25
Moving towards the goal of Universal Health Coverage (UHC) in Bangladesh Md. Ashadul Islam Director General Health Economics Unit Ministry of Health and Family Welfare
| Date post: | 23-Dec-2015 |
| Category: |
Documents |
| Upload: | elvin-bryant |
| View: | 214 times |
| Download: | 0 times |
Moving towards the goal of Universal Health Coverage (UHC) in Bangladesh
Md. Ashadul IslamDirector GeneralHealth Economics UnitMinistry of Health and Family Welfare

Health Sector of BangladeshA Story of Achievements ❶Bangladesh over the years have
achieved remarkable progress
❷Through the government agenda the country has been on track with the health MDGs
❸The country has the highest EPI coverage (82%) amongst neighboring countries
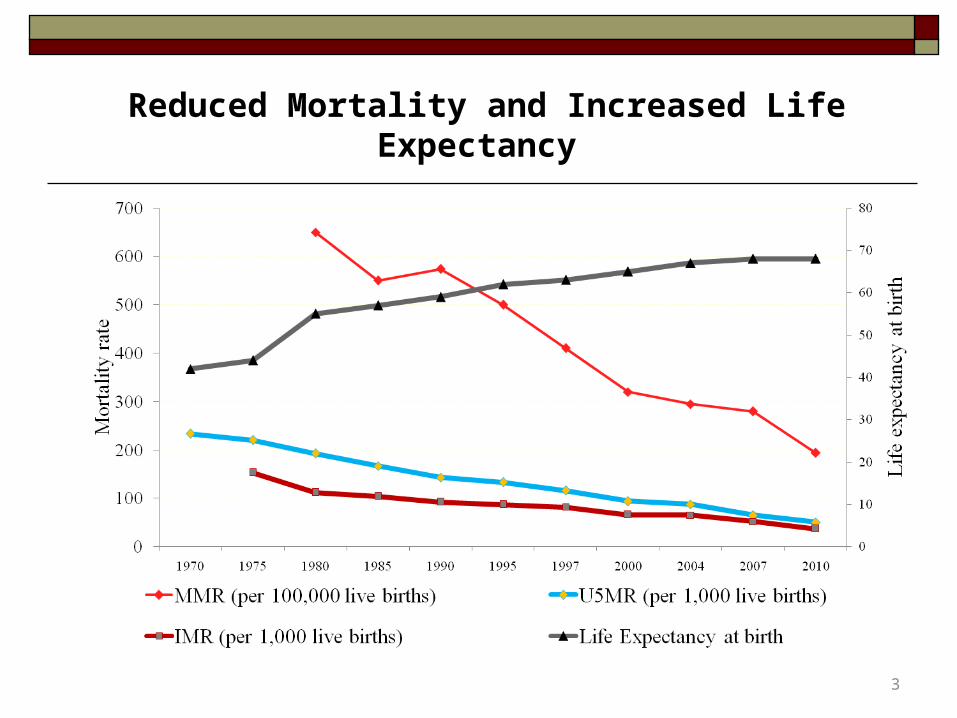
Reduced Mortality and Increased Life Expectancy
3
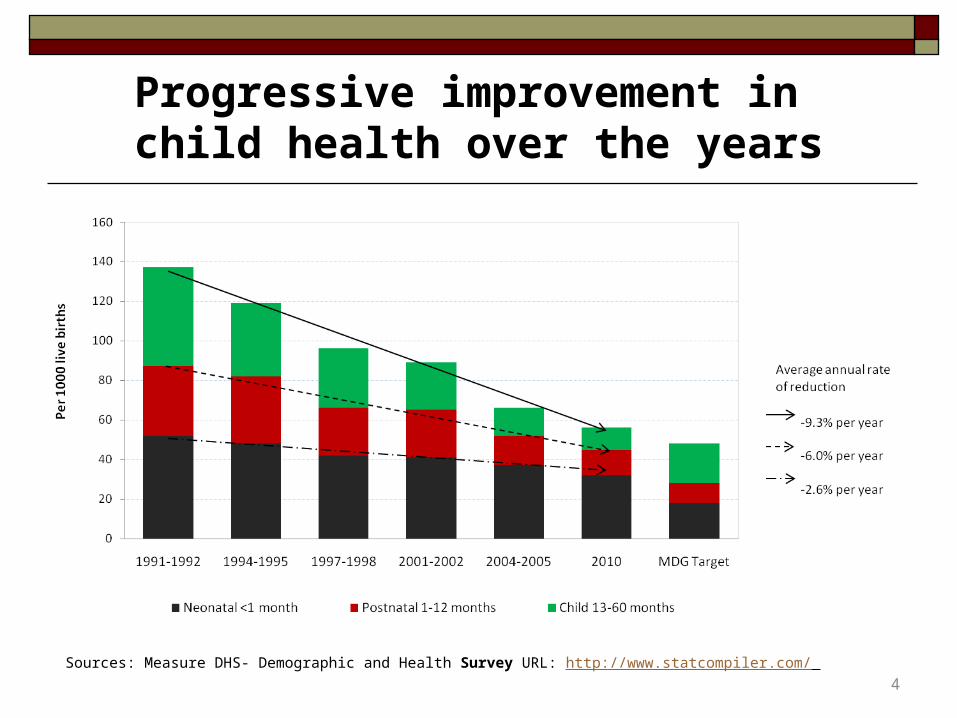
Progressive improvement in child health over the years
Sources: Measure DHS- Demographic and Health Survey URL: http://www.statcompiler.com/
4

Reduced Fertility Rate andincreased Contraceptive Prevalence Rate
5
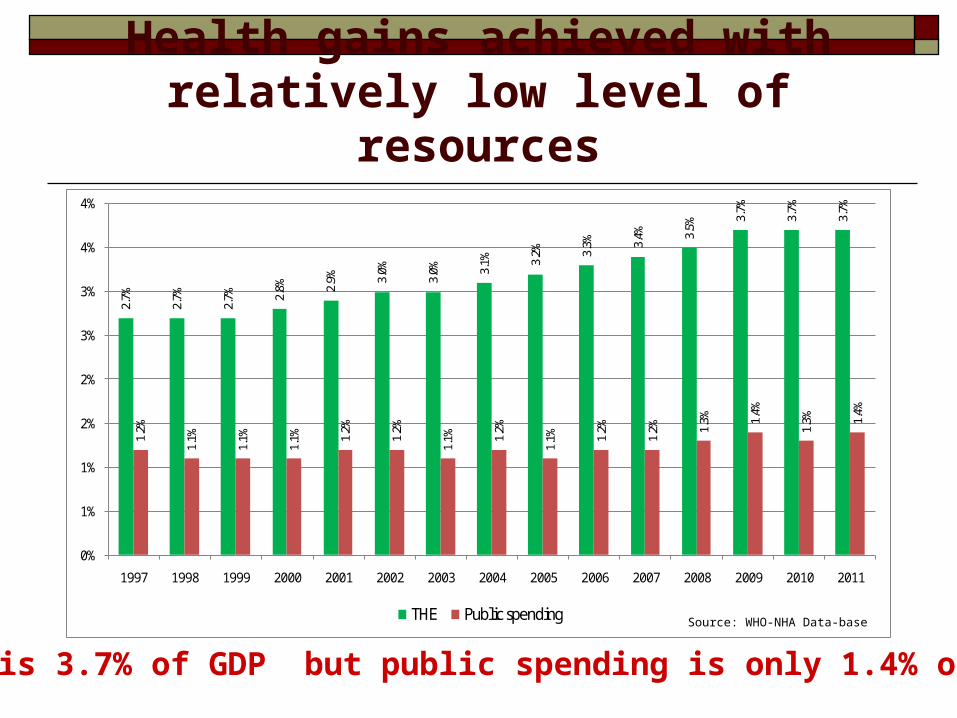
Health gains achieved with relatively low level of resources
2.7%
2.7%
2.7% 2.
8% 2.9% 3.
0%
3.0% 3.
1% 3.2% 3.
3% 3.4% 3.
5%
3.7%
3.7%
3.7%
1.2%
1.1%
1.1%
1.1% 1.
2%
1.2%
1.1% 1.
2%
1.1% 1.
2%
1.2% 1.
3% 1.4%
1.3% 1.
4%
0%
1%
1%
2%
2%
3%
3%
4%
4%
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
THE Public spending Source: WHO-NHA Data-base
THE is 3.7% of GDP but public spending is only 1.4% of GDP

Health Care Financing Features
We have a HCF system as part of the national financial management system. Main Features
❶ Share in the national budget --- 4.27% (2013-14)1
❷ Public spending as % of GDP --- around 1.4%1
❸ Per capita Health expenditure---US$ 27 (2011)1 ❹ Out-of-pocket---64% of Total health expenditure(THE)2
❺ Coverage of insurance --- <1% of THE2
❻ Government is financer and provider of services❼ Budget norms follow civil service and budgetary regulations and codes.
7

Total Health Expenditureis increasing over time, it has increased from 48,000 million taka in 1996 to 300,000 million taka in 2011 (almost 6 times in 15 years)
0
50,000
100,000
150,000
200,000
250,000
300,000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Source: WHO-NHA Data-base
8
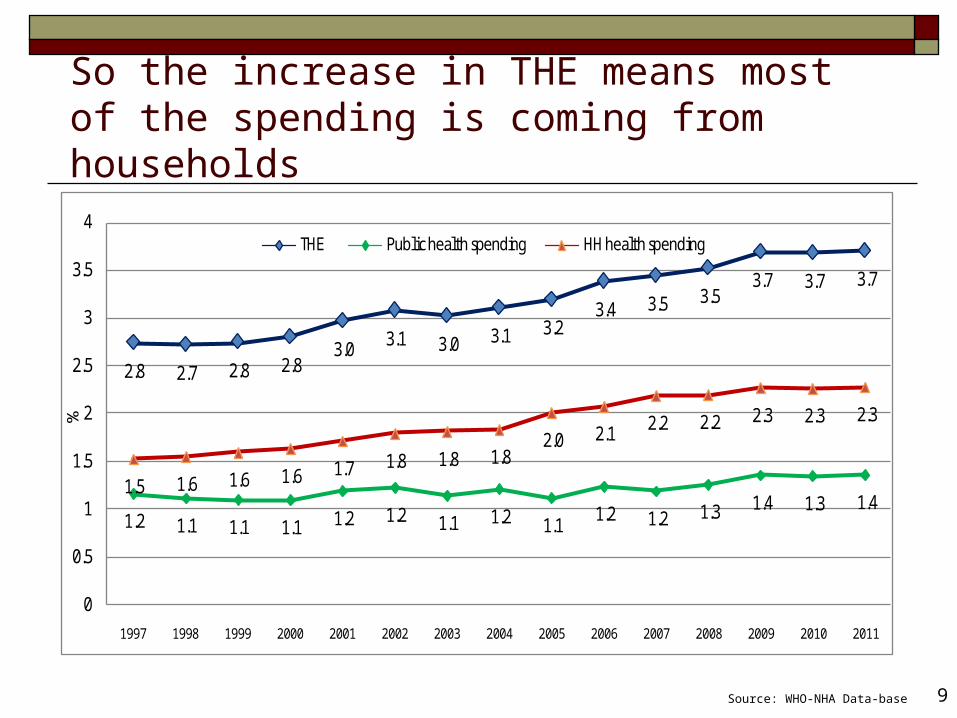
So the increase in THE means most of the spending is coming from households
2.8 2.7 2.8 2.83.0 3.1 3.0 3.1 3.2
3.4 3.5 3.53.7 3.7 3.7
1.2 1.1 1.1 1.1 1.2 1.2 1.1 1.2 1.1 1.2 1.2 1.3 1.4 1.3 1.41.5 1.6 1.6 1.6 1.7 1.8 1.8 1.8
2.0 2.1 2.2 2.2 2.3 2.3 2.3
0
0.5
1
1.5
2
2.5
3
3.5
4
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
%
THE Public health spending HH health spending
Source: WHO-NHA Data-base 9

Health Financing in Bangladesh(2006-2007)
Public SectorTk. 41,318; 26%
Rest of the WorldTk. 12,391; 08%
NGOsTk. 2,092; 0.1%
Household OOPTk. 103,459; 64%
Private FirmsTk. 1,325, 0.8%
Private InsuranceTk. 314; 0.2%
Million TakaTaka 69 = 1 US $
Source: BNHA 1997-2007

Comparison of health expenditure - 2011
Country
Per capita total health spending
(US $)
THE as % of GDP
Public HE as % of GDP
Per capita govt
spending (US $)
Bangladesh 27 3.7 1.4 9.7
India 59 3.9 1.2 18.3
Nepal 33 5.4 2.1 13.0
Pakistan 30 2.5 0.7 8.0
Sri Lanka 97 3.4 1.5 43.1
Indonesia 95 2.7 0.94 33
Vietnam 96 6.9 2.7 38
Source: WHO-NHA Data-base
11

% increase in National and Health Budget - a comparison

Challenges in Bangladesh❶ Inadequate funding for the whole health system.
-Government budget is 1.4% of GDP, Total Health Expenditure (THE) is 3.7% of GDP.
❷ Inequity in financing and utilization-main source of financing for health care is out-of-pocket payment (64% of THE)
❸ Inefficient use of resources -due to absence of proper resource allocation formula, shortage of health workers, vacant posts (44%) in public health facilities, lack of provider autonomy, no purchaser-provider split, duplication of programs and insufficient coordination leading to wastage

Common concerns across the globe
❶ Increasing health care cost
❷ Protect people from financial consequences of health care
payment
❸ Expand fiscal space in spite of macro-economic constraints
❹ Use of available resources efficiently and equitably
For all these, Health care financing is moving towards
Universal Health Coverage (UHC)
14

What’s next?

Universal Health Coverage
16 |
Ensuring that all people can use the promotive, preventive, curative and rehabilitative health services they need, of sufficient quality to be effective, while also ensuring that the use of these services does not expose the user to financial hardship (WHO)
Moving towards the UHC Goal…
❶ UHC is a continuous journey
❷ No single model of universal coverage – successful programs vary and the starting point is the country context
❸ But relevant to all (rich and poor) countries, because all want to
Reduce the gap between need and utilization Improve quality Improve financial protection
Source: Kutzin, J. (WHO) Presentation Kenya June 2013

Bangladesh Steps toward UHC… ❶ Renewed Commitment through Health Policy 2011
❷ Revitalized and established nearly 13000 community clinics and improved hospital services
❸ Increased health manpower for hospitals and health centres to provide health care services
❹ Increased efficiencies in procurement, distribution and utilization of essential medicines and equipment
❺ Expanded demand side financing for ante-natal care and deliveries attended by skilled birth attendants
❻ Adoption of the HEALTH CARE FINANCING STRATEGY
What needs to be done?

20
Bangladesh and UHC
WIDTH Population covered• Rapid expansion of health protection fund especially among the poor
HIGHT Cost covered• Zero co-payment schemes for the poor
DEPTH Services covered• Comprehensive Inpatient & Outpatient• Catastrophic benefit packages
Adoption of Health Care Financing Strategy (HCFS)
More FundsEquity
Efficiency
3
• Decrease by half the share of household out of pocket payments to total health expenditure
• Expand pre-payments for health care from tax revenues, social health insurance premiums and other pre-payment modalities

Who will benefit from UHC?

What is planned to attain “UHC”?
23
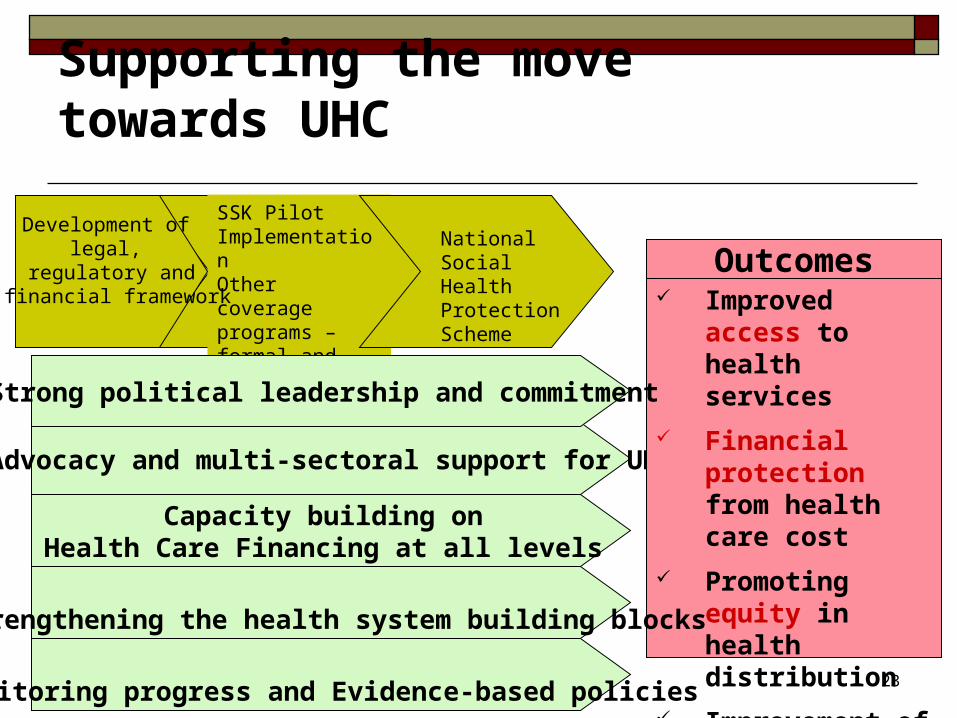
SSK Pilot ImplementationOther coverage programs – formal and informal sector
National Social Health Protection Scheme
Advocacy and multi-sectoral support for UHC
Outcomes Improved access to
health services
Financial protection from health care cost
Promoting equity in health distribution
Improvement of quality of care
Development of legal,
regulatory and financial framework
Capacity building on Health Care Financing at all levels
Supporting the move towards UHC
Strong political leadership and commitment
Strengthening the health system building blocks
Monitoring progress and Evidence-based policies

Role of Health Economics Unit
Evidence Based Policy Development
Coordination and Steering
HCFS Implementation
UHC monitoringNational Health Accounts
Legal Framework Development
Equity, Efficiency, Economy, EffectivenessEquity, Efficiency, Economy, Effectiveness


















![Universal Health Coverage UHC in Global Health · Universal Health Coverage [ UHC ] in Global Health Ariel Pablos-Méndez, MD, MPH ... Voice and Accountability matters more ! UHC](https://static.documents.pub/doc/80x56/5f0f7c537e708231d4446621/universal-health-coverage-uhc-in-global-health-universal-health-coverage-uhc-.jpg)