26
Module 2: Respiratory Anatomy
Module 2: Respiratory Anatomy
DisclaimerThis material is intended for use by trained family members and caregivers of children with tracheostomies who are patients at the Alberta Children’s Hospital. Although reasonable efforts were made to confirm the accuracy of the information, Alberta Health Services does not make any representation or warranty, express, implied or statutory, as to the accuracy, reliability, completeness, applicability or fitness for a particular purpose of such information. This material is not a substitute for the advice of a qualified health professional, so please seek medical advice from an appropriate health professional for questions regarding the care and treatment of any patient. Alberta Health Services expressly disclaims all liability for the use of these materials, and for any claims, actions, demands or suits arising from such use.
2
• A basic introduction to the normal respiratory system
• The respiratory system is the pathway where air enters and leaves the body, allowing oxygen from the air to absorb into the lungs and then to the rest of the body
• This system also allows the carbon dioxide from the blood to be breathed out as a by-product of gas exchange
Respiratory Anatomy6/1/2017
3
Children’s Home Care Edmonton Zone 2016, Used with Permission
Normal Respiratory Anatomy6/1/2017
4
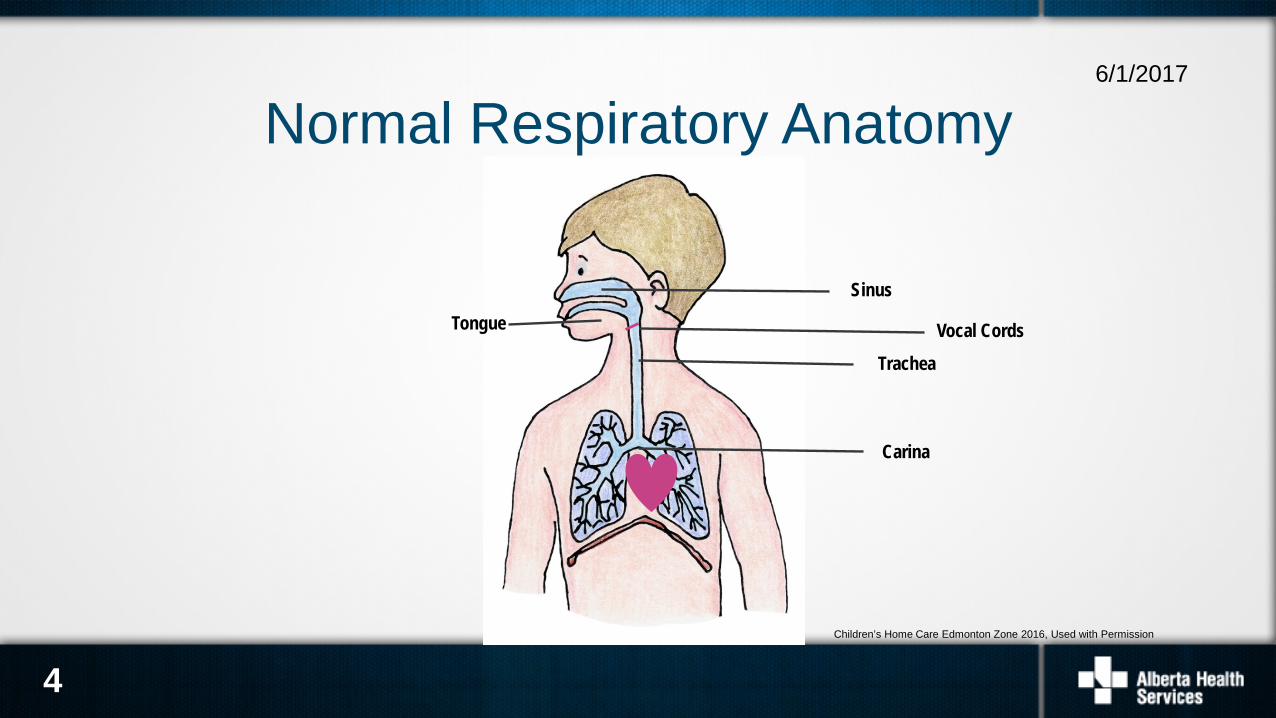
Tongue
Sinus
Vocal Cords
Carina
Trachea
Children’s Home Care Edmonton Zone 2016, Used with Permission
• Respiration, the process of breathing, is how we move air into our bodies by inhaling to breathe in oxygen (O2) that we need for body function and exhaling to breathe out carbon dioxide (CO2) as a waste gas
• The air we breathe in travels through the mouth and nose via the pharynx and larynx
• The air travels through the vocal cords, through our airways, and into the lungs
Breathing6/1/2017
5
• We normally breathe without thinking about it because breathing is controlled by the respiratory centre at the base of the brain
• This respiratory centre monitors the oxygen and carbon dioxide levels in the blood, which controls our respiratory rate and effort
Breathing6/1/2017
6
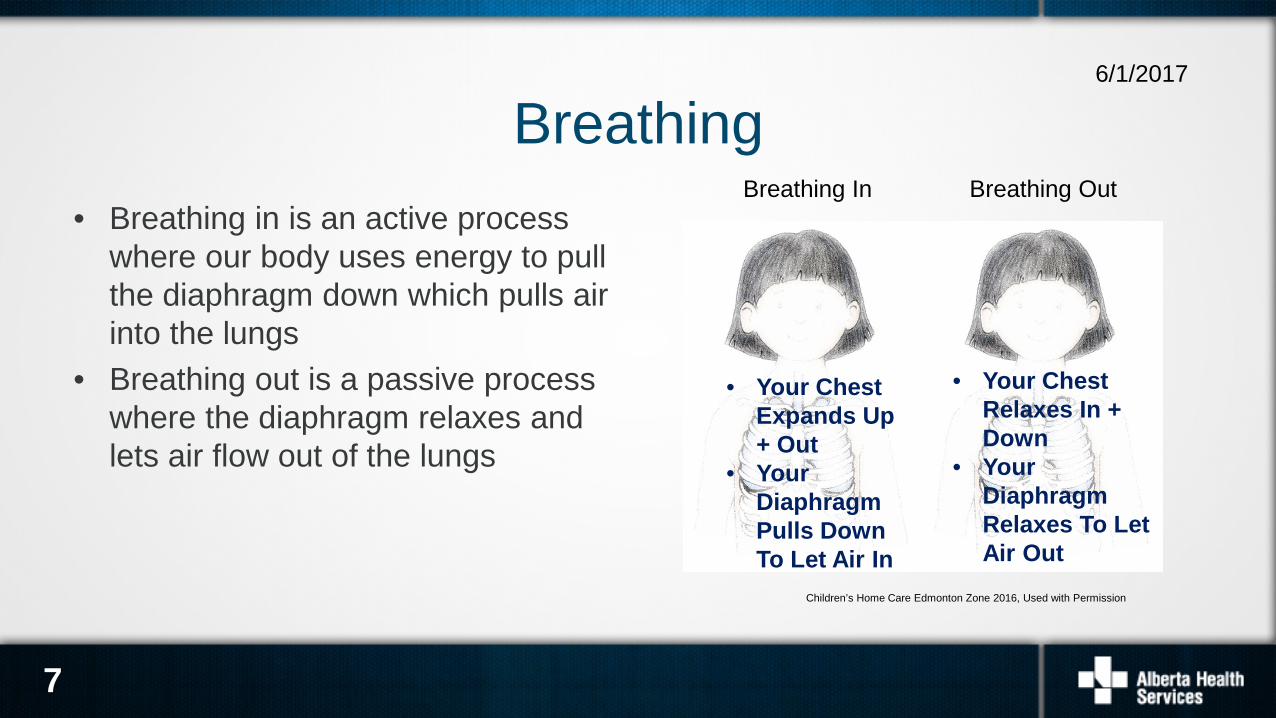
• Breathing in is an active process where our body uses energy to pull the diaphragm down which pulls air into the lungs
• Breathing out is a passive process where the diaphragm relaxes and lets air flow out of the lungs
Breathing6/1/2017
7
Breathing In Breathing Out
Children’s Home Care Edmonton Zone 2016, Used with Permission
• Your Chest Expands Up + Out
• Your Diaphragm Pulls Down To Let Air In
• Your Chest Relaxes In + Down
• Your Diaphragm Relaxes To Let Air Out

• Breathing in through the nose filters, warms, and humidifies the air from the environment as it passes through the different regions of the pharynx
• Mouth breathing does not provide as much humidity as breathing through the nose does
• The natural ability to filter, warm, and humidify air is lost when a trach tube is in place
Breathing6/1/2017
8
Children’s Home Care Edmonton Zone 2016, Used with Permission
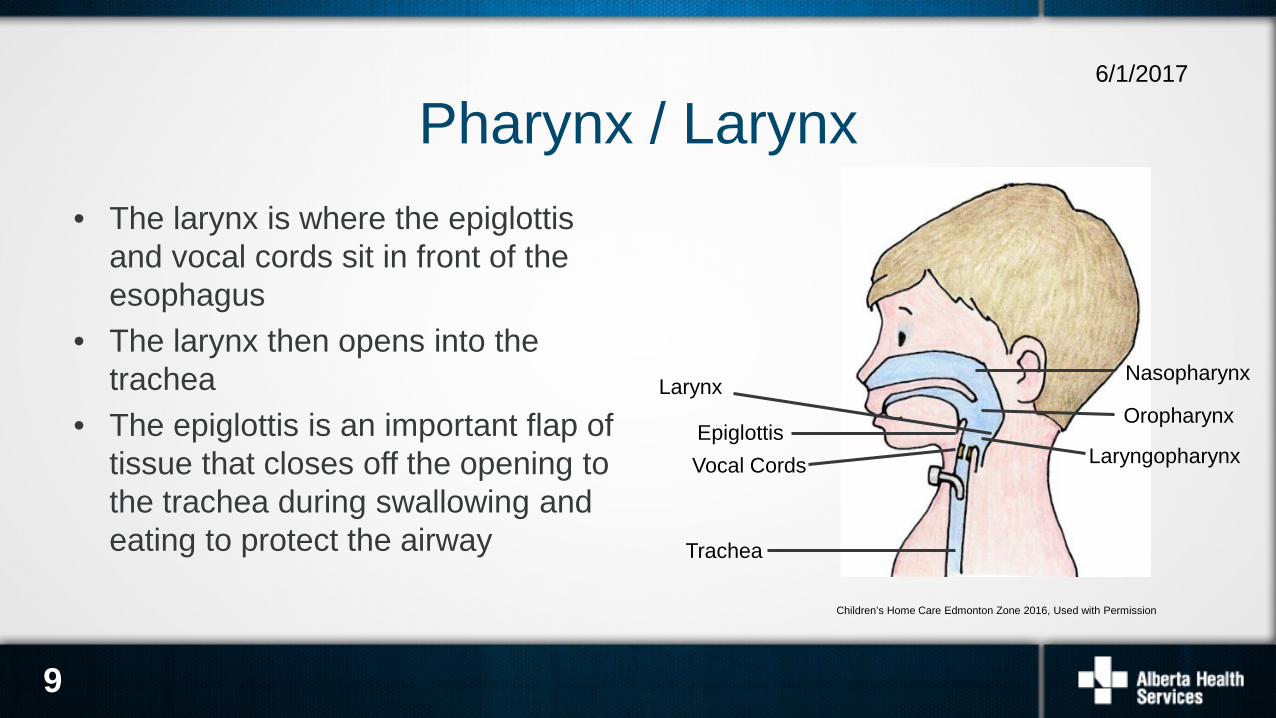
• The larynx is where the epiglottis and vocal cords sit in front of the esophagus
• The larynx then opens into the trachea
• The epiglottis is an important flap of tissue that closes off the opening to the trachea during swallowing and eating to protect the airway
Pharynx / Larynx6/1/2017
9
Children’s Home Care Edmonton Zone 2016, Used with Permission
Larynx
EpiglottisVocal Cords
Oropharynx
Nasopharynx
Laryngopharynx
Trachea
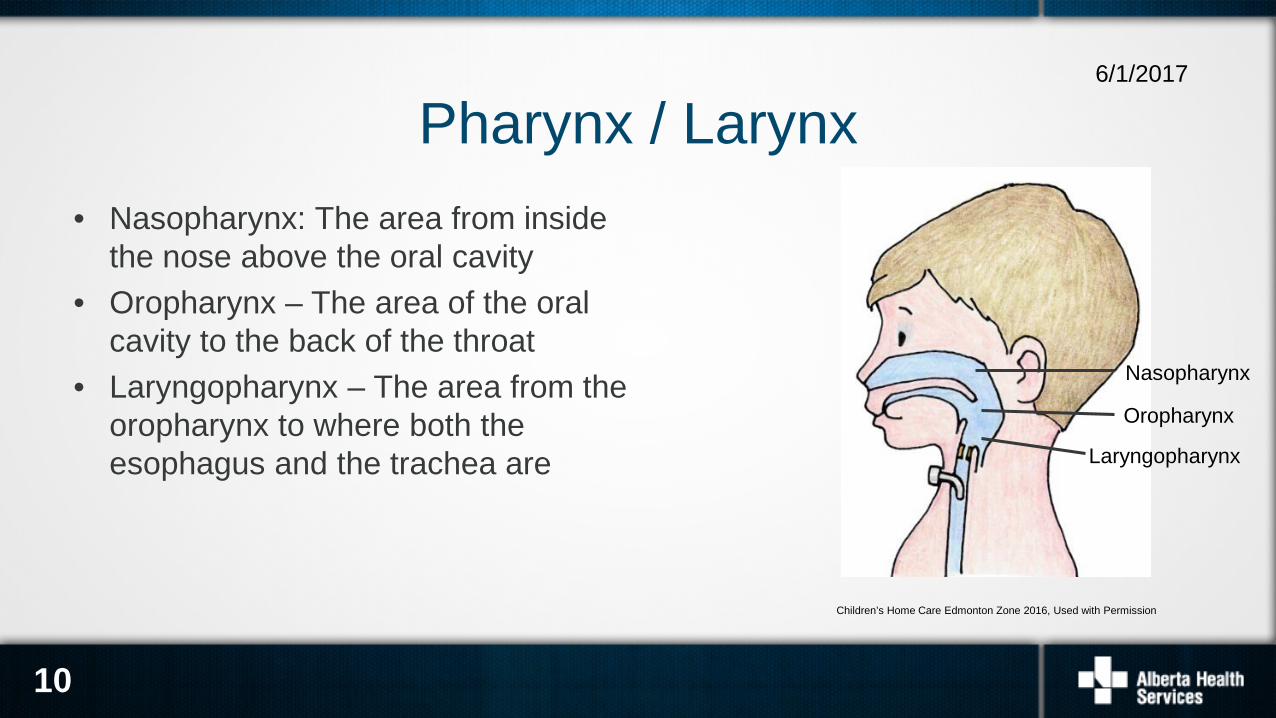
• Nasopharynx: The area from inside the nose above the oral cavity
• Oropharynx – The area of the oral cavity to the back of the throat
• Laryngopharynx – The area from the oropharynx to where both the esophagus and the trachea are
Pharynx / Larynx6/1/2017
10
Children’s Home Care Edmonton Zone 2016, Used with Permission
Oropharynx
Nasopharynx
Laryngopharynx
• Vocal cords are housed in the larynx• While breathing in – the cords are open to allow air to pass through• The vocal cords close together to create speech on breathing out• The vocal cords also close to protect the airway during eating and
drinking
Vocal Cords6/1/2017
11
12
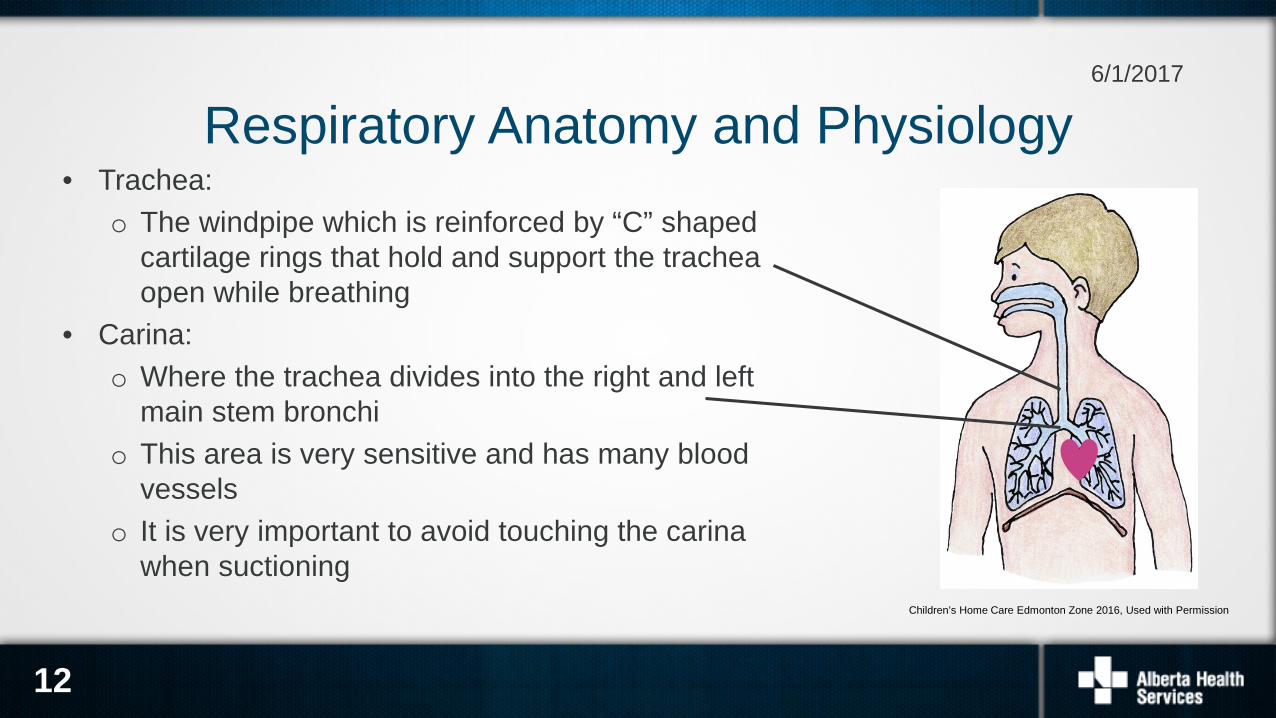
Respiratory Anatomy and Physiology• Trachea:
o The windpipe which is reinforced by “C” shaped cartilage rings that hold and support the trachea open while breathing
• Carina:o Where the trachea divides into the right and left
main stem bronchio This area is very sensitive and has many blood
vesselso It is very important to avoid touching the carina
when suctioning
6/1/2017
Children’s Home Care Edmonton Zone 2016, Used with Permission
13
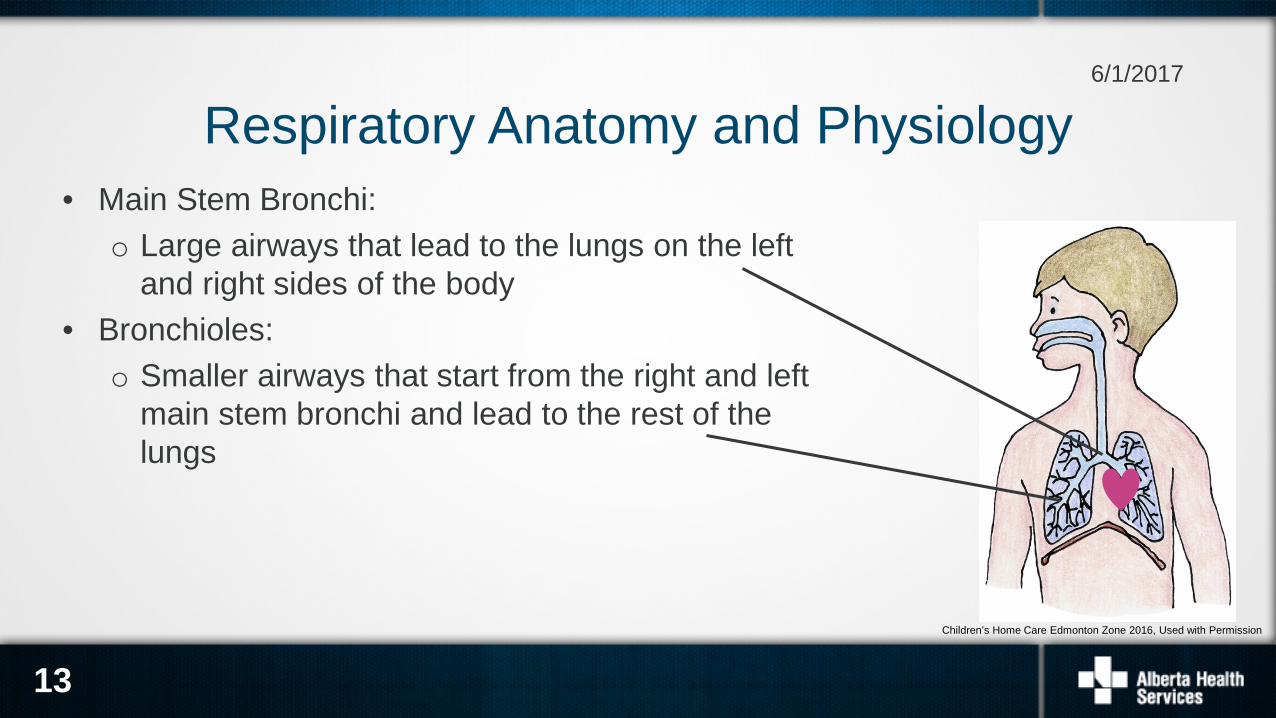
Respiratory Anatomy and Physiology• Main Stem Bronchi:
o Large airways that lead to the lungs on the left and right sides of the body
• Bronchioles:o Smaller airways that start from the right and left
main stem bronchi and lead to the rest of the lungs
6/1/2017
Children’s Home Care Edmonton Zone 2016, Used with Permission

14
Respiratory Anatomy and Physiology• Alveoli and capillaries:
o Where gas exchange happenso Oxygen from the alveoli goes into the capillaries into our blood stream
and carbon dioxide moves from the capillaries into the alveoli allowing us to breathe it out
• Mucous glands:o Glands throughout our airways and lungs that produce mucus (secretions)
to provide moisture and humidity and to help keep our lungs protected from debris
6/1/2017
15
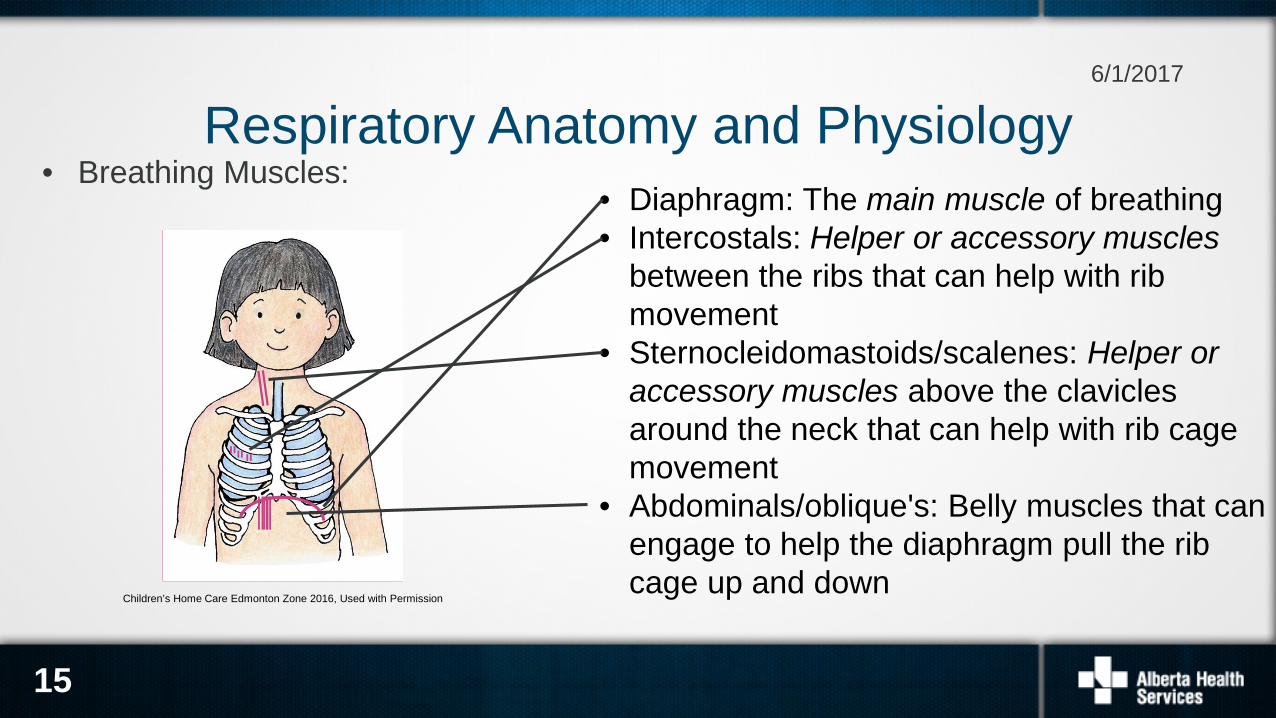
Respiratory Anatomy and Physiology• Breathing Muscles:
6/1/2017
• Diaphragm: The main muscle of breathing• Intercostals: Helper or accessory muscles
between the ribs that can help with rib movement
• Sternocleidomastoids/scalenes: Helper or accessory muscles above the clavicles around the neck that can help with rib cage movement
• Abdominals/oblique's: Belly muscles that can engage to help the diaphragm pull the rib cage up and down
Children’s Home Care Edmonton Zone 2016, Used with Permission
16
• Fetal respiratory organs develop while a baby is in the womb• Respiratory organs will continue to grow after a baby is born• As you grow, your lung volume increases as your lungs get bigger
Respiratory Development6/1/2017
There are many differences in our airways as we age from a baby to an adult:
Anatomy:• Infant tongues are larger in relation to their mouths than adults• Infant airways are smaller and more collapsible than adults• The infant epiglottis is larger and floppier than an adult’s• The infant trachea is narrower and floppier than an adult trachea
Airway Differences from Adult to Child6/1/2017
17
18
There are many differences in our airways as we age from a baby to an adult:
How we breathe: • Infants mostly breathe through their nose while older children and adults can
breathe through their nose and/or their mouth• Infants can become distressed if they are trying to breathe through a nose
that is clogged with mucus
Airway Differences6/1/2017
19
How we cope with increased respiratory effort:• Babies and children have very little respiratory reserve and will tire more
quickly than adults when in respiratory distress• Babies and children will use their accessory muscles earlier than adults when
in respiratory distress
Airway Differences6/1/2017
20
How our lungs work:• Babies have higher compliance in their lungs than adults do – this means
their lungs have the ability for more stretch and expansion when more work of breathing is occurring, which can lead to collapse easier
• Babies and children have much smaller lung sizes than adults to, which means they have less volume for gas exchange
Airway Differences6/1/2017
21
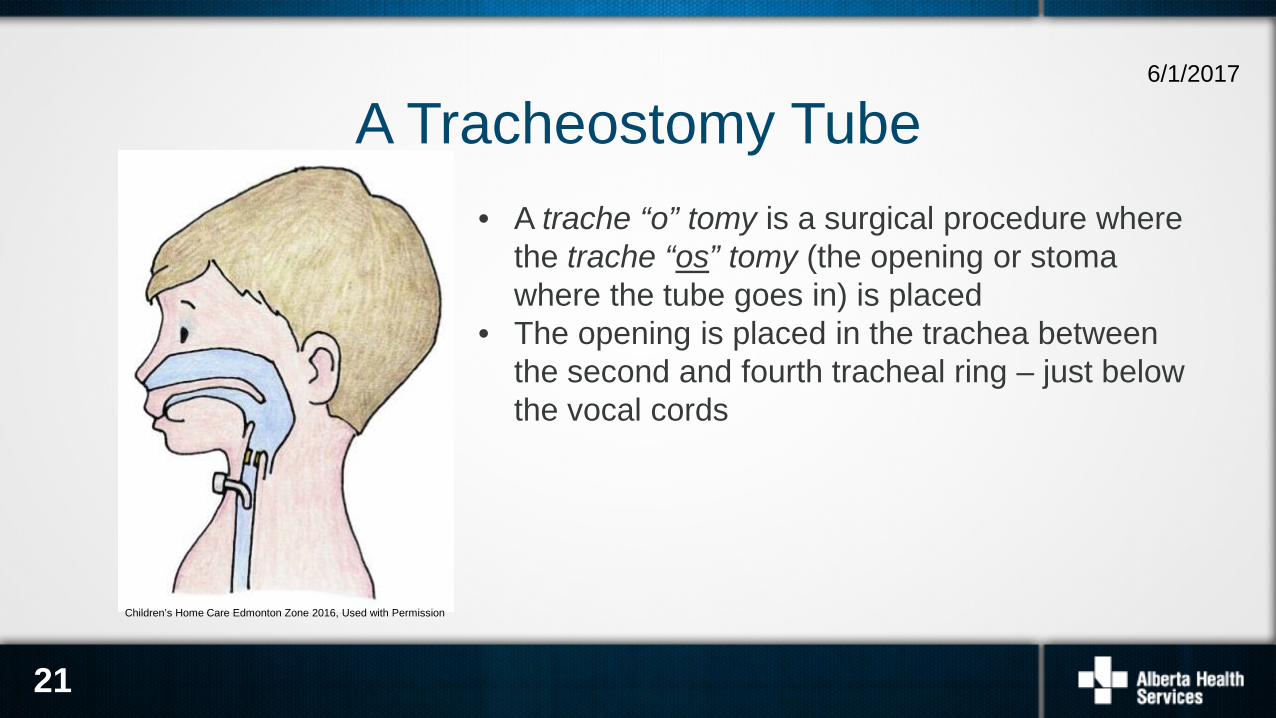
• A trache “o” tomy is a surgical procedure where the trache “os” tomy (the opening or stoma where the tube goes in) is placed
• The opening is placed in the trachea between the second and fourth tracheal ring – just below the vocal cords
A Tracheostomy Tube6/1/2017
Children’s Home Care Edmonton Zone 2016, Used with Permission
22
There are many reasons for a child to have a trach tube in place:• To relieve or bypass obstructions in the upper anatomy
o Examples: Pierre Robin Sequence, injury to the airway, vocal cord damage
• To provide long term mechanical ventilation and breathing supporto Examples: Spinal Muscular Atrophy, chronic lung disease
• To help with clearing their secretions effectivelyo Examples: Cerebral Palsy
Indications for a Tracheostomy6/1/2017
• Every child is very different as to why they have a tracheostomy tube• It is very important for you to understand why your child has a trach and the
anatomy of your child’s airway in order to understand what your child’s needs areo Some children have trachs and can breathe on their owno Some children have trachs and can not breathe on their own and need help with
their breathingo Some children have trachs but can also move air through their mouths and
noses o Some children cannot breathe any other way except through their trach
Why does your child have a trach?6/1/2017
23
24
• Irritation, inflammation or infection of the interior trachea (Tracheitis)• Irritation, inflammation or infection of the stoma site• Abnormal development of scar tissue in or around the stoma site (Granulomas)• Softening of the tracheal wall leading to collapse on inspiration (Tracheomalacia)• Permanent narrowing of the interior tracheal wall (Tracheal Stenosis)
Structural Complications of Tracheostomy6/1/2017
25
Other Potential Complications with Tracheostomy• Infection in the lungs• Bleeding around the stoma site or due to trauma from suctioning • Breathing in food or fluid which goes into the lungs – this is called aspiration
6/1/2017
26
Complications with a trach that require immediate interventions are:• Airway Obstruction: This can occur because of secretions or a mucus plug, an
improperly placed tube, an object, or aspiration of food or fluid• Dislodgement: This can occur because of loose or damaged ties, coughing, movement,
‘busy’ hands• Ensuring trach ties are securely tied can reduce the risk of dislodgement
• Good techniques of care and assessment will help decrease the risk of these events occurring
• Decisive quick action when one of these events occurs is key to prevent serious outcomes
• You will be prepared to deal with these events if they do occur
Emergency Complications6/1/2017

















