NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 1 Multidisciplinary Guidelines for the Management of the Patient with Subarachnoid Haemorrhage in NICU Introduction Aneurysmal subarachnoid haemorrhage (SAH) is a devastating disease with an incidence of 2 to 22.5 per 100,000 population, although it accounts for only 3- 5% of strokes overall. It is responsible for a large loss of productive life years because it commonly occurs in younger people, peaking between 40 and 60 years. It occurs more commonly in females (70%) than males (30%).(1) One-month case fatality is as high as 35% even in high income countries, and around one third of those who survive need life-long care, with a further third having residual cognitive impairment that affects their functional status and quality of life. Mortality is higher and good functional outcome less likely in patients with poor grade SAH, those over 65 years of age and those who develop complications. Early aggressive resuscitation and multidisciplinary intensive care management is associated with improved outcomes and consensus guidelines for the intensive care management of SAH have recently been published.(2,3) Approximately 85% of cases of SAH are related to spontaneous rupture of an intracranial aneurysm in the basal cerebral arteries, leading to escape of blood at high pressure into the subarachnoid space. Non-aneurysmal peri- mesencephalic bleeds, with haemorrhage centred anterior to the midbrain or pons, account for 10% of cases. A further 5% are divided between multiple, rarer pathologies, including traumatic causes.
Transcript
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 1
Multidisciplinary Guidelines for the Management
of the Patient with Subarachnoid Haemorrhage
in NICU
Introduction
Aneurysmal subarachnoid haemorrhage (SAH) is a devastating disease with an
incidence of 2 to 22.5 per 100,000 population, although it accounts for only 3-
5% of strokes overall. It is responsible for a large loss of productive life years
because it commonly occurs in younger people, peaking between 40 and 60
years. It occurs more commonly in females (70%) than males (30%).(1)
One-month case fatality is as high as 35% even in high income countries, and
around one third of those who survive need life-long care, with a further third
having residual cognitive impairment that affects their functional status and
quality of life.
Mortality is higher and good functional outcome less likely in patients with
poor grade SAH, those over 65 years of age and those who develop
complications.
Early aggressive resuscitation and multidisciplinary intensive care management
is associated with improved outcomes and consensus guidelines for the
intensive care management of SAH have recently been published.(2,3)
Approximately 85% of cases of SAH are related to spontaneous rupture of an
intracranial aneurysm in the basal cerebral arteries, leading to escape of blood
at high pressure into the subarachnoid space. Non-aneurysmal peri-
mesencephalic bleeds, with haemorrhage centred anterior to the midbrain or
pons, account for 10% of cases. A further 5% are divided between multiple,
rarer pathologies, including traumatic causes.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 2
First edition published 2015 Ian Littlejohn Consultant Anaesthesia and Intensive Care medicine Andrew Iverson Consultant Chemical Pathologist Christina Baker Neurosurgical Pharmacist Nathalie Pearson Senior Sister Jann Rieneker Senior Sister John Norris Consultant Neurosurgeon Linda Kinsella Practice Development Nurse Sorin Bucur Consultant Neurosurgeon Mansoor Foroughi Consultant Neurosurgeon
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 3
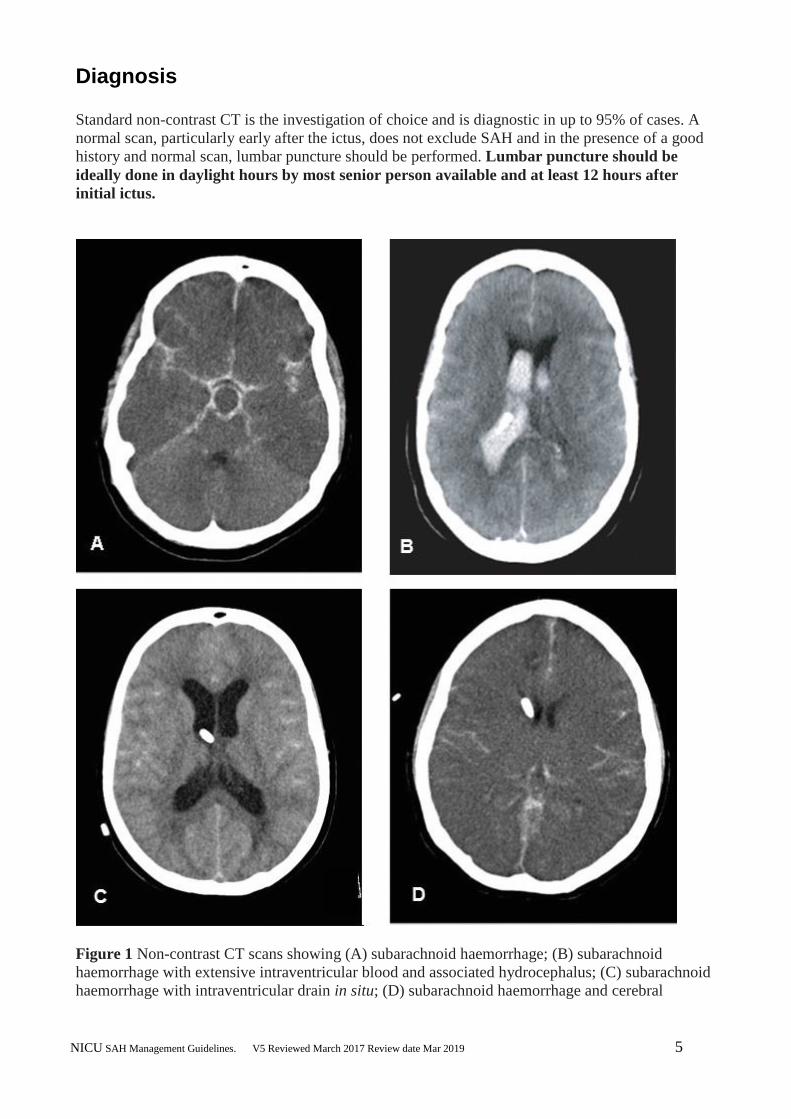
haemorrhage with extensive intraventricular blood and associated hydrocephalus; (C) subarachnoid
haemorrhage with intraventricular drain in situ; (D) subarachnoid haemorrhage and cerebral
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 6
oedema with loss of appearance of the brain sulci and gyri, and effaced ventricles (with ventricular
drain in situ) (5)
Confirmation of the presence of red blood cells or their metabolites in the cerebrospinal fluid
identifies an additional 3% of patients who subsequently have an aneurysm detected by cerebral
angiography. The diagnostic sensitivity of lumbar puncture is increased when performed at least 12
hours after the initial ictus, although this results in a delay in initiating treatment.
The opening pressure of cerebrospinal fluid must be recorded and samples analysed for protein,
cells, and glucose (paired with a serum sample) CSF bilirubin, CSF spectrophotometry and CSF
microbiology
An increase in CSF bilirubin is the key finding, which supports the occurrence of SAH but is not
specific for this. In most positive cases, bilirubin will occur with oxyhaemoglobin. Please see
BSUHT pathology for details of CSF collection:
(http://pathology.bsuh.nhs.uk/Pathology/Default.aspx?tabid=119#CSF and xanthochromia (see
below).
BSUHT Pathology Guidelines
Xanthochromia (CSF)
(CSF bilirubin, CSF scan, CSF spectrophotometry)
Spectrophotometric scan to detect and discriminate traces of Hb and/or bilirubin in cases of suspected subarachnoid haemorrhage.
Wherever possible, sample must be collected at least 12h post event.
At least 1 mL CSF in plain Universal container.
DO NOT put the CSF in Vacuette® tube.
Protect from light (wrap in foil or place sample in a thick brown envelope outside the usual plastic specimen bag). Please use yellow request forms.
Click here for full details of CSF collection. It is important to use the last sample as it is the least likely to be contaminated with blood from a traumatic tap, which greatly impairs the diagnostic sensitivity of the test.
Avoid using air tube delivery system.
Please send a clotted blood sample taken at the same time, for plasma bilirubin and total protein.
Request form should include:
- Clinical indication for request - Result of CT scan - Time of onset of symptoms/event - Time of lumbar puncture - If the differential diagnosis includes meningitis.
Recommendations from the revised National Guidelines for Analysis of Cerebrospinal Fluid for Bilirubin in Suspected Subarachnoid Haemorrhage 2008.
hyperventilation (PaCO2 4.0-4.5 kPa) may be indicated ONLY if intracranial hypertension is
suspected, e.g. in the presence of hydrocephalus, an expanding intraparenchymal haematoma or
cerebral oedema. (6)
Hypertension is a normal response to SAH, although high blood pressure increases the risk of re-
bleeding, whereas excessive reductions in blood pressure risk the development of cerebral ischemia.
Extreme hypertension (mean ABP > 130 mmHg), should be treated cautiously with short-acting
agents (labetalol infusion) but modest elevations in blood pressure (mean ABP <110 mm Hg) do
not require treatment. Analgesia should also be considered in all patients with hypertension.
Prior to securing the aneurysm, premorbid blood pressure should be used to refine pressure targets,
although mean ABP is usually maintained between 90-110 mm Hg or a systolic ABP not greater
than 160 mmHg .(2)
Patient should be nursed in bed for first 24 hours with head of bed slightly elevated 30 degrees
(although nursing flat may be considered as a temporary measure if vasospasm is suspected).
Hypotension should be meticulously avoided.
Baseline investigations
1. FBC- anaemia(sickle cell disease) and leucocytosis( after seizure, systemic
infection)
2. Clotting screen- underlying coagulopathy
3. U&Es, Mg, LFTs, glucose, CRP
4. Arterial blood gases if indicated
5. CXR – pulmonary oedema and aspiration
6. ECG – cardiac arrhythmia, ST changes
7. Troponin
8. Cross match or group and save
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 8
9. LP if indicated see above
10. CT head
11. Weight
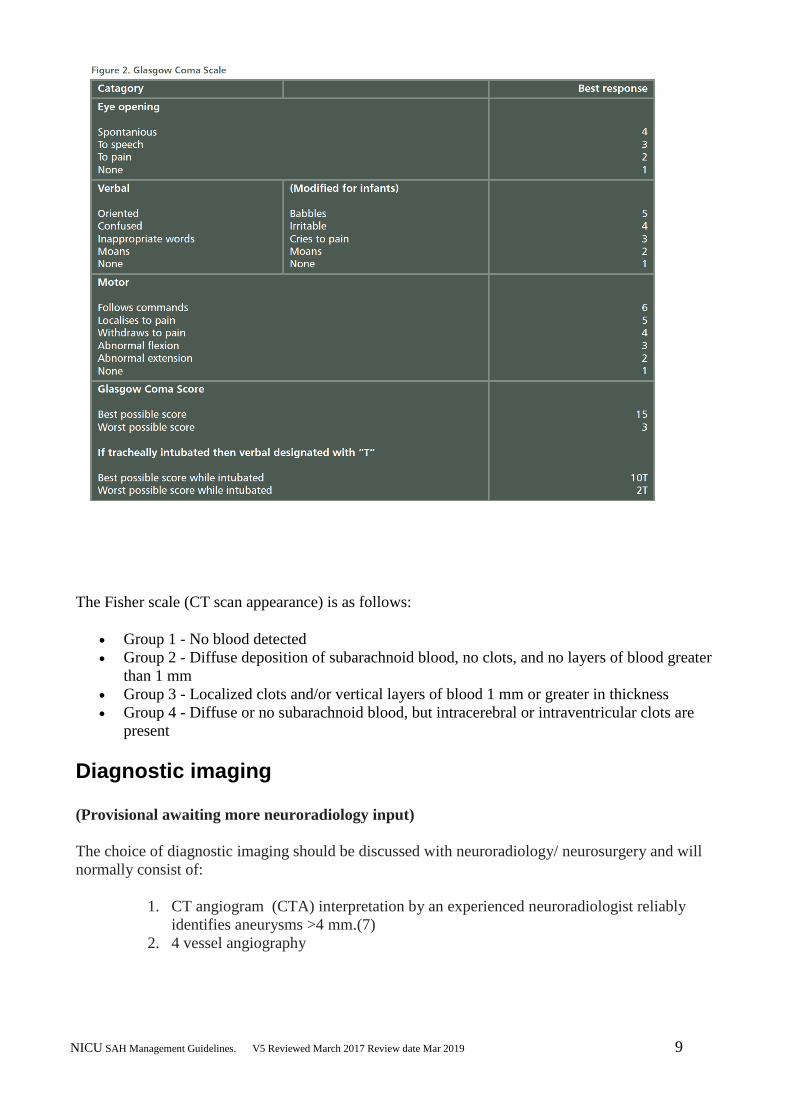
Grading
The World Federation of Neurological Surgeons grading scale standardises clinical evaluation over
time and helps estimate prognosis (Figure1).
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 9
The Fisher scale (CT scan appearance) is as follows:
Group 1 - No blood detected
Group 2 - Diffuse deposition of subarachnoid blood, no clots, and no layers of blood greater
than 1 mm
Group 3 - Localized clots and/or vertical layers of blood 1 mm or greater in thickness
Group 4 - Diffuse or no subarachnoid blood, but intracerebral or intraventricular clots are
present
Diagnostic imaging
(Provisional awaiting more neuroradiology input)
The choice of diagnostic imaging should be discussed with neuroradiology/ neurosurgery and will
normally consist of:
1. CT angiogram (CTA) interpretation by an experienced neuroradiologist reliably
identifies aneurysms >4 mm.(7)
2. 4 vessel angiography
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 10
Negative angiographic findings do not rule out aneurysm. Approximately 10-20% of patients with
clinically diagnosed SAH (on CT and/or lumbar puncture) have negative angiographic findings. A
repeat angiogram is usually required in 10-21 days in such cases.
The following may also be considered in individual cases:
1. MRI or MRI angiography
2. CT perfusion scans
Re-bleeding
Re-bleeding was previously the primary cause of death following poor grade SAH but rates have
dramatically reduced since the shift towards early securing of the ruptured aneurysm. The greatest
risk of re-bleeding occurs within the first 24 hours and is highest in those with the poorest grade.
The overall re-bleeding rate is 4-7%, with a 1.5% risk per day for up to two weeks after the ictus
and is highest in first 72 hours (5-10%).(2)
Antifibrinolytics such as tranexamic acid are NOT recommended routinely due to risk of increased
DCI but may be considered for patients with an unavoidable delay in obliteration of aneurysm but
only in short term (<72 hours).(3)
Securing the aneurysm
Early aneurysm control reduces the risk of re-bleeding and allows higher ABP to prevent or treat
cerebral hypoperfusion. The choice of aneurysm control will be different for each patient site and
type of aneurysm and will normally be either endovascular technique (GDC coiling) or surgical
technique (clipping) as decided by the neurovascular multidisciplinary meeting.
The International Subarachnoid Aneurysm Trial (ISAT) compared endovascular and surgical
techniques and confirmed an improvement in early survival in selected patients receiving
endovascular therapy, with a small excess of late bleeds.(8)
ISAT has been criticised for many reasons (9) In brief, 69% of the 9,559 patients eligible for
recruitment into the study were excluded because of lack of equipoise. Since almost all intracranial
aneurysms can be treated by surgery, it follows that a large proportion of patients was excluded
because of an assessment that their aneurysm was not suitable for coiling.
There was a rarity of posterior circulation and middle cerebral artery aneurysms in ISAT and,
because posterior circulation and middle cerebral artery aneurysms are preferentially treated by
coiling and clipping respectively, this also raises the possibility of sample bias. However, the
proportion of cases that are unsuitable for endovascular treatment is likely to be much lower today
because of advances in technology and expertise since 2002.
The majority of aneurysms are now primarily treated by endovascular options, but coiling is still
not a total replacement for surgical treatment. Aneurysms in selected locations, those >25 mm,
those with a wide neck or with branches arising from the aneurysm, may not be amenable to
coiling, and some may have a worse outcome with coiling compared to clipping. (9).
In terms of long term outcomes there is an increased risk of recurrent bleeding from a coiled
aneurysm compared with a clipped aneurysm, but the risks are small. The risk of death at 5 years
was significantly lower in the coiled group than it was in the clipped group. The standardised
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 11
mortality rate for patients treated for ruptured aneurysms was increased compared with the general
population.(10)
Each patient and aneurysm is different and a treatment decision must be made for each patient
individually by a multidisciplinary team (3).
Anaesthesia for GDC Coiling/Surgical Clipping Aneurysm Anaesthesia for GDC Coiling/Surgical Clipping Aneurysm is provided (or directly supervised) by a
Consultant Neuroanaesthetist.
All patients will require a level 2 bed postoperatively although in the case of elective cases this may
only be one night.
Deterioration Following Coiling
Acute neurological deterioration following coiling of a cerebral aneurysm may be due to
thromboembolism related to the coils or bleeding.
Thromboembolism can often be treated effectively by the prompt administration of ReoPro
(Abciximab). ReoPro is a potent anti-platelet antagonist which acts on platelet aggregation, the
cause of coil related thromboembolism. Rarely, acute neurological deterioration is due to re-
haemorrhage despite an apparently successful coiling procedure.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 12
If a patient deteriorates neurologically in the first 24 hours post-coiling:-
1. Arrange a CT head and discuss the case immediately with the duty neurosurgical SpR, who
should then contact the interventional neuroradiologist who performed the procedure or the On-call
Neuroradiologist if they are a interventional neuroradiologist.
2. ReoPro (10mg vial for reconstitution) may be indicated if the scan reveals no evidence of new
haemorrhage.
3 Discuss subsequent heparinisation and/or aspirin therapy with the interventional neuroradiologist.
4. If the aneurysm is large or giant (> 12mm) consider treatment with intravenous Dexamethasone
to reduce possible effects of peri-aneurysmal oedema related to thrombosis.
5. Continue close observation of femoral artery puncture sites, arterial lines, ventricular access
devices etc., following administration of ReoPro.
Intensive care management overview
Following securing of the aneurysm, the intensive care management of SAH involves treatment of
acute complications such as:
prevention or treatment of delayed cerebral ischemia (DCI)
Hydrocephalus
optimisation of systemic physiology
Non-neurological complications.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 13
Essential monitoring and access
1. ECG
2. Pulse oximetry
3. Capnography if intubated
4. Invasive arterial pressure monitoring ( AVOID FEMORAL PRE ANGIO)
5. Urinary catheter: hourly urine output and fluid balance recording
Following devices should be considered for suitable/poor grade patients:
1. Wide bore orogastric tube or nasogastric tube if not eating/ventilated. Follow
guidelines for confirming correct positioning of nasogastric tubes (appendix 1).
2. Quad/quin lumen CVP line ( AVOID FEMORAL PRE ANGIO AND POST-
INFECTION)
3. Cardiac output monitoring e.g. PiCCO, LiDCO, PAC, oesophageal Doppler
To be inserted if no response to fluids and no response to 0.1µg/kg/min of
Noradrenaline
If acute or pre-existing cardiac disease
Systemic sepsis
Pulmonary oedema
4. ICP monitoring
5. BIS monitor to ensure adequate sedation if ventilated
6. Peripheral Nerve Stimulator to monitor train of four if administering neuromuscular
blockade
7. Consider EEG monitor if suspected seizures
8. LICOX if ventilated
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 14
Daily investigations 1. Arterial blood gases following ventilator changes and when indicated minimum of
6hourly.
2. FBC and clotting screen.
3. U&Es, LFTs, Po4, Mg, CRP and Chloride
4. Troponin if ? myocardial injury
5. Lactate
6. Consider CXR if ventilated, chest problems or deterioration increasing FiO2.
7. Serum and urine osmolality if ?Diabetes Insipidus (DI), abnormalities of sodium or
multiple doses of osmotic diuretics
8. Weight (Kg)
9. ECG if changes
10. Urine specific gravity, more frequently if urine output > 250mls/hr. and DI
suspected.
Other investigations Patients sedated on propofol. CK which may be elevated due to rhabdomyolysis as a
result of the Propofol infusion syndrome (see head injury guidelines)
Triglyceride levels - the laboratory request must specifically state Triglyceride levels
and not lipid levels. If significant elevation occurs propofol infusion should be
stopped (Hogarth).
Consider urine electrolytes
Lolinogram profile
9am Cortisol level in case of pituitary injury (must be off steroids)
Drug levels as appropriate
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 15
Delayed Cerebral Ischemia (DCI)
DCI is a term applied to any neurological deterioration, including focal neurological deficits and
altered consciousness, which persists for more than one hour and cannot be explained by other
abnormalities identified by radiographic, laboratory or electrophysiological investigations. It may
be unrecognised clinically in some patients because of their poor clinical grade or the concurrent
administration of sedatives.
DCI occurs in around 30% of patients, peaks between four and 10 days after the ictus and persists
for several days and can occur up to day 21. It is second only to the initial haemorrhage as a cause
of morbidity and mortality after SAH.
DCI Pathophysiology
Although DCI has been attributed to cerebral vasospasm, the exact relationship between the two is
unclear. DCI can occur in the absence of vasospasm and vice versa, and ischemia often involves
more than one vascular territory. (11)
Other mechanisms contributing to DCI include vascular dysautoregulation, micro thrombi, direct
neurotoxic effects and cortical spreading depolarisation. (12)
DCI Diagnosis
DCI is detected clinically by a reduction in level of consciousness with or without a focal
neurologic deficit.
In unconscious or sedated patients, several methods can be used to identify DCI and the following
can be considered:
DSA remains the diagnostic gold standard but involves risks and time requirements
CT angiography and CT perfusion, which together allow characterisation of vascular
anatomy and associated cerebral perfusion abnormalities
Blood flow velocity (FV) >120-140 cm/s, or FV increases >50 cm/s/day from baseline, are
generally accepted to be indicative of developing or established DCI. However, there is
considerable interindividual variation and a recent study analysing 1,877 TCD examinations
found that almost 40% of patients with clinical evidence of DCI never had FVs that exceeded
120 cm/s.(13) Treatment decisions should not therefore be based on TCD findings alone. As
changes in the cerebral blood flow (CBF) affect FV, the Lindegaard ratio, which compares FV
in the ipsilateral middle and internal carotid arteries and is unaffected by changes in cerebral
blood flow (CBF), is often used. A ratio >3.0 is indicative of vasospasm and values >6 suggest
severe spasm.
Microdialysis
(NOT CURRENTLY AVAILABLE AT BSUHT)
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 16
DCI Treatment Nimodipine
All patients should receive enteral nimodipine 60 mg four-hourly immediately after diagnosis until
day 21. Nimodipine is a calcium channel blocker of the dihydropyridine group with preferential
activity on cerebral vessels. This reduces the incidence of DCI and improves outcome. (14).The
mechanisms by which nimodipine reduce DCI are uncertain because it does not reverse
angiographic vasospasm in humans.
Nimodipine can cause hypotension this may be managed by changing the dose to 30mg 2-hrly in
the first instance, if this fails the choice is either omitting other anti-hypertensive medication,
omitting the nimodipine or using intravenous nimodipine please discuss with neurosurgical team.
Although intravenous nimodipine is sometimes used in critically ill patients (must be administered
via a dedicated line), this route of administration is unproven and care must be taken to avoid
hypotension which frequently requires noradrenaline, please discuss with neurosurgical team.
Hypertensive therapy In the presence of a secured aneurysm, maintenance of ABP at supra-normal levels is the mainstay
of treatment of DCI. (15). The initial MAP usually being set at 90-100 mmHg and if DCI occurs
pressure should be increased in a stepwise fashion, guided by assessment of neurological function,
neuromonitoring or radiological evidence of improved perfusion.
Recent consensus guidance recommends that euvolaemia rather than hypervolemia should be the
target for both prophylaxis and treatment of DCI, and that haemodilution should not be used.(16)
Triple H therapy, hypervolemia, haemodilution and hypertension, was previously widely used to
prevent and treat DCI the combination but it has never been tested in a randomised controlled trial,
and while fluid therapy is a key component of the management of SAH, prophylactic
hypervolaemic therapy is not effective in raising CBF or improving neurological outcome, and
there is some evidence of harm from overly aggressive filling. (17)
Isotonic crystalloids (Hartmanns or N/saline) are the fluids of choice with a minimum intake of
3L/24 hr., although hypertonic saline solutions may sometimes have a place in patients who are
hyponatraemic but as a proportion of daily fluid intake.
In the presence of adequate volume status, noradrenaline is widely used to augment ABP.
Central venous pressure is an unreliable indicator of volume status after SAH and although invasive
ABP and cardiac output monitoring are often used to guide goal-directed volume and vasopressor
therapy, no technology has been demonstrated to improve outcome.
We generally will use a PICCO if noradrenaline requirements are either rapidly increasing, in the
presence of concurrent sepsis or when noradrenaline requirements are greater than 0.1 mcg/kg/min.
Endovascular treatment
There is some evidence that angioplasty and/or intra-arterial vasodilators may have a role if medical
therapy has failed and it should be discussed with interventional neuroradiology. (1)
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 17
DCI Novel treatments NOT used
There is no current role for the following:
1. Hypermagnesaemia. Magnesium was demonstrated in a randomised clinical trial to have
no beneficial effect on incidence of DCI, cerebral infarction or clinical outcome.(18), and a
subsequent post hoc analysis showed worse clinical outcomes.(19) In view of this
magnesium should be kept in normal range to avoid arrhythmias.
2. Statins. The STASH trial did not detect any benefit in the use of simvastatin for long-term
or short-term outcome in patients with aneurysmal subarachnoid haemorrhage.(20) Despite
demonstrating no safety concerns, it was concluded that patients with subarachnoid
haemorrhage should not be treated routinely with simvastatin during the acute stage
although those on chronic statin therapy should be continued.
3. Anti-fibrinolytics. May reduce rate of rebleeding but this is offset by a higher rate of DCI.
(21)
4. Antiplatelet agents. A Cochrane review suggested a non-significant trend towards
improved outcome in patients treated with antiplatelet agents but accompanied by increased
risk of haemorrhagic complications. (22). They may have a role after interventional
radiology discuss with Pannos
Acute hydrocephalus Acute hydrocephalus is common following SAH (15-87%) and may present either incidentally on
CT scan or with increasing headache or decreasing GCS. The treatment in the acute stage is treated
initially with one of the following EVD, lumbar drains or serial lumbar punctures and in some
chronic cases VP shunt (8.9-48%). (3)
Please discuss management with neurosurgical team.
Intracranial pressure management A small number of patients with SAH may develop intracranial hypertension.(1) The management
should focus on treatment hydrocephalus, evacuation of intracranial haemorrhage or cerebral
oedema secondary to ischaemic infarction.
The basic principle of management should be similar to head injury see BSUHT Head injury
Guidelines although higher CPP targets may be selected. (See BSUHT ICU Guidelines on intranet)
Seizure control Seizures occur in approximately 20% of patients after SAH but treatment remains controversial and
it remains unclear if these are verifiably epileptic in origin. Actual seizures must be treated
aggressively but universal prophylaxis is not recommended. Three days of treatment offers similar
seizure prevention and better outcome than longer term therapy. (23)
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 18
Phenytoin should be avoided because of associated cognitive effects and poor outcome and a short
course of levetiracetam is recommended. (24)
Continuous EEG monitoring should be considered in patients with poor grade SAH who fail to
improve or have neurological deterioration of unknown aetiology. (3)
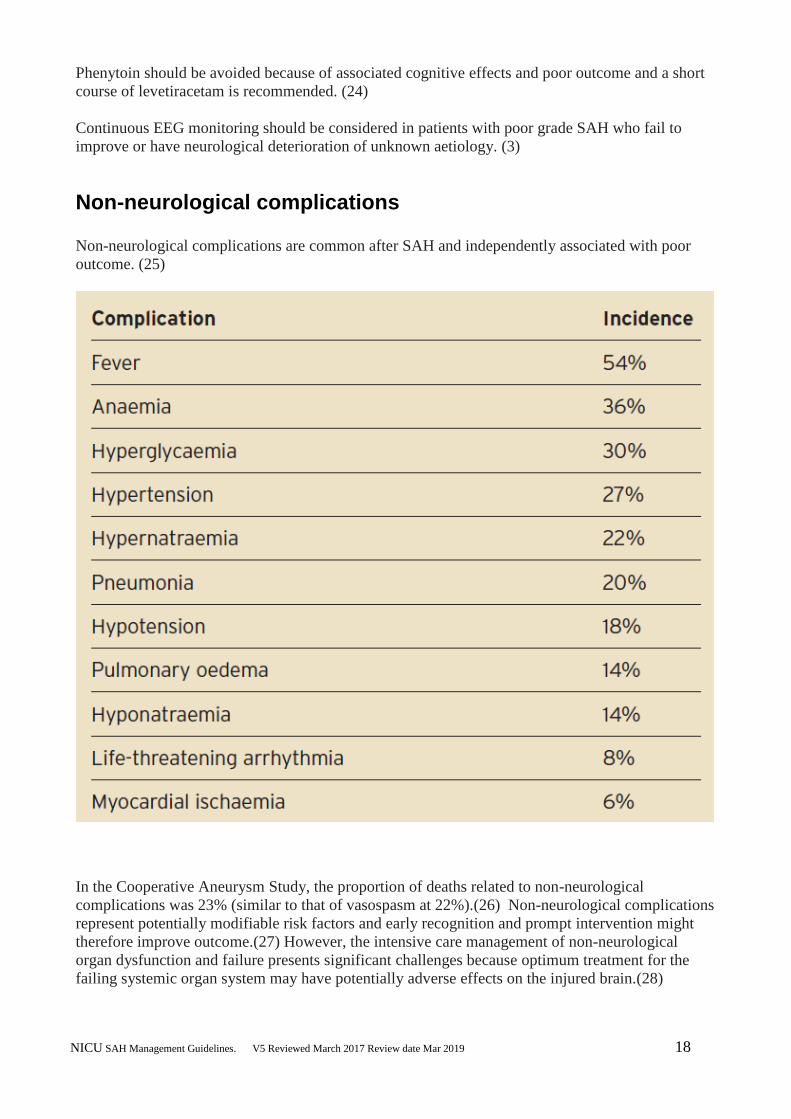
Non-neurological complications
Non-neurological complications are common after SAH and independently associated with poor
outcome. (25)
In the Cooperative Aneurysm Study, the proportion of deaths related to non-neurological
complications was 23% (similar to that of vasospasm at 22%).(26) Non-neurological complications
represent potentially modifiable risk factors and early recognition and prompt intervention might
therefore improve outcome.(27) However, the intensive care management of non-neurological
organ dysfunction and failure presents significant challenges because optimum treatment for the
failing systemic organ system may have potentially adverse effects on the injured brain.(28)
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 19
Cardiopulmonary complications
Cardiac complications are common and associated with DCI and poor outcome.(29) These are
manifest as an abnormal ECG, elevated cardiac troponin (cTnI) occurs in 20-40% of patients and a
spectrum of ventricular dysfunction collectively referred to as the neurogenic stunned myocardium
(NSM) syndrome in around 18%.(30)
NSM is caused by excessive noradrenaline release from myocardial sympathetic nerve terminals
resulting in a physiological myocardial denervation in the presence of normal coronary perfusion.
(31) This results in a characteristic pattern of LV regional wall motion abnormalities involving the
basal and middle portions of the anteroseptal and anterior ventricular walls with relative apical
sparing, reflecting the distribution of sympathetic nerves rather than specific vascular territories.
(32) The degree of myocardial dysfunction and damage is related to the severity of the SAH (33)
and, although LV dysfunction is usually temporary, it is associated with higher mortality after SAH.
Takotsubo cardiomyopathy, also referred to as left apical ballooning, is also a rare cause of
ventricular dysfunction after SAH, when it is associated with increased mortality. (34)
NSM may be associated with minimal clinical effects but, in severe cases, can lead to cardiogenic
shock and pulmonary oedema.
Inotropic support with dobutamine and, less so, milrinone is beneficial in the setting of low cardiac
output, despite a mechanism of action similar to the cause of cardiac injury. (35)
Pure vasopressors are often necessary to maintain cerebral perfusion but their adverse effects on
cardiac work risks potentiating myocardial injury. Characterising cardiac performance using
echocardiography and continuous cardiac output (PICCO) monitoring may be useful in guiding
therapy in patients with symptomatic NSM.
Neurogenic pulmonary oedema (NPO) and pneumonia are common after SAH and associated with
adverse outcome. (36, 37)
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 20
The mechanism of NPO is controversial but likely to be related to neurogenic-mediated
catecholamine release that leads to both hydrostatic and permeability oedema. Many patients with
SAH and acute lung injury can be managed safely using lung protective ventilation strategies
(ARDS Net), but in others there can be a conflict between treating the lungs and the injured brain.
(38) A ventilation strategy that maximises oxygenation while balancing risks to the lungs and
injured brain should be identified individually for each patient. (39)
Hyponatraemia Hyponatraemia after SAH is relatively common in neurointensive care (@30%) although its cause
remains controversial and has been though to related to either the syndrome of inappropriate
antidiuretic hormone secretion (SIADH) or cerebral salt wasting (CSW) syndrome, although on
occasions iatrogenic haemodilution can be implicated or certain drugs such as long term use
carbamazepine, PPI or citalopram. As plasma tonicity reduces, fluid shifts may precipitate cerebral
oedema and neurological symptoms therefore the aim is to keep Na > 135.
SIADH occurs because of excess antidiuretic hormone secretion, causing water retention, volume
overload and dilutional hyponatraemia.
CSW on the other hand is associated with raised atrial and brain natriuretic peptide and excessive
renal sodium and water loss, leading to classically circulating volume contraction with associated
hypotension and tachycardia, although many patients remain cardiovascularly stable due to a
combination of fluid replacement and a secondary ADH secretion.(40,41)
In normal situations it is important to distinguish between SIADH and CSW syndrome, since the
treatment of the two is diametrically opposed. (40) Electrolyte-free water restriction, initially to
1,000-1,500 mL/day, forms the usual mainstay of treatment of SIADH but this may worsen
cardiovascular instability and increase the risk of cerebral hypoperfusion after
SAH so this treatment should be avoided in the period of DCI (Day1-21). (2)
Consideration should be given to the use of hypertonic saline (1.8%) in hyponatraemic patients with
a high risk of DCI.
The primary treatment of CSW syndrome is volume and sodium resuscitation. Fludrocortisone or
hydrocortisone may also be used to limit the natiuresis but care must be taken to monitor for
hypokalaemia and hyperglycaemia.(2)
Pharmacological therapies such as demeclocycline and ADH-receptor antagonists are NOT
recommended. (3)
The treatment of hyponatraemia is thus controversial and difficult although the following is our
current practice derived from the most commonly used international guidelines (2, 3):
All patients with hyponatraemia (serum Na less than 135mmol/L) should have the following:
1. Random serum cortisol to exclude hypothalamic-pituitary-adrenal axis deficiency and
TFT ( free T4) to exclude hypothyroidism
2. Serum and urine osmolality and urinary Na.
3. Daily weights
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 21
4. Sodium replacement in the form of Slow Sodium tablets (600mg- 1.2 g qds) or
concentrated sodium chloride injection 30% added to the NG feed. (1.5 (5ml) -3g
(10ml) of sodium can be added to a litre bag of feed)
5. Fludrocortisone at an initial dose of 50mcg daily increasing to 200mcg
6. If Na less than 130mmol/L they should also have 1.8% NaCL ideally via a central line
at a rate of 30ml/h until serum Na is greater than 135 mmol/L. Serum Na should be
checked 4 hourly on 1.8% NaCL to prevent increases greater than 8mmol/24h and
hence avoid central pontine myelinosis.
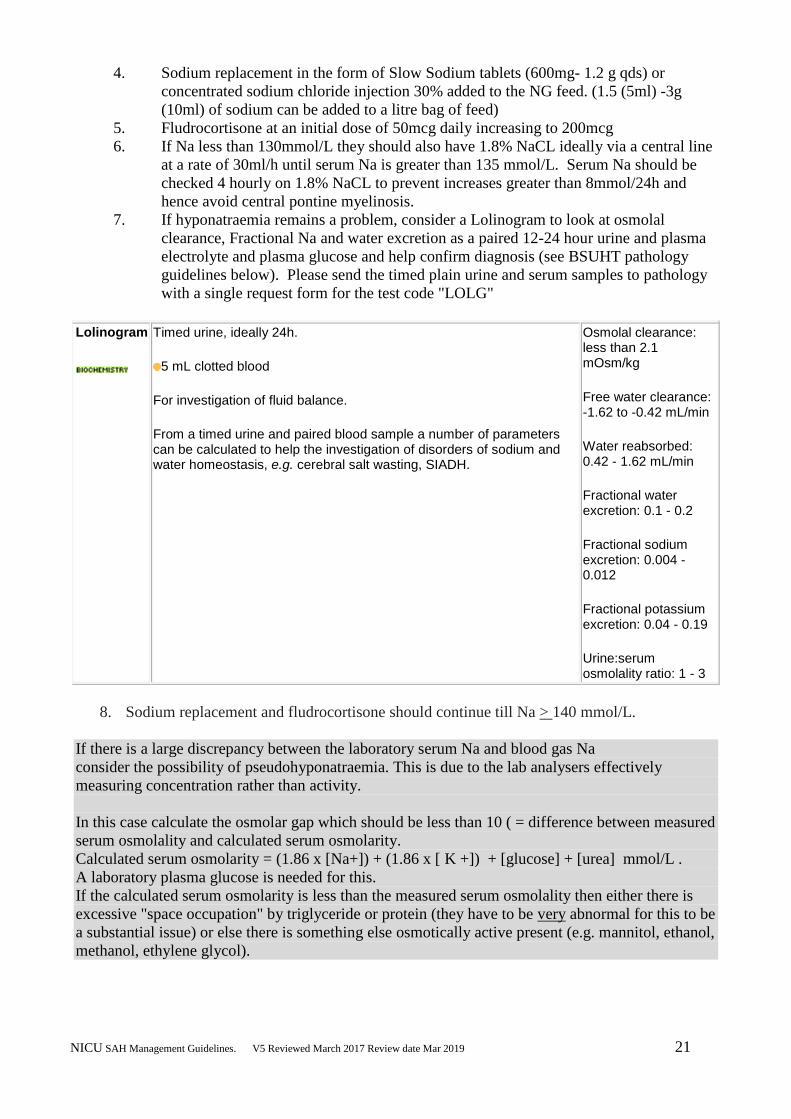
7. If hyponatraemia remains a problem, consider a Lolinogram to look at osmolal
clearance, Fractional Na and water excretion as a paired 12-24 hour urine and plasma
electrolyte and plasma glucose and help confirm diagnosis (see BSUHT pathology
guidelines below). Please send the timed plain urine and serum samples to pathology
with a single request form for the test code "LOLG"
Lolinogram
Timed urine, ideally 24h.
5 mL clotted blood
For investigation of fluid balance.
From a timed urine and paired blood sample a number of parameters can be calculated to help the investigation of disorders of sodium and water homeostasis, e.g. cerebral salt wasting, SIADH.
Osmolal clearance: less than 2.1 mOsm/kg
Free water clearance: -1.62 to -0.42 mL/min
Water reabsorbed: 0.42 - 1.62 mL/min
Fractional water excretion: 0.1 - 0.2
Fractional sodium excretion: 0.004 - 0.012
Fractional potassium excretion: 0.04 - 0.19
Urine:serum osmolality ratio: 1 - 3
8. Sodium replacement and fludrocortisone should continue till Na > 140 mmol/L.
If there is a large discrepancy between the laboratory serum Na and blood gas Na
consider the possibility of pseudohyponatraemia. This is due to the lab analysers effectively
measuring concentration rather than activity.
In this case calculate the osmolar gap which should be less than 10 ( = difference between measured
serum osmolality and calculated serum osmolarity.
Calculated serum osmolarity = (1.86 x [Na+]) + (1.86 x [ K +]) + [glucose] + [urea] mmol/L .
A laboratory plasma glucose is needed for this.
If the calculated serum osmolarity is less than the measured serum osmolality then either there is
excessive "space occupation" by triglyceride or protein (they have to be very abnormal for this to be
a substantial issue) or else there is something else osmotically active present (e.g. mannitol, ethanol,
methanol, ethylene glycol).
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 22
See also Sodium Management in Appendix
Hypernatraemia Hypernatraemia independently increases the risk of adverse cardiac outcome and death after SAH
and patients with hypernatremia should be monitored for evidence of cardiac dysfunction. (42).
Hypernatraemia in SAH is mainly caused as a consequence of either the use of osmotic diuretics or
diabetes insipidus which is commonly associated with raised intracranial pressure secondary to
intracranial haemorrhage, hydrocephalus or oedema secondary to cerebral ischemia so if diagnosis
it should prompt consideration of an urgent CT Scan. Other rare causes are dehydration before
admission or excessive saline infusion.
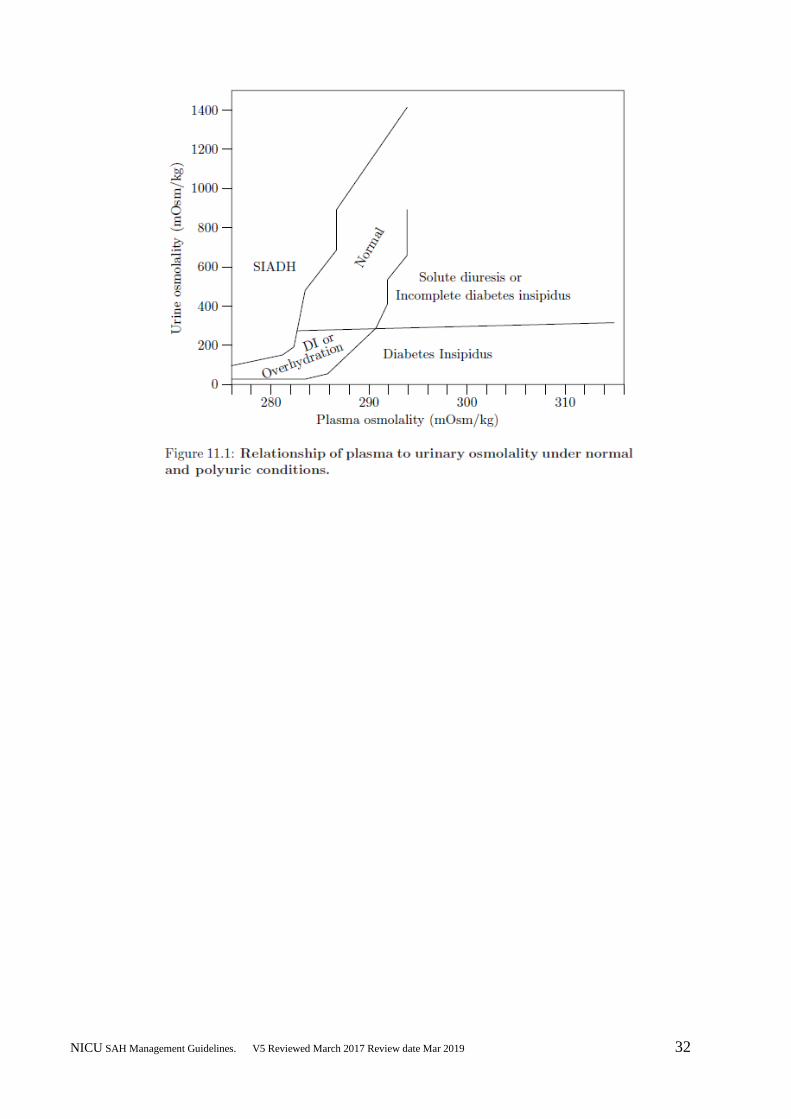
Diabetes insipidus should be suspected if urine output > 250mls/hr. for more than 3 hours and
specific gravity <1005. Confirm by measuring plasma and urinary osmolalities and
electrolytes. In DI plasma osmolality rises with a marked rise in Na+ > 150 mmols/l and urine
osmolality is very low with low electrolyte concentrations.
Remember that in many patients particularly postop diuresis may be appropriate (i.e do
they have a low plasma and urine osmolality, do they have a previous high cumulative
balance)
If confirmed on laboratory results, urine output continuing to rise and plasma Na+ >155
mmols/l give desmopressin (DDAVP) 0.5micrograms – 1 micrograms subcutaneously or
intravenously. Replace fluid with 5% Dextrose or enteral water starting at 30ml/h.
See also Sodium Management in Appendix
Fever Fever occurs in up to 70% of patients, is more common in poor grade SAH and associated with
worse outcome.(43) While an infective cause should be excluded (pneumonia is particularly
common) by daily septic screens if temperature greater than 38C, the fever can be related to the
hypothalamic effects of subarachnoid blood.
Paracetamol is first line therapy for fever control and although active cooling to normothermia has
been associated with improved outcome, the adverse effects of shivering (44) might offset its
benefits so is not used routinely.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 23
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 24
Glycaemic control
Hyperglycaemia is common after SAH, occurring in around 30% of patients, and is associated with
adverse outcome. (45)
Tight glycaemic control is not recommended since it can be associated with increased cerebral
metabolic crises. (46) Current practice has adopted more relaxed glycaemic targets (typically
6-11 mmol/L) limiting overly-aggressive insulin administration and minimising the risk of
hypoglycaemia and its known adverse effects on the injured brain. (48)
Monitor blood glucose with 2-4 hourly measurements on admission.
If the blood glucose is stable within 4.5-8.3mmol/L then reduce frequency. Monitor blood glucose
at least once a day.
Commence sliding scale if indicated. It is recommended that patients receiving intravenous insulin
receive a glucose calorie source and that blood glucose values are monitored every 1-2 hours until
glucose values and insulin infusion rates are stable and then every 4 hours thereafter (47).
Low glucose levels obtained with point of care testing of capillary blood should be interpreted with
caution; as such measurements may overestimate arterial blood or plasma glucose values. (47)
Anaemia
Anaemia is very common and associated with poor outcome after SAH, although transfusion is
itself similarly associated with adverse outcome effects.(49) Current guidance recommends that
packed red cells be administered to maintain haemoglobin concentration between 8-10 g/dL ,
although higher thresholds might be appropriate in patients at high risk of DCI.(2)
Inter-hospital transfer
If patient to be transferred between units follow Recommendations for the Safe Transfer of Patients
with Brain Injury (6) and the South East Critical Care Network Transfer Guidelines.
Intra-hospital transfer Minimum monitoring when transferring patient (e.g. to CT scan)
ECG
Oxygen saturation
ETCO2 (if ventilated)
Arterial BP or NIBP
The blocks that are in the patient’s bedside monitor should be used for the transfer.
As soon as the patient is on the portable ventilator and attached to transport monitor you must
stabilise ETCO2 prior to transfer. Check ABG
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 25
DVT Prophylaxis SAH induces a prothrombotic state that may lead to development of DVT and pulmonary embolus.
The incidence of DVT ranges from1.5%-18% (2) with highest incidence in poor grade patients.
Pneumatic compression stockings should be used in all patients.
The use of low molecular weight and unfractionated heparin in patients may be considered 48 hours
after aneurysm has been secured and should be discussed with neurosurgeon/interventional
neuroradiologist due to the increased risk of bleeding with these drugs. (50)
Nutrition
Follow guidelines for confirming correct positioning of nasogastric tubes (appendix 1).
Follow unit protocol for establishing enteral nutrition.
High dose vitamins B and C IV on admission if there is any suspicion of chronic alcohol abuse or
chronic malnutrition.
Pabrinex IV is current drug of choice and is usually given for 3 days (suggest one pair three times a
day).
Please follow the trust guidelines for vitamin replacement for either alcohol abuse or refeeding
syndrome as indicated.
Early enteral feeding - aim to start within 24 hours of admission. Patients should be fed to attain full
caloric replacement by day 7 post injury2.
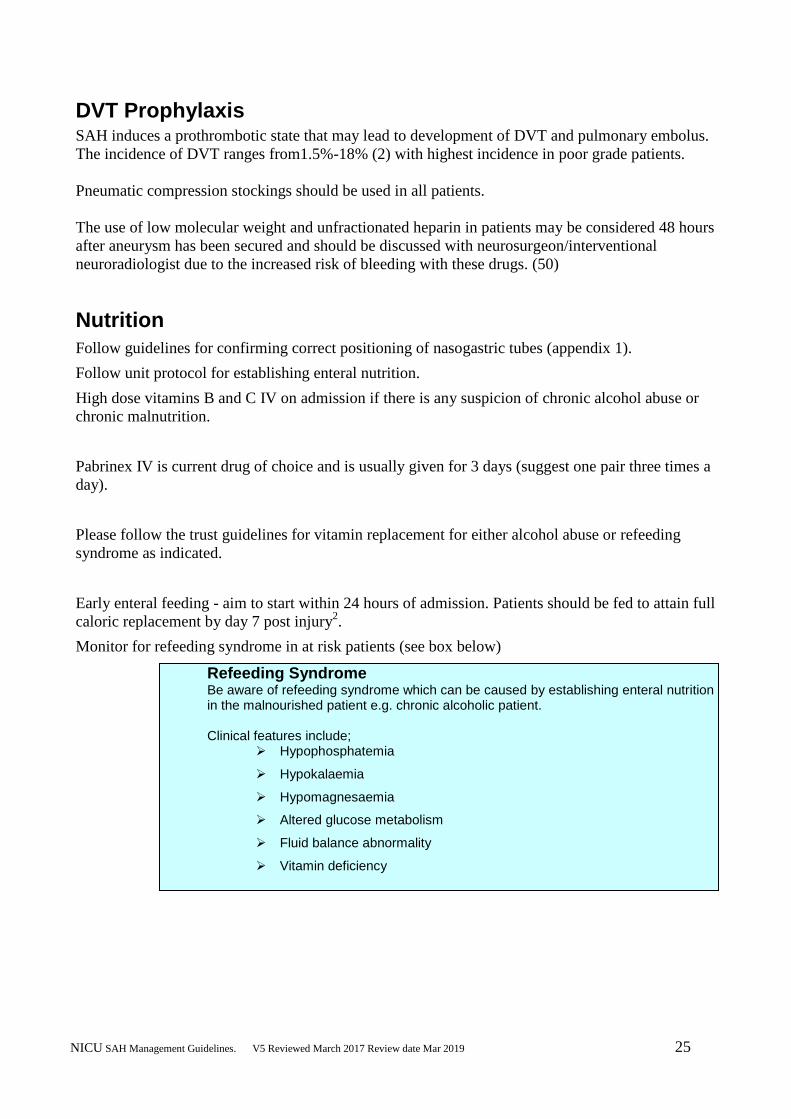
Monitor for refeeding syndrome in at risk patients (see box below)
Refeeding Syndrome Be aware of refeeding syndrome which can be caused by establishing enteral nutrition in the malnourished patient e.g. chronic alcoholic patient. Clinical features include;
Hypophosphatemia
Hypokalaemia
Hypomagnesaemia
Altered glucose metabolism
Fluid balance abnormality
Vitamin deficiency
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 26
Bowel Management
Follow unit bowel protocol
Infection Control
Follow Trust Infection Control Policy, available on the Trust intranet
Follow Trust Guidelines for Care of Central Venous Access Devices available on the Trust
intranet
Follow flow chart in Trust guidelines for changing of central venous catheters (appendix 5)
Clean bed space daily
Keep consumables in bed dividers to a minimum
Follow Trust procedures for disposing of contaminated waste and linen
No blind antibiotics unless increased CRP and/or WBC and/or pyrexia with worsening organ
function (e.g. worsening gas exchange) or systemic sepsis
Close liaison with microbiology
Neurophysiotherapy
If suspicion of increased tone and contractures developing, discuss with neuro-physiotherapist
and follow Spasticity Guidelines.
Seek advice from physiotherapist/neuro-physiotherapist regarding positioning of limbs and
passive limb movements.
Document instructions in nursing care plan.
If necessary photograph positions and place in care plan (consent must be gained from
family/carer)
If appropriate the Neuro-physiotherapist will discuss use of antispasticity medication with the
medical team.
If appropriate the neuro-physiotherapist will make resting splints with reference to the ACPIN
Guidelines for Splinting36
.
The patients splinting regime must be clearly documented in nursing care plan.
Rehabilitation will begin as soon as the patient is stable.
Clinical signs of raised ICP or cardiovascular instability will be monitored during
rehabilitation.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 27
Speech and Language Therapy
Refer patient to the Speech and Language Therapist using local referral procedure when starting to
wean patient from ventilation. This enables monitoring of communication and swallowing needs.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 28
References
1. Managing the Flow? Subarachnoid Haemorrhage: Managing the Flow (2013) NCEPOD
2. Diringer MN, Bleck TP, Claude HJ et al. Critical care management of patients following
aneurysmal subarachnoid haemorrhage: recommendations from the Neurocritical Care
Society's Multidisciplinary Consensus Conference. Neurocrit Care 2011; 15:211-40.
3. A. Connolly et al. Guidelines for the management of aneurysmal subarachnoid
haemorrhage: a guideline for healthcare professionals from the American Heart
38. Mascia L. Acute lung injury in patients with severe brain injury: a double hit model.
Neurocrit Care 2009;11:417-26.
39. Young N, Rhodes JK, Mascia L, Andrews PJ. Ventilatory strategies for patients with
acute brain injury. Curr Opin Crit Care 2010;16:45-52.
40. Tisdall M, Crocker M, Watkiss J, Smith M. Disturbances of sodium in critically ill adult
neurologic patients: a clinical review. J Neurosurg Anesthesiol 2006;18:57-63.
41. Lolin Y, Jackowski A. Hyponatraemia in neurosurgical patients: diagnosis using derived
parameters of sodium and water homeostasis. Br J Neurosurg. 1992;6:457–466
42. Fisher LA, Ko N, Miss J et al. Hypernatremia predicts adverse cardiovascular and
neurological outcomes after SAH. Neurocrit Care 2006;5:180-85.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 30
43. Fernandez A, Schmidt JM, Claassen J et al. Fever after subarachnoid hemorrhage: risk
factors and impact on outcome. Neurology 2007;68: 1013-19.
44. Scaravilli V, Tinchero G, Citerio G. Fever management in SAH. Neurocrit Care
2011;15:287-94. 45. Kruyt ND, Biessels GJ, de Haan RJ et al. Hyperglycemia and clinical outcome in
aneurysmal subarachnoid hemorrhage: a meta-analysis. Stroke 2009;40:e424-30.
46. Oddo M, Schmidt JM, Carrera E et al. Impact of tight glycemic control on cerebral
glucose metabolism after severe brain injury: a microdialysis study. Crit Care Med
2008;36:3233-38.
47. Dellinger R.P. et al. Surviving Sepsis Campaign: International guidelines for management
of severe sepsis and septic shock: 2008. Critical Care Medicine 2008; 36(1): 296-327
48. Schmutzhard E, Rabinstein AA. Spontaneous subarachnoid haemorrhage and glucose
management. Neurocrit Care 2011;15:281-86.
49. Kramer AH, Gurka MJ, Nathan B et al. Complications associated with anemia and blood
transfusion in patients with aneurysmal subarachnoid hemorrhage. Crit Care Med
2008;36:2070-75.
50. Collen JF, JacksonJl, Shorr AF, Moores LK. Prevention of venous thromboembolism in
neurosurgery: a metaanalysis. Chest. 2008;134:237-49.
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 31
Appendix 1: Sodium management
Sodium Management
Diabetes insipidus (DI) should be suspected if urine output > 250mls/hr for more than 3 hrs and specific gravity < 1005. Confirm by measuring plasma and urinary osmolalities and electrolytes. In DI plasma osmolality rises with a marked rise in Na
+ > 150 mmols/l and urine osmolality is very low with low electrolyte
concentrations.
If confirmed on laboratory results, urine output continuing to rise and plasma Na+ >155 mmols/l give
DDAVP 0.5micrograms – 1 micrograms SC or IV. Replace fluid with 5% Dextrose or enteral water.
If Na <134mmols consider Cerebral Salt Wasting (CSW) or Syndrome of Inappropriate Antidiuretic Hormone (SIADH) if patient has normal TFT and plasma cortisol
To assist in defining the abnormality a sodium clearance calculation can be provided by the laboratory by sending a timed sample of urine (e.g. 6/12/ 24 hours) in a plain bottle along with a plasma sample. This must be sent to the pathology department with a request for a Lolinogram profile.
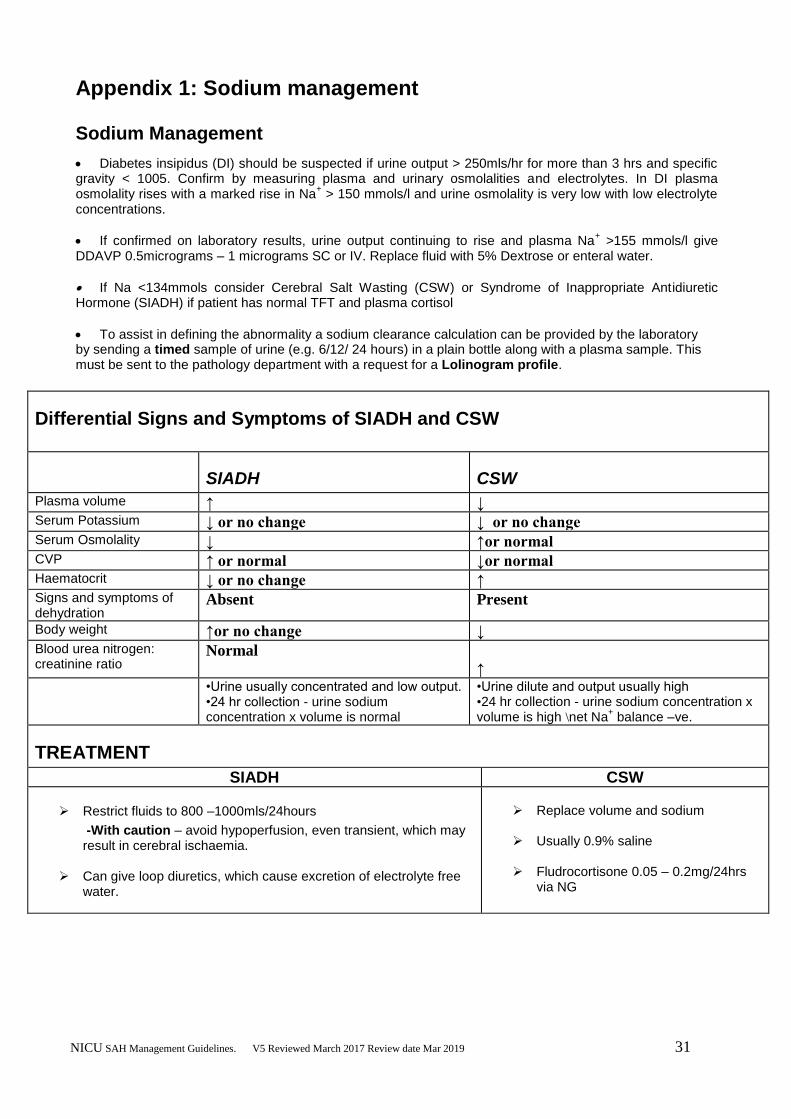
Differential Signs and Symptoms of SIADH and CSW
SIADH CSW
Plasma volume ↑ ↓ Serum Potassium ↓ or no change ↓ or no change Serum Osmolality ↓ ↑or normal CVP ↑ or normal ↓or normal Haematocrit ↓ or no change ↑ Signs and symptoms of dehydration
Absent Present
Body weight ↑or no change ↓ Blood urea nitrogen: creatinine ratio
Normal
↑ •Urine usually concentrated and low output.
•24 hr collection - urine sodium concentration x volume is normal
•Urine dilute and output usually high •24 hr collection - urine sodium concentration x volume is high \net Na
+ balance –ve.
TREATMENT
SIADH CSW
Restrict fluids to 800 –1000mls/24hours
-With caution – avoid hypoperfusion, even transient, which may result in cerebral ischaemia.
Can give loop diuretics, which cause excretion of electrolyte free
water.
Replace volume and sodium
Usually 0.9% saline
Fludrocortisone 0.05 – 0.2mg/24hrs
via NG
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 32
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 33
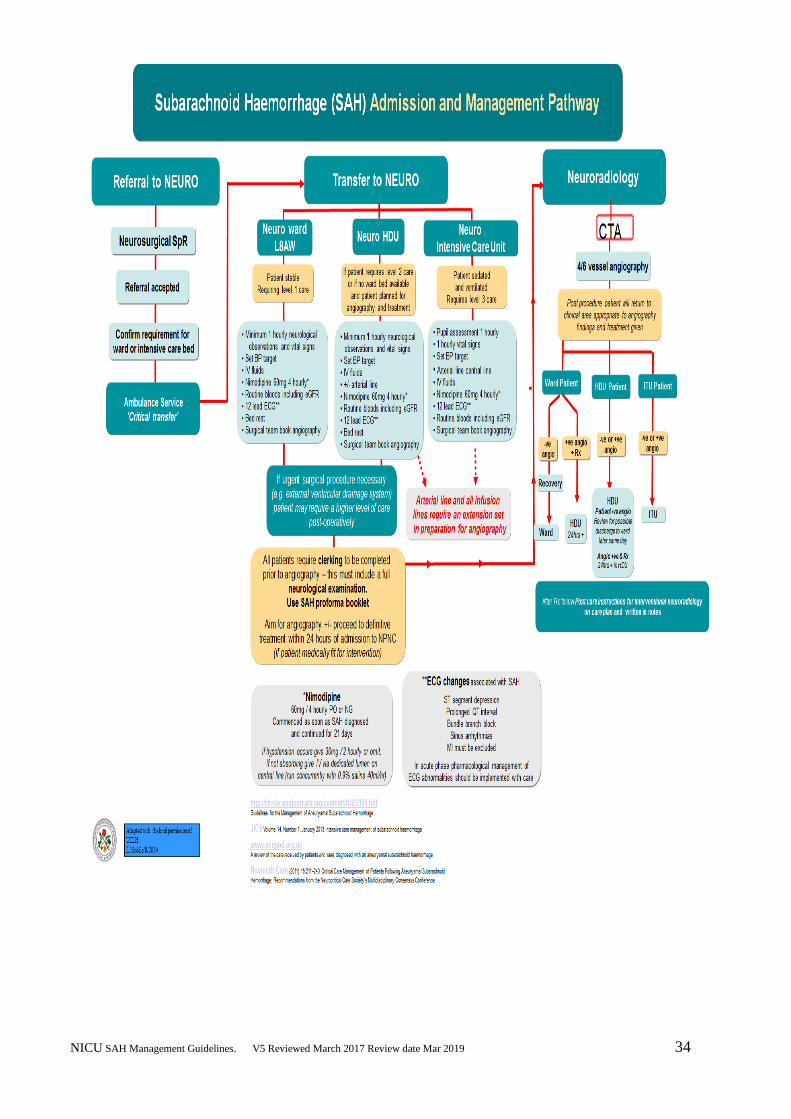
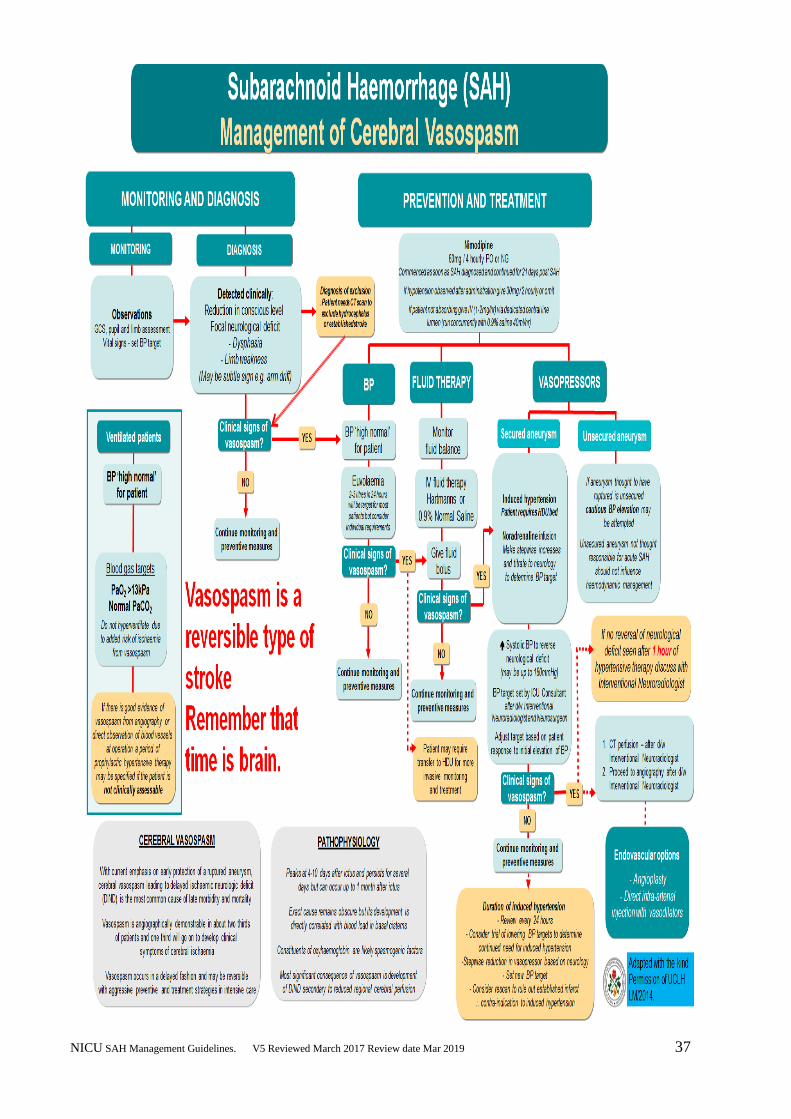
Appendix 2: SAH management and pathways flowcharts
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 34
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 35
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 36
NICU SAH Management Guidelines. V5 Reviewed March 2017 Review date Mar 2019 37