Page 1
Molecular Pathology of Lymphoma:
Focus on B-cell lymphomas
XXIV International Academy of Pathology – Arab Division (IAPAD)
Update on Molecular Pathology Khartoum, Sudan – December 7, 2012
Adam Bagg, MD Director, Hematology Medical Director, Clinical Cancer Cytogenetics University of Pennsylvania
Page 2
what why how
highlight pitfalls
IG and TCR
lymphoid stuff
myeloid stuff
Application of molecular studies to
diagnosis of hematopoietic
neoplasms
Page 3
what why how
highlight pitfalls
IG and TCR
B-cell stuff
myeloid stuff
myeloid stuff
break!! highlight pitfalls
Application of molecular studies to
diagnosis of hematopoietic
neoplasms
Page 5
Molecular targets what
Page 6
Molecular targets what
• Rearrangements - physiologic - pathologic
Page 7
A B
C
A B
A B
creation of a novel
chimeric gene
upregulated/overexpression
of a protooncogene
t(9;22) bcr-abl t(8;14) IgH + c-myc
Molecular targets what
• Rearrangements - physiologic - pathologic
qualitative quantitative
Page 8
A B
C
A B
A B
creation of a novel
chimeric gene
upregulated/overexpression
of a protooncogene
t(9;22) bcr-abl t(8;14) IgH + c-myc
Molecular targets what
• Rearrangements - physiologic - pathologic
qualitative quantitative
homogeneity vs
heterogeneity
present vs
absent
Page 9
A B
C
A B
A B
creation of a novel
chimeric gene
upregulated/overexpression
of a protooncogene
t(9;22) bcr-abl t(8;14) IgH + c-myc
Molecular targets what
• Rearrangements - physiologic - pathologic
• Mutations
qualitative quantitative
homogeneity vs
heterogeneity
present vs
absent
Page 10
A B
C
A B
A B
creation of a novel
chimeric gene
upregulated/overexpression
of a protooncogene
t(9;22) bcr-abl t(8;14) IgH + c-myc
Molecular targets what
• Rearrangements - physiologic - pathologic
• Mutations
• Additions
• Losses - deletions - silencing
qualitative quantitative
homogeneity vs
heterogeneity
present vs
absent
Page 11
Major methodologies how
Cytogenetics
Molecular genetics
FISH SKY CGH
Page 12
Major methodologies how
Cytogenetics
Molecular genetics
FISH SKY CGH
SB
Page 13
Major methodologies how
Cytogenetics
Molecular genetics
FISH SKY
PCR
CGH
SB
Page 14
Major methodologies how
Cytogenetics
Molecular genetics
FISH SKY
PCR
CGH
?CHIP SB
Page 15
Major methodologies how
Cytogenetics
Molecular genetics
FISH SKY
PCR
CGH
?CHIP SB NGS!
Page 16
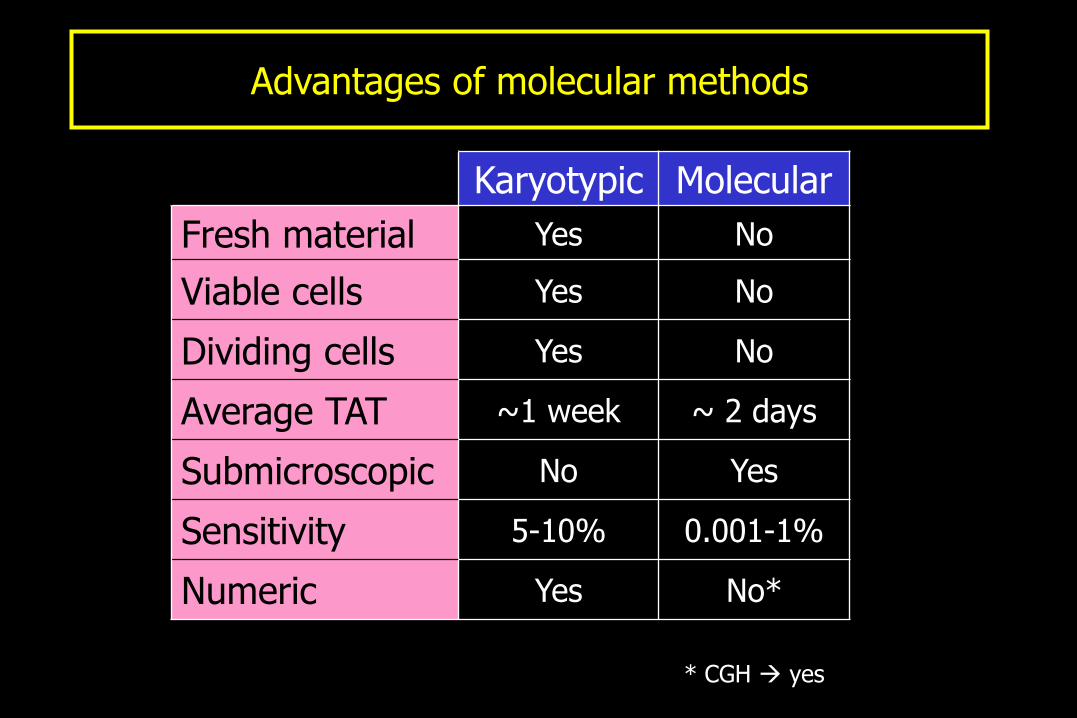
Advantages of molecular methods
Karyotypic Molecular
Fresh material Yes No
Viable cells Yes No
Dividing cells Yes No
Average TAT ~1 week ~ 2 days
Submicroscopic No Yes
Sensitivity 5-10% 0.001-1%
Numeric Yes No*
* CGH yes
Page 18
Major indications for molecular testing why
Page 19
• diagnosis - neoplastic vs reactive (and beyond)
• classification - based upon the genetic lesion [sine qua non]
• prognosis - in otherwise homogeneous diseases
• monitoring/MRD - both response and early recurrence
• cryptic abnormalities • technical reasons
Major indications for molecular testing why
Page 21
T-cell B-cell
T-cell receptor
Antigen
Immunoglobulin
Antigen receptors
Page 22
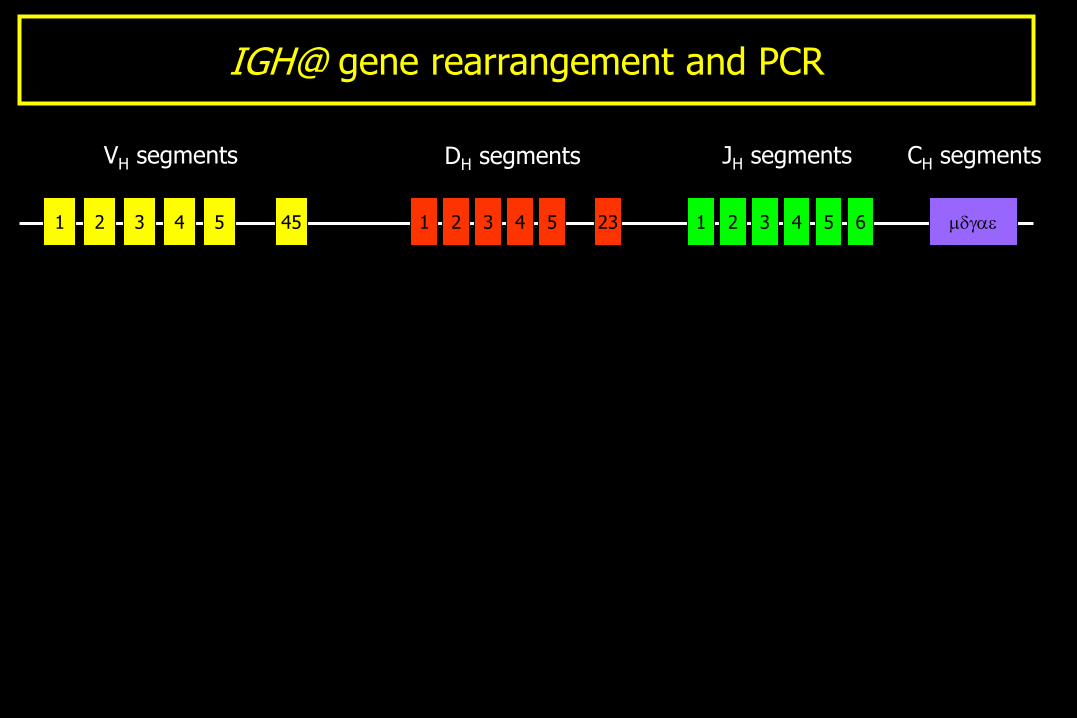
1 2 3 4 5 45 1 2 3 4 5 23 1 2 3 6 4 5 mdgae
VH segments CH segments JH segments DH segments
IGH@ gene rearrangement and PCR
Page 23
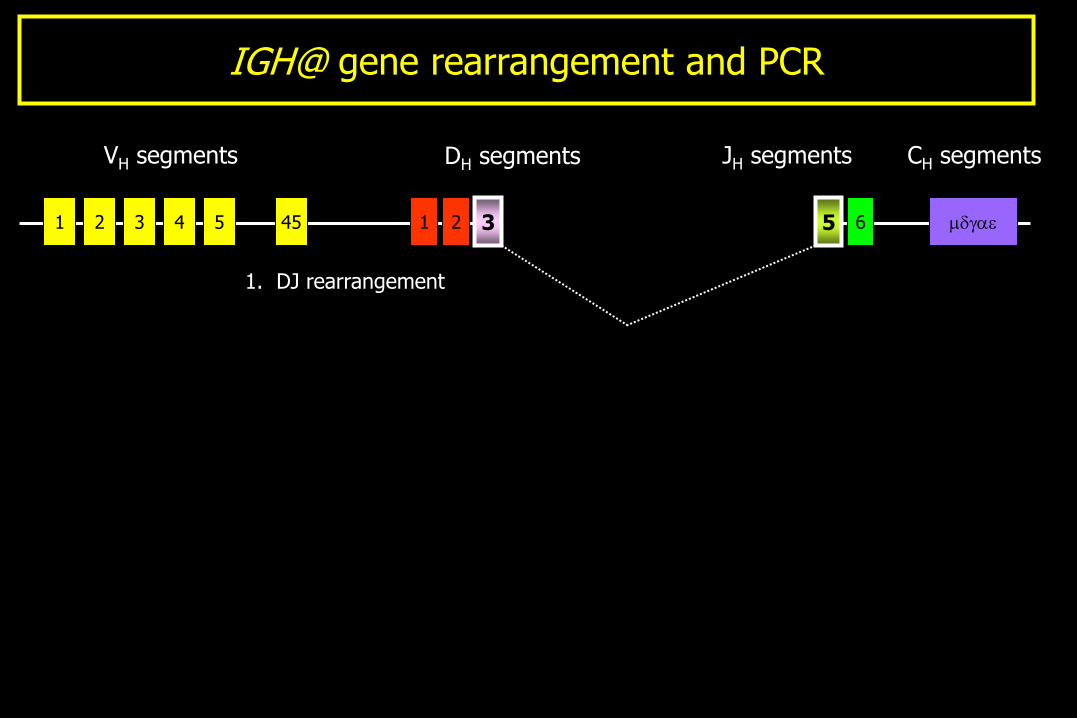
1 2 3 4 5 45 1 2 3 4 5 23 1 2 3 6 4 5
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
IGH@ gene rearrangement and PCR
Page 24
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae 3 5
IGH@ gene rearrangement and PCR
Page 25
1 2 3 4 5 45 1 2 6 mdgae
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae 3 5
3 5
IGH@ gene rearrangement and PCR
Page 26
2. V-DJ rearrangement
1 2 3 4 5 45 1 2 6
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
mdgae
3 5
3 5
IGH@ gene rearrangement and PCR
Page 27
2. V-DJ rearrangement
1 6
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
mdgae 2
3 5
3 5
IGH@ gene rearrangement and PCR
Page 28
1 6 mdgae
2. V-DJ rearrangement
1 6
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
mdgae 2
3 5
3 5
3 5 2
IGH@ gene rearrangement and PCR
Page 29
1
3. High power view
2. V-DJ rearrangement
1 6
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
mdgae
mdgae
2
3 5
3 5
6 3 5 2
VH2 DH3 JH5 N N
IGH@ gene rearrangement and PCR
Page 30
1
VH2 DH3 JH5 N N
L CDR I FR II CDR II FR III CDR III FR IV FR I
3. High power view
CDRs, FRs
2. V-DJ rearrangement
1 6
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
mdgae
mdgae
2
3 5
3 5
6 3 5 2
IGH@ gene rearrangement and PCR
Page 31
1
VH2 DH3 JH5 N N
L CDR I FR II CDR II FR III CDR III FR IV FR I
3. High power view
CDRs, FRs and primers
2. V-DJ rearrangement
1 6
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
mdgae
mdgae
2
3 5
3 5
6 3 5 2
IGH@ gene rearrangement and PCR
Page 32
1
VH2 DH3 JH5 N N
L CDR I FR II CDR II FR III CDR III FR IV FR I
3. High power view
CDRs, FRs and primers
2. V-DJ rearrangement
1 6
1 2 3 4 5 45 1 2 6
VH segments CH segments JH segments DH segments
1. DJ rearrangement
mdgae
mdgae
mdgae
2
3 5
3 5
6 3 5 2
IGH@ gene rearrangement and PCR
Page 33
IGH@ gene rearrangement and PCR
gel-based PCR product detection
Size Poly Mono Mono Mono Poly Neg
Page 34
neoplastic
IGH@ gene rearrangement and PCR
reactive
capillary electrophoresis-based PCR product detection
Page 35
Antigen receptor gene rearrangements
• atypical lymphoproliferations
• limited tissue
• equivocal immunophenotype (??)
• T-cell lymphoproliferations
• baseline for MRD
• BM: precursor B-cells
Useful in the following situations:
But not that helpful in:
• diagnosing specific entities
• unraveling the heterogeneity
Page 37
Specific lymphoma categories …
Page 38
Follicular lymphoma: t(14;18) and BCL-2
Page 39
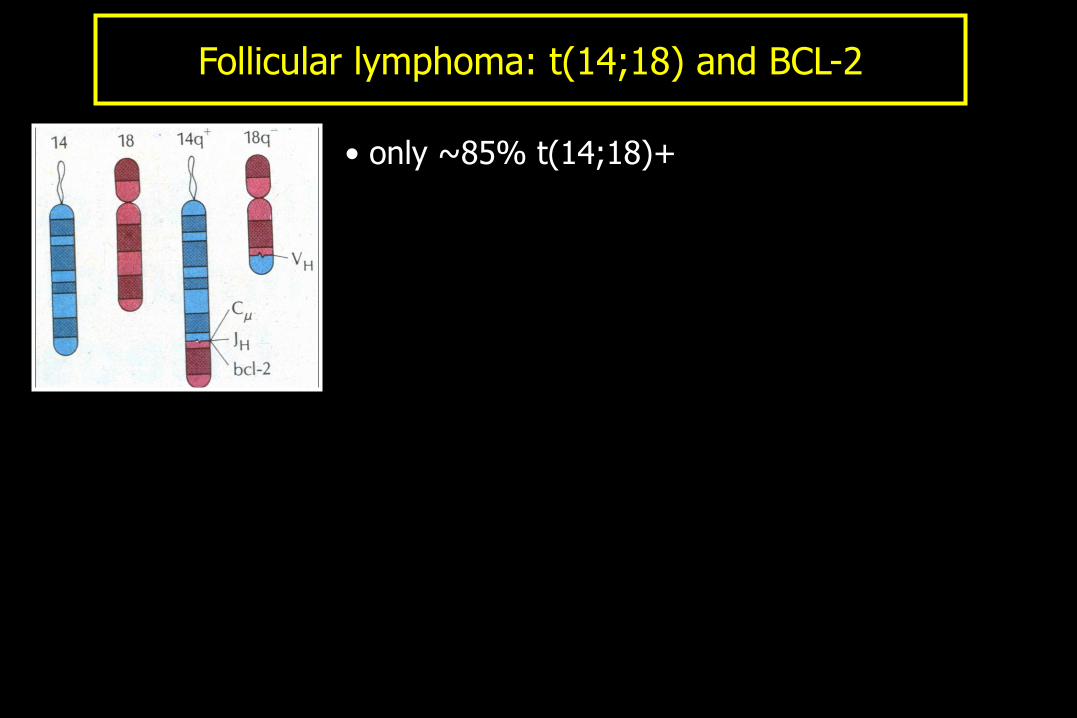
Follicular lymphoma: t(14;18) and BCL-2
• only ~85% t(14;18)+
Page 40
Follicular lymphoma: t(14;18) and BCL-2
• only ~85% t(14;18)+
• not all t(14;18)+ cases = FL
Page 41
Follicular lymphoma: t(14;18) and BCL-2
• FL vs RFH (IHC ) • FL vs other SBCL (IHC )
• only ~85% t(14;18)+
• not all t(14;18)+ cases = FL
Page 42
Follicular lymphoma: t(14;18) and BCL-2
• FL vs RFH (IHC ) • FL vs other SBCL (IHC )
• only ~85% t(14;18)+
• rare cases: - t(14;18)+; IHC-
- point mutation
• not all t(14;18)+ cases = FL
Page 43
Follicular lymphoma: t(14;18) and BCL-2
• t(14;18) PCR preferable to IGH PCR
• FL vs RFH (IHC ) • FL vs other SBCL (IHC )
• only ~85% t(14;18)+
• rare cases: - t(14;18)+; IHC-
- point mutation
• not all t(14;18)+ cases = FL
Page 44
Follicular lymphoma: t(14;18) and BCL-2
• t(14;18) PCR preferable to IGH PCR
• of the ~15% t(14;18)-negative cases:
copies chromosome 18/BCL-2 BCL-2+
t(BCL-6) BCL-2- (MUM1+, grade 3)
• FL vs RFH (IHC ) • FL vs other SBCL (IHC )
• only ~85% t(14;18)+
• rare cases: - t(14;18)+; IHC-
- point mutation
• not all t(14;18)+ cases = FL
Page 45
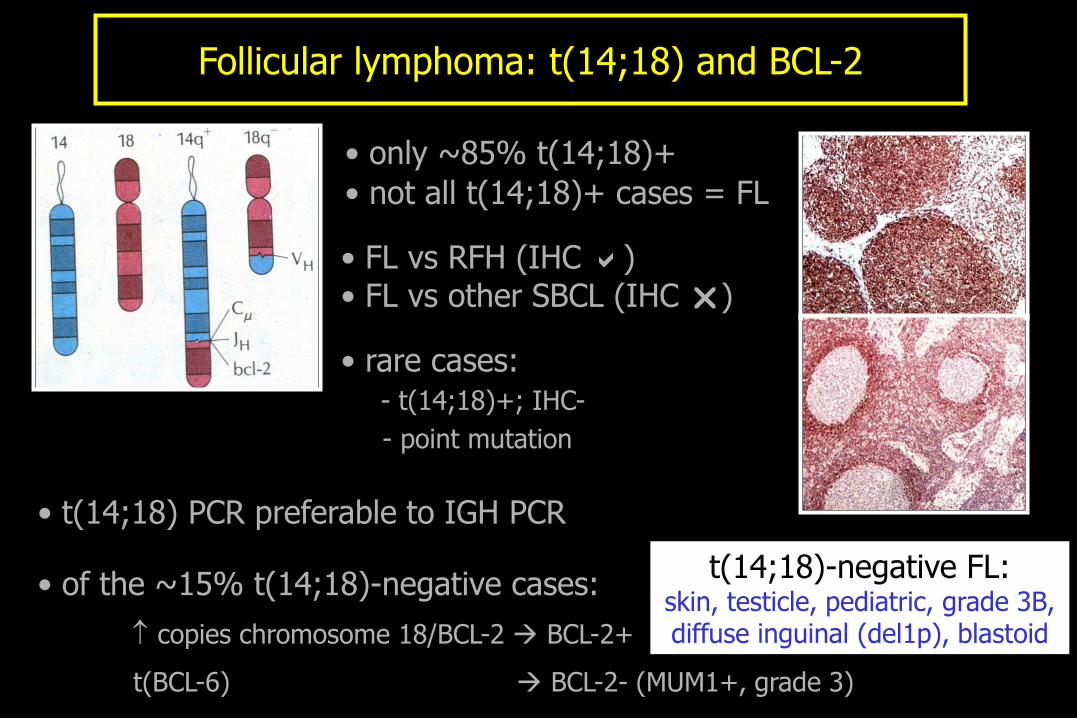
Follicular lymphoma: t(14;18) and BCL-2
• t(14;18) PCR preferable to IGH PCR
• of the ~15% t(14;18)-negative cases:
copies chromosome 18/BCL-2 BCL-2+
t(BCL-6) BCL-2- (MUM1+, grade 3)
• FL vs RFH (IHC ) • FL vs other SBCL (IHC )
• only ~85% t(14;18)+
• rare cases: - t(14;18)+; IHC-
- point mutation
• not all t(14;18)+ cases = FL
t(14;18)-negative FL: skin, testicle, pediatric, grade 3B, diffuse inguinal (del1p), blastoid
Page 46
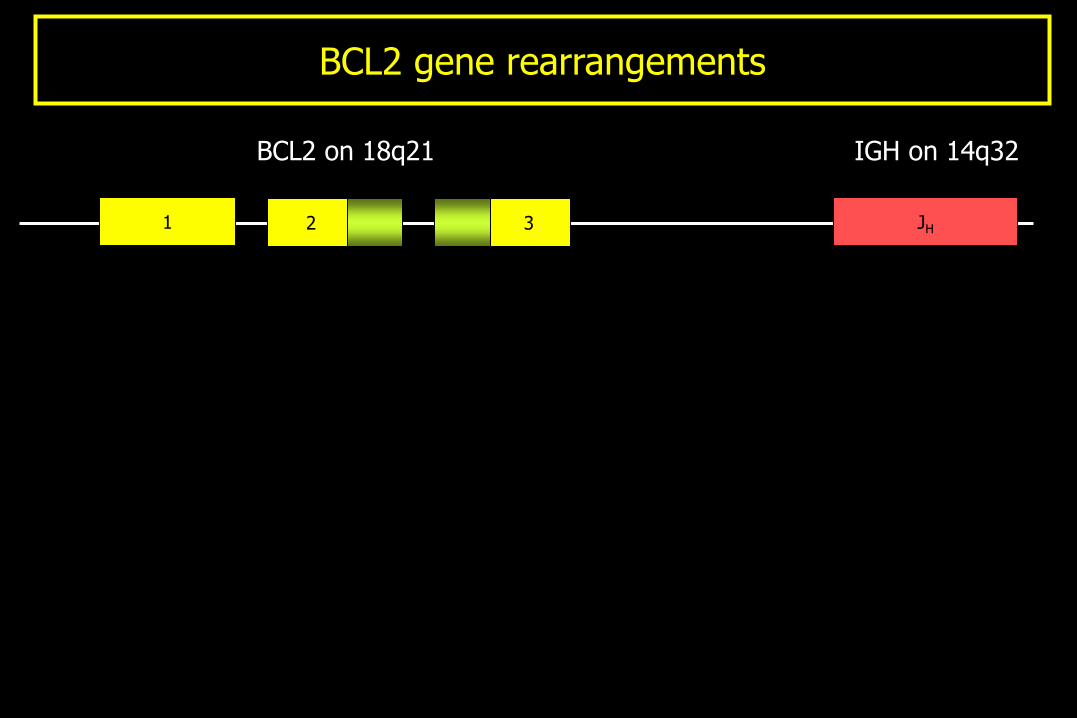
BCL2 gene rearrangements
1 2 3 JH
BCL2 on 18q21 IGH on 14q32
Page 47
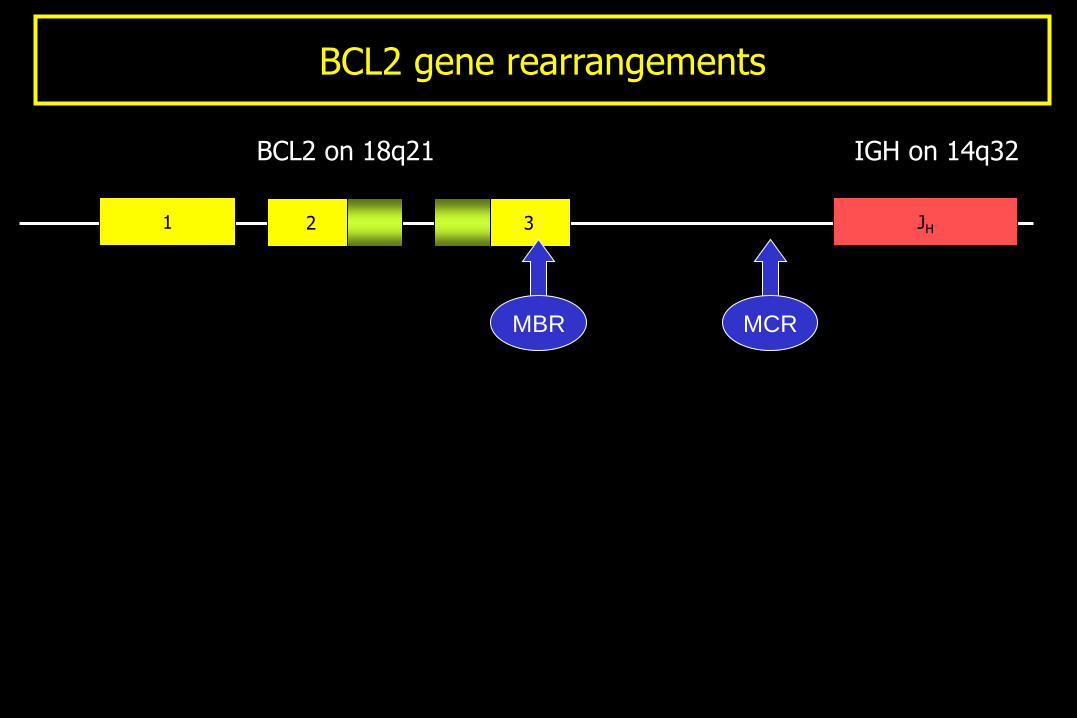
BCL2 gene rearrangements
1 2 3 JH
MBR MCR
BCL2 on 18q21 IGH on 14q32
Page 48
BCL2 gene rearrangements
1 2 3 JH
MBR MCR
PCR [~75%]
BCL2 on 18q21 IGH on 14q32
Page 49
BCL2 gene rearrangements
1 2 3 JH
VCR MBR ICR MCR
BCL2 on 18q21 IGH on 14q32
PCR [~75%]
Page 50
BCL2 gene rearrangements
1 2 3 JH
VCR MBR ICR MCR
Southern
blot
PCR [~75%]
BCL2 on 18q21 IGH on 14q32
Page 51
BCL2 gene rearrangements
1 2 3 JH
VCR MBR ICR MCR
Southern
blot
FISH
PCR [~75%]
BCL2 on 18q21 IGH on 14q32
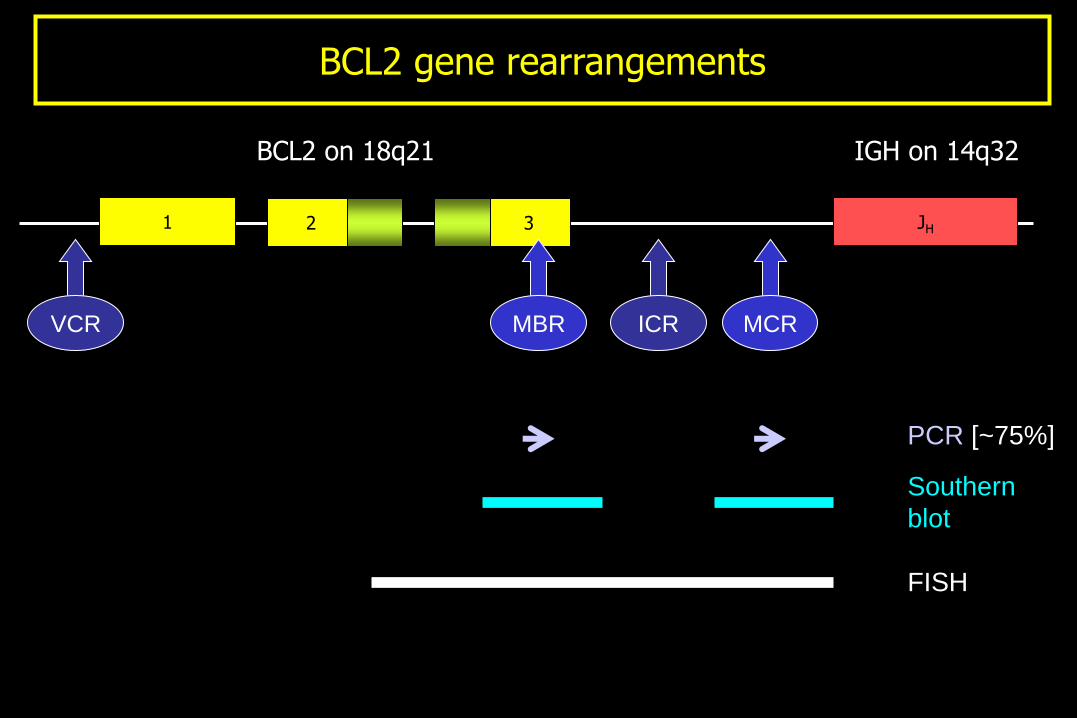
Page 52
BCL2 gene rearrangements
1 2 3 JH
VCR MBR ICR MCR
Southern
blot
Classical
cytogenetics
FISH
PCR [~75%]
BCL2 on 18q21 IGH on 14q32
Page 54
Chronic lymphocytic leukemia/SLL
Page 55
CLL: Unraveling the heterogeneity
Conventional parameters
Novel parameters
Page 56
CLL: Unraveling the heterogeneity
Novel parameters
Cytogenetics
Cell of origin
Page 58
Cytogenetics
del(13q14)
del(11q22)
+12
del(17p13) ~55%
~18%
~16%
~7%
Page 59
Cytogenetics: molecular
del(13q14)
del(11q22)
+12
del(17p13) ?miRNA
~18%
~16%
~7%
Page 60
Cytogenetics: molecular
del(13q14)
del(11q22)
+12
del(17p13)
ATM
~16%
~7% ?miRNA
Page 61
Cytogenetics: molecular
del(13q14)
del(11q22)
+12
del(17p13)
ATM
? CDK4
~7% ?miRNA
Page 62
Cytogenetics: molecular
del(13q14)
del(11q22)
+12
del(17p13)
ATM
p53
? CDK4
?miRNA
Page 63
Prognostication by cytogenetics
Dohner, H et al N Engl J Med 2000, 343:1910.
Copyright © 2000,
Massachusetts Medical Society.
All rights reserved.
Page 64
Prognostication by cytogenetics
Dohner, H et al N Engl J Med 2000, 343:1910.
Copyright © 2000,
Massachusetts Medical Society.
All rights reserved.
Page 65
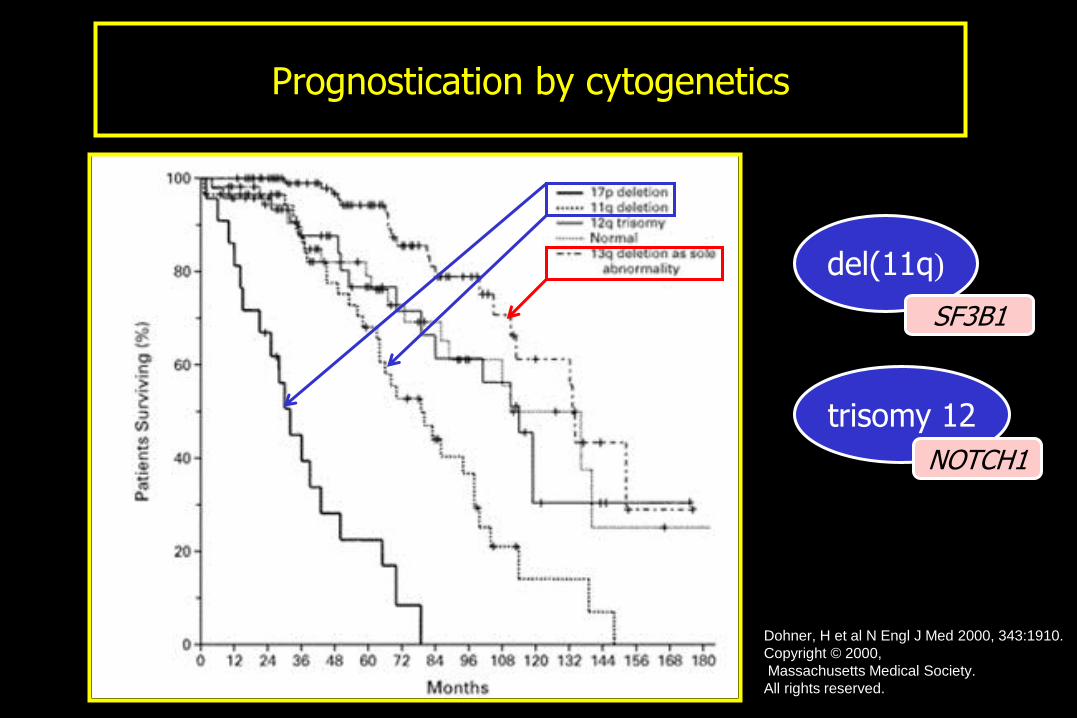
Prognostication by cytogenetics
Dohner, H et al N Engl J Med 2000, 343:1910.
Copyright © 2000,
Massachusetts Medical Society.
All rights reserved.
del(11q)
trisomy 12
SF3B1
NOTCH1
Page 66
Cell of origin
The dogma
CLL is a neoplasm of naïve B-cells …
Page 67
Cell of origin
The dogma
CLL is a neoplasm of naïve B-cells …
… but a KARma has run over this DOGma
Page 68
Chronic lymphocytic leukemia
* pre-GC - non-mutated IgH - “naïve” - poorer prognosis
post-GC - mutated IgH - memory - better prognosis
*
Page 69
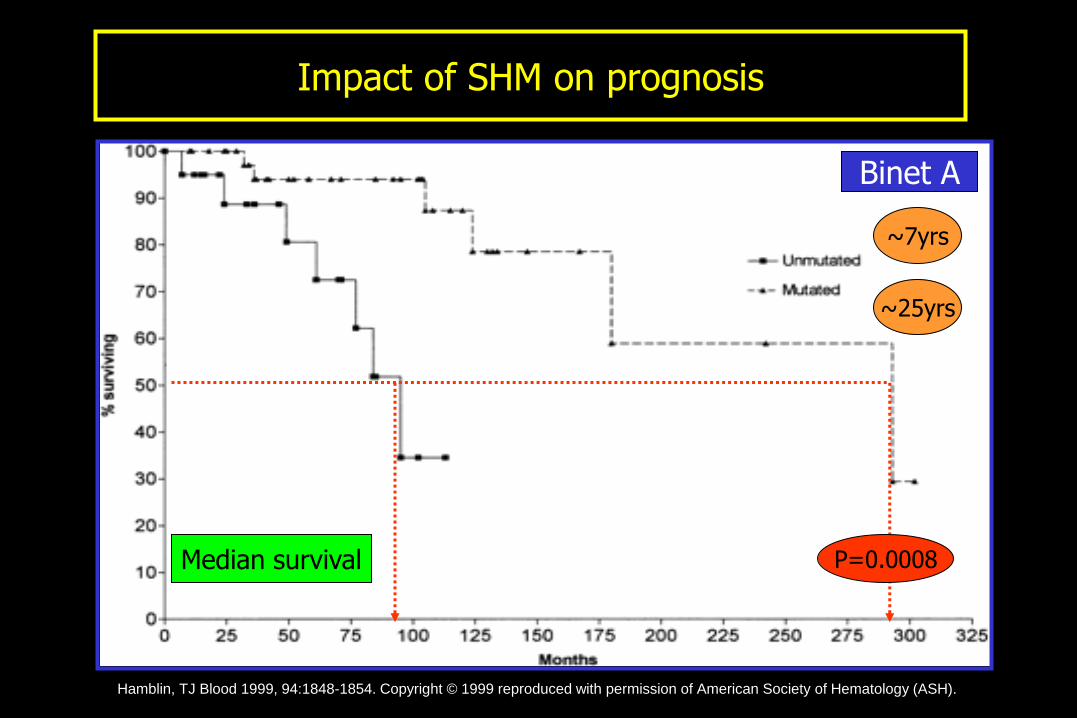
Impact of SHM on prognosis
Binet A
P=0.0008 Median survival
~7yrs
~25yrs
Hamblin, TJ Blood 1999, 94:1848-1854. Copyright © 1999 reproduced with permission of American Society of Hematology (ASH).
Page 70
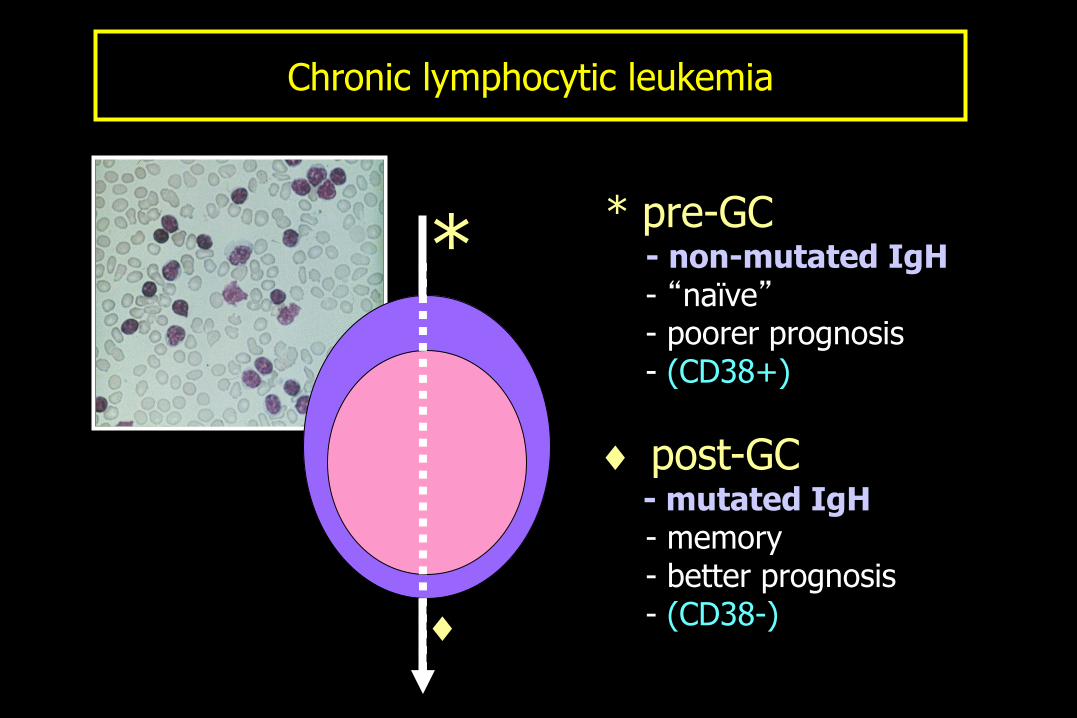
Chronic lymphocytic leukemia
* pre-GC - non-mutated IgH - “naïve” - poorer prognosis - (CD38+)
post-GC - mutated IgH - memory - better prognosis - (CD38-)
*
Page 71
* pre-GC - non-mutated IgH - “naïve” - poorer prognosis
post-GC - mutated IgH - memory - better prognosis
*
ZAP70
Chronic lymphocytic leukemia
Page 72
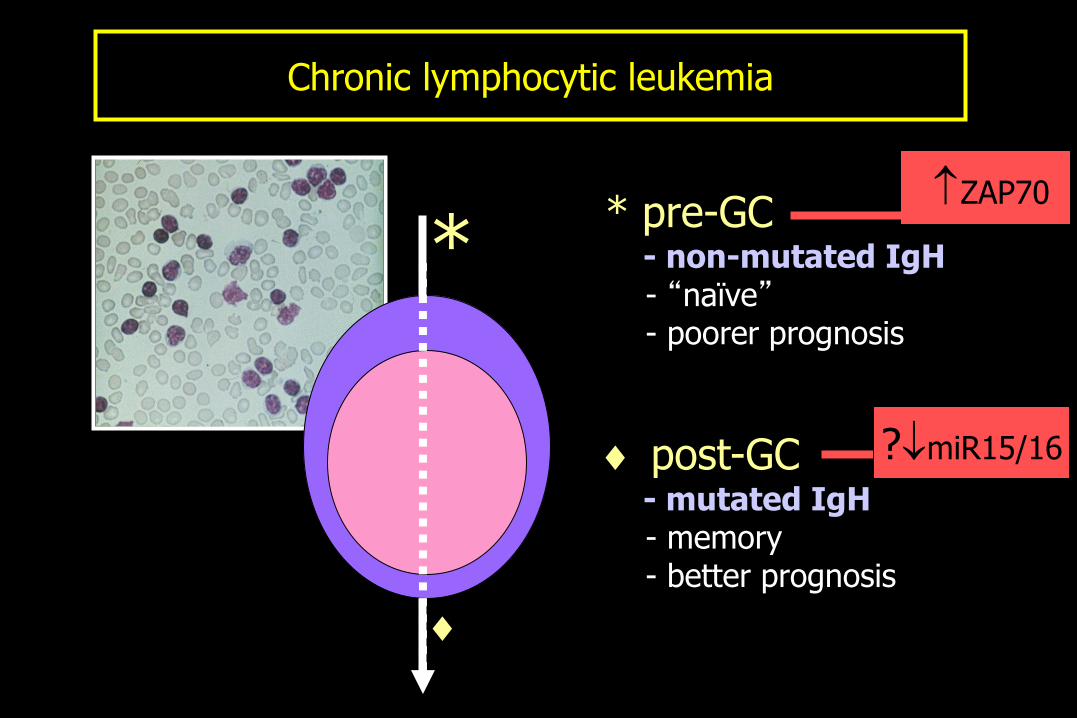
* pre-GC - non-mutated IgH - “naïve” - poorer prognosis
post-GC - mutated IgH - memory - better prognosis
*
?miR15/16
Chronic lymphocytic leukemia
ZAP70
Page 73
CD79a CD3
ZAP70 by IHC on PB
H&E
Page 74
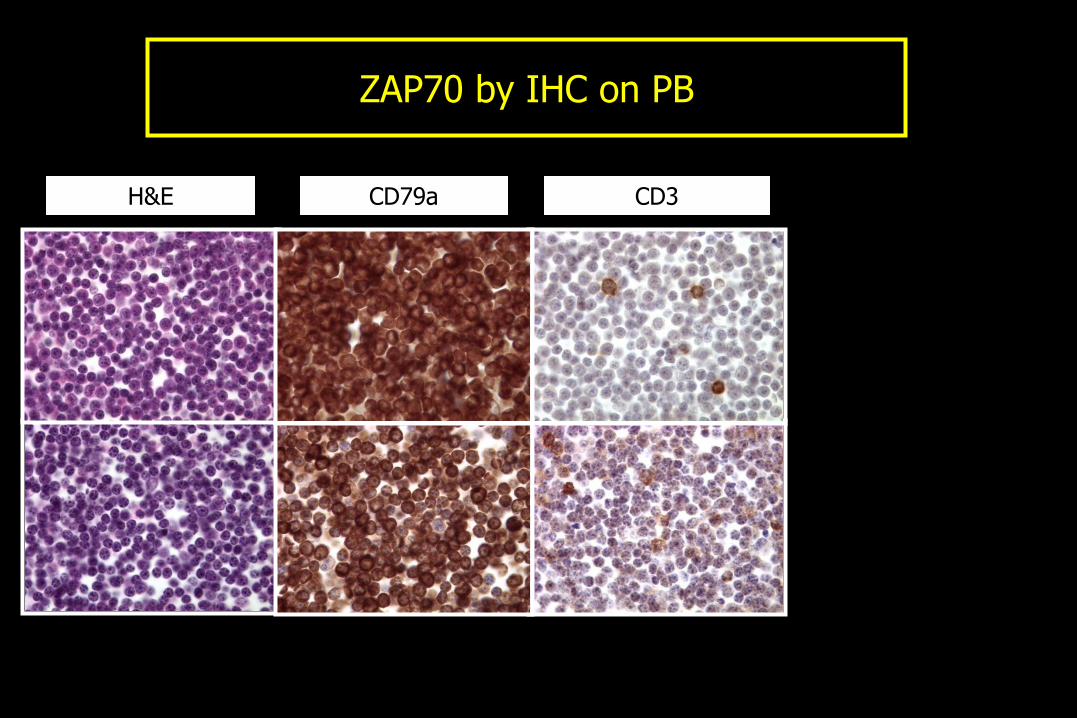
CD79a CD3 ZAP70 H&E
ZAP70 by IHC on PB
Page 75
CD79a CD3 ZAP70 H&E
SHM-
SHM+
ZAP70 by IHC on PB
Page 77
Diffuse Large B-cell Lymphoma (DLBCL)
• Morphologic: - centroblastic - immunoblastic - T-cell/histiocyte-rich - anaplastic - plasmablastic - lymphomatoid granulomatosis type
• Clinicopathologic: - primary mediastinal (thymic) large B-cell lymphoma - primary CNS lymphoma - primary effusion lymphoma - primary cutaneous large B-cell lymphoma (of the leg!) - intravascular large cell lymphoma
Page 78
Separation of DLBLs into two broad groups:
• germinal center • activated B-cell
DLBCL: Gene expression profiling
Reprinted by permission from Macmillan Publishers Ltd:
Alizadeh, A et al Nature 2000, 403:503-511 © 2000.
Page 79
That’s all very nice and impressive, but …
DLBCL: Gene expression profiling
Page 80
That’s all very nice and impressive, but … • Highly complex (10, 000’s of genes) • Expensive • Need fresh/frozen tissue
DLBCL: Gene expression profiling
Page 81
That’s all very nice and impressive, but … • Highly complex (10, 000’s of genes) • Expensive • Need fresh/frozen tissue
So, what’s a humble, information-overloaded pathologist to do?
DLBCL: Gene expression profiling
Page 82
That’s all very nice and impressive, but … • Highly complex (10, 000’s of genes) • Expensive • Need fresh/frozen tissue
So, what’s a humble, information-overloaded pathologist to do?
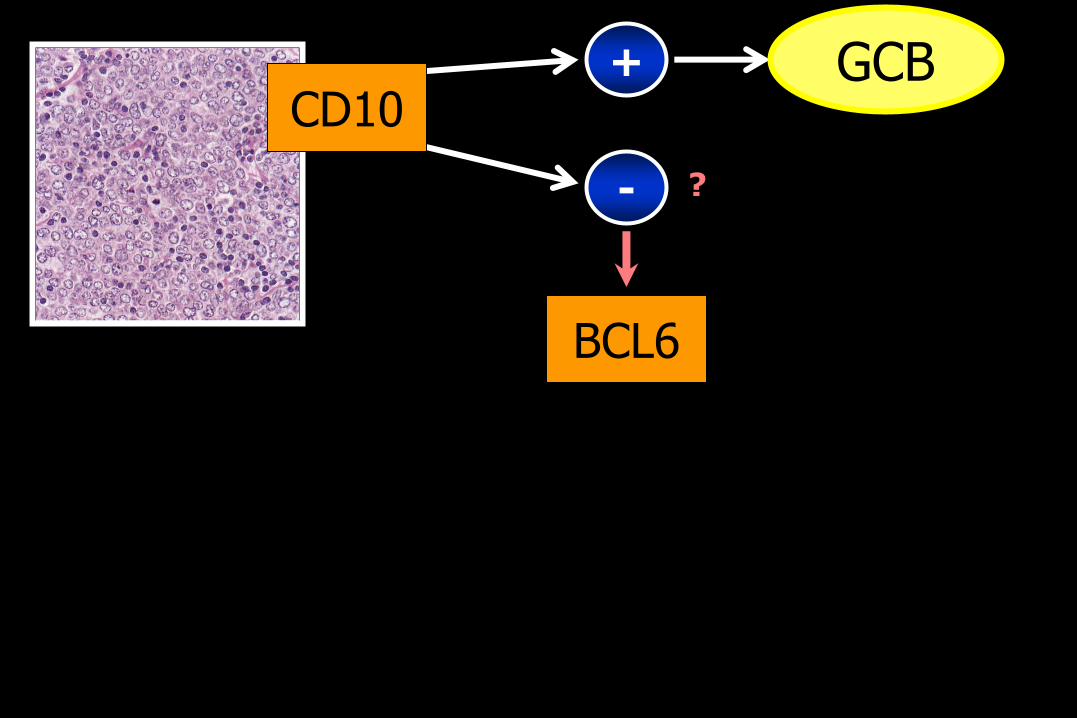
• Wait … … for the dust to settle … … and it might be … … and use IHC … (and only 3 markers at that!)
DLBCL: Gene expression profiling
Page 88
CD10 +
-
BCL6
GCB
?
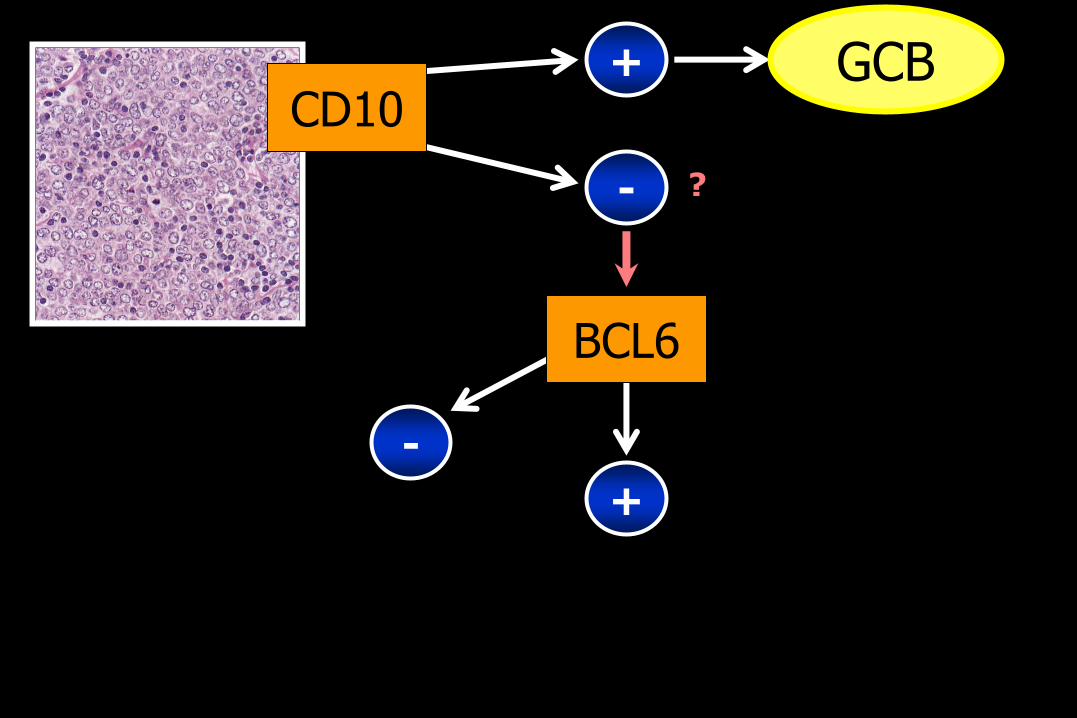
Page 89
CD10 +
-
BCL6
-
GCB
+
?
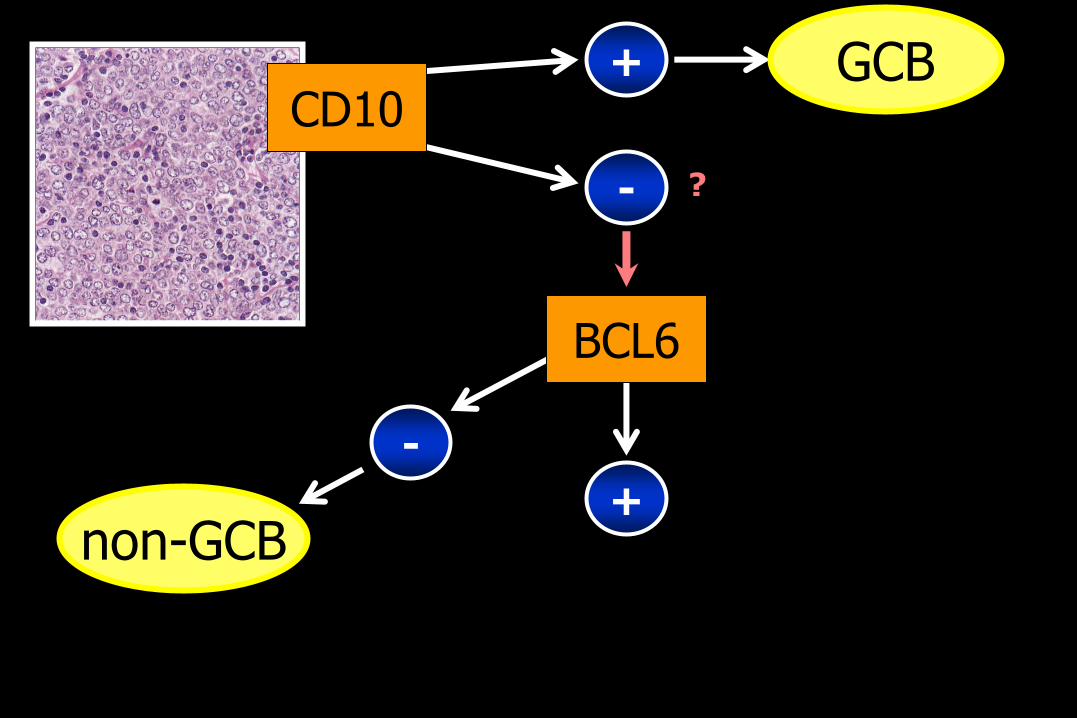
Page 90
CD10 +
-
BCL6
-
GCB
non-GCB +
?
Page 91
CD10 +
-
BCL6
-
GCB
non-GCB +
?
?
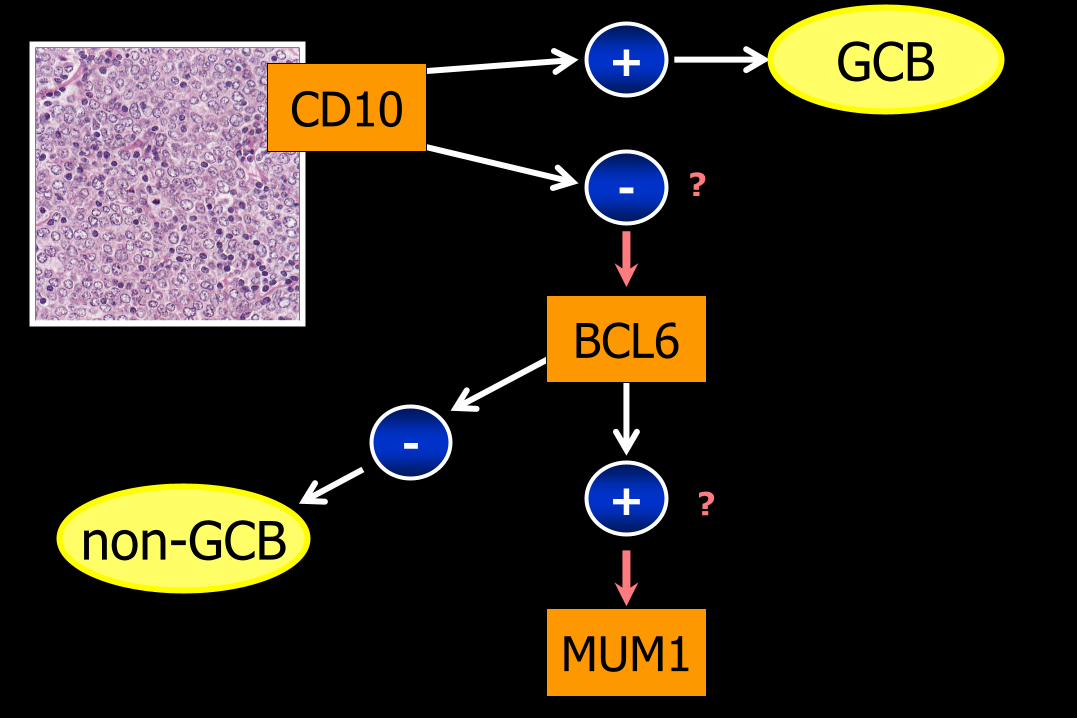
Page 92
CD10 +
-
BCL6
-
GCB
non-GCB +
MUM1
?
?
Page 93
CD10 +
-
BCL6
-
GCB
non-GCB +
MUM1 + -
?
?
Page 94
CD10 +
-
BCL6
-
GCB
non-GCB +
MUM1 + -
?
?
Page 95
CD10 +
-
BCL6
-
GCB
non-GCB +
MUM1 + -
?
?
Page 96
CD10 +
-
BCL6
-
GCB
non-GCB +
MUM1 + -
?
?
BCL2
FOXP1
GCET1
Page 97
CD10 +
-
BCL6
-
GCB
non-GCB +
MUM1 + -
?
?
BCL2
FOXP1
GCET1
Page 98
CD10 +
-
BCL6
-
GCB
non-GCB +
MUM1 + -
?
?
BCL2
FOXP1
GCET1
LMO2
CD137
Page 100
“False” positives
Pitfalls and caveats: IG and TCR PCR
Page 101
“False” positives - contamination
Pitfalls and caveats: IG and TCR PCR
Page 102
“False” positives - contamination
- pseudoclonality (small biopsies)
Pitfalls and caveats: IG and TCR PCR
Page 103
“False” positives - contamination
- pseudoclonality (small biopsies)
- reactive/inflammatory scenarios
H. pylori gastritis (but …)
Hepatitis C (but …)
Viral infections (HIV, mumps, EBV, CMV)
Sjögren syndrome
Rheumatoid arthritis
Pitfalls and caveats: IG and TCR PCR
Page 104
“False” positives - contamination
- pseudoclonality (small biopsies)
- reactive/inflammatory scenarios
H. pylori gastritis (but …)
Hepatitis C (but …)
Viral infections (HIV, mumps, EBV, CMV)
Sjögren syndrome
Rheumatoid arthritis
- canonical (TCRg)
Pitfalls and caveats: IG and TCR PCR
Page 105
“False” positives - contamination
- pseudoclonality (small biopsies)
- reactive/inflammatory scenarios
H. pylori gastritis (but …)
Hepatitis C (but …)
Viral infections (HIV, mumps, EBV, CMV)
Sjögren syndrome
Rheumatoid arthritis
- canonical (TCRg)
- immune reconstitution post BMT
- immune response to tumor
Pitfalls and caveats: IG and TCR PCR
Page 106
“False” positives - contamination
- pseudoclonality (small biopsies)
- reactive/inflammatory scenarios
H. pylori gastritis (but …)
Hepatitis C (but …)
Viral infections (HIV, mumps, EBV, CMV)
Sjögren syndrome
Rheumatoid arthritis
- canonical (TCRg)
- immune reconstitution post BMT
- immune response to tumor
- “clonal dermatitis”
Pitfalls and caveats: IG and TCR PCR
Page 107
False negatives
Pitfalls and caveats: IG and TCR PCR
Page 108
- Preanalytic variables [degradation, fixation, representative sampling]
- Technical
consensus primers
using CDR3 IgH primers only
- Biologic
pre GC/ intra/post GC
precursor B-cells
• partial DJ
• oligoclonal
(~1/3 precursor B-ALL)
• ongoing rearrangements at relapse
False negatives
• somatic hypermutation
(primary/ongoing)
(follicular lymphoma,
myeloma)
• IgH deletions
(~1/10 lymphomas)
Pitfalls and caveats: IG and TCR PCR
Page 109
- Preanalytic variables [degradation, fixation, representative sampling]
- Technical
consensus primers
using CDR3 IgH primers only
- Biologic
pre GC/ intra/post GC
precursor B-cells
• partial DJ
• oligoclonal
(~1/3 precursor B-ALL)
• ongoing rearrangements at relapse
False negatives
• somatic hypermutation
(primary/ongoing)
(follicular lymphoma,
myeloma)
• IgH deletions
(~1/10 lymphomas)
Pitfalls and caveats: IG and TCR PCR
Page 110
- Preanalytic variables [degradation, fixation, representative sampling]
- Technical
consensus primers
using CDR3 IGH primers only
- Biologic
pre GC/ intra/post GC
precursor B-cells
• partial DJ
• oligoclonal
(~1/3 precursor B-ALL)
• ongoing rearrangements at relapse
False negatives
• somatic hypermutation
(primary/ongoing)
(follicular lymphoma,
myeloma)
• IgH deletions
(~1/10 lymphomas)
Pitfalls and caveats: IG and TCR PCR
Page 111
- Preanalytic variables [degradation, fixation, representative sampling]
- Technical
consensus primers
using CDR3 IGH primers only
- Biologic
pre GC/ intra/post GC
precursor B-cells
• partial DJ
• oligoclonal
(~1/3 precursor B-ALL)
• ongoing rearrangements at relapse
False negatives
• somatic hypermutation
(primary/ongoing)
(follicular lymphoma,
myeloma)
• IgH deletions
(~1/10 lymphomas)
Pitfalls and caveats: IG and TCR PCR
Page 112
False negatives
- Preanalytic variables [degradation, fixation, representative sampling]
- Technical
consensus primers
using CDR3 IGH primers only
- Biologic
pre GC/ intra/post GC
precursor B-cells
• partial DJ
• oligoclonal
(~1/3 precursor B-ALL)
• ongoing rearrangements at relapse
• somatic hypermutation
(primary/ongoing)
(follicular lymphoma,
myeloma)
• IgH deletions
(~1/10 lymphomas)
Pitfalls and caveats: IG and TCR PCR
Page 113
False negatives
- Preanalytic variables [degradation, fixation, representative sampling]
- Technical
consensus primers
using CDR3 IGH primers only
- Biologic
pre GC/ intra/post GC
precursor B-cells
• partial DJ
• oligoclonal
(~1/3 precursor B-ALL)
• ongoing rearrangements at relapse
• somatic hypermutation
(primary/ongoing)
(follicular lymphoma,
myeloma)
• IGH deletions
(~1/10 lymphomas)
Pitfalls and caveats: IG and TCR PCR
Page 114
• Powerful … but one piece of the puzzle
The last slide …
Page 115
• Powerful … but one piece of the puzzle
• Positive result: not always = neoplastic
The last slide …
Page 116
• Powerful … but one piece of the puzzle
• Positive result: not always = neoplastic
• Negative result: not always = not neoplastic
The last slide …
Page 117
• Powerful … but one piece of the puzzle
• Positive result: not always = neoplastic
• Negative result: not always = not neoplastic
• Integrate: with morphologic, immunophenotypic, clinical data
The last slide …
Page 118
• Powerful … but one piece of the puzzle
• Positive result: not always = neoplastic
• Negative result: not always = not neoplastic
• Integrate: with morphologic, immunophenotypic, clinical data
• Decision to perform/ability to interpret: contextual
The last slide …
Page 119
• Powerful … but one piece of the puzzle
• Positive result: not always = neoplastic
• Negative result: not always = not neoplastic
• Integrate: with morphologic, immunophenotypic, clinical data
• Decision to perform/ability to interpret: contextual
• More rational, biologically-based diagnosis: more appropriate, targeted Rx
The last slide …