38ournal of Neurology, Neurosurgery, and Psychiatry 1995;59:38-44 Multifocal motor neuropathy with conduction block: a study of 24 patients Pierre Bouche, Antoine Moulonguet, Amena Ben Younes-Chennoufi, David Adams, Nicole Baumann, Vincent Meininger, Jean-Marc Leger, Gerard Said Abstract Twenty four patients with pure motor neuropathy are reported. The chronic motor involvement associated with fascic- ulations and cramps, mainly in the arms, led, in most patients, to an initial diagno- sis of motor neuron disease. In some patients (nine of 24), there was no appre- ciable muscle atrophy. Tendon reflexes were often absent or weak. The finding of persistent multifocal conduction block confined to motor nerve fibres raises questions about the nature and the importance of this syndrome. Segmental reduction of motor conduction velocity occurred at the site of the block, but sig- nificant slowing of motor nerve conduc- tion was not found outside this site. The response to intravenous IVIg treatment seems to be correlated with the absence of amyotrophy. Patients with little or no amyotrophy had an initial and sustained response to IVIg, and did not develop amyotrophy during the follow up study. They could be considered to have a vari- ant of chronic inflammatory demyelin- ating polyneuropathy. Patients with pronounced amyotrophy independent of the disease duration did not respond as well to IVIg treatment, suggesting the existence of a distinct entity. Among the patients treated about two thirds who had an initial good response to IVIg had high or significant antiganglioside GM1 (anti- GM1) antibody titres, but there was no correlation between the high titres before treatment and long lasting response to IVIg treatment. (J Neurol Neurosurg Psychiatry 1995;59:38-44) Keywords: motor neuropathy; conduction block; anti- GM1 antibodies; immunoglobulin treatment Since the description, by Lewis et al in 1982,' of a multifocal chronic sensory-motor periph- eral neuropathy with persistent conduction blocks, pure multifocal motor neuropathy with persistent conduction blocks has been widely reported.2 2 The patients have multi- ple mononeuropathy with purely motor mani- festations. There is asymmetric weakness with various degrees of amyotrophy, cramps, fascic- ulations, and preserved or abolished tendon reflexes. Most patients were initially diag- nosed as having motor neuron disease. In some cases, the presence of a high serum anti- GM1 antibody titre5 10 13 19 and the response to immunosuppressive treatment2' 26 suggested an immunopathological mechanism. This was supported by the fact that anti-GM1 antibod- ies bind at the node of Ranvier,27 and that demyelination occurs at the site of the con- duction block.28 Although some authors20' suggest that mul- tifocal motor neuropathy may be a variant of a chronic inflammatory demyelinating polyneu- ropathy, many questions persist concerning the nature of the underlying process, the nat- ural history, the homogeneity of the syn- drome,'9 3"33 and its response to treatment. We report here the clinical, electrophysiologi- cal, histological, and biological findings and response to treatment in 24 patients with pure multifocal motor neuropathy and persistent conduction block. Patients and methods PATIENTS Most patients were referred with a diagnosis of motor neuron disease, although they lacked signs of upper motor neuron or bulbar involvement. Patients were considered to have multifocal motor neuropathy if they had had progressive weakness in at least one limb for at least six months without sensory loss, and multifocal conduction block in at least two nerves. CLINICAL EXAMINATIONS The patients were assessed using: (a) the Medical Research Council (MRC) rating scale for muscle strength; five muscle groups corresponding to proximal and distal upper and lower limbs were examined and tested according to the MRC scale. (b) A modified Rankin disability scale: 0 = asymptomatic; 1 = non-disabling symptoms that do not interfere with lifestyle; 2 = minor disability symptoms that lead to some restriction to lifestyle, but do not interfere with the patients' capacity to look after themselves; 3 = moderate disability symptoms that significantly interfere with lifestyle or prevent totally independent existence; 4 = moderately severe disability symptoms that clearly prevent independent existence although the patient does not need constant attention day and night; 5 = severely disabled, totally dependent, requiring con- stant attention day and night. ELECTRODIAGNOSTIC STUDIES Electrodiagnostic studies were performed with a Viking Nicolet electromyograph. Hopital de la Salpetriere, Paris, France P Bouche J-M Uger Hopital de Bicetre, le Kremlin-Bicetre, Paris, France A Moulonguet D Adams G Said H6pital de l'Hotel- Dieu de Paris, France V Meininger Unite Inserm 134, h6pital de la Salpetriere, Paris, France A B Younes-Chennoufi N Baumann Correspondence to: Dr Pierre Bouche, Laboratoire d'Explorations Functionelles Neurolo gi e, Hopital de la Salpkerieve, 47-83 Boulevard de l'Hopital, 75651 Paris cedex 13, France. Received 2 November 1995 and in final revised form 16 March 1995. Accepted 16th March 1995 38 on 3 February 2019 by guest. Protected by copyright. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. Downloaded from
Transcript
38ournal of Neurology, Neurosurgery, and Psychiatry 1995;59:38-44
Multifocal motor neuropathy with conductionblock: a study of 24 patients
Pierre Bouche, Antoine Moulonguet, Amena Ben Younes-Chennoufi, David Adams,Nicole Baumann, Vincent Meininger, Jean-Marc Leger, Gerard Said
AbstractTwenty four patients with pure motorneuropathy are reported. The chronicmotor involvement associated with fascic-ulations and cramps, mainly in the arms,led, in most patients, to an initial diagno-sis of motor neuron disease. In somepatients (nine of 24), there was no appre-ciable muscle atrophy. Tendon reflexeswere often absent or weak. The finding ofpersistent multifocal conduction blockconfined to motor nerve fibres raisesquestions about the nature and theimportance of this syndrome. Segmentalreduction of motor conduction velocityoccurred at the site of the block, but sig-nificant slowing of motor nerve conduc-tion was not found outside this site. Theresponse to intravenous IVIg treatmentseems to be correlated with the absenceof amyotrophy. Patients with little or noamyotrophy had an initial and sustainedresponse to IVIg, and did not developamyotrophy during the follow up study.They could be considered to have a vari-ant of chronic inflammatory demyelin-ating polyneuropathy. Patients withpronounced amyotrophy independent ofthe disease duration did not respond aswell to IVIg treatment, suggesting theexistence of a distinct entity. Among thepatients treated about two thirds who hadan initial good response to IVIg had highor significant antiganglioside GM1 (anti-GM1) antibody titres, but there was nocorrelation between the high titres beforetreatment and long lasting response toIVIg treatment.
(J Neurol Neurosurg Psychiatry 1995;59:38-44)
Keywords: motor neuropathy; conduction block; anti-GM1 antibodies; immunoglobulin treatment
Since the description, by Lewis et al in 1982,'of a multifocal chronic sensory-motor periph-eral neuropathy with persistent conductionblocks, pure multifocal motor neuropathywith persistent conduction blocks has beenwidely reported.2 2 The patients have multi-ple mononeuropathy with purely motor mani-festations. There is asymmetric weakness withvarious degrees of amyotrophy, cramps, fascic-ulations, and preserved or abolished tendonreflexes. Most patients were initially diag-nosed as having motor neuron disease. Insome cases, the presence of a high serum anti-
GM1 antibody titre5 10 13 19 and the response toimmunosuppressive treatment2' 26 suggestedan immunopathological mechanism. This wassupported by the fact that anti-GM1 antibod-ies bind at the node of Ranvier,27 and thatdemyelination occurs at the site of the con-duction block.28
Although some authors20' suggest that mul-tifocal motor neuropathy may be a variant of achronic inflammatory demyelinating polyneu-ropathy, many questions persist concerningthe nature of the underlying process, the nat-ural history, the homogeneity of the syn-drome,'9 3"33 and its response to treatment.We report here the clinical, electrophysiologi-cal, histological, and biological findings andresponse to treatment in 24 patients with puremultifocal motor neuropathy and persistentconduction block.
Patients and methodsPATIENTSMost patients were referred with a diagnosisof motor neuron disease, although they lackedsigns of upper motor neuron or bulbarinvolvement. Patients were considered to havemultifocal motor neuropathy if they had hadprogressive weakness in at least one limb forat least six months without sensory loss, andmultifocal conduction block in at least twonerves.
CLINICAL EXAMINATIONSThe patients were assessed using: (a) theMedical Research Council (MRC) ratingscale for muscle strength; five muscle groupscorresponding to proximal and distal upperand lower limbs were examined and testedaccording to the MRC scale. (b) A modifiedRankin disability scale: 0 = asymptomatic;1 = non-disabling symptoms that do notinterfere with lifestyle; 2 = minor disabilitysymptoms that lead to some restriction tolifestyle, but do not interfere with the patients'capacity to look after themselves; 3 = moderatedisability symptoms that significantly interferewith lifestyle or prevent totally independentexistence; 4 = moderately severe disabilitysymptoms that clearly prevent independentexistence although the patient does not needconstant attention day and night; 5 = severelydisabled, totally dependent, requiring con-stant attention day and night.
ELECTRODIAGNOSTIC STUDIES
Electrodiagnostic studies were performedwith a Viking Nicolet electromyograph.
Hopital de laSalpetriere, Paris,FranceP BoucheJ-M UgerHopital de Bicetre, leKremlin-Bicetre,Paris, FranceA MoulonguetD AdamsG SaidH6pital de l'Hotel-Dieu de Paris, FranceV MeiningerUnite Inserm 134,h6pital de laSalpetriere, Paris,FranceA B Younes-ChennoufiN Baumann
Correspondence to:Dr Pierre Bouche,Laboratoire d'ExplorationsFunctionelles Neurologi e,Hopital de la Salpkerieve,47-83 Boulevard del'Hopital, 75651 Pariscedex 13, France.Received 2 November 1995and in final revised form16 March 1995.Accepted 16th March 1995
38
on 3 February 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. D
Needle EMG examination was performed inall patients. The incidence of spontaneousactivity at rest (fibrillation potentials and posi-tive sharp waves) was recorded. The size ofmotor unit potentials (MUPs) and the patternof recruitment during maximal effort werealso analysed.Motor nerve conduction studies were per-
formed with supramaximal percutaneousnerve stimulation, whereas compound muscleaction potentials (CMAPs) were recordedwith surface electrodes. For all patients,median, ulnar, and peroneal nerves wereexamined on both sides. The median nervewas stimulated at the wrist, elbow, axilla, andErb's point. The ulnar nerve was stimulatedat the wrist, below and above the elbow, onthe axilla, and at Erb's point. At Erb's point,the nerve was stimulated with monopolarelectrodes. We did not systematically searchfor conduction block in the radial nerve, asthis was considered unreliable. The peronealnerve was stimulated at the ankle, below andabove the fibular head. For all nerve conduc-tion studies skin temperature was maintainedat 36°C. Distal latencies, conduction velocity,evoked motor response amplitudes (baselineto negative peak), and areas under the nega-tive phase and its duration were measured. Inupper limbs, the nerves were stimulated atfive sites, corresponding to four segments. Nosegments exceeded 25 cm in length. Variationin the proximal/distal amplitude and area ratioand conduction velocity were measured foreach segment. Latencies for F waves weremeasured after distal supramaximal stimula-tion (at least 16 stimuli) in the median, ulnar,and peroneal nerves.
Sensory nerve conduction and amplitudewere measured in the median, ulnar, superfi-cial peroneal, and sural nerves with surfacerecording and stimulating electrodes. Thenerves were stimulated by orthodromic tech-niques in the upper limbs and antidromictechniques in the lower limbs. Amplitudeswere measured peak to peak.To determine if the reduction in amplitude
was due to conduction block, or temporal dis-persion, or both, we analysed the amplitude,
area, and duration of the negative phase of theCMAP elicited from each site of stimulation.Between Erb's point and the axilla, a loss of50% of the CMAP amplitude and area afterproximal stimulation suggested a possible par-tial conduction block. More distally a loss of30% was considered sufficient to confirm theblock. The reduction of CMAP amplitudewas considered to be due to temporal disper-sion if the duration of the CMAP increased bymore than 30% and the corresponding loss ofarea did not exceed 50%. The amplitude andarea changes occurred abruptly over eachnerve segment rather than as gradual lossesalong the length of the nerve.
HISTOLOGICAL EXAMINATIONSMorphological examination of a sensory nerve(radial cutaneous), including teased fibrestudies, was performed in 12 patients underlocal anaesthesia. The nerve specimens werefixed in 3-6% glutaraldehyde. The fragmentswere postfixed in osmium tetroxide. Onenerve fragment was studied by teasing theendoneurial content. Another was embeddedin epon and thionin stained 1 ju thick sectionswere examined.
BIOLOGICAL EXAMINATIONSSerum enzymes and conventional biologicalvariables were assayed. Protein immunoelec-trophoresis was performed and CSF wasexamined. In all cases, the patients were sam-pled before immunosuppressive treatment.Anti-GM1 antibody titres were measured byenzyme linked immunosorbent assay (ELISA)according to two techniques previouslydescribed.'8 34 Table 1 summarises these andthey have been evaluated previously.35 Theresults of the assays were expressed differ-ently. In technique A, serum was consideredto contain anti-GM1 antibodies when, at a1:20 dilution, the optical density (OD) wasmore than 2 SD above the mean obtainedwith 10 internal standards (ODX). The titrewas defined as the reciprocal of the serumdilution required to obtain the ODX. Thus intechnique A, a titre > 20 was considered tobe significant (+ ) and a titre > 100 was con-sidered to be high (+ +). In technique B,serum was considered to contain anti-GM1antibodies when, at a 1:100 dilution, the opti-cal density was three times the mean of thenormal controls at the same dilution. Asreported by Sadiq et al,'7 anti-GM1 antibodieswere found in normal serum up to a 1:400dilution. The titre was considered significant(+) when antibodies were detected at 1:800dilution, and high (+ +) when detected at> 1:3200. In technique B, all positive caseswere confirmed by immunodetection on thinlayer chromatography as described by Maillyet al'6 with serum at a 1:100 dilution. Whenpositivity was not confirmed by thin layerchromatography the sample was considered tobe negative. Controls consisted of patientswith chronic inflammatory demyelinatingpolyneuropathy and normal subjects of thesame age groups.
39 on 3 F
ebruary 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. Dow
Bouche, Moulonguet, Younes-Chennoufi, Adams, Baumann, Meininger, Leger, Said
Table 2 Clinical characteristics
All patients Group 1 Group 2(n = 24) (n = 15) (n = 9)
Sex ratio MJF 20/4 14/1 6/3Age at onset (y) (mean (SD)) 49-8 (9 5) 50 3 (8-8) 47 3 (11 2)Disease duration (y) (mean (SD)) 9 2 (6 3) 12 06 (6-8) 6 7 (2.6)*Limb onset (No of patients):Upper 21 13 8Lower 3 2 1
Cramp (No of cases) 14 9 5Fasciculation (No of cases) 17 11 6Myokymia (No of cases) 2 1 1Tendon reflex (No of cases):
Normal 6 3 3Absent orweak 17 12 5Brisk 1 - 1
Group 1 = patients with amyotrophy; group 2 = patients without amyotrophy.* P < 0 05, group 1 v group 2.
ResultsCLINICAL CHARACTERISTICS (TABLE 2)Twenty four patients, 20 men and fourwomen, were selected on the basis of persis-tent multifocal conduction blocks in motor
fibres. The mean age (SD, range) at onset ofsymptoms was 49-8 (9 5, 32-70) years. Themean duration of the disease was 9-2 (6-3,3-28) years.
Onset occurred in one distal upper limb in21 of 24 patients. In three patients, onset was
unilateral in the lower limbs. There were no
particular circumstances surrounding theonset, except in two patients with proximalpain in an upper limb. Painful cramps were a
usual complaint in 14 of 24 patients. Therewere no sensory symptoms and the motordeficit was isolated. The disease usually had a
very slow progression.When the deficit was fully developed,
upper limb involvement was present in allpatients: motor weakness was distal and uni-lateral in nine patients, distal and bilateral in13, and affected the proximal and distal partsof the limbs in two patients. In the lowerlimbs, motor weakness, when it occurred (in12 cases), was always distal and was unilateralin six cases. The motor deficit thereforeaffected the distal muscles in the median andulnar distribution in the upper limbs,although in one third of patients, the deficitmainly affected the wrist and finger extensorsin a radial distribution. In six patients, themotor deficit was limited to one upper limb,without amyotrophy in five. Overt muscleatrophy was present in 15 of 24 patients andwas usually located at the site of maximalmotor deficit. In nine patients no appreciablemuscle atrophy was found. One of them withradial motor weakness had hypertrophy of theextensor carpi radialis longus and brevis. Asignificant difference in the duration of thedisease occurred in these two categories ofpatients: in patients with amyotrophy themean duration was 12 (SD 6 7) years v 6-6(SD 2-5) years in the non-atrophied group(P = 0 033). In the first group the onset ofamyotrophy always appeared during the firstyear of evolution.
Fasciculations were seen in 17 of 24patients, usually in the involved limb, whereasmyokymia occurred in only two patients. Thetendon reflexes were weak or abolished in the
involved territories in 17 of 24 patients. Theywere brisk without Babinski's sign in only onepatient, who spontaneously improved andwhose deficit was localised in the right distalupper limb.
ELECTROPHYSIOLOGICAL CHARACTERISTICSIn the upper limbs, conduction blocks werefound at proximal sites between Erb's pointand the axilla, at intermediate sites betweenaxilla and elbow, and at distal sites below theelbow. In lower limbs, the conduction blockswere located only below or in the area of thefibular head on the peroneal nerve.Conduction blocks were always found in theupper limbs. In the lower limbs conductionblocks were only found in six patients. Thelocation of conduction blocks was similar inboth nerves and there were no predominantsites in the distribution of the conductionblocks. In all cases, the degree of the conduc-tion block exceeded 50%, which excluded areduction of the CMAP area due to an inter-phase cancellation.37 Motor nerve conductionvelocities were usually normal outside the siteof the blocked segments. Across the blockedsegments, the motor conduction velocity wassometimes greatly reduced. In one patient, apronounced slowing of proximal conductionwithout associated conduction block was ini-tially found, but distal amplitude was verylow. After IVIg treatment, an improvement indistal CMAP amplitude was found and aproximal conduction block could therefore bedemonstrated. Motor distal latencies wereslightly prolonged in most patients: for themedian nerve, 19 of 24 patients had latenciesof more than 3-6 (mean (SD) 4-2 (0 7)) ms;for the ulnar nerve, 15 of 24 patients hadlatencies of more than 3 (mean 3-5 (0 9)) ms;for the peroneal nerve, and 12 of 24 hadlatencies of more than 5 (mean 5-3 (1 1)) ms.
Distal CMAPs were considerably reducedin some blocked nerves, although in otherblocked nerves in the same patient they werenormal. In most patients, the reduction inCMAP amplitude was correlated with thedegree of muscle atrophy. In a few patientshowever, despite some degree of clinical atro-phy, the reduction in CMAP amplitude wasless than expected. In the case of a large reduc-tion in distal CMAP amplitude (less than 1mv), conduction block was mostly difficult todemonstrate. Only one patient had normal Fwave latencies in all nerves. Some patients hadnormal F wave latencies even in the presenceof blocks, but a prolonged or absent F wavelatency was found in at least one of the nervesexamined. In some patients, an F wave wasnot obtained or its latency was prolonged evenin the absence of conduction blocks. In ninecases, an intermediate wave with electrophysio-logical characteristics of an axonal reflex wasfound in the upper limbs: in the median nervein four patients, in the ulnar nerve in threepatients and in both nerves in two patients.
Sensory potential was usually normal orslightly altered: in the median nerve, it wasbelow 15,v in eight of 21 patients (mean23-5 (SD 17-1) ,pv); in the ulnar nerve, it was
40 on 3 F
ebruary 2019 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. Dow
Group 1 = patients with amyotrophy; group 2 = patients without amyotrophy.
below 10 ,uv in nine of 21 patients (mean 12-2(SD 7-9) ,uv); in peroneal nerve it was below10 pv in five of 22 patients (mean 17-6 (SD1 1-7) puv).Needle EMG showed fibrillation potentials
in distal muscles in five of 20 patients in theupper limbs and in six of 24 patients in thelower limbs. The interference pattern wasreduced but no giant units were detected.
LABORATORY EXAMINATIONS (TABLE 3)The CSF was examined in 19 of 24 patients,and was normal in all. Serum immunoelec-trophoresis was performed in 23 of 24patients; no monoclonal peaks were found. Apolyclonal profile was found in five patients(three IgM, two IgG), one patient hadhypogammaglobulinaemia. The other biologi-cal variables were normal.
ANTI-GM1 ANTIBODIESTable 3 summarises anti-GM1 antibodytitres. All the significant or high antibodytitres were of the IgM class. In one patient,
anti-GM1 antibodies were not titred withtechnique B. When examined with techniqueA, 10 of 24 patients (42%) and eight of 23(35%) with technique B had high titres. Withtechnique A seven of 24 (29%) and with tech-nique B four of 23 (17%) had significanttitres. Thus with technique A, 17 of 24 (71 %)of the patients and with technique B 12 of 23(52%) had significant or high antibody titres.Assayed by technique A, 17-5% normal sub-jects had low levels of anti-GM1 antibodies.By technique B, they were excluded as thetitres were always below or equal to 1:400.18With both techniques, 13% of patients withCIDP without conduction blocks had low butsignificant anti-GMI antibody titres.
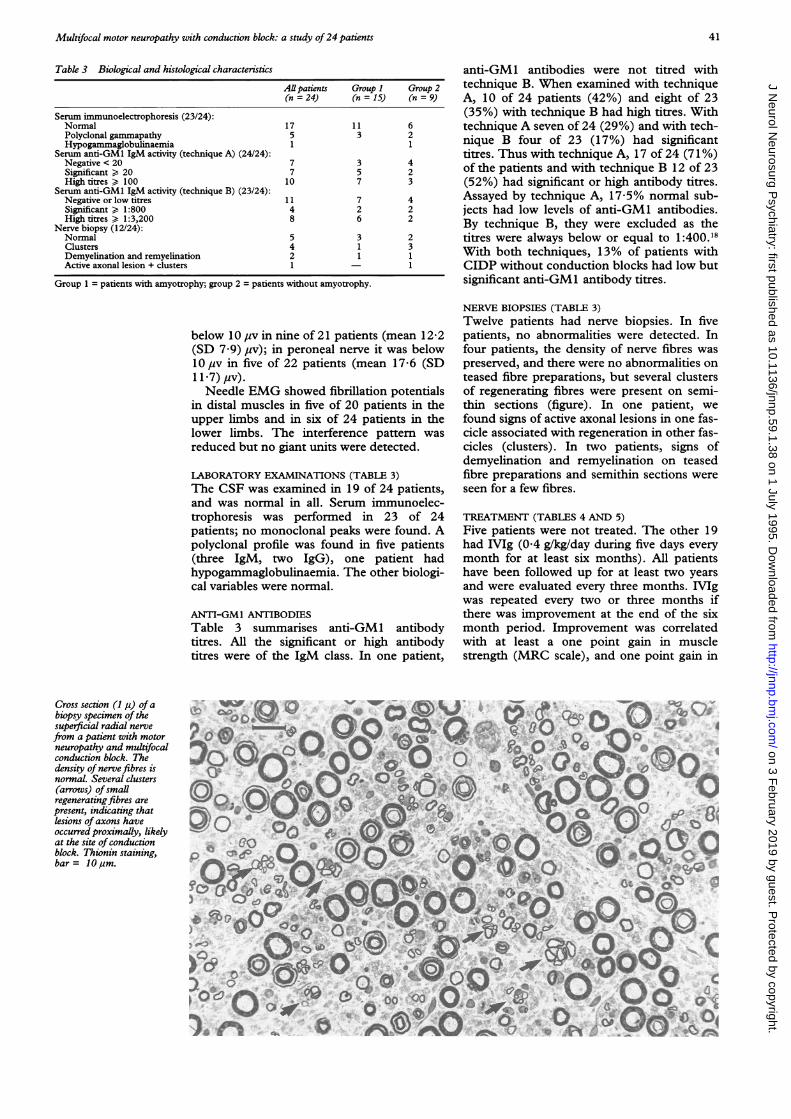
NERVE BIOPSIES (TABLE 3)Twelve patients had nerve biopsies. In fivepatients, no abnormalities were detected. Infour patients, the density of nerve fibres waspreserved, and there were no abnormalities onteased fibre preparations, but several clustersof regenerating fibres were present on semi-thin sections (figure). In one patient, wefound signs of active axonal lesions in one fas-cicle associated with regeneration in other fas-cicles (clusters). In two patients, signs ofdemyelination and remyelination on teasedfibre preparations and semithin sections wereseen for a few fibres.
TREATMENT (TABLES 4 AND 5)Five patients were not treated. The other 19had IVIg (0.4 g/kg/day during five days everymonth for at least six months). All patientshave been followed up for at least two yearsand were evaluated every three months. IVIgwas repeated every two or three months ifthere was improvement at the end of the sixmonth period. Improvement was correlatedwith at least a one point gain in musclestrength (MRC scale), and one point gain in
Cross section (1 p) ofabiopsy specimen of thesuperficial radial nervefrom a patient with motorneuropathy and multifocalconduction block. Thedensity of nervefibres isnormal. Several clusters(arrows) of smallregeneratingfibres arepresent, indicating thatlesions of axons haveoccurred proximally, likelyat the site of conductionblock. Thionin staining,bar = 10lm.
41
on 3 February 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. D
Group 1 = patients with amyotrophy; group 2 = patients without amyotrophy; transient = tran-sient response to IVIg lasting no longer than six months; sustained = response to IVIg lastinglonger than six months; follow up study = follow-up study after six months (mean duration =three years).
the score of the functional activity scale. Twopatients showed no response to IVIg, but onewas recently stabilised by an immunosuppres-sive drug (azathioprine). Six patients had avery good initial and sustained response thatstarted after the first infusion. Five of themwho had no muscle atrophy, had a one to twopoint gain on the MRC scale and two pointsor more on the functional activity scale, whichpersisted after six months. They were essen-tially those with radial involvement. Some ofthem totally recovered their wrist extension.The last one, with muscle atrophy, had a twopoint gain on the functional activity scale.The others (11 patients) had a good initialresponse that did not last more than sixmonths. Most patients showed a dramaticchange in their daily living due to improvedhand skill only during the first IVIg treat-ments, although the MRC scale did not showsignificant variation. Ten of the 11 patientswith a transient response to IVIg treatmenthad pronounced distal upper limb amyotro-phy. In the group of patients who had longterm improvement, repetition of the treat-ment did not have the same response.Nevertheless, motor weakness remained bet-ter than their original state. Of the 19 treatedpatients who had significant or high anti-GM1 antibodies (13 (68%) with technique Aand 11 (58%) with technique B) were associ-
ated with an initial good response to IVIg.Four patients with technique A and five withtechnique B with an initially good clinicalresponse had low or negative values (one ofthe 17 patients who initially responded toIVIg was not titred with technique B). One ofthe patients who did not respond to the IVIgtreatment had no anti-GM1 antibodies withboth techniques, and the other had significanttitres with technique A only. Of the fivepatients who were not treated, one improvedspontaneously and had negative titres. Amongthe four others, who all stabilised, three hadhigh or significant titres with technique A andone with technique B. Of the 19 treatedpatients, during the follow up study siximproved, four had high or significant titreswith technique A and five with technique B.Twelve stabilised, nine had high or significanttitres with technique A and six with techniqueB. Therefore, of the 18 patients who stabilisedor improved with IVIg treatment, 13 (72%)had high or significant titres with technique Aor technique B. The patient who worsenedhad high titres with technique A.
DiscussionWe have studied 24 patients with a pure
motor syndrome resulting from persistentmultifocal conduction blocks. Some patientshad minor sensory symptoms, such as shoul-der pain or slight distal paraesthesiae, butnone had sensory loss. Tendon reflexes were
normal, decreased, or abolished in all cases
but one. There were no signs of upper motorneuron involvement or bulbar signs. In most,onset was in the distal upper limbs, usuallyasymmetrically. Upper limbs were alwaysaffected. Onset was always insidious, althoughin two patients it was preceded by proximalpain in the upper limbs. The syndrome usu-
ally progressed over several years. In some
patients there was a clear multifocal patternaffecting several limbs, primarily distally. Inothers, the distribution was more confined toone limb, mimicking the motor involvementseen at the onset of motor neuron disease.The pattern of muscle wasting varied. In somepatients it was pronounced, whereas in others
Table 5 Response to treatment in relation to the titre of anti-GM1 activity
High titres Significant titres
All patients Technique A Technique B Technique A Technique Bn =24 n =24 n =23 n =24 n =23
Treatment:None 5 1 1 2Intravenous IVIg 19 9 7 5 4
Response to IVIg treatment (19/24):Absent 2 - - 1 -
Transient = transient response to IVIg lasting no longer than six months; sustained = response to IVIg lasting longer than sixmonths; follow-up study = follow-up study after six months (mean duration = three years).
42
on 3 February 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. D
Multifocal motor neuropathy with conduction block: a study of24 patients
it was absent, even after five years of evolu-tion. It was, therefore, possible to distinguishtwo groups of patients according to the pres-ence or absence of muscle atrophy. The dura-tion of the disease was significantly longer inthe patients with atrophy, although the amy-otrophy did not depend on the duration. Theamyotrophy was always present during thefirst year of the disease. Cramps and fascicula-tions were present in most patients, mainly atthe onset of the symptoms.Motor involvement usually interfered with
daily living, but in most cases, less thanexpected from the intensity of the motordeficit and wasting. Patients did not have thesame pattern of evolution: most, after an ini-tial worsening, were stable, and motorinvolvement did not show the progressionusually found in motor neuron disease. A fewpatients progressively worsened. One patientimproved spontaneously.
Conduction blocks were found constantlyin the upper limbs in all patients. These wereusually multifocal with no site predominance,although in three patients who presented withmonomelic upper limb involvement, conduc-tion blocks were located proximally. In somecases, conduction blocks occurred withoutcorresponding clinical motor deficit in thenerve territory, although in most of thepatients there was a good correlation betweenconduction block and motor deficit.A segmental reduction of motor nerve con-
duction velocity was found at the sites ofblocks, contrasting, in proximal blocks, withnormal or slightly reduced distal velocities,except in one case. It is difficult, however, tointerpret the importance of the conductionfailure because the type and size of fibres inwhich conduction velocity was measured werenot the same. Conduction velocities through,and distal to, the site of block cannot there-fore be compared.F waves were altered in most of the nerves
with conduction blocks, as already reported.9Abnormal F waves in the absence of conduc-tion blocks suggest more proximal involve-ment. In these patients, spinal cervicalstimulation is thought to be helpful,9 but notin the six patients in whom it was performedin our series. In patients with motor neurondisease, F waves are never altered to the samedegree.'8 Altogether, alteration of F wavesseemed to be a reliable electrophysiologicalvariable in this type of neuropathy.
Multifocal motor neuropathies are there-fore in almost all cases associated with con-duction blocks and segmental reduction ofconduction velocity. In some cases, slowing ofsegmental conduction may precede the detec-tion of a conduction block, as in one of ourcases. It is more than likely that patients withmultifocal motor neuropathy with segmentalconduction slowing can be grouped togetherwith patients with persistent conductionblock.
In some patients an intermediate lateresponse was found, which was considered tobe an axon reflex.39 This response is neverfound in motor neuron disease, but occurs
occasionally in patients with multifocal motorneuropathy and persistent conduction block.2
In some patients, we found a slight alter-ation of the SNAPs in the nerves tested, withor without motor conduction block, despitenormal clinical examination of the differentsensory modalities.Minor abnormalities on biopsy specimens
of the superficial radial nerve showed that sen-sory fibres were not completely spared. Butthese abnormalities were not predictive forresponse to immunosuppressive treatment aswas reported by Sahenk et al.40 In a few cases,subclinical involvement of sensory nerves wasdetected by electrophysiological examination.The slight electrophysiological abnormalitiesof SNAPs and the moderate morphologicalmodifications of the radial cutaneous nerve insome patients could indicate that there is acontinuum between purely motor neu-ropathies with conduction block and the sen-sory-motor neuropathies with conductionblock of the type reported by Lewis et al.'Abnormal sensory potentials have also beendescribed in motor neuron disease.4' 42We found high titres of anti-GM1 antibod-
ies in 42% of patients with technique A and35% with technique B and in none of the con-trol groups with CIDP or normal controls,confirming the specificity of high titres of anti-GM1 antibodies in this group.'443 When usingtechnique A and technique B, respectively29% and 48% of the patients examined hadno significant or detectable titres of anti-GM1antibodies. It is known, however, that otherautoantibodies can be found in this pathologyand these should be assayed. In a previousstudy, Ben Younes-Chennoufi et al'8 foundIgM reactivity against other glycolipids. Thepatients without anti-GMI antibodies never-theless had the typical clinical and electro-physiological features of multifocal motorneuropathy. Low concentrations of anti-GM1antibodies, which are non-specific, can beencountered in other neurological diseasessuch as amyotrophic lateral sclerosis andstroke as well as in normal controls.'6-'9303444Zielasek et al,35 who evaluated those tech-niques and others, only found discrepanciesfor negative or low titres. The fact that thereare natural antibodies with low titres in nor-mal controls, however, does not negate theeffect of high titres in autoimmune diseases.45
All but five patients were treated by IVIg.Most of them improved initially, althoughonly one third seemed to show a lastingresponse. Only one patient with amyotrophywho had an initial good response to IVIgtreatment had a sustained response. Theabsence of amyotrophy therefore seemed topredict a good and prolonged response toIVIg treatment. The patients without amy-otrophy, in our experience, did not developmuscle wasting during follow up. This findingseems to justify the separation of patients intotwo groups.Among the patients treated, about two
thirds with an initial good response to IVIg,whatever the subsequent responses, had highor significant anti-GM1 antibody titres, but
43
on 3 February 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. D
Bouche, Moulonguet, Younes-Chennoufi, Adams, Baumann, Meininger, Leger, Said
less than half of the patients had high titres.Only 50% of the patients with an initial goodand sustained response had high titres. A cor-relation between the presence of high titres ofanti-GMI antibodies and the long lastingresponse to IVIg cannot therefore be con-firmed, but no follow up study of the anti-GM1 antibody titre in relation to the patient'sresponse was performed.
CONCLUSIONTwo patterns of clinical presentation could beisolated-namely, patients with motor deficitwithout pronounced muscle wasting, with agood response to IVIg suggesting a demyeli-nating lesion on a motor nerve leading to aconduction block; and those with pronouncedamyotrophy mimicking a spinal muscularatrophy with a predilection for upper limbs,and a lesser sensitivity to IVIg treatment. Thehomogeneity of the syndrome of multifocalmotor neuropathy with persistent conductionblocks and underlying physiopathologicalmechanism is therefore uncertain. Althoughthere was no obvious correlation between thelong lasting response to IVIg treatment andthe presence of high anti-GMI antibodytitres, further studies should be performed todetect antiglycolipid antibodies to other com-ponents of the nodes of Ranvier, and to evalu-ate the utility of the titres of these antibodiesin determining the clinical response.
1 Lewis RA, Sumner AJ, Brown MJ, Asbury AK. Multifocaldemyelinating neuropathy with persistent conductionblock. Neurology 1982;32:958-64.
2 Roth G, Rohr J, Magistris MR, Ochsner F. Motor neu-ropathy with proximal multifocal persistent conductionblock, fasciculations and myokymia. Evolution totetraplegia. Eur Neurol 1986;25:416-23.
3 Roth G, Magistris MR. Neuropathies with prolonged con-duction block, single and grouped fasciculations, local-ized limb myokymia. Electroencephalogr Clin Neurophysiol1987;67:428-38.
4 Parry GJ, Clarke S. Multifocal acquired demyelinatingneuropathy masquerading as motor neuron disease.Muscle Nerve 1988;11:103-7.
5 Pestronk A, Cornblath DR, Ilyas AA, Baba H, et al. Atreatable multifocal motor neuropathy with antibodies toGM1 ganglioside. Ann Neurol 1988;24:73-8.
6 Auer RN, Bell RB, Lee MA. Neuropathy with onion bulbformations and pure motor manifestations. Can .7 NeurolSci1989;16:194-7.
7 Van den Bergh P, Logician EL, Kelly JJ. Motor neuropa-thy with multifocal conduction blocks. Muscle Nerve1989;11:26-31.
8 Krarup C, Stewart JD, Sumner AJ, Pestronk A, LiptonSA. A syndrome of asymmetric limb weakness withmotor conduction block. Neurology 1990;40: 118-27.
9 Lange DJ, Trojaborg W, Latov N, et al. Multifocal motorneuropathy with conduction block: Is it a distinct clinicalentity? Neurology 1992;42:497-505.
10 Adams D, Kuntzer T, Steck AJ, Lobrinus A, Janzer RC,Regli F. Motor conduction block and high titres of anti-GM1 ganglioside antibodies: pathological evidence of amotor neuropathy in a patient with lower motor neuronsyndrome. I Neurol Neurosurg Psychiatry 1993;56:982-7.
11 Lange DJ, Trojaborg W, McDonald TD, Blake DM.Persistent and transient "conduction block" in motorneuron diseases. Muscle Nerve 1993;16:896-903.
13 Freddo L, Yu RK, Latov N, et al. Gangliosides GM1andGDlb are antigens for IgM M-protein in a patient withmotor neuron disease. Neurology 1986;36:454-8.
14 Latov N, Hays AP, Donofrio PD, et al. Monoclonal IgMwith unique specificity to gangliosides GM1 and GDlband to lacto-N-tetraose associated with human motorneuron disease. Neurology 1988;38:763-8.
15 Nardelli E, Steck AJ, Barkas T, Schluep M, Jerusalem F.Motor neuron syndrome and monoclonal IgM with anti-body activity against gangliosides GM1 and GDlb. AnnNeurol 1988;23:524-8.
16 Nobile-Orazio E, Carpo M, Legname G, Meucci N,Sonnino S, Scarlato G. Anti-GMI IgM antibodies inmotor neuron disease and neuropathy. Neurology 1990;40:1747-50.
17 Sadiq SA, Thomas FP, Kilidireas K, et al. The spectrum ofneurologic disease associated with anti-GMI antibodies.Neurology 1990;40: 1067-72.
18 Ben Younes-Chennoufi A, Meininger V, Leger JM,Bouche P, Jauberteau MO, Baumann N.Antiganglioside antibodies in motor neuron diseases andperipheral neuropathies: study by ELISA technique andimmunodetection on thin-layer chromatography.Neurochemistry International 1992;20:353-7.
19 Apostolski S, Latov N. Clinical syndromes associated withanti-GMI antibodies. Sem in Neurology 1993;13:264-8.
20 Feldman EL, Bromberg MB, Albers JW, Pestronk A.Immunosuppressive treatment in multifocal motor neu-ropathy. Ann Neurol 1991;30:397-401.
22 Chaudhry V, Corse AM, Cornblath DR, et al. Multifocalmotor neuropathy: response to human immune globulin.Ann Neurol 1993;33:237-42.
23 Cruz Martinez A, Arpa J, Lara M. Electrophysiologicalimprovement after intravenous immunoglobulin inmotor neuropathy with multifocal conduction block. .7Neurol Neurosurg Psychiatry 1993;56: 1236-7.
24 Nobile-Orazio E, Meucci N, Barbieri S, Carpo M,Scarlato G. High-dose intravenous immunoglobulintherapy in multifocal motor neuropathy. Neurology 1993;43:537-44.
25 Tsai CP, Lin KP, Liao KK, et al. Immunosuppressivetreatment in lower motor neuron syndrome with autoan-tibodies against GM1 ganglioside. Eur Neurol 1993;33:446-9.
26 Tan E, Lynn J, Amato AA, Kissel JT, et al. Immuno-suppressive treatment of motor neuron syndromes. ArchNeurol 1994;51:194-200.
27 Santoro M, Thomas FP, Fink ME, et al. IgM deposits atnodes of Ranvier in a patient with amyotrophic lateralsclerosis, anti-GM1 antibodies, and multifocal motorconduction block. Ann Neurol 1990;28:373-7.
28 Kaji R, Oka N, Tsuji T, et al. Pathological findings at thesite of conduction block in multifocal motor neuropathy.Ann Neurol 1993;33:152-8.
29 Krendel DA, Costigan DA. Multifocal motor neuropathyor CIDP? Ann Neurol 1993;34:750.
30 Steck AJ, Adams D. Motor neuron syndromes and mono-clonal IgM antibodies to gangliosides. In: Roland LP,ed. Advances in neurology. Vol 56: amyotrophic lateralsclerosis and other motor neuron diseases. New York: RavenPress, 1991:421-5.
31 Sumner AJ. Separating motor neuron diseases from puremotor neuropathies. Multifocal motor neuropathy withpersistent conduction block. In: Roland LP, ed.Advances in neurology. Vol 56: amyotrophic lateral sclerosisand other motor neuron diseases. New York: Raven Press,1991:399-403.
32 Parry GJ, Sumner AJ. Multifocal motor neuropathy. In:Dyck PJ, ed. Penipheral neuropathy: new concepts and treat-ments. Neurologic clinics, Philadelphia: WB SaundersCo, 1992:671-84.
33 Serratrice G. Neuropathies motrices avec anticorpsantiglycolipides. La Presse Medicale 1993;22:705-7.
34 Adams D, Kuntzer T, Burger D, etal. Predictive value ofanti-GM1 ganglioside antibodies in neuromuscular dis-eases: a study of 180 sera. I Neuroimmunol 1991;32:223-30.
36 Mailly P, Ben Younes-Chennoufi A, Bon S. The mono-clonal antibodies Elec-39, HNK-1 and NC-1 recognizecommon structures in the nervous system and musclesof vertebrates. Neurochemistry International 1989;15:517-30.
37 Rhee EK, England JD, Sumner AJ. A computer simulationof conduction block: effects produced by actual blockversus interphase cancellation. Ann Neurol 1990;28:146-56.
38 Comblath DR, Kuncl RW, Mellits ED, et al. Nerve con-duction studies in amyotrophic lateral sclerosis. MuscleNerve 1992;15:1111-5.
39 Magistris MR, Roth G. Motor axon reflex and indirectdouble discharge: ephaptic transmission? A reappraisal.Electroencephalogr Clin Neurophysiol 1992;85: 124-30.
40 Sahenk Z, Tan E, Kissel JT, Lynn J, Barohn RJ, MendellJR. Immunosuppressive treatment in motor neuron syn-dromes: sural nerve biopsy findings. Neurology 1993;43(suppl 4):258.
41 Shefner JM, Tyler HR, Krarup C. Abnormalities in thesensory action potential in patients with amyotrophic lat-eral sclerosis. Muscle Nerve 199 1;14:1242-5.
42 Mondelli M, Rossi A, Passero S, Guazzi GC. Involvementof peripheral sensory fibers in amyotrophic lateral sclero-sis: electrophysiological study of 64 cases. Muscle Nerve1993;16.:166-72.
43 Pestronk A. Motor neuropathies, motor neuron disorders,and antiglycolipid antibodies. Muscle Nerve 1991;14:927-36.
44 Lamb NL, Patten BM. Clinical correlations of anti-GMIantibodies in amyotrophic lateral sclerosis and neu-ropathies. Muscle Nerve 199 1;14:1021-7.
45 Avrameas S, Ternynck T. The natural autoantibodies sys-tem: between hypotheses and facts. Mol Immunol 1993;30:1133-42.
44
on 3 February 2019 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.59.1.38 on 1 July 1995. D