Journal of the American Society of Nephrology 2271 Modulators of Crescentic Glomerulonephritis1 Robert C. Atkins,2 David J. Nikolic-Paterson, Qing Song, and Hui V. Lan PATHOGENESIS OF CRESCENT FORMATION R.C. Atkins, D,J. Nikolic-Paterson, Q, Song, HY, Lan, Department of Nephrology, Monash Medical Centre, Clayton Road, Clayton, Victoria, Australia (J, Am. Soc. Nephrol. 1996; 7:2271-2278) ABSTRACT Glomerular crescent formation is a prominent feature of aggressive forms of glomerulonephritis and is asso- ciated with a poor prognosis. An understanding of the mechanisms involved in crescent formation is crucial for the development of new therapies for this disease. This article reviews current ideas on the pathogenesis of glomerular crescent formation and describes methods for modulation of this process. Emphasis is given to the role of the proinflammatory cytokines interleukin- and tumor necrosis factor-a in crescent development and its modulation by cytokine block- ade. Key Words: Interleukin- 1. tumor necrosis factor-a, cytokine, Therapy G lomerular crescents are a feature of rapidly progressive glomerulonephritis. which is asso- elated with a poor prognosis (1 ). In general, those patients with the most severe renal failure and rapidly progressive disease have the highest percentage of glomeruli with crescent formation (2,3). Although a consensus on treatment regimens for this heteroge- neous group of patients is emerging (4), there is a pressing need to develop new drugs that will reduce the proportion of patients progressing to end-stage renal failure. Thus, much emphasis has been placed on understanding the pathogenic mechanisms in- volved in glomerular crescent formation with the aim of identifying new therapeutic targets. This article discusses current ideas on the pathogenesis of cres- cent formation and possible strategies for modulation of crescentic glomerulonephritis. In particular, the role of the proinflammatory cytokines interleuki.n- 1 (IL- 1) and tumour necrosis factor a (TNF-a) in crescent formation is discussed on the basis of in vivo blocking studies. 1 ReceIved February 20, 1996. Accepted May 9, 1996. 2 Correspondence to Dr. P.C. Atkins, Department of Nephrology, Monash MedI- cal Cenfre, Clayton Road, Clayton, Victoria 3168, Australia. 1046.6673/071 1-227) $030010 Journal of the American Society of Nephrology Copyright C 1996 by the American Society of Nephrology Examination of biopsy specimens from patients with crescentic glomerulonephritis show heterogene- ity in both the percentage of crescents and the stages ofcrescent development between glomeruli. Crescents can be divided into two main types: (1 ) cellular cres- cents, which contain cells with little or no collagen deposition within Bowman’s space; and (2) crescents with varying degrees of fibrous organization, which are described as either fibrocellular or fibrous, de- pending on the balance of cells and fibrosis within Bowman’s space. It is thought that cellular crescents represent the first stage of crescent formation, which can subsequently develop fibrous organization (5). This later step is thought to occur by the migration of periglomerular fibroblasts into Bowman’s space through areas of disruption of Bowman’s capsule (6,7). A schematic model of glomerular crescent for- mation is shown in Figure 1. Cellular Crescents Cellular crescents are defined as the presence of two or more layers of cells within Bowman’s space. How- ever, the composition of cellular crescents has been a controversial issue. Some studies have identified epi- thelial cells as the main component, whereas other investigations have demonstrated that macrophages are the major cell type within cellular crescents (8- 13). These results suggest that cellular crescents are highly heterogeneous, with marked differences seen in various disease categories and also within individual kidneys. Humoral reactants. Deposition of fibrin and plas- ma-derived fibronectin within Bowman’s space is of- ten associated with cellular crescent formation. The importance of fibrin deposition has been shown by the ability of ancrod and streptokinase treatment to pre- vent crescent formation in rabbit anti-glomerular basement membrane (anti-GBM) glomerulonephritis ( 14). Procoagulant activity of infiltrating glomerular macrophages is also crucial in fibrin deposition within Bowman’s space ( 15). Deposition of plasma fibronec- tin within Bowman’s space is thought to facilitate cell proliferation and accumulation during crescent for- mation (16). Reversibility of cellular crescents. Not all crescents become fibrotic. As shown schematically in Figure 1, cellular crescents can either progress or resolve. Res- olution of crescent formation is seen in the spontane- ous recovery of a subgroup of patients with rapidly progressive glomerulonephritis (reviewed in Reference 17). Similarly, 90% of glomeruli exhibited cellular accumulation or exudate material within Bowman’s
Transcript
Journal of the American Society of Nephrology 2271
Modulators of Crescentic Glomerulonephritis1Robert C. Atkins,2 David J. Nikolic-Paterson, Qing Song, and Hui V. Lan
PATHOGENESIS OF CRESCENT FORMATION
R.C. Atkins, D,J. Nikolic-Paterson, Q, Song, HY, Lan,Department of Nephrology, Monash Medical Centre,Clayton Road, Clayton, Victoria, Australia
(J, Am. Soc. Nephrol. 1996; 7:2271-2278)
ABSTRACTGlomerular crescent formation is a prominent featureof aggressive forms of glomerulonephritis and is asso-ciated with a poor prognosis. An understanding of themechanisms involved in crescent formation is crucialfor the development of new therapies for this disease.This article reviews current ideas on the pathogenesisof glomerular crescent formation and describesmethods for modulation of this process. Emphasis isgiven to the role of the proinflammatory cytokinesinterleukin-� and tumor necrosis factor-a in crescentdevelopment and its modulation by cytokine block-ade.
G lomerular crescents are a feature of rapidlyprogressive glomerulonephritis. which is asso-
elated with a poor prognosis ( 1 ). In general, thosepatients with the most severe renal failure and rapidlyprogressive disease have the highest percentage ofglomeruli with crescent formation (2,3). Although a
consensus on treatment regimens for this heteroge-neous group of patients is emerging (4), there is a
pressing need to develop new drugs that will reduce
the proportion of patients progressing to end-stagerenal failure. Thus, much emphasis has been placed
on understanding the pathogenic mechanisms in-volved in glomerular crescent formation with the aimof identifying new therapeutic targets. This articlediscusses current ideas on the pathogenesis of cres-cent formation and possible strategies for modulationof crescentic glomerulonephritis. In particular, therole of the proinflammatory cytokines interleuki.n- 1(IL- 1 ) and tumour necrosis factor a (TNF-a) in crescent
formation is discussed on the basis of in vivo blockingstudies.
1 ReceIved February 20, 1996. Accepted May 9, 1996.
2 Correspondence to Dr. P.C. Atkins, Department of Nephrology, Monash MedI-
cal Cenfre, Clayton Road, Clayton, Victoria 3168, Australia.
1046.6673/071 1-227) $030010Journal of the American Society of NephrologyCopyright C 1996 by the American Society of Nephrology
Examination of biopsy specimens from patientswith crescentic glomerulonephritis show heterogene-ity in both the percentage of crescents and the stagesofcrescent development between glomeruli. Crescentscan be divided into two main types: (1 ) cellular cres-
cents, which contain cells with little or no collagendeposition within Bowman’s space; and (2) crescentswith varying degrees of fibrous organization, whichare described as either fibrocellular or fibrous, de-pending on the balance of cells and fibrosis withinBowman’s space. It is thought that cellular crescentsrepresent the first stage of crescent formation, whichcan subsequently develop fibrous organization (5).
This later step is thought to occur by the migration of
periglomerular fibroblasts into Bowman’s spacethrough areas of disruption of Bowman’s capsule(6,7). A schematic model of glomerular crescent for-mation is shown in Figure 1.
Cellular Crescents
Cellular crescents are defined as the presence of two
or more layers of cells within Bowman’s space. How-ever, the composition of cellular crescents has been acontroversial issue. Some studies have identified epi-
thelial cells as the main component, whereas otherinvestigations have demonstrated that macrophagesare the major cell type within cellular crescents (8-13). These results suggest that cellular crescents arehighly heterogeneous, with marked differences seen in
various disease categories and also within individual
kidneys.Humoral reactants. Deposition of fibrin and plas-
ma-derived fibronectin within Bowman’s space is of-ten associated with cellular crescent formation. Theimportance of fibrin deposition has been shown by the
ability of ancrod and streptokinase treatment to pre-
vent crescent formation in rabbit anti-glomerular
basement membrane (anti-GBM) glomerulonephritis( 14). Procoagulant activity of infiltrating glomerular
macrophages is also crucial in fibrin deposition withinBowman’s space ( 15). Deposition of plasma fibronec-tin within Bowman’s space is thought to facilitate cellproliferation and accumulation during crescent for-mation (16).
Reversibility of cellular crescents. Not all crescents
become fibrotic. As shown schematically in Figure 1,cellular crescents can either progress or resolve. Res-olution of crescent formation is seen in the spontane-ous recovery of a subgroup of patients with rapidlyprogressive glomerulonephritis (reviewed in Reference17). Similarly, 90% of glomeruli exhibited cellular
accumulation or exudate material within Bowman’s
SS
Cellular
J4,
Normal
Advanced
/
Modulators of Crescentic Glomerulonephritis
2272 Volume 7 . Number 1 1 #{149}199#{243}
Fibrous
.
S S
S
Fibrocellular
;�II,.
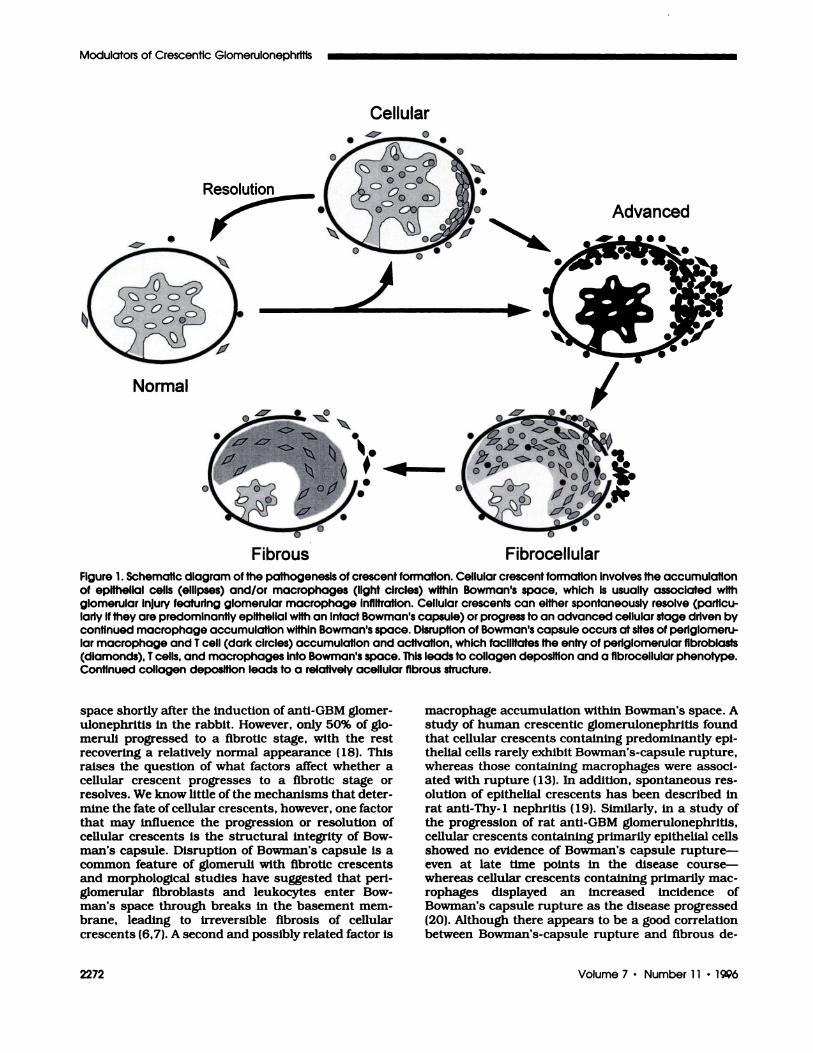
Figure 1 . Schematic diagram of the pathogenesis of crescent formation. Cellular crescent formation involves the accumulationof epithellal cells (ellipses) and/or macrophages (light circles) within Bowman’s space, which Is usually associated withglomerular Injury featuring glomerular macrophage infiltration. Cellular crescents can either spontaneously resolve (particu-larly if they are predominantly epithellal with an intact Bowman’s capsule) or progress to an advanced cellular stage driven bycontinued macrophage accumulation within Bowman’s space. Disruption of Bowman’s capsule occurs at sites of periglomeru-br macrophage and I cell (dark circles) accumulation and activation, which facilitates the entry of periglomerular fibroblasts(diamonds), I cells, and macrophages Into Bowman’s space. This leads to collagen deposition and a fibrocellular phenotype.Continued collagen deposition leads to a relatively acellular fibrous structure.
space shortly after the induction of anti-GBM glomer-
ulonephritis in the rabbit. However, only 50% of gb-merull progressed to a fibrotic stage, with the restrecovering a relatively normal appearance ( 18). Thisraises the question of what factors affect whether acellular crescent progresses to a fibrotic stage or
resolves. We know litHe of the mechanisms that deter-mine the fate of cellular crescents, however, one factorthat may influence the progression or resolution ofcellular crescents is the structural integrity of Bow-man’s capsule. Disruption of Bowman’s capsule is acommon feature of glomeruli with fibrotic crescentsand morphological studies have suggested that pen-gbomerular fibroblasts and leukocytes enter Bow-man’s space through breaks in the basement mem-brane, leading to irreversible fibrosis of cellularcrescents (6,7). A second and possibly related factor is
macrophage accumulation within Bowman’s space. Astudy of human crescentic gbomerulonephnitis foundthat cellular crescents containing predominantly epi-
thelial cells rarely exhibit Bowman’s-capsule rupture,whereas those containing macrophages were associ-ated with rupture ( 13). In addition, spontaneous res-olution of epithelial crescents has been described inrat anti-Thy- 1 nephnitis ( 19). Similarly, in a study ofthe progression of rat anti-GBM gbomerubonephritis,cellular crescents containing primarily epithelial cells
showed no evidence of Bowman’s capsule rupture-even at late time points In the disease course-whereas cellular crescents containing primarily mac-rophages displayed an increased incidence ofBowman’s capsule rupture as the disease progressed
(20). Although there appears to be a good correlation
between Bowman’s-capsule rupture and fibrous de-
Atkins et al
Journal of the American Society of Nephrology 2273
velopment of glomerular crescents, there is no direct
evidence of a cause-and-effect relationship to support
this postulate. Other possible mechanisms determin-ing the fate of cellular crescents may be the nature of
the chemotactic molecules, inflammatory cytokines,and prosclerotic growth factors produced by crescent
cells or resident glomerular cells, such as parietal
epithelial cells.
Macrophage accumulation in Bowman’s space. The
primary feature in the development of advanced cel-
lular crescents is the large accumulation of macro-
phages within Bowman’s space. One mechanism of
macrophage accumulation within Bowman’s space is
migration of macrophages from the glomenular tuft, a
process that is likely to involve chemotactic molecules
and cell-matrix and cell-cell adhesion interactions.Fibnin is the only chemotactic molecule directly
implicated in macrophage accumulation in Bowman’s
space. However, several other molecules may be in-
volved, such as monocyte chemoattractant protein-i
(MCP- 1 ), macrophage colony stimulating factor, and
macrophage migration inhibitory factor. Production of
MCP- 1 within crescents has been demonstrated by
immunostaining in human glomerulonephritis (21).
Also, each of these chemotactic molecules can besynthesized by proximal tubular cells, indicating that
they might be produced by parietal epithelial cellsduring crescent formation (22-24).
Macrophages express a variety of adhesion mole-
cules, such as VLA-4 and Mac- 1 of the integnin family,
that facilitate adhesion to fibronectin and fibninogen-
two molecules often present in Bowman’s space at the
start of crescent formation. In addition, VLA-4 andLFA- 1 mediate adhesion to cells expressing VCAM- 1and ICAM- 1 , respectively. There is strong upregula-
tion of VCAM- 1 and ICAM- 1 expressIon by parietal
epithelial cells in most forms of glomerulonephnitis,
which may play a role in the accumulation of macro-
phages in Bowman’s space during crescent formation
(25). Indeed, administration of anti-ICAM- 1 or anti-LFA- 1 antibodies not only inhibits the induction of rat
autoimmune anti-GBM glomerulonephritis, but can
intervene in established disease and prevent further
crescent formation, demonstrating a pathogenic role
for the LFA- 1 /ICAM- 1 interaction in this disease
model (26).Another adhesion molecule that may be involved in
macrophage accumulation within Bowman’s space is
CD44. This cell-surface glycoprotein mediates adhe-
sion to hyaluronic acid and is expressed by macro-phages and a variety of other cell types (27). The
combination of de novo CD44 expression by parietal
epithelial cells and hyaluronic acid deposition in Bow-man’s space in rat anti-GBM glomerulonephnitis may
facilitate the migration and accumulation of CD44+macrophages within Bowman’s space through mac-
rophage-matnix and hyaluronic acid-dependent mac-
rophage-epitheliaJ cell interactions (28,29).Local macrophage proliferation within Bowman’s
space. Migration from the glomerular tuft is one route
of macrophage accumulation within crescents. A sec-ond possibility is that macrophages proliferate locallywithin Bowman’s space. Macrophage proliferationwithin cellular crescents in rat anti-GBM glomerulo-nephritis has been shown by the presence of mitoticfigures, bromodeoxyunidine incorporation, and ex-pression of the proliferating cell nuclear antigen by
ED 1 � macrophages. In one study, the number of
proliferating macnophages within Bowman’s spacegave a significant positive correlation with the total
number of macrophages within Bowman’s space, buta negative correlation with the total number of mac-
rophages within the glomerular tuft, suggesting that
macrophage proliferation occurred locally within Bow-
man’s space (Lan HY, Nikolic-Paterson DJ, Mu W,
Atkins RC, unpublished observations). If local prolif-eration were to prove to be a general mechanism ofmacrophage accumulation in crescentic glomerulone-phritis, this would be a target for future drug develop-
ment.T cells in crescents. Although glomerular macro-
phage accumulation is evident in many forms of hu-
man glomerulonephritis, significant glomerular T cell
infiltration is usually restricted to rapidly progressive
glomerulonephnitis (30). In a study of immunoglobulin(Ig) A disease, glomerular infiltration of immune-acti-
vated (IL-2 receptor-positive) T cells was prominent in“active” crescentic glomerulonephnltis and correlatedwith the loss of renal function. Furthermore, thepresence of glomerular T cells was associated with
extensive disruption of Bowman’s capsule and sug-
gested the participation of a delayed-type hypersensi-tivity mechanism in crescent formation (3 1).
The importance of T cells in crescent formation hasbeen demonstrated in animal models of glomerulone-phnitis. In a rat model of immune cell-mediated renalinjury induced by immunization with the hapten azo-benzenearsonate, followed by planting of the antigenin the kidney, glomerular crescent formation and
Bowman’s-capsule rupture was observed in associa-
tion with granulomatous inflammation (32). Similarly,
an active model of crescentic glomerulonephnltis inWKY rats induced by immunization with GBM wasinhibited by blocking T cell activation. This wasachieved by administration of CTLA-4-Ig, whichblocks the CD28/B7 co-signal for T cell activation
during antigen presentation. Indeed, when adminis-
tration of CTLA-4-Ig was delayed until disease was
established, there was still some reduction in the
severity ofcrescent formation (33). In addition, the use
of monoclonal antibodies to deplete T cells has dem-onstrated the requirement for CD4� T cells in theinduction of glomerular injury and glomerular cres-cent formation in munine lupus nephnitis and rataccelerated anti-GBM glomerulonephnitis (34,35).
Disruption of Bowman’s capsule. The presence of
interstitial collagens within Bowman’s space is aprominent feature in the fibrous organization of cellu-lar crescents. This is generally thought to be the resultof interstitial fibroblasts entering Bowman’s space
Modulators of Crescentic Glomerulonephritis
2274 Volume 7 . Number 1 1 . 1996
through ruptured areas of Bowman’s capsule (6,7).Indeed, in rabbit anti-GBM glomerulonephnitis, colla-gen deposition occurs in the peniglomerular area inassociation with leukocyte infiltration before deposi-tion is seen within the glomerulus (36). However,interstitial collagens have been noted within glomer-ular crescents in human glomerulonephritls in the ab-
sence ofBowman’s-capsule rupture, indicating that res-
ident glomerular cells such as podocytes can produceinterstitial collagens under some circumstances (37).
Peniglomerular leukocytic inifitration is a commonfeature of aggressive forms of glomerulonephnitis andthere is evidence to implicate these cells in the disrup-tion of Bowman’s capsule. In rat anti-GBM glomeru-
lonephnitis, focal infiltrates of immune-activated T
cells and macrophages are invariably associated withBowman’s-capsule rupture. Indeed, the presence of Tcells within Bowman’s space is only apparent in thoseglomeruli with disruption of the capsule (20). Thesefindings suggest that Bowman’s capsule is damaged
through a delayed-type hypersensitivity mechanism,
consistent with studies demonstrating the T cell de-pendence of crescentic glomerulonephritis describedabove.
The association of peniglomerular leukocytes andBowman’s-capsule rupture raises the question ofwhether capsular damage is mediated by crescentcells or peniglomerular leukocytes. In rat anti-GBMglomerulonephnitis, 26 to 52% of glomeruli with nip-tuned Bowman’s capsule had no evidence of crescentformation, suggesting that peniglomerular-but notcrescent-cells are essential for Bowman’s-capsule
rupture (20). This observation suggests the intriguing
possibility that some crescents may develop second-
ary to Bowman’s-capsule rupture, allowing the entry
of macrophages, T cells, and fibroblasts into Bow-man’s space. Indeed, it has been proposed that migra-tion through tears in Bowman’s capsule is the majorroute of leukocyte entry into Bowman’s space duringcrescent formation (13).
Fibrocellular Crescents
Fibrocellular crescents are characterized by thepresence of fibroblasts and collagen deposition withinBowman’s space. Numerous macrophages are stillevident within Bowman’s space at this stage, whereasT cells are also seen in fibrocellular crescents. Both Tcells and fibroblasts are thought to enter Bowman’sspace from the peniglomerular area through gaps inBowman’s capsule. There is a gradual transition from
a fibrocellular to a fibrous crescent phenotype, whichinvolves the proliferation of fibroblasts and depositionof large amounts of collagen and other matrix mole-cules such as fibronectin. Fibroblast proliferation islikely to be driven by local production of growth fac-tons such as acidic and basic fibroblast growth factors
(FGF- 1 and FGF-2). Combined immunohistochemis-try and in situ hybridization studies have demon-strated FGF-receptor expression by fibroblast-like
cells within fibrocellular crescents in rat crescenticglomerulonephritis. In addition, FGF- 1 and FGF-2mRNA and protein is expressed by several cell types-parietal epithelial cells, macrophages, and fibro-blasts-within these crescents (38). Transforminggrowth factor j3 (TGF-13) is likely to play an importantrole in the deposition of collagen in Bowman’s space
(39). Indeed, the presence of active TGF-f3 in urine isassociated with glomerular scarring in crescentic gb-merubonephnitis in the rabbit (40).
Fibrous Crescents
Progressive collagen deposition within Bowman’s
space leads to the development of a relatively acellularmatrix structure akin to that seen in scar formation.
The gradual loss of macrophages, T cells, and fibro-blasts from Bowman’s space seen during the scarringprocess may be mediated by apoptosis (41). By thisstage, the gbomerular tuft is substantially compressed
with marked capillary obliteration and is relativelyacellubar. The fibrotic process can progress furtheruntil the remaining capillary tuft is completely oblit-erated, resulting in global glomerular sclerosis.
MODULATION OF CRESCENT FORMATION
Gbomerular crescent formation is an index of dis-
ease severity and as such usually requires aggressivetherapy. Although it is clear that cell-mediated immu-nity plays a key role in crescent formation, we are farfrom optimizing immunosuppressive therapies. Drugssuch as prednisobone and cyclophosphamide are po-
tent immunosuppressive agents, but their use is lim-ited by a range of side effects, which include the risk ofopportunistic infection. Therefore, we need to developdrugs that can inhibit specific aspects of the immuneresponse within the kidney without significant toxicity
or causing a state of general immunosuppnession.Such an approach depends upon gaining a detailedunderstanding of the mechanisms of disease patho-genesis. In this section, the role of the cytokines IL-iand TNF-a in crescent formation is described, followed
by a brief consideration of future therapeutic possibil-
ities for crescentic gbomerubonephnitis.
Cytokines IL-i and TNF-a
Interleukin- 1 and TNF-a are considered to be classic
proinflammatory cytokines. Although the two cyto-kines are structurally quite distinct and work throughseparate cell-surface receptors, they share a greatmany biological activities, which include: upregula-tion of leukocyte adhesion molecule expression; in-duction of cytokines (interleukins 1 , 2, 6 and 8,
TNF-a, and MCP- 1); expression of the inducible formof nitric oxide synthase; induction of metalboprotein-ases; and induction of fever and wasting syndromes
(42,43). A number of strategies for blocking the ac-tions of these cytokine have been developed. For ex-ample, IL- 1 activity can be blocked in vivo by neutral-
izing antibodies, a naturally occurring IL- 1 receptor
Atkins et al
Journal of the American Society of Nephrology 2275
antagonist (IL- 1 ra) that competes with both IL- 1 a and
13 isoforms for receptor binding, and soluble forms ofthe IL- 1 receptor. Similarly, TNF-a activity can beblocked by neutralizing antibodies and soluble formsofthe TNF-a receptors (42,43). Using these reagents, a
pathogenic role for IL- 1 and TNF-a has been demon-
strated in a number of animal models of inflammatory
disease. Although in vitro studies have identified func-
tional redundancy between IL- 1 and TNF-a, this has
yet to be established in animal models of disease.
IL-i in Crescentic Glomerulonephritis
Gbomerular IL- 1 production has been demonstratedin human and experimental crescentic gbomerubone-phnitis, with infiltrating macrophages implicated asthe main source of this cytokine (44-48). Administra-
tion of IL- 1 j3 exacerbates gbomerular injury during the
first 24 h of endotoxin-enhanced anti-GBM glomeru-
suppresses the induction ofgbomerular injury in some
models of anti-GBM disease (50-52). Blockade of IL-i
activity over a 2-wk period by constant administration
of the IL- 1 ra prevented a loss in renal function andinhibited crescent formation in spite of continued
moderate proteinunia in rat anti-GBM gbomerubone-phnitis (53). IL- 1 promotes both gbomerular, and par-
ticular interstitial, macrophage infiltration by upregu-
bating ICAM- 1 expression (5 1 ,54). In addition, IL-i
promotes glomerular cell proliferation, although
whether this is direct action has yet to be determined
(53).The role of IL- i in the progression of established
crescentic gbomerulonephnitis was examined by delay-ing IL- ira treatment until gbomerular crescent forma-
tion was already established. Infusion of IL- ira over
Days 7 to 2 1 of rat anti-GBM disease restored renal
function and prevented further crescent formation(55). Indeed, blockade of IL- 1 activity had a profoundeffect on the phenotype of crescents. In untreatedanimals, crescents seen at Day 7 were mostly of the
early epithelial phenotype, whereas they were virtually
all of the advanced or fibrocellular type by Day 2 i . In
contrast, those crescents still evident in rats receivingIL- ira treatment over Days 7 to 2 i were of a predom-
inantly early epithelial phenotype, demonstrating that
IL- i is important in macrophage accumulation within
Bowman’s space during the progression of early to
advanced and fibrocellular crescents.
TNF-a in Crescentic Glomerulonephritis
Glomerular production of TNF-a has also been de-scnibed in human and experimental crescentic gb-merulonephnitis (45,46,56-58). Blockade of endoge-nous TNF-a has been shown to suppress theinduction of gbomerular injury in rat anti-GBM gb-merubonephnitis (50,52). In addition, daily adminis-tration of anti-TNF-a anti-serum for 8 days, starting
from the time of injection of anti-GBM serum, inprimed rats caused a significant reduction in urinary
albumin excretion, gbomerular necrosis, and fibrindeposition. However, the consequence ofTNF-a block-ade on gbomerular macrophage accumulation was notdetermined and few crescents were seen in this dis-ease model (59). These findings have been confirmedand extended in a recent study demonstrating thepathogenic role of TNF-a in rat anti-GBM crescenticgbomerubonephnitis (60). In this study, TNF-a activitywas blocked by the daily administration of a solubledimenic form of the p55 chain of the Type I TNF-areceptor (TNFbp) from the time of anti-GBM serum
injection until rats were euthanized 10 days later.Compared with the saline control, TNFbp treatmentprevented a fall in renal function, produced a 39%reduction in proteinunia (P < 0.05 versus saline treat-ment) and almost abolished gbomerular crescent for-mation (4 ± i .4 versus 24 ± 2.8% crescents withTNFbp and saline treatments, respectively; P <
0.00 1 ). This suppression of crescentic gbomerubone-phnitis was the result of a marked inhibition of gb-
merubar and interstitial macrophage infiltration and a
reduction in gbomerular cell proliferation (60).Given that IL- i and TNF-a share many proinflam-
matory properties, it is important to determinewhether the inhibition of both cytokines will provide
an added benefit over blocking each individually. Thiswas addressed in rat crescentic anti-GBM gbomerubo-nephritis by treatment with IL- ira alone, TNFbpalone, or IL- ira plus TNFbp over Days 0 to 10. Eachtreatment prevented a boss of renal function and
produced a similar degree of suppression of protein-unia (27%, 39%, and 28%, respectively; all P < 0.05versus saline). Similarly, each treatment markedlyinhibited gbomerubar crescent formation (85%, 83%,and 92% reduction, respectively; all P < 0.00 1 versus
saline) and caused comparable reductions in gbomer-ular leukocyte infiltration and proliferation, gbomeru-
bar lesions, tubular atrophy, and interstitial fibrosis
(60). These results indicate that IL- i and TNF-a actthrough similar pathways in gbomerubonephnitis. One
possible common pathway of action is through thetranscription factor NF-kappaB. Both IL- i and TNF-aactive NF-kappaB in vitro and many of the geneswhose transcription is upregulated by IL- 1 and TNF-ahave NF-kappaB sites in their promoter regions (61-63). This is typified by the presence of NF-kappaBsites in the promoters of the genes encoding both IL-iand TNF-a (64,65). Whatever the common pathways of
IL- 1 and TNF-a action are, the results of this studysuggest that no added benefit will be gained by at-tempting to block both cytokines simultaneously inclinical studies of gbomerubonephnitis.
FUTURE THERAPEUTIC STRATEGIES IN CRESCENTICGLOMERULONEPHRITIS
There has been a dramatic increase in our under-standing of immune, inflammatory, and fibrotic dis-ease processes. One major benefit of this understand-ing has been the identification of common molecular
relatively few specific immunosuppressive drugs havebeen tested in animal models of gbomerubonephritisfeaturing crescent formation, there are many potentialtherapeutic targets in this disease as outlined in Table
Fibrin deposition within Bowman’s space is knownto facilitate crescent formation in animals models of
disease (14). However, current anticoagulant thera-
pies have been disappointing clinically, showing little
TABLE 1. Modulation of glomerular crescentformatlona
MODULATION POTENTIAL STRATEGY
Inhibit Fibrin Deposition Block extravascularcoagulation (Inhibit tissuefactor, administer TFPI)
Inhibit the synthesis, secretion,or receptor binding of IL-iand TNF-a
Block the action of molecules
chemotactic formacrophages (MCP-i andM-CSF) and I cells (RANTES,MCP-i)
Systemic depletion of I cellsby monoclonal antibodies
if any benefit in terms of renal function. Recent evi-dence has pointed to the activation of tissue factor asthe main mechanism of extravascular coagulation(66). Thus, strategies to inhibit tissue-factor activa-tion by neutralizing antibodies or recombinant tissue-factor pathway inhibitor (TFPI) may be effective in
crescentic gbomerubonephnitis (67-69).
Inhibiting the accumulation of macnophages and T
cells within Bowman’s space, indeed within the kidneyas a whole, is a clear therapeutic goal. As outlined inTable 1 , there are several levels at which mononuclearcell accumulation within the kidney can be blocked bytargeting chemotactic molecules, proinflammatory cy-
tokines, leukocyte adhesion molecules, and growth
factors driving local proliferation. Some of these ap-proaches have proven successful in models of cres-centic gbomerubonephnitis using agents such as mono-cbonal antibodies and recombinant receptors andreceptor antagonists (26,35,53,59). Having estab-lished the efficacy of such approaches, effort will be
put into seeking better ways of blocking these mech-
anisms in vivo. For example, local production of sobu-bbe cytokine receptors or receptor antagonists throughtargeted gene therapy is an attractive option, althoughmany technical difficulties remain to be overcome in
such as approach (70).
As systemic inhibition of mononuclear cell recruit-
ment to sites of inflammation may not be feasible on along-term basis, an alternative approach is to inhibitthe activation of macrophages and T cells that haveentered the kidney. A number of cytokines and cell-
surface glycoproteins are known to play important
roles in the activation of macrophages and T cells(Table 1 ; References 7 1 through 73). The importanceof one such T cell costimulating molecule, CD28, increscent formation has been established in a ratmodel of autoimmune gbomerulonephnitis (33). Analternative means of inhibiting mononuclear cell acti-vation is to block the intracellular signals generated
through cell-surface activation. Although this is atechnically difficult proposition, it is very attractivebecause activation of transcription factors, such asNF-kappaB and NF-ATp, play a crucial role in macro-
phage and T cell activation and in coordinating manycomponents of the inflammatory response (74-77).Indeed, one of the mechanisms by which corticoste-roids exert their anti-inflammatory action is through
blockage of NF-kappaB activation (78). Thus, specificinhibitors of NF-kappaB activation would be expected
to be potent immunosuppressants without many ofthe side-effects of corticosteroids.
As the entry of fibroblasts into Bowman’s spacemarks the point ofirreversibility for cellular crescents,targeting of the fibroblast response could also be ofbenefit. This could take the form ofbbocking the actionof growth factors that stimulate fibroblast prolifera-tion within the crescent (FGF, PDGF) or growth factorsthat promote matrix deposition (TGF-�3). The ability ofdecorin treatment to inhibit matrix deposition in ex-penimental gbomerubonephritis suggests that local de-
Atkins et al
Journal of the American Society of Nephrology 2277
livery of deconin-expressing plasmids into the kidney
could provide substantial protection against progres-sive fibrosis, including fibrous organization of cellular
crescents (79).
SUMMARY
The importance of cellular immune mechanisms in
the progression of glomerulonephnitis, including cres-
centic disease, has become increasingly evident. Therapid advances in our understanding of the steps
involved in the induction and execution of the cellular
immune response has led to the development of avariety of highly specific immunosuppressive agents.
In particular, the impressive ability of cytokine block-
ade to suppress experimental crescentic gbomerubone-
phnitis has opened the way for clinical trials using
agents such as IL- ira or the TNFbp as adjuncts to
current therapies.
ACKNOWLEDGMENTS
This study was funded by NatIonal Health & Medical ResearchCouncil Grant 950,9 1 2 and by the Baxter Extramural Grant Program.
REFERENCES
1 . Kerr PG, Lan LW, Atkins RC. Rapidly progressive gb-merulonephritis. In: Schrier RW, Gottschalk CW, eds.Diseases of the Kidney, 6th ed. Boston: Little, Brown;1996:in press.
2. Morrin PA, Hinglais N, Nabarra B, Kreis H: Rapidlyprogressive gbomerulonephritis. A clinical and pathologicstudy. Am J Med 1978;65:446-460.
6. Morel-Maroger Striker L, Killen PD, Chi E, Striker GE:The composition ofglomerubosclerosis. I. Studies in focalsclerosis , crescentic gbomerubonephritis, and mem-branoproliferative gbomerubonephnitis. Lab Invest 1984;51: 18 1-192.
7. Silva FG, Hoyer JR. Pirani CL: Sequential studies of gb-merubar crescent formation in rats with antigbomerularbasement membrane-induced gbomerubonephnitis and therole of coagulation factors. Lab Invest 1984;51:404-415.
8. Monita T, Suzuki Y, ChurgJ: Structure and development ofthe gbomerular crescent. Am J Pathol 1973;72:349-368.
9. Atkins RC, Holdsworth SR, Glasgow EF, Matthews FE:The macrophage in human rapidly progressive gbomeru-bonephritis. Lancet 1976; 1:830-832.
10. Cattell V, Jamieson SW: The origin of gbomerular cres-cents in experimental nephrotoxic serum nephritis inthe rabbit. Lab Invest 1978;39:584-590.
1 1 . Hancock WW, Atkins RC: Cellular composition of cres-cents In human rapidly progressive glomerubonephritisidentified using monocbonab antibodies. Am J Nephrob1984;4: 177-181.
12. Magil AB: Histogenesis of gbomerular crescents. Immu-nohistochemical demonstration of cytokeratin in cres-cent cells. Am J Pathol 1985;120:222-229.
13. Boucher A, Droz D, Adafer E, Noel LH: Relationshipbetween the integrity of Bowman’s capsule and thecomposition of cellular crescents in human crescenticgbomerubonephritis. Lab Invest 1987;56:526-533.
14. Tipping PG, Thomson NM, Holdsworth SR: A compari-son of fibrinolytic and defibrinating agents in establishedexperimental gbomerubonephritis. Br J Exp Pathol 1986;
merular fibrin deposition in experimental gbomerubone-phritis in the rabbit. J Clin Invest 1985;76: 1367-1374.
16. Goyal M, Wiggins R: Fibronectin mRNA and proteinaccumulation, distribution, and breakdown in rabbitanti-gbomerular basement membrane disease. J Am SocNephrol 1991;1: 1334-1342.
18. Downer G, Phan SH, Wiggins RC: Analysis of renalfibrosis in a rabbit model of crescentic nephritis. J ClinInvest 1988;82:998-1006.
19. Bagchus WM, Hoedemaeker PJ, Rozing J, Bakker WW:Gbomerubonephritls induced by monocbonab anti-Thy 1.1antibodies. A sequential histological and ultrastructuralstudy in the rat. Lab Invest 1986;55:680-687.
20. Lan 1W, Nikolic-Paterson DJ, Atkins RC: Involvement ofactivated perigbomerular leukocytes in the rupture ofBowman’s capsule and gbomerubar crescent progressionin experimental gbomerulonephritis. Lab Invest 1992;67:743-751.
2 1 . Rovin BH, Rumancik M, Tan L, Dickerson J: Gbomeru-bar expression of monocyte chemoattractant protein- 1 inexperimental and human gbomerubonephritis. Lab Invest1994;71 :536-542.
23. Bloom PD, Florquin 5, Singer GG, Brennan DC, KelleyVR: Colony stimulating factor- 1 in the induction of lupusnephnitis. Kidney Int 1993;43: 1000-1009.
24. Lan HY, Mu W, Meinhard A, et at.: Macrophage migra-tion inhibitory factor (MIF)-a previously unrecognisedkidney-derived cytokine-which participates in localmacrophage accumulation and proliferation in the pro-gression of rat anti-GBM gbomerubonephritis [Abstracti.Kidney Int 1996, in press.
25. Nikolic-Paterson DJ, Main 1W, Lan HY, Hill PA, AtkinsRC: Adhesion molecules in gbomerulonephritis. SpringerSemin Immunopathol 1994; 16:3-22.
26. Nishikawa K, Guo YJ, Miyasaka M, et at.: Antibodies tointercellular adhesion molecule 1 /lymphocyte function-associated antigen 1 prevent crescent formation in ratautoimmune gbomerubonephritis. J Exp Med 1993;177:667-677.
27. LesbeyJ, Hyman R, Kincade PW: CD44 and its interactionwith extracellular matrix. Adv hnrnunol 1993;54:27l-335.
28. Zhao J, Lan 1W, Atkins RC, et at.: CD44 expression inrat anti-GBM gbomerubonephritis (Abstracti. Kidney mt1996, in press.
29. Nishikawa K, Andres G, Bhan AK, et al. : Hyaluronate isa component of crescents in rat autoimmune gbomeru-bonephritis. Lab Invest 1993;68: 146-153.
30. Hooke DH, Gee DC, Atkins RC: Leukocyte analysisusing monocbonal antibodies in human gbomerubone-phritis. Kidney Int 1987;3 1:964-972.
3 1 . Li HL, Hancock WW, Dowbing JP, Atkins RC: Activated(IL-2R+ ) intragbomerular mononuclear cells in crescen-tic gbomerubonephritis. Kidney Int 199 1 ;39:793-798.
32. Rennke HG, Klein PS, Sandstrom DJ, Mendrick DL:Cell-mediated immune injury in the kidney: Acute ne-phritis induced in the rat by azobenzenearsonate. Kid-ney mt 1994;45:1044-1056.
33. Nishikawa K, Linsley PS, Collins AS, Stamenkovic I,McCluskey RT, Andres G: Effect of CTLA-4 chimericprotein on rat autoimmune anti-glomerular basementmembrane gbomerubonephritis. Eur J Immunol 1994;24:1249-1254.
34. Carteron NL, Schimenti CL, Wofsy D: Treatment ofmurine lupus with F(ab’)2 fragments of monocbonalantibody to L3T4. Suppression of autoimmunity doesnot depend on T helper cell depletion. J Immunol 1989;142:1470-1475.
crescent formation. Kidney Int 1994;46:69-78.36. Merritt SE, Killen PD, Phan SH, Wiggins RC: Analysis of
alpha 1 (I) procollagen alpha 1 (IV) collagen, and beta-actin mRNA in glomerulus and cortex of rabbits withexperimental anti-gbomerular basement membrane dis-ease. Evidence for early extragbomerular collagen bio-synthesis. Lab Invest 1990;63:762-769.
37. Buyukbabani N, Droz D: Distribution ofthe extracellularmatrix components in human gbomerubar lesions.J Pathol 1994:172:199-207.
38. Ng Y, Nikolic-Paterson DJ, Mu W, Atkins RC, Lan LW:Expression of basic fibroblast growth factor and itsreceptor in the progression of rat crescentic glomerulo-nephritis. Nephrobogy 1995; 1:569-575.
39. Border WA, Noble NA: Transforming growth factor j3 intissue fibrosis. N Engl J Med 1994;331:1286-1292.
40. Colmbra T, Wiggins R, Noh JW, Merritt 5, Phan SH:Transforming growth factor-n production in anti-gbomerular basement membrane disease in the rabbit.Am J Pathol 1991;l38:223-234.
4 1 . Desmouliere A, Redard M, Darby I, Gabbiani G: Apopto-sis mediates the decrease in cellularity during the tran-sition between granulation tissue and scar. Am J Pathob1995; 146:55-66.
43. Dinarebbo CA: Interleukin- 1 and tumor necrosis factor:Effector cytokines In autoimmune diseases. Semin Im-munol 1992;4:133-145.
44. Matsumoto K, Dowling J, Atkins RC: Production ofinterleukin 1 in gbomerular cell cultures from patientswith rapidly progressive crescentic gbomerulonephritis.Am J Nephrol 1988;8:463-470.
45. Noronha IL, Kruger C, Andrassy K, Ritz E, Waldherr R:In situ production of TNF-alpha, IL- 1 beta and IL-2R inANCA-positive gbomerubonephritis. Kidney hit 1993;43:682-692.
46. Yoshioka K, Takemura T, Murakami K, et at.: In situexpression of cytokines In IgA nephritis. Kidney Int1993;44:825-833.
47. Boswebl JM, Yui MA, Endres 5, Burt DW, Kelley VE:Novel and enhanced IL- 1 gene expression in autoim-mune mice with lupus. J Immunol 1988; 141:118-124.
48. Matsumoto K: Production ofinterleukin- 1 by gbomerularmacrophages In nephrotoxic serum nephritis. Am JNephrol 1990; 10:502-506.
49. Tomosugi NI, Cashman SJ, Hay H, et al: Modulation ofantibody-mediated glomerular Injury in vivo by bacteriallipopolysaccharide, tumor necrosis factor, and IL- 1.J Immunol 1989;142:3083-3090.
50. Mulligan MS, Johnson KJ, Todd HF 3rd, et at.: Require-ments for beukocyte adhesion molecules in nephrotoxicnephritis. J Chin Invest 1993;91:577-587.
52. Karkar AM, Tam FWK, Steinkasserer A, et at.: Modula-tion of antibody-mediated glomerular injury in vivo byIL- ira, soluble IL- 1 receptor, and soluble TNF receptor.Kidney Int 1995;48:1738-1746.
53. Lan LW, Nikolic-Paterson DJ, Zarama M, Vannice JL,Atkins RC: Suppression of experimental crescentic gb-merulonephritis by the interleukin- 1 receptor antago-nist. Kidney Int 1993;43:479-485.
54. Nikobic-Paterson DJ, Lan LW, Hifi PA, Vannice JL,Atkins RC: Suppression of experimental gbomerulone-phritis by the interleukin- 1 receptor antagonist: Inhibi-tion of intercellular adhesion molecule- 1 expression. JAm Soc Nephrol 1994;4:1695-1700.
55. Lan LW, Nikolic-Paterson DJ, Mu W, Vannice JL, AtkinsRC: Interleukin- 1 receptor antagonist halts the progres-sion of established crescentic glomerubonephritis in therat. Kidney Int 1995;47: 1303-1309.
56. Boswell JM, Yui MA, Burt DW, Kelley VE: Increasedtumor necrosis factor and IL-i beta gene expression inthe kidneys of mice with lupus nephritis. J Immunol1988; 141:3050-3054.
57. Hruby ZW, Lowry HP: Mechanisms of glomerular injuryin experimental immune nephritis. I. Tumor necrosisfactor is released by renal gbomeruli of nephritic rats.Arch Immunol Ther Exp (Warsz) 199139:563-574.
58. Tipping PG, Leong TW, Holdsworth SR: Tumor necrosisfactor production by gbomerular macrophages in anti-gbomerular basement membrane gbomerulonephritis inrabbits. Lab Invest 199 1;65:272-279.
60. Lan LW, Song Q’ Nikolic-Paterson DJ, et at.: Functionalblocking of TNFa in rat crescentic gbomerubonephritisand comparison with IL- 1 blockade [Abstract]. KidneyInt 1996, in press.
6 1 . Beg A.A, Finco TS, Nantermet PV, Baldwin AS Jr: Tumornecrosis factor and interleukin- 1 lead to phosphorylationand loss of I kappa B alpha: A mechanism for NV-kappa Bactivation. Mob Cell Blob 1993;13:3301-3310.
62. Chen CC, Manning AM: Transcriptional regulation ofendothellal cell adhesion molecules: A dominant role forNF-kappa B. Agents Actions Suppl 1995;47: 13�-141.
63. Kopp EB, Ghosh 5: NF-kappa B and rel proteins ininnate immunity. Adv Immunol l995;58: 1-27.
64. Hlscott J, Marois J, Garoufabis J, et at.: Characteriza-tion of a functional NF-kappa B site in the humaninterbeukin 1 beta promoter: Evidence for a positiveautoregulatory loop. Mob Cell Blob 1993; 13:6231-6240.
65. Trede NS, Tsytsykova AV, Chatila T, Goldfeld AE, GehaRS: Transcriptional activation of the human TNF-alphapromoter by superantigen in human monocytic cells:Role of NF-kappa B. J Immunol 1995; 155:902-908.
66. RufW, Edglngton TS: Structural biology oftissue factor,the initiator of thrombogenesis In vivo. FASEB J 1994;8:385-390.
67. Levi M, ten Cate H, Bauer KA, et a!.: Inhibition of endo-toxin-induced activation of coagulation and fibri.nolysls bypento,dfylllne or by a monoclonal anti-tissue factor anti-body in chimpanzees. J Clin Invest 1994;93: 114-120.
68. Erblch J, Tipping P. Holdsworth: Inhibition of tissuefactor (TF) reduces renal injury and gbomerular fibrindeposition in crescentic gbomerubonephritis (GN) [ab-stracti. Kidney Int, in press.
72. Jenkins MX, Johnson JG: Molecules involved in T-cellcostimubation. Curr Opin Immunol 1993;5:36 1-377.
73. June CH, Bluestone JA, Nadber LM, Thompson CB: TheB7 and CD28 receptor families. Immunol Today 1994;15:321-33 1.
74. Chen F, Sun SC, Kuh DC, Gaydos LI, Demers LM:Essential role of NF-kappa B activation in silica-inducedinflammatory mediator production in macrophages. Bio-chem Biophys Res Commun 1995;214:985-992.
75. Kopp EB, Ghosh 5: NF-kappa B and rel proteins ininnate Immunity. Adv Immunol 1995;58: 1-27.
76. Northrop JP, Ho SN, Chen L: NF-AT components definea family of transcription factors targeted in T-cebb activa-tion. Nature (Lond) 1994;369:497-502.
77. Rao A: NF-ATp: A transcription factor required for theco-ordinate induction of several cytokine genes. Immu-nob Today 1994;15:274-28l.
78. Auphan N, DiDonato JA, Rosette C, Helmberg A, KaninM: Immunosuppression by glucocorticoids: Inhibition ofNF-kappa B activity through induction of I kappa Bsynthesis. Science 1995;270:286-290.