64
1 MRCP 2- SLIDES Dermatomyositis. Systemic sclerosis/CREST (the skin of the digits is clearly thickened and tight-sclerodactyly).

1
MRCP 2- SLIDES
Dermatomyositis.
Systemic sclerosis/CREST (the skin of the digits is clearly thickened and tight-sclerodactyly).

2
Jaccoud's arthropathy. The picture shows joint subluxations and swan neck deformities. Seen in: SLE;
rheumatic fever, Parkinson's disease; hypocomplementaemic urticarial vasculitis. The plain x-ray of this
man's hands does not show any evidence of bone erosion.
An acute attack of monoarticular arthritis. Typical of gout.

3
The slide shows the typical appearance of chronic tophaceous gout
Palmar xanthoma diagnostic of type III hyperlipidaemia.

4
Porphyria cutanea tarda (PCT) is associated with deficiency of hepatic uroporphyrinogen (URO)
decarboxylase. Cutaneous photosensitivity is the predominant clinical finding.
Subungual fibromas, characteristic of tuberose sclerosis. Fibromas may also develop within the CNS,
where they calcify. Other manifestations of tuberose sclerosis include Ash-leaf macules (discrete areas
of hypopigmentation; often present at birth), shagreen patch (rough patch of skin with a texture similar
to shark skin), adenoma sebaceum (angiofibromas of the face).

5
Erythema nodosum.

6
Purpuric rash of meningiococcal septicaemia.
Typical appearance of cutaneous anthrax, caused by Bacillus anthracis.

7
Necrobiosis lipoidica diabeticorum.
8
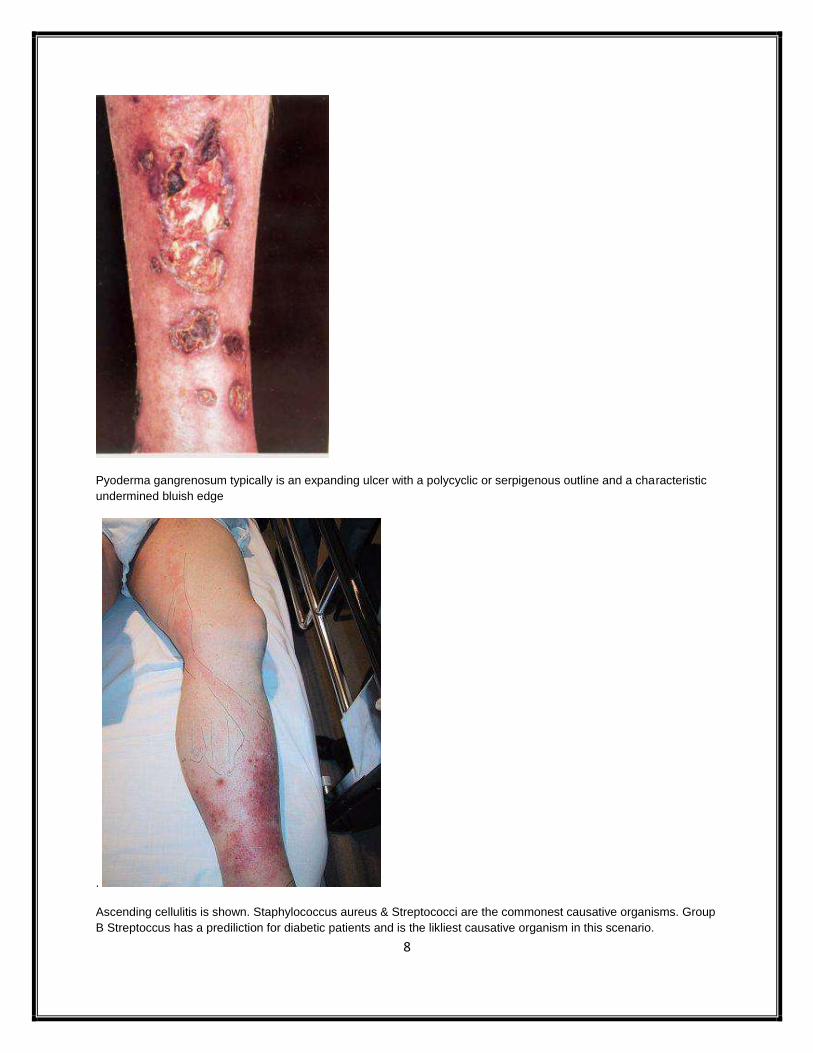
Pyoderma gangrenosum typically is an expanding ulcer with a polycyclic or serpigenous outline and a characteristic
undermined bluish edge
.
Ascending cellulitis is shown. Staphylococcus aureus & Streptococci are the commonest causative organisms. Group
B Streptoccus has a prediliction for diabetic patients and is the likliest causative organism in this scenario.

9
Erythema ab igne (due to sitting too close to a fire). It frequently occurs on the front of the shins or lower back, the
latter is especially associated with the use of a hot water bottle. In this patient’s case the confusion and coldness with
erythema ab igne suggest a diagnosis of hypothyroidism.
This is pre-tibial myxoedema with slightly raised, pinkish, indurated patches usually on the fronts of the shins or
dorsum of the foot and often associated with acropachy.

10
Typical appearance of Pagetic tibiae is shown, with characteristic bowing.
Relapsing polychondritis. The picture of his ear shows auricular chondritis, inflammation of the auricle with sparing of
the earlobe. This is a characteristic finding of RP, because only the cartilaginous portion of the ear is affected,
separating it from cellulitis/infection.

11
Chicken pox (residue of calamine lotion).

12
Typical telangiectasia of hereditary haemorrhagic telangiectasia (aka Osler-Weber-Rendu syndrome).
Typical appearance of Hereditary Haemorrhagic Telangiectasia.

13
Systemic sclerosis. facial telangiectasia, small mouth, beaking of the nose.
Addison's disease as reflected by the pigmented appearance. (RT: buccal mucosa)
14
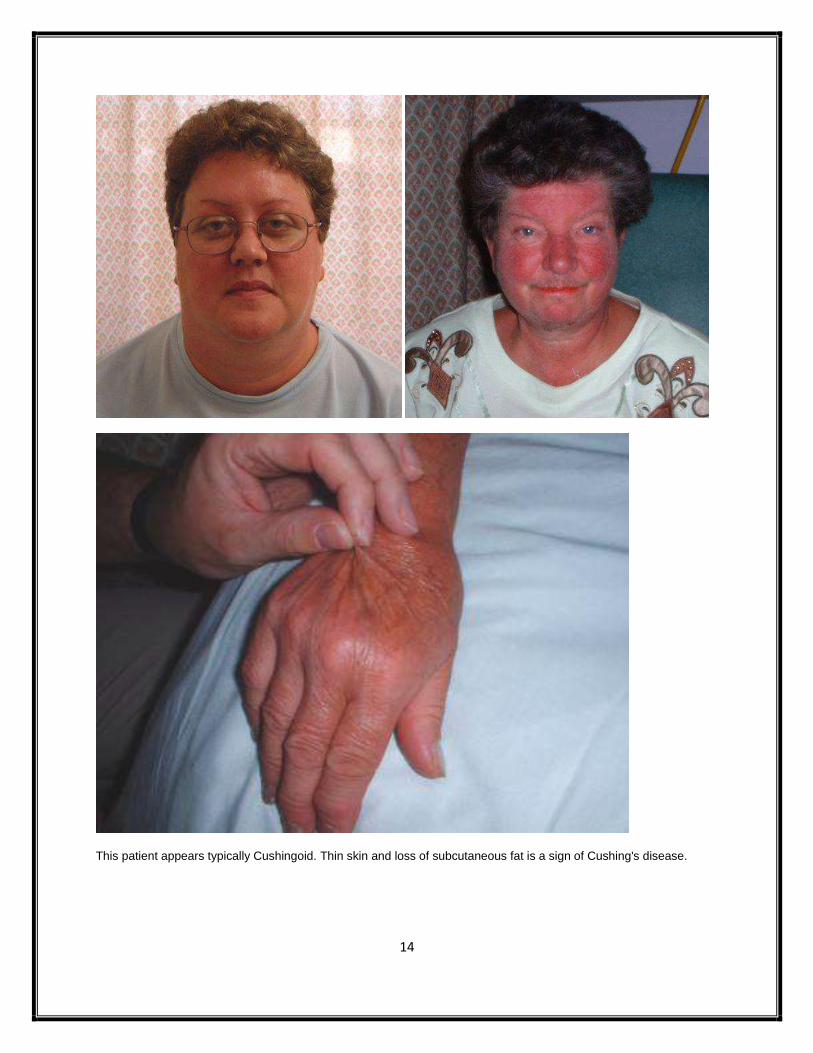
This patient appears typically Cushingoid. Thin skin and loss of subcutaneous fat is a sign of Cushing's disease.

15
Post-pituitary resection, GH deficiency.(Hypopit)
This patient has a fixed facial flush and symptoms suggestive of Carcinoid syndrome.

16
An appearance suggestive of hypothyroidism. The most likely cause of this would be Hashimoto’s thyroiditis with
microsomal antibodies (aka Antithyroid peroxidase antibodies) expected.
Secondary hyperthyroidism with elevated TSH, T3 and T4. MRI headscan may be expected to demonstrate a
pituitary macroadenoma.

17
This patient appears acromegalic.
Myotonic dystrophy. Features include frontal baldness in men, atrophy of temporalis, masseters and facial muscle.

18
The slide shows gynaecomastia; the history (tall stature and small testes) suggests Klinefelter's syndrome.
19
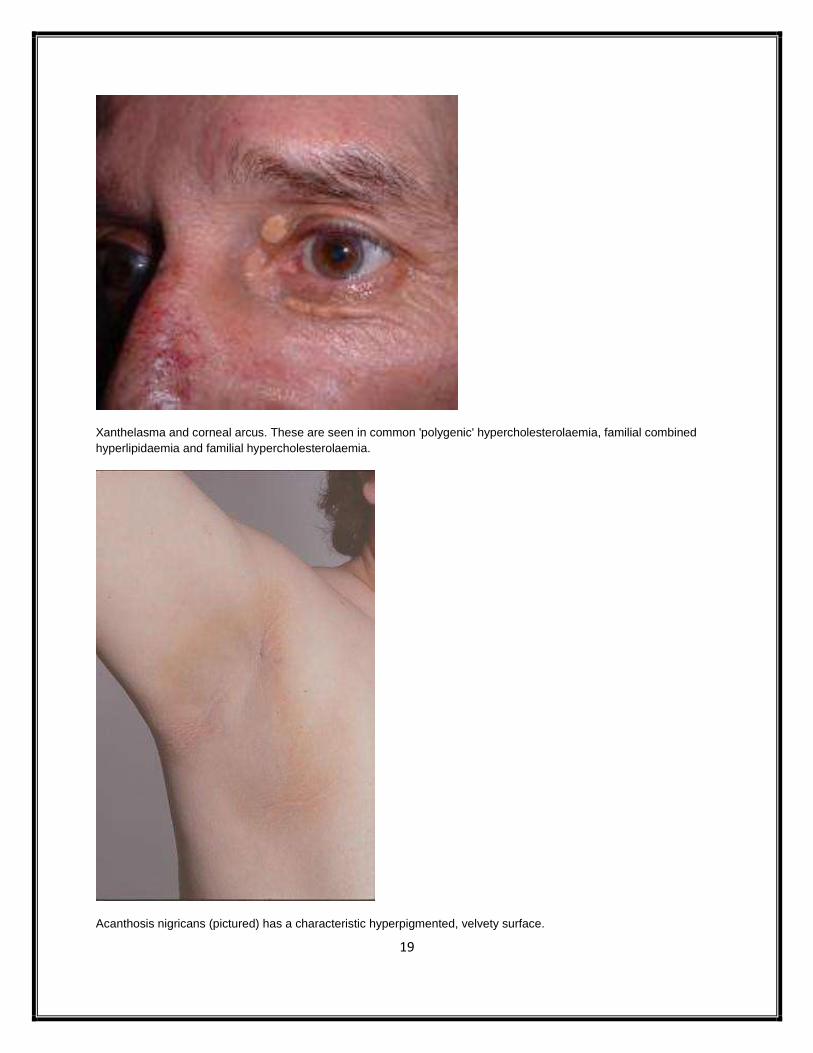
Xanthelasma and corneal arcus. These are seen in common 'polygenic' hypercholesterolaemia, familial combined
hyperlipidaemia and familial hypercholesterolaemia.
Acanthosis nigricans (pictured) has a characteristic hyperpigmented, velvety surface.

20
Typical 'plucked chicken skin' appearance of pseudoxanthoma elasticum.
Plucked chicken skin’ appearance to skin folds in the neck (pseudoxanthoma elasticum).

21
Ehlers-Danlos syndrome (EDS). Cigarette-paper (papyraceous) scarring of the skin.
Typical VZV (shingles).

22
Erysipelas is a Streptococcus pyogenes infection of the deep dermis and subcutis.
Cutaneous tuberculosis (lupus vulgaris).
23
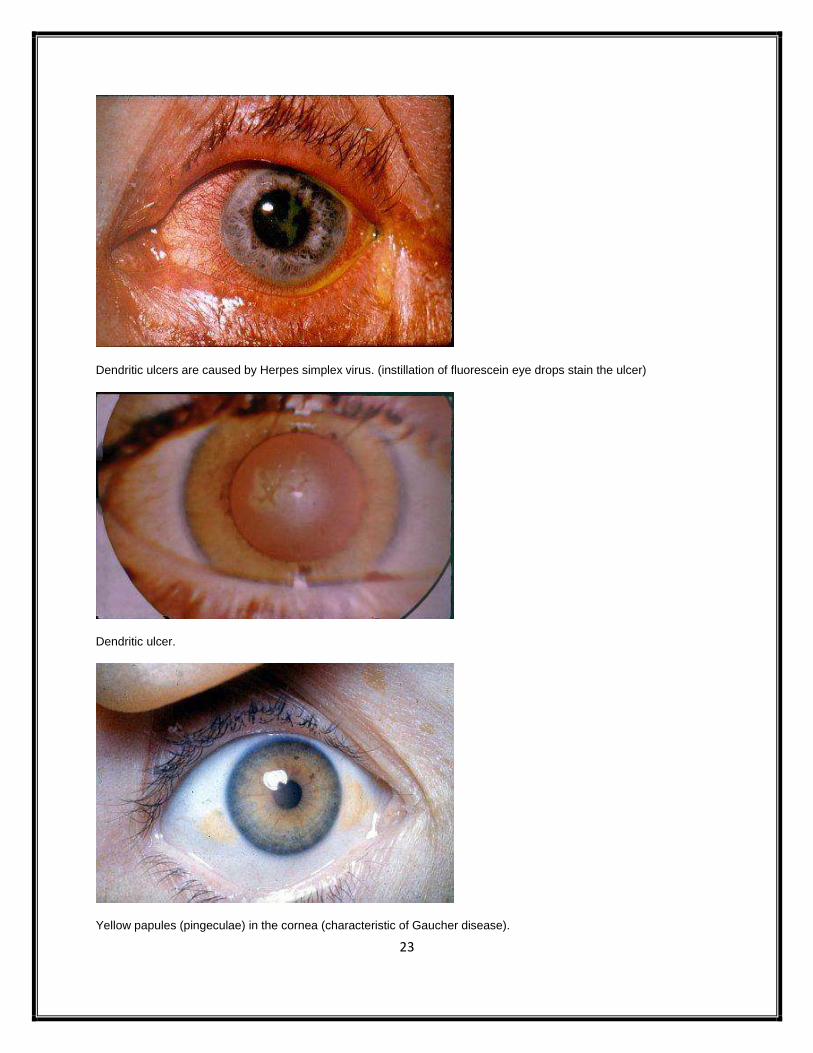
Dendritic ulcers are caused by Herpes simplex virus. (instillation of fluorescein eye drops stain the ulcer)
Dendritic ulcer.
Yellow papules (pingeculae) in the cornea (characteristic of Gaucher disease).

24
Pituitary apoplexy with affection of the 3rd
cranial nerve.
Damage to the oculomotor nerve during its course results in ipsilateral ptosis; at rest, the globe is diverted
downwards and laterally. The eye cannot be moved medially, superiorly or inferiorly.
Characteristic features of severe Grave's eye disease – termed 'malignant exophthalmos' in this case – proptosis,
chemosis, palpebral oedema and periorbital swelling. (induced by radio-iodine).

25
Subconjunctival haemorrhage which is an alarming adverse effect of aspirin therapy (and other antiplatelets).
Hyphaema, blood in the anterior chamber. Usually caused by trauma – often small objects (champagne corks,
squash balls) hitting the eye.
Typical papules (with central umbilcation) associated with molluscum contagiosum. The condition is caused by
infection with a pox virus and is seen in advanced HIV disease and AIDS.
26
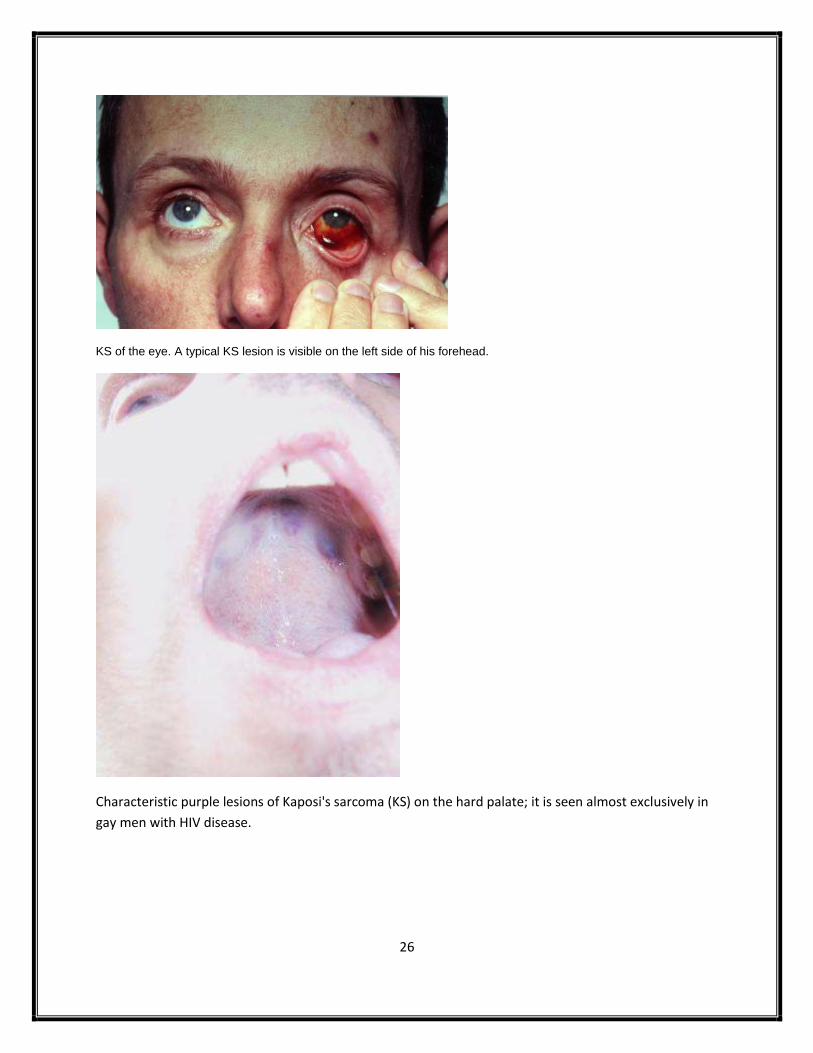
KS of the eye. A typical KS lesion is visible on the left side of his forehead.
Characteristic purple lesions of Kaposi's sarcoma (KS) on the hard palate; it is seen almost exclusively in
gay men with HIV disease.
27
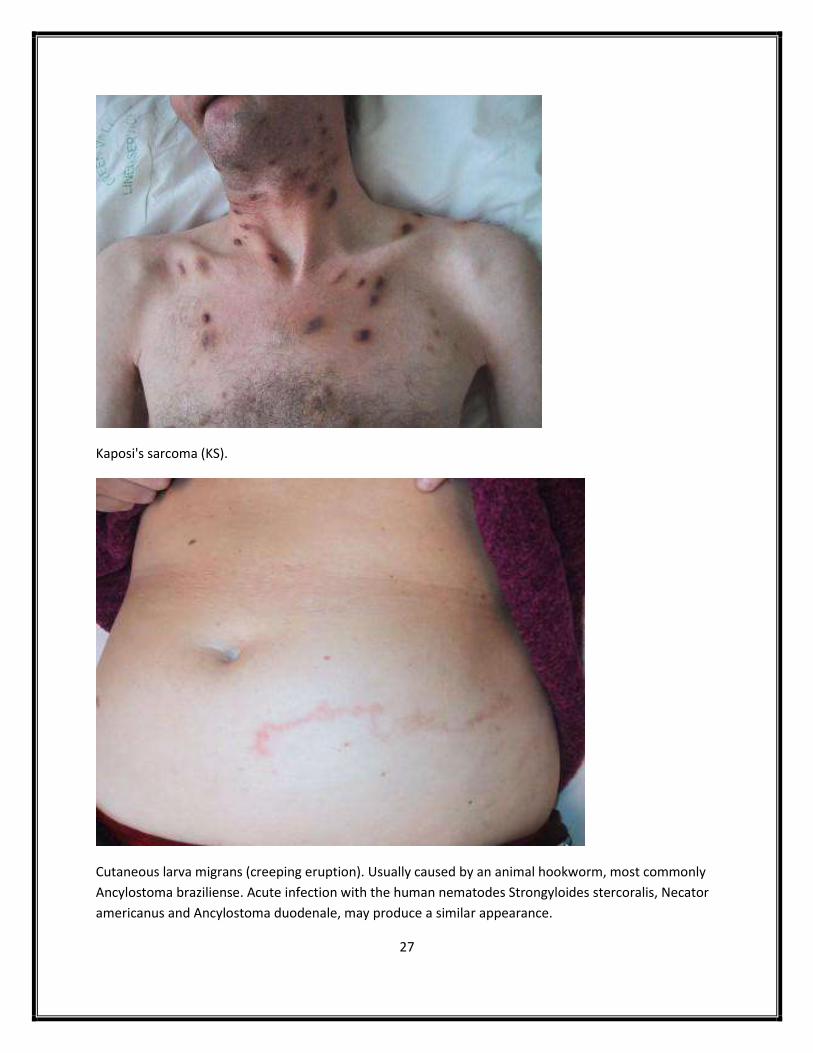
Kaposi's sarcoma (KS).
Cutaneous larva migrans (creeping eruption). Usually caused by an animal hookworm, most commonly
Ancylostoma braziliense. Acute infection with the human nematodes Strongyloides stercoralis, Necator
americanus and Ancylostoma duodenale, may produce a similar appearance.

28
Guttate psoriasis following Streptococcal tonsillitis.
Oral ulceration (Behcet’s).

29
Erythema multiforme. Herpes simplex virus infection is the commonest cause. Other common causes
include infection with mycoplasma and streptococci; EM may also be idiopathic, drug-induced
(sulfonamides, sulphonylurea, barbiturates), or occur in systemic diseases (SLE, inflammatory bowel
disease, malignancy).
Typical target lesions of erythema multiforme. (Erythematous papules surrounded by a raised,
erythematous ring, which is in turn encircled by an erythematous outer ring. The lesions are generally
located on the extremities).

30
Pityriasis rosea.
Typical lesions of eruptive xanthomata are shown: raised lesions, typically occurring on extensor
surfaces. Eruptive xanthomata occur in hyperlipidaemic states associated with hypertriglyceridaemia.
Well-recognised associations of hypertriglyceridaemia include acute pancreatitis and lipaemia retinalis.

31
Mycosis fungoides, a cutaneous T-cell lymphoma.
'Ferning' or 'arborescent' rash pathognomonic of a lightning strike. Also known as Lichtenberg figures.

32
Abscess in the right mid-zone.
Lateral chest x-ray with an abscess cavity (with fluid level) in the right mid zone.

33
Aspiration pneumonia.
Lobar consolidation (Legionella pneumonia).
34
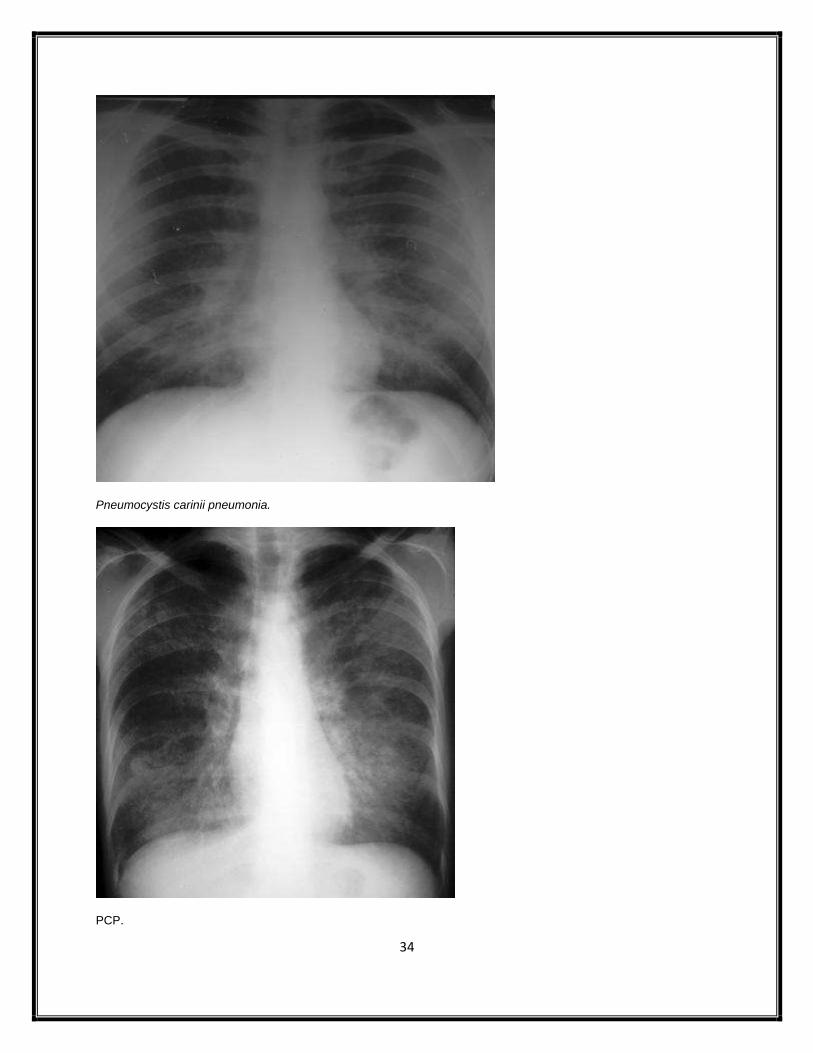
Pneumocystis carinii pneumonia.
PCP.

35
Left upper lobar consolidation (Pancoast’s tumour).
Rt apical pneumothorax.

36
Large left sided pneumothorax with midline shift (tension pneumothorax).
Bilateral reticulonodular shadowing and bilateral hilar lymphadenopathy (sarcoidosis).

37
The chest x-ray shows a large heart shadow and venous diversion to upper lobes. (severe chronic AR)
Extensive pleural plaques from previous exposure to asbestos.

38
Typical x-ray appearance of Paget's disease of the tibia.
Calcaneal spur. This is associated with a plantar fasciitis and can occur in conditions such as ankylosing spondylitis
and Reiter's disease. It is also associated with Gout.

39
Acute gout. There are well defined punched-out juxta-articular erosions related to both sides of the 1st metatarsal
bone. Classical site for gout. with sclerotic margins and overhanging edges, sometimes termed rat bite erosions.
Rheumatoid arthritis. The characteristic feature are periarticular erosions. Juxtaarticular osteopaenia occurs early on
in inflammatory joint disease.

40
Calcification in the area of the pancreas which would support a diagnosis of diarrhoea secondary to chronic
pancreatitis with pancreatic insufficiency.
Barium follow through reveals narrowing of loops of small bowel and a stricture of the terminal ileum, suggesting a
diagnosis of Crohn's disease. Although it is possible to have such appearances with peritoneal TB.
41
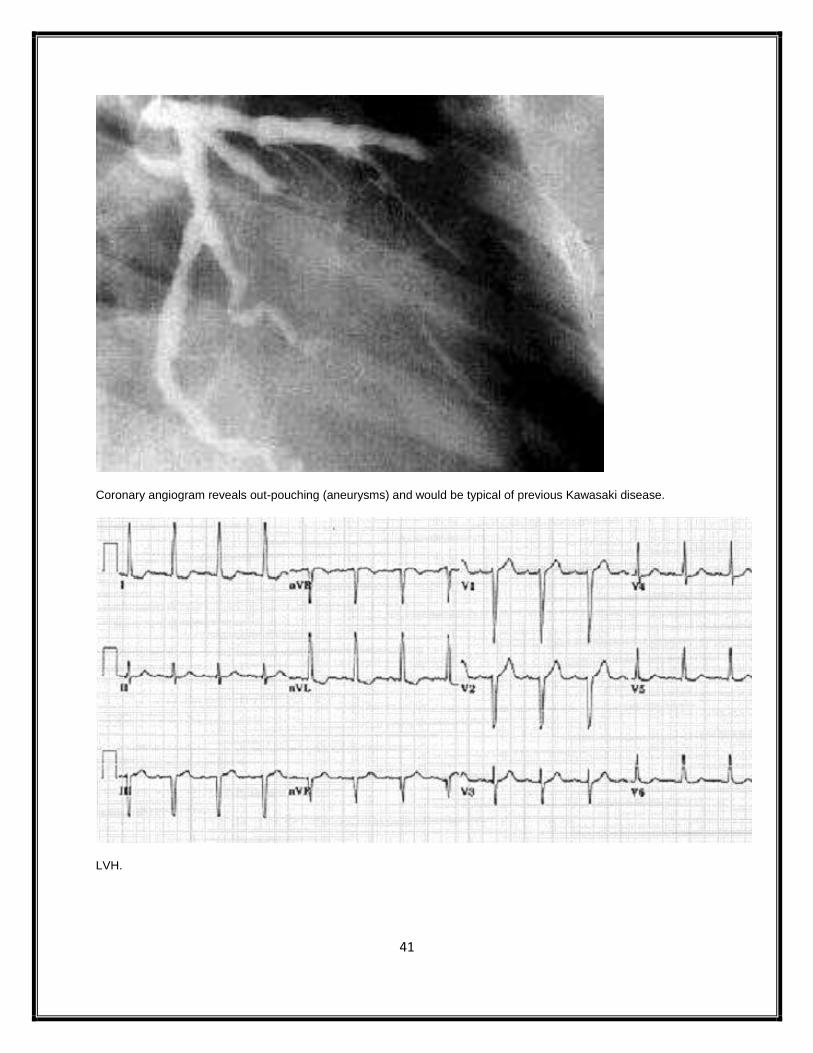
Coronary angiogram reveals out-pouching (aneurysms) and would be typical of previous Kawasaki disease.
LVH.

42
Long QT interval and Torsade-de-pointes ventricular tachycardia.
Prominant R wave in lead V1 and ST depression in V1 - V3. There is also ST elevation in leads V5 and V6. The
clinical history, age and ECG all suggest an acute myocardial infarction - in this case a postero-lateral MI. The most
appropriate management is thrombolysis.
43
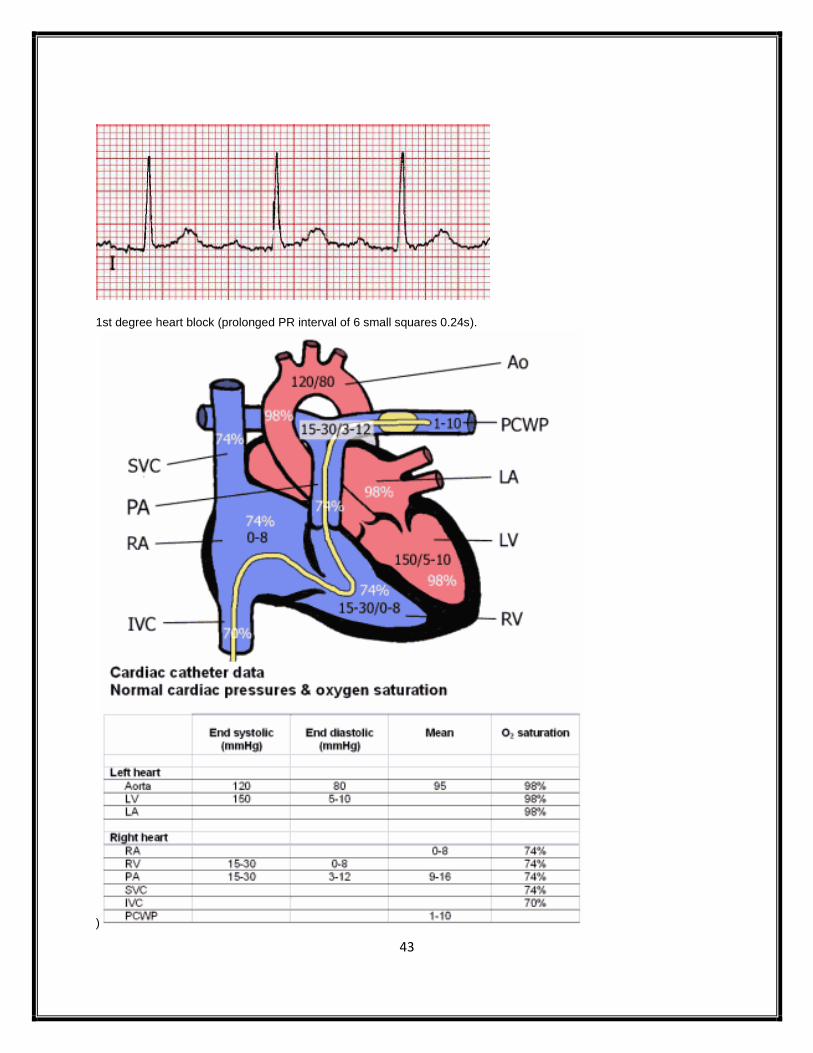
1st degree heart block (prolonged PR interval of 6 small squares 0.24s).
)

44
Non-caseating granulomata (berylliosis).
Non-caseating granulomata (sarcoidosis).

45
Rectal biopsy material which shows numerous macrophages filled with brown pigment within the
lamina propria (Melanosis coli). The discolouration is caused by deposits of lipofuscin.
Liver biopsy showing Porphyria cutanea tarda.

46
Actinomycosis .
Howell-Jolly bodies. These are spherical bluish inclusions within erythrocytes and are nuclear fragments
of condensed DNA which are normally removed by the spleen. They are seen in severe haemolytic
anaemias or in dysfunctional/asplenic patients.

47
The blood film shows variation in erythrocyte size (anisocytosis) and shape (poikilocytosis). Howell-Jolly
bodies are seen, which are intracellular inclusion bodies consisting of remnants of DNA. (hyposplenism)
Target cells which are typically found in hyposplenism.
48
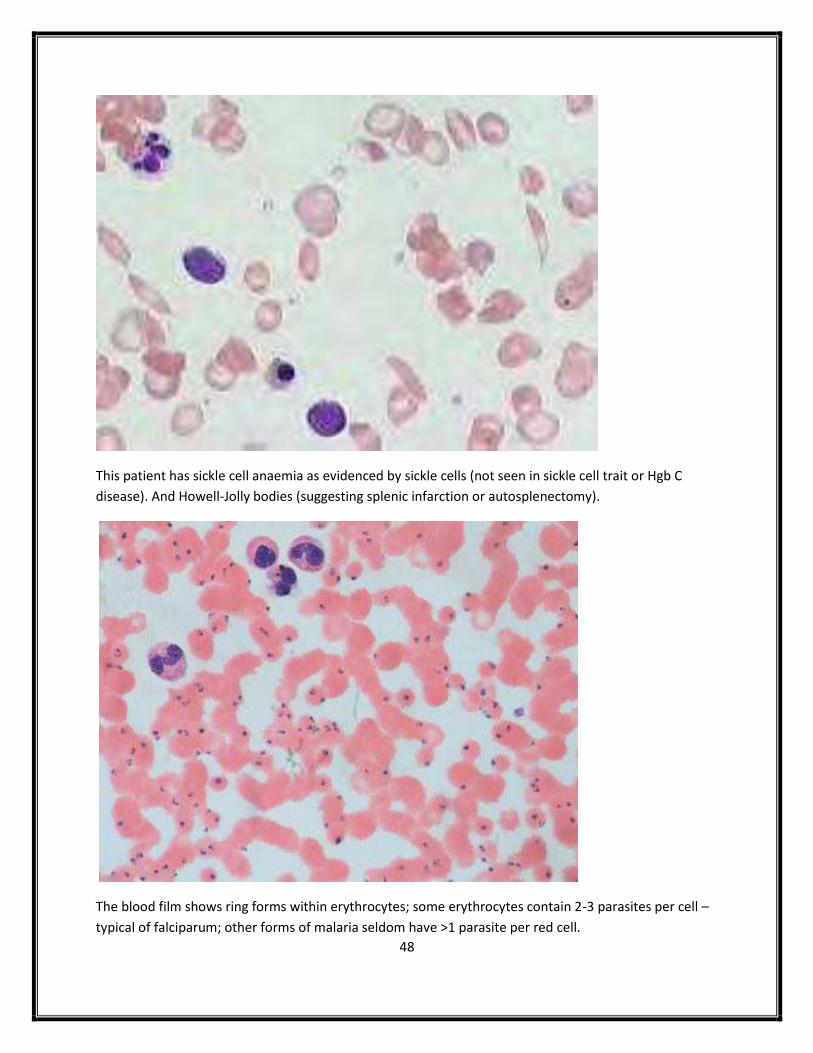
This patient has sickle cell anaemia as evidenced by sickle cells (not seen in sickle cell trait or Hgb C
disease). And Howell-Jolly bodies (suggesting splenic infarction or autosplenectomy).
The blood film shows ring forms within erythrocytes; some erythrocytes contain 2-3 parasites per cell –
typical of falciparum; other forms of malaria seldom have >1 parasite per red cell.
49
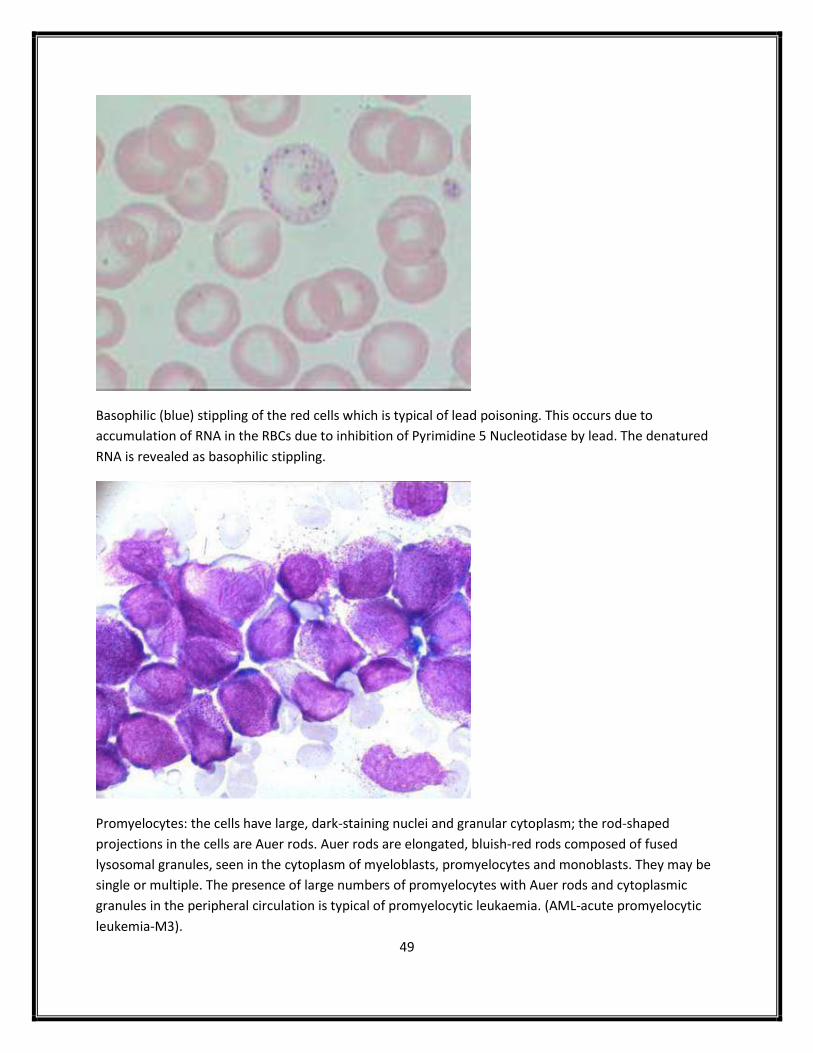
Basophilic (blue) stippling of the red cells which is typical of lead poisoning. This occurs due to
accumulation of RNA in the RBCs due to inhibition of Pyrimidine 5 Nucleotidase by lead. The denatured
RNA is revealed as basophilic stippling.
Promyelocytes: the cells have large, dark-staining nuclei and granular cytoplasm; the rod-shaped
projections in the cells are Auer rods. Auer rods are elongated, bluish-red rods composed of fused
lysosomal granules, seen in the cytoplasm of myeloblasts, promyelocytes and monoblasts. They may be
single or multiple. The presence of large numbers of promyelocytes with Auer rods and cytoplasmic
granules in the peripheral circulation is typical of promyelocytic leukaemia. (AML-acute promyelocytic
leukemia-M3).

50
Blood film shows red cell agglutination, suggesting the presence of cold agglutinin which is associated
with Iymphoma (antibodies against anti-i), Mycoplasma pneumonia (antibodies against anti-I), and
rarely infectious mononucleosis (antibodies against anti-i).
The Gram stain shows Gram positive cocci growing in clusters – typical of Staphylococcus aureus.
51
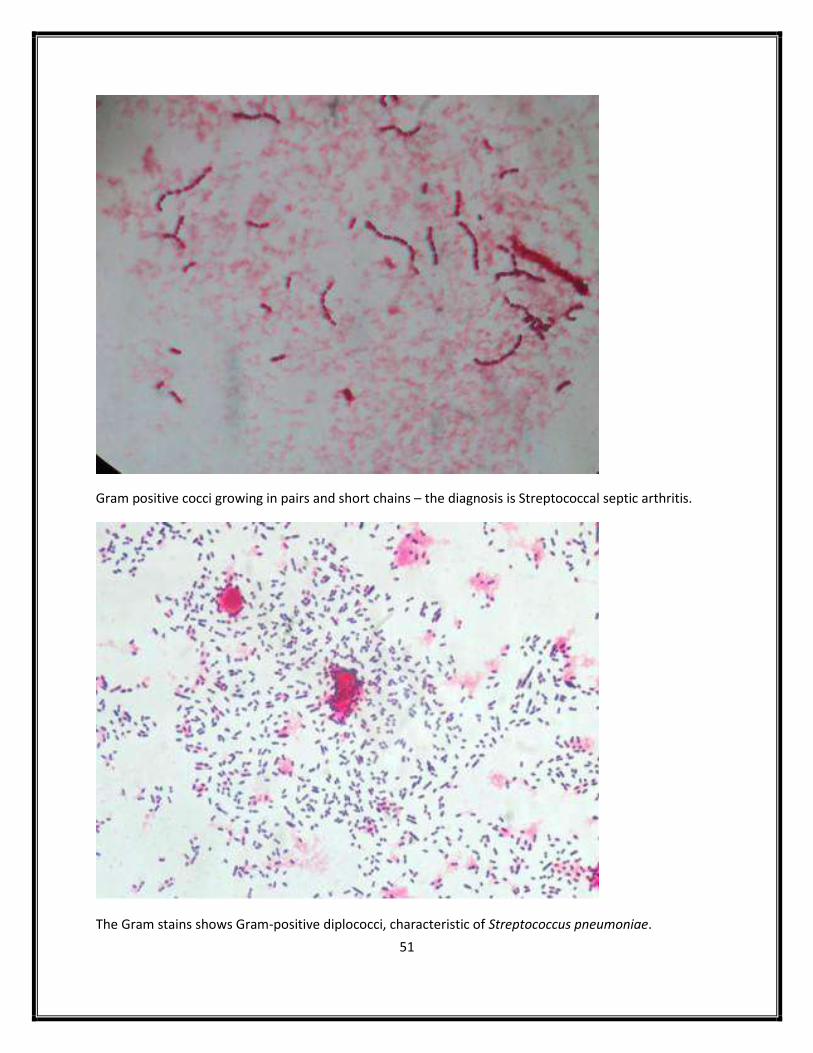
Gram positive cocci growing in pairs and short chains – the diagnosis is Streptococcal septic arthritis.
The Gram stains shows Gram-positive diplococci, characteristic of Streptococcus pneumoniae.

52
Enterobius vermicularis.
Giardiasis.

53
Cryptococcal meningitis: C. neoformans in the CSF – shown on an India ink stain: the thick
polysaccharide capsule is highlighted around the cell.
Ascaris lumbricoides.

54
An excised Meckel’s diverticulum.
There is complete destruction of the aortic valve, with vegetations attached to its remnants.
Staphylococcus aureus endocarditis is an aggressive disease frequently associated with valve destruction
and abscess formation.
55
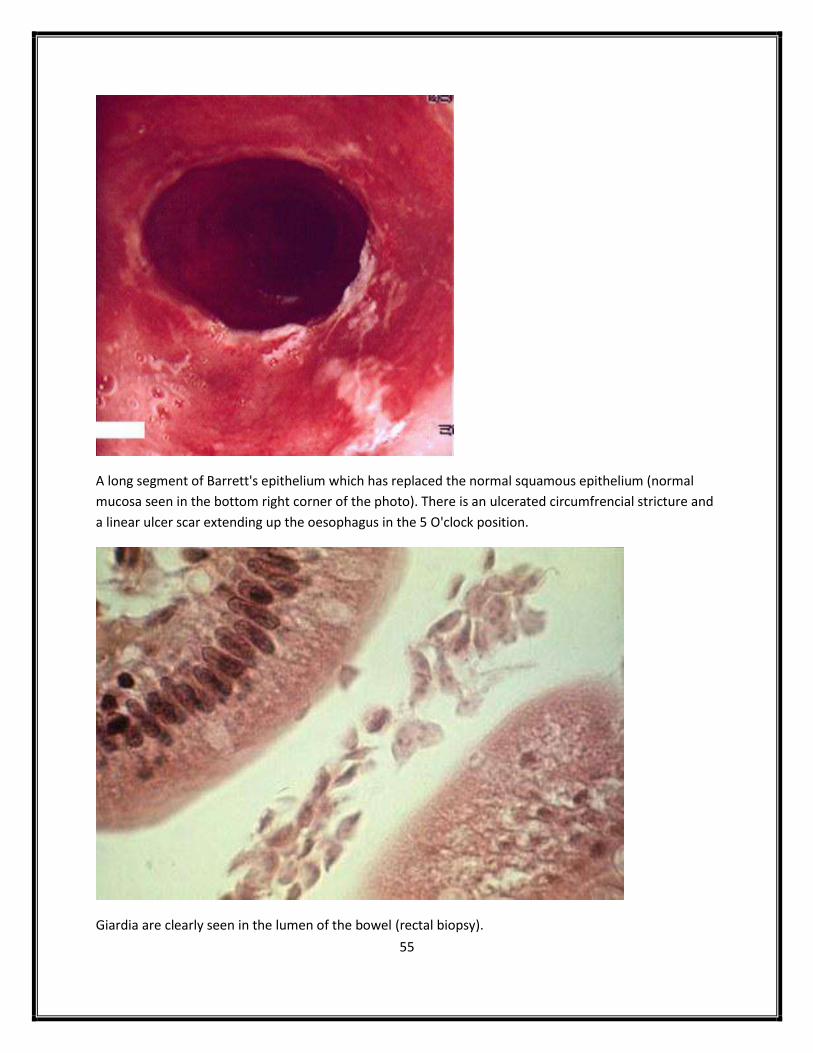
A long segment of Barrett's epithelium which has replaced the normal squamous epithelium (normal
mucosa seen in the bottom right corner of the photo). There is an ulcerated circumfrencial stricture and
a linear ulcer scar extending up the oesophagus in the 5 O'clock position.
Giardia are clearly seen in the lumen of the bowel (rectal biopsy).

56
Section of excised bowel showing typical 'cobblestone mucosa' of Crohn’s disease.
Thick pseudomembrane adherent to the colonic mucosa (pseudomembranous colitis).

57
Typical morphology of Aspergillus fumigates.
The culture plate shows a growth of Pseudomonas aeruginosa, characterized by the green colouration of
the colonies - due to production of the pigment pyocyanin.

58
Milky looking serum sample is due to hyperchylomicronaemia/hypertriglycerideamia and is a
consequence of deficiency of Lipoprotein Lipase.
The slide shows the typical appearance of toxocara retinitis with a lesion at the macula. In retinitis due to Toxocara
canis, there is usually only a single, well demarcated lesion. (central visual field defect)
59
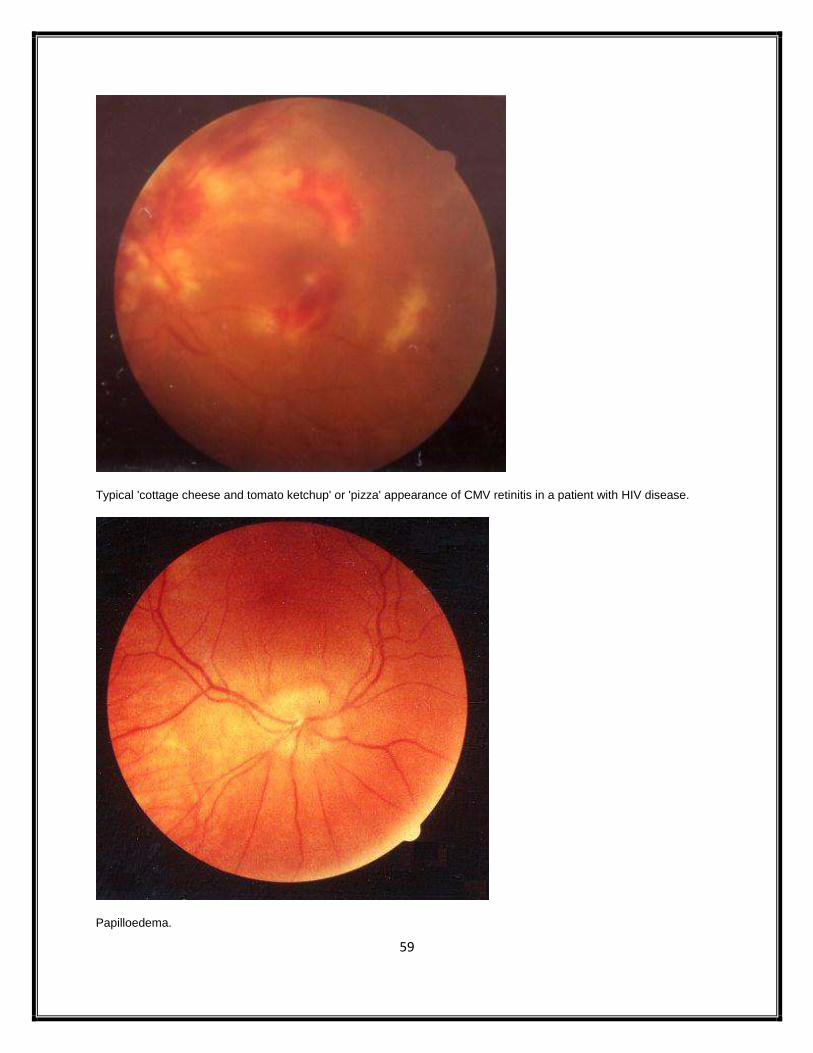
Typical 'cottage cheese and tomato ketchup' or 'pizza' appearance of CMV retinitis in a patient with HIV disease.
Papilloedema.

60
The slide shows angioid streaks, caused by breaks in Bruch's membrane. Angioid streaks may be associated with
pseudoxanthoma elasticum, Ehlers-Danlos syndrome, sickle cell disease, Acromegaly (and other pituitary disorders),
and Paget's disease.
CRVO.
61
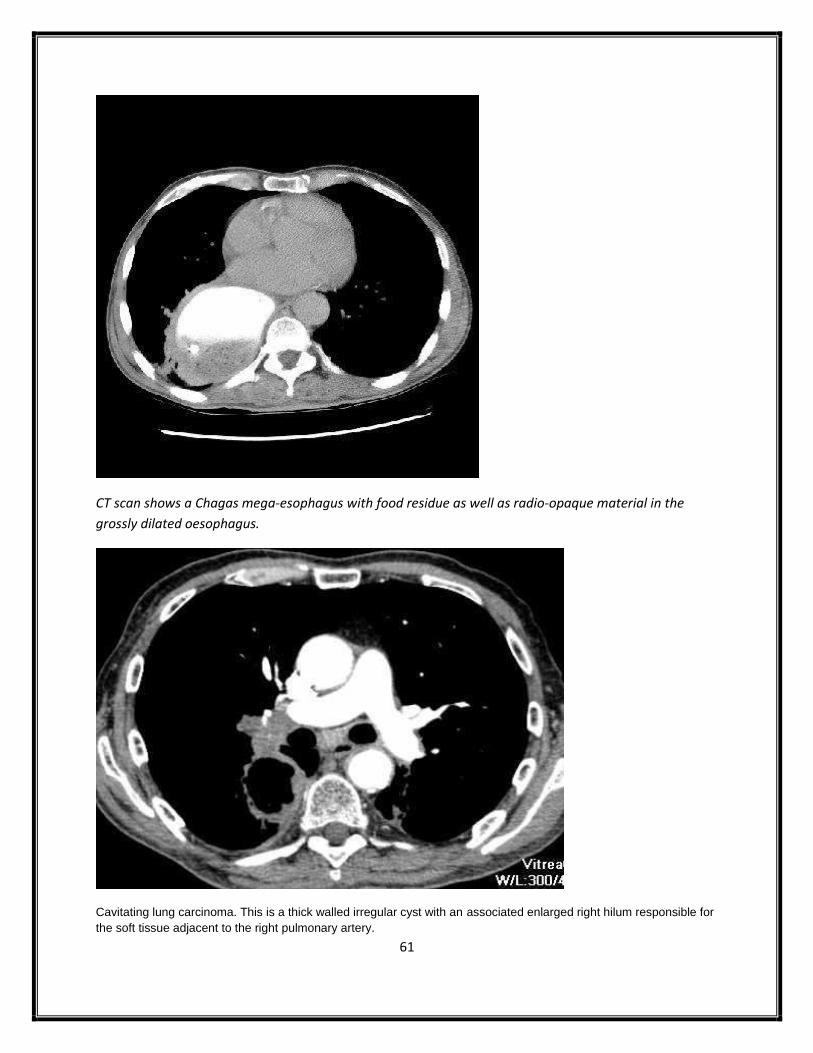
CT scan shows a Chagas mega-esophagus with food residue as well as radio-opaque material in the
grossly dilated oesophagus.
Cavitating lung carcinoma. This is a thick walled irregular cyst with an associated enlarged right hilum responsible for
the soft tissue adjacent to the right pulmonary artery.

62
CT brain: the most likely diagnosis with a solitary frontal lesion in a young patient with chronic sinusitis is a frontal
brain abscess.
Cerebral toxoplasmosis .The typical appearance on CT is of multiple ring-enhancing lesions.

63
Non-contrasted phase of the CT scan showing Falx calcification.
Karyotype. 46 XY. (Normal male)

64
Mitochonrial e.g. Leber’s optic atrophy.
XLR e.g. Hemophila A & B, Duchenne muscular dystrophy, Becker muscular dystrophy, G6PD deficiency,
Lesch-Nyhan syn, nephrogenic DI, Hunter’s syn, Anderson Fabry dis, ocular albinism.

















