55
Moderator: Dr. P.S. Chandra Dr Deepak Gupta Dr . Deepak Gupta
Moderator: Dr. P.S. ChandraDr Deepak GuptaDr. Deepak Gupta



Classification?Classification system should be:
ComprehensiveUsableAccuratePredictableAble to guide intervention
A precise, comprehensive, ideal and informative classification system has eluded spine surgeons since Boehler first proposed his injury categories in 1929 Boehler first proposed his injury categories in 1929.

classification ?classification ?
• Holdsworth (JBJS, 1970)o ds o t (J JS, 970)• Denis (Spine, 1983)• McAfee Classification(JBJS 65‐A; 1983)(J J 5 ; 9 3)• Load‐sharing Classification(McCormack et.al.
Spine 19; 1994)• Comprehensive Classification(Magerl Eur J Spine
3; 199Gertzbein Spine 19; 1994)h l b• Thoracolumbar Injury Severity Score
(TLISS)(Spine 2007 Feb 1;32(3).)

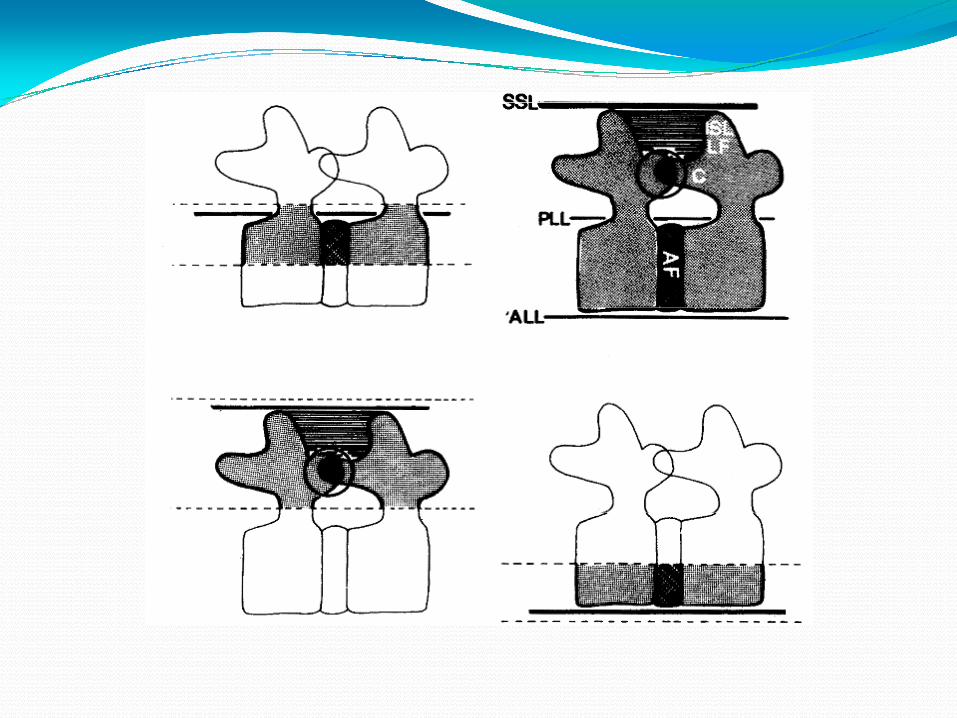
Denis (Spine, 1983)1st classification after introduction of CTModified the column concept of HoldsworthSpinal stability is based on 3 columnMiddle column: important of structural stability.Degree of instability: included the neurological status
f ti t of patient.
McCormack and Gaines (Spine 19; 1994)Load sharing classificationDegree of vertebral body comminution, apposition of fracture fragments, and the amount of sagittal plane deformitydeformity.Sought to predict the risk of implant failure.

AO(Arbeitsgemeinschaft fur Osteosynthesenfragen)/ Magerl (Eur J Spine 3; 1994)
Based on Pathomorphological criteria.And review of 1445 consecutive TL cases.
Advantage Disadvantage
Comprehensive Complex
Does not define stability
Moderate reliability. Eur Spine J. 2002 Jun;11(3):235‐45. Epub 2002 Jan 29
Does not include neurological deficit

Type A : vertebral body compression A1: impaction fractureA2: split fractureA3: burst fractureType B : distraction ( all 3 columns)B1: posterior injury – ligamentousp j y gB2: posterior injury – osseousB3: anterior injury through discType c : rotational (all 3 columns)yp ( 3 )C1: type A with rotationC2: type B with rotationC3: rotational shearC3

TLISS (Spine 2007 Feb 1;32(3).)To assist in clinical decision making for operative g pversus non operative careMechanism of injury, integrity of the PLC, and
lneurologic status.<3 : non operative , > 5 : operative, stabilization with or without decompressionor without decompression.
Advantage Disadvantage
Comprehensive Validity and ability to prove outcome i remain unproven
Define stability Validation studies performed by spine trauma study group.Spine J 2009 Sep;9(9):780‐8Spine J. 2009 Sep;9(9):780‐8.
Moderate reliability J Spinal DisordTech. 2009 Aug;22(6):422‐7.
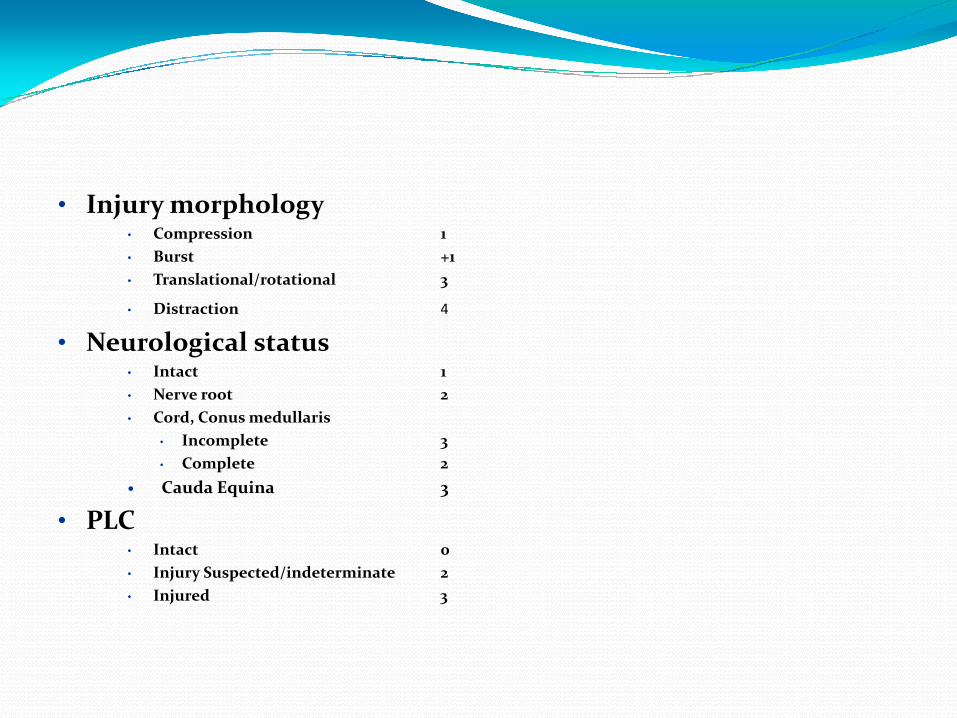
• Injury morphology• Injury morphology• Compression 1• Burst +1• Translational/rotational 3
Distraction 4• Distraction 4
• Neurological status• Intact 1• Nerve root 2• Cord, Conus medullaris
• Incomplete 3• Complete 2Cauda Equina 3
PLC• PLC• Intact 0• Injury Suspected/indeterminate 2• Injured 3


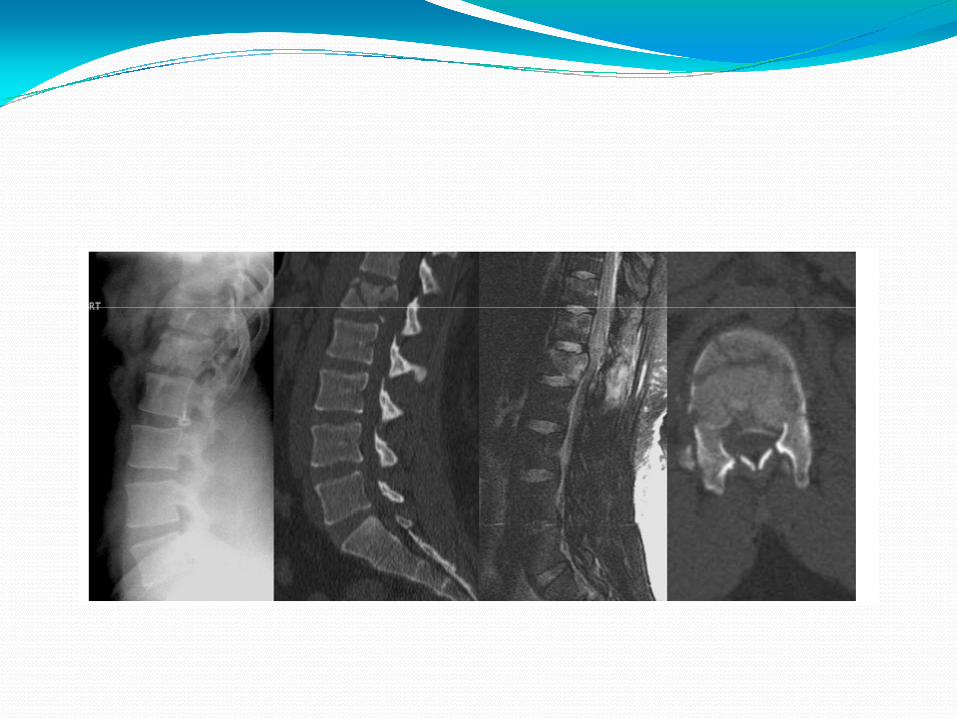


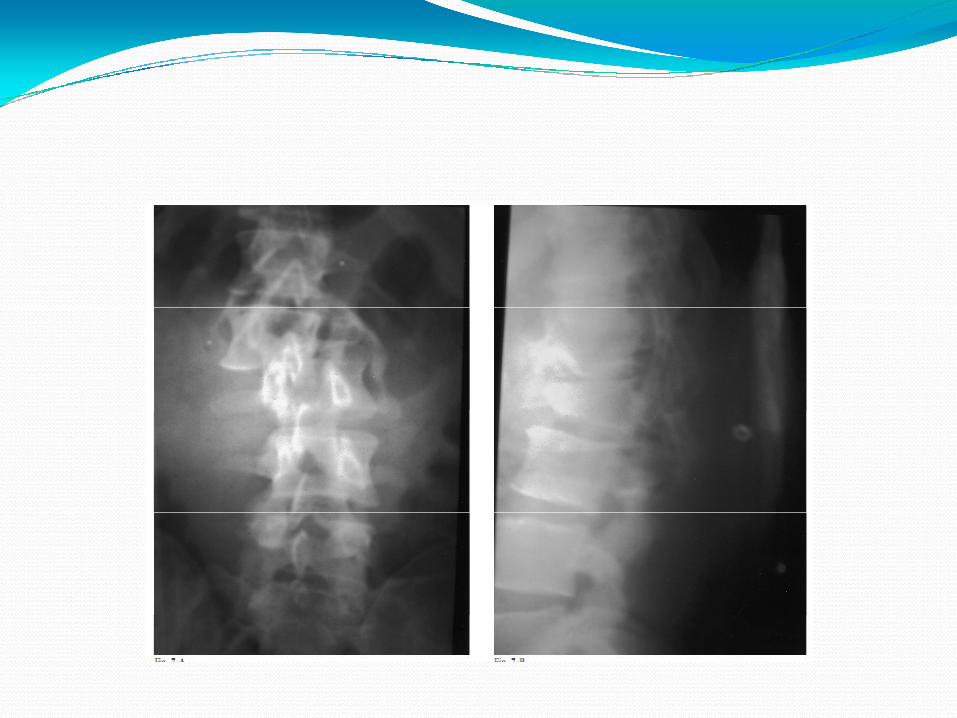
Imaging X rayInexpensive and quickDemonstrate loss of vertebral height.Kyphotic angleInterspinous distance in AP and Lateral view with alignment of spinous process for rotation of vertebra.A t i t b l b d l t l iAssess posterior vertebral body on lateral view.
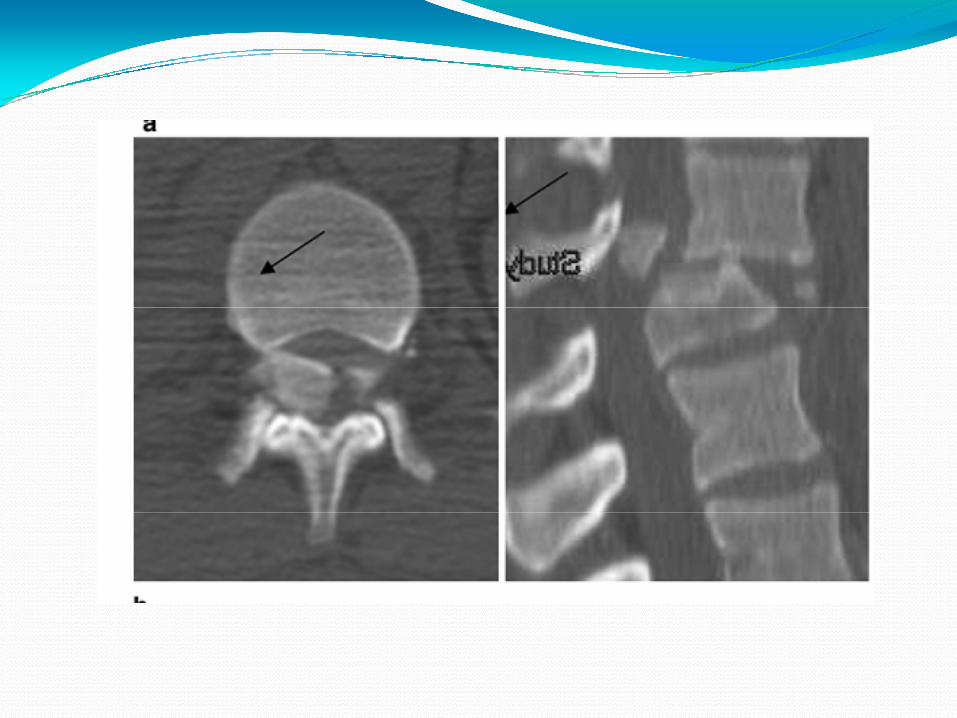
CT scanExcellent visualization of bony anatomy , particularly
iddl i l l i l l h d middle spinal column, spinal canal shape and patency.Reverse cortical sign – contraindication for ligamentotaxis in posterior approachligamentotaxis in posterior approach.

MRI scanExcellent visualization of soft tissue i.e. ligament (post li ) di i l dligament), disc , spinal cord.Poor prognostic factor : edema extending two vertebral level and presence of hematoma within spinal cordlevel and presence of hematoma within spinal cord.


Defining instabilityWhy is it important to look for instability?
‘ Instability’ is the key to therapeutic indications because it equates, in many cases, with a need for internal stabilizationstabilization.
Francis Denis, M.D. Spinal stability as defined by the three‐ column i i i l CORR 8 6 6 spine concept in acute spinal trauma. CORR. 189: 65‐ 76

f f b l f l d bDefinition of stability as formulated by Whitesides ,Magrel and Denis‘A stable spine is one which can withstand axial
forces anteriorly, tensile forces posteriorly and rotational forces, so as to hold the body erect, , y ,protecting the contents of the canal and preventing progressive kyphosis’
Whitesides TE Jr (1977) Traumatic kyphosis of the thoracolumbar spine. Clin Orthoped 128: 78‐ 92
Francis Denis. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine Vol 8; No 8: 817‐ 831

If l i i h hIf neurology is intact whether to operate or not
No superiority of conservative therapy over operative therapy
• Surg Neurol. 2007 Mar;67(3):221‐31; discussion 231.A i f th t f th l b b t f tA review of the management of thoracolumbar burst fractures.Dai LY
• J Bone Joint Surg Am. 2003 May;85‐A(5):773‐81.Operative compared with nonoperative treatment of a thoracolumbar burst fracture Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study.
• Wood K, Cochrane Database Syst Rev. 2006 Oct 18;(4):CD005079.Operative versus non‐operative treatment for thoracolumbar burst fractures
h l l d fwithout neurological deficit.Yi L

Stable thoracolumbar burst without neurology (vertebral compression or canal encroachment < 40% or kyphosis <15 degrees with a stable posterior column)or kyphosis <15 degrees with a stable posterior column)Medically unfitJ Neurosurg 1997 Jan;86(1):48‐55J Neurosurg. 1997 Jan;86(1):48 55
Whether cast bracing can be usedWhether cast bracing can be used in stable/unstable burst fracture
J Neurosurg Spine 2009
Christopher S. Baileyp yA thoracolumbar burst fracture, in exclusion of
an associated posterior ligamentous complex injury, is inherently a very stable injury and may not require a brace.
Spine Sep 1996 Chow, Gregory H.Functional Outcome of Thoracolumbar Burst Fractures Managed With
Hyperextension Casting or Bracing and Early Mobilization
N ti t f th l b b t • Non operative management of thoracolumbar burst fractures with hyperextension casting or bracing was proven to be a safe and effective method of treatment in selected patients patients.
• Clinical results were favorable.• No neurologic deterioration was observed.
H i li i i i i i d• Hospitalization times were minimized.• Patient satisfaction was high. • The authors do not believe that ligamentous injury of the g j y f
posterior column is a contraindication to nonoperativemanagement of thoracolumbar burst fractures.
What is the ideal time for surgeryWhat is the ideal time for surgerySpine (Phila Pa 1976). 2010 Apr 20;35(9 Suppl):S138‐45.Does early fracture fixation of thoracolumbar spine fractures decrease morbidity or mortality?spine fractures decrease morbidity or mortality?Bellabarba C
• These studies demonstrated that early stabilization of fractures reduced ‐ the mean number of days on a ventilator,‐ the number of days in intensive care unit and in hospital
• Ideally, patients with unstable thoracic fractures y, pshould undergo early (<72 hours) stabilization of their injury to reduce morbidity and, possibly, mortality.

J Spinal Cord Med. 2005;28(1):11‐9.
Timing of surgery following spinal cord injury. g g y g p j yKishan S
• Early surgical treatment ( within 24 hrs ) is beneficial in terms of ‐ reducing complications
l h f d ‐ length of stay, and ‐ hospital costs.
F th t di d d t l l d t t th • Further studies are needed to clearly demonstrate the impact of operative timing on neurological outcome.
Those patients in whom operations were performed within first 24 hour
had a lower rate of complications.Willberger JE (1991)

• Early surgery ( <5 days) : Ligamentotaxis /Annulotaxis useful in burst fractures.A i h W i d f h i • Anterior approach : Wait 3‐4 days for hyperemeia to subside, less bleeding.
• Severely injured : early surgery: Few c/c shorter • Severely injured : early surgery: Few c/c, shorter hospital stay, reduced ventilatory requirement.A retrospective analysis of treatment outcomes. Olumide A p yDanisa. Spine surgery, Virginia, JNS 1995.
Approach ?Approach ?• Journal of Spinal Disorders & Techniques. February 2006
Surgical Decision Making for Unstable Thoracolumbar Spine Injuries: Results of a Consensus Panel Review by the Spine Trauma Study Group.Vaccaro Alexander R Vaccaro, Alexander R
Decision making for the surgical treatment of thoracolumbar injuries is largely dependent on three patient characteristics: j g y p pInjury morphology Neurologic status Posterior ligament integrity. g g yA logical and practical decision‐making process based on these characteristics may guide treatment even for the most complicated fracture patterns.
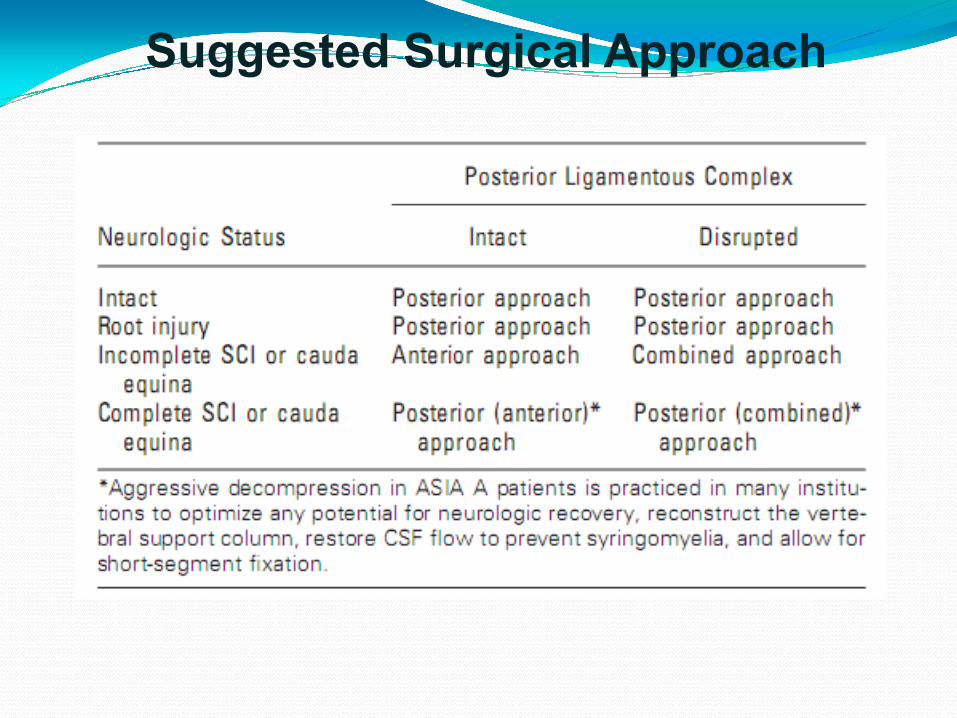
Suggested Surgical Approach

Anterior approach Posterior approach
Advantage: Predictable canal decompression,
Advantage :Spinal stability, deformity correction,
improvement neurology, no increased morbidity
low morbidity
Disadvantage Di d tDisadvantage –Stiffness : 15% + than normal spineInstrument failure :4‐11%Loss of correction : 1‐4 degrees
Disadvantage‐Stiffness of normal spine : 76%Instrument failure rate : 9‐54%Loss of correction 3‐12 degreesL ti L bl d l l Less time, Less blood loss, less expensive ( JNS 1995,Virginia)
Is decompression indicated forIs decompression indicated for complete spinal cord injury
( )Journal Bone Joint Surg Br. 2000 Jul;82(5):629‐35.Does 'canal clearance' affect neurological outcome after thoracolumbar burst fractures? Boerger TOg
The paralysis occurs at the moment of injury and is not related to the position of thefragments of the fracture on subsequent imaging.Alteration of the canal by 'surgical clearance' does not affect the neurological outcome.There is no established advantage of surgical over non‐surgical treatment as regardsneurological improvement.Surgical treatment for burst fracture in the belief that neurological improvement can beSurgical treatment for burst fracture in the belief that neurological improvement can beachieved is not justified, although surgery may still occasionally be indicated forstructural reasons.

Length of fusion : short versus long segmentShort segment fusion : fracture without translation (LSC )(LSC 6 or <6).Long segment fusion : fracture with translation ( LSC 7 8 9) Better but loses spinal mobility7,8,9). Better but loses spinal mobility.

Surgical approaches: anterior, posterior or anteroposteriorP i fi i LSC Posterior fixation : LSC 6 or <6.Anterior fixation : LSC >7LSC i h l i l i j i f ll d b LSC >7 with translational injury : anterior followed by posterior fixation.

Can anterior reconstruction be avoided by long segment posteriorCan anterior reconstruction be avoided by long segment posterior fixation in unstable Thoraco Lumbar burst fracture ?
J Spinal Disord Tech. 2005 Dec;18(6):485‐8.Posterior fixation of thoracolumbar burst fracture: short segment Posterior fixation of thoracolumbar burst fracture: short‐segment pedicle fixation versus long‐segment instrumentation.Tezeren G
LS instrumentation is a more effective management of LS instrumentation is a more effective management of thoracolumbar burst fractures.Anterior column support would negate the need for LS Anterior column support would negate the need for LS fixationNevertheless, clinical outcome is same between the two groups.
Compression fracture in osteoporotic bones
Balloon kyphoplasty versus vertebroplasty for treatment of osteoporotic vertebral compression fracture: a prospective, comparative, and randomized clinical studyp , y
Higher cost of the kyphotic balloon procedure, we recommend vertebroplasty over kyphoplasty for the treatment of osteoporotic VCFs.Osteoporos Int. 2010 Feb;21(2):359‐64. Epub 2009 Jun 10.
Vertebral body stentingVBS is an innovative technique which allows for the possibly complete reduction of vertebral compression fractures and helps maintain the restored height by means fractures and helps maintain the restored height by means of a stent. The height loss after balloon deflation is significantly decreased by using VBS compared to k h l h ff i i i i f kyphoplasty, thus offering a new promising option for vertebral augmentation.Eur Spine J (2010) 19:916–923p 9 9 9 3


Comparison of anterolateral and posterior approaches in the management of h l b b fthoracolumbar burst fractures.
Angular deformity is more successfully corrected d i t i d h th t i h i and maintained when the anterior approach is
used. Retrospective study T12 L2 fracture 63 patientRetrospective study, T12‐L2 fracture , 63 patient.J Neurosurg Spine 5:117–125, 2006

Unstable Thoracolumbar Burst Fractures Anterior‐Only Versus Short‐Segment Posterior FixationThis study compares anterior only fixation utilizing a corpectomy strut graft and a modern thoracolumbarplating system with a posterior‐only construct using
di l d l d h i h k f h f pedicle screws and load sharing hooks for the treatment of unstable burst fractures.Anterior only group continued to demonstrate statistically i ifi t i t i itt l li t t f ll significant improvement in sagittal alignment at follow‐up
compared to preoperative measurements.J Spinal Disord Tech 2006;19:242–248

PLIF in thoracolumbar trauma: technique and radiological results This technique can be an alternative procedure to combined operations regarding the presented
di l i l lt f f l f i d l f radiological results of successful fusion and loss of correction.Eur Spine J (2010) 19:1079–1086.Eur Spine J (2010) 19:1079 1086.
Is Methylprednisolone really useful.UncertainUncertain
Various studies have shown contradicting results
Three multi Centre NASCIS studies in US inconclusive
• Recommendationswithin 3 hrs : for 24 hrswithin 3 hrs : for 24 hrs3‐8 hrs : for 48 hrs
However it should be mentioned that there is no d fi i l i id f b fi i l ff d definite conclusive evidence of a beneficial effect and that there could be some complications related to its use.
DoseBolus – IV 30 mg/kg body weight over 15 minutesConstant infusion – 5.4 mg/kg/hour for 23 hours

Take Home Message
Classification ?No ideal systemNo ideal systemTLICS, AO, Denis suitable available options
Defining instabilityg yA stable spine is one which can withstand axial forces anteriorly, tensile forces posteriorly and rotational forces, so as to hold the body erect, protecting the contents of the canal and preventing progressive k h i ’kyphosis’.Injury to PLC is a main indicator of instability.
Role of cast bracing in stable/unstable burst gfractureProven to be a safe and effective method of treatment in selected patients selected patients.

Ideal time for surgeryAs soon as the general condition is stable.
Role of Surgery in neurologically intact ptsThere is no superiority of conservative therapy over operative th t i l t ti t i h th h therapy except in poly trauma patients in whom the surgery has better results.
Approach?Determined by incompleteness and PLC involvement.

Is decompression indicated for complete SCI. Surgical decompression is not vital to the neurological recovery but may obviate later complications of syrinx and may provide a patent canal for any future successful regenerative therapypatent canal for any future successful regenerative therapy.
Role of pedicle screws in the fracture vertebra?• Helps to provide better kyphosis correction and biomechanicalHelps to provide better kyphosis correction and biomechanical
stability.
Does anterior reconstruction avoid long segmentposterior fixation in unstable thoraco Lumbar burstfracture ?r
Particularly useful in preserving rotation in SCI.

Role of augumentation of the fracturedRole of augumentation of the fracturedvertebrae with kyphoplasty
Provides excellent immediate reduction of post‐traumatic segmental kyphosis.
Is methylprednisolone really usefulIs methylprednisolone really usefulUncertainFor all patients reporting within 8 hours of injury the p p g j yoption of using methylprednisolone could be given to the patients.

Th k YThank You

















