40
MNT For Anemia By: Hayley Morgan By: Hayley Morgan
| Date post: | 22-Dec-2015 |
| Category: |
Documents |
| Upload: | augustine-cunningham |
| View: | 217 times |
| Download: | 2 times |

MNT For Anemia
By: Hayley Morgan
By: Hayley Morgan

What is Anemia?
Inability of blood to supply tissues with adequate oxygen for proper metabolic function. Diagnosis made by patient history, physical exam, signs and symptoms, and hematological laboratory findings. Usually associated with decreased levels of hemo- globin or hematocrit (packed red cell volume) – Abnormal hemoglobin may give appearance of anemia (methemoglobin). Usually associated with decreased RBCs.

Types of anemia
Iron Deficiency AnemiaMegaloblastic AnemiaPernicious AnemiaAnemia of Chronic DiseaseAplastic AnemiaBlood Loss AnemiaFanconi AnemiaHemolytic AnemiaSickle Cell AnemiaThalassemias (Cooley’s Anemia)

Types of Anemia
Microcytic (<80 fL) • Iron deficiency • Thalassemia • Anemia of chronic disease
Macrocytic (>100 fL)• Vitamin B12 deficiency• Folate deficiency • Myelodysplasia• Chemotherapy• Liver disease • Increased reticulocytosis• Myxedema
Normocytic• Anemia of chronic disease• Aplasia• Protein-energy malnutrition• Chronic renal failure• Post-hemorrhagic

Iron deficiency anemia
Iron Stores• Humans contain ~2.5g of iron, with 2.0-2.5g circulating as part of heme in hemoglobin.• Another ~0.3g found in myoglobin, in heme cytochromes, and in Fe-S complexes.• Iron stored in body primarily as protein complexes (ferritin and hemosiderin.)
Nutritional Iron Balance Intake • Dietary iron intake• Medicinal iron• PRBC transfusions
Excretion • Gastrointestinal
bleeding • Menses• Other forms of bleedings• Loss of epidermal cells
for the skin and gut

Assessment
Physical Exam• Cheilosis
• Fissures at the corner of the mouth
• Koilonychia• Spooning of
the fingernails
Biochemical Findings• Hypochromic (Low Hemoglobin)• Microcytic Cells (Low MCV)• Target Cells (Codocytes)
Signs and Symptoms• Pale or yellow “sallow” skin• Unexplained fatigue/ lack of energy• Shortness of Breathe• Headaches• Picophagia, craving ice or clay

Treatment
MNT
• Diet: beef, poultry, especially organ meats. Fish; especially shellfish, sardines, and anchovies. Leafy greens like the cabbage family, broccoli, kale, and spinach. Legumes, and iron enriched pastas.
• Iron supplements: 50-200mg of inorganic ferrous form supplement. Vitamin C supplement can increase absorption.
Other
• IV Iron; patient can not tolerate oral supplementation, severe iron deficiency, chronic bleeding, and patients receiving supplemental erythropoietin.
• Blood Transfusions

Megaloblastic Anemia
• Due to impaired DNA synthesis
• Affects cells primarily having relatively rapid turnover, especially hematopoietic precursors and gastrointestinal epithelial cells
• Cell division is sluggish, but cytoplasmic development progresses normally, so megaloblastic cells tend to be large, with an increased ratio of RNA to DNA.
• Megaloblastic erythroid progenitors tend to be destroyed in the marrow
• Marrow cellularity is often increased but production of red blood cells (RBC) is decreased

Assessment• Vitamin B12 Deficiency
• Inadequate intake: vegans (rare) • Malabsorption
• Defective release of cobalamin from food • Gastric achlorhydria• Partial gastrectomy• Drugs that block acid secretion • Inadequate production of intrinsic factor (IF)
• Pernicious anemia• Total gastrectomy
• Disorders of terminal ileum• Sprue• Regional enteritis• Intestinal resection
• Competition for cobalamin • Fish tapeworm (Diphyllobothrium latum)• Bacteria: "blind loop" syndrome • Drugs: p-aminosalicylic acid, colchicine, neomycin

Assessment
• Hematologic• High MCV• High MCH• Low RBC count
• Gastrointestinal• Glossitis• Anorexia• Diarrhea
• Neurologic (found in 3/4th of individuals with pernicious anemia)• Numbness and paresthesia in the extremities, Weakness, Ataxia• Sphincter disturbances• Disturbances of mentation
• Mild irritability and forgetfulness to severe dementia or frank psychosis.
• Demyelination, Axonal degeneration, and then Neuronal death• Last stage is irreversible
Megaloblastic Anemia
• Macrocytic RBC
• Hypersegmented Neutrophil

Vitamin b12 absorption
• Oral Phase
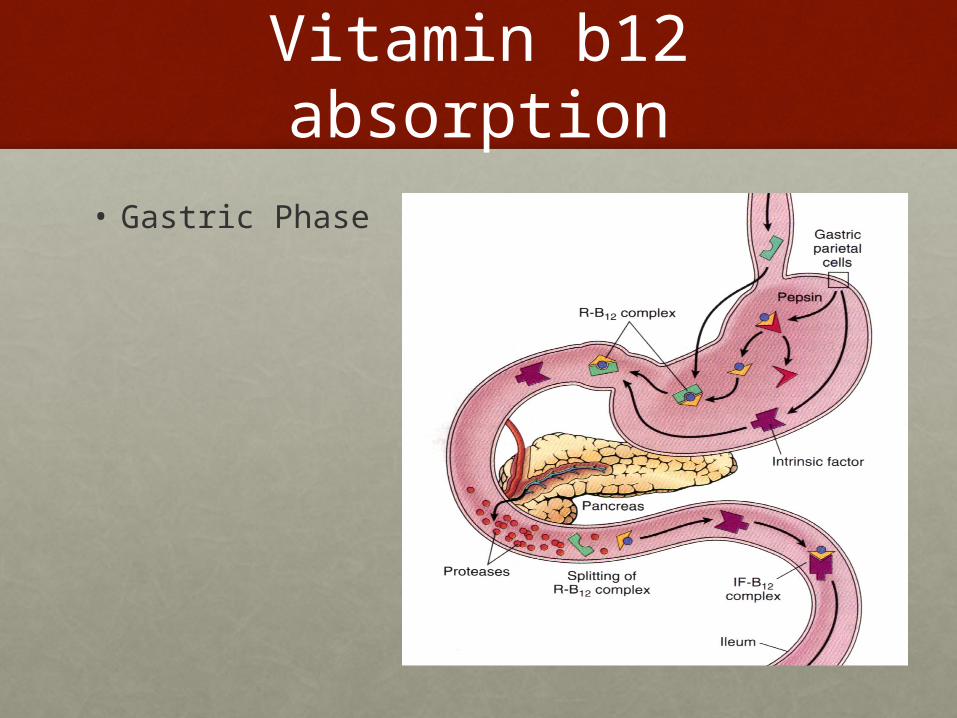
Vitamin b12 absorption
• Gastric Phase

Vitamin B12 absorption
• Intestinal Phase

Vitamin b12 deficiency
• Any interruption along this path can result in cobalamin deficiency
• Gastrectomy results in low production of IF• Terminal ileal resection (>100 cm), decreases the
site absorption of B12- IF complex
Pernicious anemia
• Most common cause of cobalamin deficiency
• Caused by the absence of IF• Atrophy of the mucosa• Autoimmune destruction of parietal cells
• Seen mostly in the elderly, average age of 60

Diagnosis of vitamin b12 deficiency
• Macrocytosis
• Peripheral blood smear
• Cobalamin levels
• Elevated serum methylmalonic acid and homocysteine levels
• Schilling Test (rarely used)

Treatment of vitamin b12 deficiency
• Replacement therapy• Parenteral treatment given weekly intramuscularly
for 8 weeks, followed by intramuscularly every month for the rest of the patients life
• Daily oral replacement therapy

Causes of megaloblastic anemia
• Folate Deficiency• Inadequate intake; unbalanced diet (common in alcoholics, teens, some
infants)• Increased requirements
• Pregnancy
• Infancy
• Malignancy
• Increased hematopoiesis (chronic hemolytic anemias)
• Chronic exfoliative skin disorders
• Hemodialysis
• Malabsorption • Sprue – Celiac Disease• Drugs; Phenytoin, barbiturates, ethanol
• Impaired metabolism• Inhibitors of dihydrofolate reductase; methotrexate, pyrimethamine,
triamterene, pentamidine, trimethoprim• Alcohol• Rare enzyme deficiencies; dihydrofolate reductase, others
Assessment
• More often malnourished than those with B12 deficiency
• Gastrointestinal manifestations • More widespread and more severe than those of
pernicious anemia• Diarrhea is often present • Cheilosis• Glossitis
• Neurologic abnormalities do not occur

Stages of folate deficiency
1. Negative folate balance (decreased serum folate)
2. Decreased RBC folate levels and hypersegmented neutrophils
3. Macroovalocytes, increased MCV, and decreased hemoglobin

Diagnosis of folate deficiency
• Peripheral blood and bone marrow biopsy look exactly like B12 deficiency
• Plasma folate <3 ng/ml- fluctuates with recent dietary intake
• RBC folate- more reliable of tissue stores <140 ng/ml
• Only increased serum homocysteine levels but NOT serum methylmalonic acid levels
Treatment of folate deficiency
• Replacement therapy
• Folate prophylaxis • Women planning pregnancy are advised to take 400g
folic acid daily before conception and until 12 weeks of pregnancy to prevent neural-tube defects (5mg/day for women with a previous affected pregnancy)
• Folate fortification of cereal grains at 1-4 mg/kg has been made mandatory in the USA as an additional method of improving the folate status of the population
• Folate is also recommended in other states of increased demand such as long-term hemodialysis and chronic hemolytic disorders
Non-effective treatment of pernicious anemia with folate
• Vitamin B12 deficiency anemia can be temporarily correct by folate supplementation
• However, this does not correct the neurologic deficits
• Folate “draws” vitamin B12 away from neurologic systems for RBC production and can exacerbate combined systems degeneration.

Current researchAnemia of Chronic Disease
CHF, Oncology, & CKD

Anemia of chronic disease (ACD)
• Most patients suffering from chronic infections, chronic inflammations, or various malignancies develop a mild to moderate anemia. This anemia, designated anemia of chronic disease, is characterized by a low serum iron level, a low to normal transferrin level, and a high to normal ferritin level. However, the anemia appears to be caused, not by these changes in iron metabolism, but, rather, by the effect of a number of suppressor cytokines. Tissues injured by infections or inflammation and neoplastic cells release cytokines, such as interleukin-1, tumor necrosis factor, and interferon gamma, known to reduce the production of erythropoietin in the kidney and impair its action in the marrow. As such, the anemia is probably caused primarily by a reduction in erythropoietin-generated red cell production. Therapeutic trials have revealed that the anemia is indeed responsive to erythropoietin, and in most cases, it can be ameliorated by the parental administration of sufficient amounts of human recombinant erythropoietin.
Erythropoietin
In addition to cleaning the blood, kidneys perform other functions. One of those functions is producing the hormone erythropoietin (EPO). Erythropoietin signals bone marrow to produce red blood cells. As renal disease progresses, the diseased kidneys cannot
produce enough erythropoietin, therefore, not as many red blood cells are made.
chf
• The Use of Subcutaneous Erythropoietin and Intravenous Iron for the Treatment of Anemia of Severe, Resistant Congestive Heart Failure Improves Cardiac and Renal Function and Functional Cardiac Class, and Markedly Reduces Hospitalizations• Journal of the American College of Cardiology • Silverberg, Donald S., Dov Wexler, Miriam Blum, Gad Keren, David Sheps,
Eyal Leibovitch, David Brosh, Shlomo Laniado, Doron Schwartz, Tatyana Yachnin, Itzhak Shapira, Dov Gavish, Ron Baruch, Bella Koifman, Carl Kaplan, Shoshana Steinbruch, and Adrian Iaina. "The Use of Subcutaneous Erythropoietin and Intravenous Iron for the Treatment of the Anemia of Severe, Resistant Congestive Heart Failure Improves Cardiac and Renal Function and Functional Cardiac Class, and Markedly Reduces Hospitalizations." Journal of the American College of Cardiology 49.7 (2008): 1737-744. Print.

CHFObjective: The study evaluated the prevalence and severity of anemia in patients with CHF and the effect of its correction on cardiac and renal function and hospitalization.
Methods: The prevalence and severity of anemia in patients with CHF was studied through a retrospective study on 142 patients from a CHF clinic. An intervention study was performed on 26 of these patients by administering subcutaneous erythropoietin and iron sufficient to increase the Hb to 12g%. The doses of CHF medications, except diuretics, were not changed during the intervention period.
Results: The prevalence of anemia in the 142 patients increased with the severity of CHF. 79% of 142 patients were found to have anemia. In the intervention study, the anemia of 26 patients was treated for a mean of 7.2 +/- 5.5 months. The mean Hb level and mean left ventricular ejection fraction increased significantly. The mean number of hospitalizations decreased 91.9% compared with a similar period before the study. The doses of oral and intravenous furosemide decreased, and the rate of fall of the glomerular filtration rate slowed with treatment.

Oncology
• Darbepoetin Alfa for the treatment of Anemia in Patients with Active Cancer not Receiving Chemotherapy or Radiotherapy• Smith, Robert E., Matti S. Appro, Heinz Ludwig,
Tomas Pinter, and Martin Smakal. "Darbepoetin Alfa for the Treatment of Anemia in Patients with Active Cancer Not Receiving Chemotherapy or Radiotherapy." Journal of Clinical Oncology 26.7 (2008): 1040-050. Web.
Oncology
Objective: Test the efficacy and safety of synthetic erythropoietin, Darbepoetin Alfa (DA) for treating patients with active cancer and anemia not receiving or planning to receive cytotoxic chemotherapy or radiotherapy.
Methods: Patients with active cancer and anemia not receiving treatment were enrolled onto a phase III, multicenter, randomized, placebo-controlled study. Patients received DA or placebo every 4 weeks for 16 weeks, with 2-year follow-up for survival.
oncology
Results: The incidence of transfusions between weeks 5 and 17 was lower in the DA group but was not statistically significant compared to placebo group. DA group was associated with an increased incidence of cardiovascular and thromboembolic events and more deaths during the initial 16-week treatment period. Long-term survival data demonstrated statistically significant poorer survival in patients treated with DA versus placebo.
Conclusion: DA was not associated with statistically significant reduction in transfusion. Shorter survival with DA. This study does not support the use of erythropoiesis-stimulating agents for this group of patients.

Chronic kidney Disease
• CKD has adverse consequences on almost all body systems. The kidney participates in erythropoiesis. Anemia is prevalent in CKD with effects on the cardiovascular system. It is mostly due to erythropoietin deficiency, inhibition of erythropoiesis by uremic solutes, and reduction of RBC life span.
• Endogenous erythropoietin dysfunction occurs when GFR falls below 20-25 ml/min.
• Treating anemia of CKD is based on correction of iron deficiency and replacement of decreased erythropoietin production by erythropoietin stimulating agents (ESA’s)
• Health related quality of life in CKD patients can be improved by treating anemia. Newly available ESA’s and newly developed epotinbiosimilars are expected to lead to improvements in the management of CKD

CKD
• Epoetin in the management of anemia associated with chronic kidney disease, differential pharmacology and clinical utility• Davis, Mary-lynn, Jun Wu, Katherine Downton,
Emile Ludman, and Virginia Noxon. "Epoetin in the Management of Anemia Associated with Chronic Kidney Disease, Differential Pharmacology and Clinical Utility." Biologics 8 (2014): 155-67. Web.

CKD
Objective: Effectiveness of ESA’s in patients with renal anemia, (Renal anemia is cauterized with a Hb level <13.0 g/dL in adult males and <12.0 g/dL in adult females) secondary to Chronic Kidney Disease.
Methods: Large scale study referencing previous studies on 165 name brands of ESA’s where the patients were being treated for renal anemia after iron dosing failed to increased Hb levels.
Results: Dosage of epoetin of 93-97 IU/kg/week to treat anemia resulted in significant stimulation of erythropoiesis and increased levels of Hb >11.5g/dL
Conclusion: Patients with symptomatic renal anemia subsequent to ESRD or CKD of at least stage 3 (est. GFR <60) whose Hb levels are <10 g/dL should be considered for epoetin therapy.
Case Study 1
• Emma an 18yo female consulted her physician for weakness, lethargy, and breathlessness. She revealed that she has been experiencing excessive bleeding with menstruation.
• RBC count 3.5
• Hb 7g/dL
• Hct 30%
• Serum Iron – low
• MCV- low
• MCHC- low
• What type of anemia does Emma most likely have? What are some physical symptoms she may have upon examination? What would your recommendation be for nutrition intervention?

Case study 2
• Marg a 65yo female reports about 2 months of tiredness, feeling faint from “getting up too fast”, and “memory problems”.
• RBC count- low
• MCV- high
• MCH- high
• MCHC- normal
What type of anemia does Marg have? Are there other tests that should be ordered? What would you recommend as a nutrition intervention?

Pes statements
• Discuss
Questions?• http://www.hematology.org
• https://www.nhlbi.nih.gov
• Hark, Lisa, and Gail Morrison. Medical Nutrition and Disease: A Case-based Approach. Chichester, UK: Wiley-Blackwell, Print.
• Nahikian-Nelms, Marcia. Nutrition Therapy and Pathophysiology. Belmont, CA: Wadsworth, Cengage Learning, 2011. Print.
• Escott-Stump, Sylvia. Nutrition and Diagnosis-related Care. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins, 2012. Print.
• Ludwig H, Van Belle S, Barrett-Lee, et al. The European Cancer Anaemia Survey (ECAS): a large, multinational, prospective survey defining the prevalence, incidence, and treatment of anaemia in cancer patients. Eur J Cancer 2004;40:2293-2306.
• Caro JJ, Salas M, Ward A, et al. Anemia as an independent prognostic factor for survival in patients with cancer: a systematic, quantitative review. Cancer 2002;94:2793-2796.
• http://content.onlinejacc.org/article.aspx?articleid=1130180
• Impacts of Recombinant Human Erythropoietin Treatment During Predialysis Periods on the Progression of Chronic Kidney Disease in a Large-Scale Cohort Study

Thank you!
• Silverberg, Donald S., Dov Wexler, Miriam Blum, Gad Keren, David Sheps, Eyal Leibovitch, David Brosh, Shlomo Laniado, Doron Schwartz, Tatyana Yachnin, Itzhak Shapira, Dov Gavish, Ron Baruch, Bella Koifman, Carl Kaplan, Shoshana Steinbruch, and Adrian Iaina. "The Use of Subcutaneous Erythropoietin and Intravenous Iron for the Treatment of the Anemia of Severe, Resistant Congestive Heart Failure Improves Cardiac and Renal Function and Functional Cardiac Class, and Markedly Reduces Hospitalizations." Journal of the American College of Cardiology 49.7 (2008): 1737-744. Print.
• Smith, Robert E., Matti S. Appro, Heinz Ludwig, Tomas Pinter, and Martin Smakal. "Darbepoetin Alfa for the Treatment of Anemia in Patients with Active Cancer Not Receiving Chemotherapy or Radiotherapy." Journal of Clinical Oncology 26.7 (2008): 1040-050. Web.
• Davis, Mary-lynn, Jun Wu, Katherine Downton, Emile Ludman, and Virginia Noxon. "Epoetin in the Management of Anemia Associated with Chronic Kidney Disease, Differential Pharmacology and Clinical Utility." Biologics 8 (2014): 155-67. Web.

















