulmonary vascular resistance (PVR) was calculated as (mPAP – PCWP) / cardiac output 148
(measured using the estimated Fick method), and patients were classified as having elevated 149
PVR if the value was > 3 Wood units.1 Transpulmonary gradient (TPG) was calculated as mPAP 150
– PCWP, and patients were classified as having elevated TPG if the value was ≥ 12.13
151
152
Statistical Analysis 153
The accuracy of a mean PCWP ≤ 15mmHg vs. > 15mmHg in distinguishing between WHO 154
Groups 1 and 2 PH (i.e. PAH versus PVH) was assessed by calculating the proportion of patients 155
that would be reclassified by instead using LVEDP of ≤ 15mmHg vs. > 15mmHg. 156
157
The calibration of PCWP to LVEDP was assessed using a Bland-Altman analysis14
and the 158
Hosmer-Lemeshow goodness-of-fit test.15
When conducting the goodness-of-fit test, LVEDP 159
was dichotomized as ≤ 15mmHg vs. > 15mmHg; sensitivity analyses were performed using 160
LVEDP cut-points from 10 to 20mmHg. 161
162
The area under the receiver-operating characteristic curve (AUROC)16
was calculated to 163
determine the ability of PCWP to discriminate patients with LVEDP ≤ 15mmHg vs. > 15mmHg. 164
Wilcoxon rank-sum tests were used to compare hemodynamic values between patients who 165
underwent combined catheterizations vs. right-heart catheterization alone. Stata 9.2 (Stata Corp., 166
College Station, Texas) was used for all analyses. 167
Page 9 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 11
10
168
Results 169
There were 12,744 eligible unique patients who underwent right-heart catheterization at our 170
institution from 1998 – 2007. Of these, 11,523 had combined catheterizations, and 4,320 (37.5%) 171
of these patients had PH (Figure 1). 172
173
Disease classification 174
Among 3,926 patients (90.9%) with PH and complete data, 580 (14.8%) met criteria for PAH 175
based on a low PCWP (≤ 15mmHg). However, 310 (53.5%) of these patients would be 176
classified as having PVH if LVEDP were used instead (Table – Panel A and Figure 2). By 177
contrast, among the 3,346 patients classified as having PVH using PCWP, only 152 (4.5%) 178
would meet criteria for PAH if LVEDP were used instead. 179
180
To determine rates of misclassification among patients who might be considered to have 181
“pulmonary hypertension out of proportion to left-heart disease,5, 6
” we restricted our analyses to 182
those patients with either a PVR > 3 Wood units (1,116 patients) or a TPG > 12 (1,300 patients). 183
Among patients with an elevated PVR, 361 (32.4%) would be classified as PAH using PCWP, 184
but 148 of these (41.0%) would be reclassified as PVH based upon the LVEDP (Table – Panel 185
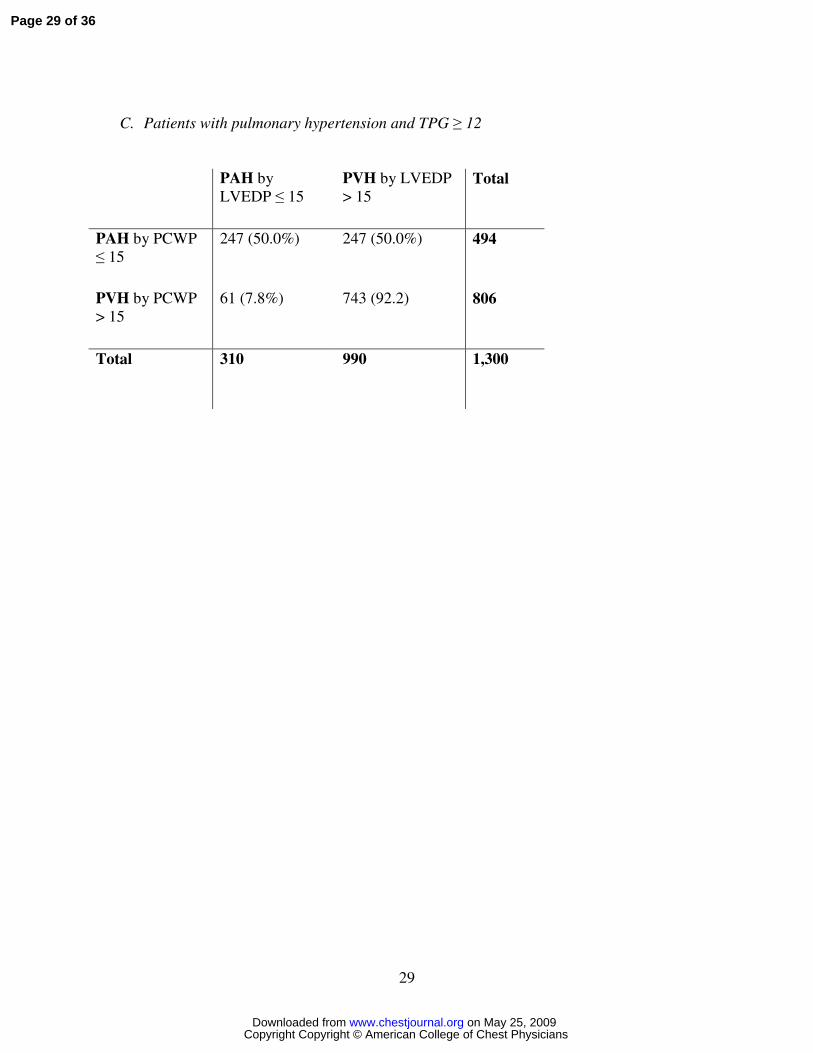
B). Among patients with an elevated TPG, 494 (38.0%) would be classified as PAH using 186
PCWP, but 247 of these (50.0%) would be reclassified as PVH based upon the LVEDP (Table – 187
Panel C). 188
189
Page 10 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 12
11
Compared with patients undergoing right-heart catheterization alone, the patients who underwent 190
combined catheterizations had a lower PVR (median = 2.1 Wood units, interquartile range 1.4 – 191
3.3 vs. median = 3.2 Wood units, interquartile range 1.9 – 5.9; p < 0.0001) and TPG (median = 192
9.8, interquartile range 6.7 – 14.0 vs. median = 13.3, interquartile range 8.0 – 24.3; p < 0.0001). 193
However, the two groups had similar PCWP (median = 22.0mmHg, interquartile range 14.0 – 194
30.0 vs. median = 22.0mmHg, interquartile range 18.0 – 27.0; p = 0.31). 195
196
Disease classification among patients catheterized specifically for evaluation of PH 197
To more specifically address the utility of left-heart catheterization among patients being 198
evaluated for PH, we restricted analyses to the 604 patients who were referred for catheterization 199
by PH specialists as part of their initial evaluation of PH. Of these, 340 (56.3%) had a combined 200
catheterization, and 282 (83.9%) of these patients had PH. Of the 265 patients with documented 201
PH, who had been referred for combined catheterization as part of their PH evaluation, and for 202
whom LVEDP was measured, 164 (61.9%) met criteria for PAH by virtue of having a PCWP ≤ 203
15mmHg, but 34 of these patients (20.7%) had an LVEDP > 15mmHg. 204
205
Calibration 206
In the complete sample of patients with PH and combined catheterizations, Bland-Altman 207
analysis revealed that on average, PCWP underestimated LVEDP by 2.9 mmHg (95% CI = 2.7 – 208
3.0) (Figure 3). In 39.0% of patients, the absolute difference between PCWP and LVEDP was > 209
5mmHg; in 11.3% it was > 10mmHg. The 95% limits of agreement were -15.2 mmHg to 210
9.5mmHg, indicating that even after excluding the 5% of patients with the most discrepant 211
Page 11 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 13
12
values between PCWP and LVEDP, the PCWP underestimated LVEDP by as much as 15.2 212
mmHg and overestimated LVEDP by as much as 9.5 mmHg. 213
214
Using LVEPD ≤ 15mmHg vs. > 15mmHg as a dichotomous outcome in a logistic regression 215
model, the calibration of PCWP was poor, as indicated by a Hosmer-Lemeshow χ2statistic of 216
155.4 (p < 0.0001). The goodness-of-fit test remained significant (indicating poor calibration) 217
for all cutpoints of LVEDP between 10mmHg and 20mmHg. 218
219
Because the large sample size could account for the statistical significance of the goodness-of-fit 220
test, we performed 1000 iterations of bootstrap resampling with 20% random samples of the total 221
(785 patients each). The goodness-of-fit test remained significant in 72.4% of these samples, 222
confirming the poor calibration. 223
224
Discrimination 225
The AUROC was 0.84 (95% CI = 0.81 – 0.86) (Figure 4). This indicates that among all 226
randomly selected pairs of patients in which one has an LVEDP ≤ 15mmHg and the other has an 227
LVEDP > 15mmHg, the patient with the higher LVEDP would have a higher PCWP in 84% of 228
cases. These results were similar using LVEDP cut-points of 10mmHg or 20mmHg (Figure 4). 229
230
Comparison with patients without pulmonary hypertension 231
Among 7,117 patients who underwent combined catheterizations and did not have pulmonary 232
hypertension, complete data were available in 6,551 (92.0%) patients. Misclassification was also 233
evident among these patients, as 2,253 of 5,454 patients with PCWP ≤ 15mmHg (41.3%) had 234
LVEDP > 15mmHg. A Bland-Altman analysis of calibration in this group revealed that PCWP 235
Page 12 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 14
13
underestimated LVEDP by 4.7 mmHg (95% CI = 4.6 – 4.8), with 95% limits of agreement from 236
-14.5mmHg to 5.1mmHg. Finally, the ability of PCWP to discriminate patients with high or low 237
LVEDP among patients without pulmonary hypertension, as assessed by the AUROC, was 80% 238
(95% CI = 79% – 81%). 239
240
241
Discussion 242
This study of a large number of patients undergoing sequential measurement of PCWP and 243
LVEDP suggests that PCWP frequently underestimates LVEDP, that it is poorly calibrated to 244
LVEDP, and that it has a moderate ability to discriminate between patients with normal or 245
elevated LVEDP. Perhaps most importantly, these results suggest that approximately half of all 246
patients who meet hemodynamic criteria for PAH on the basis of PCWP measurements may, in 247
fact, have elevated left-ventricular filling pressures. 248
249
This degree of misclassification was robust even when we restricted the sample to patients with 250
an elevated PVR or TPG, groups hypothesized to be more homogenous and reflective of true 251
PAH patients.5 These results emphasize the importance of avoiding the conclusion that a patient 252
has “pulmonary hypertension out of proportion to left heart disease” without evaluating the 253
LVEDP. 254
255
Although many of the patients in our study underwent cardiac catheterization for reasons other 256
than evaluation of PH, disease misclassification remained common even among patients 257
specifically referred for catheterization by PH specialists as part of their PH evaluation. Among 258
Page 13 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 15
14
such selected patients, one fifth of those who would be classified as having PAH by PCWP 259
would instead be classified as having PVH by LVEDP. 260
261
Bias resulting from the selective referral of certain patients for combined catheterization is 262
unlikely to have influenced these results. First, discrepancies between PCWP and LVEDP 263
persisted even among patients with elevations in PVR or TPG. Second, the median PCWP did 264
not differ between patients undergoing combined catheterization versus those undergoing right-265
heart catheterization. 266
267
The clinical consequences of mistakenly classifying patients as having PAH when left-heart 268
disease is present are incompletely understood. However, the potential for PAH-specific 269
therapies such as pulmonary vasodilators to precipitate the acute deterioration of patients with 270
PVH is well described.5, 6, 17
Even if frank deterioration occurs infrequently following use of 271
PAH therapies for patients with PVH, there are no high-quality data to suggest that patients with 272
PVH would benefit from these therapies. It is thus critical to make the correct diagnosis prior to 273
instituting therapies that are inappropriate, potentially harmful, and tremendously expensive. 274
275
In addition to these clinical considerations, disease misclassification due to reliance on PCWP 276
may influence the results of clinical trials. For example, the modest mean treatment effects 277
noted in most randomized trials of approved treatments for PAH may be attributable, in part, to 278
the enrollment of heterogeneous patient populations. If only some enrolled patients are afflicted 279
with diseases likely to respond to these therapies, summary treatment effect estimates would be 280
Page 14 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 16
15
biased toward the null and would not reflect the treatment benefits that true PAH patients might 281
achieve. 282
283
The implications of this study depend, in part, on the mechanisms that account for the poor 284
correspondence between PCWP and LVEDP in patients with pulmonary hypertension. One 285
possibility is that the observed measurement errors are attributable to fundamental alterations of 286
the pulmonary vascular bed among patients with pulmonary hypertension that make it difficult to 287
obtain an accurate PCWP.5 However, this explanation seems unlikely because the poor 288
calibration and moderate discrimination of PCWP were similarly evident among patients without 289
pulmonary hypertension. 290
291
Second, it is possible that PCWP systematically underestimates LVEDP in all patients. This 292
conclusion is supported by the consistent underestimation noted in our study among patients with 293
and without pulmonary hypertension, as well as by smaller studies showing that PCWP 294
underestimates LVEDP in the contexts of acute myocardial infarction18
and generalized critical 295
illness.19
However, the width of the limits of agreement in the Bland-Altman analysis and the 296
consistently poor fit of the regression slope between PCWP and LVEDP suggest that systematic 297
bias is not the only problem. Thus, clinicians cannot overcome this problem simply by adding a 298
set value to the PCWP to better estimate LVEDP or by using a different PCWP cutpoint. 299
300
Rather, the observed measurement variability suggests that PCWP is genuinely unreliable in 301
estimating left-ventricular filling pressure, that physicians err in measuring PCWP or LVEDP, or 302
that both of these explanations are true. These hypotheses have been offered previously in 303
Page 15 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 17
16
attempts to explain the consistently negative or null effects of right-heart catheterization to guide 304
therapy in many critically ill populations,20-25
including patients with left-ventricular disease.24
305
306
The present study is limited by our inability to directly review the hemodynamic tracings from 307
the catheterizations because they were not routinely stored during the study period. Thus, we 308
cannot exclude the possibility that although PCWP was recorded as a mean pressure, LVEDP 309
may have been recorded following the A wave in some patients. This could cause PCWP to 310
underestimate LVEDP. Other measurement errors, however, are unlikely to explain our results. 311
Contrast injection for ventriculography or coronary angiography might artificially elevate the 312
LVEDP, but LVEDP was measured before contrast injection in this study. Additionally, 313
although physicians did not routinely confirm proper wedge position by measuring pulmonary 314
venous saturation with the balloon inflated,5 difficulties obtaining a proper wedge position in 315
patients with pulmonary hypertension should cause PCWP to overestimate LVEDP, whereas we 316
found the opposite. Furthermore, because these “wedge saturations” are not routinely performed 317
in most settings, our results may reflect current practice more generally. 318
319
A second limitation of this study is that the use of deidentified data precluded assessment of 320
whether discrepancies between PCWP and LVEDP were particularly common when the 321
catheterizations were performed by specific physicians. However, the validity and 322
generalizability of our results are supported by the similar findings of Soto and colleagues10
at a 323
different institution. 324
325
Page 16 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 18
17
Third, we were unable to evaluate whether specific subgroups of patients were particularly likely 326
to have discrepant PCWP and LVEDP values. Patients with left ventricular diastolic dysfunction 327
(e.g., older patients with long-standing systemic hypertension), may be particularly likely to have 328
PVH despite a low PCWP measurement.17
Because the de-identified nature of our data 329
precluded confirmation of this hypothesis, future studies are needed to determine whether certain 330
patient characteristics can be used to help clinicians determine when discrepancies between 331
PCWP and LVEDP are likely to be present. 332
333
Conclusions 334
Some might conclude from our results that LVEDP should be measured routinely among all 335
patients referred for catheterization as part of an evaluation for pulmonary hypertension. 336
However, this approach carries increased risks and inconveniences for patients as well as 337
increased costs and resource utilization. We therefore suggest a more conservative approach in 338
routine practice in which clinicians obtain left-heart hemodynamic measurements whenever there 339
are reasons to suspect left-heart disease based on the patient’s history or physical exam, 340
whenever the diagnosis is uncertain following right-heart catheterization, and when patients do 341
not show favorable responses to initial therapy. If future studies identify types of patients who 342
are particularly likely to have discrepancies between PCWP and LVEDP, then combined 343
catheterization may represent a prudent initial diagnostic approach in such patients. 344
345
Ultimately, a randomized trial may be needed to determine whether treatment guided by 346
combined catheterizations leads to improved patient-centered outcomes such as quality of life, 347
symptom control, or mortality; such evidence would provide the strongest possible justification 348
Page 17 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 19
18
for routinely measuring LVEDP. Indeed, such an approach may prove to be cost-effective or 349
even cost-saving if it helps prevent the needless and potentially dangerous prescription of 350
expensive PAH therapies. 351
Page 18 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 20
19
References 352
1. Galie N, Torbicki A, Barst R, et al. Guidelines on diagnosis and treatment of pulmonary 353
arterial hypertension. The Task Force on Diagnosis and Treatment of Pulmonary Arterial 354
Hypertension of the European Society of Cardiology. European Heart Journal 2004;25:2243-78. 355
2. Rubin LJ, American College of Chest P. Diagnosis and management of pulmonary 356
arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest 2004;126:7S-357
10S. 358
3. Taichman DB, Mandel J. Epidemiology of pulmonary arterial hypertension. Clinics in 359
Chest Medicine 2007;28:1-22. 360
4. Badesch DB, Abman SH, Simonneau G, Rubin LJ, McLaughlin VV. Medical therapy for 361
pulmonary arterial hypertension: updated ACCP evidence-based clinical practice guidelines. 362
Chest 2007;131:1917-28. 363
5. Benza RL, Tallaj JA. Pulmonary hypertension out of proportion to left heart disease. 364
Advances in Pulmonary Hypertension 2005;5:21-9. 365
6. Oudiz RJ. Pulmonary hypertension associated with left-sided heart disease. Clinics in 366
Chest Medicine 2007;28:233-41. 367
7. Barst RJ, McGoon M, Torbicki A, et al. Diagnosis and differential assessment of 368
pulmonary arterial hypertension. Journal of the American College of Cardiology 2004;43:40S-369
7S. 370
8. McLaughlin VV, McGoon MD. Pulmonary arterial hypertension. Circulation 371
2006;114:1417-31. 372
9. Fishman AP. A century of pulmonary hemodynamics. American Journal of Respiratory 373
& Critical Care Medicine 2004;170:109-13. 374
10. Soto FJ, Siegel R, Marks D, et al. Performance of pulmonary capillary wedge pressure 375
(PCWP) vs. left ventricular end diastolic pressure (LVEDP) in the diagnosis/classification of 376
patients with suspect pulmonary arterial hypertension. Chest 2005;128:137S [abstract]. 377
11. Halpern SD, Taichman DB. Misclassification of pulmonary arterial hypertension due to 378
use of pulmonary capillary wedge pressure (PCWP) Rather than left-ventricular end-diastolic 379
pressure (LVEDP) [abstract]. American Journal of Respiratory & Critical Care Medicine 380
2008;177:A259. 381
Page 19 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 21
20
12. Pulmonary Artery Catheter Education Project (PACEP). (Accessed June 8, 2008, at 382
www.pacep.org.) 383
13. Klotz S, Wenzelburger F, Stypmann J, et al. Reversible pulmonary hypertension in heart 384
transplant candidates: To transplant or not to transplant. The Annals of Thoracic Surgery 385
2006;82:1770-3. 386
14. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods 387
of clinical measurement. Lancet 1986;i:307-10. 388
15. Hosmer DW, Lemeshow S. Model building strategies and methods for logistic 389
regression. In: Hosmer DW, Lemeshow S, eds. Applied Logistic Regression, 2nd Edition. New 390
York: John Wiley & Sons; 2000. 391
16. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating 392
characteristic (ROC) curve. Radiology 1982;143:29-36. 393
17. Soto FJ. Pulmonary venous hypertension: A diagnostic and therapeutic dilemma. 394
Advances in Pulmonary Hypertension 2007;6:168-75. 395
18. Rahimtoola SH, Sinno MZ, Rosen KM, et al. Relationship of pulmonary-artery to left 396
ventricular diastolic pressures in acute myocardial infarction. Circulation 1972;46:283-90. 397
19. Calvin JE, Driedger AA, Sibbald WJ. Does the pulmonary capillary wedge pressure 398
predict left ventricular preload in critically ill patients? Crit Care Med 1981;9:437-43. 399
20. Harvey S, Harrison D, Singer M, et al. Assessment of the clinical effectiveness of 400
pulmonary artery catheters in management of patients in intensive care (PAC-Man): a 401
randomised controlled trial. Lancet 2005;366:472-7. 402
21. Richard C, Warszawski J, Anguel N, et al. Early Use of the Pulmonary Artery Catheter 403
and Outcomes in Patients With Shock and Acute Respiratory Distress Syndrome: A Randomized 404
Controlled Trial. JAMA 2003;290:2713-20. 405
22. Sandham JD, Hull RD, Brant RF, et al. A Randomized, Controlled Trial of the Use of 406
Pulmonary-Artery Catheters in High-Risk Surgical Patients. N Engl J Med 2003;348:5-14. 407
23. Shah MR, Hasselblad V, Stevenson LW, et al. Impact of the pulmonary artery catheter in 408
critically ill patients: Meta-analysis of randomized clinical trials. JAMA 2005;294:1664-70. 409
24. The ESCAPE Investigators and ESCAPE Study Coordinators. Evaluation study of 410
congestive heart failure and pulmonary artery catheterization effectiveness: The ESCAPE trial. 411
JAMA 2005;294:1625-33. 412
Page 20 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 22
21
25. The National Heart Lung and Blood Institute Acute Respiratory Distress Syndrome 413
(ARDS) Clinical Trials Network. Pulmonary-Artery versus Central Venous Catheter to Guide 414
Treatment of Acute Lung Injury. N Engl J Med 2006;354:2213-24. 415
26. Rubenfeld GD, McNamara-Aslin E, Rubinson L. The pulmonary artery catheter, 1967-416
2007. Rest in peace? JAMA 2007;298:458-61. 417
418
Page 21 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 23
22
Legend to Figure 1 419
420 RHC, right-heart catheterization; LHC, left-heart catheterization; mPAP, mean pulmonary artery 421
pressure; PCWP, pulmonary capillary wedge pressure; LVEDP, left ventricular end-diastolic pressure. 422
Page 22 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 24
23
Legend to Table 423
Percentages reflect proportions within rows. PAH, pulmonary arterial hypertension; PVH, pulmonary 424
venous hypertension; PCWP, pulmonary capillary wedge pressure; LVEDP, left ventricular end-425
diastolic pressure; TPG, transpulmonary gradient. 426
Page 23 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 25
24
Legend to Figure 2 427
PCWP, pulmonary capillary wedge pressure; LVEDP, left ventricular end-diastolic pressure. 428
Page 24 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 26
25
Legend to Figure 3 429
*Difference represents PCWP – LVEDP, Average represents (PCWP + LVEDP)/2. Larger circles 430
represent identical observations among multiple patients. Mean bias = -2.9 mmHg (95% CI = -3.0 – -2.7); 431
Limits of agreement = -15.2 – 9.5 mmHg. PCWP, pulmonary capillary wedge pressure; LVEDP, left 432
ventricular end-diastolic pressure. 433
Page 25 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 27
26
Legend to Figure 4 434
Area under receiver-operating characteristic curve (AUROC) = 0.84 (95% CI = 0.81 – 0.86) 435
using a cutpoint of LVEDP of ≤15 mmHg to indicate PAH. If a cutpoint of LVEDP ≤ 10 mmHg 436
were used, the AUROC would be 0.86 (95% CI = 0.82 – 0.91). If a cutpoint of LVEDP ≤ 20 437
mmHg were used, the AUROC would be 0.81 (95% CI = 0.80 – 0.83). Sens, sensitivity for the 438
outcome of LVEDP > 15 mmHg; Spec, specificity for the outcome of LVEDP > 15 mmHg; 439
PCWP, pulmonary capillary wedge pressure; LVEDP, left ventricular end-diastolic pressure. 440
Page 26 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 28
27
Figure 1: Flow diagram
RHC performed: 12,823 Patients
Simultaneous LHC and RHC: 11,523
patients
RHC only: 1,211 patients
mPAP ≥ 25
mmHg: 4,320
mPAP < 25
mmHg: 7,117 mPAP ≥ 25
mmHg: 873
mPAP < 25
mmHg: 338
mPAP
missing: 86
LVEDP
missing: 346
PCWP
missing: 48
PCWP
missing: 6
3,926 evaluable
patients with
pulmonary
hypertension
867 evaluable
patients with
pulmonary
hypertension
PCWP ≤ 15:
580
PCWP > 15:
3,346
PCWP ≤ 15:
240
PCWP > 15:
627
Eligible for study: 12,744 Patients
Excluded due to:
mitral stenosis: 69
tachycardia: 25
Page 27 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 29
28
Table: Classification of PAH using PCWP or LVEDP
A. All patients with pulmonary hypertension
PAH by
LVEDP ≤ 15
PVH by LVEDP
> 15 Total
PAH by PCWP
≤ 15
270 (46.5%) 310 (53.5%)
580
PVH by PCWP
> 15
152 (4.5%) 3,194 (95.5%) 3,346
Total 422 3,504 3,926
B. Patients with pulmonary hypertension and PVR > 3
PAH by
LVEDP ≤ 15
PVH by LVEDP
> 15 Total
PAH by PCWP
≤ 15
213 (59.0%) 148 (41.0%)
361
PVH by PCWP
> 15
65 (8.6%) 690 (91.4) 755
Total 278 842 1,116
Page 28 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 30
29
C. Patients with pulmonary hypertension and TPG ≥ 12
PAH by
LVEDP ≤ 15
PVH by LVEDP
> 15 Total
PAH by PCWP
≤ 15
247 (50.0%) 247 (50.0%)
494
PVH by PCWP
> 15
61 (7.8%) 743 (92.2) 806
Total 310 990 1,300
Page 29 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 31
30
Figure 2: Scatter plot of PCWP and LVEDP among 3,926 patients with pulmonary
hypertension
0
510
15
20
25
30
35
40
45
50
LV
ED
P
0 5 10 15 20 25 30 35 40 45 50PCWP
Page 30 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 32
31
Figure 3: Bland-Altman plot of PCWP and LVEDP among 3,926 patients with pulmonary
hypertension
Diffe
ren
ce
Average0 10 20 30 40 50
-40
-30
-20
-10
0
10
20
30
40
Page 31 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 33
32
Figure 4: Receiver operating-characteristic curve of PCWP against LVEDP among 3,926
patients with pulmonary hypertension
0.0
00.2
50.5
00.7
51.0
0S
en
sitiv
ity
0.00 0.25 0.50 0.75 1.001 - Specificity
Area under ROC curve = 0.8254
PCWP = 15mmHg
Sens = 94.2%,
Spec = 60.2%
Page 32 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 34
215x282mm (600 x 600 DPI)
Page 33 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 35
215x283mm (600 x 600 DPI)
Page 34 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 36
215x283mm (600 x 600 DPI)
Page 35 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 37
215x283mm (600 x 600 DPI)
Page 36 of 36
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from
Page 38
DOI 10.1378/chest.08-2784; Prepublished online March 2, 2009;Chest
Scott D. Halpern and Darren B. TaichmanPressure
Capillary Wedge Pressure Rather Than Left-Ventricular End-Diastolic Misclassification of Pulmonary Hypertension Due to Reliance on Pulmonary
May 25, 2009This information is current as of
& ServicesUpdated Information
784http://www.chestjournal.org/content/early/2009/02/20/chest.08-2figures, can be found at:Updated Information and services, including high-resolution
Open Access Freely available online through CHEST open access option
Permissions & Licensing
http://www.chestjournal.org/site/misc/reprints.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.chestjournal.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
Email alerting serviceup in the box at the top right corner of the online article.Receive free email alerts when new articles cit this article. sign
formatImages in PowerPoint
article figure for directions.teaching purposes in PowerPoint slide format. See any online Figures that appear in CHEST articles can be downloaded for
articles must include the digital object identifier (DOIs) and date of initial publication. priority; they are indexed by PubMed from initial publication. Citations to Advance online prior to final publication). Advance online articles are citable and establish publicationyet appeared in the paper journal (edited, typeset versions may be posted when available Advance online articles have been peer reviewed and accepted for publication but have not
Copyright Copyright © American College of Chest Physicians on May 25, 2009www.chestjournal.orgDownloaded from