Page 1
Monitoring Chemical Contamination of Medical Air UsingLow-Cost Sensors
by
Hosna Movahhedinia
A thesis submitted in conformity with the requirementsfor the degree of Master of Applied Science
Department of Chemical Engineering and Applied ChemistryUniversity of Toronto
c© Copyright 2018 by Hosna Movahhedinia
Page 2
Abstract
Monitoring Chemical Contamination of Medical Air Using Low-Cost Sensors
Hosna Movahhedinia
Master of Applied Science
Department of Chemical Engineering and Applied Chemistry
University of Toronto
2018
Medical air is used in hospitals for patients suffering from a wide range of health prob-
lems. This air is typically produced by pressurizing outdoor air on-site and supplying it
to patients through piping system. Thus, it may contain chemical pollution from out-
door sources or can be polluted because of technical problems in the production system.
Hospitals in North America are mandated to meet the medical air quality standards
established by the United States Pharmacopeia (USP), yet medical air quality is often
unmonitored. Thus, potentially failing to meet the patients’ health requirements. In this
study, concentration of CO, CO2, NOx, and O3, black carbon, and ultrafine particles
in medical air were evaluated. Simultaneous measurements were made at the outdoor
intake and patient-room ends of a medical air system at a Canadian hospital. The results
showed a strong association between outdoor air pollution and the medical air quality
based on correlation analysis.
ii
Page 3
Acknowledgements
”Laudation to the God of majesty and glory! Obedience to him is a cause of approach
and gratitude in increase of benefits. Every inhalation of the breath prolongs life and
every expiration of it gladdens our nature; wherefore every breath confers two benefits
(blessings) and for every benefit gratitude is due.
Whose hand and tongue is capable to fulfill the obligations of thanks to him?”
Gulistan, Sadi Shirazi, 1258
I am very grateful to Prof. Greg Evans for giving me this research opportunity and
supporting me with his supervision. I am also very thankful to Dr. Samira Mubareka
for her valuable advice and guidance.
I would like to thank our collaborators at Sunnybrook Research Centre and Air Liquide
S.A., namely Nicolas Groulx, Faisal Qureshi, and Paul Edwards, without whom this
research would not have been possible. I also would like to acknowledge all the members
of SOCAAR for their insight and support.
iii
Page 4
Contents
Acknowledgements iii
Contents iv
List of Tables vii
List of Figures viii
1 Introduction 1
1.1 What is Medical Air . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
1.2 How is Medical Air Produced . . . . . . . . . . . . . . . . . . . . . . . . 1
1.2.1 Intake for the Medical Air . . . . . . . . . . . . . . . . . . . . . . 3
1.2.2 Inlet Filter . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.2.3 Air Compressor . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
1.2.4 After-Coolers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.2.5 Receiver . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.2.6 Air Dryer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.2.7 Final Line Filters . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
1.2.8 Air Quality Monitoring System . . . . . . . . . . . . . . . . . . . 5
1.2.9 Alarms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.2.10 Final Line Regulators . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.2.11 Piping . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
1.3 Typical Sources of Contamination . . . . . . . . . . . . . . . . . . . . . . 6
iv
Page 5
1.4 Medical Air Standards and Their Shortcomings Compared to Outdoor
Standard Specifications . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
1.5 Potential Hazards in Using Medical Air . . . . . . . . . . . . . . . . . . . 7
1.6 Previous Studies on the Quality of Medical Air . . . . . . . . . . . . . . . 9
1.7 Thesis Summary and Objective of the Chapter . . . . . . . . . . . . . . . 10
2 Literature Review 11
2.1 Health Impacts of Air Pollution . . . . . . . . . . . . . . . . . . . . . . . 11
2.1.1 Particulate Matter (PM) . . . . . . . . . . . . . . . . . . . . . . . 11
2.1.2 Ozone (O3) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
2.1.3 Nitrogen Dioxide (NO2) . . . . . . . . . . . . . . . . . . . . . . . 12
2.1.4 Sulfur Dioxide (SO2) . . . . . . . . . . . . . . . . . . . . . . . . . 13
2.1.5 Carbon Monoxide and Carbon Dioxide (CO and CO2) . . . . . . 13
2.2 Low-Cost Air Quality Sensors . . . . . . . . . . . . . . . . . . . . . . . . 14
2.2.1 Metal Oxide Semiconductor (MOS) Sensors . . . . . . . . . . . . 16
2.2.2 Electrochemical (EC) Sensors . . . . . . . . . . . . . . . . . . . . 17
2.2.3 Optical Sensors . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
2.3 Machine Learning Algorithms Used for Calibrating Sensors . . . . . . . . 19
2.3.1 Multiple Linear Regression (MLR) . . . . . . . . . . . . . . . . . 19
2.3.2 Random Forest (RF) . . . . . . . . . . . . . . . . . . . . . . . . . 20
2.3.3 Artificial Neural Network (ANN) . . . . . . . . . . . . . . . . . . 21
2.3.4 Recurrent Neural Network (RNN) . . . . . . . . . . . . . . . . . . 25
2.4 Summary of the Chapter . . . . . . . . . . . . . . . . . . . . . . . . . . . 26
3 Methodology 27
3.1 Study Site . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
3.2 Sensor Calibration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
3.2.1 Calibration Site and Instrumentation . . . . . . . . . . . . . . . . 31
3.3 Data Analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
3.3.1 Data Preparation . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
3.3.2 Data Exploration . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
v
Page 6
3.3.3 Generating Calibration Models . . . . . . . . . . . . . . . . . . . 32
3.3.4 Evaluating Calibration Models . . . . . . . . . . . . . . . . . . . . 33
3.4 Calibrating CO2 Sensors . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
3.4.1 Investigating the Effect of Humidity on the CO2 Sensor . . . . . . 34
3.4.2 Calibrating CO2 Sensors Under Real Conditions . . . . . . . . . . 34
3.5 Summary of the Chapter . . . . . . . . . . . . . . . . . . . . . . . . . . . 34
4 Results and Discussion 35
4.1 Exploring Calibration Data . . . . . . . . . . . . . . . . . . . . . . . . . 35
4.2 Feature Selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
4.3 Evaluating and Comparing Calibration Models . . . . . . . . . . . . . . . 42
4.4 Calibrating CO2 Sensors . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
4.5 Investigating the Cross-Sensitivity of the CO2 Sensor to Water Vapor . . 54
4.6 Application to Air Quality Monitoring at the Hospital and Wallberg Building 61
4.7 Summary of the Chapter . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
5 Conclusion and Future Work 69
References 71
6 References 71
Appendix A Quality of Compressed Air at the Wallberg Building 80
Appendix B Comparison Between O3 and NOx Levels in Medical and
Outdoor Air 83
vi
Page 7
List of Tables
1.1 Comparing medical air and ambient air quality standards . . . . . . . . . 7
2.1 Summary of characteristics of low-cost sensors . . . . . . . . . . . . . . . 15
3.1 Specifications of the portable devices . . . . . . . . . . . . . . . . . . . . 28
3.2 List of sensors applied to this study . . . . . . . . . . . . . . . . . . . . . 29
3.3 Reference instruments . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31
4.1 Selected sensors for building calibration models . . . . . . . . . . . . . . 41
4.2 List of parameters used for RNN and ANN. . . . . . . . . . . . . . . . . 43
4.3 Comparing calibration models’ performance on the training set . . . . . . 44
4.4 Comparing RNN and MLR’s performance on the test set . . . . . . . . . 45
4.5 Comparing the raw K30 data and the results of applying MLR and RF
models. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
4.6 Coefficients of the calibration model. . . . . . . . . . . . . . . . . . . . . 60
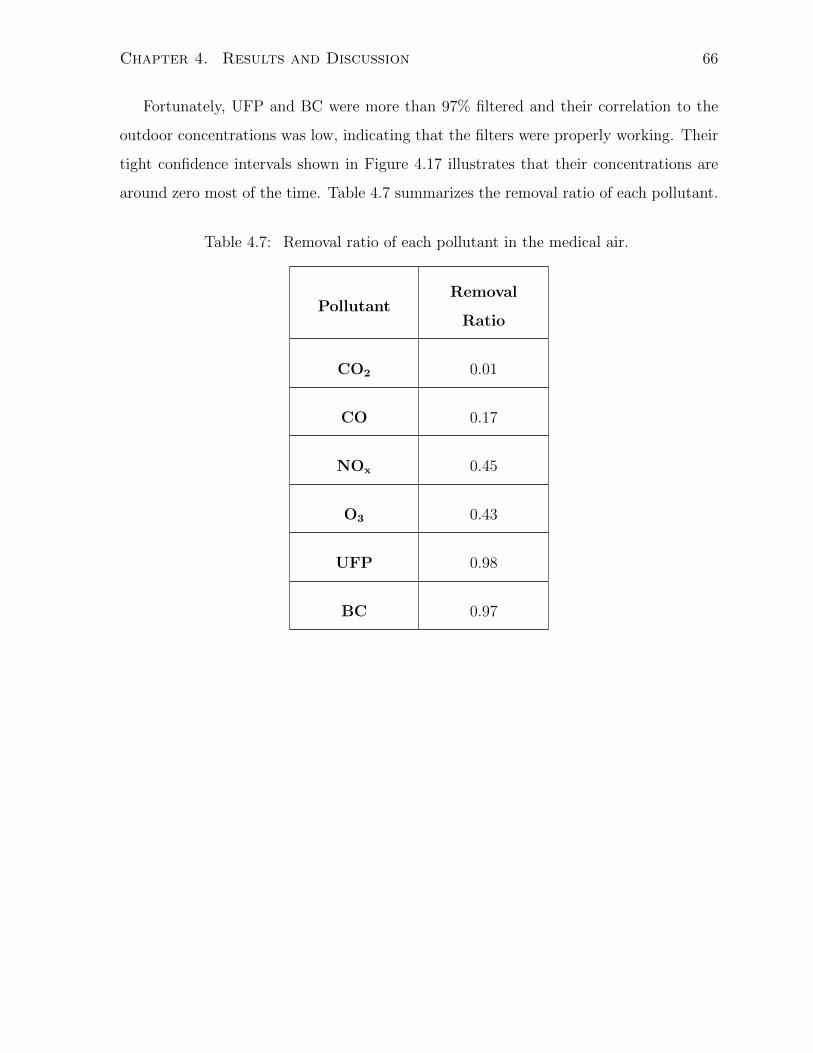
4.7 Removal ratio of each pollutant in the medical air. . . . . . . . . . . . . . 66
B.1 Contribution of outdoor pollution to NOx and O3 levels in medical air. . 83
vii
Page 8
List of Figures
1.1 Schematic of the medical air system . . . . . . . . . . . . . . . . . . . . . 2
2.1 Sensing mechanism of MOS sensors . . . . . . . . . . . . . . . . . . . . . 16
2.2 Schematic of electrochemical sensors . . . . . . . . . . . . . . . . . . . . 17
2.3 Schematic of optical sensors . . . . . . . . . . . . . . . . . . . . . . . . . 18
2.4 Schematic of a Random Forest algorithm . . . . . . . . . . . . . . . . . . 21
2.5 Architecture of an Artificial Neural Network . . . . . . . . . . . . . . . . 22
2.6 A Neural Network with weights and activation functions . . . . . . . . . 22
2.7 Activation functions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
2.8 Feed Forward Neural Network . . . . . . . . . . . . . . . . . . . . . . . . 24
2.9 Back Propagation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
2.10 Recurrent Neural Network . . . . . . . . . . . . . . . . . . . . . . . . . . 25
3.1 Sampling box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28
4.1 Histograms and whisker plots of pollutants concentration at the calibration
site. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
4.2 Correlation matrix of the sensors and pollutants. . . . . . . . . . . . . . . 38
4.3 Results of regsubsets function for selecting models’ independent variables. 40
4.4 Comparing box plots of RNN and MLR predictions with the reference
measurements. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47
4.5 Calibrating a K30 CO2 sensor using calibration gases . . . . . . . . . . . 49
4.6 Pressure, temperature, partial pressure of water vapor, and CO2 level at
highway 401 and its comparison to the K30 readings. . . . . . . . . . . . 50
viii
Page 9
4.7 Calibrating a CO2 sensor based on environmental parameters. . . . . . . 51
4.8 MLR and RF calibration results Vs. the reference measurements at Wall-
berg Building . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
4.9 Investigating the effect of humidity on the K30 CO2 sensor. . . . . . . . . 56
4.10 Investigating the effect of humidity in the dropping periods. . . . . . . . 57
4.11 Applying calibration model on the data from the humidity experiment. . 58
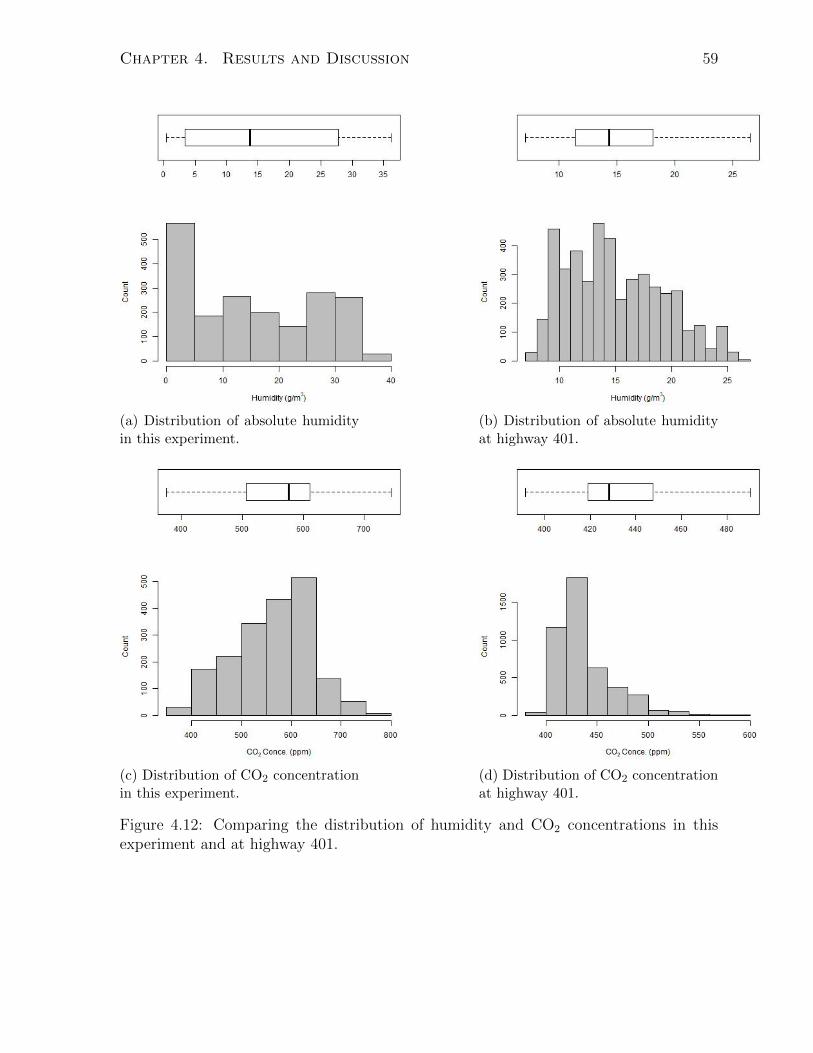
4.12 Comparing the distribution of humidity and CO2 concentrations in this
experiment and at highway 401. . . . . . . . . . . . . . . . . . . . . . . . 59
4.13 Comparing the reference CO2 concentrations and sensor measurements. . 60
4.14 Diurnal patterns of CO and CO2 concentration . . . . . . . . . . . . . . 62
4.15 Comparison between time series concentrations in medical air and outdoor
air. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63
4.16 Diurnal patterns of O3 and NOx concentration . . . . . . . . . . . . . . . 65
4.17 Diurnal patterns of UFP and BC concentration . . . . . . . . . . . . . . 67
A.1 Comparison between time series CO and CO2 concentration in Compressed
Air and outdoor air at Wallberg Building. . . . . . . . . . . . . . . . . . 81
A.2 Comparison between time series O3 and NOx concentration in Compressed
Air and outdoor air at Wallberg Building. . . . . . . . . . . . . . . . . . 82
B.1 NOx and O3 in outdoor air Vs. in medical air . . . . . . . . . . . . . . . 84
ix
Page 10
Chapter 1
Introduction
1.1 What is Medical Air
Medical air is an odorless, tasteless, colorless gas with a similar composition to the air
we breathe. It is comprised of about 78% nitrogen, 21% oxygen, and 1% of other compo-
nents such as water vapor, carbon dioxide, hydrogen, and argon [1]. Such air is produced
or conditioned for breathing purposes on-site in hospitals and dental surgeries [2]. It is
considered to be a therapeutic product by the United States Pharmacopoeia (USP) and
is named medical air USP or Air USP [3].
Medical air USP is primarily used for long-term life support such as in intensive care,
neonatal intensive care, and critical care units. It is used in respiratory therapies such
as ventilation, high flow nasal cannula therapy, inhaled nitric oxide delivery, aerosolized
medicine, and pulmonary drug delivery [4]. The quality of medical air is important,
because it is intended for infants, the elderly, and other vulnerable populations [3].
1.2 How is Medical Air Produced
Medical air is most often produced on-site in hospitals and healthcare institutions by
pulling outdoor air into Medical grade compressors, filtering and drying the compressed
air, and distributing it in the hospital’s piping system. However, if the outdoor air quality
1
Page 11
Chapter 1. Introduction 2
is poor or when only a small amount of air is required, medical air is produced by mixing
pure oxygen and nitrogen and is stored inside cylinders. In general, on-site production is
more practical and economical for the large volumes of air consumed in hospitals. The
downside of on-site manufacturing is that it requires a more complex and costly design
which must be installed and maintained carefully to keep patients safe and minimize the
risk of contamination [5].
The complexity of the medical air system and the purity of the produced air is un-
clear to most healthcare staff [5]. Any undesired gases or impurity in the air entering the
system will be compressed and delivered to the patients, unless it is removed through
the compression and the filtration system. In one instance, hospital staff reported that
a bird was drawn into the medical air system and patients had complained about the
odor resulted from the decaying bird [5]. Another example is a case where the intake
was located beside an air conditioning system; while cleaning the system with an acidic
solution, the fumes were drawn into the medical air inlet [5]. Based on these examples
and other similar incidences, it can be understood that the composition of medical air
cannot always be confidently known at the hospital bedside end of the distribution sys-
tem. Figure 1.1 shows the medical air system schematically. In the following, we will
discuss each part of the system in more detail.
Figure 1.1: Schematic of the medical air system
Page 12
Chapter 1. Introduction 3
1.2.1 Intake for the Medical Air
The location of the inlet has a great impact on the quality of medical air. The National
Fire Protection Association Code 99 (NFPA99) recommends standards for location, de-
sign, and components of medical air systems. Based on this standard, the inlet should
be placed outdoors, on the roof, at least 10ft away from any doors, windows, or other
openings, at least 20ft above the ground, and should be protected against the entry of
water, animals, and insects. In the case of installing multiple compression systems in a
building, NFPA99 allows hospitals to share one intake for all the systems which must
be sized properly, and each system must be designed to be disconnected from the line
safely. If the outdoor air is polluted and indoor air has an equal or better quality, intake
may be located within the building, but the purity must be checked regularly and if the
outdoor air quality has improved the intake should be moved back outdoors [5].
1.2.2 Inlet Filter
The inlet filter should be located before the compressors to remove dirt and coarse parti-
cles from the ambient air. This filter is meant to reduce fouling of the internal compressor
components, increase compressor’s lifespan, and decrease the end line filters’ workload
and operation noise. However, NFPA99 does not mandate the installation of this piece
of equipment in the medical air system [5].
1.2.3 Air Compressor
The compressing system increases ambient air pressure by 8 times. Usually, more than
one compressor is installed to provide the required volume of medical air in an average
hospital, and a backup system is provided for the case if one unit needs maintenance
[5]. Each compressor must be provided with appropriate valves to be insulated from the
system for servicing. Each unit must be capable of producing an adequate volume of air
at the maximum demand [5].
The medical air system is designed to produce air used exclusively for breathing
Page 13
Chapter 1. Introduction 4
purposes and should not be used for non-medical applications. Such use can increase the
demand on the system, reduce system lifetime, and open new sources of contamination to
the system. Based on NFPA99, the installed compressors must not introduce oil droplets,
water, or toxic oil products into the medical air, or the system must be designed to
separate out these contaminants [5].
1.2.4 After-Coolers
The after-cooler is an optional piece of equipment installed based on the system design
to lower the temperature after the compression system. They should be equipped with
water traps to drain the condensed water and isolation valves, so that after-coolers can
be disconnected without shutting down the whole system [5].
1.2.5 Receiver
The receiver is a cylinder that stabilizes the air pressure after compression. The receivers
should be provided with a pressure relief valve, sight glass, pressure gauge, and a water
trap to drain condensed water. While stainless steel cylinders are recommended, NFPA99
permits the iron receivers, which may rust and make flakes into the air [5].
1.2.6 Air Dryer
Dryers remove condensed water after the air passes through the compressing system.
They are mostly of the desiccant or refrigerant type. Desiccant dryers have a bed of
absorbent material, normally made from Activated Alumina, which removes the moisture
from the air stream. While only one dryer works at a time, two dryers must be installed
to allow for service maintenance and recovery. Each dryer should be able to handle the
peak load and have a bypass valve for disconnection during servicing [5, 6].
1.2.7 Final Line Filters
Final line filters prevent entry of upstream particles, oil droplets, and odor into the hos-
pital’s distribution system. Each of the filters must be sized to work with 98% efficiency
Page 14
Chapter 1. Introduction 5
at 1 micron and handle 100% of the peak system demand at the design condition. As
a result of compression, all the pollutants such as particulate matter, pollen, water, and
gaseous pollution are concentrated. Final filters are capable of removing particulates;
however, water can pass through filters and make its way to patient rooms. Also, special
scrubbers may be required to remove CO in more polluted environments [5]. Neverthe-
less, in most cases, no gas-specific filters are installed in medical air system, meaning any
outdoor gas pollution may be delivered to the patients.
1.2.8 Air Quality Monitoring System
Air quality monitoring systems are installed after the final filters and are intended to
measure pollutants at concentration levels of the USP standards, which can be orders of
magnitude higher than the normally encountered levels in outdoor air. The specifications
of this system is not mentioned in the standards.
1.2.9 Alarms
An alarm will be activated visually and audibly if concentrations rise above the USP
standard thresholds or if the downstream pressure is outside the desired range [5]. The
warning signals should be available to all the building services.
1.2.10 Final Line Regulators
Final line regulators are one of the most important parts of the system, as they adjust
the air pressure throughout the building. The final pressure should be reduced from
80− 100psig to 50− 55psig before entering the hospital’s piping system [5].
1.2.11 Piping
The material used for pipelines should be non-corrosive and resistant to water conden-
sates, such as copper and brass [5]. Copper also has an antibacterial effect and as such
is more preferred. The piping between the compressor, dryer, receiver, and after-cooler
also must be non-corrosive [5].
Page 15
Chapter 1. Introduction 6
1.3 Typical Sources of Contamination
Contamination might enter the medical air from several sources, the more common ones
being:
• Water can pass through the filters and contaminate the air or damage equipment.
• Water contamination may result from dryer saturation or inadequate maintenance,
failure of the automatic drains, or if the compressors malfunction.
• Oil can be introduced to the medical air after compression, due to malfunctioning
of compressors or installing inappropriate compressors.
• Sand, solder, and dirt may enter medical air due to poor construction techniques.
• Metal elements might enter medical air from welded parts of the pipelines.
• Filters might have limitations in removing nanoparticles.
1.4 Medical Air Standards and Their Shortcomings
Compared to Outdoor Standard Specifications
Canadian commercial producers of medical air and hospitals are mandated to validate
the quality of their final product to USP specifications. However, these standard regula-
tions are inadequate to meet the requirements of patient’s health and safety. This is due
to three main limitations: specifications allow for higher concentration of air pollutants
than outdoor standards, do not include all the conventional pollutants, and do not spec-
ify the allowable exposure time.
Most often outdoor air is assumed to be clean enough for sensitive populations, to
breath it from several hours to a few months [7]; however, previous studies have shown
the adverse effects of outdoor air pollution on patients, which will be discussed in the next
chapter. Medical air standards are less stringent than outdoor regulations, allowing for
Page 16
Chapter 1. Introduction 7
higher levels of air pollution exposure, which is inappropriate for sensitive patients. As
an example, standard thresholds of CO, NOx, and SO2 in medical air are multiple times
higher than ambient air quality standard. Also, ozone is a common air pollutant which
is unspecified in medical air standards. In addition, the time period of exposure to the
maximum level of pollutants should be specified in these standards. Finally, the medical
air standard of 500 ppm for CO2 is very close to the level above 400 ppm typical of
outdoor air, making exceedances quite likely. Table 1.1 compares standards for outdoor
air quality with medical air standards.
Table 1.1: Comparing medical air and ambient air quality standards
Pollutant Ambient Air [9] Medical Air [8] Ratio
Averaging Time Level (ppb) (ppb) (Medical
Ambient)
SO2 1hr 70 5,000 71
NO2 1hr 60 2,500 41
CO 8hr 9,000 [10] 10,000 1.1
CO2 - N/A 500,000 -
O3 8hr 62 N/A -
1.5 Potential Hazards in Using Medical Air
Most of the studies investigating the factors associated with the quality of medical air
have focused on two main concerns: breathing cold and dry air and inhaling uncontrolled
concentrations of oxygen. These problems can cause both long and short-term adverse
effects on neonates and susceptible adults.
An unconditioned, cold, and dry mixture of medical air and oxygen is usually used in
Page 17
Chapter 1. Introduction 8
resuscitation of infants during the first minutes of their life [11, 12], which may decrease
pulmonary compliance and conductance during short-term exposure while longterm ex-
posure can result in serious lung injuries and reduction in infants’ core body temperature.
Exposure to dry medical air also contributes to tension and deformation of the lung cells,
ciliary function disorders, high mucus viscosity, and lung inflammation and during short-
term exposure proves detrimental to the mucosal cells in adult patients [13, 14, 15].
Oxygen is the essential component in most of Medical gas mixtures. Too short an
exposure or a decrease in oxygen concentration might damage patients’ organs or cause
death, and too long an exposure or excessive concentration of oxygen is associated with
increased morbidity and mortality in very low birth weight infants. Long-term use of
high oxygen concentration also results in permanent blindness in premature neonates
caused by overgrowth of blood vessels in their eyes [16, 17].
Medical air is used for ventilating incubators and supporting neonates’ breathing after
birth. Most preterm births occur in the last weeks of gestation when the most rapid lung
maturation occurs. Preterm lungs continue growth after birth and their maturation is
highly affected by air pollution exposure. Chemical exposure during fetal development
and postnatal life can delay the lungs’ development and is associated with many long
and short-term health problems such as abnormal lung development, low and very low
birth weight, preterm birth, congenital defects, childhood asthma, behavioral problems,
neurocognitive decrements, and infant mortality [18, 19].
Previous studies have suggested that air pollution may enhance the risk of asthma,
chronic obstructive pulmonary diseases (COPD), lung cancer, respiratory infections, and
cardiovascular disorders in more susceptible populations such as infants, children, and
the elderly [19, 20]. Among all the chemical air pollutants PM2.5, ozone, and nitrogen
dioxide have the most exacerbating health effects [20]. In the following chapter, we will
discuss the health effects of these common pollutants.
Page 18
Chapter 1. Introduction 9
1.6 Previous Studies on the Quality of Medical Air
Only in recent years has there been study on the quality of medical air. Potentially
the first serious discussion and analysis of pollution levels in medical air were performed
by Benzing et al. (1999), who observed clinically significant concentrations of nitrogen
oxide (> 80ppb) in the compressed air at a university hospital during 40% of the working
days [21]. Unintentional inhalation of nitric oxide had caused lung damage to patients.
In addition, Nakata et al. (2002) showed that the concentration of NOx and CO in
medical air peaked during rush hours [22]. Yet, the relationship between outdoor air
quality and pollution concentration in the medical air is unknown. Recently, Edwards
et al. (2018) measured the carbon dioxide concentration in the medical air produced on-
site at a Canadian hospital, and demonstrated that the level of carbon dioxide exceeded
the USP standard threshold for 1% of the total test period [4]. The current research
investigated the effect of outdoor pollution on the medical air quality in the patient
rooms by deploying low-cost sensors and portable devices near the air intake and at the
outlet of the medical air.
Page 19
Chapter 1. Introduction 10
1.7 Thesis Summary and Objective of the Chapter
Medical air is defined as a therapeutic medicine, commonly produced on-site at health-
care facilities. The medical air system takes the outdoor air, compresses, dries, filters out
particulates, and delivers the produced air to patients. However, usually no filters are
installed to remove gaseous pollution. The quality of medical air is monitored after man-
ufacturing and an alarm goes off if the pollution levels exceed the standard thresholds;
however, patients’ exposure is not monitored continuously at the endpoint. Maximum
allowable pollution concentration in medical air is regulated by the United States Phar-
macopoeia. These standards do not include all common outdoor air pollutants, allow for
far higher concentrations than outdoor standard levels, and do not specify the allowable
exposure time. Previous studies have shown considerable levels of pollution in medical
air, which was associated with adverse health outcomes.
The main objectives of this research were to deploy low-cost sensors at hospitals and
investigate the relationship between outdoor air pollution and the medical air quality.
Chapter 2 synthesizes relevant literature to provide context. The methodology developed
and applied is described in Chapter 3. Results are discussed in Chapter 4 and Chapter
5 concludes the project.
Page 20
Chapter 2
Literature Review
2.1 Health Impacts of Air Pollution
2.1.1 Particulate Matter (PM)
Particulate matter (PM) is emitted from both human and natural activities. Human
activities include wood and fuel combustion, agricultural operations, transportation,
construction, biomass burning, and industrial processes. A significant portion of PM
is generated from natural sources such as wildfires and dust winds [23, 24]. Exposure
to PM has negative impacts on human and animals’ health, ecosystems, and visibility,
and it is estimated to cause millions of deaths annually [23, 26]. Exposure to low con-
centrations of PM is associated with heart disease and stroke; with a stronger risk for
women than for men, for non-smokers than for smokers, and for higher socioeconomic
classes [27]. Annual global average concentration of PM is approximately 7µg/m3 [25];
however, previous studies have suggested strong links between various syndromes, such
as attention deficit hyperactivity disorder, autism, loss of cognitive function, anxiety,
asthma, COPD, and hypertension with PM exposure [26]. Long-term exposure to high
levels of PM is associated with a range of respiratory and cardiovascular diseases, Parkin-
son [28, 29], cell death mechanism disorders, DNA damage, and a higher risk of cancer
[28]. Prenatal exposure to PM adversely affects microRNAs (miRNAs) by altering gene
expression profile, which may have long-term health outcomes in their later-life [30, 31].
11
Page 21
Chapter 2. Literature Review 12
In addition, short-term exposure to PM2.5 and PM10 is significantly associated with out-
of-hospital cardiac arrest (OHCA) and mortality, with strongest association being with
PM2.5 [32, 33].
2.1.2 Ozone (O3)
Ozone is a highly toxic, reactive, and oxidative gas associated with an increased risk of a
variety of adverse respiratory and cardiovascular system outcomes, such as asthma, out-
of-hospital cardiac arrest, mis-balancing of autonomic components and arterial pressure
control, oxidative stress, inflammation, coagulation, myocardial infarction, cardiac auto-
nomic disorders, arrhythmia, and a rise in the rate of mortality and morbidity [33, 34, 35].
Epidemiological evidence has estimated that 16,000 premature deaths were related to o-
zone exposure in European Union in 2013 [35]. Ozone is an important factor of increased
risk in asthma with a higher vulnerability in children [36]. Air pollution monitoring sites
worldwide show that ozone concentration often exceeds the World Health Organization
(WHO) regulated standard level for the human health protection [35]. Daily 8-hour
exposure to the maximum allowable ozone concentration and the number of patients
suffering from asthma are significantly correlated for all ages [36]. Despite the negative
health impacts of ozone, the USP standards do not include safe levels of this pollutant
for sensitive populations, and patients’ exposure is not monitored at most hospitals.
2.1.3 Nitrogen Dioxide (NO2)
Nitrogen dioxide (NO2) is an undesirable by-product of combustion in vehicles, industry,
and household gas appliances such as stoves in indoor settings [37, 38]. It has simi-
lar health impacts as ozone, but at higher concentrations [39]. Public health effects of
nitrogen dioxide range from acute symptoms and vulnerability to respiratory infection,
to permanent lung function damage and chronic diseases [38, 40]. Children, asthmat-
ic individuals, and athletes are at a greater risk [39]. Long-term exposure to nitrogen
dioxide enhances the risk of respiratory tract infections, cardiopulmonary diseases, and
lung cancer mortality in non-smokers [41, 42]. In indoor settings, gas cooking with poor
Page 22
Chapter 2. Literature Review 13
ventilation generates high concentrations of nitrogen oxides [41], which is associated with
an increased risk of asthmatic symptoms including coughs, chest tightness, breathless-
ness, and asthma attacks [40, 38]. Epidemiological studies have indicated that exposing
children to hourly peak levels of 80ppb NO2 is connected to adverse respiratory effects
[43, 44]. These impacts may or may not be specific to NO2 as NO2 has often been used
in epidemiology as a marker of exposure to the complex mixture that makes up traffic
related air pollution. Although nitrogen dioxide has been associated with adverse health
outcomes at levels encountered outdoors, its allowable concentration in medical air is far
above the ambient air quality standards.
2.1.4 Sulfur Dioxide (SO2)
Exposure to sulfur dioxide (SO2) can affect both healthy and sensitive populations. Based
on findings from laboratory studies of controlled exposure to sulfur dioxide, the US En-
vironmental Protection Agency (EPA) has concluded that short-term exposure to SO2 is
associated with a higher risk of respiratory morbidity [45]. Respiratory effects are report-
ed at moderate (< 500ppb) and high concentrations (> 500ppb) in both healthy patients
and those with pulmonary disease; however, no associated annoyance and lung function
disorders are observed at exposures up to 200ppb in healthy populations; in other words,
studies have not confirmed a clear dose-dependent health risk response to this pollutant
at low concentrations [42, 46].
Exposure to SO2 in pregnancy, perinatal, and postnatal life has more severe health
outcomes. In pregnancy, maternal exposure may cause low birth weight, during perinatal
development may damage the parasympathetic regulation of cardiovascular activity, and
in postnatal life disrupts the neurotransmission to cardiac vagal neurons [47].
2.1.5 Carbon Monoxide and Carbon Dioxide (CO and CO2)
Both carbon monoxide (CO) and carbon dioxide (CO2) are generated from wood and fuel
combustion, emitted from vehicles or indoor heating and cooking appliances. Outdoor
Page 23
Chapter 2. Literature Review 14
concentrations of CO and CO2 are typically below the standard safe levels of exposure;
however, since people spend about 90% of their time indoors, vehicular pollutant expo-
sure in near-road buildings can be 6-9 times higher than that at road sidewalks [48].
Both CO and CO2 have acute health outcomes at high concentrations, mostly occur-
ing indoors due to poor ventilation and malfunctioning of combustion appliances [49]. A
study in 2007 demonstrated that CO concentration in 67% of households with gas heaters
and 60% of those with wood heaters is above the World Health Organization’s (WHO)
standards [50]. At high concentrations, CO is a toxic inhalation hazard, may cause eye
irritation, dizziness, concentration difficulties, headaches, sensorineural hearing loss, and
even death [51, 52, 53].
Exposure to high levels of CO2 in low oxygen concentration can result in adverse
health effects such as headaches, fatigue, sleepiness, dizziness, poor memory, difficulty
to concentrate and think clearly, tinnitus, loss of eye movement and vision problems,
and personality changes [54, 55]. Long-term exposure to lower concentrations of CO2
in presence of normal oxygen may potentially induce longer-term adverse effects in both
healthy patients and vulnerable populations [54].
2.2 Low-Cost Air Quality Sensors
Compared to traditional methods of monitoring air quality, low-cost sensors have intro-
duced an inexpensive method for collecting large amounts of high spatial and temporal
resolution data. Low-cost sensors are small, portable, easy to install, and can be used
for applications where deploying traditional monitoring devices is likely impossible, such
as measuring exposure levels inside vehicles, public transportation, and trains. However,
calibrating these sensors is a complex challenge [56, 57, 58].
Various calibration algorithms have been developed to increase the accuracy of the
low-cost instruments’ measurements. These calibration models usually use an array of
Page 24
Chapter 2. Literature Review 15
sensors to account for the cross-sensitivity of different pollutants and the effect of envi-
ronmental parameters. There are three main types of low-cost sensors which are different
in price, pollutant selectivity, and sensitivity: Metal Oxide Semiconductor (MOS), Elec-
trochemical (EC), and optical sensors. In general, the MOS sensors are more affordable
but less selective than the EC and optical sensors. Electrochemical sensors have rela-
tively high selectivity and sensitivity making them proper for measuring a wide range of
pollutants. Optical sensors have an acceptable selectivity, but are moderately expensive
and have a high detection limit. Table 2.1 summarizes the characteristics of the gas
sensors.
Table 2.1: Summary of characteristics of low-cost sensors [59]
SensorRelative
CostSelectivity Sensitivity Typical Pollutants
MOS $ Uncertain Acceptable CO, O3, NO2, NH3
EC $$ Moderate Good CO, O2, NO, NO2, Cl2, SO2, H2S
Optical $$ Moderate Poor CO2, Hydrocarbons, PM
In the following section, we will explain these types of sensors in more detail and
introduce four frequently used calibration models.
Page 25
Chapter 2. Literature Review 16
2.2.1 Metal Oxide Semiconductor (MOS) Sensors
These sensors usually have an internal heater and an active sensing element made of
tin oxide or aluminum oxide. The sensing mechanism occurs through reactions between
oxygen and pollutant molecules on the surface of the sensing element at high temperatures
(300-500 ◦C). Molecular oxygen is adsorbed to the surface and forms O2-, O-, or O2-
and reacts with the gas molecules [60]. These reactions cause measurable changes in the
electrical conductivity, which can be related to the pollution concentration [59]. Typically,
MOS sensor’s response has a nonlinear relationship with the pollution level, which makes
their calibration more sophisticated [59]. Figure 2.1 shows the sensing mechanism of
MOS sensors.
Figure 2.1: Sensing mechanism of MOS sensors [59]
Page 26
Chapter 2. Literature Review 17
2.2.2 Electrochemical (EC) Sensors
These sensors are based on oxidation-reduction reactions between pollutant molecules
and the electrodes within the sensor. There are three electrodes inside the small sensor’s
chamber: the working, counter, and reference electrodes. The working electrode is coated
with a catalyst to provide a high surface area for a reduction or oxidation reaction with
the gas molecules. The electronic charge generated on the working electrode balances
with a reaction on the counter electrode to form a pair of redox chemical reactions,
which produces a measurable current proportional to the pollutant concentration. The
reference electrode is used to maintain the working electrode at a constant electrical
potential during the sensing operation, and the counter electrode has a floating potential
to compensate for the generated current at the working electrode [61]. The opening of
the sensor has a gas-permeable membrane which prevents the electrolyte to leak from
the small chamber and decreases the interference of unintended pollutants [59]. Figure
2.2 illustrates the schematic of an electrochemical sensor.
Figure 2.2: Schematic of electrochemical sensors [59]
Page 27
Chapter 2. Literature Review 18
2.2.3 Optical Sensors
These sensors consist of a light source, band-pass filter, a sample chamber, and a detector.
They work based on sensing the deviation or absorption of light at a specific wavelength.
Light deviation is usually used to measure particulate matter, and absorption is applied
to monitor gaseous pollutants.
The Beer-Lambert law is used to quantify atmospheric pollutant levels when measured
with an optical sensor:
I = I0exp(−σ ×N × b) (2.1)
Where I0 and I are light intensity before and after crossing a sample, respectively, σ
is absorption cross-section (m2), N is concentration of the absorbing gas (molecule/m3),
and b is the length of the light path (m) [59]. One limitation of this type of sensor is its
large detection limit (> 10ppm), which makes it inappropriate for measuring atmospher-
ic levels of most pollutants [59]. Also, compounds with close absorption wavelengths
can interfere with each other. For example, water vapor interferes with measuring CO2
concentration. Figure 2.3 shows a schematic of these sensors.
Figure 2.3: Schematic of optical sensors [59]
Page 28
Chapter 2. Literature Review 19
2.3 Machine Learning Algorithms Used for Calibrat-
ing Sensors
While some sensors directly convert their output to a digital pollutant concentration
measurement, the outputs of most sensors are voltages or numbers proportional to the
pollutant levels. These outputs need to be related to actual concentrations through
Machine Learning algorithms. Four common models are explained here:
2.3.1 Multiple Linear Regression (MLR)
Multiple Linear Regression (MLR) is a method used to model a linear relationship be-
tween the concentration and one or more sensor outputs. This model is fit such that the
sum of squares of the differences between the observed values and predicted concentra-
tions is minimized [62].
Observed data→ y = b0 + b1X1 + ...+ bnXn + ε (2.2)
Predicted data→ y′= b0 + b1X1 + ...+ bnXn (2.3)
error→ ε = y − y′(2.4)
Minimize∑
(y − y′)2 (2.5)
Page 29
Chapter 2. Literature Review 20
This model has four assumptions:
• The outcome variable and the independent variables have a linear relationship with
each other.
• The residuals are normally distributed.
• The independent variables are not highly correlated with each other.
• The variance of errors is similar across the values of the independent variables.
This model usually works very well for electrochemical sensors; however, since the
assumptions are not always valid for a combination of EC and MOS sensors or for an
array of MOS sensors, non-linear models are usually more preferred.
2.3.2 Random Forest (RF)
Random Forest (RF) consists of several Decision Trees with a random subset of indepen-
dent variables. Every Decision Tree breaks down the dataset into smaller subsets and
finds rules to predict the target. The results of all the trees are averaged to make the
final decision. Figure 2.4 shows a Random Forest.
One problem with RF is that it can only predict values within the range of training
set, thus usually is not transferable from one place to another. For example, an RF model
trained on an unpolluted area is unable to estimate the peak values in a polluted area.
Page 30
Chapter 2. Literature Review 21
Figure 2.4: Schematic of a Random Forest algorithm [63]
2.3.3 Artificial Neural Network (ANN)
Artificial Neural Networks replicate the biological neural network of a living brain. It
is comprised of several layers of artificial neurons (or nodes) connected to each other to
form a network. There are three types of layers: input, hidden, and output layers. A
Neural Network has one input layer, one output layer, and one or more hidden layers.
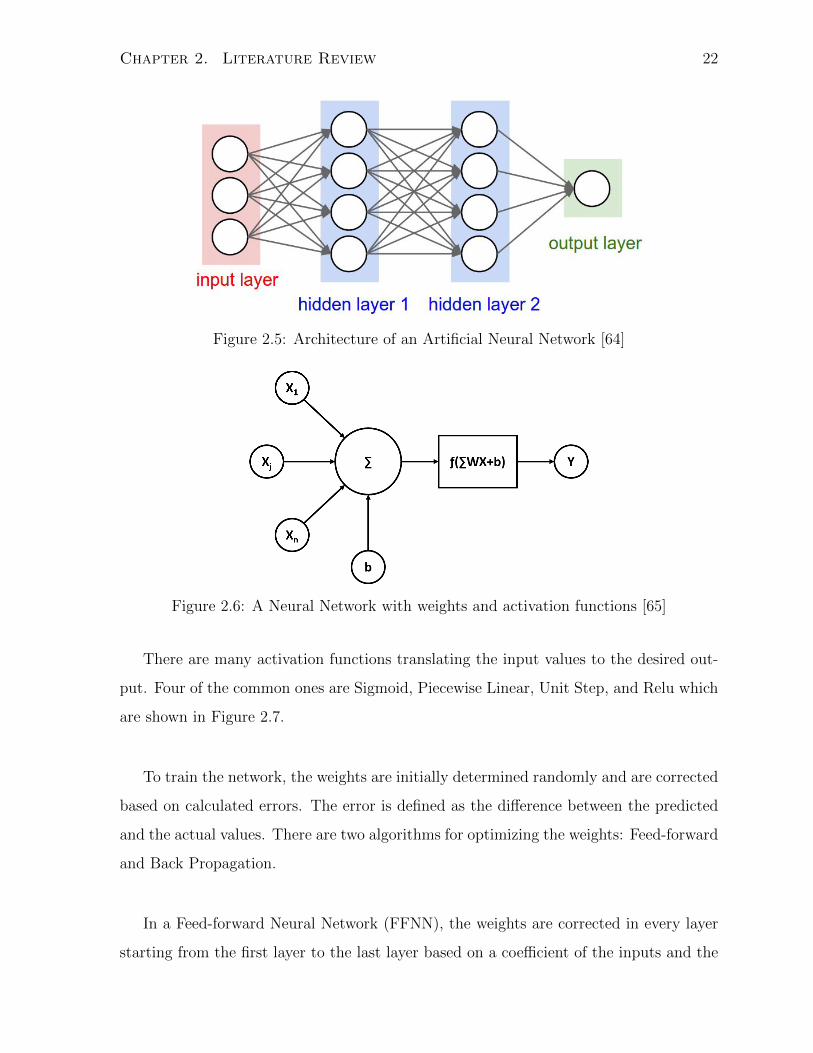
Figure 2.5 shows a typical network architecture.
The input data enters from the input layer and passes to the hidden layer. The values
are multiplied by weights when passing between nodes. Each node sums the values it
receives and modifies based on an activation function. This process continues to the
last layer of the network, which represents the final value; in our case is the predicted
concentration. Figure 2.6 shows how a Neural Network works.
Page 31
Chapter 2. Literature Review 22
Figure 2.5: Architecture of an Artificial Neural Network [64]
Figure 2.6: A Neural Network with weights and activation functions [65]
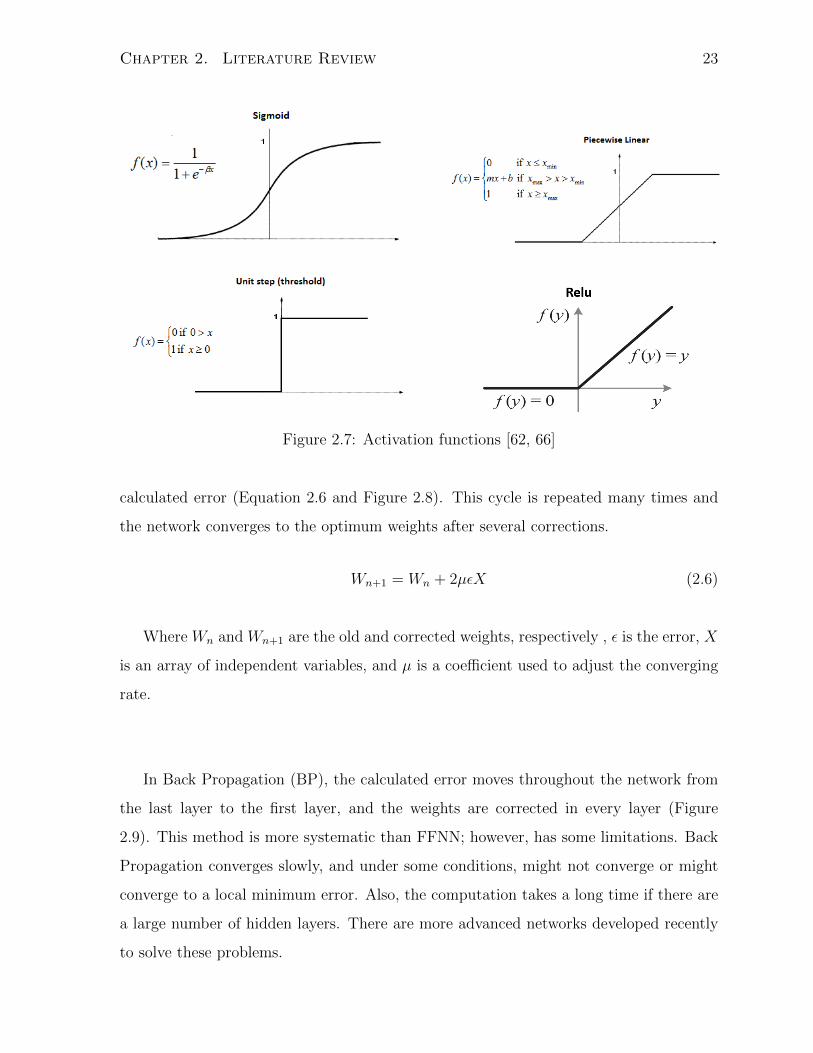
There are many activation functions translating the input values to the desired out-
put. Four of the common ones are Sigmoid, Piecewise Linear, Unit Step, and Relu which
are shown in Figure 2.7.
To train the network, the weights are initially determined randomly and are corrected
based on calculated errors. The error is defined as the difference between the predicted
and the actual values. There are two algorithms for optimizing the weights: Feed-forward
and Back Propagation.
In a Feed-forward Neural Network (FFNN), the weights are corrected in every layer
starting from the first layer to the last layer based on a coefficient of the inputs and the
Page 32
Chapter 2. Literature Review 23
Figure 2.7: Activation functions [62, 66]
calculated error (Equation 2.6 and Figure 2.8). This cycle is repeated many times and
the network converges to the optimum weights after several corrections.
Wn+1 = Wn + 2µεX (2.6)
Where Wn and Wn+1 are the old and corrected weights, respectively , ε is the error, X
is an array of independent variables, and µ is a coefficient used to adjust the converging
rate.
In Back Propagation (BP), the calculated error moves throughout the network from
the last layer to the first layer, and the weights are corrected in every layer (Figure
2.9). This method is more systematic than FFNN; however, has some limitations. Back
Propagation converges slowly, and under some conditions, might not converge or might
converge to a local minimum error. Also, the computation takes a long time if there are
a large number of hidden layers. There are more advanced networks developed recently
to solve these problems.
Page 33
Chapter 2. Literature Review 24
Figure 2.8: Feed Forward Neural Network
Figure 2.9: Back Propagation
Where X1 to Xn are input data, W1i to Wni are weights of the first to the nth nodes,
f is activation function, y′
is output of the network, and y is the reference measurement.
In BP, the weights are corrected using the output of the layers and the calculated
error:
Wn+1 = Wn + µδX (2.7)
Where Wn and Wn+1 are the old and corrected weights, respectively , µ is a coefficient
Page 34
Chapter 2. Literature Review 25
to adjust the converging rate, X is the input to every later, and δ is a function of error
and the output at every layer.
2.3.4 Recurrent Neural Network (RNN)
A Recurrent Neural Network (RNN) uses the previous predicted values to make a new
prediction. This algorithm is usually used for time series data, where the previous mea-
surements can affect the future values. For example, pollutant concentration at time tn
is affected by the concentration at time tn-1. The figure below shows the architecture of
this network.
Figure 2.10: Recurrent Neural Network
Where x0 to xn and y’0 to y’n are the inputs and predictions at each sequence, re-
spectively.
The challenge in using this calibration model is to decide an appropriate number of
previous predictions and training iterations. Applying too many of the previous pre-
dictions might bring some errors to the final prediction. Also, training the model for
excessive times might overfit the network on the training set.
Page 35
Chapter 2. Literature Review 26
2.4 Summary of the Chapter
In this chapter we reviewed the health effects of air pollution with a focus on premature
neonates. Among common pollutants, PM2.5 and NO2 have the most acute outcomes.
We introduced three types of low-cost sensors. Metal Oxide Semiconductor sensors work
based on changes in the conductivity of their active surface. Electrochemical sensors
are based on reduction-oxidation reactions between pollutants and the electrodes inside
the sensor, and optical sensors are based on light deviation or absorption at a specific
wavelength. Lastly, we introduced four common algorithms used to calibrate low-cost
sensors.
Page 36
Chapter 3
Methodology
3.1 Study Site
This research was conducted at a Canadian hospital located on the corner of two major
roadways and close to a highway. The sampling was performed near the air intake on
the third floor and from a medical air outlet in a patient room on the fourth floor for ap-
proximately seven months from November 2017 to June 2018. The concentration of CO,
CO2, nitrogen oxides (NOx), O3, Black Carbon (BC), and ultrafine particles (UFP) were
monitored on both locations simultaneously. The gaseous pollutants except CO2 were
monitored by a low-cost air pollution measuring device known as AirSENCE, which is
equipped with several Metal Oxide, two Electrochemical, and temperature and Relative
Humidity (RH) sensors. Carbon Dioxide was monitored by an optical sensor independent
from the AirSENCE. Black Carbon and UFP were measured using microAeth and DiS-
Cmini particle counter, respectively. To monitor the medical air, all the portable devices
were placed inside a sampling box connected to an outlet (Figure 3.1 a and b). Electro-
chemical and optical sensors work at atmospheric pressure, so the box was designed to
attenuate high pressure of medical air. It was about 130 liters, equipped with an inlet
and an outlet valve to control the air flow, and a pressure gauge to ensure the internal
pressure is at atmospheric level. Table 3.1 demonstrates the specification of the sensors
and the portable devices.
27
Page 37
Chapter 3. Methodology 28
(a) Sampling box connected to a med-ical air outlet.
(b) Portable devices were placed insid-e the sampling box.
Figure 3.1: Sampling box
Table 3.1: Specifications of the portable devices
Instrument Target Pollutant Time Resolution
AirSENCE NO, NO2, CO, O3 1 sec
Senseair K30 CO2 2 sec
microAeth BC 10 sec
DiSCmini UFP (10-300 nm) 10 sec
Page 38
Chapter 3. Methodology 29
Table 3.2: List of sensors applied to this study
Sensor Name Target PollutantSensor
Type
Interfering
Pollutant
Senseair K30 CO2 Optical Water vapor
Plantower PMS
7003PM10, PM2.5, PM1 Optical -
DHT22Temperature, Relative
Humidity- -
NO-B4 NO EC
H2S, NO2,CL2,
SO2, H2, CO,
NH3, CO2, O3
[67]
CO-B4 CO EC
H2S, NO2,CL2,
NO, SO2, H2,
C2H4, NH3 [68]
MQ131 O3 MOS -
MiCS-5521CO, Hydrocarbons, Volatile
Organic CompoundsMOS -
MiCS-5524 CO, H2,NH3,CH4, Ethanol MOS -
MiCS-5526 CO, H2,NH3,CH4, Ethanol MOS -
MiCS-4514
ReductionCO, Hydrocarbons MOS -
Page 39
Chapter 3. Methodology 30
MiCS-4514
OxidationNO2 MOS O3
MiCS-2614 O3 MOS -
MQ-3Alcohol, Benzene, CH4,
Hexane, LPG, COMOS -
SN706 NOx MOS -
TGS2620
CO, CH4, H2, Ethanol,
Iso-butan, Organic Solvent
Vapors
MOS -
TGS2600
CO, CH4, H2, Ethanol,
Isobutane, Organic Solvent
Vapor
MOS -
TGS822
CO, CH4, n-Hexane,
Benzene, Ethanol, Acetone,
Iso-butan, Organic Solvent
Vapor
MOS -
Page 40
Chapter 3. Methodology 31
3.2 Sensor Calibration
3.2.1 Calibration Site and Instrumentation
All the portable devices were calibrated beside reference instruments for two weeks at the
Wallberg Building, at a height of approximately 15 meters, in downtown Toronto prior to
deploying at the hospital. The reference instruments represent accurate concentrations
and are calibrated regularly. Table 3.2 lists these reference instruments.
Table 3.3: Reference instruments
Instrument Target Pollutant
NOx Thermo 42i NO, NO2
Thermo 49c O3
LICOR LI-840A CO2, H2O
Thermo 48i-TLE CO
3.3 Data Analysis
3.3.1 Data Preparation
Prior to performing any data analysis, all the negative, extremely large, or false mea-
surements were removed. There are two main steps before training and deploying a
calibration model: averaging and scaling. Averaging alleviates the noise and increases
the confidence; however, averaging to a low time resolution might omit instant variations.
In our study, a 5-minute time resolution was reasonable for keeping the detail of events
while reducing the noise.
Scaling is a very important step when building a neural network model. It makes
Page 41
Chapter 3. Methodology 32
the range of variables closer, and decreases the training time. There are two ways of
scaling, Normalization and Standardization. Normalization (Equation 3.1) makes the
variable range between zero and one, while standardization (Equation 3.2) makes the
mean equal to zero and the standard deviation equal to one. In this research, we chose
Standardization because the mean and standard deviation are less likely to change with
the sample size.
Normalization: Z =x− xmin
xmax − xmin
(3.1)
Standardization: Z =x− µσ
(3.2)
Where Z is the scaled value, x is the variable, xmin and xmax are the minimum and
maximum values, respectively, µ is the mean, and σ is the standard deviation.
3.3.2 Data Exploration
We explored the data by means of statistical and visualization techniques to find impor-
tant aspects of each variable and the relationship between them. Variables’ distributions
were visualized on histogram and box plots, and correlation analysis was performed be-
tween every two sensors and between sensors and pollutants.
3.3.3 Generating Calibration Models
To build the calibration models, the sensors worked beside the reference instruments for
about two weeks, then the dataset was divided into two sets, a training set and a test
set. The calibration model is trained on the training set and the performance is verified
on the test set. Majority of the data is used for training and the rest is used for testing;
in this research we used 70% of the data for building the models and 30% for verifying
them. The dataset is usually divided randomly for most of the calibration algorithms;
however, for Recurrent Neural Network we keep the sequence of the data because every
estimated value is used in predicting the next few measurements. So, the last 30% of the
Page 42
Chapter 3. Methodology 33
calibration data was used for testing RNN model.
The R programming language was used to build Multiple Linear Regression, Random
Forest, and Neural Network models, and Recurrent Neural Network was built in Python,
using the Tensorflow library. The models were compared, and the best one was chosen
based on the R2 value and how the model tracks the reference instrument. The sensors
used in every model were initially determined by a function named ”regsubsets” in the
Leaps package in R, which takes a random set of variables and calculates the adjusted
R2 of the best fitted model several times. Then sensors were added or removed step by
step to find the best combination of variables.
3.3.4 Evaluating Calibration Models
To evaluate the calibration models we applied them on the test set and fit a linear model
on the scatter graph of the predicted values against the reference instrument. The slope
of the line represents accuracy of the calibrated model, and ideally should be one, which
means the reference instrument and the model estimate the same values. The intercept
compares the model’s baseline with the reference data, with a large intercept indicating
majority of the predicted values are above or below the actual concentration. R2 of the
line represents how much of the variability is accounted by the model, with a R2 closer
to one indicating the model can predict a large portion of variability of the dataset.
Also, the Root Mean Squared Error (RMSE) of the calibration models were compared
to choose the best model.
3.4 Calibrating CO2 Sensors
We calibrated a Senseair K30 CO2 sensor under laboratory conditions using CO2 cali-
bration gas. The effect of humidity on the sensor’s readings was tested under controlled
conditions. Also, calibration models were built based on environmental temperature,
relative humidity, and pressure.
Page 43
Chapter 3. Methodology 34
3.4.1 Investigating the Effect of Humidity on the CO2 Sensor
Optical low-cost CO2 sensors work based on absorbing light at infrared wavelengths.
Water vapor has a strong absorption close to this wavelength and can interfere with CO2
readings. To test the effect of humidity on the Senseair K30 sensor, a vaporizer was
placed beside the temperature, RH, and the CO2 sensor inside the sampling box. The
medical air valve was opened for several minutes to fill the box, and then the inlet and
outlet were closed. Then the CO2 sensor was allowed to work for about 5 min before
turning on the vaporizer to find the initial readings. Then the vaporizer was repeatedly
turned on for about 30 sec, then off for 2 minutes to slowly increase the humidity. The
signals were averaged in every step and changes in the reported CO2 concentration were
observed to see how vapor interfered based on the Beer-Lambert law.
3.4.2 Calibrating CO2 Sensors Under Real Conditions
Two different sites with different concentrations and available reference data were used
for calibration and evaluation of the models. The first site was located at the Wallberg
Building, and the second site was next to the highway 401, in Toronto. A Random
Forest and a Multiple Linear Regression were trained and tested on the data, and the
improvement of the readings and transferability of the models were evaluated at both
sites.
3.5 Summary of the Chapter
This study was performed at a hospital near highway, and portable low-cost devices
were used to measure the concentration of NOx, O3, CO, CO2, BC, and UFP. The gas
sensors’ outputs were calibrated against reference instruments prior to starting the study.
Four calibration algorithms were trained at Wallberg Building and the best model was
chosen based on RMSE, R2, and scatter plot of the estimated values against the reference
instruments. The effect of humidity on the CO2 sensor was studied under controlled and
real conditions.
Page 44
Chapter 4
Results and Discussion
4.1 Exploring Calibration Data
Carbon monoxide, carbon dioxide, and nitrogen oxides concentration distributions at the
calibration site are positively skewed. Carbon monoxide concentration varies over a wide
range from less than 100ppb to 500ppb, with outliers spreading to 800ppb, while carbon
dioxide level is mostly focused around 420ppm. The concentration of nitrogen oxides
mostly ranged from about 7ppb to 20ppb, which is above the detection limit of the NOx
sensors (> 5ppb). Ozone had a wider distribution ranging from > 5ppb to about 60ppb.
Temperature and RH had a quite broad range from 5 ◦C to 25 ◦C and 30% to 90%,
respectively. Histogram and box plots of the pollutants are shown in Figure 4.1.
35
Page 45
Chapter 4. Results and Discussion 36
Figure 4.1: Histograms and box plots of pollutants concentration at the calibration site.
Page 46
Chapter 4. Results and Discussion 37
The two AirSENCE devices used in this study, were equipped with different sets of
sensors. AirSENCE #1 had an Electrochemical CO sensor (CO-B4) which is not includ-
ed on the other device, while AirSENCE #2 contained more metal oxide CO and NOx
sensors.
Electrochemical sensors have two outputs, from a working electrode (WE) and auxil-
iary electrode (AE). The WE output was correlated with temperature and the pollutant
concentration, whereas AE was also exponentially proportional to temperature and used
to correct the WE readings. Temperature was a determining parameter affecting sensor
performance and was correlated with both Electrochemical and Metal Oxide sensors.
Ozone was one of the key interfering pollutants, correlated with most of the sensors,
especially NO and NO2. The MOS sensors were mostly correlated with ozone, nitrogen
dioxide, and carbon monoxide. Also, some of the MOS sensors were strongly inter-
correlated, indicating their cross-sensitivity to different pollutants. Figure 4.2 shows the
correlation analysis between all sensors and pollutants.
Page 47
Chapter 4. Results and Discussion 38
(a) AirSENCE #1
(b) AirSENCE #2
Figure 4.2: Correlation matrix of all sensors and pollutants.
Page 48
Chapter 4. Results and Discussion 39
4.2 Feature Selection
The features were initially selected based on correlation analysis and the results from the
regsubsets function. This function uses maximum likelihood method to build a search
tree for finding the best fitting models of different sizes and builds an MLR model on
each subset. Figure 4.3 shows the output of this function. Each row in these graphs
represents a model; the shaded rectangles in the columns indicate the variables included
in the given model. The numbers on the left margin are the adjusted R2 values in
order; the highest and the lowest numbers represent the maximum and the minimum R2s
achieved, respectively. The darkness of the shading simply represents the ordering of the
R2 values. As an example, the red bar shown in Figure 4.3 b indicates a model which has
an adjusted R2 around 0.93 and its variables are Temperature, MiCS5121, MiCS4514 OX,
TGS880, MiCS2614 1, and MiCS2614 2. The sensors that have no shading were a weak
predictor of the target pollutant and were not selected in any of the subsets, such as
TGS822 and MiCS5526 in this figure.
Page 49
Chapter 4. Results and Discussion 40
(a) Ozone on AirSENCE #1 (b) Ozone on AirSENCE #2
(c) Nitrogen Oxides on AirSENCE #1 (d) Nitrogen Oxides on AirSENCE #2
(e) Carbon Monoxide on AirSENCE #1 (f) Carbon Monoxide on AirSENCE #2
Figure 4.3: Results of regsubsets function for selecting models’ independent variables.
Page 50
Chapter 4. Results and Discussion 41
The sensors which were more frequently used and had led to a higher R2 were se-
lected as the main features. Other parameters were included if they improved the R2
significantly. Table 4.1 shows the parameters selected for predicting each pollutant.
Table 4.1: Selected sensors for building calibration models
Pollutant AirSENCE # 1 AirSENCE #2
O3
Temperature, TGS2620 Temperature, TGS2620
MQ131, MiCS5524 MiCS5524, MiCS5121
TGS822 MiCS4514-OX, TGS880
TGS2600
NOx
Temperature, TGS2620 Temperature, NO-B4-WE
NO-B4-WE, NO-B4-AE NO-B4-AE, MiCS4514-OX
MiCS4514-OX, MiCS5524 SN706
TGS822
CO
TGS2620, TGS2600 Temperature, TGS2620
MiCS4514-OX, MiCS5524 TGS822, MiCS5524
CO-B4-WE, CO-B4-AE MQ3, TGS880
MQ3 MiCS4514-RED
Page 51
Chapter 4. Results and Discussion 42
4.3 Evaluating and Comparing Calibration Models
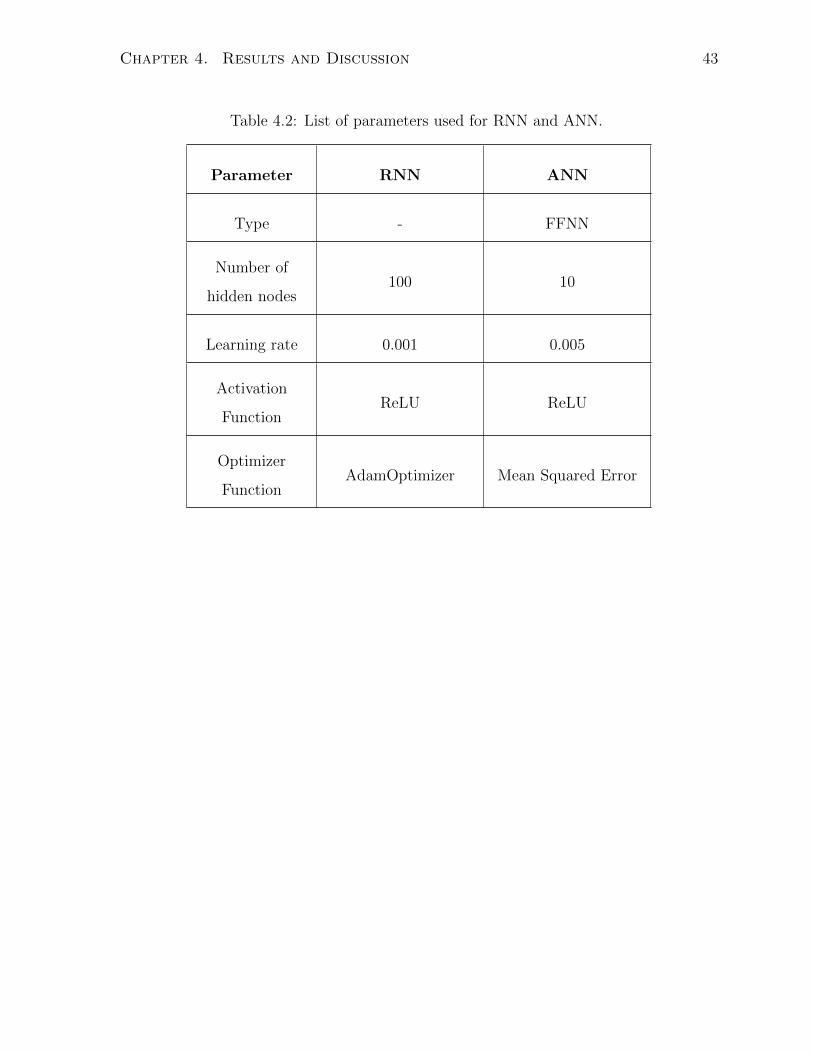
Four calibration models were trained on both devices, the parameters used for RNN and
ANN models are specified in Table 4.2. The R2, slope, and intercept of the predictions
against the reference line, and RMSE were considered for model evaluation and compar-
ison. Table 4.3 indicates the models’ performance on the training set.
Random Forest had the best performance on the training data with the highest R2
(≥ 0.98) and the lowest RMSE for all the pollutants on both devices. The slope of this
model is very close to one (≥ 0.92) and the intercept is small relative to the range of the
pollutants concentration. However, this model cannot extrapolate measurements above
or below the training range [69], and the predictions are usually not transferable from
one place to another, thus it is not preferred over other models.
After Random Forest, Recurrent Neural Network has the highest R2, but its RMSE
is close to MLR, thus this needs to be studied in more detail. Since this model uses the
previous outputs to estimate new measurements, missing values in a dataset can cause
significant errors. Also, this model is prone to overfit on the training data in a few it-
erations. Although Multiple Linear Regression has a comparable RMSE to RNN, it is
more scattered and less accurate. The testing results of these two models were compared.
RNN and MLR were applied on the test set to select the best model for each pollutant.
The results are summarized in table 4.4. Although RNN performs better than MLR on
the training set, its R2 is not as high on the test set, except for NOx on the second device.
The slopes of the two models are close for most of the pollutants, except O3 on device
#1 (RNN: 0.41 and MLR: 0.84) and NOx on device #2 (RNN: 0.95 and MLR: 0.56).
However, MLR has a smaller RMSE for all the pollutants, and the intercept is close to
zero for NOx and O3.
Page 52
Chapter 4. Results and Discussion 43
Table 4.2: List of parameters used for RNN and ANN.
Parameter RNN ANN
Type - FFNN
Number of
hidden nodes100 10
Learning rate 0.001 0.005
Activation
FunctionReLU ReLU
Optimizer
FunctionAdamOptimizer Mean Squared Error
Page 53
Chapter 4. Results and Discussion 44
Table 4.3: Comparing calibration models’ performance on the training set
Pollutant Model
AirSENCE #1 AirSENCE #2
RF RNN MLR ANN RF RNN MLR ANN
O3
R2 0.99 0.94 0.81 0.43 1.00 0.98 0.94 0.30
Slope 0.96 0.94 0.85 0.79 0.98 0.98 0.94 0.77
Intercept 0.92 1.49 3.71 1.67 0.30 0.42 1.53 4.42
RMSE 1.11 2.98 4.69 11.0 0.67 3.27 1.98 16.9
NOx
R2 0.99 0.96 0.75 0.07 0.98 0.73 0.59 0.13
Slope 0.96 0.95 0.75 0.67 0.92 0.95 0.59 0.36
Intercept 0.63 0.70 4.13 0.07 1.01 -5.27 5.19 6.31
RMSE 1.49 3.27 7.34 37.9 1.78 3.75 7.34 13.5
CO
R2 0.99 0.85 0.76 0.39 0.98 0.90 0.71 0.30
Slope 0.96 0.86 0.76 0.47 0.95 0.93 0.70 0.54
Intercept 0.98 0.90 0.71 140 15.70 24.3 94.30 166
RMSE 11.6 42.7 48.1 78.0 17.5 46.5 73.9 128
Page 54
Chapter 4. Results and Discussion 45
Table 4.4: Comparing RNN and MLR’s performance on the test set
Pollutant Parameter
AirSENCE #1 AirSENCE #2
RNN MLR RNN MLR
O3
R2 0.51 0.81 0.89 0.94
Slope 0.41 0.84 0.92 0.93
Intercept 3.71 -0.69 3.71 1.91
RMSE 8.62 4.97 4.73 3.40
NOx
R2 0.41 0.81 0.73 0.58
Slope 0.70 0.84 0.95 0.56
Intercept 24.9 4.12 -5.27 5.45
RMSE 23.34 6.84 9.01 7.66
CO
R2 0.33 0.69 0.42 0.69
Slope 0.67 0.72 0.68 0.70
Intercept 15.7 74.10 85.6 97.9
RMSE 99.2 53.7 86.7 74.3
Page 55
Chapter 4. Results and Discussion 46
The box plots of the predictions on the test set were compared with the reference
measurements, which is shown in Figure 4.4. The median, first, and third quantiles of
the MLR model on both AirSENCEs are very close to the reference data for all the pol-
lutants, whereas RNN has a noticeable difference. Also, MLR predictions vary in a closer
range to the reference measurements for NOx and CO and can better estimate the outliers.
Based on all the analyses discussed above, Multiple Linear Regression was selected
and applied to predict the pollutants concentration at the hospital.
(a) Ozone on AirSENCE #1 (b) Ozone on AirSENCE #2
.
Page 56
Chapter 4. Results and Discussion 47
(c) Nitrogen Oxides on AirSENCE #1 (d) Nitrogen Oxides on AirSENCE #2
(e) Carbon Monoxide on AirSENCE #1 (f) Carbon Monoxide on AirSENCE #2
Figure 4.4: Comparing box plots of RNN and MLR predictions with the reference mea-surements.
Page 57
Chapter 4. Results and Discussion 48
4.4 Calibrating CO2 Sensors
The CO2 sensor was calibrated using calibration CO2 and zero gases. The sensor was
placed inside a small chamber and CO2 concentration was increased from zero to 1000ppm
by 100ppm intervals, while RH and temperature were held constant at around 4% and
22.4 ◦C (Figure 4.5.a). The CO2 reading at each level was averaged and plotted against
the actual concentration, as shown in Figure 4.5.b. The slope and R2 of the fitted line
were very close to one indicating that the sensor is potentially very accurate, but the
intercept was significant.
(a) Increasing CO2 concentration with 100ppm intervals
Page 58
Chapter 4. Results and Discussion 49
(b) Measured CO2 concentration Vs. the actual level
Figure 4.5: Calibrating a K30 CO2 sensor using calibration gases.
The CO2 sensor was then calibrated outdoors based on the environmental parameters.
The sensor was operated at a site beside highway 401 for two weeks before the calibration.
Figure 4.6 compares the K30 CO2 readings with the reference measurements and shows
the pressure, temperature, and partial pressure of water vapor (PWater). Pressure was
measured by the reference instrument, while temperature and RH were measured by the
AirSENCE. PWater was calculated from the Antoine Equation:
PSat = 108.07131−
1730.63
233.426 + T (4.1)
PWater = RH × PSat (4.2)
Where PSat is the saturated vapor pressure in mmHg, T is temperature in ◦C, and
the calculated PWater is in mmHg.
Page 59
Chapter 4. Results and Discussion 50
Figure 4.6: Pressure, temperature, partial pressure of water vapor, and CO2 level athighway 401 and its comparison to the K30 readings.
An MLR and a RF models were used to correct the sensor readings for the effect of
temperature and water vapor. The slope and R2 of the corrected values against the ref-
erence instrument were 0.86 and 0.98 for MLR and RF, respectively, and the intercepts
were small compared to the range of the concentration (Figure 4.7 a and b). To test
the transferability of the models, they were applied to a data collected at the Wallberg
Building.
K30 CO2 sensor had a built-in Automatic Background Calibration (ABC) algorith-
m that allowed the sensor to dynamically shift its CO2 reading by a constant. This
algorithm compared the minimum reported measurement with the approximate global
average CO2 concentration of 400 ppm and added a value to sensor’s readings. Although
this sensor had an acceptable accuracy without any correction, this algorithm caused two
clusters of data, circled in Figure 4.7 a.
Page 60
Chapter 4. Results and Discussion 51
(a) Multiple Linear Regression
(b) Random Forest
Figure 4.7: Calibrating a CO2 sensor based on environmental parameters.
Page 61
Chapter 4. Results and Discussion 52
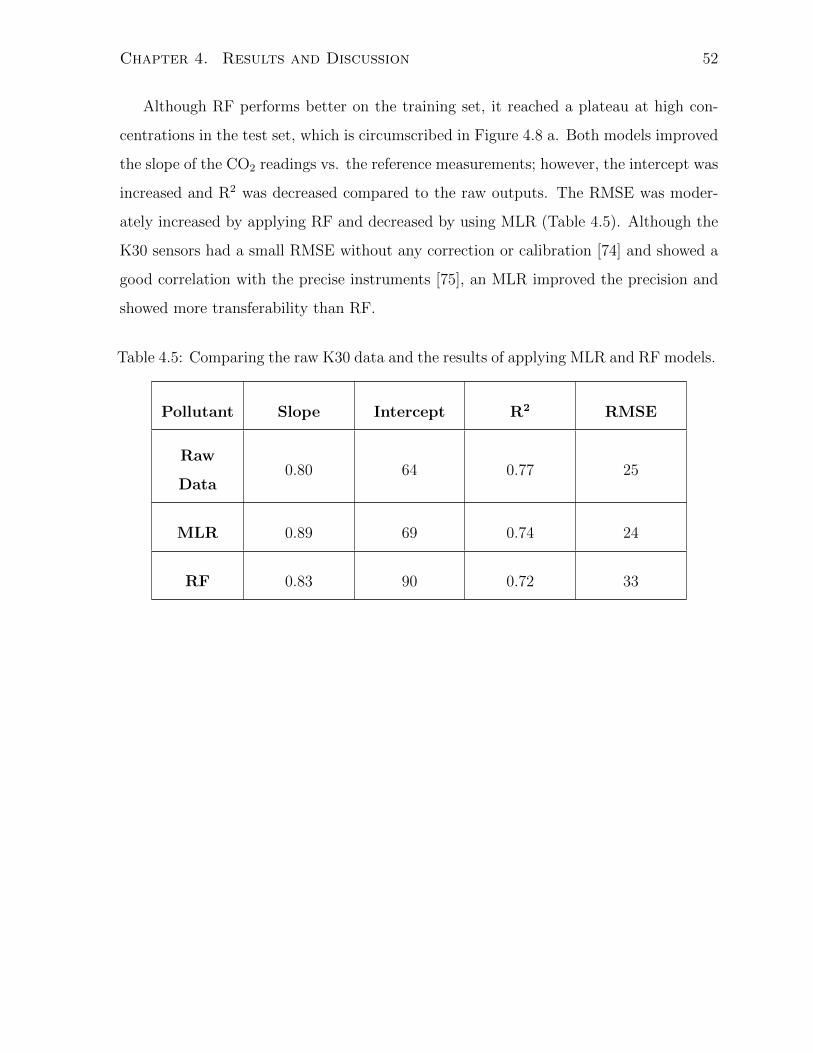
Although RF performs better on the training set, it reached a plateau at high con-
centrations in the test set, which is circumscribed in Figure 4.8 a. Both models improved
the slope of the CO2 readings vs. the reference measurements; however, the intercept was
increased and R2 was decreased compared to the raw outputs. The RMSE was moder-
ately increased by applying RF and decreased by using MLR (Table 4.5). Although the
K30 sensors had a small RMSE without any correction or calibration [74] and showed a
good correlation with the precise instruments [75], an MLR improved the precision and
showed more transferability than RF.
Table 4.5: Comparing the raw K30 data and the results of applying MLR and RF models.
Pollutant Slope Intercept R2 RMSE
Raw
Data0.80 64 0.77 25
MLR 0.89 69 0.74 24
RF 0.83 90 0.72 33
Page 62
Chapter 4. Results and Discussion 53
(a) Random Forest
(b) Multiple Linear Regression
Figure 4.8: MLR and RF calibration results Vs. the reference measurements at theWallberg Building.
Page 63
Chapter 4. Results and Discussion 54
4.5 Investigating the Cross-Sensitivity of the CO2
Sensor to Water Vapor
To investigate the effect of humidity on the CO2 readings, a vaporizer was placed inside
the sampling box, and humidity was increased gradually (Figure 4.9 a). As the humidity
rose, the sensor detected higher levels of CO2, which indicated its cross-sensitivity to
water vapor. The temperature, relative humidity, and CO2 measurements were averaged
in every constant humidity period (Figure 4.9 b). The CO2 measurements increased from
480ppm to 620ppm by increasing RH from zero to 70%, while temperature decreased for
only about 0.5 ◦C, which is considered negligible. The rise in the CO2 readings should
be proportional to the absorption by water vapor.
The Beer-Lambert law was used to calculate the equivalency in the light wave ab-
sorption of CO2 and water vapor.
Absorption: A = 0.4343×N × σ × b (4.3)
A∆CO2= A∆V apor → N∆CO2
× σ∆CO2= N∆V apor × σ∆V apor (4.4)
Thus: N∆CO2=σ∆V apor
σ∆CO2
N∆V apor (4.5)
Where A is absorption, N is number density of the gas molecules (molec/m3), σ is
absorption cross section, and b is the length of the sample.
The number density of added water molecules has a linear relationship with the num-
ber density of the CO2 molecules which could increase the sensor readings to the same
measurements if were added to the air. The slope of this line is the ratio of vapor to CO2
absorption cross sections. From literature, the absorption cross sections of carbon dioxide
and water vapor at the CO2 absorption wavelength of 4.3 µm are 6.74× 10-24cm2/molec
and 1.20× 10-25cm2/molec, respectively [76].
Page 64
Chapter 4. Results and Discussion 55
∆CO2 and ∆V apor at each step were calculated by subtracting the initial CO2 and
RH from their respective values at every point and number densities of gases were calcu-
lated using the ideal gas law. The values used in this experiment are the direct outputs of
the sensor and no calibrations are applied to the measurements. To improve the calcula-
tions, only points 1 to 7 of the CO2 curve in Figure 4.9 b were used to plot N∆CO2against
N∆V apor, and a line of best fit was found for the graph (Figure 4.9 c). The intercept of
this line was forced to zero and the response time of the sensors were removed prior to
calculations.
(a) Effect of increase in RH on CO2 measurements
Page 65
Chapter 4. Results and Discussion 56
(b) Average of temperature, RH, and CO2 readings at each step
(c) N∆CO2Vs. N∆V apor
Figure 4.9: Investigating the effect of humidity on the K30 CO2 sensor.
Page 66
Chapter 4. Results and Discussion 57
The absorption cross section ratio is 0.0178 and the slope of this line of 0.0174 is
consistent with this ratio given the spread in the data; therefore, our experimental values
match with that expected in theory. At high humidities, vapor condensates can cover
the surface of the light detectors inside the sensor and decrease its sensitivity; points 7
to 9 in Figure 4.9 b show that CO2 measurements deviate from the expected ascending
trend at high humidities.
For more investigation, these calculations were repeated for every period where both
RH and CO2 measurements were falling simultaneously. N∆CO2against N∆V apor graph
is shown in Figure 4.10.
Figure 4.10: Investigating the effect of humidity in the dropping periods.
Part of the data is consistent with the ratio of 0.0178; however, the slope of the best
fit line deviated from the theoretical value, which could be because at higher humidities
the peak CO2 measurements were lower than expected.
Page 67
Chapter 4. Results and Discussion 58
This experiment demonstrates the effect of humidity on the sensor outputs; however,
in real conditions, the calibration models should be applied to correct the measurements.
Thus, we applied our calibration model discussed in section 4.4 on this experimental
data.
Figure 4.11: Applying calibration model on the data from the humidity experiment.
This figure shows that the calibration model slightly improved the measurements,
and the difference between the calibrated data and original values increased by increas-
ing humidity; however, ideally the values at high humidities should be close to the first
measurement after calibration. This inefficiency of the model could be because humidity
and CO2 concentrations in this experiment have wider ranges than in real condition-
s. Figure 4.12 compares the distributions of humidity and CO2 concentrations in this
experiment and at highway 401.
Page 68
Chapter 4. Results and Discussion 59
(a) Distribution of absolute humidityin this experiment.
(b) Distribution of absolute humidityat highway 401.
(c) Distribution of CO2 concentrationin this experiment.
(d) Distribution of CO2 concentrationat highway 401.
Figure 4.12: Comparing the distribution of humidity and CO2 concentrations in thisexperiment and at highway 401.
Page 69
Chapter 4. Results and Discussion 60
Also, sensor measurements under real conditions are very close to the reference values
and follows the variations very well (Figure 4.13 a and b). This makes the calibration
model to significantly relay on the CO2 sensor. Table 4.6 shows the coefficients of the
calibration model. Larger coefficient of the CO2 sensor shows that this parameter is more
influencing the calibrated concentrations.
Table 4.6: Coefficients of the calibration model.
CO2 sensor
(mol/m3)
Humidity
(mol/m3)Temperature
Coefficient 0.98 -0.002 -0.00026
(a) Box plots of the reference CO2 con-centrations and sensor measurements.
(b) Time series of the reference CO2 con-centrations and sensor measurements.
Figure 4.13: Comparing the reference CO2 concentrations and sensor measurements.
Page 70
Chapter 4. Results and Discussion 61
4.6 Application to Air Quality Monitoring at the
Hospital and Wallberg Building
After calibration, the sensors’ outputs at the hospital were transferred to concentrations.
The measurements show that only 17% of the outdoor CO was removed in the medical
air system, while CO2 concentration in the outlet was as high as the outdoor air. The
diurnal patterns of CO and CO2 in the medical air were strongly correlated to those
outdoors (0.82 and 0.96, respectively), which is shown in Figure 4.14. Also, the time
series monitoring data of the Medical, shown in Figure 4.15 indicated that the CO and
CO2 concentrations in the medical air and strongly followed the outdoor trend and that
changes in the inlet concentrations were rapidly delivered to the outlet. The CO2 con-
centration in the medical air in 2% of the time passed the USP standard level of 500ppm,
when the outdoor level was at peak; one of the concentration exceedances is indicated in
Figure 4.15.a. This agrees with findings from Edwards et al (2018), who demonstrated
that CO2 level in the medical air exceeds the USP threshold at 1% of the time [4]. The
large confidence interval of the medical air curve in Figure 4.14 shows that CO2 level
varied over a wide range. This could be because the activated alumina used in desiccant
dryers can capture CO2 [70], and release it throughout the course of several days.
Page 71
Chapter 4. Results and Discussion 62
Figure 4.14: Diurnal patterns of CO and CO2 concentration
Page 72
Chapter 4. Results and Discussion 63
(a) CO2 concentration
(b) CO concentration, USP threshold is 10ppm.
Figure 4.15: Comparison between time series concentrations in medical air and outdoorair.
Page 73
Chapter 4. Results and Discussion 64
Although no gas filters were installed in the medical air system, the concentrations of
NOx and O3 were about half of those in the outdoor air. Specifically, 45% and 43%, of
the NOx and O3 , respectively, were removed relative to the outdoor air. Although, their
concentrations had a very small variation, the diurnal patterns of these pollutants in the
medical air were partially related to the outdoor air, which shows that ambient air pol-
lution has affected pollutant concentrations in medical air. For more details please refer
to Appendix B. Unlike, the low concentrations of NOx and O3 observed in this research,
Benzing et al. (1999) and Nakata et al. (2002) measured significant levels of NOx in
medical air [21, 22]. Several parameters could cause this contrast, such as length of the
pipelines and type of the catalysts used in the dryers. NOx can react with atomic copper
and copper (II) oxide (CuO) under certain circumstances [71, 72], and long pipelines can
provide enough residence time for the reactions. In addition, zeolite type desiccants can
absorb nitrogen dioxide at room temperature [73]. Further the outdoor concentrations
of these pollutants may have been higher in these earlier studies. The small confidence
interval of NOx and O3 concentrations in the medical air indicates their small ranges of
variation (Figure 4.16).
Page 74
Chapter 4. Results and Discussion 65
Figure 4.16: Diurnal patterns of O3 and NOx concentration
Page 75
Chapter 4. Results and Discussion 66
Fortunately, UFP and BC were more than 97% filtered and their correlation to the
outdoor concentrations was low, indicating that the filters were properly working. Their
tight confidence intervals shown in Figure 4.17 illustrates that their concentrations are
around zero most of the time. Table 4.7 summarizes the removal ratio of each pollutant.
Table 4.7: Removal ratio of each pollutant in the medical air.
PollutantRemoval
Ratio
CO2 0.01
CO 0.17
NOx 0.45
O3 0.43
UFP 0.98
BC 0.97
Page 76
Chapter 4. Results and Discussion 67
Figure 4.17: Diurnal patterns of UFP and BC concentration
Page 77
Chapter 4. Results and Discussion 68
4.7 Summary of the Chapter
In this chapter we explained four steps of datamining, namely data exploration, building
calibration models, evaluating the models, and deploying them at a new study site.
In data exploration, pollutants were visualized on histogram graphs and a correlation
analysis was performed between all the parameters. To predict pollutant concentrations,
input parameters were selected based on the correlation analysis, and improvement in
R2 of the fitted models. Four calibration models were trained and compared with each
other. The best model was selected based on RMSE of the predictions and reference
measurements and the R2, slope, and intercept of the best fitted line on predictions Vs.
reference values plot. Random Forest had the best results on the training set, however,
does not work as well as MLR at other sites. RNN also has a good performance, but
overfits on the training set, and ANN did not have a high R2 for most of the pollutants,
so MLR was selected to estimate the pollution levels in the inlet and outlet of the medical
air system. A CO2 sensor was calibrated under laboratory conditions and in the outdoor
environment. The CO2 sensor showed promising reliability comparing to the reference
instrument, but is cross-sensitive to water vapor and should therefore be corrected for
the effects of environmental parameters. The results showed that CO and CO2 taken
from outdoors were delivered unchanged to the patient rooms, while NOx and O3 were
more than 40% removed, were still present. Ultrafine particles and black carbon were
more than 97% removed, showing that the particulate filters were working properly in
the medical air system.
Page 78
Chapter 5
Conclusion and Future Work
The goal of this research was to investigate the effect of outdoor air pollution on the
quality of medical air produced on-site in health care facilities for breathing purposes.
This research showed that low-cost sensors can be deployed at hospitals to monitor the
quality of medical air, and showed that the pollutants concentration in the medical air
is a strong function of the outdoor air quality. Also, this research indicated that the
medical air standards allow for concentrations far above ambient levels, and that levels
of pollution allowed in medical air could potentially cause negative health outcomes. In
the future, the medical air regulations should be revised to include a standard for ozone
and other common pollutants and correct the current limits of other pollutants to be
more aligned fit ambient air quality standards. There seems to be no reason to justify
why hospital patients including neonatal babies should be allowed to experience much
higher exposure to air pollution than the general public.
The next step in this research might be to develop a monitoring setup compatible
with the hospitals’ environment to continuously measure the levels of pollution in med-
ical air in the patient rooms. Being aware of the air pollution concentration in medical
air should help medical professionals make informed decisions on providing a better air
quality for sensitive patients.
One possible solution for purifying the medical air is to install gas pollution filters in
69
Page 79
Chapter 5. Conclusion and Future Work 70
the medical air system or in the patient rooms. This solution is more suitable in polluted
cities where the outdoor air needs to be continuously cleaned, or at hospitals with an old
medical air system where the produced air is not clean enough for breathing purposes.
Modern commercial filters can remove more than 90% of gaseous pollutants, though they
are expensive and require regular maintenance.
An alternative solution which is applicable for places with better outdoor air quality
is to provide a medical air cylinder at patient rooms to bypass the main system when
the outdoor air pollution exceeds a safe level. In this case, the medical air system work-
s in the same way as the current systems but is able to switch to a cylinder if high
pollutant concentrations are detected in the medical air outlets. However, the prereq-
uisite for this solution is to establish safe levels of air pollution for vulnerable populations.
Page 80
Chapter 6
References
[1] Medical Air. (n.d.). Retrieved from http://www.gasafrica.com/medical-air.html.
[2] MEDICAL AIR. (n.d.). Retrieved from https://www.drugs.com/uk/medical-air-
leaflet.html.
[3] Kanegsberg, B., Kanegsberg, E., Baier, R.E., Nagathan, P., Cleaning, welding, and
medical air, Galvanotechnik, 102(2011):297-300
[4] Edwards, P., Therriault, P., Katz, I., Onsite production of medical air: Is purity a
problem? Multidisciplinary Respiratory Medicine, 13(2018).
[5] Medical Air. (n.d.). Retrieved from https://www.apsf.org/article/medical-air/.
[6] NFPA 99 Medical Air Dewpoint Requirements. (n.d.). Retrieved from
https://www.airbestpractices.com/standards/nfpa-99-medical-air/nfpa-99-medical-
air-dewpoint-requirements.
[7] Allen, M., Oil-free compressor benefits explained, Health Estate, 68(2014)37-39.
[8] The Pharmacopeia of the United States of America: (The United States pharma-
copeia). (1970). Bethesda, MD: United States Pharmacopeial Convention.
[9] CAAQS Table. (2020). Retrieved from http://airquality-qualitedelair.ccme.ca/en/
71
Page 81
Chapter 6. References 72
[10] NAAQS Table. (2016, December 20). Retrieved from https://www.epa.gov/criteria-
air-pollutants/naaqs-table
[11] Pillow, J. J., Hillman, N. H., Polglase, G. R., Moss, T. J., Cheah, S. G., Kramer,
B. W., Jobe, A. H., Oxygen, temperature and humidity of inspired gases and their
influences on airway and lung tissue in near-term lambs, Intensive Care Medicine,
35(2009) 2157-2163.
[12] Haq, I., Gopalakaje, S., Fenton, A., McKean, M., OBrien, C., Brodlie, M., The
evidence for high flow nasal cannula devices in infants, Paediatric Respiratory Reviews,
15(2014) 124-134.
[13] Tucci, M. R., Costa, E. L., Humidification During Invasive Mechanical Ventilation:
Less Lung Inflammation With Optimal Gas Conditioning, Respiratory Care, 60(2015)
1854-1855, DOI: https://doi.org/10.4187/respcare.04512.
[14] Farley, R., Gibbons, K., Jardine, L., Shearman, A., Effect of flow rate, humidi-
fier dome and water volume on maximising heated, humidified gas use for neonatal
resuscitation. Resuscitation (2013) 1428-1432.
[15] Owen, L. S., Dawson, J. A., Middleburgh, R., Buttner, S., McGrory, L., Davis, P.
G., Feasibility and Practical Considerations for Heating and Humidifying Gases during
Newborn Stabilisation: An in vitro Model, Neonatology (2014) 156-162.
[16] Frawley, G., Special considerations in the premature and ex-premature infant,
Anaesthesia & Intensive Care Medicine, 18(2017) 79-83.
[17] Chanyagorn, P., Kiratiwudhikul, P. (n.d.), Fuzzy control of oxygen gas content
for premature labor infants oxygen therapy, ICEIC(2016), DOI: 10.1109/ELINFO-
COM.2016.7563026.
[18] Pike, KC., Lucas JS., Respiratory consequences of late preterm birth, Paediatr
Respir Rev, 16(2015) 182-8.
Page 82
Chapter 6. References 73
[19] Pinkerton, KE., Joad, JP., Influence of air pollution on respiratory health during
perinatal development, Clin Exp Pharmacol Physiol, 33(2006) 269-72.
[20] Kurt, O.K., Zhang, J., Pinkerton, K.E., Pulmonary Health Effects of Air Pollution,
Curr Opin Pulm Med, 22(2016) 138143.
[21] Benzing, A., Loop, T., Mols, G., Geiger, K., Unintended Inhalation of Nitric Oxide
by Contamination of Compressed Air. Anesthesiology, 91(1999), 945.
[22] Nakata, Y., Kawasaki, Y., Matsukawa, K., Goto, T., Niimi, Y., Morita, S., Pollution
of the medical air at a university hospital in the metropolitan Tokyo area. Journal of
Clinical Anesthesia, 14(2002), 193-195.
[23] Zhu, Y., Huang, L., Li, J., Yingb, Q., Zhang, H., Liu, X., Liao, H., Li, N., Liu, Z.,
Mao, Y., Fang, H., Hu, J., Sources of particulate matter in China: Insights from source
apportionment studies published in 1987-2017, Environment International, 115(2018)
343-357.
[24] Significant Primary and Secondary Particulate Matter Sources. (n.d.). Retrieved
from http://www.valleyair.org/air quality plans/AQ plans PM sources.htm.
[25] Statistics Canada. (2017, July 12). Health Reports Exposure to fine particulate
matter air pollution in CanadaHealth Reports Exposure to fine particulate matter air
pollution in Canada. Retrieved from https://www150.statcan.gc.ca/n1/pub/82-003-
x/2017003/article/14781-eng.htm
[26] Thompson, JE., Airborne Particulate Matter: Human Exposure and Health Effects,
J Occup Environ Med, 60(2018) 392-423.
[27] Stockfelt, L., Andersson, EM., Molnr, P., Gidhagen, L., Segersson, D., Rosengren,
A., Barregard, L., Sallsten, G., Long-term effects of total and source-specific particulate
air pollution on incident cardiovascular disease in Gothenburg, Sweden, Environ Res,
158(2017) 61-71.
Page 83
Chapter 6. References 74
[28] Peixoto, MS., de Oliveira Galvo, MF., Batistuzzo de Medeiros, SR., Cell death
pathways of particulate matter toxicity, Chemosphere, 188(2017) 32-48.
[29] Chen, CY., Hung, HJ., Chang, KH., Hsu, CY., Muo, CH., Tsai, CH., Wu, TN.,
Long-term exposure to air pollution and the incidence of Parkinson’s disease: A nested
case-control study, PLoS One, 15(2017), doi: 10.1371/journal.pone.0182834.
[30] Tsamou, M., Vrijens, K., Madhloum, N., Lefebvre, W., Vanpoucke, C., Nawrot, TS.
Air pollution-induced placental epigenetic alterations in early life: a candidate miRNA
approach, Epigenetics, 13(2018) 135-146.
[31] Pergoli, L., Cantone, L., Favero C., Angelici, L., Iodice, S., Pinatel, E., Hoxha,
M., Dioni, L., Letizia, M., Albetti, B., Tarantini, L., Rota, F., Bertazzi, PA., Tirelli,
AS., Dolo, V., Cattaneo, A., Vigna, L., Battaglia, C., Carugno, M., Bonzini, M.,
Pesatori, AC., Bollati, V., Extracellular vesicle-packaged miRNA release after short-
term exposure to particulate matter is associated with increased coagulation, Part
Fibre Toxicol, 14(2017) 32, doi: 10.1186/s12989-017-0214-4.
[32] Jerrett, M., Turner, M.C., Beckerman, B.S., Pope III, C.A., Donkelaar, A.V, Martin,
R.V., Serre, M., Crouse, D., Gapstur, S.M., Krewski, D., Diver, W.R., Coogan, P.F.,
Thurston, G.D., Burnett R.T., Comparing the Health Effects of Ambient Particulate
Matter Estimated Using Ground-Based versus Remote Sensing Exposure Estimates,
Environ Health Perspect, 125(2017) 552559.
[33] Zhao, R., Chen, S., Wang, W., Huang, J., Wang, K., Liu, L., Wei, S., The impact
of short-term exposure to air pollutants on the onset of out-of-hospital cardiac arrest:
A systematic review and meta-analysis, Int J Cardiol, 226(2017) 110-117.
[34] Cakmak, S., Hebbern, C., Vanos, J., Crouse, D.L., Burnett, R., Ozone exposure
and cardiovascular-related mortality in the Canadian Census Health and Environment
Cohort (CANCHEC) by spatial synoptic classification zone, Environmental Pollution,
217(2016) 589-599.
Page 84
Chapter 6. References 75
[35] Nuvolone, D., Petri, D., Voller, F., The effects of ozone on human health, Environ
Sci Pollut Res Int, 25(2018) 8074-8088.
[36] Zu, K., Liu, X., Shi, L., Tao, G., Loftus, CT., Lange, S., Goodman, JE.,
Concentration-response of short-term ozone exposure and hospital admissions for asth-
ma in Texas, Environ Int, 104(2017) 139-145.
[37] Zallaghi, E., Geravandi, S., Haddad, M.N., Goudarzi, G., Valipour, L., Salmanzadeh,
S., Hashemzadeh, B., Zahedi, A., Mohammadi, M.J., Soltani, F., Estimation of Health
Effects Attributed to Nitrogen Dioxide Exposure Using the AirQ Model in Tabriz City,
Iran, Health Scope, (2015), DOI: 10.17795/jhealthscope-30164.
[38] Smith, BJ., Nitschke, M., Pilotto, LS., Ruffin, RE., Pisaniello, DL., Willson, KJ.,
Health effects of daily indoor nitrogen dioxide exposure in people with asthma, Eur
Respir J. 16(2017) 879-85.
[39] Germany, B., Health Aspects of Air Pollution with Particulate Matter, Ozone and
Nitrogen Dioxide, Report on a WHO Working Group, 2003.
[40] Yorifuji, T., Kashima, S., Tsuda, T., Takao, S., Suzuki, E., Doi, H., Sugiyama, M.,
Ishikawa-Takata, K., Ohta, T., Long-term exposure to traffic-related air pollution and
mortality in Shizuoka, Japan, Occup Environ Med, 67(2010) 111-7.
[41] Dennekamp, M., Howarth, S., Dick, C.A.J., Cherriea, J.W., Donaldson, K., Seaton,
A., Ultrafine particles and nitrogen oxides generated by gas and electric cooking, Oc-
cupational & Environmental Medicine, 58(2001) 511-516.
[42] Chen, TM., Gokhale, J., Shofer, S., Kuschner, WG., Outdoor air pollution: nitrogen
dioxide, sulfur dioxide, and carbon monoxide health effects, Am J Med Sci, 333(2007)
249-56.
[43] Nitschke, M., Respiratory health effects of nitrogen dioxide exposure and current
guidelines, International Journal of Environmental Health Research, 9(1999) 39-53.
Page 85
Chapter 6. References 76
[44] Pilotto, L., Douglas, R., Attewell, R., Wilson, S., Respiratory effects associated with
indoor nitrogen dioxide exposure in children. International Journal of Epidemiology,
26(1997), 788-796.
[45] Johns, DO., Linn, WS., A review of controlled human SO exposure studies con-
tributing to the US EPA integrated science assessment for sulfur oxides, Inhal Toxicol,
23(2011) 33-43.
[46] Thriel, C. V., Schper, M., Kleinbeck, S., Kiesswetter, E., Blaszkewicz, M., Golka, K.,
Brning, T., Sensory and pulmonary effects of acute exposure to sulfur dioxide (SO2).
Toxicology Letters, 196(2010), 42-50.
[47] Woerman, A. L., Mendelowitz, D. Postnatal Sulfur Dioxide Exposure Reversibly
Alters Parasympathetic Regulation of Heart Rate. Hypertension, 62(2013), 274-280.
[48] Hang, J., Luo, Z., Wang, X., He, L., Wang, B., Zhu, W., The influence of street
layouts and viaduct settings on daily carbon monoxide exposure and intake fraction
in idealized urban canyons. Environmental Pollution, 220(2017), 72-86.
[49] Green, E., Short, S., Shuker, L., Harrison, P. Carbon Monoxide Exposure in the
Home Environment and the Evaluation of Risks to Health - A UK Perspective. Indoor
and Built Environment, 8(1999), 168-175.
[50] Montoya, T., Gurian, P. L., Velzquez-Angulo, G., Corella-Barud, V., Rojo, A.,
Graham, J. P. Carbon monoxide exposure in households in Ciudad Jurez, Mxico.
International Journal of Hygiene and Environmental Health, 211(2008), 40-49.
[51] Ryter, S. W., Choi, A. M. Carbon monoxide: Present and future indications for a
medical gas. The Korean Journal of Internal Medicine, 28(2013), 123.
[52] Ellegrd, A., Health effects of cooking air pollution among women using coal bri-
quettes in Hanoi. Environmental Technology, 18(1997), 409-4151.
[53] Hassan, M. S., Ray, J., Wilson, F., Carbon monoxide poisoning and sensorineural
hearing loss. The Journal of Laryngology & Otology, 117(2003)
Page 86
Chapter 6. References 77
[54] Rice, S.A., Human Health Risk Assesment of CO2: Survivors of Acute High-Level
Exposure and Populations Sensitive to Prolonged Low-Level Exposure, Third Annual
Conference on Carbon Sequestration, 2004.
[55] Zhang, X., Wargocki, P., Lian, Z., Thyregod, C., Effects of exposure to carbon
dioxide and bioeffluents on perceived air quality, self-assessed acute health symptoms,
and cognitive performance. Indoor Air, 27(2016), 47-64.
[56] H. Nakagawa, S. Okazaki, S. Asakura, K. Fukuda, H. Akimoto, S. Takahashi, S.
Shigemori, An automated car ventilation system, Sens. Actuators B: Chem. 65(2000)
133137.
[57] M.C. Carotta, G. Martinelli, L. Crema, M. Gallana, M. Merli, G. Ghiotti, E. Traver-
sa, Array of thick film sensors for atmospheric pollutant monitoring, Sens. Actuators
B: Chem. 68(2000) 18.
[58] C. Pijolat, C. Pupier, M. Sauvan, G. Tournier, R. Lalauze, Gas detection for auto-
motive pollution control, Sens. Actuators B: Chem. 59(1999)195202.
[59] Thompson, J.E., Crowd-sourced air quality studies: A review of the literature &
portable sensors, Trends in Environmental Analytical Chemistry, 11(2016) 2334.
[60] M. Iwamoto, in: S. Yamauchi (Ed.), Chemical Sensor Technology, Kodansha, Tokyo,
4(1992), pp. 63.
[61] Mead, M.I., Popoola, O.A.M., Stewart, G.B., Landshoff, P., Calleja, M., Hayesb, M.,
Baldovi, J.J., McLeod, M.W., Hodgson, T.F., Dicks, J., Lewis, A., Cohen, J., Baron,
R., Saffell, J.R., Jones, R.L., The use of electrochemical sensors for monitoring urban
air quality in low-cost, high-density networks, Atmospheric Environment, 70(2013)
186-203.
[62] Data Mining Map. (n.d.). Retrieved from http://www.saedsayad.com/data mining map.htm
[63] Random Forest. (2016, May 22). Retrieved from
http://www.assignmentpoint.com/science/computer/random-forest.html
Page 87
Chapter 6. References 78
[64] Challenges in Deep Learning Hacker Noon. Retrieved from
https://hackernoon.com/challenges-in-deep-learning-57bbf6e73bb
[65] Hagan, M. T., Demuth, H. B., Beale, M. H., Jesus, O. D. (2016). Neural network
design. S. l.: S. n.
[66] Relu. (n.d.). Retrieved from http://armelection.info/bef/relu.htm
[67] Alphasense, NO-B4 Nitric Oxide Sensor 4-Elecrode, 07/2018, 44 (n.d.) 12.
[68] Alphasense, CO-B4 Carbon Monoxide Sensor 4-Elecrode, 07/2018, 44 (n.d.) 12.
[69] Zimmerman, N., Presto, A. A., Kumar, S. P., Gu, J., Hauryliuk, A., Robinson, E. S.,
Robinson, A. L. A machine learning calibration model using random forests to improve
sensor performance for lower-cost air quality monitoring. Atmospheric Measurement
Techniques, 11(1)(2018) 291-313.
[70] Auta, M., Hameed, B. Adsorption of carbon dioxide by diethanolamine activated
alumina beads in a fixed bed. Chemical Engineering Journal, 253(2014) 350-355.
[71] Kneer, J., Wllenstein, J., Palzer, S. Manipulating the gassurface interaction between
copper(II) oxide and mono-nitrogen oxides using temperature. Sensors and Actuators
B: Chemical, 229 (2016) 57-62.
[72] Worden, D., Ball, D. W. Reaction of nitrogen dioxide with copper atoms in argon
matrixes. The Journal of Physical Chemistry, 96(1992) 7167-7169.
[73] Kumpanenko, I. V., Roshchin, A. V., Ivanova, N. A., Novikov, V. V., Skryl’Nikov, A.
M., Podvalny, A. M., Usin, V. V. Dynamic adsorption of nitrogen dioxide on zeolites.
Russian Journal of Physical Chemistry B, 11(1)(2017) 154-166.
[74] Martin, C. R., Zeng, N., Karion, A., Dickerson, R. R., Ren, X., Turpie, B. N., Weber,
K. J. Evaluation and environmental correction of ambient CO2 measurements from a
low-cost NDIR sensor. Atmospheric Measurement Techniques, 10(7)(2017), 2383-2395.
[75] Pandey, S., Kim, K. The Relative Performance of NDIR-based Sensors in the Near
Real-time Analysis of CO2 in Air. Sensors, 7(9) (2007), 1683-1696.
Page 88
Chapter 6. References 79
[76] Hill, C. (n.d.). HITRANonline. Retrieved from http://hitran.org/
Page 89
Appendix A
Quality of Compressed Air at the
Wallberg Building
The compressed air system at the University of Toronto’s Wallberg Building is very close
to medical air system, consisting of similar equipment, except that the pollution levels
are not monitored after production. In addition to sampling at the hospital, pollution
concentrations of compressed air at the Wallberg Building were measured with reference
instruments for about two weeks.
Similar to the medical air, the time series data of the compressed air, shown in Figure
A.1 indicated that the CO and CO2 concentrations in the compressed air strongly followed
the outdoor trend and that changes in the inlet concentrations were rapidly delivered to
the outlet. Also, CO2 concentration dropped down to 150 ppm and rose to about 400ppm
every four days.
80
Page 90
Appendix A. Quality of Compressed Air at the Wallberg Building 81
Figure A.1: Comparison between time series CO and CO2 concentration in CompressedAir and outdoor air at Wallberg Building.
Figure A.2 shows that concentrations of NOx and ozone in the Compressed Air at the
Wallberg was very low and did not follow variations in outdoor levels.
Page 91
Appendix A. Quality of Compressed Air at the Wallberg Building 82
Figure A.2: Comparison between time series O3 and NOx concentration in CompressedAir and outdoor air at Wallberg Building.
Page 92
Appendix B
Comparison Between O3 and NOx
Levels in Medical and Outdoor Air
Table B.1: Contribution of outdoor pollution to NOx and O3 levels in medical air.
PollutantAveraged
ConcentrationIntercept 1− Intercept
AveragedConc.
O3 10.32 8.69 0.16
NOx 16.17 13.32 0.19
83
Page 93
Appendix B. Comparison Between O3 and NOx Levels in Medical and Outdoor Air84
Figure B.1: NOx and O3 in outdoor air Vs. in medical air