15
Mixed Connective Tissue Disease by Farshid Mokhberi Shahid beheshti University Of Medical Sciences & health services
| Date post: | 13-Apr-2017 |
| Category: |
Documents |
| Upload: | samisaz-pharmaceutical-co |
| View: | 412 times |
| Download: | 0 times |

Mixed Connective Tissue Disease
by
Farshid MokhberiShahid beheshti University Of Medical Sciences & health
services
Definition
•Mixed connective-tissue disease (MCTD) was first recognized by Sharp and colleagues (1972) in a group of patients with overlapping clinical features:
Systemic lupus erythematosus Scleroderma Myositis
Pathophysiology•B-lymphocyte hyperactivity•T-lymphocyte activationin•Apoptotic modification of the U1-70 kd
antigen•Immune response against apoptotically
modified self-antigens•Genetic association with major
histocompatibility genes human leukocyte antigen (HLA)–DRB1*04/*15
•Vascular endothelial proliferation with widespread lymphocytic and plasmacytic infiltration of tissues
Etiology• The fundamental cause of MCTD remains
unknown.
• Autoimmunity to components of the U1-70 kd snRNP are a hallmark of disease. Anti-RNP antibodies can precede overt clinical manifestations of MCTD but after 1 year.
• The loss of T-lymphocyte and B-lymphocyte tolerance, abnormalities of apoptosis, or molecular mimicry by infectious agents, and driven by U1-RNA-induced innate immune responses, are proposed current theories of pathogenesis.
Differential Diagnoses
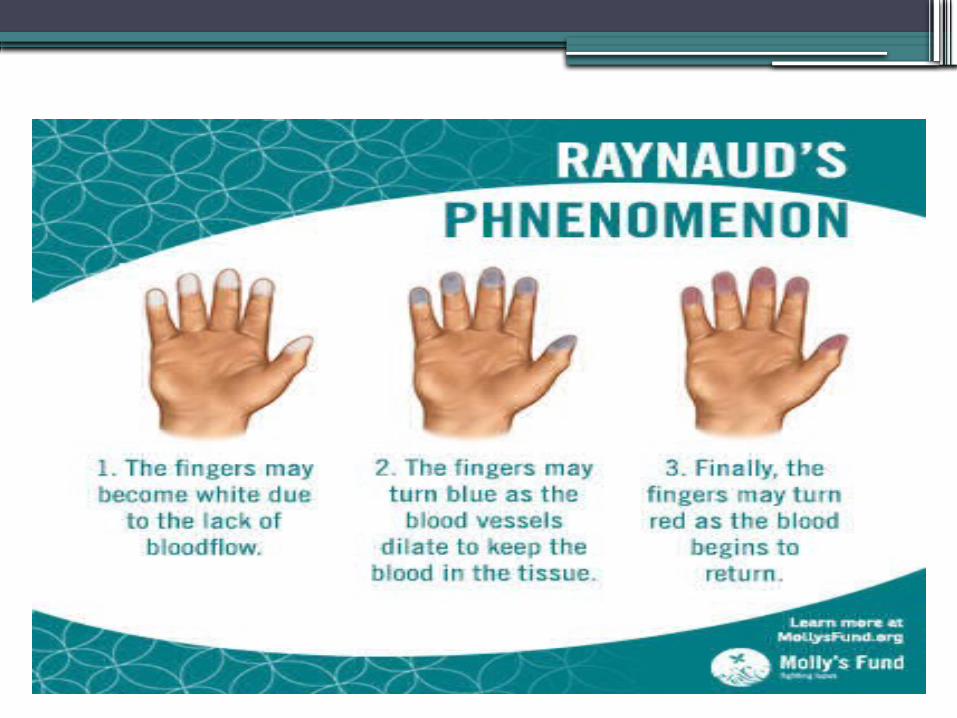
•Bacterial Sepsis•Dermatomyositis•Polymyositis•Primary Pulmonary Hypertension•Raynaud Phenomenon•Rheumatoid Arthritis•Scleroderma•Systemic Lupus Erythematosus (SLE)
Diagnosis•High titers of anti-U1-RNP antibody, of SLE,
scleroderma, and inflammatory myositis.•High-titer speckled pattern fluorescent
antinuclear antibody (FANA) is typical of MCTD
•Anti-RNP antibodies are required for diagnosis of MCTD.The presence of anti–U1-70 kd is characteristic of MCTD.
•MCTD can enter sustained remission later in the clinical course. Anti-RNP autoantibodies typically become undetectable in patients in remission.
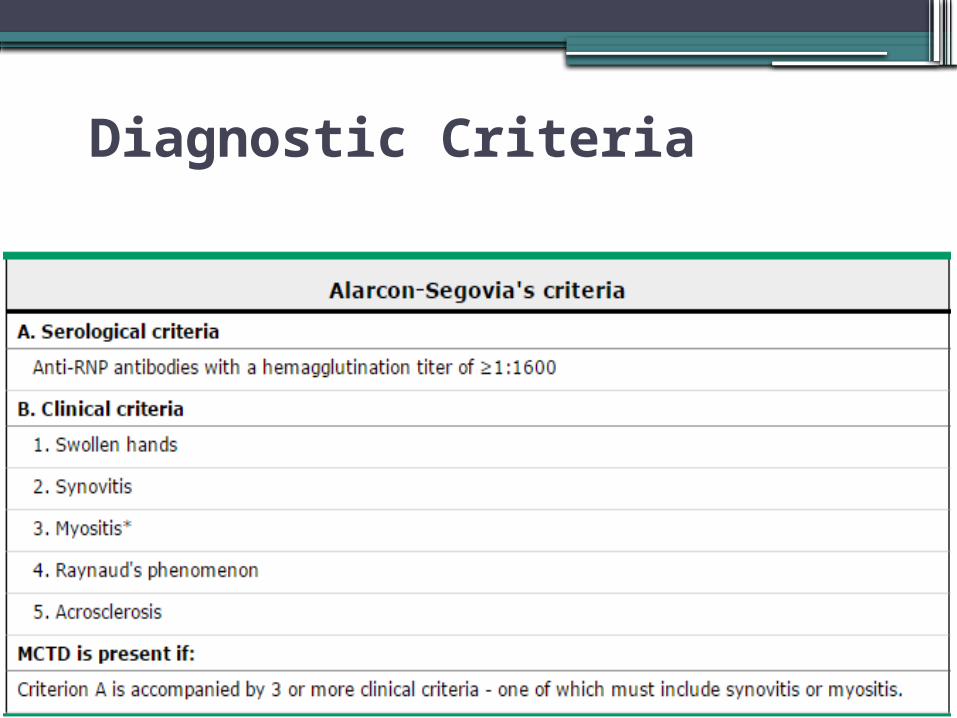
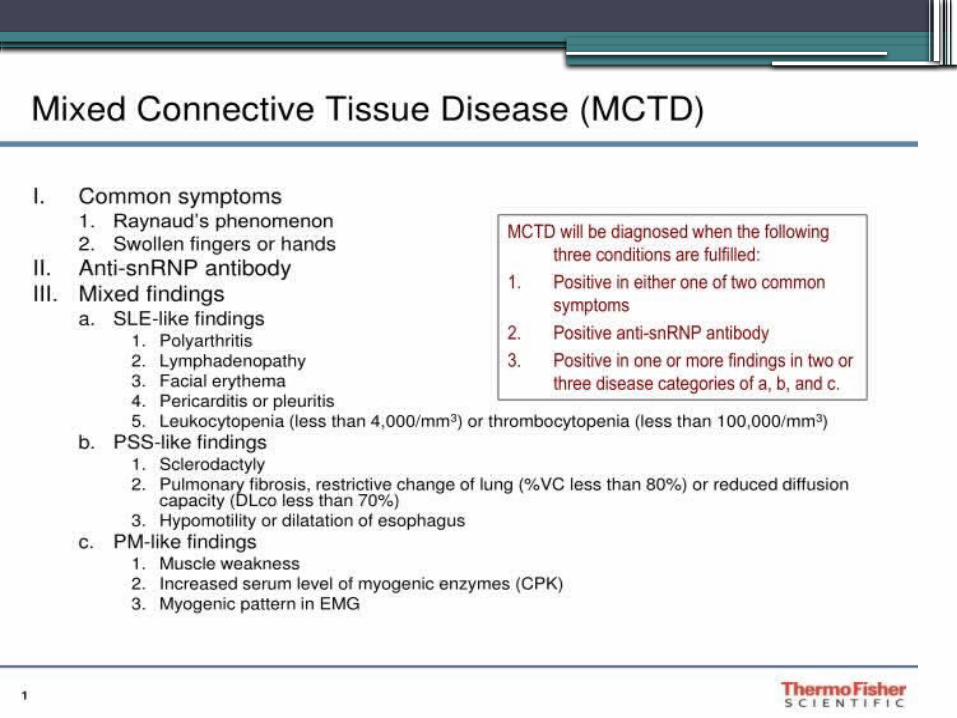
Diagnostic Criteria
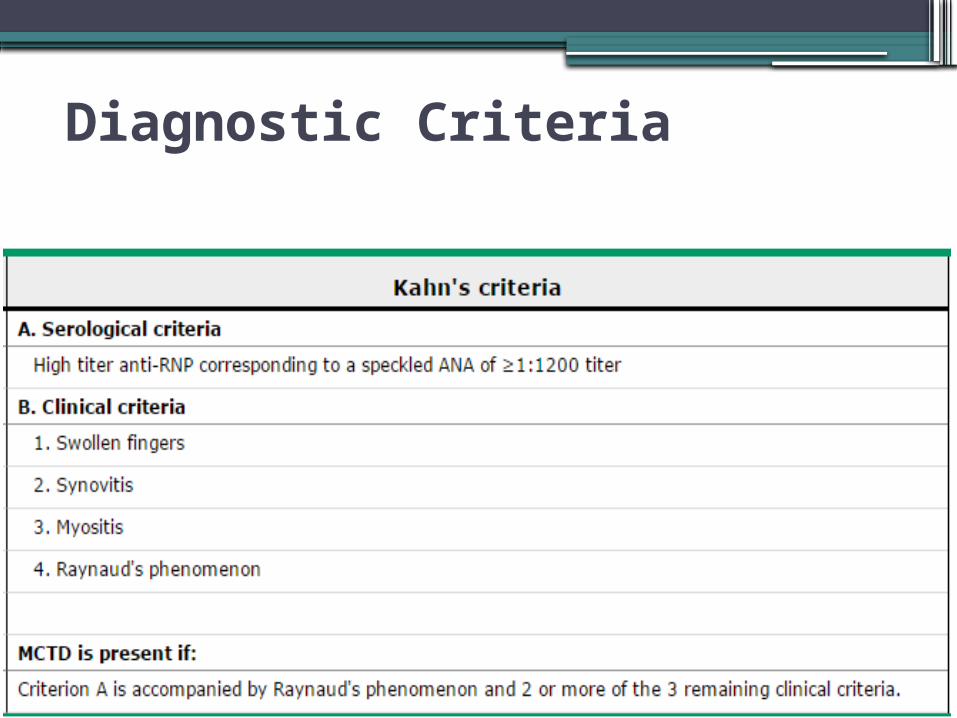
Diagnostic Criteria
Imaging Studies•Chest radiography : infiltrates, effusion, or
cardiomegaly
•Echocardiography: effusion ,pulmonary hypertension
•Ultrasonography/CT scanning :abdominal pain (indicated for evidence of serositis, pancreatitis, or visceral perforation related to vasculitis)
•MRI - Used to assess neuropsychiatric signs or symptoms
Treatment•MCTD: extremely responsive to Glucocorticoids

Prognosis Mortality:
• Progressive pulmonary hypertension and its cardiac complications.
• Pulmonary hypertension due to scleroderma-like vasculopathy can lead to death in a few weeks.
• Myocarditis
• Renovascular hypertension and cerebral hemorrhage
Morbidity:
• recurrent musculoskeletal pain
• low energy levels
• Flares of polymyositis
• glucocorticoid use:
aseptic necrosis, vertebral compression fractures, cataracts, weight gain, accelerated atherosclerosis, nosocomial infections, and proximal myopathy.
•Thanks for your attention

















