23
Moving Forward with eHealth in the Waterloo Wellington LHIN The HEALTHeCONNECTIONS Project 9 th Annual eHealth Summit June 10-12, 2009 Dr. Glenn Holder CIO, WWLHIN
Moving Forward with eHealth in theWaterloo Wellington LHIN
The HEALTHeCONNECTIONS Project
9th Annual eHealth SummitJune 10-12, 2009
Dr. Glenn HolderCIO, WWLHIN
2
3
4
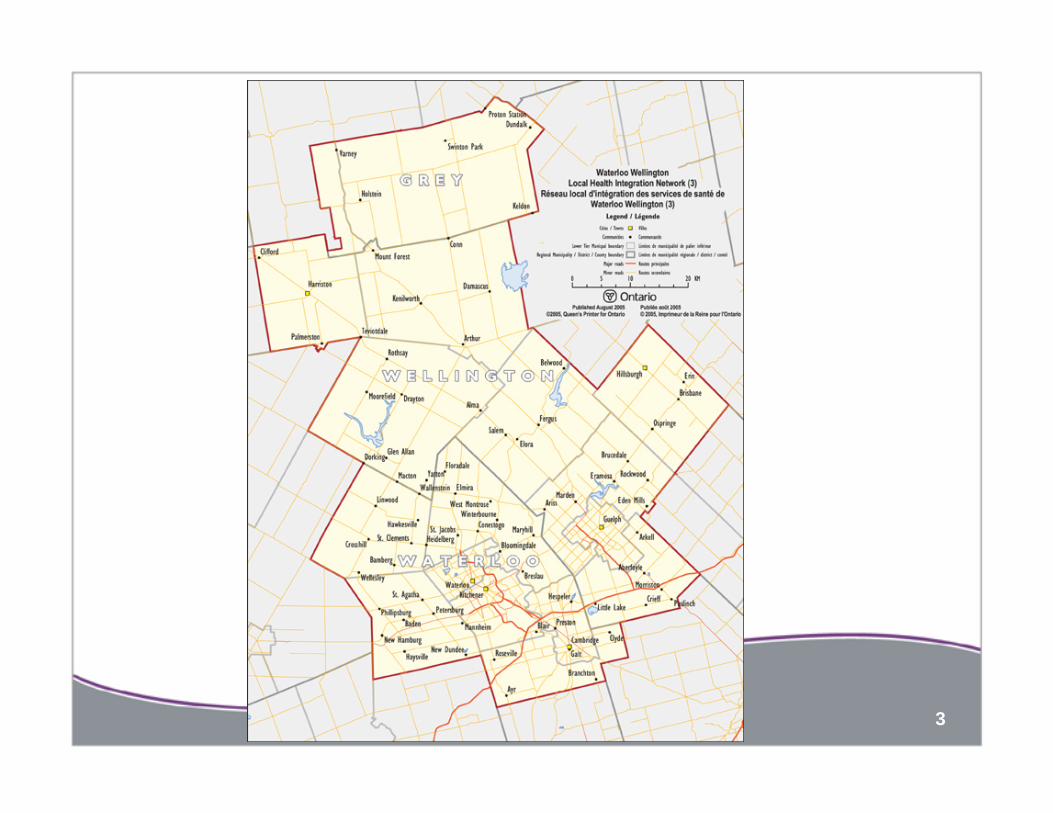
Waterloo Wellington LHIN• Population: 750,000 (rural and urban centres)• Geography: 4800 sq km (Waterloo Region, Wellington County,
South Grey)
• 10 hospital sites (8 hospital corporations)• 1 community care access centre• 30 community support services• 21 community mental health and addictions services• 35 long term care homes• 4 community health centres (with 3 satellites)
• 9 family health teams • 3 public health units• 956 physicians• Numerous other non-transfer-payment local providers
5

6
Introduction• HEALTHeCONNECTIONS Project
• a demonstration project supported through Canada Health Infoway’s Patient Access to Quality Care (PAQC) Program and by eHealth Ontario
• using individual-empowering eHealth elements to create new and innovative care delivery models
• an initial focus on chronic disease prevention and management (diabetes)
• is currently in implementation phase
• Presentation Overview• Challenge• Unique attributes of WWLHIN • Guiding principles• Approach and anticipated outcomes
7
Challenge
• Healthcare has tended to be provider- and organization-focused• Minimal integration of information or services
• Healthcare must become individual-centered and consumer-driven. • Enabling eHealth services are prerequisite
8
WWLHIN provides a unique opportunity for addressing this challenge
• Moderate size and complexity
• Community-based alternative health service delivery models
• Implementation and standardization of clinical systems
• Demonstrated commitment
• High-tech communities with very high IT literacy
• World class academic institutions
9
HEALTHeCONNECTIONS Guiding Principles
• eHealth solutions/services + individual-centered healthcare delivery models
• Flexibility to respond to local and regional priorities
• Communities must collaborate• Focus on cultural and clinical change• Build on the relationship between primary care
providers and individuals • Manageable scope
10
HEALTHeCONNECTIONS Approach
• Care networks• eHealth enabled, individual-centred diabetes
care model• Personal Health Record/Portal (PHRP) with
CDM tools• Clinical portal• Benefits Evaluation (BE) program
11
Project Scope
• 1,600 diabetes patients using the PHRP/CDM
• Up to 37,500 patients using the PHRP
• 9 family health teams – 150 physicians + 100 allied providers
• 5 diabetes education centres
• 25 diabetes related specialists
• 6 acute care hospitals/emergs.

12
Solution Overview
Primary CareEMRs
Monitoring Device(e.g. , )
FHTCare Network
Individuals &Informal Care Providers
PHRP/CDM tools
Primary CareEMRs
Clinical Portal
Community CareCase Mngmt
Acute CareEMRs
mydoctor.ca
PracticeSolutions
ClinicalConnect(MedSeek)
Red=HEALTHeCONNECTIONSDeliverable
13
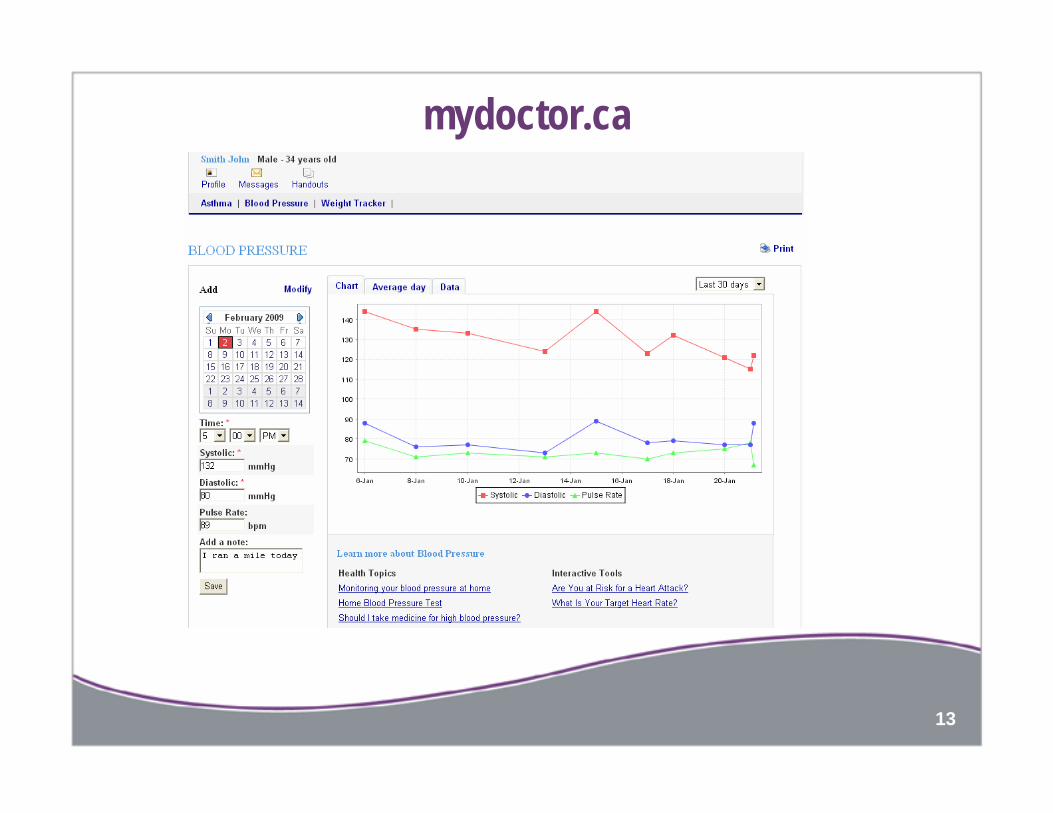
mydoctor.ca
14
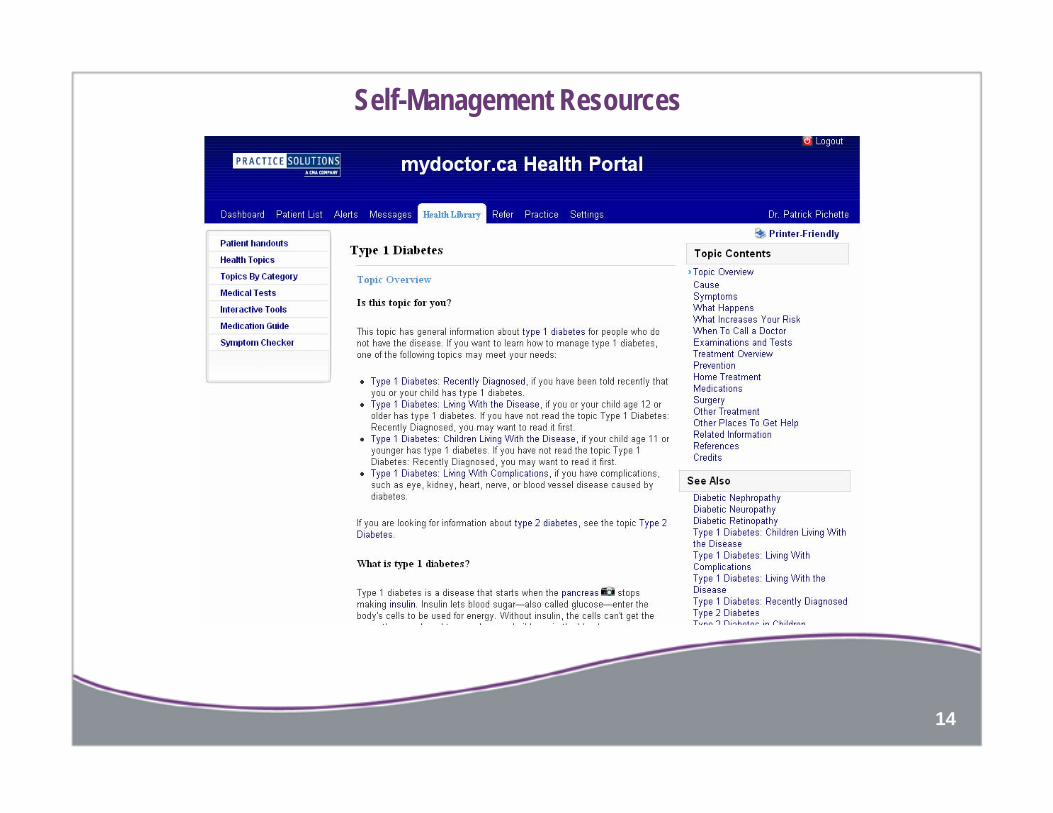
Self-Management Resources
15
Clinical Transformation – Roles of stakeholders
• Care networks
• Primary care
• Diabetes education centres
• Specialists
• Individuals
• Others
*All of the above will participate in the benefits evaluation
16
Partner Funding Program
• Offset the one-time costs of healthcare provider participation • Clinical transformation • Patient education and enrolment, • Establishing electronic information sharing
mechanisms and processes• Benefits evaluation program
• Outcome based• Enrolment targets• Retention targets
17
Benefits Evaluation
• Expected benefits• Quality• Access• Productivity
• Indicators and metrics
18
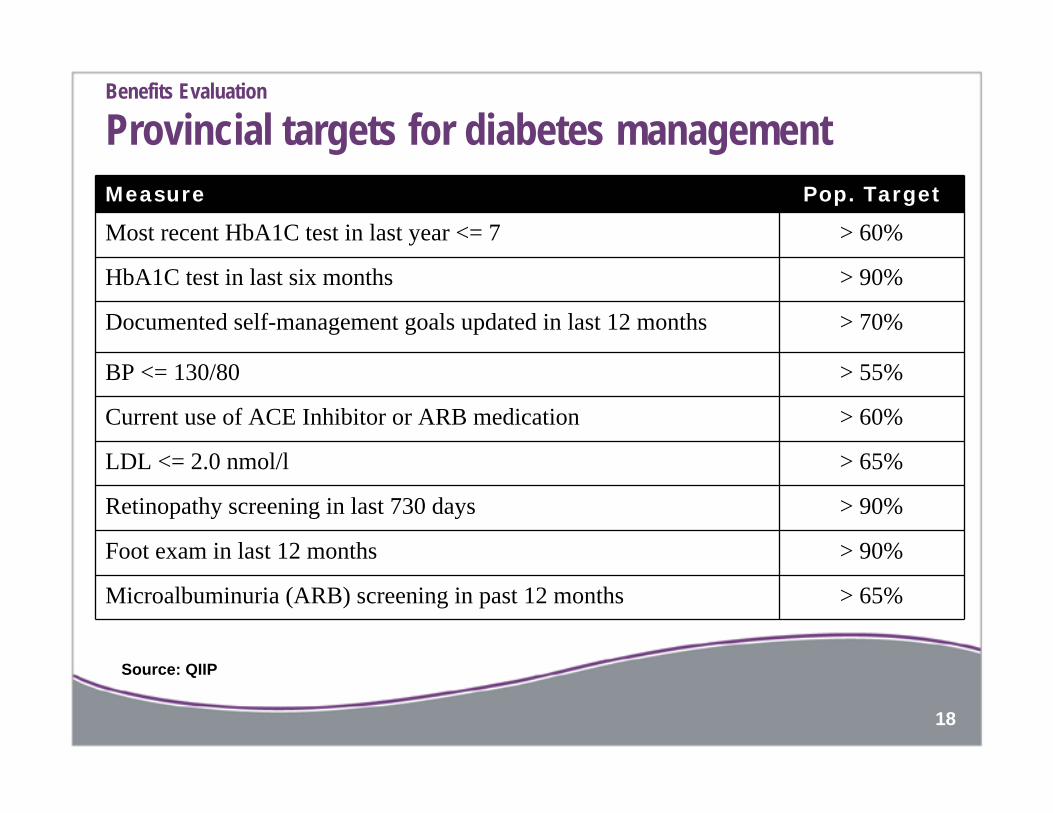
Benefits Evaluation
Provincial targets for diabetes managementMeasure Pop. Target
Most recent HbA1C test in last year <= 7 > 60%
HbA1C test in last six months > 90%
Documented self-management goals updated in last 12 months > 70%
BP <= 130/80 > 55%
Current use of ACE Inhibitor or ARB medication > 60%
LDL <= 2.0 nmol/l > 65%
Retinopathy screening in last 730 days > 90%
Foot exam in last 12 months > 90%
Microalbuminuria (ARB) screening in past 12 months > 65%
Source: QIIP
19
Timing
• Implementation of eHealth-enabled, individual-centered care delivery model for diabetes management by Fall 2009
• Benefits evaluation through to Summer 2010

20
Strategic Alignment
• Ontario and WWLHIN strategic healthcare priorities
• Ontario and WWLHIN e-Health strategy, architecture, standards and implementation
• CHI Patient Access to Quality Care (PAQC) Program
21
Looking Forward
• Applying the model beyond diabetes management
• New classes of eHealth services
• Options for an open, standards-based PHRP platform
• An ecosystem for innovation in consumer eHealth services with WWLHIN as a living laboratory
22
Acknowledgements
23

















