35
Models for stewardship in Hospital - UK Models Philip Howard Consultant Antimicrobial Pharmacist [email protected] Twitter: @AntibioticLeeds
| Date post: | 24-Apr-2018 |
| Category: |
Documents |
| Upload: | truongkiet |
| View: | 217 times |
| Download: | 2 times |
Models for stewardship in Hospital - UK Models
Philip Howard
Consultant Antimicrobial Pharmacist
Twitter: @AntibioticLeeds

United Kingdom of England, Scotland, Wales & Northern Ireland
One Kingdom
but four
variations of a
National Health
Service
5.3m
3.1m
1.8m
53m
Early UK AMR & AMS activities • 1994: BSAC Survey of Hospital antibiotic control measures
• 1998: Standing Medical Advisory Committee (SMAC) report on Antimicrobial Resistance
• 2000: Dept Health AMR Strategy & Action Plan
• 2001: WHO Global Strategy for Containment of Antimicrobial Resistance
• 2001: Standing Advisory Committee on Antimicrobial Resistance (SACAR) established
• 2003: Hospital Pharmacy Initiative (£12m over 3 years for AMS)
• 2008: Health & Social Care Act: HCAI (C.difficile and MRSA)
• 2011: DH Antimicrobial Stewardship Guidelines – Start Smart then Focus
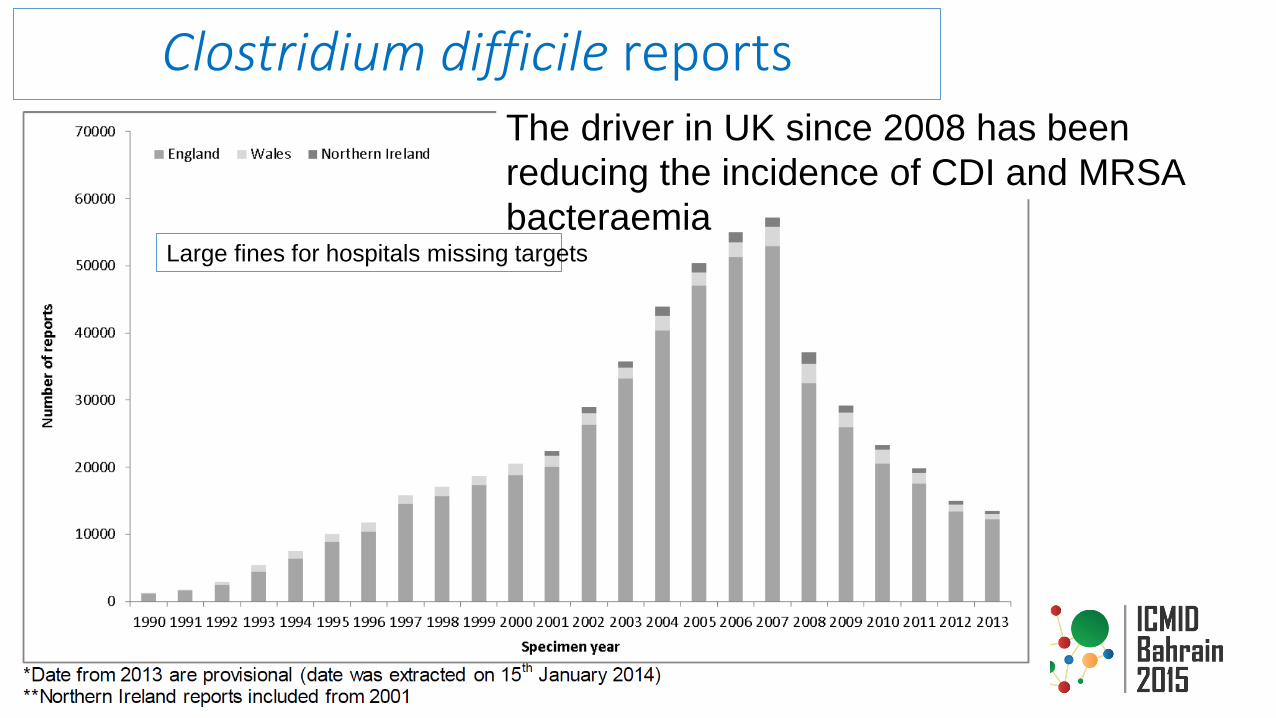
The driver in UK since 2008 has been
reducing the incidence of CDI and MRSA
bacteraemia
Clostridium difficile reports
Large fines for hospitals missing targets

Scottish Antimicrobial Prescribing Group
• Funded as a multidisciplinary national forum in March 2008 by Scottish Government as part of The Scottish Management of Antimicrobial Resistance Action Plan 2008.
• SAPG co-ordinates & delivers a national AMS framework: • antibiotic consumption and prescribing guidance
• resistance surveillance
• organisational accountability for antimicrobial stewardship
• antimicrobial prescribing education for healthcare professionals and infection management
• Highly successful model with representation from all 13 Health Boards
www.scottishmedicines.org.uk/SAPG/Scottish_Antimicrobial_Prescribing_Group__SAPG_
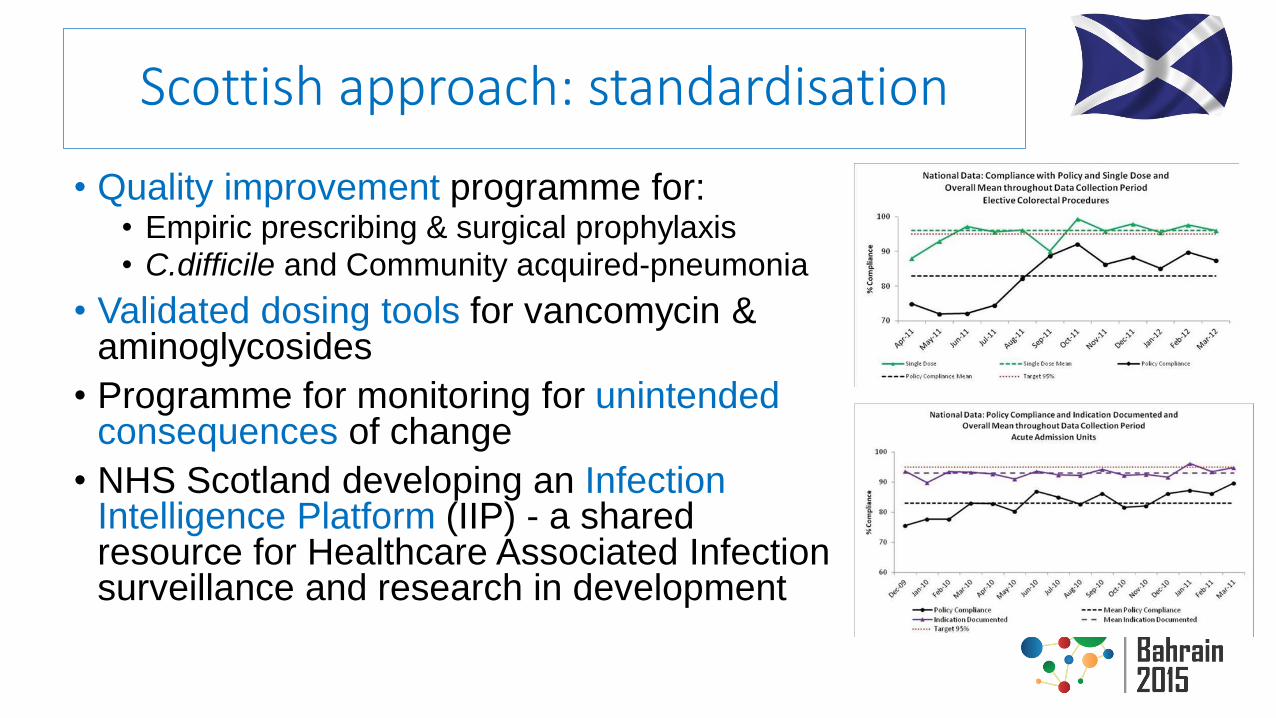
Scottish approach: standardisation
• Quality improvement programme for: • Empiric prescribing & surgical prophylaxis
• C.difficile and Community acquired-pneumonia
• Validated dosing tools for vancomycin & aminoglycosides
• Programme for monitoring for unintended consequences of change
• NHS Scotland developing an Infection Intelligence Platform (IIP) - a shared resource for Healthcare Associated Infection surveillance and research in development
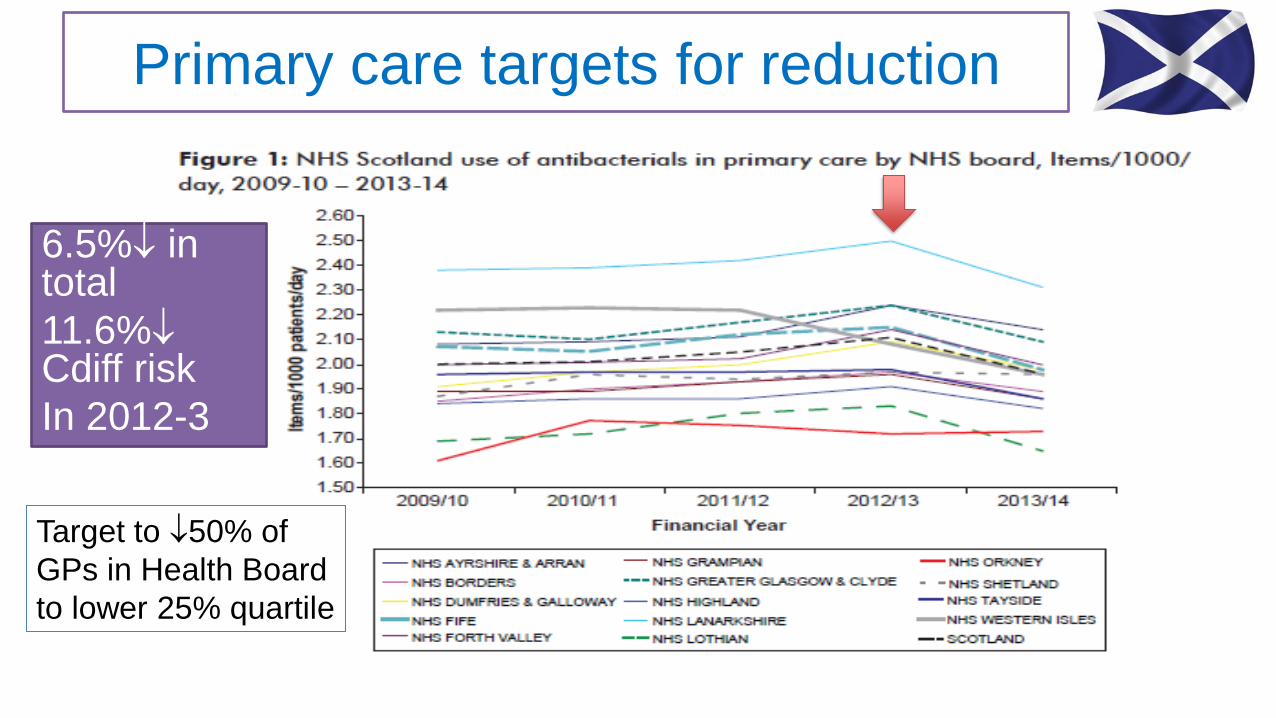
Primary care targets for reduction
6.5% in total
11.6% Cdiff risk
In 2012-3
Target to 50% of
GPs in Health Board
to lower 25% quartile

High-risk Clostridium difficile antibiotics reduction
• Driving down the use of broad-spectrum antibiotics in hospitals & community
• Much better performance than England or Wales

NHS Wales – centralised antimicrobial usage and resistance data provided to all hospitals
• Follow English AMS guidance
• Amoxicillin-clavulanate (COA) resistance & E.coli resistance identified as major issue as cefalosporin & quinolone use
NHS England (pre 2013): national AMS guidance but no antimicrobials usage or resistance data in hospitals
• Informal regional networks of: • Medical microbiologists and infectious diseases
• Antimicrobial pharmacists in hospitals
• National AMS guidelines (Nov-2011) for hospitals: “Start Smart then Focus” and community: TARGET.
• No AMR information or usage data available at national level in hospitals, but available in community
• Local information only for hospitals
• HCAI performance based around C.difficile and MRSA bacteraemia reduction
• ASAT (AMS for Acute Trusts) tool to measure performance
• Commissioners / external assurance agencies (CQC/TDA/Monitor) could request to see AMS programme and results.
2013: UK 5 year AMR Strategy
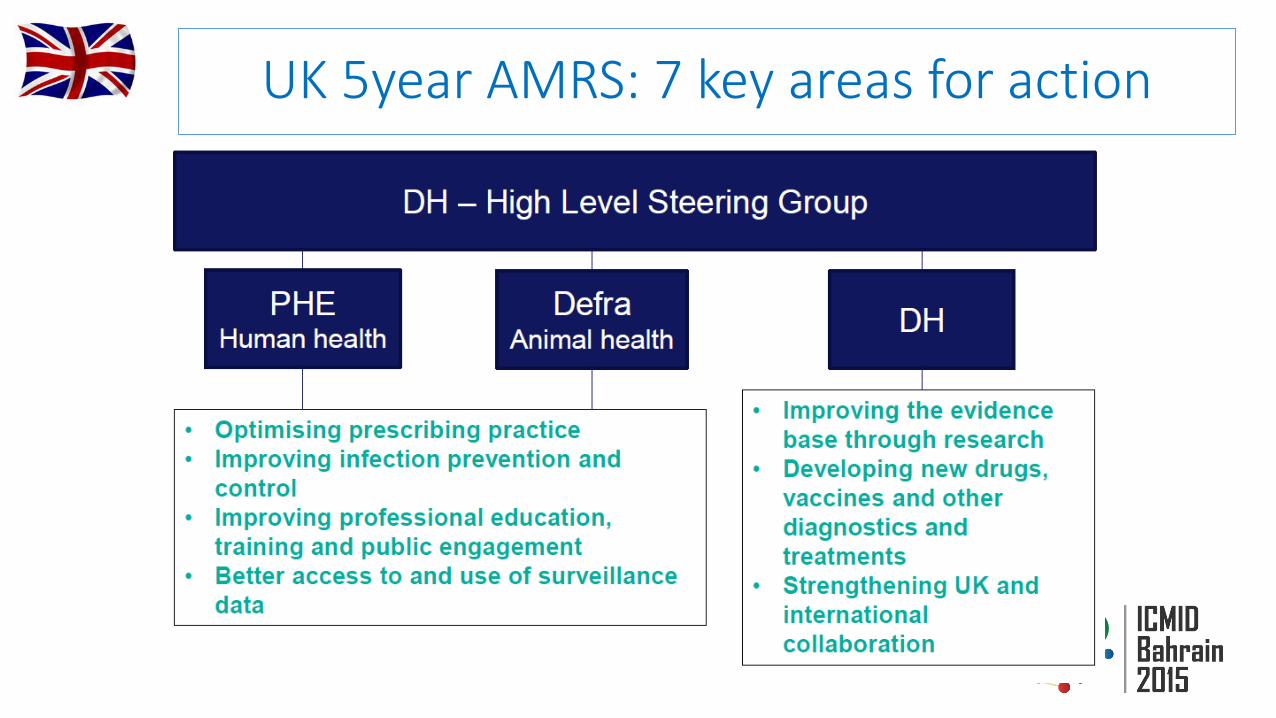
UK 5year AMRS: 7 key areas for action
UK 5 year AMR strategy
• 2013-14: detailed implementation plan developing outcome metrics & establishing surveillance systems
• 2014-15: ESPAUR to report AMR and antimicrobial usage
• 2015-16: Enough information to assess whether strategy on-course to achieve goals by 2018
• Government holding NHS to account to deliver on strategy
• Devolved countries to lead on own implementation

Progress in year 1 of 5 year AMR strategy
English Surveillance Plan for Antimicrobial Usage and Resistance (ESPAUR 2014 report)
• Programme set up to monitor antimicrobial use and resistance • First time reporting for national and regional surveillance of AMR and usage data in
hospitals and community. Report on AMS activity in hospitals
• Prescribing Quality Measures to reduce antibiotic usage to 2010 levels
• Unified message for European Antibiotics Awareness Day in human & animal health. “Antibiotic Guardian” campaign.
• Establishment of 2 NIHR Health Protection Research Units for AMR & HCAI (Imperial & Oxford). Themed NIHR AMR research call.
• Looked at factors in influencing prescribing in Vets
• International collaboration: Lead on WHO AMR resolution. Enrofloxacin-colistin withdrawn in animals.
• New drug discovery & diagnostics. PM commissioned a review by Jim O’Neill (Economist)

Undergraduate AMS teaching (Imperial 2014)
1.Infection prevention and control
2.Antimicrobial resistance and antimicrobials
3.Prescribing antimicrobials
4.Antimicrobial stewardship
5.Monitoring and learning
Antimicrobial Prescribing
and Stewardship
Competencies
Health Education England: New mandatory framework for
education and training on AMR & AMS in 2015-6 for all
healthcare staff at undergraduate and post-registration levels

ESPAUR 2104 England still has less AMR than Europe
English Surveillance Programme for
Antimicrobial Utilisation & Resistance

6% in consumption between 2010-13
1.4% last year
GPs: 78% of total with 4.1% growth in 2010-3 but 3.5% last
year
Hospitals: 9.1% IP and 6.2% OP, but 11.9% over 3 years
for IP
Significant regional variation in antibiotic use
Changes in antibiotic use: 2010 – 2013 • Pressure to reduce cefalosporins and quinolones to C.difficile
• 48% overall in cefalosporins (GPs 55% and Hospitals 10%)
• 5% in quinolones (GPs 6%, Hospital IP 10%, Hospital OP 5%)
• Big increases in tetracyclines, pencillins & nitrofurantoin
• Amoxicillin-clavulanate 13% (mainly in hospital), piperacillin-tazobactam by 46%
• 31% in carbapenems
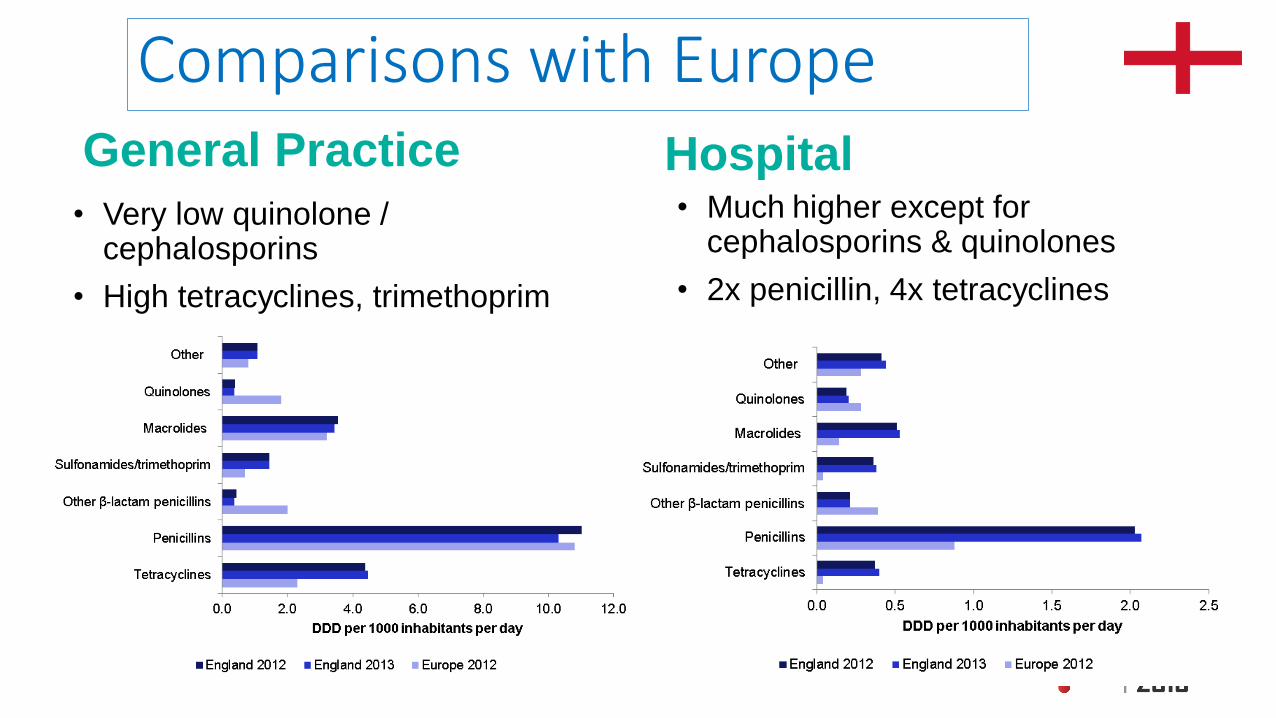
Comparisons with Europe
• Very low quinolone / cephalosporins
• High tetracyclines, trimethoprim
• Much higher except for cephalosporins & quinolones
• 2x penicillin, 4x tetracyclines
General Practice Hospital

ESPAUR 2014: 1st total sector data. We’re not
as good as we thought!
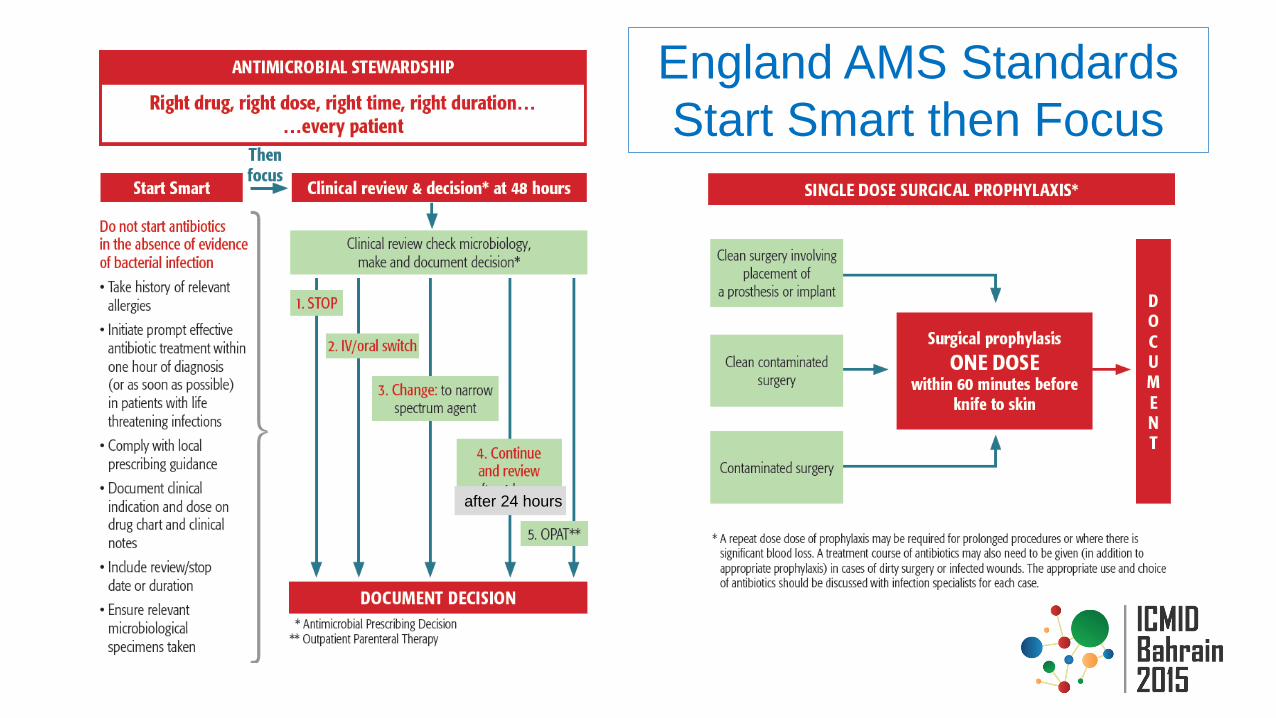
England AMS Standards
Start Smart then Focus
after 24 hours
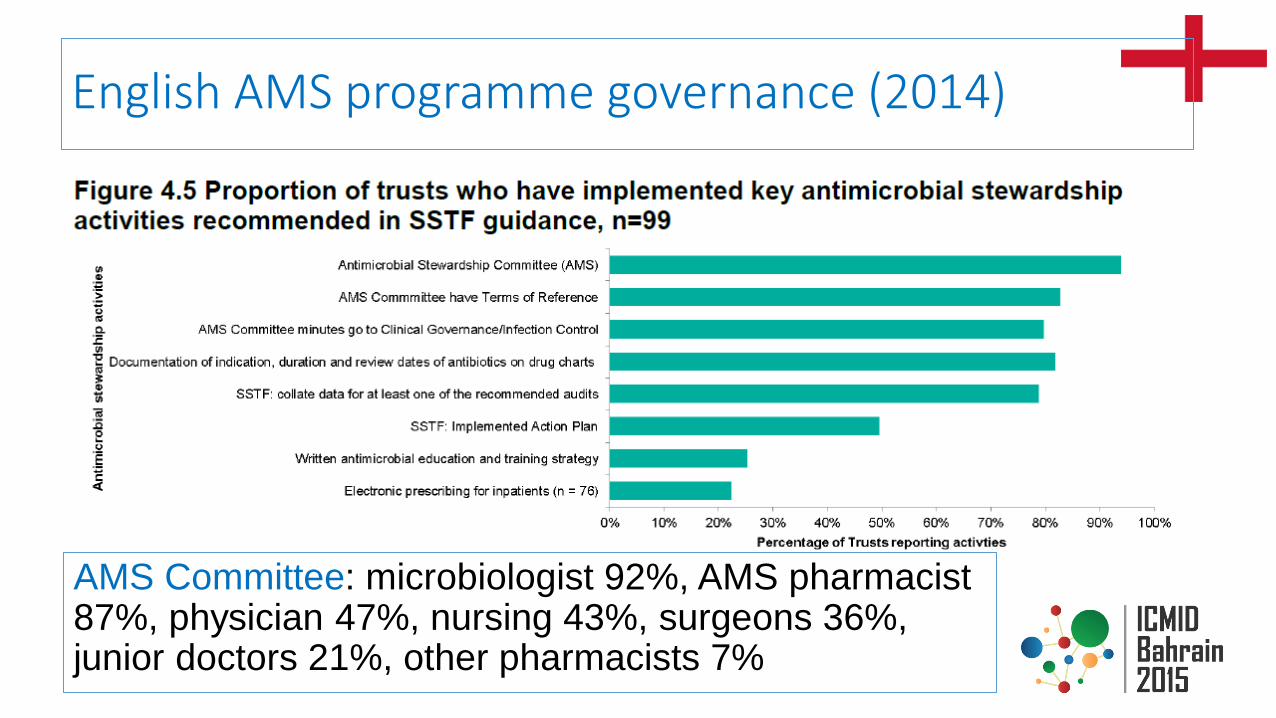
English AMS programme governance (2014)
AMS Committee: microbiologist 92%, AMS pharmacist 87%, physician 47%, nursing 43%, surgeons 36%, junior doctors 21%, other pharmacists 7%

AMS policy in hospitals: key elements
• 2003: £12m 3yr funding to establish AMS
• National hospital AMS Standards in 2011: Start Smart then Focus
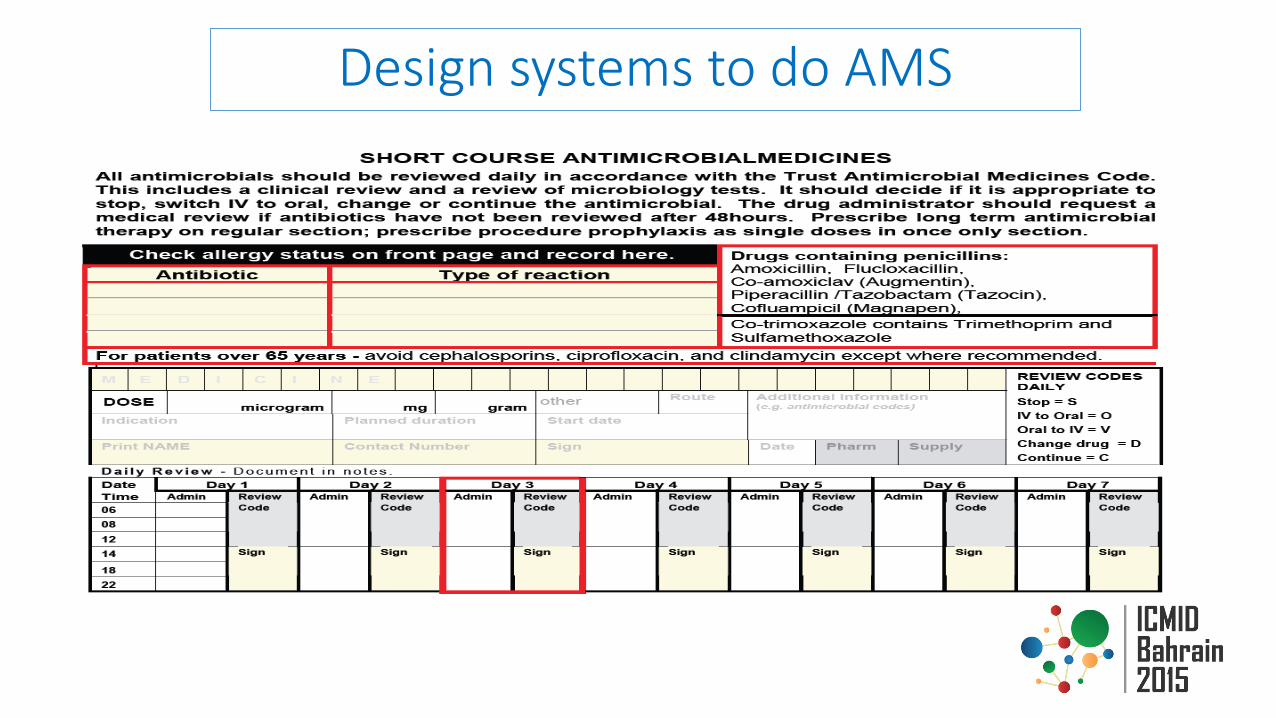
Design systems to do AMS

Models of delivering AMS
• Usually weekly ward rounds with clinical team
• Audit meeting presentations
• Patients on IV AB > 5 days or less
• Restricted antibiotic follow up
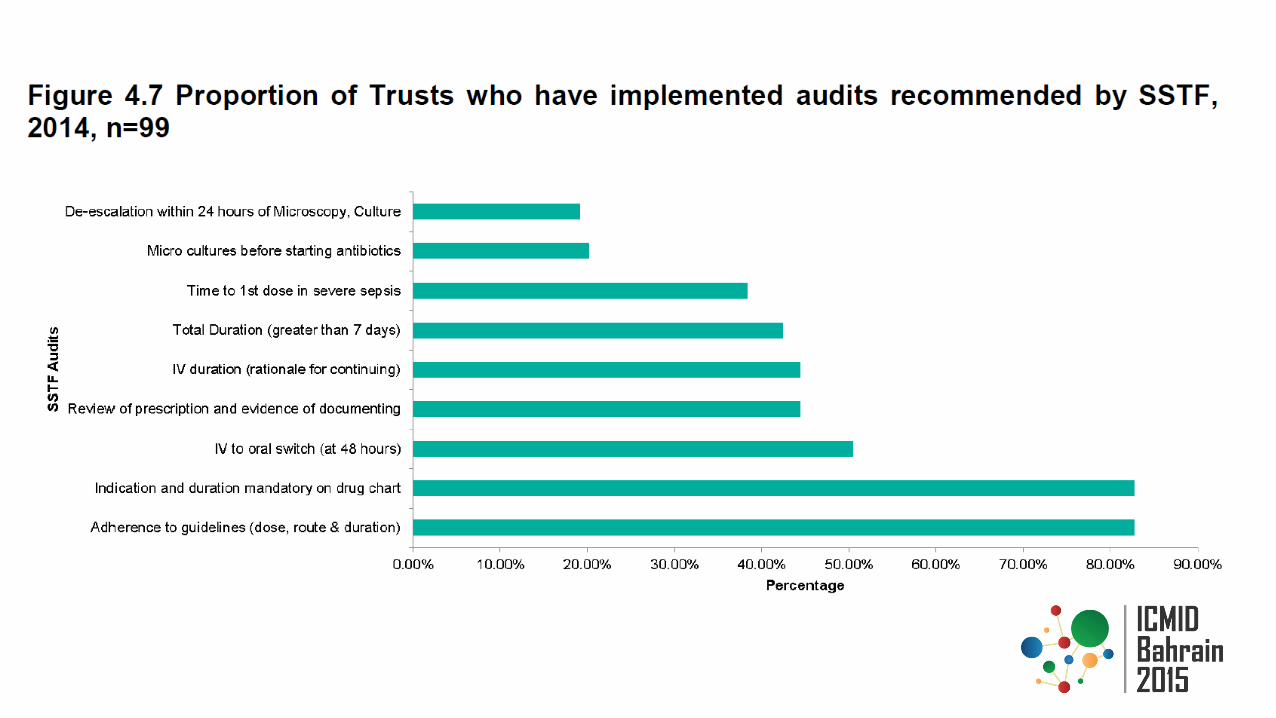
• Antimicrobial audits
• Comprehensive guidelines
• Wards ring for patient specific
advice to micro or ID
• Proactive follow up of bacteraemic patients
• Complex patients by specialty or AMR
Bacteraemia & ITU daily
ward rounds
Reactive call taking by
micro
Educational ward rounds
Pharmacy referral system
Antimicrobial Pharmacist role
• Most hospitals had a senior pharmacist for AMS plus 0.5wte of a junior pharmacist or a technician
• Writing guidelines 97%, formulary 94% (horizon scanning 71%)
• Referrals by phone or pager 88%
• Input into hospital IPC group 90%
• AMS ward rounds where high AB use 65%
• Publicising local AMR patterns 56%
• Working with local community AMS lead 37%
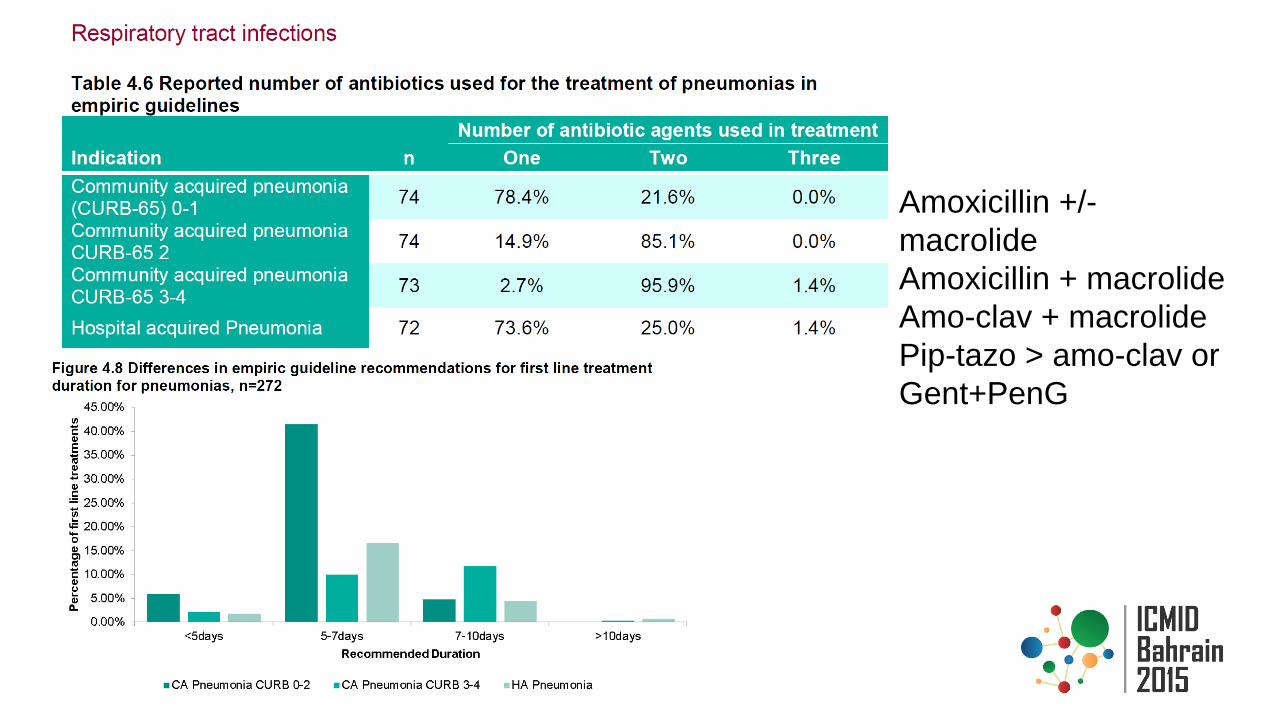
Amoxicillin +/-
macrolide
Amoxicillin + macrolide
Amo-clav + macrolide
Pip-tazo > amo-clav or
Gent+PenG
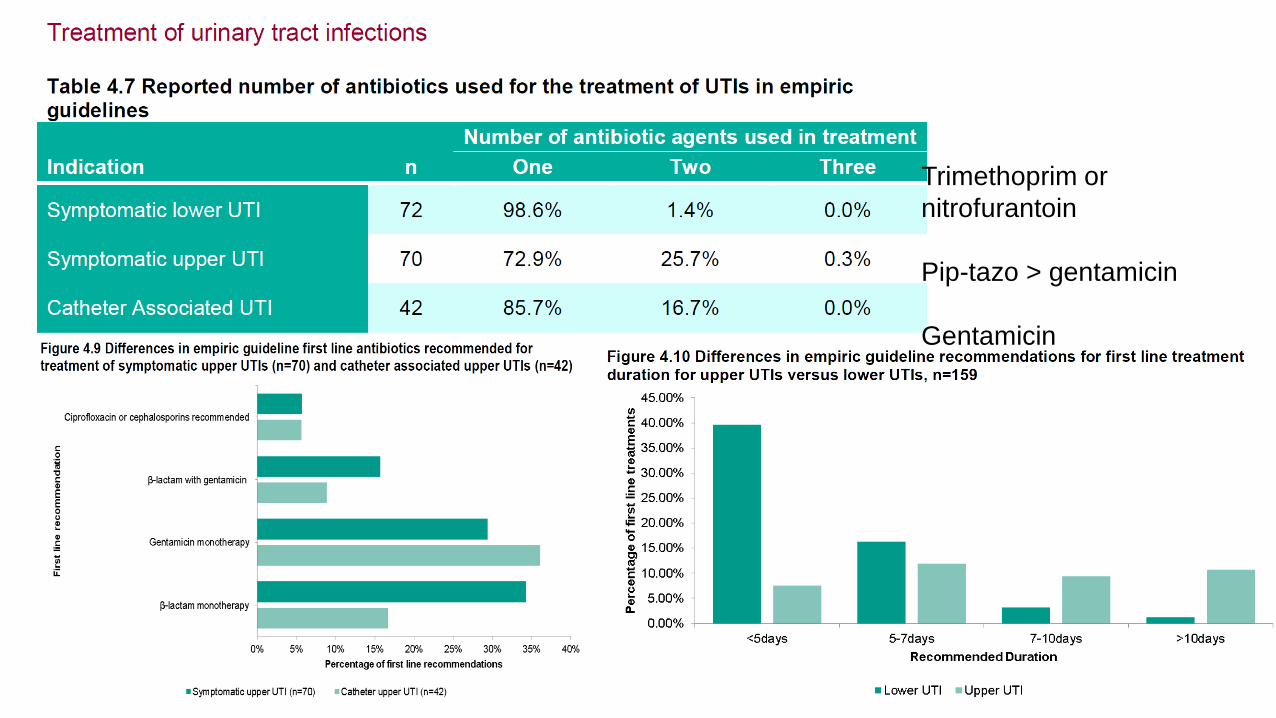
Trimethoprim or
nitrofurantoin
Pip-tazo > gentamicin
Gentamicin
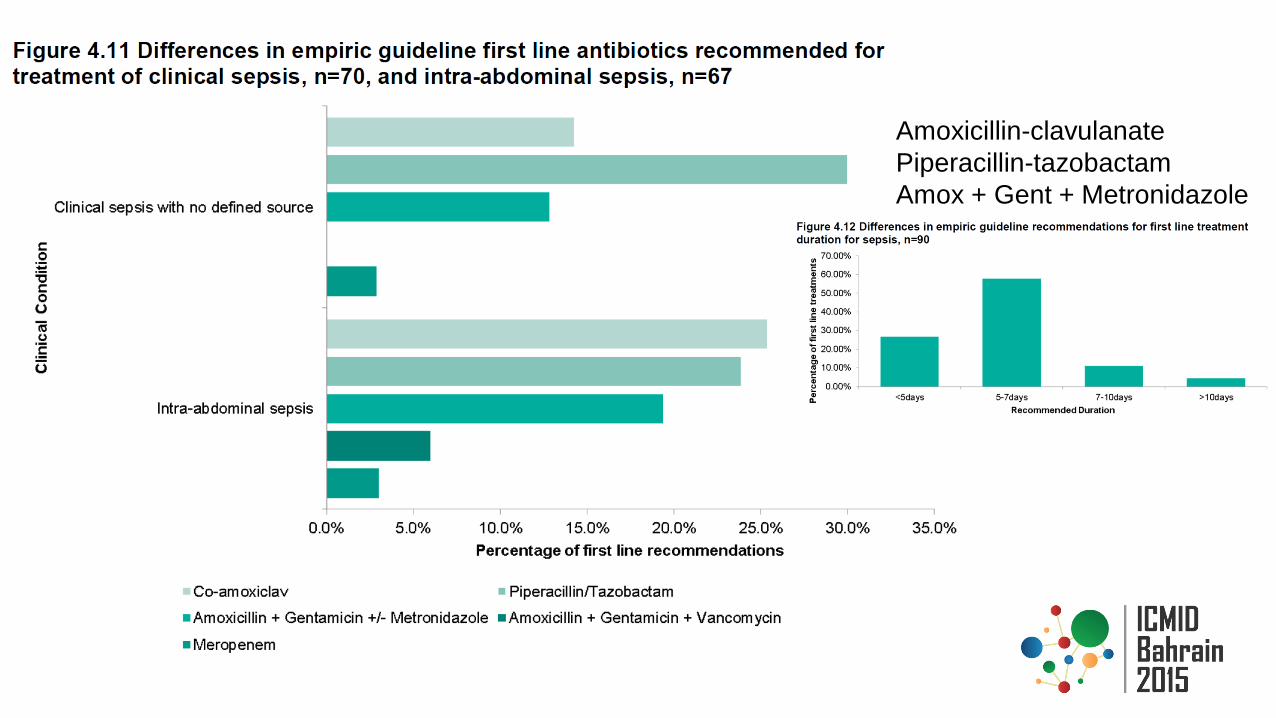
Amoxicillin-clavulanate
Piperacillin-tazobactam
Amox + Gent + Metronidazole

2015-6 AMR & AMS drivers • Quality Premium
• Overall aim, return to 2010 prescribing levels in hospitals & community
• Reduce antibiotic prescribing by 1% next year
• Hospitals: validate data & following year to carbapenems by 1%
• Primary care: 10% in quinolones + cefalosporins + amoxicillin-clavulanate as % of total ABs
• NICE Antimicrobial Stewardship guideline • Consultation on draft in Feb-15, launch May-15
• Quality standards to assess implementation
• Update hospital AMS guidelines • Require assurance that AMS is happening
Summary for AMS Models in UK
• UK 5 year AMR strategy has been a big lever for making improvements quickly
• Improve AMR and usage reporting for UK to report into Europe
• Setting targets (and seeing early reduction) in antimicrobial usage
• Improved mandatory education strategy for AMR & AMS
• Giving AMS a higher priority alongside IPC
• Moving the focus away from Clost.difficile & MRSA
• Scotland probably have the best model for AMS that demonstrates continual quality improvement

Models for stewardship in Hospital - UK Models
Philip Howard
Consultant Antimicrobial Pharmacist
Twitter: @AntibioticLeeds

















