More Than Just Three Pairs of Stalks: Comprehensive Interactive Case Review of Bilateral Cerebellar Peduncle Abnormalities Yin Jie Chen 1 , Andreas Rauschecker 1 , Arastoo Vossough 2 , Laurie A. Loevner 1 , Suyash Mohan 1 1. Department of Radiology, Hospital of the University of Pennsylvania 2. Department of Radiology, Children’s Hospital of Philadelphia Control #: 1252 eEdE-02-7538
Transcript
More Than Just Three Pairs of Stalks: Comprehensive Interactive Case Review of
Bilateral Cerebellar Peduncle Abnormalities
Yin Jie Chen1, Andreas Rauschecker1, Arastoo Vossough2, Laurie A. Loevner1, Suyash Mohan1
1. Department of Radiology, Hospital of the University of Pennsylvania2. Department of Radiology, Children’s Hospital of Philadelphia
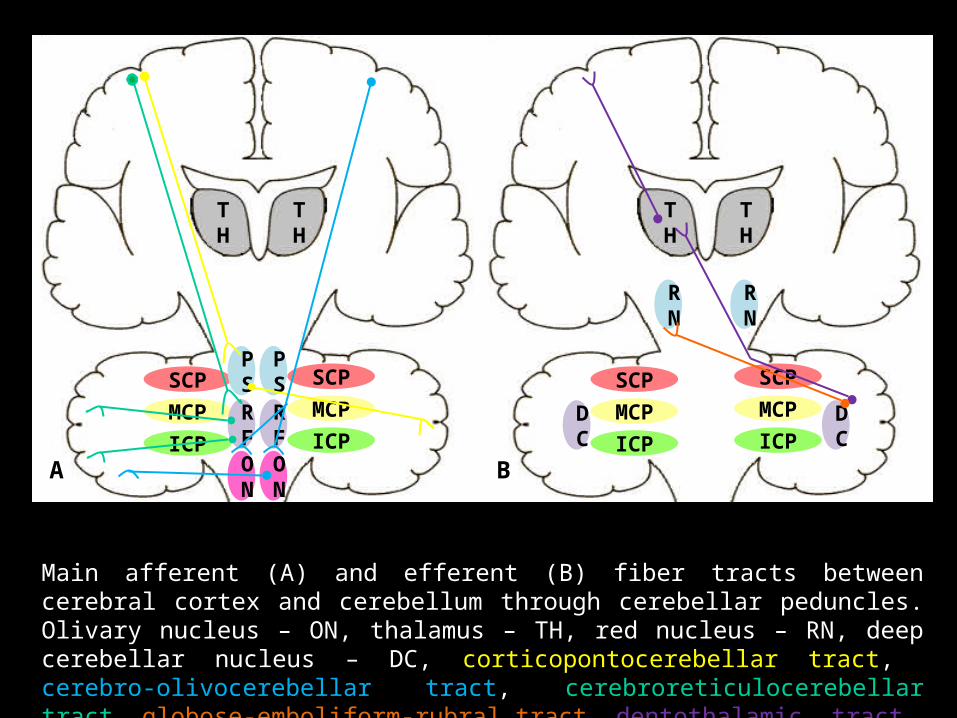
Main afferent (A) and efferent (B) fiber tracts between cerebral cortex and cerebellum through cerebellar peduncles. Olivary nucleus – ON, thalamus – TH, red nucleus – RN, deep cerebellar nucleus – DC, corticopontocerebellar tract, cerebro-olivocerebellar tract, cerebroreticulocerebellar tract, globose-emboliform-rubral tract, dentothalamic tract.
A
SCPMCPICP
SCPMCPICP
PS
PS
RF
RF
B
SCPMCPICP
SCPMCPICP
RN
RN
DC
DC
ON
ON
TH
TH
TH
TH
Important Fiber Tracts• Corticopontocerebellar tract
– Conveys information on planning and initiation of movement
– From cerebral cortex to contralateral cerebellum
• Cerebro-olivocerebellar tract– Conveys control from cerebral cortex
to cerebellar cortex via inferior olivary nuclei and climbing fibers
– Terminate directly on Purkinje cells
• Cerebroreticulocerebellar tract– Involved in regulation of voluntary
movement– In particular adjustment of muscle
activity as result of cortical input – Input primarily from sensorimotor
areas
• Globose-emboliform-rubral tract– Controls ipsilateral motor activity – Connection from globose and
emboliform nuclei to contralateral red nucleus, then crossing via rubrospinal tract to ipsilateral motor neurons in spinal cord
• Dentothalamic tract– Affects ipsilateral motor activity – Connection from dentate nucleus
to contralateral ventrolateral nucleus of the thalamus, in turn connecting to contralateral cerebral motor cortex
PEDIATRIC POPULATIONINTERACTIVE CASE SERIES
15 M boy with developmental delay, hypotonia, abnormal breathing patterns, and polydactyly
Axial T1 MPRAGE pre-contrast and axial T2 images show “molar tooth” sign with deep interpeduncular fossa and thick straight SCPs, as well as hypoplastic vermis.
T1-Pre T1-Pre
Dx: Joubert Syndrome
T2
Joubert Syndrome• Clinical features
– Autosomal recessive – 1 of 13 mutations pos in >75% – Defects in primary cilium– Facial dysmorphism– Polydactyly– Most children reach adulthood– Outcome not related to severity of
imaging findings– Spectrum of abnormalities
• Developmental delay / mental retardation
• Hypotonia• Respiratory difficulties• Seizures• Occulomotor, oral-motor, and speech
problems
• Diagnostic pearls – "Molar tooth" sign
• Deep interpeduncular fossa• Thick, straight SCP• Hypoplastic vermis
– Absence of fiber decussation– Joubert Syndrome-related Disorders
• “Molar tooth” sign plus other signs• Cerebello-oculo-renal syndrome• COACH syndrome (Coloboma,
• "Molar tooth" sign not a feature– Chiari malformation
• Obliteration of cisterna magna– Mega cisterna magna
• No associated malformation
Patient with Joubert Syndrome Normal Patient
Diffusion tensor imaging shows absence of decussation of fibers (transversely oriented fibers in red) at the level of SCPs in
patient with Joubert Syndrome, compared to normal patient
16 Y/M with developmental delay now with progressive gait abnormality & palatal myoclonus
Axial T1 pre-contrast image show intrinsic T1 hyperintensities in the supratentorial deep white matter. Axial T1 pre and post images demonstrate faint enhancement in deep cerebellar structures. Axial FLAIR images show supratentorial and infratentorial FLAIR hyperintensities, with sparing of the deep gray structures and subcortical white matter.
T1-Pre T1-Pre T1-Post
FLAIR
Dx: Alexander Disease
Alexander Disease
Infantile Alexander Disease with bifrontal
white matter abnormalities
• Diagnosed by genetic testing – GFAP gene (D360H missense mutation for this
12 y/o) forms– Accumulation of Rosenthal fibers (RFs) in astrocytes
& hypo-/demyelination
– Diagnostic pearls • Enhancement in brainstem and cerebellar peduncles
typically exist early in disease course (non-infantile forms)
• Infantile form more localized abnormalities in bifrontal white matter
• Rostral-caudal gradient less pronounced in juvenile/adult forms
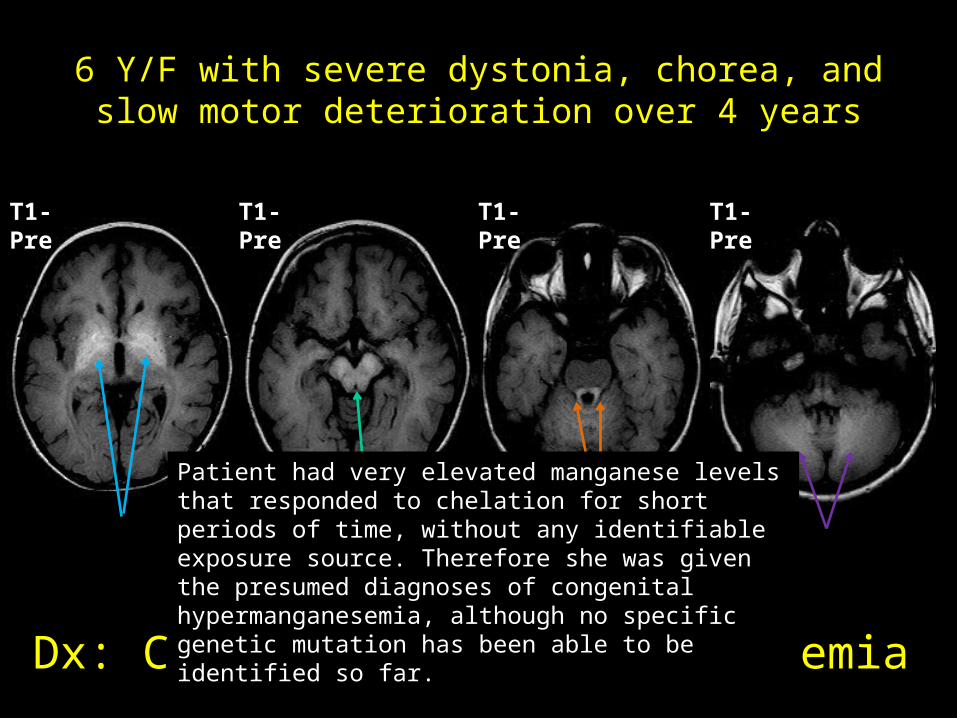
6 Y/F with severe dystonia, chorea, and slow motor deterioration over 4 years
Axial T1 pre-contrast images show intrinsic T1 hyperintensities in the basal ganglia, midbrain, SCP, and cerebellar hemispheres. No signal alterations on other sequences.Dx: Congenital Hypermanganesemia
Patient had very elevated manganese levels that responded to chelation for short periods of time, without any identifiable exposure source. Therefore she was given the presumed diagnoses of congenital hypermanganesemia, although no specific genetic mutation has been able to be identified so far.
T1-Pre T1-Pre T1-Pre T1-Pre
Hypoplasia of pons and MCPs in newborn with feeding difficulty who was diagnosed with
PTCD
• Other leukodystrophies– Krabbe Disease– X-linked adrenoleukodystrophy– Mitochondrial leukodystrophy
• Pontine tegmental cap dysplasia (PTCD)
• Maple syrup urine disease (MSUD)
• Other leukodystrophies– Krabbe Disease– X-linked adrenoleukodystrophy– Mitochondrial leukodystrophy
• Pontine tegmental cap dysplasia (PTCD)
• Maple syrup urine disease (MSUD)
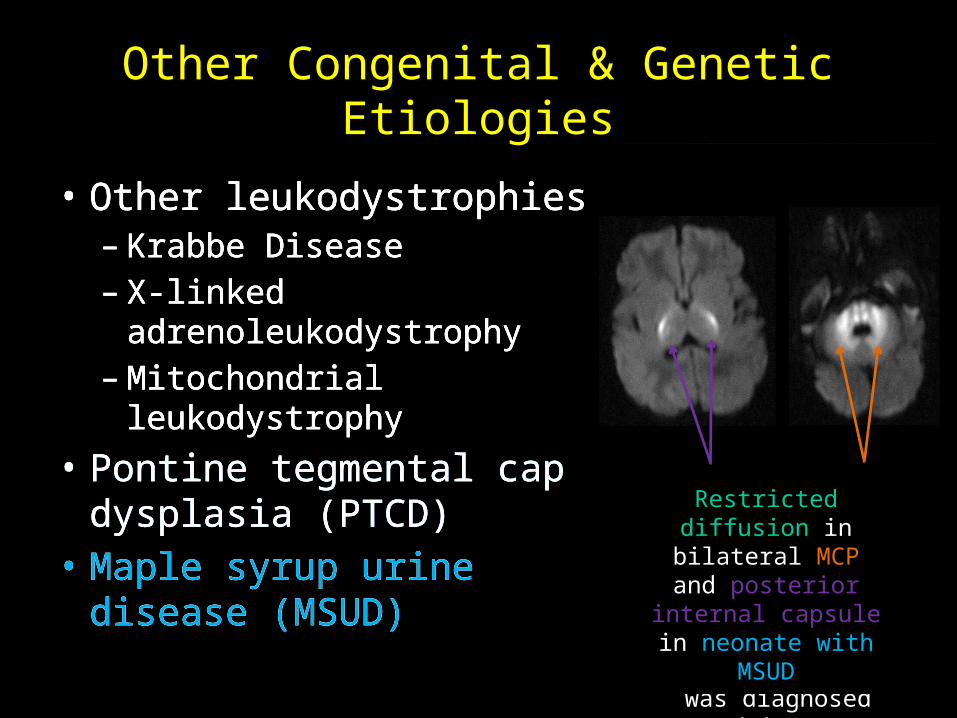
Other Congenital & Genetic Etiologies
• Other leukodystrophies– Krabbe Disease– X-linked adrenoleukodystrophy– Mitochondrial leukodystrophy
• Pontine tegmental cap dysplasia (PTCD)
• Maple syrup urine disease (MSUD)
• Other leukodystrophies– Krabbe Disease– X-linked adrenoleukodystrophy– Mitochondrial leukodystrophy
• Pontine tegmental cap dysplasia (PTCD)
• Maple syrup urine disease (MSUD)
Restricted diffusion in bilateral MCP and posterior internal
capsule in neonate with MSUD
GERIATRIC POPULATIONINTERACTIVE CASE SERIES
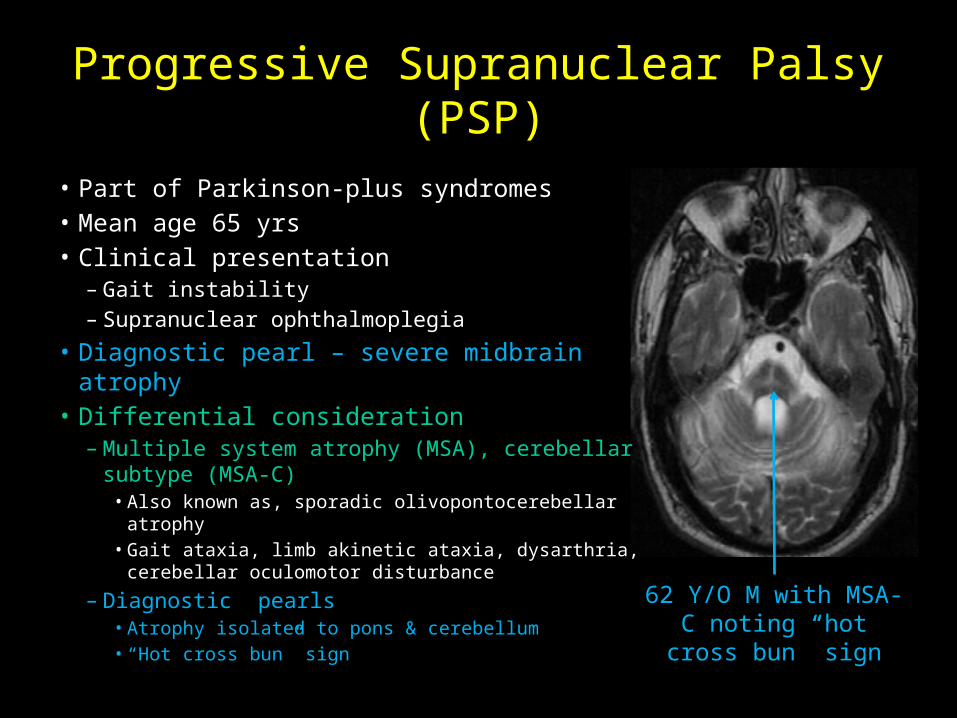
Axial T2 image demonstrates bilateral MCP hyperintensities. Coronal T2 image depicts diffuse supratentorial and infratentorial volume loss. Sagittal T1 image shows midbrain atrophy, so called “hummingbird” sign.Dx: Progressive Supranuclear Palsy
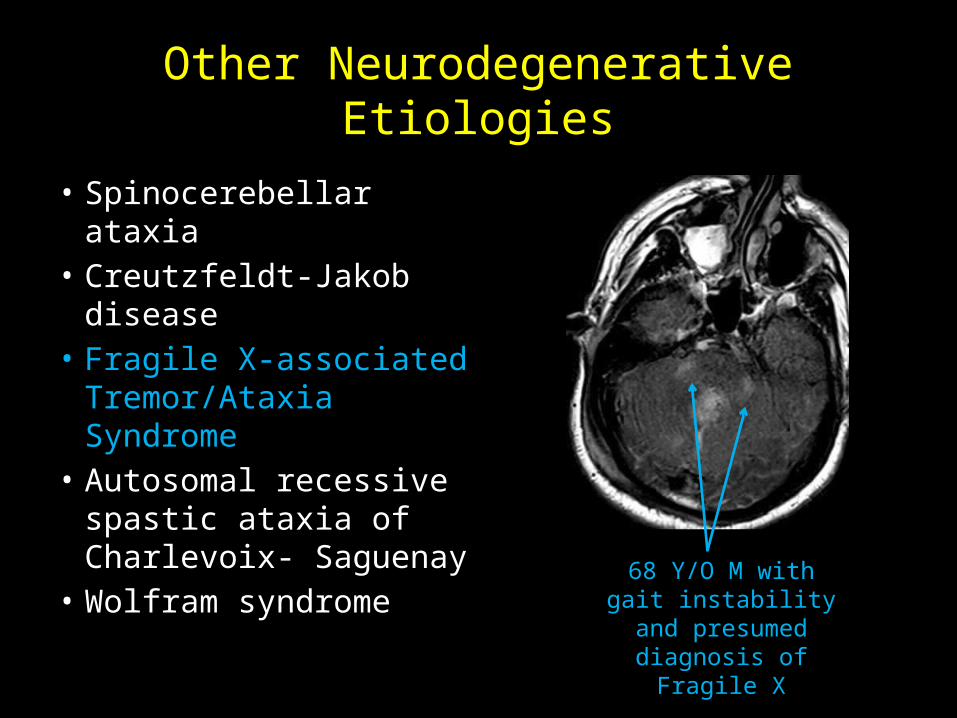
• Autosomal recessive spastic ataxia of Charlevoix- Saguenay
• Wolfram syndrome
68 Y/O M with gait instability and
presumed diagnosis of Fragile X
• Spinocerebellar ataxia• Creutzfeldt-Jakob
disease• Fragile X-associated
Tremor/Ataxia Syndrome
• Autosomal recessive spastic ataxia of Charlevoix- Saguenay
• Wolfram syndrome
ALL AGESINTERACTIVE CASE SERIES
Axial T1 image shows intrinsic T1 hyperintensity in basal ganglia bilaterally. Axial FLAIR image demonstrates FLAIR hyperintensity in MCP bilaterally. After receiving proper treatment, axial FLAIR image from six months later depicts decreased hyperintensity in MCP bilaterally.
Dx: Hepatic Encephalopathy
60 Y/F with long history of alcohol abuse present with headache, speech disturbance, & tremors
T1-Pre FLAIR
Six Months Later
FLAIR
Hepatic Encephalopathy• Occurs in severe liver dysfunction• Occurs in more than 50% cirrhotic
patients• Clinical presentation
– Altered mental status– Motor abnormalities (e.g., tremor,
ataxia, etc)– Fetor hepaticus
• Diagnostic pearls– Liver dysfunction, most commonly
caused by alcohol– T1 hyperintensity in basal ganglia
• Thought to be secondary to manganese deposition
• Similar to congenital hypermanganesemia
– FLAIR hyperintensity within hemispheric white matter and corticospinal tract
Companion Case:31 Y/M with alcohol abuse , tremors, & Wernicke's encephalopathy (symptoms improved with thiamine & folate). T2
hyperintensities within bilateral mammillary bodies and MCP.
Other Metabolic Etiologies
• Wilson disease• Extra-pontine
myelinolysis• Hypoglycemia• Toluene toxicity
23 Y/F with Wilson’s Disease, noting T1 hyperintensity in
basal ganglia and bilateral MCP T2 hyperintensity
• Wilson disease• Extra-pontine
myelinolysis• Hypoglycemia• Toluene toxicity
Axial FLAIR images demonstrate FLAIR hyperintensities in bilateral posterior internal capsule, right occipital lobe, and MCP. Axial DWI and ADC images depict a focus of restricted diffusion in right MCP.
Dx: Posterior Reversible Encephalopathy Syndrome
56 Y/F with AML admitted for acute renal failure presented with abnormal eye movements
Companion Case:Cyclosporine toxicity with FLAIR hyperintensity in thalami, pons, parieto-occipital white matter &
cerebellum. Note: vasogenic edema
• Most commonly seen in acute / malignant hypertension – Disruption of auto-regulation
and blood brain barrier – Several other causes including
drug toxicity
• Diagnostic pearls – Patchy foci of T1 hypo- and T2
hyper-intensities in posterior circulation
– Usually only vasogenic edema, but can have foci of cytotoxic edema
• Unknown Case One • Unknown Case Two• Bilateral anterior inferior cerebellar arteries (AICA) infarct
• Wallerian degeneration of pontocerebellar tracts
Other Cerebrovascular Etiologies
43 Y/F status post TEVAR, noting bilateral restricted diffusion in AICA territory
61 Y/M with recent pontine infarct due to basilar artery stenosis now with bilateral MCP FLAIR hyperintensities
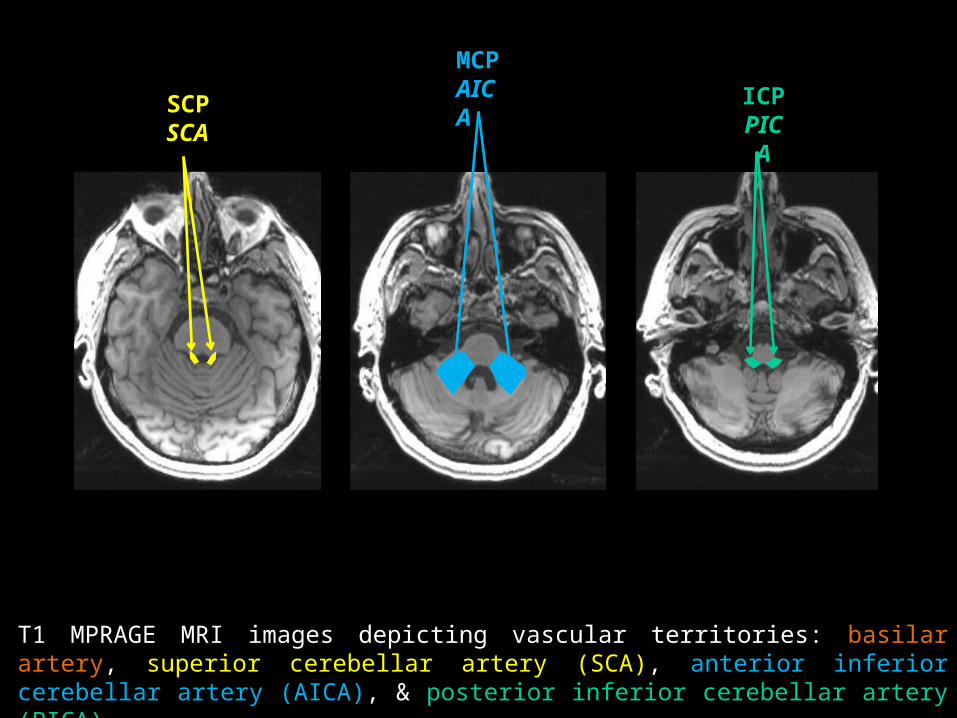
POP QUIZWhat is the arterial blood supply to the MCP?A. Superior cerebellar arteryB. Anterior inferior cerebellar arteryC. Posterior inferior cerebellar arteryD. Basilar artery
POP QUIZWhat is the arterial blood supply to the MCP?A. Superior cerebellar arteryB. Anterior inferior cerebellar arteryC. Posterior inferior cerebellar arteryD. Basilar artery
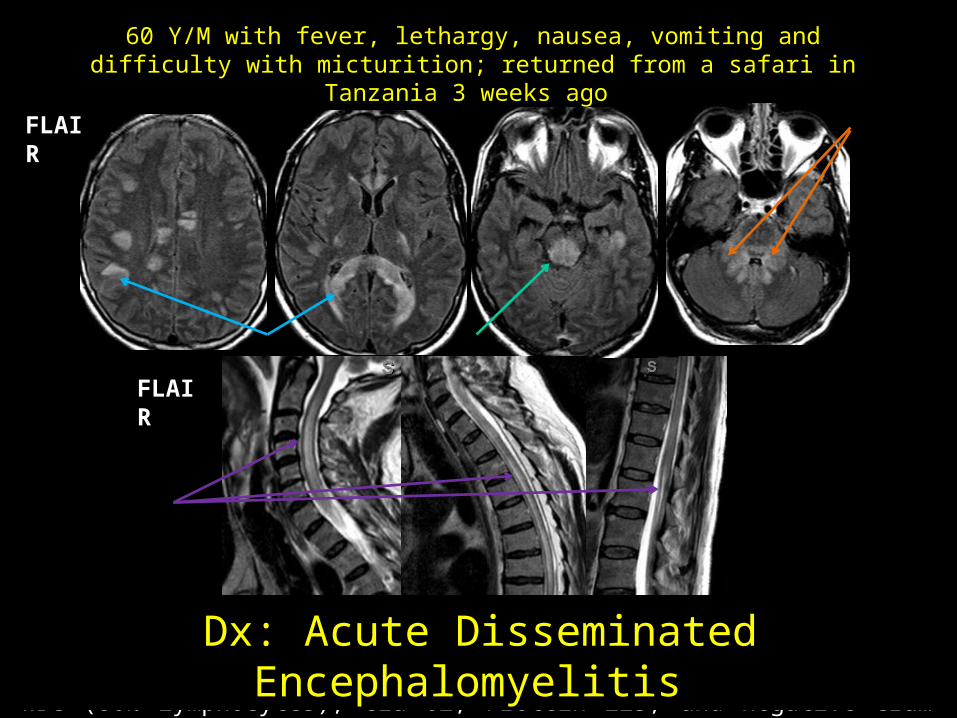
FLAIR images of the brain and spine demonstrate FLAIR hyperintensities in the subcortical / deep white matter, midbrain, MCP, and spine cord. CSF studies showed 8 RBC, 385 WBC (86% lymphocytes), Glu 62, Protein 223, and negative Gram stain and culture.Dx: Acute Disseminated Encephalomyelitis
60 Y/M with fever, lethargy, nausea, vomiting and difficulty with micturition; returned from a safari in Tanzania 3 weeks ago
FLAIR
FLAIR
Acute Disseminated Encephalomyelitis (ADEM)
• Autoimmune-mediated acute demyelination
• Prodromal phase (fever, malaise, myalgia), followed by symptoms such as headache and drowsiness, with progression to lethargy or even coma
• Diagnostic pearls– Multifocal T2/FLAIR white matter
hyperintensities,– Possibly also deep grey structures – Following recent infection, often
viral (can be post-vaccination)
Companion Case:51 Y/M with AML s/p SCT
with acute encephalopathy
FLAIR hyperintensities in periventricular WM, midbrain,
and cerebellar peduncles (bilateral SCP, MCP, and ICP,
top to bottom)
Dx: Immune-mediated Demylination (Presumed to be related to SCT)
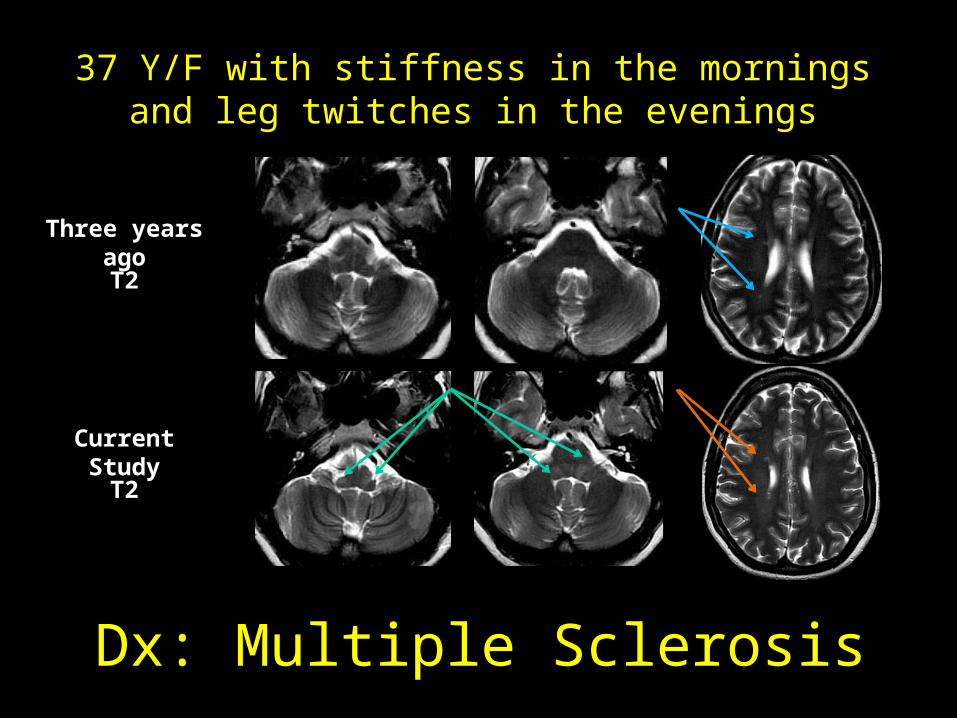
MRI from three years ago shows scatter periventricular T2 hyperintensities. Current study shows new T2 hyperintensities involving both ICPS, in addition to the periventricular lesions.Dx: Multiple Sclerosis
37 Y/F with stiffness in the mornings and leg twitches in the evenings
Three years ago
T2
T2
Current Study
Multiple Sclerosis• Demographics
– Age: 20-40 years– Prevalence: F > M– Caucasian most common– Variable symptoms
• Weak, numb, tingling, gait disturbance, • Optic neuritis, other cranial nerve palsies• Spinal cord involved in 80%
– Infratentorial in 10%– Acutely demyelinating lesions can enhance
(nodular or ring)– Polyphasic
• Relapsing-remitting – most common (>80%)• Secondary-progressive• Primary-progressive• Progressive-replapsing – rare
Companion Case:MS patient with scattered FLAIR
hyperintensities in periventricular white matter and bilateral MCP
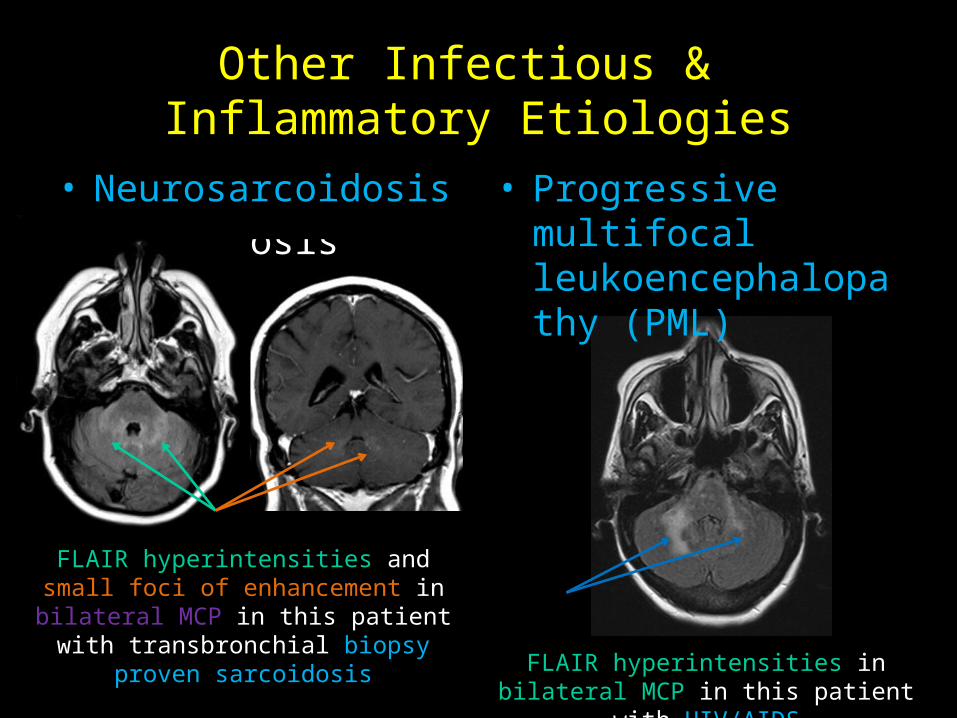
• History of sarcoidosis• Neurosarcoidosis
Other Infectious & Inflammatory Etiologies
FLAIR hyperintensities and small foci of enhancement in bilateral MCP in this patient with transbronchial biopsy proven sarcoidosis
FLAIR hyperintensities in bilateral MCP in this patient with HIV/AIDS
• History of HIV/AIDS• Progressive multifocal leukoencephalopathy (PML)
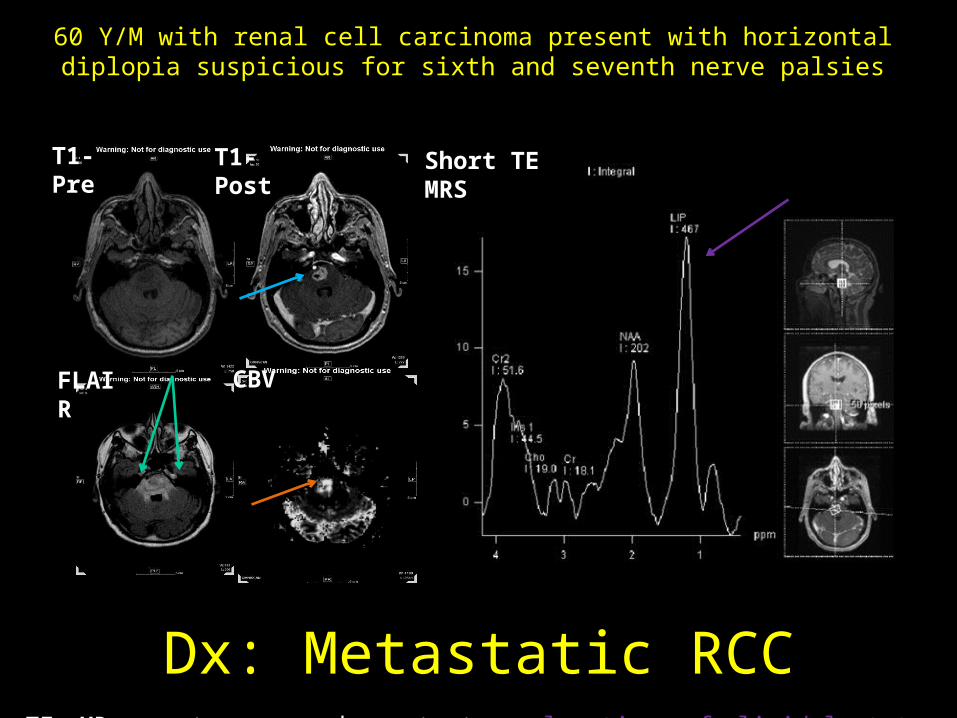
Axial T1 pre and post contrast images shows a heterogeneously enhancing mass centered in the pons, associated with surrounding FLAIR hyperintensities extending into bilateral MCP, as well increased relative cerebral blood volume. Short TE MR spectroscopy demonstrates elevation of lipid-lactate peaks.
Dx: Metastatic RCC
60 Y/M with renal cell carcinoma present with horizontal diplopia suspicious for sixth and seventh nerve palsies
T1-Pre T1-Post
FLAIR CBV
Short TE MRS
Metastatic RCC• Stereotactic biopsy - clear cell carcinoma consistent with
renal origin• Diagnostic pearls
– Known primary malignancy, especially with known metastases elsewhere
– Mass with aggressive features on perfusion and spectroscopy studies
• Differential consideration– Glioma
• Enhancement pattern varies depending on type• Often less surrounding vasogenic edema than metastases
– Lymphoma • More homogenous enhancement • Usually hyperdense on CT and can show restricted diffusion
– Radiation changes / necrosis• Expect to decrease over time• Necrosis
– Most often 12-24 months post radiation– Expect very low NAA, Cho, and Cr peaks on MR spectroscopy
FLAIR hyperintensity in bilateral MCP from
radiation change related to prior treatment of left
temporal lobe astrocytoma
15 Y/M with tectal pilocytic astrocytoma s/p resection & proton therapy, now with refusal to speak
Pre-operative T1-MPRAGE pre-/post-contrast images show avidly enhancing tectal mass. Post-treatment MRI (when patient presented with mutism) show no residual enhancing tumor and increased FLAIR signal in the both SCPs.
Pre-Operative Current Exam
T1-Pre
Dx: Cerebellar Mutism Syndrome
T1-Pre
T1-Post T1-Post
FLAIRFLAIR
Cerebellar Mutism Syndrome• Also called posterior fossa
syndrome• Typically occur after resection
of posterior fossa tumors• Incidence post midline
posterior fossa tumor resection as high as 40%
• Clinical symptoms– Transient mutism (days to
weeks)– Cognitive & behavioral issues– Emotional liability– Persistent ataxia and motor
coordination issues can occur
• Attributed to damage of bilateral dentate nuclei or cerebellar output pathways (SCPs)
• SCPs vulnerable during resection due to their close relationship to the 4th ventricle
• Ojemann JG, et al., showed that diffusion tensor imaging of SCPs can identify patients who did and did not develop cerebellar mutism syndrome in a small sized patient population
Conclusions
• SCP, MCP, and ICP are vital to proper communication between cerebral cortex and cerebellum
• Bilateral cerebellar peduncle abnormalities can be seen in many disease processes
• Considering image findings in the appropriate clinical settings is vital in narrowing differential diagnoses
• Diagnostic considerations– Congenital & genetic causes common in pediatric population– Neurodegenerative causes common in geriatric population– Most other causes can be seen in all age groups
Conclusions
• Disease specific diagnostic pearls– Congenital & Genetic
• Joubert Syndrome – “Molar tooth” sign• Alexander Disease - enhancement in brainstem and cerebellar
peduncles early in disease course (non-infantile forms)• Congenital hypermanganesemia – abnormal heavy metal labs• Pontine tegmental cap dysplasia – newborn with hypoplasia
• Disease specific diagnostic pearls, continued– Metabolic
• Hepatic encephalopathy – alcohol most common causative agent• Wilson disease - T1 hyperintensity in basal ganglia
– Cerebrovascular • PRES – HTN or drug toxicity, posterior circulation abnormalities• Stroke – AICA territory, rare to have bilateral• Wallerian degeneration of pontocerebellar tracts – prior pontine
insult
– Infectious & inflammatory • ADEM – most commonly follow viral infection, monophasic• MS – multiple lesions separate in space and time
Conclusions
• Disease specific diagnostic pearls, continued– Neoplastic
• Metastases - Known primary malignancy• Glioma – less surrouding vasogenic edema• Lymphoma – more homogenous enhancement• Radiation changes / necrosis – within radiation portal • Cerebellar mutism syndrome – post-resection of
posterior fossa tumor, abnormal signal in SCPs
References• Apartis E, Blancher A, Meissner WG, et al. FXTAS: new insights and the need for revised diagnostic criteria. Neurology. 2012;79(18):1898-907.• Graff-Radford J, Schwartz K, Gavrilova RH, et al. Neuroimaging and clinical features in type II (late-onset) Alexander disease. Neurology.
2014;82(1):49-56.• Ito S, Sakakibara R, Hattori T. Wolfram syndrome presenting marked brain MR imaging abnormalities with few neurologic abnormalities. AJNR Am
J Neuroradiol. 2007;28(2):305-6.• Kataoka H, Izumi T, Kinoshita S, et al. Infarction limited to both middle cerebellar peduncles. J Neuroimaging. 2011;21(2):e171-2.• Lee NK, Lee BH, Hwang YJ, et al. Serial computed tomography and magnetic resonance imaging findings of biphasic acute hemorrhagic
leukoencephalitis localized to the brain stem and cerebellum. Jpn J Radiol. 2011;29(3):212-6.• Liptai Z, Papp E, Barsi P, et al. Progressive multifocal leukoencephalopathy in an HIV-infected child. Neuropediatrics. 2007;38(1):32-5.• Maria B, Quisling RG, Rosainz LC, et al. Molar tooth sign in Joubert Syndrome: clinical, radiologic, and pathologic significance. J Child Neurol.
1999;14:368-76.• Nishida T, Tokumaru AM, Doh-Ura K, et al. Probable sporadic Creutzfeldt-Jakob disease with valine homozygosity at codon 129 and bilateral
middle cerebellar peduncle lesions. Intern Med. 2003;42(2):199-202.• Ojemann JG, Partridge SC, Poliakov AV, et al. Diffusion tensor imaging of the superior cerebellar peduncle identifies patients with posterior fossa
syndrome. Childs Nerv Syst. 2013;29:2071-7.• Okamoto K, Tokiguchi S, Furusawa T, et al. MR features of diseases involving bilateral middle cerebellar peduncles. AJNR. 2003;24(10):1946-54.• Preziosa P, Rocca MA, Mesaros S, et al. Relationship between damage to the cerebellar peduncles and clinical disability in multiple sclerosis.
Radiology. 2014;271(3):822-30. • Reginold W, Lang AE, Marras C, et al. Longitudinal quantitative MRI in multiple system atrophy and progressive supranuclear palsy. Parkinsonism
Relat Disord. 2014;20(2):222-5.• Shimazaki H, Takiyama Y, Honda J, et al. Middle cerebellar peduncles and Pontine T2 hypointensities in ARSACS. J Neuroimaging. 2013;23(1):82-5.• Suzuki K, Wakayama Y, Takada H, et al. A case of chronic toluene intoxication with abnormal MRI findings: abnormal intensity areas in cerebral
white matter, basal ganglia, internal capsule, brain stem and middle cerebellar peduncle. Rinsho Shinkeigaku. 1992;32(1):84-7.• Wells EM, Khademian ZP, Walsh KS, et al. Postoperative cerebellar mutism syndrome following treatment of medulloblastoma: neuroradiographic
features and origin. J Neurosurg Pediatrics. 2010;5:329-34.