29
MULTIPLE SCLEROSIS Xu, Ping Neurologic department of the 1 st affiliated hospital, Z
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | elwin-paul |
| View: | 215 times |
| Download: | 0 times |

MULTIPLE SCLEROSIS
Xu, PingNeurologic department of the 1st affiliated hospital, ZMU

Most common disabling condition in young adults
Most common demyelinating disorderChronic disease of the CNS Progresses to disability in majority of cas
esUnpredictable course variety of signs and symptoms; sometim
es mistaken for psychiatric diagnosis
FACTS

DEFINITION
MS— Chronic inflammatory autoimmune disorderOf white matter Demyelination In the CNS
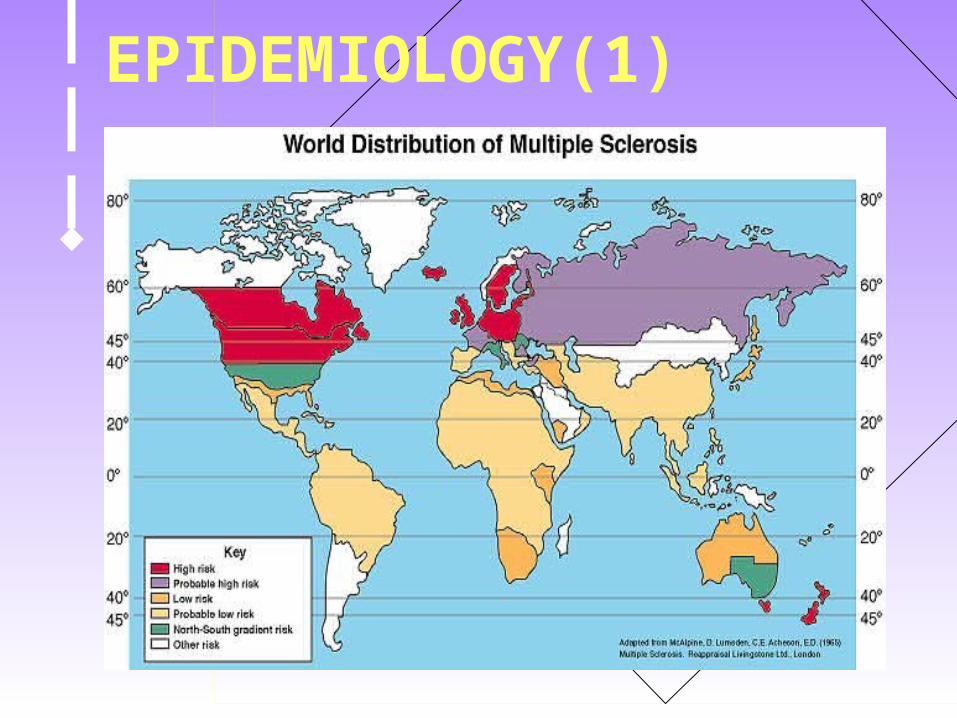
EPIDEMIOLOGY(1)

EPIDEMIOLOGY(2)
Risk is increasing with the latitude
Female dominance (F:M=2:1)
Mainly young adults involved
Peak age 20-40, mostly before 55

ETIOLOGY(1)
Still unknown!

ETIOLOGY(2)
Multifactory: Autoimmune(myelin antibody)
Genetics---no clear-cut pattern of inheritance
20 fold increased familial incidence
Infection---raised titres of many common
viruses(HSV) in CSF and serum
no virus-induced animal MS model

PATHOLOGY(2)Perivascular inflammation and demyeli
nationPlaques occur anywhere in the CNS
Most frequent: Periventricular region of the brain Optic nerve Brainstem Cerebellum Spinal cord

PATHOLOGY(3)
M ultiple---- Multifocal Multi-temporal Relapse-remitting progress S clerosis----plaques

Degenerative changes in myelinInfiltration with macrophages or microgliaPreservation of axonsDegree of oligodendrocyte preservation determines remyelination potential Slower conduction time along affected nerve
PATHOLOGY(4)


CLINICAL FEATURESInducement:infection, fatigue, delivery a baby…Initial symptoms:
Impaired vision Disequilibrium 平衡失调Heat intolerance 热耐受不良Problems with bladder controlSensory disturbance Motor weakness
Initial symptoms indicate the site of onset

SENSORY DISTURBANCES
Ascending numbness starting in feet
Bilateral hand numbness Hemiparesthesia/dysesthesia 感觉迟钝
Dorsal column signs 脊髓Loss of vibration/proprioception 本体感受
Lhermitte’s sign

VISION DISTURBANCE
Unilateral or bilateral partial/complete internuclear ophthalmoplegia 眼肌麻痹
Optic neuritis

Weakness
(mono-, hemi- or quadriparesis)
Increased spasticity
Pathologic signs
(Babinski, Chaddock, Hoffman)
Dysarthria( 构音不良 )
MOTOR DISTURBANCE

Urinary incontinence, 尿失禁
incomplete emptying
Cognitive and emotional abnormalities (depression, anxiety, emotional lability)
Fatigue
Sexual dysfunction
OTHER SYMPTOMS

INVESTIGATIONS
CSF (Oligoclonal bands)
Evoked potentials(VEP,BREP,SSEP)
MRIBlood and urine(non-specific)

MRI
Most useful tool in diagnosis MRI is abnormal in 90% of definite MSGadolinium enhancement identifies acti
ve lesions
Lesions abutting central ventricles, with diameter of >0.6 cm,in the posterior fossa, help to diagnose MS

MRI—cerebellum

MRI—optic nerve

MRI—cerebral hemisphere

Diagnostic criteria
Clinical definite MS (CDMS): ① two times of attack and two lesions; ② two attacks, one lesion and one subclinical evidence;
Laboratory supported definite MS (LSDMS): ① Two attacks, one subclinical evidence and CSF /OB/IgG; ② One attack, two lesions and CSF OB/IgG ; ③ One attack , one lesion, one subclinical evidence and CSF OB/IgG;

Diagnostic criteria
Clinical probable MS (CPMS): ① two attacks, one lesion ; ② one attack, two lesions ; ③ one attack, one lesion and other subclinical evidence;
Laboratory supported probable MS (LSPMS) ① Two attacks ; CSF OB/IgG; ② Two attacks involving different part of CNS, intermission at lest one month ; each attack must continue for 24hs.
Treatment--acute
Immunotherapy with steroids or ACTHSuppress inflammatory responseDecrease severity/duration of exacerbationsInhibit demyelinating processIV (3-5 days), then oral taper
Other immunomodulators (imuran, 硫唑嘌呤 cytoxan, methotrexate)

Treatment— relapse prevention
Interferon 1-beta (Betaseron) Interferon 1-alpha (Avonex)Useful for relapsing-remitting , not for
progressive type Significant side effects (nephrotoxicity,
leukopenia)
Prognosis
EXTREMELY VARIABLE
50% chance of walking unaided 15 years after onset of disease
Estimated longevity 25-35 years after diagnosis
Common causes of death: secondary complications of immobility; depression (suicide)

Thank you!



















