Detecting Soft Failures in Pediatric Cochlear Implants:Relating Behavior to Language Outcomes
Aaron C. Moberly, D. Bradley Welling, and Susan Nittrouer
The Ohio State University Wexner Medical Center, Columbus, Ohio, U.S.A.
Hypothesis: Undesirable behaviors in young children with co-chlear implants suggest device soft failure.Background: Cochlear implant soft failure refers to nonoptimalperformance not detectable with routine hardware checks. Pe-diatric failures may delay language development, but failuredetection is difficult. A 2005 soft failure consensus statement re-commended a checklist for suspected device malfunctions. Thatchecklist included the appearance of ‘‘bad’’ behaviors and ag-gression (externalizing behaviors) or self-injury and inattentiveness(internalizing behaviors) as indicators of soft failure. Accordingly,these behaviors should predict slowed language growth, and theanalyses reported here sought evidence of that predictive power.Methods: Data from a longitudinal study of 80 children withcochlear implants collected at 6 times between 18 and 48 monthswere reexamined. Language measures included auditory com-prehension, expressive vocabulary, and unstructured language.A parent questionnaire, the Child Behavior Checklist, examined
externalizing and internalizing behaviors. Behavior measureswere correlated with language measures in a series of analyses.Results: Externalizing and internalizing behaviors did not con-sistently correlate with language at the ages tested. Additionally,early behaviors did not predict later language abilities. Individuallanguage measures correlated best with overall language de-velopment 12 months later.Conclusion: This study fails to support the hypothesis thatexternalizing and internalizing behaviors in pediatric cochlearimplant users correlate with slowed language advance. Thesebehaviors should not be seen as evidence of declining lan-guage performance as may be seen with device soft failure.Instead clinical assessments of language abilities are necessary.Key Words: Child behaviorVCochlear implantsVProsthesisfailure.
Otol Neurotol 34:1648Y1655, 2013.
Cochlear implant (CI) ‘‘soft’’ failure is a working di-agnosis that is supported by clinical, audiologic, and ra-diographic criteria (1,2). Typically, patients present witha deterioration in their previous implant performance, afailure to progress in language development, or new symp-toms such as facial nerve stimulation or pain with use ofthe implant. Four criteria identified in a 2005 consensusstatement on identification of CI soft failures includedthe following: 1) the exclusion of detectable hardware- orsoftware-related causes, 2) exclusion of medical problemsthat could lead to device failure, 3) radiographic evidenceof proper device and electrode array placement, and 4)improved function or symptom alleviation with device re-implantation (2).
Diagnosis of pediatric soft failure may be significantlymore challenging than that for adults, and even definingthe term soft failure in children is difficult. It has beenstated, ‘‘[Soft] device malfunction is suspected but can-not be proven. It is a working diagnosis, based on char-acteristics such as shocking sensations, popping sounds,intermittency, or unexplained progressive decrement inperformance’’ (2). Marlowe et al. (3) described 18 casesof pediatric device reimplantations for device soft failure(there termed suspected failures), which was defined as‘‘diminished or stagnant speech perception.’’ Many youngchildren are not able to verbalize their experience of newsymptoms or a deterioration in speech perception. More-over, the rate of language development is variable amongpediatric CI users, so it may not be apparent if a child isstraying from his or her previous trajectory of languagedevelopment. Device failures may be missed in childrenunless an observant caregiver or teacher detects a declinein language abilities or poorer-than-expected progress.Sensitive clinical tools are not readily available to identifythese children, so the identification of device soft failurecontinues to equate with poor language development ora decline in language performance.
Address correspondence and reprint requests to Aaron C. Moberly,M.D., OtolaryngologyYHead & Neck Surgery, The Ohio State Univer-sity, 915 Olentangy River Road, Suite 4000, Columbus, OH 43212;E-mail: [email protected] work was supported by Grant No. R01 DC006237 (to S. N.)
from the National Institute on Deafness and Other CommunicationDisorders, the National Institutes of Health.The authors disclose no conflicts of interest.
Otology & Neurotology34:1648Y1655 � 2013, Otology & Neurotology, Inc.
Several authors have reported their institutions’ inci-dence of soft failure (sometimes referred to as suspecteddevice failure) in pediatric CI users. Marlowe et al. (4)reported a revision pediatric cochlear implantation rate of12.9% in 482 CI surgeries, 29% of which were performedfor suspected device failure. In another large series ofpediatric implants, Brown et al. (5) reported a 7.3% im-plant revision rate with 23% performed for soft failure.Cullen et al. (6) reported a 11.2% revision rate in 952pediatric CI users, with a 15% soft failure rate. In eachseries, soft failure was diagnosed by identification of aver-sive symptoms, a decrement in language performance, ora failure to progress appropriately in language develop-ment. Considering the difficulty posed by trying to identifylanguage decrement or failure to progress in pediatric pa-tients, it is conceivable that actual soft failure rates may beeven higher than those reported.
A suggested Soft Failure Assessment Checklist wasdeveloped by the 2005 consensus panel consisting ofleaders in the implant field to assist clinicians in recog-nizing device soft failures (Appendix A) (2). Included inthis checklist were a number of behavioral factors thatwere thought to be useful in identifying at-risk individuals:an increase in ‘‘bad’’ behaviors or aggressiveness (‘‘ex-ternalizing’’ behaviors), unwillingness to wear the device,head hitting, or inattentiveness (‘‘internalizing’’ behav-iors). It is reasonable to believe that these behaviorscould serve as ‘‘red flags’’ for device malfunction. Un-fortunately, there is little data to date to support therelationships between these behaviors and language de-velopment or device failure.
The purpose of this study was to evaluate whether thepresence of externalizing or internalizing behaviors suchas those listed above can be used as a warning sign ofpoor language development and should rouse suspicionof a device soft failure. Identification of these behaviorsin a child with a CI would be a much simpler task forcaregivers, teachers, and clinicians than identifying a gen-eral language decline or failure to progress in languagedevelopment. The reported evaluation was accomplishedby reanalysis of a subset of previously published data (7)to gauge the strength of relationship between suspect be-haviors and language skill.
MATERIALS AND METHODS
ParticipantsParticipants were 80 children with cochlear implants who
were part of an ongoing longitudinal study (7), and a full reportof demographic factors can be found there. Table 1 presents groupmeans (and SDs) for selected demographic measures. All chil-dren in the study had profound sensorineural hearing loss. Allwere identified before 2 years of age and most before 1 year.Children received their CIs early, which for most meant at orbefore 2 years of age. Consequently, these children had con-siderable experience with their CIs. Forty-two of the childrenwore CIs bilaterally by the age of 48 months. Sixty-one percentof the children wore devices by Cochlear Corporation, 35%wore devices by Advanced Bionics, and 4% wore devices by
Med-El. To be in the study, children were required to have beenfull-term newborns and have no medical problems other thanhearing loss that could be expected to delay language acquisi-tion. English was the only language spoken in the home, andparents were required to have normal hearing. Socioeconomicstatus was indexed using a 2-factor scale on which both thehighest educational level and the occupational status of theprimary income earner in the home is considered (8). Thesescores suggest that all children came from middle-class families,so had reasonably rich language environments in the home. Allchildren had received intervention starting shortly after theirhearing loss was identified at least once per week until the age of36 months and then attended preschool programs designed forchildren with hearing loss for at least 16 hours per week afterage 36 months. These programs emphasized spoken language.Data collected from these children between 18 and 48 monthsare reported.
EquipmentEach test session was video and audio recorded using a Sony
DCR-TRV19 video recorder. Sessions were recorded, so scor-ing could be done at a later time. Children wore Sony FM trans-mitters in specially designed vests that transmitted speech signalsto the receivers, which provided direct line input to the harddrives of the cameras. This procedure ensured good soundquality for all recordings. All children were tested wearing theircustomary auditory prostheses (unilateral CI, bilateral CI, or uni-lateral CI with contralateral hearing aid), which were checked atthe start of testing.
General ProceduresTesting took place at multiple sites across the United States as
described by Nittrouer (7), with all examiners having undergonetwo 2-day training sessions prior to testing. Measures collectedduring those sessions and used in this report are described here.They include children’s auditory comprehension, expressivevocabulary, and unstructured language.
Task-Specific ProceduresMultiple measures of language, including auditory compre-
hension, vocabulary, and children’s use of unstructured lan-guage, were collected and were correlated with measures ofinternalizing and externalizing behaviors. Task-specific pro-cedures will be described in brief in this report. See Nittrouer (7)for a more complete description of each task.
Auditory ComprehensionThe Auditory Comprehension subscale of the Preschool
Language Scales-4 (PLS-4) was used to measure this ability (9).This test is a standardized assessment tool generally used forchildren between birth and 7 years of age. Most items requirethe child to demonstrate spoken language comprehension byperforming specific commands provided by the examiner. Items
TABLE 1. Mean values for demographic measures
n Mean (SD)
Age of identification (mo) 80 6.13 (7.13)Age of first amplification (mo) 80 7.80 (6.96)Age of first implant (mo) 80 17.09 (6.85)Age of second implant (mo) 42 35.14 (10.75)Better-ear pure tone average 80 103.76 (13.83)
on this test are organized hierarchically, as older children wouldbe expected to understand more complex linguistic structure thanyounger children. The Auditory Comprehension subscale hasexcellent reliability to evaluate specific components of com-prehension, including lexical, syntactic, and grammatical ele-ments. Standard scores were used in analyses.
Expressive VocabularyTwo measures of expressive vocabulary were used for this
study. For children between the ages of 18 and 30 months, theLanguage Development Survey (LDS) was used (10). The LDShas been shown to correlate well with direct measures of ex-pressive vocabulary. This test consists of 310 words, and parentsfilled out a survey by circling the words that their childrensay spontaneously and with consistent pronunciation. Numberof words spoken was used in analysis.For children between 36 and 48 months of age, the Expressive
One-Word Picture Vocabulary Test (EOWPVT) was admin-istered (11). For this test, the child is shown a picture and isasked to name the picture with the appropriate vocabulary word.Standard scores were used in analyses.
Unstructured LanguageAt every test age, a 20-minute language sample was obtained
and scored to provide a comprehensive measure of children’sproductive language abilities. Four measures that were made toindex the form and function of children’s early communicationare reported here. First, the number of real-word utterances wascalculated as the number of utterances consisting of real wordsin the entire 20-minute language sample. Second, the numberof answers children produced in 20 minutes was obtained as ametric of how responsive children were in a meaningful way.Third, the total number of vocalizations produced during this20-minute sample was calculated. Finally, the total number ofimitations was calculated during the same sample.Twomeasures of productive syntax obtained from the 20-minute
language sample are also reported. Systematic Analysis of Lan-guage Transcripts, Version 9 (SALT) was used to obtain thesemetrics (12). First, mean length of utterance (MLU) was used,defined as the mean number of morphemes per utterance. Thenumber of pronouns used correctly in those 50 utterances is theother measure reported.
Latent Language MeasureTo more comprehensively evaluate language development, a
composite measure of language was developed (7). This com-posite measure, referred to as a latent language measure, allowedthe characterization of developmental trajectories of individualchildren. Details on calculating a composite language score usinglatent growth modeling are found in Nittrouer (7). In brief, anestimate of the effects of multiple predictor variables on a de-pendent language measure can be made. Eight measures wereused in the construction of the latent language measure: auditorycomprehension, expressive vocabulary, real-word utterances,answers, imitations, number of vocalizations, mean length of ut-terance, and the Leiter International Performance ScaleYRevised(LIPS-R) classification score, which is a measure of cognitivedevelopment (13).
Internalizing and Externalizing BehaviorsTo evaluate internalizing and externalizing behaviors, the
Child Behavior Checklist (CBCL) (14) was used. The CBCL isappropriate for children between 18 months and 5 years of ageand examines 100 separate behaviors. It is a questionnaire that
is completed by parents, who respond to each item by circlinga number from 0 to 2, indicating whether ascribing the behaviorto their child would be not true (0), somewhat or sometimestrue (1), or very true or often true (2). A weighted sum of responsesis obtained, with results loaded on seven clusters: EmotionallyReactive (I), Anxious/Depressed (II), Somatic Complaints (III),Withdrawn (IV), Sleep Problems (V), Attention Problems (VI),and Aggressive Behavior (VII). The sum of scores on clusters Ithrough IV serves as a general ‘‘internalizing index,’’ and thesum on clusters VI and VII serves as a general ‘‘externalizingindex.’’ Raw scores were used in statistical analyses. Clinicalsignificance on this measure is suspected when a raw scoreexceeds 18 for internalizing behaviors and 24 for externalizingbehaviors.
Correlational AnalysesTo examine the relationship of behaviors and language devel-
opment, several series of correlation analyses were performed. Ineach analysis, Pearson product-moment (i.e., zero-order) cor-relation coefficients were computed between each behavioralvariable (internalizing index and externalizing index) and eachlanguage measure (auditory comprehension, vocabulary, un-structured language measures, and latent language measure).
RESULTS
The reported analyses examine the language and be-havior measures of a group of pediatric CI users. For anin-depth analysis of the language outcomes of these pa-tients as compared with children with normal hearing orhearing aids, the reader is encouraged to review the re-sults of the ongoing longitudinal study (7). In brief, nosignificant differences were found between the internal-izing or externalizing behavior index among the groupsfor CI users, hearing aid users, or children with normalhearing. On the other hand, CI users on the whole per-formed approximately one standard deviation below themean for normal-hearing children on all language mea-sures, including the latent language measure. For a senseof the range of scores for the CI users, mean scores (andstandard deviations) at 48 months were the following:internalizing behavior index, 6.2 (SD, 5.5); externalizingbehavior index, 9.3 (SD, 7.4); and latent language mea-sure, 7.5 (SD, 1.9).
Correlating Behaviors With LanguageThe first analysis was performed to examine how well
internalizing and externalizing behaviors correlated withlanguage development at that same age. In other words,would the presence of internalizing and externalizingbehaviors serve as a red flag that language was not de-veloping appropriately? Figures 1 and 2 display zero-order correlation coefficients between each behaviorindex, internalizing or externalizing, respectively, and thelanguage measures at each age. By taking the square ofthe correlation coefficients, it is possible to index theamount of variance in language development that can beexplained by each behavioral index. The dotted linesshow the points above and below which more than 10%of the language measure is explained by the behavioral
index measure, with 10% generally accepted as the amountof variance that is sufficient to be of interest. Below 10%,the behavioral index measure is unlikely to be worthwhilein explaining variance in language development. Exam-ination of these coefficients reveals that neither internal-izing nor externalizing behaviors consistently explainedgreater than 10% of the variance in the language mea-sures, including the latent language measure.
Behaviors as Predictors of LaterLanguage Development
The second analysis was performed to examine howwell internalizing and externalizing behaviors at 36 monthscould predict language development at 48 months. Thisanalysis examined whether the earlier presence of inter-nalizing and externalizing behaviors might suggest animpending problem with language development, which
FIG. 2. Zero-order correlation coefficients between externalizing behavior index and language measures at each age. The dotted linesshow the points above and below which more than 10% of the variance in the language measure is explained by the behavioral indexmeasure. LDS: Language Development Survey; EOWPVT: Expressive One-Word Picture Vocabulary Test.
FIG. 1. Zero-order correlation coefficients between internalizing behavior index and language measures at each age. The dotted linesshow the points above and below which more than 10% of the variance in the language measure is explained by the behavioral indexmeasure. LDS: Language Development Survey; EOWPVT: Expressive One-Word Picture Vocabulary Test.
would become evident at a later age. The older ages werechosen because they would best represent ages of morecomplex language and behavior. Mean length of utter-ance (MLU) was chosen as representative of unstructuredlanguage for this analysis because it is the most commonlyevaluated measure of syntactic development. Figure 3shows zero-order correlation coefficients calculated be-tween each behavior index (internalizing or externalizing)at age 36 months and the variable of the latent languagemeasure at age 48 months. No significant correlationswere found (internalizing index r = 0.040, p = 0.83; ex-ternalizing index r = j0.132, p = 0.48). Similar corre-lation coefficients were calculated between each behaviorindex at 36 months and each separate language measure(auditory comprehension, expressive vocabulary, andmeanlength of utterance) at 48 months, and no correlationswere significant.
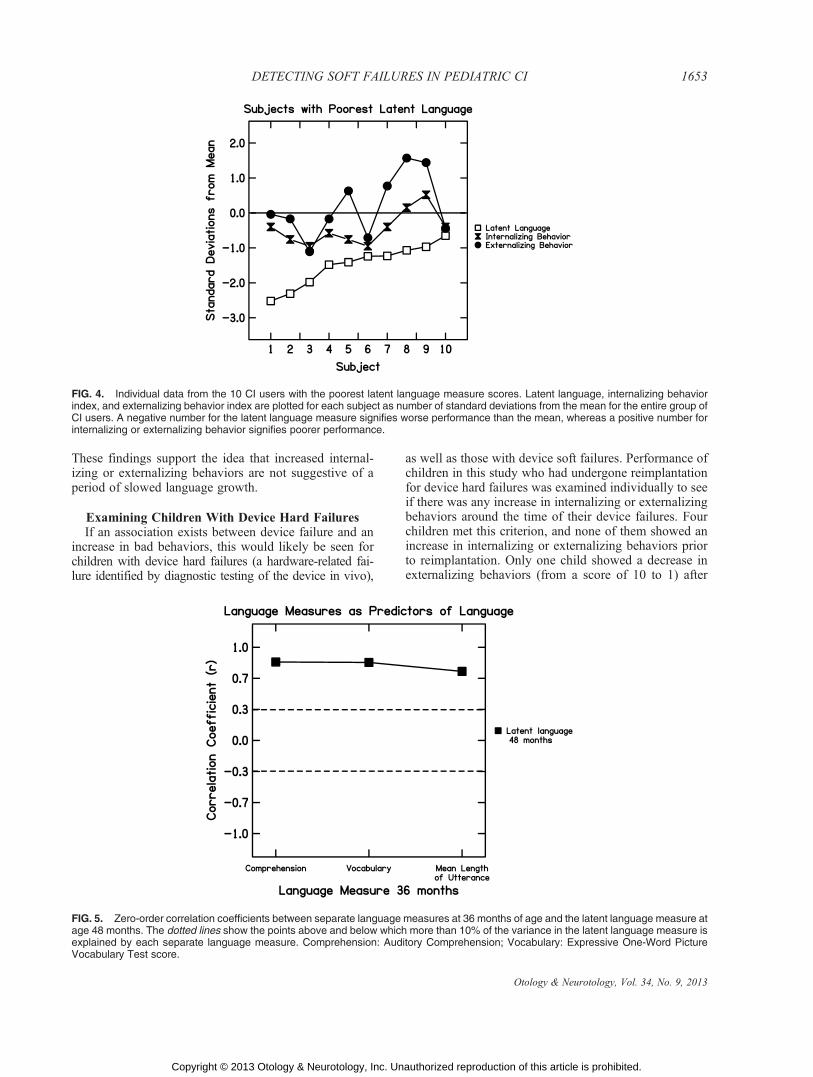
Examining the Poorest Language PerformersThe above findings suggested there was no significant
relationship between the presence of internalizing or exter-nalizing behaviors and poor language skills in the groupof children with CIs as a whole. However, it was possiblethat the individual children with the poorest languageskills would still show a larger number of these behaviors.Therefore, the 10 children with the poorest latent lan-guage measure value at 48 months (all worse than onestandard deviation below the mean for the group) wereexamined independently. As seen in Figure 4, wide var-iability in internalizing and externalizing behaviors was
seen for these children with the poorest language skills.These findings suggest that even for the children withthe poorest language skills, behavior scores varied greatly.In addition, none of these children had behavior indicesreaching clinical significance for either internalizing orexternalizing behaviors.
Examining Children With SlowedLanguage Development
In addition to failure to progress appropriately in lan-guage development, device soft failure has been definedas deterioration of previous performance. Therefore, thedevelopmental trajectory of each child was examined toidentify children who showed deterioration in perfor-mance over time and to determine whether they showedan increase in internalizing or externalizing behaviorsaround the time of language deterioration. Individual la-tent language measure data were examined across agesfor each child. No child showed a decline in latent lan-guage measure over time.
Next, individuals were identified who showed a slowedrate of growth in latent language measure score. For thegroup as a whole, the average increase in latent languagemeasure score over each 6-month period was approxi-mately 1.0. A ‘‘slowed’’ language growth rate was de-fined as an increase in latent language measure score ofless than 0.5 over at least one 6-month period. Eightchildren met this criterion. Among these children, no con-sistent increase in internalizing or externalizing behaviorswas seen around the period of their slowed language growth.
FIG. 3. Zero-order correlation coefficients between internalizing and externalizing behavior indices at age 36 months and languagemeasures at age 48 months. The dotted lines show the points above and below which more than 10% of the variance in the languagemeasure is explained by the behavioral index measure. Comprehension: Auditory Comprehension; Vocabulary: Expressive One-WordPicture Vocabulary Test score.
These findings support the idea that increased internal-izing or externalizing behaviors are not suggestive of aperiod of slowed language growth.
Examining Children With Device Hard FailuresIf an association exists between device failure and an
increase in bad behaviors, this would likely be seen forchildren with device hard failures (a hardware-related fai-lure identified by diagnostic testing of the device in vivo),
as well as those with device soft failures. Performance ofchildren in this study who had undergone reimplantationfor device hard failures was examined individually to seeif there was any increase in internalizing or externalizingbehaviors around the time of their device failures. Fourchildren met this criterion, and none of them showed anincrease in internalizing or externalizing behaviors priorto reimplantation. Only one child showed a decrease inexternalizing behaviors (from a score of 10 to 1) after
FIG. 4. Individual data from the 10 CI users with the poorest latent language measure scores. Latent language, internalizing behaviorindex, and externalizing behavior index are plotted for each subject as number of standard deviations from the mean for the entire group ofCI users. A negative number for the latent language measure signifies worse performance than the mean, whereas a positive number forinternalizing or externalizing behavior signifies poorer performance.
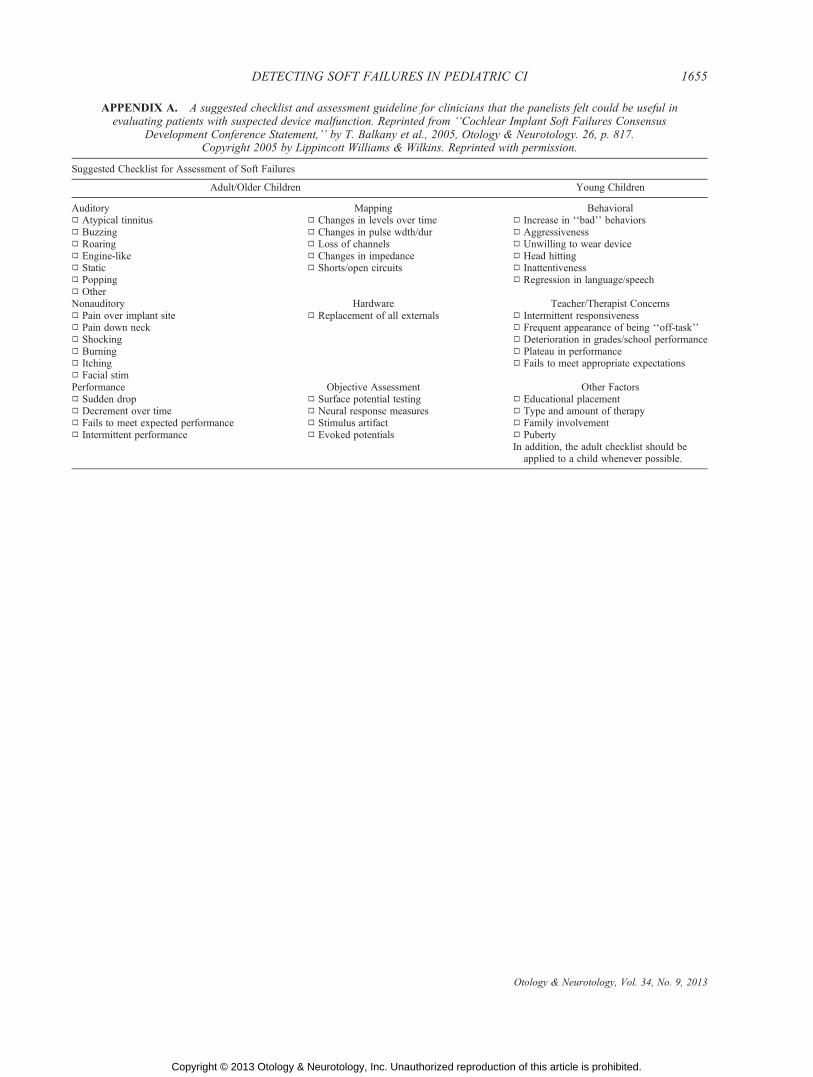
FIG. 5. Zero-order correlation coefficients between separate language measures at 36 months of age and the latent language measure atage 48 months. The dotted lines show the points above and below which more than 10% of the variance in the latent language measure isexplained by each separate language measure. Comprehension: Auditory Comprehension; Vocabulary: Expressive One-Word PictureVocabulary Test score.
reimplantation. Although not conclusive based on thesmall number of subjects included, these findings implythat hard device failure is not associated with an increasein internalizing or externalizing behaviors.
Separate Language Measures as Predictors of LaterLanguage Development
Because internalizing and externalizing behaviors at36 months did not significantly predict language develop-ment at 48 months, a final analysis was performed to exa-minewhich separate early languagemeasures at 36monthsserved as the strongest predictors of language develop-ment at age 48 months. Figure 5 shows zero-order cor-relation coefficients calculated between each languagemeasure at 36 months and the dependent variable of thelatent language measure at 48 months. Each independentlanguage measure at age 36 months was a strong predictorof the latent language score at 48 months. Each languagemeasure predicted about 50% or greater of the variance inlatent language score, found by taking the square of thecorrelation coefficient, with auditory comprehension andvocabulary being the strongest predictors.
DISCUSSION
In children, a diagnosis of CI soft failure is difficult tomake but is often considered when a child shows de-clining language performance or a failure to make satis-factory gains in language skills. It has been suggested thatthe presence of ‘‘bad’’ behaviors in young children shouldalert the clinician of a possible soft failure, as describedin the soft failures consensus statement (2). The purposeof the reanalysis reported here was to see if there was anyevidence to support this relationship of ‘‘bad’’ behaviorswith poor implant performance suggestive of device fai-lure in a group of children between the ages of 18 and48 months. The results revealed that internalizing andexternalizing behaviors were neither good at explainingvariance in language outcomes at each age nor good atpredicting later language outcomes. The children with aperiod of slowed language growth did not have associa-ted increases in internalizing or externalizing behaviors.Device hard failures were also not associated with anincrease in bad behaviors, although only a few patientswith hard failures were presented in this series. The find-ings of this study suggest that assessment of internaliz-ing and externalizing behaviors in pediatric CI users isnot a sensitive tool for identifying children who are at riskfor a possible device soft failure. On the other hand, se-parate language measures, such as auditory comprehen-sion, vocabulary, and unstructured language measures,were found to strongly predict the overall language de-velopment a year later. These findings reinforce the con-clusions of previous work, showing that to best predictthe language skills of children with CIs, individual mea-sures of language are essential (15,16). Because language
performance is likely one of the strongest indicators of de-vice integrity in the pediatric population, language de-velopment should be thoroughly and carefully monitored.
As intuitive as it seems, the findings of this study sug-gest that to identify a failure to progress in language de-velopment by children with cochlear implants, such asmay be seen with a device soft failure, clinicians need tofocus on directly evaluating aspects of language devel-opment. Tests of auditory comprehension, vocabulary,and language production should be developed for use byclinicians to better assess overall language developmentof children with implants and to identify those who arefailing to progress appropriately.
Acknowledgment: The authors acknowledge AmandaCaldwell-Tarr, Ph.D., for assistance in data analysis and man-uscript editing.
REFERENCES
1. Chung D, Kim AH, Parisier S, et al. Revision cochlear implantsurgery in patients with suspected soft failures. Otol Neurotol 2010;31:1194Y8.
2. Balkany TJ, Hodges AV, Buchman CA, et al. Cochlear implant softfailures consensus development conference statement. Otol Neurotol2005;26:815Y8.
3. Peterson NR, Pisoni DB, Miyamoto RT. Cochlear implants andspoken language processing abilities: review and assessment of theliterature. Restor Neurol Neurosci 2010;28:237Y50.
4. Marlowe AL, Chinnici JE, Rivas A, et al. Revision cochlear implantsurgery in children: the Johns Hopkins experience. Otol Neurotol2009;31:74Y82.
5. Brown KD, Connell SS, Balkany TJ, et al. Incidence and indica-tions for revision cochlear implant surgery in adults and children.Laryngoscope 2009;119:152Y7.
6. Cullen RD, Fayad JN, Luxford WM, et al. Revision cochlear im-plant surgery in children. Otol Neurotol 2008;29:214Y20.
7. Nittrouer S. Early Development of Children with Hearing Loss.San Diego, CA: Plural Publishing, 2010.
8. Nittrouer S, Burton LT. The role of early language experience inthe development of speech perception and phonological processingabilities: evidence from 5-year-olds with histories of otitis mediawith effusion and low socioeconomic status. J Commun Disord2005;38:29Y63.
9. Zimmerman IL, Steiner VG, Pond RE. Preschool Language Scale,4th ed. San Antonio, TX: The Psychological Corporation, 2002.
10. Achenbach TM, Rescorla LA. Manual for the ASEBA PreschoolForms and Profiles. Burlington, VT: University of Vermont, Re-search Center for Children, Youth, & Families, 2000.
12. Miller J, Chapman R. Systematic Analysis of Language Transcripts(SALT): Version 9. Madison, WI: University of Wisconsin-Madison, Language Analysis Laboratory, 2006.
13. Roid GH, Miller LJ. Leiter International Performance Scale-Revised (LIPS-R). Wood Dale, IL: Stoelting, 2002.
14. Achenbach TM, Rescorla LA. Manual for the ASEBA preschoolforms and profiles. Burlington, VT: University of Vermont, Re-search Center for Children, Youth, & Families, 2000.
15. Nittrouer S, Caldwell A, Holloman C. Measuring what matters:effectively predicting language and literacy in children with cochlearimplants. Int J Ped Otorhinolaryngol 2012;76:1148Y58.
16. Nittrouer S, Chapman C. The effects of bilateral electric and bimodalelectric-acoustic stimulation on language development. Trends InAmplif 2009;13:190Y205.
APPENDIX A. A suggested checklist and assessment guideline for clinicians that the panelists felt could be useful inevaluating patients with suspected device malfunction. Reprinted from ‘‘Cochlear Implant Soft Failures Consensus
Development Conference Statement,’’ by T. Balkany et al., 2005, Otology & Neurotology. 26, p. 817.Copyright 2005 by Lippincott Williams & Wilkins. Reprinted with permission.
Suggested Checklist for Assessment of Soft Failures
Adult/Older Children Young Children
Auditory Mapping BehavioralÌ Atypical tinnitus Ì Changes in levels over time Ì Increase in ‘‘bad’’ behaviorsÌ Buzzing Ì Changes in pulse wdth/dur Ì AggressivenessÌ Roaring Ì Loss of channels Ì Unwilling to wear deviceÌ Engine-like Ì Changes in impedance Ì Head hittingÌ Static Ì Shorts/open circuits Ì InattentivenessÌ Popping Ì Regression in language/speechÌ OtherNonauditory Hardware Teacher/Therapist ConcernsÌ Pain over implant site Ì Replacement of all externals Ì Intermittent responsivenessÌ Pain down neck Ì Frequent appearance of being ‘‘off-task’’Ì Shocking Ì Deterioration in grades/school performanceÌ Burning Ì Plateau in performanceÌ Itching Ì Fails to meet appropriate expectationsÌ Facial stimPerformance Objective Assessment Other FactorsÌ Sudden drop Ì Surface potential testing Ì Educational placementÌ Decrement over time Ì Neural response measures Ì Type and amount of therapyÌ Fails to meet expected performance Ì Stimulus artifact Ì Family involvementÌ Intermittent performance Ì Evoked potentials Ì Puberty
In addition, the adult checklist should beapplied to a child whenever possible.