Obstetrica }i Ginecologia 41 Obstetrica }i Ginecologia LXVI (2018) 41-45 Case Report CORESPONDENCE:Cristina Capatina, e-mail:crisitna.capatina@yahoo.com KEY WORDS: hyperandrogenism; hyperestrogenism; postmenopausal woman; complications; thecoma. MULTIPLE COMPLICATIONS OF SEVERE HYPERANDROGENISM IN A POSTMENOPAUSAL WOMAN Cristina Capatina*,** Alexandru Scafa-Udriste*, Adela Ghinea **, Anda Dumitrascu**, Catalina Poiana*,** * “Carol Davila” University of medicine and pharmacy, Bucharest, Romania ** “C.I.Parhon » National Institute of Endocrinology and Metabolism, Bucharest, Romania Abstract Introduction. Severe hyperandrogenism in postmenopausal women has frequently a neoplastic etiology and is associated with an increased risk of cardiovascular, respiratory, metabolic complications as well as with higher risk of endometrial or breast cancer. Case report. An obese 68 years-old diabetic woman with a recent history of severe arterial hypertension, cardiogenic pulmonary edema, respiratory failure, worsening of glycemic values was referred to our department due to the severely androgenic phenotype. The clinical examination showed android obesity, very severe male- pattern alopecia, important hirsutism, coarse voice. The cardiological examination revealed severe, resistant arterial hypertension with hypertrophic cardiomyopathy and congestive heart failure. Severe chronic respiratory failure and obstructive sleep apnea syndrome were also present. The patient had extremely elevated serum testosterone level, hyperestrogenism, normal serum levels of the adrenal androgens. Computed tomography of the abdomen revealed a tumoral mass in the right ovary and markedly increased uterine volume and endometrial hyperplasia. Surgery was performed and revealed a benign ovarian thecoma with no suspicious endometrial findings. Significant clinical improvement was noted as early as one month after surgery. Conclusions. The presence of severe hyperandrogenism in a postmenopausal women should prompt the search for an androgen-secreting tumor and can be associated with important complications. Rezumat: Multiple complicaţii ale hiperandrogenismului sever la o femeie postmenopauză Introducere. Hiperandrogenismul sever la femeile postmenopauză are frecvent o etiologie neoplazică şi se asociază cu creşterea riscului de complicaţii cardiovasculare, respiratorii şi metabolice precum şi cu un risc crescut de cancer endometrial sau mamar. Prezentarea cazului. O femeie în vârstă de 68 de ani, cu obezitate şi diabet zaharat, cu istoric recent de hipertensiune arterială severă, edem pulmonar cardiogenic, insuficienţă respiratorie, agravarea hiperglicemiei a fost evaluate în clinica noastră pentru fenotipul hiperandrogenic sever. La examenul clinic s-au evidenţiat obezitate android, alopecie foarte severă cu pattern masculin, hirsutism important, voce îngroşată. La examenul cardiologic s-a diagnosticat hipertensiune arterial severă, rezistentă cu cardiomiopatie hipertrofică şi insuficienţă cardiacă. Pacienta prezenta de asemenea insuficienţă respiratorie cronică severă şi sindrom de apnee de somn obstructivă. Valorile testosteronului şi estradiolului seric u fost foarte crescute, androgenii adrenali în limite normale. Examenul computer tomografic al abdomenului a evidenţiat formaţiune tumorală de ovar drept şi hiperplazie endometrială marcată. S-a recomandat intervenţia chirurgicală, examenul histopatologic a descris tecom ovarian benign, hiperplazie endometrială fără elemente de malignitate. La o lună postoperator pacienta prezenta deja ameliorare semnificativă clinic. Concluzii. Hiperandrogenismul sever la o femeie în postmenopauză poate fi asociat cu complicaţii severe şi trebuie să ducă la căutarea unei posibile tumori secretante de androgeni. Cuvinte cheie: hiperandrogenism; hiperestrogenism; femeie în postmenopauză; complicaţii; tecom.
Transcript
Obstetrica }i Ginecologia 41
Obstetrica }i Ginecologia LXVI (2018) 41-45 Case Report
MULTIPLE COMPLICATIONS OF SEVEREHYPERANDROGENISM IN A POSTMENOPAUSAL WOMAN
Cristina Capatina*,** Alexandru Scafa-Udriste*, Adela Ghinea **, Anda Dumitrascu**, Catalina Poiana*,**
* “Carol Davila” University of medicine and pharmacy, Bucharest, Romania** “C.I.Parhon » National Institute of Endocrinology and Metabolism, Bucharest, Romania
Abstract
Introduction. Severe hyperandrogenism in postmenopausal women has frequently a neoplastic etiologyand is associated with an increased risk of cardiovascular, respiratory, metabolic complications as well as withhigher risk of endometrial or breast cancer.
Case report. An obese 68 years-old diabetic woman with a recent history of severe arterial hypertension,cardiogenic pulmonary edema, respiratory failure, worsening of glycemic values was referred to our departmentdue to the severely androgenic phenotype. The clinical examination showed android obesity, very severe male-pattern alopecia, important hirsutism, coarse voice. The cardiological examination revealed severe, resistantarterial hypertension with hypertrophic cardiomyopathy and congestive heart failure. Severe chronic respiratoryfailure and obstructive sleep apnea syndrome were also present. The patient had extremely elevated serum testosteronelevel, hyperestrogenism, normal serum levels of the adrenal androgens. Computed tomography of the abdomenrevealed a tumoral mass in the right ovary and markedly increased uterine volume and endometrial hyperplasia.Surgery was performed and revealed a benign ovarian thecoma with no suspicious endometrial findings. Significantclinical improvement was noted as early as one month after surgery.
Conclusions. The presence of severe hyperandrogenism in a postmenopausal women should prompt thesearch for an androgen-secreting tumor and can be associated with important complications.
Rezumat: Multiple complicaţii ale hiperandrogenismului sever la o femeie postmenopauză
Introducere. Hiperandrogenismul sever la femeile postmenopauză are frecvent o etiologie neoplazică şi seasociază cu creşterea riscului de complicaţii cardiovasculare, respiratorii şi metabolice precum şi cu un risccrescut de cancer endometrial sau mamar.
Prezentarea cazului. O femeie în vârstă de 68 de ani, cu obezitate şi diabet zaharat, cu istoric recent dehipertensiune arterială severă, edem pulmonar cardiogenic, insuficienţă respiratorie, agravarea hiperglicemiei afost evaluate în clinica noastră pentru fenotipul hiperandrogenic sever. La examenul clinic s-au evidenţiat obezitateandroid, alopecie foarte severă cu pattern masculin, hirsutism important, voce îngroşată. La examenul cardiologics-a diagnosticat hipertensiune arterial severă, rezistentă cu cardiomiopatie hipertrofică şi insuficienţă cardiacă.Pacienta prezenta de asemenea insuficienţă respiratorie cronică severă şi sindrom de apnee de somn obstructivă.Valorile testosteronului şi estradiolului seric u fost foarte crescute, androgenii adrenali în limite normale. Examenulcomputer tomografic al abdomenului a evidenţiat formaţiune tumorală de ovar drept şi hiperplazie endometrialămarcată. S-a recomandat intervenţia chirurgicală, examenul histopatologic a descris tecom ovarian benign,hiperplazie endometrială fără elemente de malignitate. La o lună postoperator pacienta prezenta deja amelioraresemnificativă clinic.
Concluzii. Hiperandrogenismul sever la o femeie în postmenopauză poate fi asociat cu complicaţii severeşi trebuie să ducă la căutarea unei posibile tumori secretante de androgeni.
Cuvinte cheie: hiperandrogenism; hiperestrogenism; femeie în postmenopauză; complicaţii; tecom.
42 Obstetrica }i Ginecologia
Multiple complications of severe hyperandrogenism in a postmenopausal woman
Introduction
Hyperandrogenism is not uncommon inyoung, premenopausal women (most frequentlycaused by polycystic ovary syndrome) but new onsethyperandrogenism is a relatively rare occurrence inpostmenopausal women. In these cases, theinvestigation should necessarily be directed towardan androgen-secreting tumor, especially if serumandrogen concetrations are very high. Severehyperandrogenism is associated with cardiovascular,respiratory and metabolic complications, partlymediated by hyperinsulinism. (1,2) It also increasesthe neoplastic risk (endometrial, breast cancer)because of the secondary hyperestrogenism (resultingfrom the aromatisation of the excessiveandrogens)(3,4)
Case report
We report the case of a 68 years-old womanwith a recent history of severe arterial hypertensionpresenting as cardiogenic pulmonary edema, recent-onset diabetes mellitus, severe respiratory failure andmarked, progressive obesity. She was referred to ourdepartment mainly due to her severely androgenicphenotype (developed during the last 18 monthsbefore admission).
The clinical examination showed androidobesity, severe male-pattern alopecia (see figure nr1), marked hirsutism involving the face but especiallythe trunk, deepening of the voice.
Severe, resistant arterial hypertension withhypertrophic cardiomyopathy and congestive heartfailure was also present. The patient associatedchronic respiratory failure, severe obstructive sleepapnea syndrome, recent-onset diabetes mellitus(maximum blood glucose 211 mg/dl, HbA1c of 6.8%).
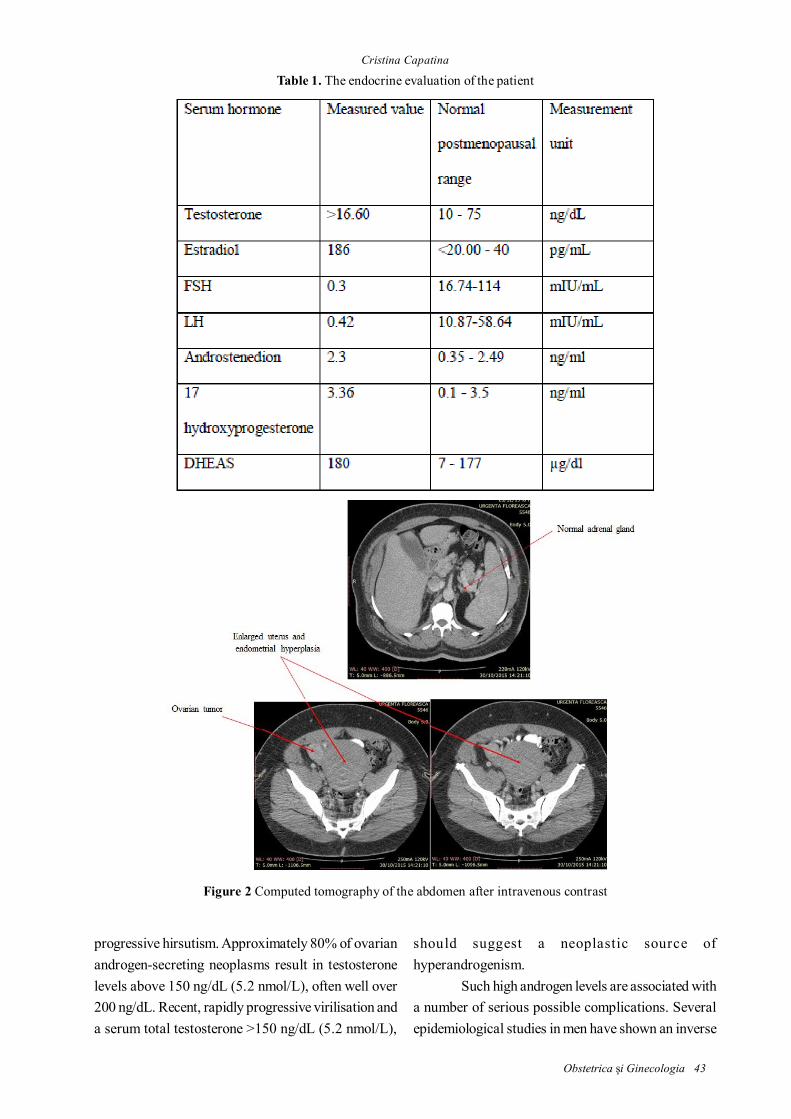
The endocrine evaluation revealed:erythrocytosis, extremely elevated serum testosteronelevel, high serum estradiol- by aromatization ofandrogens, low gonadotropins discordant with thepostmenopausal status - caused by the increase inestradiol and testosterone levels- see table nr. 1,normal adrenal function.
Computed tomography of the abdomenshowed normal adrenal glands, right ovarian tumor,markedly increased uterine volume with severeendometrial hyperplasia-see figure 2.
Surgery was recommended and performed,with significant early clinical improvement. As soonas 3 weeks after surgery the blood pressure andglycemic control improved markedly. Thehistopathological examination revealed a benign sexcord-stromal tumor (thecoma) with no suspiciousendometrial findings.
Discussion
Severe hyperandrogenism in apostmenopausal woman is a relatively rareoccurrence and should raise the suspicion of a tumoralcause. Women with androgen-secreting tumorstypically present with recent-onset, rapidly
Figure 1. Clinical appearance of the patient showing severe signs of androgen excess
Obstetrica }i Ginecologia 43
progressive hirsutism. Approximately 80% of ovarianandrogen-secreting neoplasms result in testosteronelevels above 150 ng/dL (5.2 nmol/L), often well over200 ng/dL. Recent, rapidly progressive virilisation anda serum total testosterone >150 ng/dL (5.2 nmol/L),
should suggest a neoplastic source ofhyperandrogenism.
Such high androgen levels are associated witha number of serious possible complications. Severalepidemiological studies in men have shown an inverse
Figure 2 Computed tomography of the abdomen after intravenous contrast
Table 1. The endocrine evaluation of the patientCristina Capatina
44 Obstetrica }i Ginecologia
relationship between serum testosterone levels andseveral cardiovascular risks factors (eg diabetesmellitus, increased visceral adiposity, insulin resistanceand metabolic syndrome).(5,6) In contrast, in menprimarily diagnosed with obesity and metabolicsyndrome serum testosterone levels are typically lowbut whether this is a cause-effect relationship remainsto be determined. In contrast, in women, elevatedserum androgens levels are positively correlated withobesity and metabolic syndrome.(7) The Women’sIschemia Syndrome Evaluation (WISE) studyrevealed that in postmenopausal womenhyperandrogenism is significantly associated with ahigher incidence of central adiposity and coronaryartery disease than women withouthyperandrogenemia(8). The mechanisms behind thedifferential action of androgens in males and femalesremain unclear.
Granulosa cell tumors and thecomas are moreoften hyperestrogenic, but androgenic cases havebeen reported.(9) Hyperandrogenism of ovarianorigin may be associated with endometrial hyperplasiaand/or carcinoma (10), especially in postmenopausalwomen . (11,12) as a result of increased peripheralestrogen production (aromatisation of androgens).Some postmenopausal women withhyperandrogenism caused by a tumor also experienceuterine bleeding due to peripheral aromatization ofandrogens to estrogens. (13)
In almost all cases with severehyperandrogenism, insulin resistance andhyperinsulinemia are present and women are atincreased risk for type 2 diabetes and cardiovasculardisease . Additional physical findings may includecentral obesity, skin tags, and acanthosis nigricans.
Most women with ovarian hyperandrogenismhave tissue resistance to insulin that is identified byfasting hyperinsulinemia or subnormal insulin-mediated glucose uptake (from euglycemic clampstudies).(14) The molecular basis for the tissueresistance to insulin in these women is not known.Studies in cultured skin fibroblasts suggest thatapproximately 50 percent of them have a defect inphosphorylation of the insulin receptor.(15) Peripheralinsulin resistance likely plays a more important rolein the development of hypertension(16). Increased
cardiovascular risk was implicated in women withhyperandrogenism. Serum testosterone independentlyincreases risk for cardiovascular disease, andcorrelates even with indices of subclinicalatherosclerosis in various populations ofpostmenopausal women.(3)
Conclusions
The presence of severe hyperandrogenismin postmenopausal women is frequently the result ofan androgen-secreting tumor and can be associatedwith important complications.
References
1. Barbieri RL, Hornstein MD. Hyperinsulinemia andovarian hyperandrogenism. Cause and effect. EndocrinolMetab Clin North Am 1988; 17:685-7032. Christakou CD, Diamanti-Kandarakis E. Role ofandrogen excess on metabolic aberrations andcardiovascular risk in women with polycystic ovarysyndrome. Womens Health (Lond) 2008; 4:583-5943. Macut D, Antic IB, Bjekic-Macut J. Cardiovascular riskfactors and events in women with androgen excess. JEndocrinol Invest 2015; 38:295-3014. Secreto G, Sieri S, Agnoli C, Grioni S, Muti P, Zumoff B,Sant M, Meneghini E, Krogh V. A novel approach to breastcancer prevention: reducing excessive ovarian androgenproduction in elderly women. Breast Cancer Res Treat 2016;158:553-5615. Kelly DM, Jones TH. Testosterone and obesity. ObesRev 2015; 16:581-6066. Stanworth RD, Jones TH. Testosterone in obesity,metabolic syndrome and type 2 diabetes. Front Horm Res2009; 37:74-907. Valderhaug TG, Hertel JK, Nordstrand N, Dale PO, HofsoD, Hjelmesaeth J. The association betweenhyperandrogenemia and the metabolic syndrome inmorbidly obese women. Diabetol Metab Syndr 2015; 7:468. Shaw LJ, Bairey Merz CN, Azziz R, Stanczyk FZ, SopkoG, Braunstein GD, Kelsey SF, Kip KE, Cooper-Dehoff RM,Johnson BD, Vaccarino V, Reis SE, Bittner V, HodgsonTK, Rogers W, Pepine CJ. Postmenopausal women with ahistory of irregular menses and elevated androgenmeasurements at high risk for worsening cardiovascularevent-free survival: results from the National Institutes ofHealth—National Heart, Lung, and Blood Institutesponsored Women’s Ischemia Syndrome Evaluation. J ClinEndocrinol Metab 2008; 93:1276-12849. Outwater EK, Wagner BJ, Mannion C, McLarney JK,Kim B. Sex cord-stromal and steroid cell tumors of theovary. Radiographics 1998; 18:1523-154610. Potischman N, Hoover RN, Brinton LA, Siiteri P, DorganJF, Swanson CA, Berman ML, Mortel R, Twiggs LB, Barrett
Multiple complications of severe hyperandrogenism in a postmenopausal woman
Obstetrica }i Ginecologia 45
Cristina Capatina
RJ, Wilbanks GD, Persky V, Lurain JR. Case-control studyof endogenous steroid hormones and endometrial cancer.J Natl Cancer Inst 1996; 88:1127-113511. Barth JH, Jenkins M, Belchetz PE. Ovarianhyperthecosis, diabetes and hirsuties in post-menopausalwomen. Clin Endocrinol (Oxf) 1997; 46:123-12812. Krug E, Berga SL. Postmenopausal hyperthecosis:functional dysregulation of androgenesis in climactericovary. Obstet Gynecol 2002; 99:893-89713. Kaltsas GA, Isidori AM, Kola BP, Skelly RH, Chew SL,Jenkins PJ, Monson JP, Grossman AB, Besser GM. Thevalue of the low-dose dexamethasone suppression test inthe differential diagnosis of hyperandrogenism in women.J Clin Endocrinol Metab 2003; 88:2634-2643
14. Dunaif A, Segal KR, Shelley DR, Green G, DobrjanskyA, Licholai T. Evidence for distinctive and intrinsic defectsin insulin action in polycystic ovary syndrome. Diabetes1992; 41:1257-126615. Dunaif A, Xia J, Book CB, Schenker E, Tang Z.Excessive insulin receptor serine phosphorylation incultured fibroblasts and in skeletal muscle. A potentialmechanism for insulin resistance in the polycystic ovarysyndrome. J Clin Invest 1995; 96:801-81016. Han T, Lan L, Qu R, Xu Q, Jiang R, Na L, Sun C. TemporalRelationship Between Hyperuricemia and InsulinResistance and Its Impact on Future Risk of Hypertension.Hypertension 2017; 70:703-711