45
Monovision Monovision
| Date post: | 16-Jul-2015 |
| Category: |
Education |
| Upload: | tickky-tickky |
| View: | 181 times |
| Download: | 1 times |

MonovisionMonovision
Monovision
• This optical condition allows the relief of presbyopia symptoms.– one eye is corrected for distance vision– The other eye is corrected for near vision
• Goal of treatment– To give patients clear vision both near and
far

Concept
• Intention to produces anisometropic blur – the image in one eye is focused while the
image in the other eye is defocused.– Suppress blur in nondominant eye will be
easier than in dominant eye.
• Person'€™s brain learns to use the distance focused eye for distance viewing and the near focused eye for near viewing
Monovision
• Dominant eye corrected for distance vision
• Nondominant for near vision
• Induced anisometropic 1.25- 2.5 dipoters
• Mini monovision lower level of myopia for near vision -0.5 to -0.75 D

Ocular dominanceOcular dominance
Ocular dominanceOcular dominanceOcular dominanceOcular dominance
MotorMotorMotorMotor
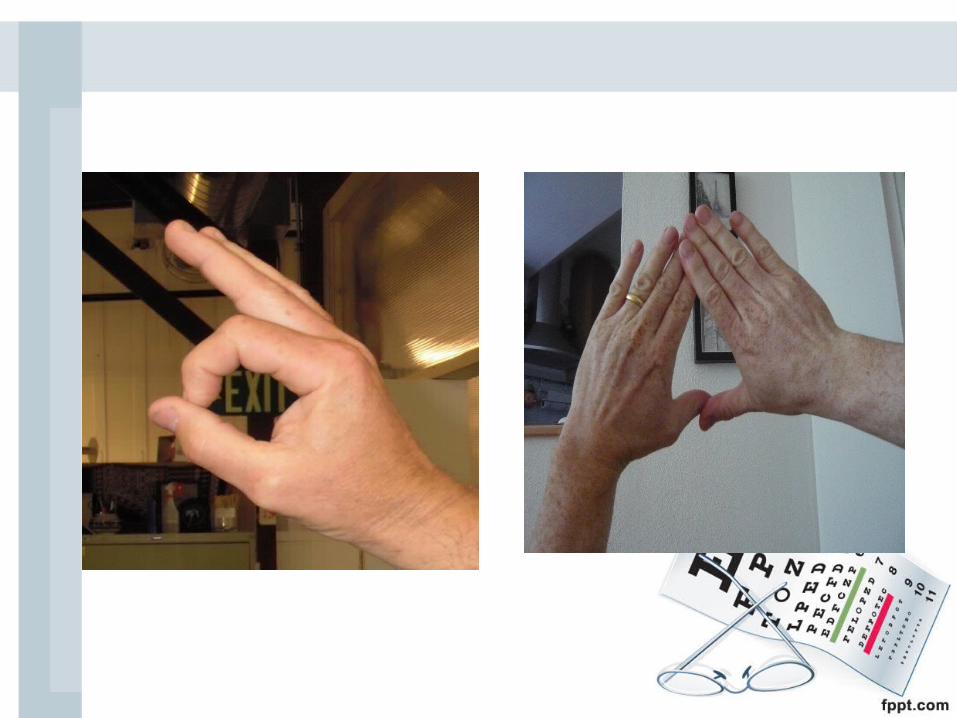
Pointing-a-finger testPointing-a-finger testHole- in- card testHole- in- card testPointing-a-finger testPointing-a-finger testHole- in- card testHole- in- card test
Binocular rivalry targetBinocular rivalry targetStereodisparate objectsStereodisparate objectsBinocular rivalry targetBinocular rivalry targetStereodisparate objectsStereodisparate objects
sensorysensorysensorysensory
Seijas O, Liano P, Liano R, Roberts C, Piedrahita E, Diaz E. Ocular Dominance Diagnosis and Its Influence in Monovision. Am J Ophthalmol.2007;144:209–16.
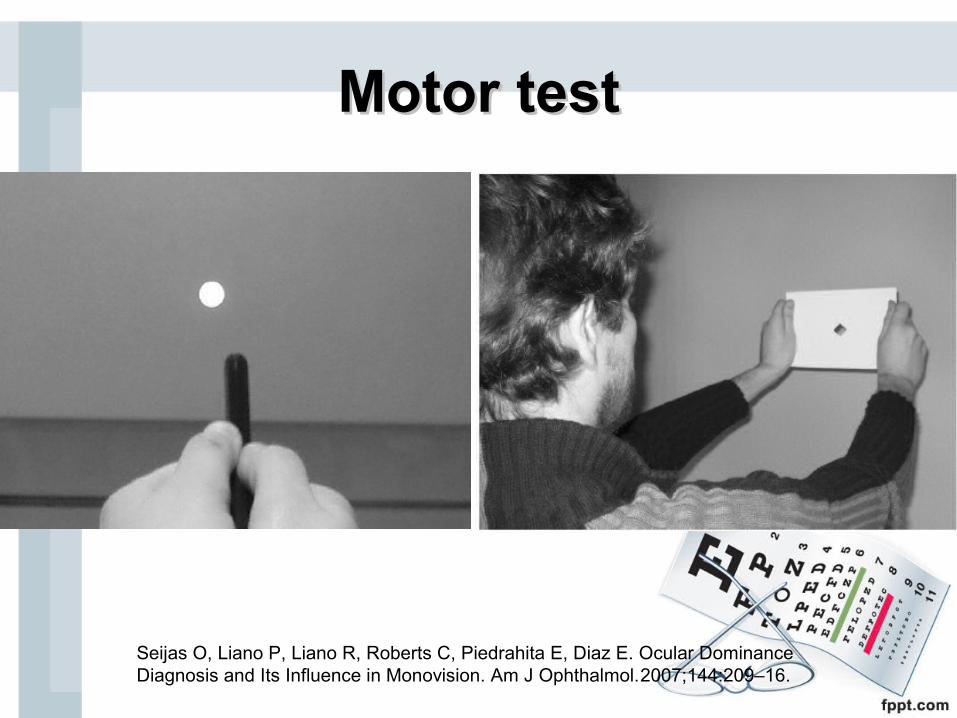
MotorMotor testtest
Seijas O, Liano P, Liano R, Roberts C, Piedrahita E, Diaz E. Ocular Dominance Diagnosis and Its Influence in Monovision. Am J Ophthalmol.2007;144:209–16.

Ocular dominanceOcular dominance
• Ogle’s eye dominance test
x
x x x
o
o o o
Method
• Test dominant eye
• Refraction– Dominant Full correction for distance vision– Nondomiant Myopia undercorrection
Hyperopia overcorrection
• Trial Lens or CL trial at home
adaptation period should be greater than 2-3 wks
How is monovison obtained?
• Contact lenses
• Refractive surgery
• Conductive Keratoplasty
• Corneal inley
• IOL

Refractive surgery
• Multifocal corneal ablationo A small central steep zoneo Inferior near zone ablation patterno Inferior decentered hyperopic ablationoCentral distance ablation with
intermediate/near midperipheral abration

Patterns of Multifocal Ablation
Near
Far
Near
Far
Far
Near

Conductive Keratoplasty
• Nonablation collagen-shrinking procedure approve for correction low level of hyperopia ( +0.75 - + 3.25 D)
• Radiofrequency(RF) energy is delivered through tip into peripheral corneal stroma


Intracorneal Inlays
• Lamellar corneal flap created (8.0mm and 160µm)• Placing a biocompatible polymer lens in the central
cornea over pupil


Corneal inley
• ProsExtraocularEasy to do Easy to reverse
• ConsInvolves visual axisAdversely effects distance vision in emmetropesCases of epithelial ingrowth resulting in thinning
and melt of flap
Intraocular lens
• Multifocal IOL
• Monofocal IOL ( Monovision)
Monovision
• Success rate mean 76%
Depend onDepend on
• Ocular dominance and sighting preference
• Interocular suppression of blur
• Age
• Stereoacuity
• phorias
Jain S, Arora I, Azar D. Success of Monovision in Presbyopes: Review of theLiterature and Potential Applications
toRefractive Surgery. Surv Ophthalmol.1996;40:491-99.

Patient selection
• Best candidate are myopic patient over the age of 40
• Age & near addition of the patient can be predictive of success
• Visual needs & lifestyle, occupation, patient’s expectation

Advantages
• Correct presbyopia glass free
• Functional vision at distance and near
Disadvantages of Monovision
• ↓ in visual acuity, stereopsis, depth perception, contrast sensitivity
• Difficulty in seeing clearly at an intermediate distance
• Driving is compromised, especially at night
• Distance and near ghosting (incomplete suppression of interocular blur)

Modified monovision
• Dominant eye distance vision
• Nondominant eye bifocal Lens near and intermediate distance
Modified trivision• Dominant eye distance vision + low add
power for intermediate distance
• Nondominant eye bifocal Lens near and intermediate distance

Varies Forms and Examples of Modified Monovision
Distance EyeDistance Eye Near eyeNear eye
Single-vision lens Bifocal lens power biased toward near vision
Bifocal lens power biased toward distance vision
Bifocal lens power biased toward near vision
Large OZ for distance/center Small OZ for distance/center
Small OZ for near/center Large OZ for near/center
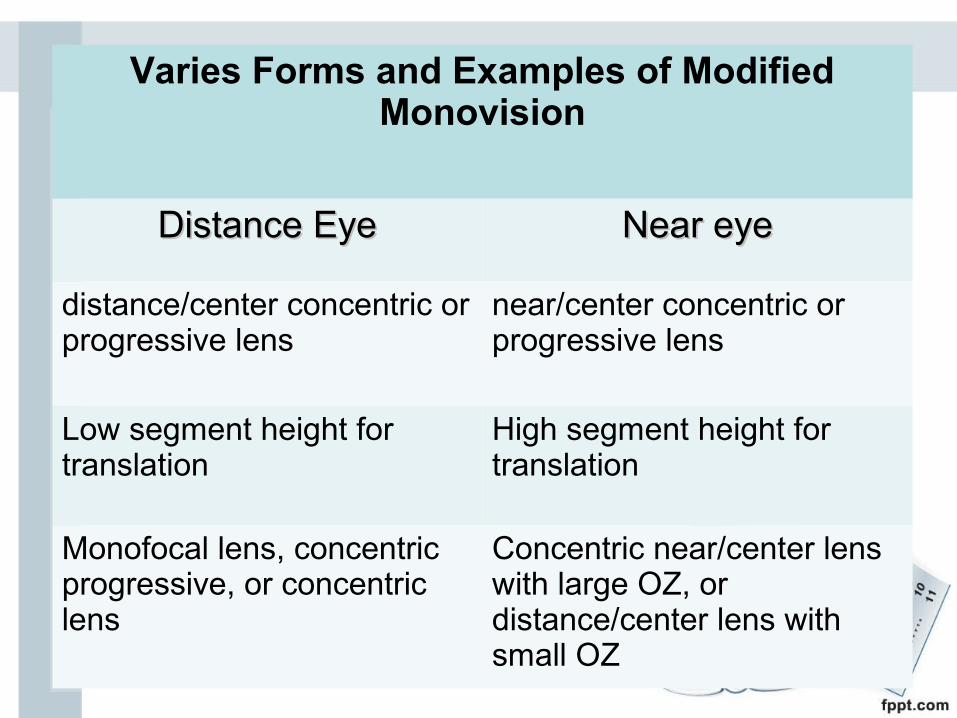
Varies Forms and Examples of Modified Monovision
Distance EyeDistance Eye Near eyeNear eye
distance/center concentric or progressive lens
near/center concentric or progressive lens
Low segment height for translation
High segment height for translation
Monofocal lens, concentric progressive, or concentric lens
Concentric near/center lens with large OZ, or distance/center lens with small OZ

Multifocal IOL

Multifocal IOLMultifocal IOL

12345
Bright light/ Distance dominant zoneLarge Near dominant zone
Low light/ Distance dominant zone
Distance zone
Near zone
Aspheric transition

REFRACTIVE MULTIFOCAL IOLs
Multiple focal points of a refractive MIOL

Silicone MIOLs
Array multifocal IOL (AMO)
First FDA approved foldable MIOL
Acrylic MIOLs
ReZoom multifocal IOL (AMO)
AcrySof ReSTOR lens (Alcon)
Tecnis multifocal IOL (AMO)
Multifocal IOLMultifocal IOL

The ARRAY®IOLRefractive Multifocal IOL Design
• Five concentric zones
• Each zone has a near or distance weighting
• Centre is distance weighted
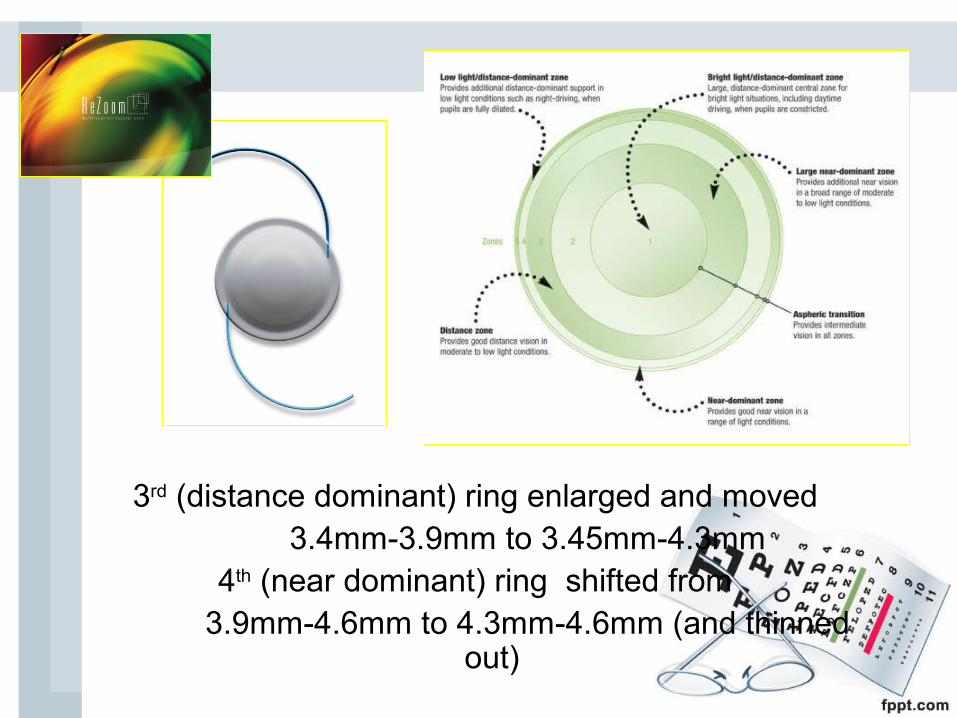
3rd (distance dominant) ring enlarged and moved 3.4mm-3.9mm to 3.45mm-4.3mm
4th (near dominant) ring shifted from 3.9mm-4.6mm to 4.3mm-4.6mm (and thinned
out)
AMO ReZoom™
Good:• Provides excellent distance vision• Provides reasonable intermediate vision • Fewer halo and glare problems than the Array
Not-so-good:• Reading ability (near acuity) variable• Reading ability is pupil dependent• Less tolerable in myopes
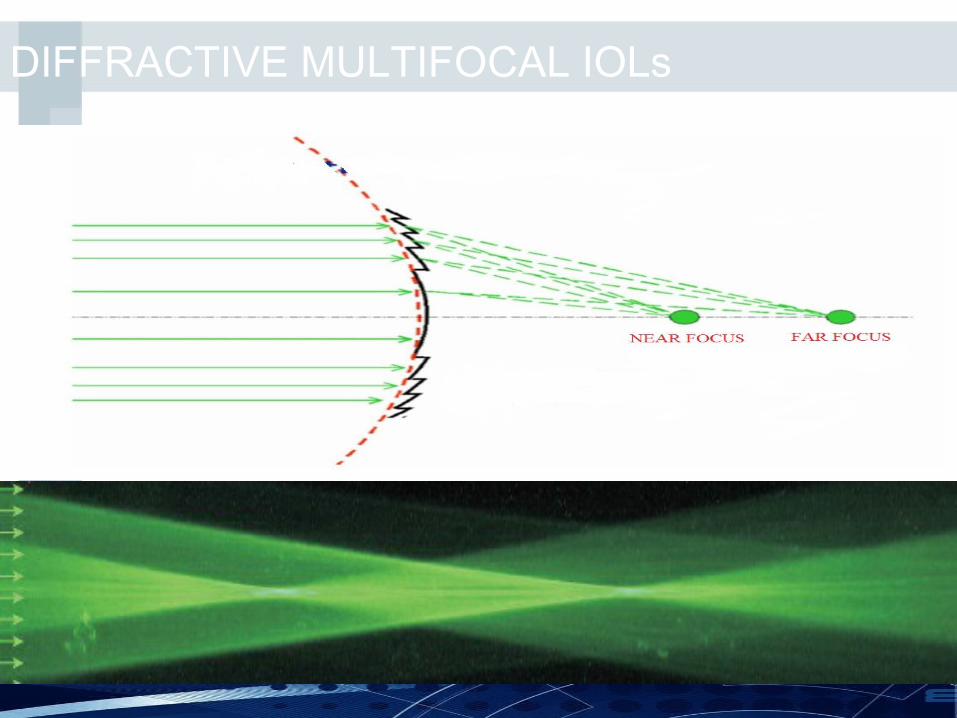
DIFFRACTIVE MULTIFOCAL IOLs
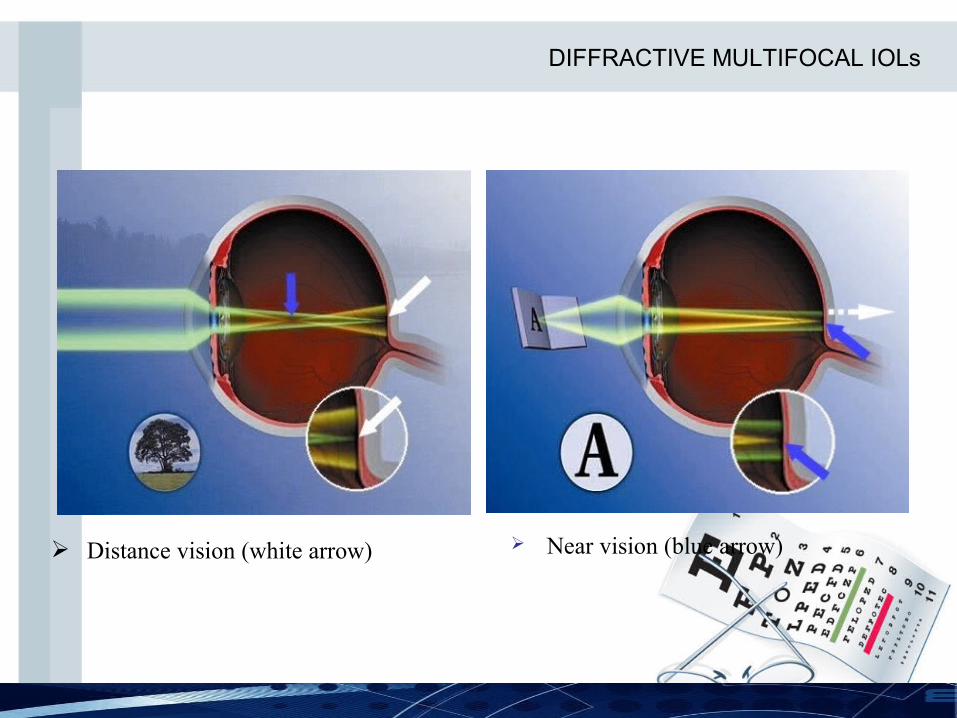
Distance vision (white arrow) Near vision (blue arrow)
DIFFRACTIVE MULTIFOCAL IOLs
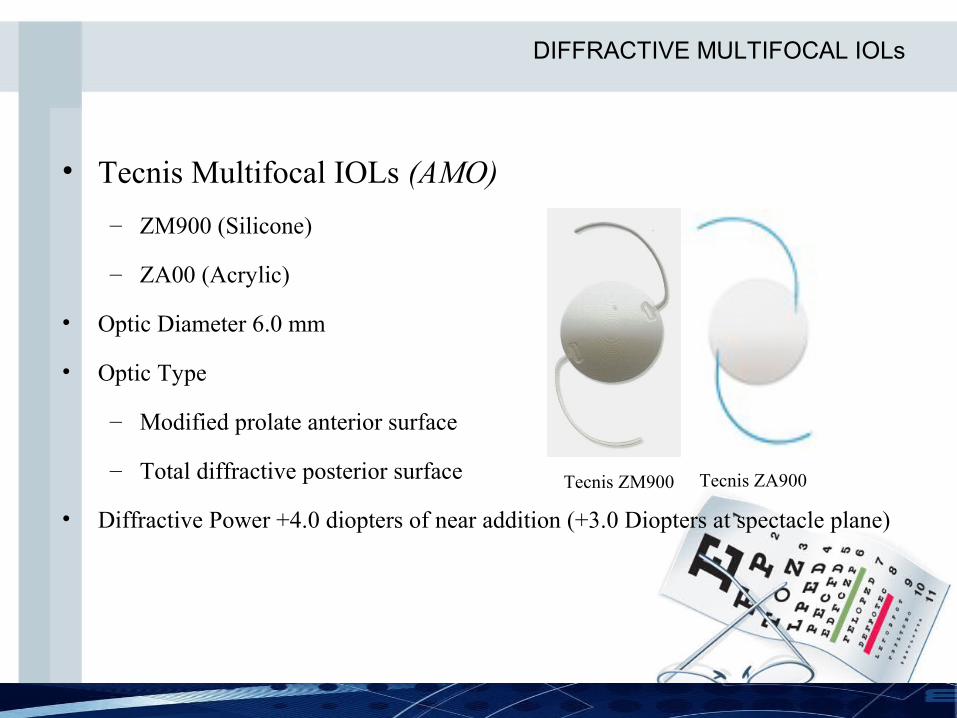
• Tecnis Multifocal IOLs (AMO)
– ZM900 (Silicone)
– ZA00 (Acrylic)
• Optic Diameter 6.0 mm
• Optic Type
– Modified prolate anterior surface
– Total diffractive posterior surface
• Diffractive Power +4.0 diopters of near addition (+3.0 Diopters at spectacle plane)
Tecnis ZM900 Tecnis ZA900
DIFFRACTIVE MULTIFOCAL IOLs
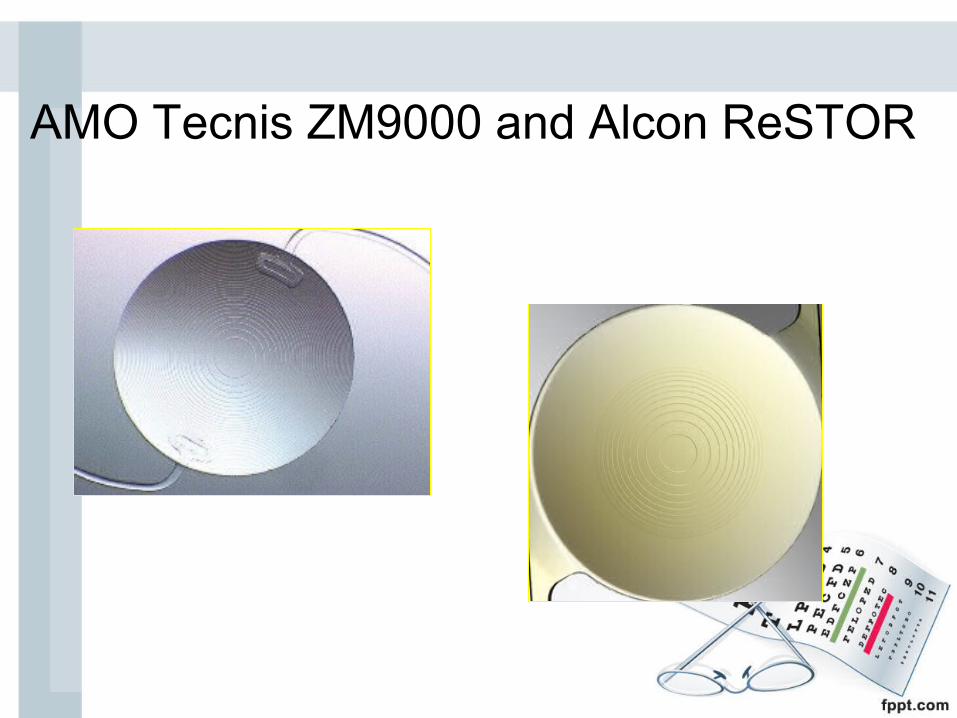
AMO Tecnis ZM9000 and Alcon ReSTOR

Alcon ReSTOR: Partial Optic Diffractive Apodized
• Only the central 3.6mm of optic contains diffractive rings with steps of certain height
• Now available in aspheric form• Step heights get progressively lower from centre to
periphery
AMO Tecnis™ ZM900 Multifocal and Alcon ReSTOR
Good:• Provide excellent distance and near vision• Fewer halo and glare problems than the Array• Most appreciated by hypermetropes• Well tolerated by (higher) myopesNot-so-good:• Intermediate vision suboptimal: problem for computer
users• Quality of vision not as acute as with a monofocal
(contrast sensitivity suffers)
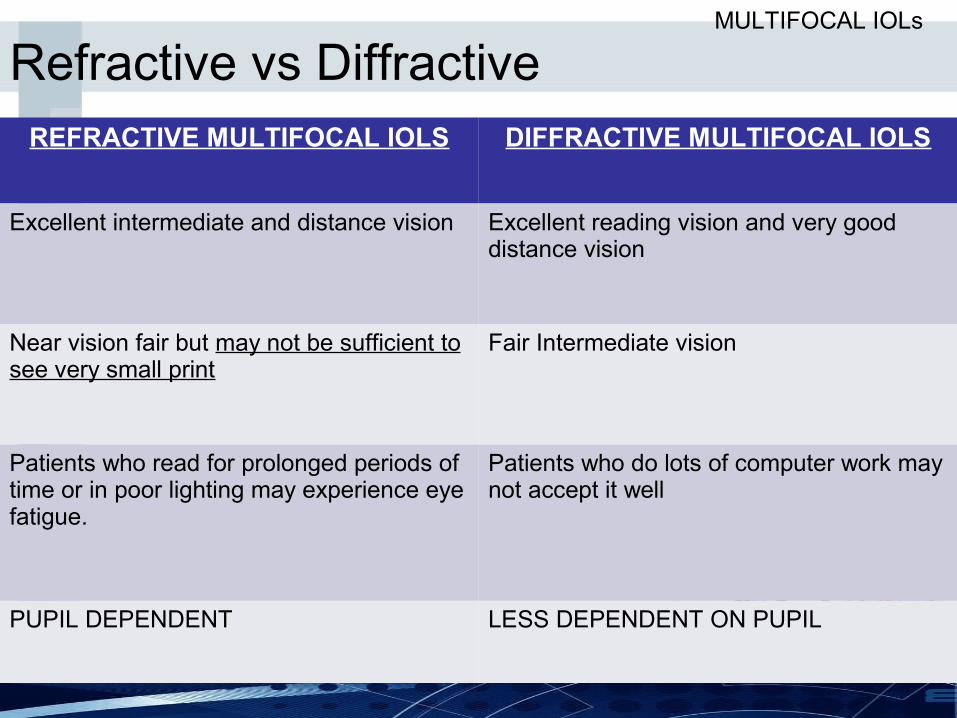
REFRACTIVE MULTIFOCAL IOLS DIFFRACTIVE MULTIFOCAL IOLS
Excellent intermediate and distance vision Excellent reading vision and very good distance vision
Near vision fair but may not be sufficient to see very small print
Fair Intermediate vision
Patients who read for prolonged periods of time or in poor lighting may experience eye fatigue.
Patients who do lots of computer work may not accept it well
PUPIL DEPENDENT LESS DEPENDENT ON PUPIL
Refractive vs DiffractiveMULTIFOCAL IOLs
Disadvantages
• Reduction of contrast sensitivity
• Glare, haloes
• Less satisfactory visualization of fundus- difficulty in vitreo-retinal procedures
• Requires Visual-Cortical Neuro-adaptation
• Requires
• Accurate biometry
• Precise IOL implantation
• Astigmatic reduction
MULTIFOCAL IOLs
Monovision Vs multifocal IOLMonovision Vs multifocal IOL




















