91
MORA Initiative: MORA Initiative: Musculoskeletal Disorders Musculoskeletal Disorders Lower Back Injuries in Health Care Settings
| Date post: | 23-Jan-2018 |
| Category: |
Healthcare |
| Upload: | denise-dumont-bernier |
| View: | 18 times |
| Download: | 0 times |

MORA Initiative:MORA Initiative:Musculoskeletal DisordersMusculoskeletal Disorders
Lower Back Injuries in Health Care Settings

Prevalence of the Problem
Denise Dumont, PTDenise Dumont, PTArea ManagerU. S. HealthWorks Medical Group of Maine, Inc.

Resident handling tasks such as lifting and transferring cause more than 73% of back pain or strain injuries

Back Injuries
The Hazard:
Pain and Injuries to muscles tendons, discs and other parts of the back

Who is at Risk?Workers who lift
and move patients Those with jobs in :
Laundries Kitchens Environmental Services Others who must lift, push, pull objects

Maine DOL: Occupation of Worker
1997 1998 1999 2000 2001Nurses Aides, orderlies, attendants 413 428 698 672 650% of All Injuries 42.8% 40.8% 45.8% 42.9% 41.4%RNs 191 156 207 247 251Health Aids 35 79 100 74 80Maids and housemen 43 43 62 66 109Janitors and cleaners 31 50 75 88 67Technologists 22 45 46 43 43LPNs 35 39 32 34 35Cooks 25 23 33 28 25Misc Food prep 12 23 24 32 25Laundry 16 13 14 19 21% of all injuries 85.4% 85.7% 84.7% 83.2% 83.2%

Types of InjuriesLow Back Pain- Non-specificHerniated DiscsStrained Muscles and tendonsSprained ligamentsSciatica

Issues Staffing Levels in Health Care Facilities Turnover Mandatory Overtime Patient Population/types
Violence Weights
Inexperience or Lack of Training Facility Lift Policies, Ergonomics, Equipment Interventions and Their Effectiveness?

When Staff Are InjuredWhen Staff Are InjuredLife discomfort from having a back
injury.
Medical Costs
Loss of Income
Stress for staff (increased paperwork, relationship with co-workers & residents' families)

When Staff Are InjuredWhen Staff Are InjuredStaff Replacement Costs:
OvertimeOutside AgencyTraining & Orientation of New StaffExtra time from co-workersRecruitment

$1
Hidden Costs
$7
Direct Medical & Indemnity
AdditionalReplacement Costs
Retraining
Premiums
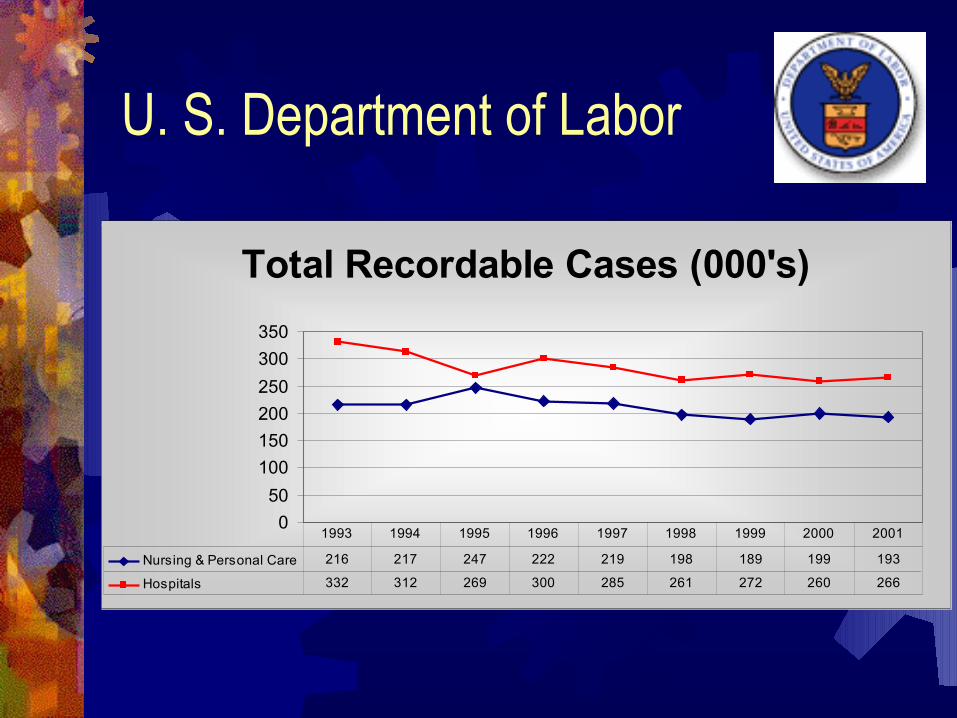
U. S. Department of Labor
Total Recordable Cases (000's)
0
50
100
150
200
250
300
350
Nursing & Personal Care 216 217 247 222 219 198 189 199 193
Hospitals 332 312 269 300 285 261 272 260 266
1993 1994 1995 1996 1997 1998 1999 2000 2001

90
100
110
120
130
Lost Workday Cases (000's)
Nursing & Personal Care Facilities 112 109 120 112 119 114 107 114 107
Hospitals 126 119 115 115 120 112 121 120 122
1993 1994 1995 1996 1997 1998 1999 2000 2001
U. S. Department of Labor

Maine Department of Labor Standards Data Data from Worker’s Comp Board based on a
First Report of Occupational Injury or Disease Only Lost Time Claims data available 805-806 SIC codes Disabling Cases 1997-2001 = 6675 or 1335
per year average Upward Trends Noted from year to year Total Costs $24 Million

Total Disabling Injuries Maine DOL
0
1000
2000
Total Disabling Cases 964 1050 1524 1566 1571
1997 1998 1999 2000 2001

Maine DOL: Nature of InjuryNature of Injury
Sprain, Strain and Tears Most prevalent (30-43% of all injuries)
293366
577
692 678
0
100
200
300
400
500
600
700
800
1997 1998 1999 2000 2001
Sprain, strain, tears

Maine BLS: Body Part/Region
524568
784 823 842
0
200
400
600
800
1000
1997 1998 1999 2000 2001
Spine Related Injuries51-54% of all Injuries are spine related

Maine BLS: Event Leading to Injury 67-72% of all injuries
Event Leading to Injury 1997 1998 1999 2000 2001Overexertion in Lifting 193 261 408 462 501Fall to floor 82 80 99 105 146Overexertion Holding, carrying, turning object52 66 96 121 73Overexertion in pulling/pushing objects46 52 107 93 81Overexertion, UNS 85 59 64 83 64Overexertion, NEC 69 74 107 50 38Nonclassifiable 76 53 57 46 46Bending/climbing/reaching/twisting 57 38 51 57 60

PrevalenceLarge WC Insurance Company Data Includes Medical Only claims as well as
Lost time claimsTotal Claims : 8768805 and 806 SIC Codes onlyNursing & Personal Care Facilities: 46%Hospitals: 54% of claims

Demographics 1456 Employers withApproximately 33,108 Total EmployeesAge : Average and Median = 408768 Total Injuries or 3.7% Injury Rate16.5 % incurred $0Spans 7 year history of Claim numbersSpans 4 years of Claims Cost Data
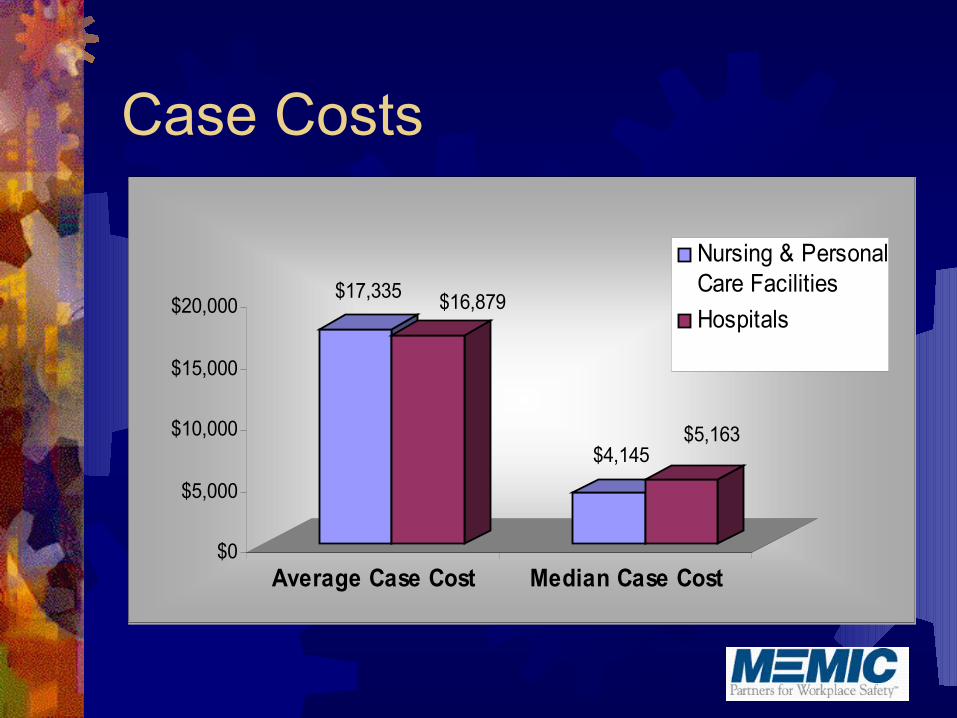
Case Costs
$17,335 $16,879
$4,145$5,163
$0
$5,000
$10,000
$15,000
$20,000
Average Case Cost Median Case Cost
Nursing & PersonalCare Facilities
Hospitals

Occupation
65%
20%
15%
Professional (RN/RT)
Technical (LPN, Techs,Admin)
Service (CNA, Dietary,Housekeeping)

Average Cost Per ClaimMedical Only vs Indemnity Claims
$0
$1,000
$2,000
$3,000
$4,000
$5,000
$6,000
$7,000
$8,000
$9,000
$10,000
Medical Only Claims
Indemnity Claims
Medical Only Claims $712 $712 $565 $565
Indemnity Claims $8,596 $4,606 $3,991 $5,546 $3,293 $2,074
2001 Ave WC
Cost/claim
2001 Ave Medical
Cost/Claim
2001 Average
Indemnity
2002 Ave WC
Cost/claim
2002 Ave Medical
Cost/Claim
2002 Average
Indemnity

Complex ProblemWorker’s Compensation Costs
General Health Insurance
Disability
Medical Community
OSHA Regulations
UnionsADA
Aging Workforce
Employee Health and Wellness
Job Accommodation
FMLA EEOC
Competition
DownsizingTurnover

THE SPINE
The Vertebrae

THE DISC

THE NERVES and SPINAL CORD

MUSCLE STRAINS/SPRAINS

Awkward Joint Positions Awkward Joint Positions and Posturesand PosturesRisk Factors for LBP Bending and leaning Excessive reach especially with weight Heavy lifting Static awkward positions Twisting Constant sitting

Poor Physical ConditionPoor Physical Condition
It is not always the work that causes injury,
it is the lack
of physical
condition to
perform the work

ERGONOMICS IS AN INEXACT SCIENCE

Unnecessary Strain Can Be Caused by:
Excessive Reaching Prolonged Static Positions Awkward Postures Repetitive Motions Bending and Twisting Faulty Ergonomic Workstations

The mechanics of the spine and lifting
The amount of force you place on your back in lifting may surprise you!

The Forces InvolvedWhen you add in the average weight of 105 pounds for the upper torso, you see that lifting a ten pound object actually puts 1,150 pounds of pressure on the lower back.

The Forces InvolvedIf you are 25 pounds
overweight, it would add
an additional 250
pounds of pressure
on your back
every time you
bend over.

The lifting solution Wide base of support
Object in center of stance Neutral spine Butt down Grasp object with both hands
Hug the load Raise with head and shoulders first
Slow and smoothly Keep spine in neutral
Once standing, move your feet in the direction you are going to move in, do not twist Repeat to put load down

The message is….TAKE CARE OF YOUR BACK
……And it will take care of you Exercise daily Get the proper amount of sleep/rest Eat right Do not ignore your signs and symptoms Limit your exposures during “heavy” lifting Get Help with heavy or bulky objects If you must bend, do it properly Avoid twisting at the waist when moving objects Always be aware of your environment and watch where
you are going Work with your environment not “in it”

Job Accommodation
Does the Functional Capacity of the Injured Worker Meet the Physical
Demands of the Job?
If Yes � Assign Job
If No � Modify Job or
Improve Worker Tolerance

Accommodations
Possibilities Restructure jobs-
Reassign parts of jobs Alter Physical Facilities Acquire or modify equipment or device Modify Work schedules Provide readers or interpreters Reassignment of Employee (last resort)
Experts on Accommodation #1 the disabled person #2 the rehab professional

Improve Worker Tolerance Gradual exposure to
unaccustomed work Restrict overtime Gradual increase in weight
lifted/ forces Gradual increase to
Cardiovascular demands Monitor Progress!

Distribution by Hour of Shift
12.30%
10.20%
10.10%
8.80%
7.30%
6.90%
6.40%
5.60%
7.80%
0% 2% 4% 6% 8% 10% 12% 14%
1st
3rd
5th
7th
9th

Nature of Injury
50.90%
8.80%
8.30%
7.70%
3.20%
0.02
1.90%
0% 10% 20% 30% 40% 50% 60%
Sprains, Strains
Cut, Laceration
Contusion, Bruise
Fracture
Multiple Injuries
Hernia Rupture
Nervous System
East

FIT FOR WORK“Stretching Programs”
Warm-up exercises Stretching exercises All major muscle groups Performed in standing position Ten minutes to complete Flexibility tests Injured workers can perform the
program Progression: Isometrics
(Strengthening)? “Stick with it”

Work Site Visits/ Evaluations Patient education/ understand their work Ergonomic evaluation & recommendations Job task analysis /ADA Risk analysis Communications/
close the loop Build relationships

BACK SCHOOLS Quiz Introduction: Prevalence of back problems, issues, etc.. Teach functional Anatomy & Physiology of the spine Understand different types of back disorders: Disc
herniations,muscle strains, arthritis, joint stiffness, etc. Explain risk factors: Poor postures, body mechanics, physical
fitness, ergonomic considerations Describe diagnostics and treatments: X-rays, MRIs,
manipulation, encourage active forms of treatments and early mobility
Proper lifting and body mechanics Prevention: work site problem solving,
discussion, Activities of daily living

PREVENTATIVE EDUCATIONAL PROGRAMS
� Back Schools� CTD Schools� VDT training� FIT FOR WORK Stretching
Program� Ergonomics training� Supervisor Work Injury
Management� Customized programs

Back Injuries in Health Care Settings
A Long Term Care Provider’s A Long Term Care Provider’s PerspectivePerspective
Susanne Heeschen, RNCDirector of OperationsSandy River Health Care Systems
Who Are We?
Maine based Long Term Care ProviderPresent in 12 Communities Throughout
Maine777 Skilled Nursing Beds215 Assisted Living BedsOne Outpatient BI Rehab ProgramTwo Adult Day Care Programs

Employee ProfileTotal Employees 1535Total Nursing Employees 1032 (67%)Total Employees age 50 and Over 445
(29%)Total Nursing Employees age 50 and
Over 259 (58% 0f all employees age 50 & over)

Safety Management Profile
2002 65% of total incidents First Aid 29% of total incidents Medical Only 6% of total incidents Lost Time 75% of total incidents Nursing 31% of total incidents Strains 14% of all incidents Resident Behavior

Other Data 2001 20022001 2002Total Claims 211 227 7% inc.Total $$ 389,717 333,006 14.5% dec.Ave$/injury 1847 1467 20% dec.Total Spr/Str 130 146 12% inc.Ave$/Spr-Str 2162 1983 8% dec.Exp Mod .90 .84 ( 2003 .78 )

What Makes A Difference? Culture Commitment to Prevention Safety Committee Tracking and Trending Training Equipment-Availability and Use Effective Occupational Health Services Claims Management Early Return to Work Efforts

ChallengesNature of Patient Care in LTC SettingsKeeping Staff Current in Their PracticesFundingAging WorkforceHealthcare Worker ShortageHealth Care Practices of Workers

A Management Process to Improve Outcomes in Healthcare Applying
Guy Fragala, PhDGuy Fragala, PhDDirector of Environmental Health and SafetyDirector of Environmental Health and SafetyUniversity of Massachusetts Medical CenterUniversity of Massachusetts Medical Center

G o o d E n g i n e e r i n g S o l u t i o n s G o o d M a n a g e m e n t P r o g r a m
T h e E r g o n o m i c M a n a g e m e n t P r o c e s s
R e d u c e d L o s s a n d I m p r o v e d O u t c o m e s

A Simple Look at an ERGONOMIC APPROACH
1. Identify jobs and job tasks which stress body parts beyond limits.
2. Develop solutions to change these task demands.
3. Implement these changes in the work place.
4. Review the design of the physical work environment to remove barriers, minimize travel and consider spacial relations.

Initiation Team Members Safety and health function Human Resources/Workers’ Compensation Manager or supervisor Rehab or therapy specialist Direct care staff Senior administrator Who else? Who will champion?

Scope of the Problem
Cure world hungerFeed a few hungry people

What are Occupational Injuries Costing You?
Direct cost Indirect costHow are you paying?

A 5 Step Process
STEP 1 - Risk Identification and Assessment
STEP 2 - Risk Analysis
STEP 3 - Develop Recommendations
STEP 4 - Program Implementation
STEP 5 - Measurement and Results

Step 1: Risk Identification and Assessment
Perceived high risk jobsSpecific high risk job tasksElement of high risk job tasksHigh risk departments or areasTask intensity and durationWork posturesGeneral design of equipment and
spaceWhere do we think problems exist?

Methods to Gather Data General observation Employee discussions Employee questionnaires Review of medical data Symptom surveys Quantitative evaluations Previous studies Job consistency and fatigue Brainstorming and group activities

Patient Handling Tasks Transferring patient from bathtub to chair Transferring patient from chair to bed Weighing patient Transferring patient from toilet to chair Making bed with patient in it Transferring patient from bed to chair Transferring patient from chair to toilet Undressing patient Repositioning patient in chair Making bed when patient is not in it Lifting patient up in bed Feeding bed-ridden patient Changing absorbent pad Repositioning patient in bed

Step 2: Risk Analysis
Confirm perceived problemsAnalyze cost dataSpecify high risk jobs and areasSet prioritiesFormal job analysisStudy risk factorsQuantify risk factors

Step 3: Develop Recommendations
Achievable and simpleConstraintsApproaches
Engineering Administrative

Engineering Control Strategies …the preferred control method
Eliminate the need to do the hazardous activity
Redesign the activity to reduce the hazard
Utilize an aiding device to minimize the hazard

Basic Transfer AidsGait belts with handlesHand slingsSliding boardsStand assist and repositioning aids
on furnishings on walls self supporting

Gait/Transfer Belt with Handles
What do you do? Fit the belt around the patient’s
waist
What happens next? Use the handles to improve your
grasp
What are they used for? Assisting and transferring
partially dependent patients

Sliding Boards

Lateral Transfer Aids
Friction reducing lateral slide aids rigid boards flexible sheets rollers air assisted
Mechanical lateral transfer aids hand cranks electric motor

Friction Reducing Lateral Sliding Aids
Friction Reducing Lateral Sliding Aids

Mechanical Lateral Transfer Aids
What do you do? Position the device as
directed What happens next?
Start the motor or turn the crank to slide the patient over to the new surface
What are they used for? Lateral transfers

Mechanical LiftsPortable base full slingPortable base stand assistCeiling mounted trackWall mountedBathingPool Automobile

Floor-Based Ceiling-Mounted
Powered Full Body Sling Lifts

Powered Standing Assist and Repositioning Lifts

Ergonomic Furnishings
Transfer chairBed improvements
aiding transfers minimizing transfers minimizing repositioning
StretchersToiletsTubs and showers


Resident Dependency Classification
Height Adjustable
BedFull Sling Lift
Stand Assist Lift
Lift WalkerStand Assist
AidGait Belt with
HandlesFriction Reducing
Aid
0 - Independent
Recommended
Never Rarely Rarely Rarely Rarely Rarely
1 – Supervision
Recommended
RarelyOccasionally Occasionally Normally Occasionally
Rarely
2 – Limited Assistance
StronglyRecommende
dRarely
Normally Normally Normally Normally Normally
3 – Extensive Assistance
Required Normally Normally NormallyRarely Rarely
Always
4 – Total Dependence
Required AlwaysNever Never Never Never
Always
Lift Aid Equipment Determination Grid(recommended example)
For a typical resident with the dependency status classification as shown, this grid indicates normal equipment requirements to conduct a safe transfer. Some residents may have special characteristics
and not exactly match a typical profile. In those situations, special consideration will be required.

Step 4: Program Implementation
The Implementation TeamEducation and training Involve everyone affectedResistance to changePolicies and proceduresGoals and objectivesMedical management

Traditional Back Injury Training Efforts
The comprehensive all-inclusive back school The traditional most popular approach
training in lifting and body mechanics Evaluating the true effectiveness of these
approaches Is it time for a change? What are the barriers to change?

Step 5: Measurement and Results
Select measures Improvements
Quality of work life Quality of care
Reporting resultsOngoing efforts and interestContinuous improvement cycle

Effective Ergonomic Interventions in Healthcare
Results of what has been achievedHow was the program implemented? Key points contributing to success

Summary of Improvement from Ergonomic Management ProgramMasonic Home and Hospital
Pre-Intervention Post-Intervention
Annual lost work days 1,025 81
Injury assessments four-month period
$174,412 $4,500
Incurred annual workers compensation
costs $628,511 $142,995

The Champion
Assistant Director of
Human Resources

Reason for Improvement
1,025 lost workdays
$628,511 direct cost

Risk IdentificationBrainstorming sessions
Created buy-in Perceived high risk activity

Risk Analysis
No correlation with staffing patterns and injuries
Existing training programs not effectiveConfirmed high risk units

Formulation of Recommendations
Engineering Controls Mechanical lifts Gait belts

Implementation
Initiation team became Implementation and CQI Team
High interaction of team with staffKey operator/unit contact

Evaluation
Lost workdaysDirect cost of injury
Workers comp premiums Injury incurred cost

Key Points Contributing to Success
Establish the need Define the problem Form the team Establish top management support Provide educational awareness for buy-in Involve staff Create and follow a time line

















