Monotherapy using 6-MP or azathioprine for Crohn’s disease is dead: out with the old and in with the new Stephen B. Hanauer, MD Professor of Medicine Clinical Director, Digestive Health Center
Transcript
Monotherapy using 6-MP or azathioprine for Crohn’s disease is dead: out with the old and in
with the newStephen B. Hanauer, MDProfessor of MedicineClinical Director, Digestive Health Center
Because it has NEVER been effective
Monotherapy is Dead!
Thiopurines in CD 1980s-1990s
• 1979 NCCD study: azathioprine not effective for induction or maintenance in CD
• 1980 Present: 6MP effective as induction/maintenance in CD (n=83, dur=8y, f/u=2y)- Mean time to response: 3.1 months- Require < 6 months to reach maximal efficacy
• GETAID: 24 French centers• 147 adult patients (IMM/biologic naïve) with:- newly diagnosed CD (<6 months) - Risk factors for disabling disease (>2):
• Younger than 40• Active perianal lesions• Corticosteroids within 3 months of diagnosis
- Early (Immediate) azathioprine- Conventional azathioprine when:
•Corticosteroid dependence•Chronic active disease with frequent flare•Poor response to treatment with steroids•Development of severe perianal disease
Two study arms:RAPID Trial
• Primary End Point:- Proportion of trimesters in remission
during follow-up• Secondary End Points:- Proportion of trimesters with flare- CD-related hospitalization- Active perianal disease- Perianal/Intestinal surgery- Steroid/anti-TNF use
RAPID Trial
Rapid TrialResults: Proportion of patients in corticosteroid-free, anti-TNF-free remission per trimester
AZTEC TrialGETECCUSpain
AZTEC trial:
- 18 months- Double-blind randomized trial- Intended to replicate Markowitz study
• Two study arms (stratified by age and steroid use):- Azathioprine- Placebo
Study Design
• GETECCU: 31 Spanish centers
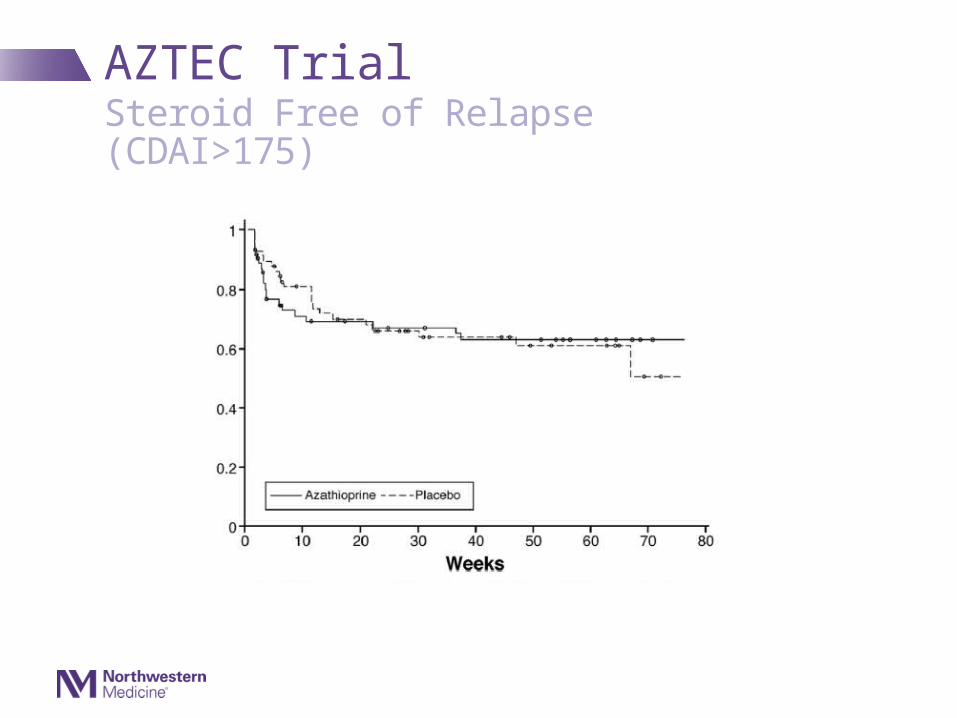
AZTEC TrialSteroid Free of Relapse (CDAI>175)
AZTEC Trial
• In Early AZA:- 44% with steroid-free remission at 76 weeks vs
37% for placebo (p=0.48)- No difference in proportion of patients with SFR at
weeks 28 or 50, relapse-free survival rates, CDAI scores or CRP over time
- Post-hoc analysis:• Relapse after week 12 (defined as CDAI >220) 12% vs 30% (p=0.01)
Results
Conclusions
• Early “top-down” therapy with thiopurines not more effective than conventional therapy or placebo in adults with newly diagnosed CD
• Cast doubt on applicability of 2000 pediatric study
RAPID + AZTEC
RAPID + AZTEC
• Inactive/mild disease (compared to Markowitz)• Open-label (GETAID)• Primary end point never used before (GETAID)• No optimization of 6TGN levels• Remission defined by CDAI• Better predictors of high risk??• Median delay of 11 months between 2 groups in GETAID study
• Early termination of AZTEC
Problems with Interpretations
In additon….
Assimilating results from observational series
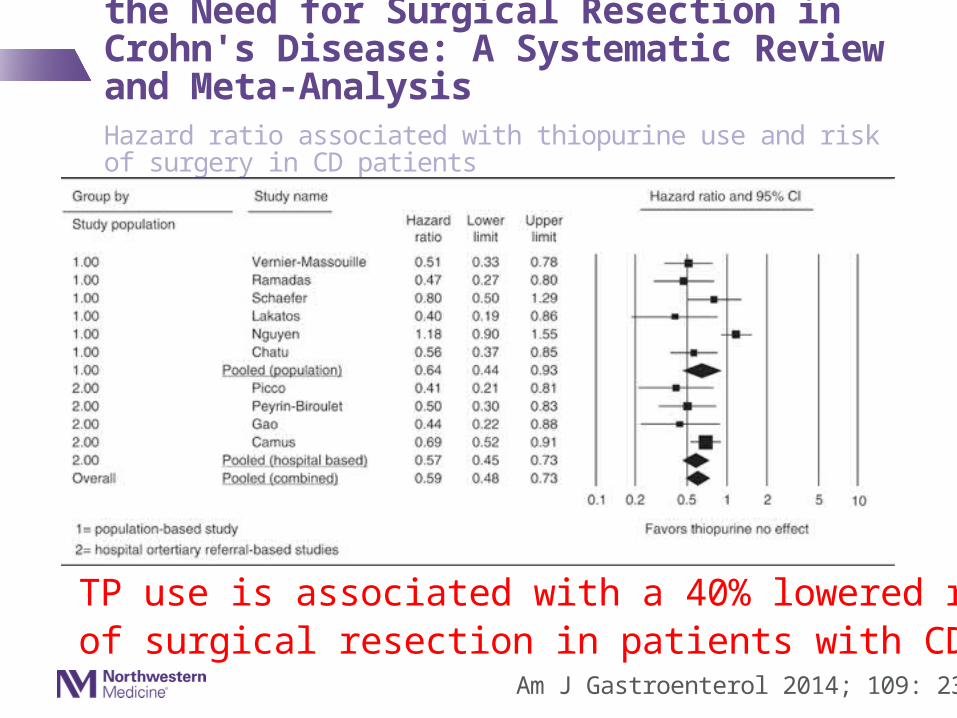
The Role of Thiopurines in Reducing the Need for Surgical Resection in Crohn's Disease: A Systematic Review and Meta-AnalysisHazard ratio associated with thiopurine use and risk of surgery in CD patients
Am J Gastroenterol 2014; 109: 23–34
TP use is associated with a 40% lowered risk of surgical resection in patients with CD
Conclusions
Remaining indications for thiopurines:- Maintenance of steroid-induced
remission/steroid sparing in patients with CD (?not newly diagnosed) – modest effect
- Prevention of postoperative recurrence- modest effect
Strongest indication: in combination with biologics
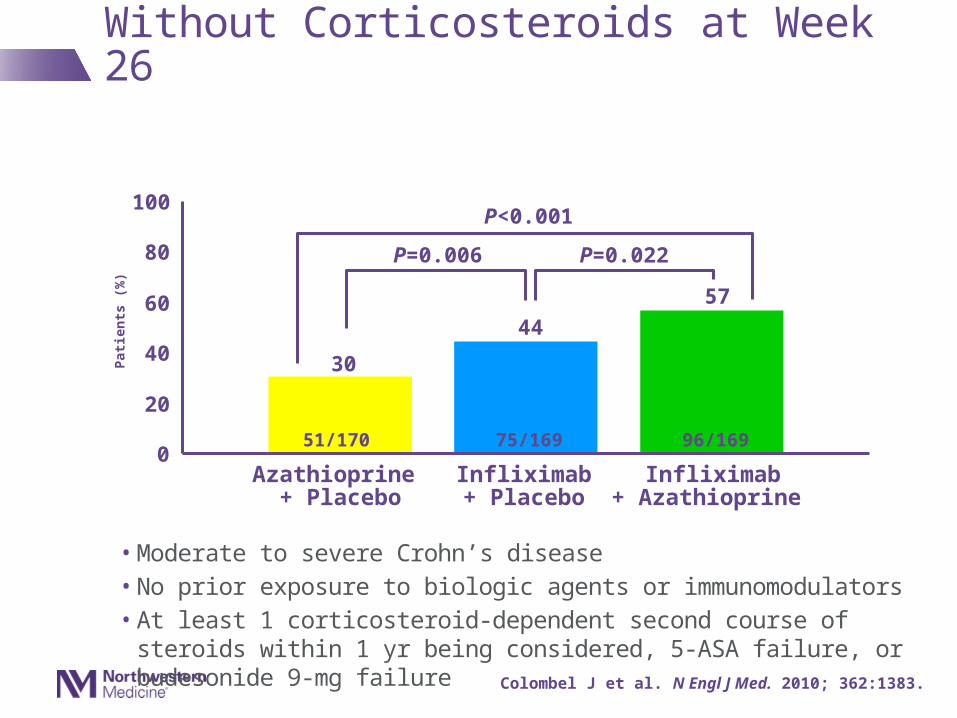
SONIC: Clinical Remission Without Corticosteroids at Week 26
• Moderate to severe Crohn’s disease• No prior exposure to biologic agents or immunomodulators• At least 1 corticosteroid-dependent second course of steroids within 1 yr being
considered, 5-ASA failure, or budesonide 9-mg failure
30
44
57
0
20
40
60
80
100
Pat
ien
ts (
%)
Azathioprine + Placebo
Infliximab+ Placebo
Infliximab+ Azathioprine
P<0.001
P=0.006 P=0.022
51/170 75/169 96/169
Colombel J et al. N Engl J Med. 2010; 362:1383.
Risk Benefits of Thiopurines
Benefits/Indication Risks/Indication
Risks of Thiopurines and Methotrexate
• Thiopurines- Skin Cancer
• NMSC/Melanoma- Lymphoma
• EBV• HSTC (with biologics)
- Myelodysplasia
Neoplastic
• We Suggest Against Using Thiopurine Monotherapy to Induce Remission in Patients With Moderately Severe CD
(Weak Recommendation, Moderate-Quality Evidence)
Gastroenterology. 2013;145(6):1459-63
AGA Guideline on the Use of Thiopurines, Methotrexate, and Anti–TNF-α Biologic Drugs for Induction and Maintenance of Remission in Crohn's Disease
AGA Guideline on the Use of Thiopurines, Methotrexate, and Anti–TNF-α Biologic Drugs for Induction and Maintenance of Remission in Crohn's Disease
• We Suggest Using Anti–TNF-α Drugs in Combination With Thiopurines Over Anti–TNF-α Drug Monotherapy to Induce Remission in Patients Who Have Moderately Severe CD
(Weak Recommendation, Moderate-Quality Evidence)
Gastroenterology. 2013;145(6):1459-63
• We Recommend Using Thiopurines Over No Immunomodulator Therapy to Maintain a Corticosteroid-Induced Remission in Patients With CD