Molecular Advances in the Diagnosis and Classification of Myeloproliferative Neoplasms International Society for Laboratory Hematology Chicago, IL – May 2015 Adam Bagg, MD Director, Hematology Medical Director, Clinical Cancer Cytogenetics Interim Director, Hematopathology University of Pennsylvania
Transcript
Molecular Advances in the Diagnosis and Classification ofMyeloproliferative Neoplasms
International Society for Laboratory HematologyChicago, IL – May 2015
Adam Bagg, MDDirector, Hematology
Medical Director, Clinical Cancer CytogeneticsInterim Director, Hematopathology
University of Pennsylvania
Major flavors of myeloid neoplasms
AML
MPN
MDS
MPN/MDS
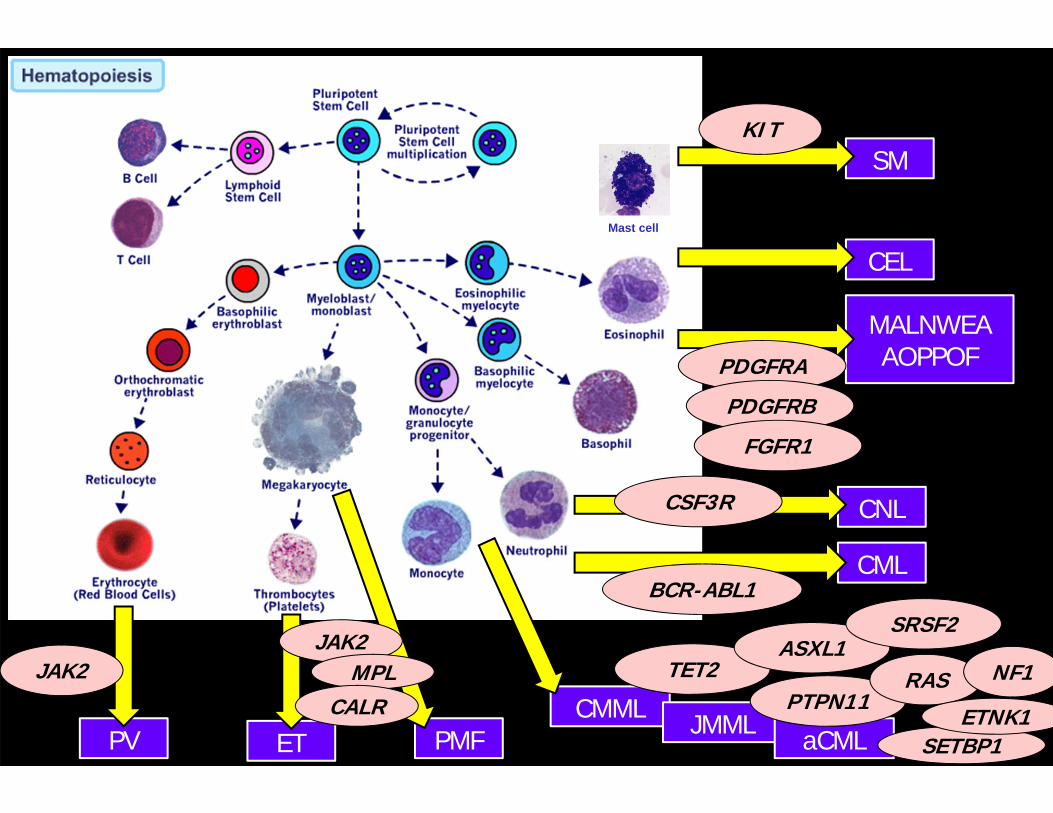
MALNWEAAOPPOF
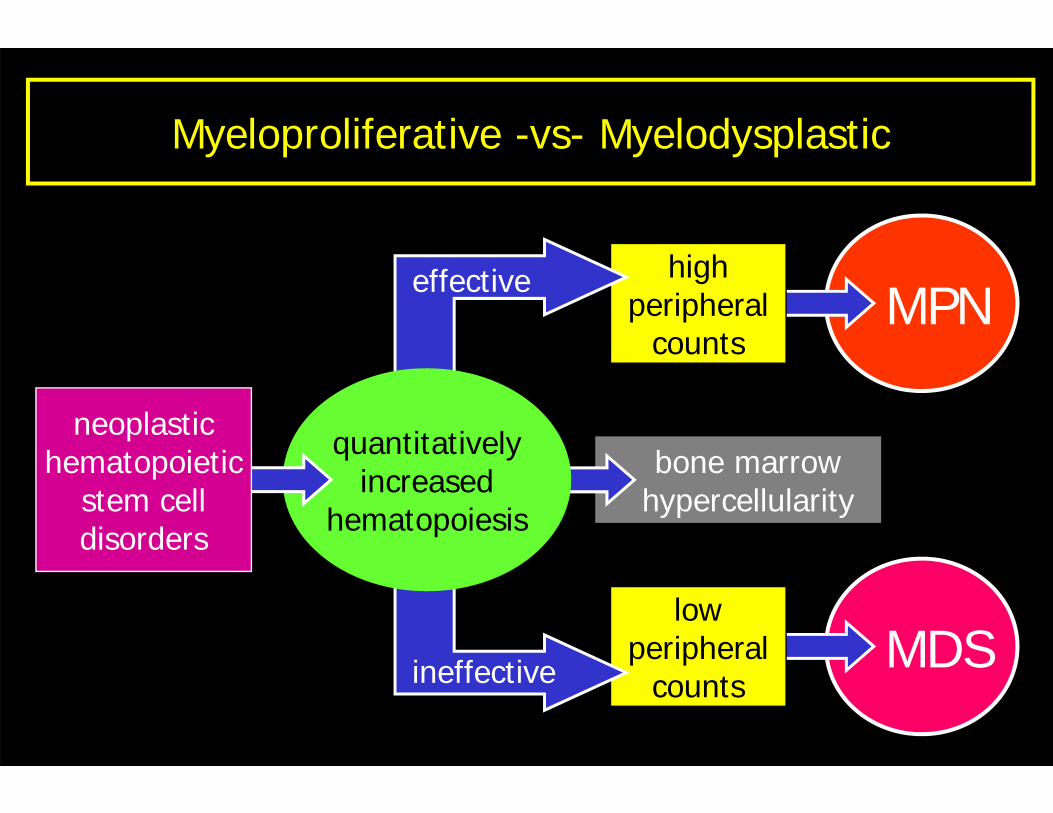
Myeloproliferative -vs- Myelodysplastic
bone marrowhypercellularity
MPNhigh
peripheralcounts
MDSlow
peripheralcounts
quantitativelyincreased
hematopoiesis
effective
ineffective
neoplastichematopoietic
stem celldisorders
CEL Mastocytosis
UnclassifiableCNL
Flavors of myeloproliferative neoplasms
CML
Ph-neg MPNs“Classical”
“Non-classical”
MPN
CMML
JMML
aCML
Unclassifiable
MPN/MDS
PV
ET
PMF
CML – a peripheral blood diagnosis
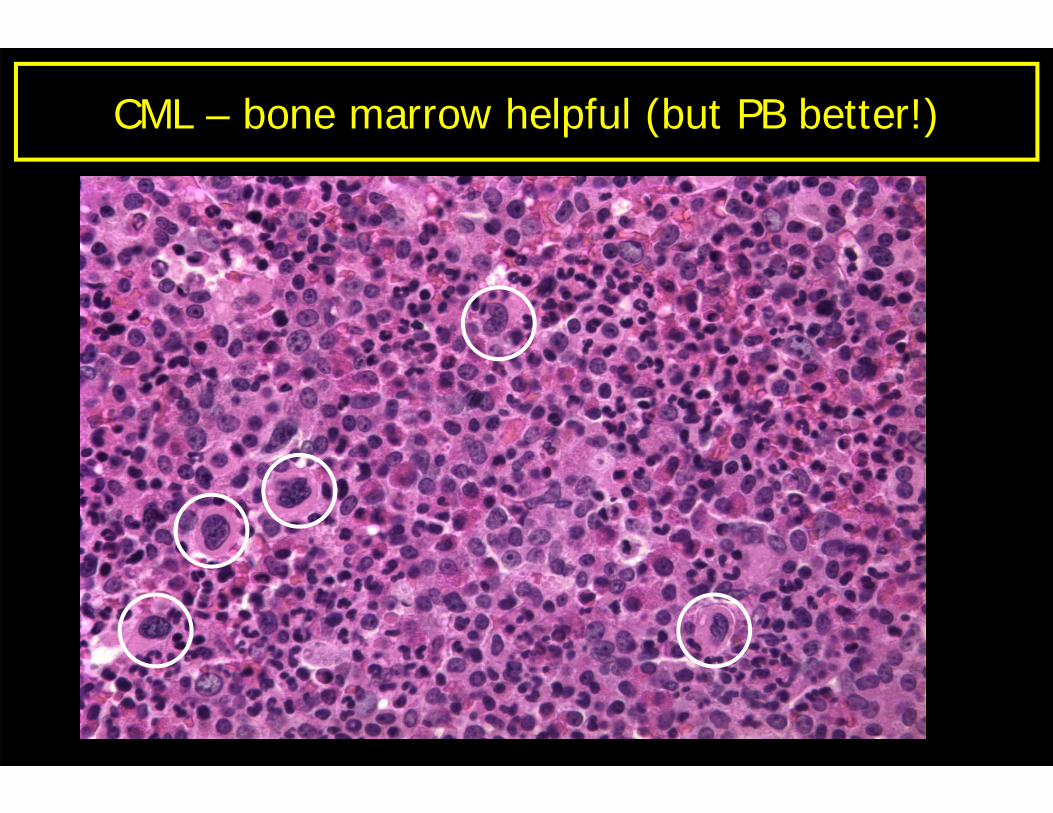
CML – bone marrow helpful (but PB better!)
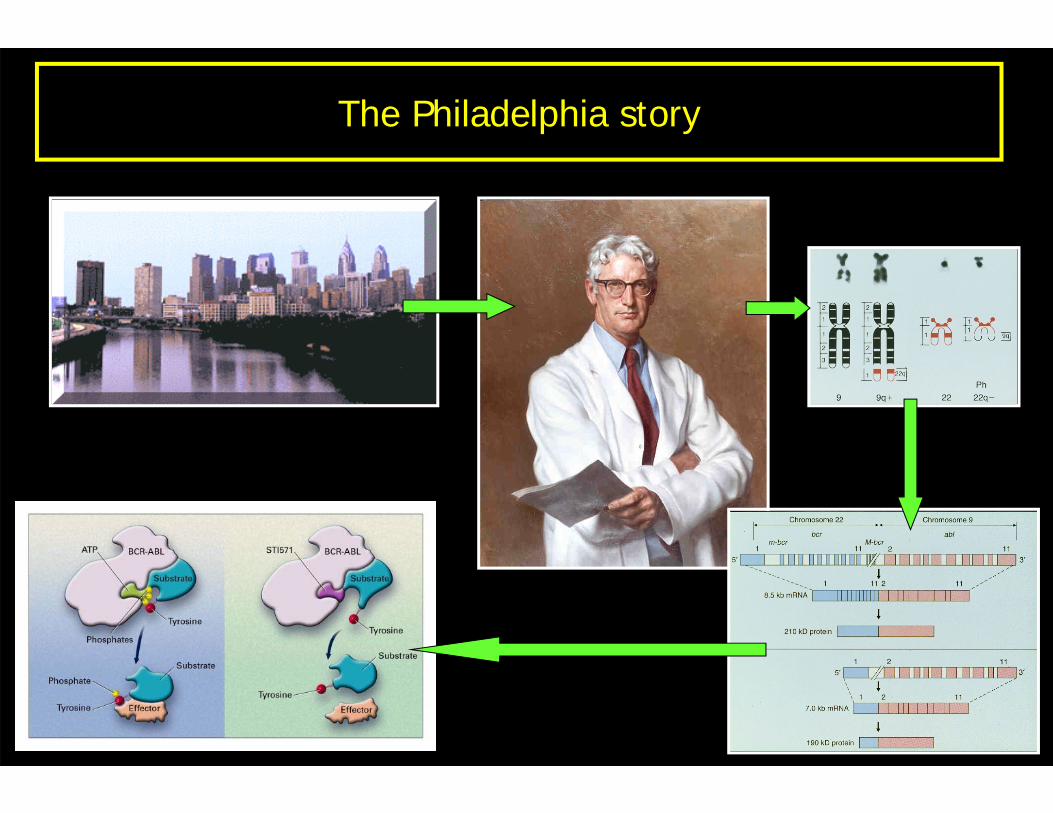
The Philadelphia story
Molecular testing in CML
Diagnosis
Monitoring
Resistance
Diagnosis
Monitoring
Resistance
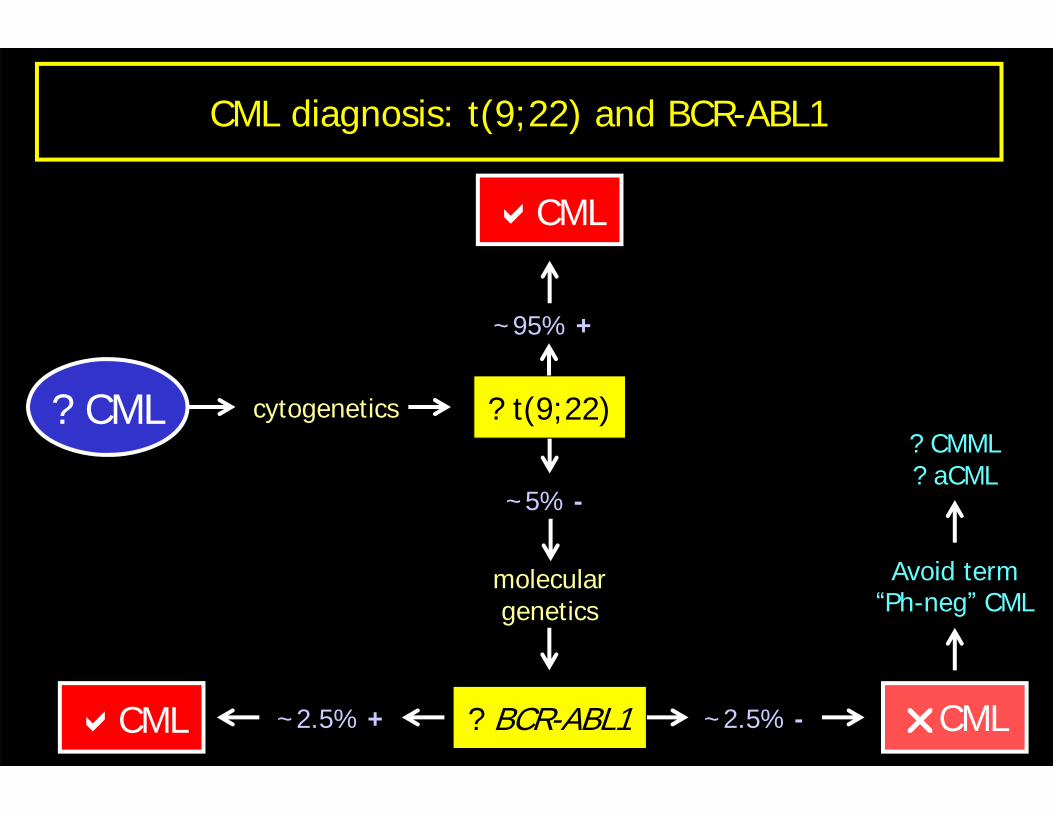
? CML cytogenetics
CML ~2.5% -~2.5% + CML
Avoid term“Ph-neg” CML
? CMML? aCML
? BCR-ABL1
~95% +
CML
~5% -
moleculargenetics
? t(9;22)
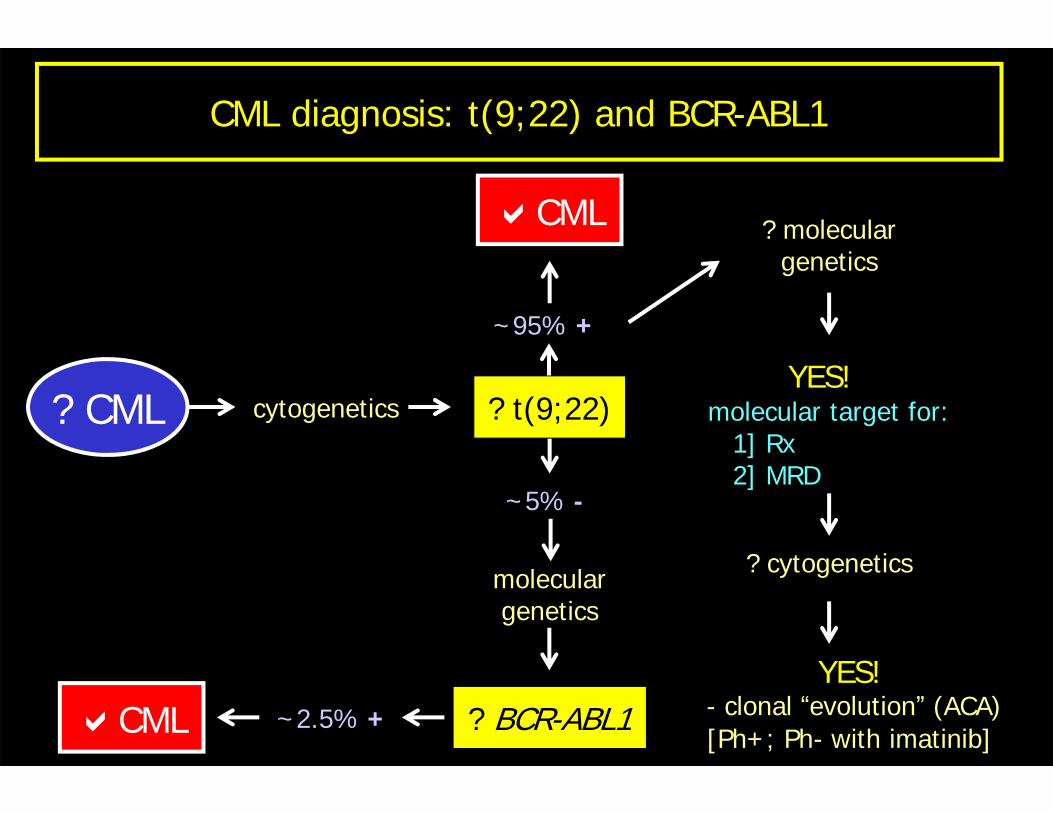
CML diagnosis: t(9;22) and BCR-ABL1
? CML cytogenetics
CML ~2.5% +
? moleculargenetics
YES!molecular target for:
1] Rx2] MRD
? cytogenetics
YES!- clonal “evolution” (ACA)[Ph+; Ph- with imatinib]
? BCR-ABL1
~95% +
CML
~5% -
moleculargenetics
? t(9;22)
CML diagnosis: t(9;22) and BCR-ABL1
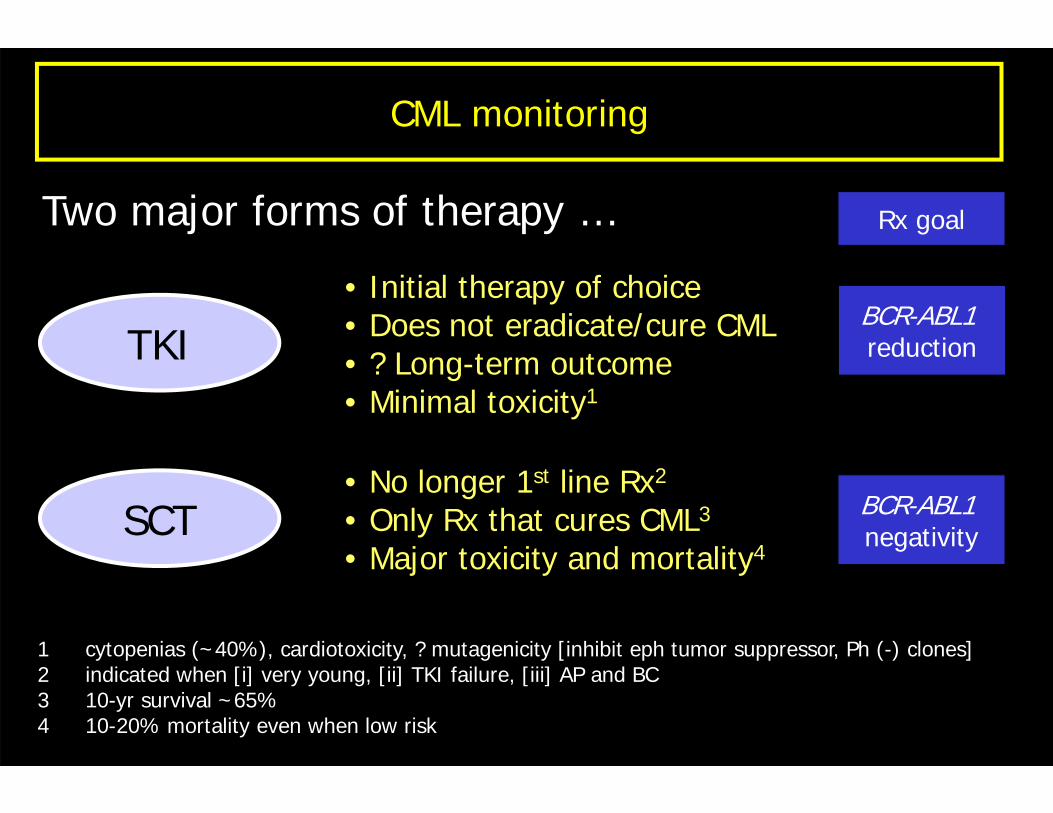
CML monitoring
Two major forms of therapy …
TKI
SCT
• Initial therapy of choice• Does not eradicate/cure CML• ? Long-term outcome• Minimal toxicity1
1 cytopenias (~40%), cardiotoxicity, ? mutagenicity [inhibit eph tumor suppressor, Ph (-) clones]2 indicated when [i] very young, [ii] TKI failure, [iii] AP and BC3 10-yr survival ~65%4 10-20% mortality even when low risk