Cynthia Webner www.cardionursing.com 1 Multisystem Issues in Critical Care Presented by: Cynthia Webner DNP, ACNPC-AG, CCNS, CCRN- CMC, CHFN 1 2016 Patient-centered care definition: “Providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions.” - Institute of Medicine - Crossing the Quality Chasm, 2001 3
• Flexible visitation decreases patient anxiety, confusion, and agitation
• Reduces cardiovascular complications
• Decreases length of ICU stay,
• Makes the patient feel more secure
• Increases patient satisfaction
• Increases quality and safety 5
Cynthia Webner www.cardionursing.com 3
Consider:
• Flexible visitation
• Meet with family daily
• Learn to work while being observed by visitors
• Unit rooms should be built with family in mind
Nurse Barriers:
• Continue to resist open visitation
• Fear consequences
• Fail to understand the importance of families
• See presence at the bedside as a privilege not a necessity that is important to patient care 6
• Facilitate unrestricted access to patient chosen support person(s)
• Ensure an approved written practice document regarding support person(s) ability to remain at the bedside as desires
• Assure policies are not discriminatory
• Policies to include provision of visitation limitations for those infringing on rights of others, safety of others, health of patient
7
Cynthia Webner www.cardionursing.com 4
• Family should be given the option to be at the bedside
• All units should have policy/procedure in place regarding family presence during CPR
• Support person observing resuscitation of loved one had less:– PTSD symptoms
– Depressive episodes
– Complicated grief
8
• Engage in care
• Actively involve family in care
• Address questions and concerns
• Facilitate communication
• Incorporate cultural and spiritual needs
• Family participation in rounds
• Ways family can help– Speak softly
– Re-orient patient
– Talk about family and friends and the past
– Remember glasses, hearing aids
– Help with mobilization
– Document ICU stay with a diary• ↓ incidence of PTSD after
ICU by > 60%
9
Cynthia Webner www.cardionursing.com 5
• Provide permission to speak up
• Create a safe environment to speak openly
• Create culture that supports questioning what staff is doing
• Three key areas:
– Shared decision making
– Safety
– Future care expectations
10
• Do WITH – not FOR or TO
• Requires full disclosure of patient status
• Requires regular meetings
• Staff needs:– Good communication skills
– Meeting facilitation skills
– Conflict management skills
• Families recognize uncertainty exists but expects honesty
11
Cynthia Webner www.cardionursing.com 6
• Control symptoms
• Improve quality of life
• Prevent hospitalization
• Prevent mortality
• Advance care measures
• Experimental surgery or drugs
• Palliative care and hospice
12
End of Life Decision Making
• Palliative Care versus Hospice
–When should they be involved
–Never to early to get them involved
• Make an assessment – Help patient and family understand the
trajectory of the disease process
• Have the discussion
13
Cynthia Webner www.cardionursing.com 7
14
Components of Effective Shared Decision Making:
• Establishing trust
• Identifying patient values, preferences, and goals for care early in the course of treatment
• Using the framework “Ask-Tell-Ask” to determine both what patients know and what they want to know
• Understanding the reasons why there are conflicts regarding decisions of care
• Using numeric data in a clear and understandable way as a decision aid
• Respecting that patient’s may change their goals as the disease progresses
Allen, 2012. 15
Cynthia Webner www.cardionursing.com 8
Palliative Care
• An approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual. (World Health Organization)
• Focuses on providing patients with relief from the symptoms and stress of a serious illness. The goal is to improve quality of life for both the patient and the family.
16
Palliative Care
• Provides relief from pain and other distressing symptoms;
• Affirms life and regards dying as a normal process;
• Intends neither to hasten or postpone death;
• Integrates the psychological and spiritual aspects of patient care;
• Offers a support system to help patients live as actively as possible until death;
• Offers a support system to help the family cope during the patients illness and in their own bereavement;
• Uses a team approach to address the needs of patients and their families, including bereavement counseling, if indicated;
• Will enhance quality of life, and may also positively influence the course of illness;
• Applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications.
• Can help decide when end of life care is appropriate17
Cynthia Webner www.cardionursing.com 9
Hospice Care
• Care provided to patients with a life expectancy of six months or less.
• No longer seeking a cure• Aims to make remaining time as comfortable and as
meaningful as possible. • Relief of pain.• Emotional support (for patient and family) and help
with everyday tasks.• Goal: Ensure every moment counts, in the last six
months of life. • Medicare / insurance benefit with covered services
18
CLABSI
• 30,100 Central line-associated bloodstream infections annually
• 15,000 preventable CLABSIs still occurred in intensive care units in 2010
• Use of a Central Catheter Maintenance Bundle in Long-Term Acute Care Hospitals. American Journal of Critical Care, 25(2), 165-172. Grigonis, A. M., Dawson, A. M., Burkett, M., Dylag, A., Sears, M., Helber, B., & Snyder, L. K. (2016).
• 14 Point Bundle adapted from CDC bundle of care• Decreased CLABSI from 1.28/1000 to .98/1000 days in
14 months
19
Cynthia Webner www.cardionursing.com 10
CLABSI
• A trained central catheter team of nurses who follow the regimented bundle protocol
• Competency testing before being certified for the team
• Education on the bundle protocol
• Knowledge assessments on the evidence-based practices of central catheter maintenance
• Documented daily review of the necessity of the central catheter and checklists
• Hand hygiene and aseptic technique
• Gloved dressing changes
20
CLABSI
• Sterile gauze or sterile, transparent, semipermeable dressing
• Replacement of transparent dressing at least every 7 days • Gauze dressing if patient is diaphoretic or if site is bleeding
or oozing, replaced every 48 hours • Catheter site assessed every shift for redness, tenderness,
pain, or exudate • Alcohol-based central catheter caps • Change of dressing if compromised, loose, or damp • Application of a chlorhexidine-impregnated sponge
dressing
21
Cynthia Webner www.cardionursing.com 11
CAUTI
• 15-25% of Hospitalized patients have catheter• Most common type of healthcare-associated
infection– Estimated > 560,000 nosocomial UTIs annually– Attributable to 13,000 deaths annually– Extends LOS 2-4 days– Increases cost : $0.4-0.5 billion / year nationally
• Source of microorganisms– Meatal, rectal, vaginal– Contaminated hands of health care personnel
22
CAUTI
Modifiable Risk Factors
• Prolonged catheterization
• Disconnection of drainage system
• Lower professional training of inserter
Other Risks
• Female
• Older age
• Impaired immunity
• Placement of catheter outside the OR
• Incontinence
• Diabetes
• Renal Dysfunction
23
Cynthia Webner www.cardionursing.com 12
CAUTI
• Insert catheters for appropriate indications– Acute urinary retention or bladder outlet obstruction– Need for accurate measurement of urinary output in
critically ill patients– Perioperatively in some surgeries– To assist in healing of open sacral or perineal wounds
in incontinent patients– Patients with prolonged immobilization– To improve comfort in end of life care
• Implement quality program to enhance appropriate use of catheters
24
CAUTI
• Insert catheters using aseptic technique and sterile equipment– Hand hygeine– Sterile setting– Properly secure catheter
• Maintain a closed drainage system– If disconnection, leakage or
breaks in aseptic technique or sterile system – replace all
– Obtain urine samples aseptically
• Maintain unobstructed urine flow– Keep system free from
kinking– Keep collection bag below
level of bladder– Empty bag regularly
• Ensure spigot does not contact nonsterile container
• Leave catheter in place only as long as needed– Post op - remove within 24
hours
25
Cynthia Webner www.cardionursing.com 13
Rhabdomyolysis
• Syndrome caused by injury to skeletal muscle and involves leakage of large quantities of potentially toxic intracellular contents into plasma
• Myoglobin: Myocyte compound released into plasma
• After muscle injury– Massive plasma myoglobin levels exceed protein
binding of haptoglobin– Precipitates in the glomerular filtrate– Excessive myoglobin can cause renal tubular
obstruction, intrarenal vasoconstriction and AKI
26
Rhabdomyolysis
Signs and Symptoms
• Myalgias
• Generalized weakness
• Darkened urine
• Less common– Fever
– Nausea
– Vomiting
Causes
• Alcohol use and resultant unresponsiveness
• Illicit drug use
• Use of prescribed medications
• Heatstroke
• Infection
• Trauma
• Metabolic disorders
• Inflammatory myopathies
27
Cynthia Webner www.cardionursing.com 14
Physical Exam
• Muscular pain and tenderness
• Decreased muscle strength
• Soft tissue swelling
• Skin changes consistent with pressure necrosis
• Hyperthermia, hypothermia, and electrical injuries
• Creatine kinase – Most reliable and sensitive indicator of muscle injury– Failure to decrease suggest ongoing muscle injury– Levels 5 times normal suggest rhabdomyolysis (suspect at 2-3
times normal)– Draw every 6-12 hours until peak level is established
• Urine myoglobin– Urine dipstick test positive for blood but there is an absence of
red blood cells. 29
Cynthia Webner www.cardionursing.com 15
• Ensure adequate hydration– Isotonic solution at a rate 400ml/hour (up to
1000ml/hour)
– Titrate to maintain urine output of 200ml/hour
• Monitor urine output – foley
• Correct cause
• Monitor for compartment syndrome– Areas with severe focal muscle tenderness
– Fasciotomy needed if compartment pressure is sustained in excess of 25-30 mm HG
Rhabdomyolysis - Treatment
30
• 40-50% will develop AKI• Predictors of potentially renal failure include the following:
– Peak CK level higher than 6000 IU/L– Dehydration (hematocrit >50, serum sodium level >150 mEq/L,
orthostasis, pulmonary wedge pressure < 5 mm Hg, urinary fractional excretion of sodium < 1%)
– Sepsis– Hyperkalemia or hyperphosphatemia on admission– Hypoalbuminemia
• Might treat with urine alkalization– 0.9% NaCl with sodium bicarbonate at 100ml/h– Maintain urine pH > 6.5-7.0
• Dialysis may be required if develop oliguric renal failure
Rhabdomyolysis -AKI
31
Cynthia Webner www.cardionursing.com 16
32
Shock
• Definition:
– The condition of insufficient perfusion of cells and vital organs causing tissue hypoxia (inadequate oxygen to the tissue)
– Perfusion is inadequate to sustain life
– Results in cellular, metabolic and hemodynamic derangements
33
Cynthia Webner www.cardionursing.com 17
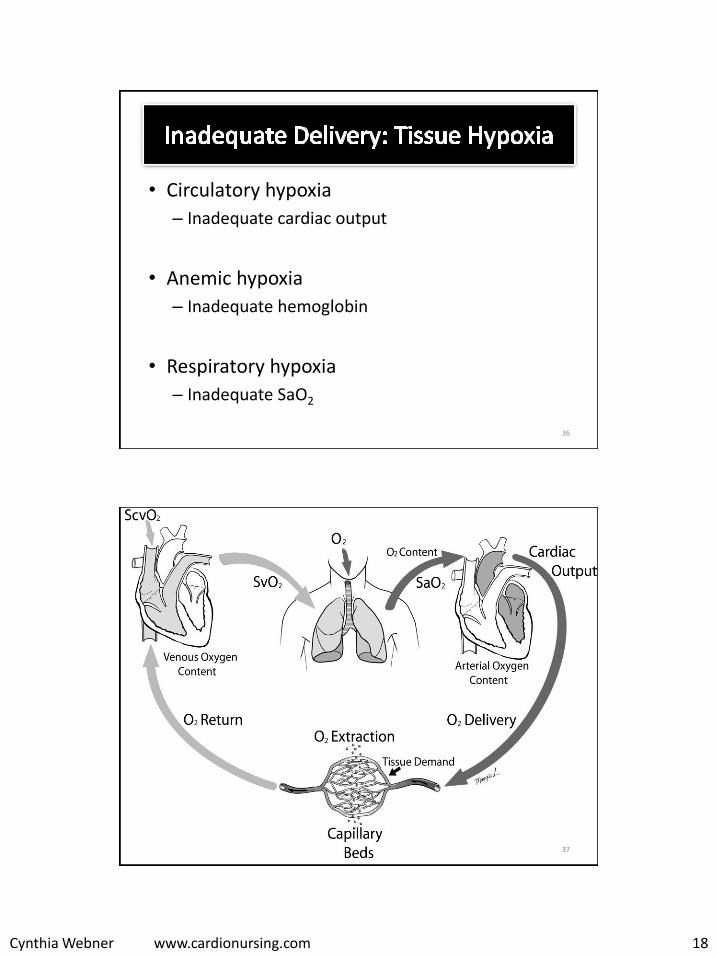
Oxygen Delivery to Tissues
34
• Oxygen delivery measured as DO2:
Volume of oxygen delivered to tissues each minute
• DO2= cardiac output x arterial oxygen content (hemoglobin x arterial oxygen saturation)
35
Cynthia Webner www.cardionursing.com 18
• Circulatory hypoxia
– Inadequate cardiac output
• Anemic hypoxia
– Inadequate hemoglobin
• Respiratory hypoxia
– Inadequate SaO2
36
37
Cynthia Webner www.cardionursing.com 19
• DO2 formula = CO x Hgb x SaO2 x 13.4 (constant)
• Normal DO2 = 900- 1100 ml/min
(1000)
• Normal DO2I = 550 – 650 ml/min
38
• Oxygen delivery can be improved by increasing cardiac output, hemoglobin or SaO2
39
Cynthia Webner www.cardionursing.com 20
• Measured as VO2
• Volume of oxygen consumed by the tissues each minute
• Determined by comparing oxygen content in arterial blood to the oxygen content in mixed venous blood– Normal CaO2 is 20 ml/dl and normal CVO2 is 15 ml/dl
• Normal VO2: 200 – 300 ml / min (250 ml / min)
40
• Fever per 1 degree C
• Shivering
• Suctioning
• Sepsis
• Non Family Visitor
• Position Change
• Sling Scale Weight
• Bath
• CXR
• Multi Organ Failure
• 10%
• 50-100%
• 7-70%
• 5-10%
• 22%
• 31%
• 36%
• 23%
• 25%
• 20-80%
41
Cynthia Webner www.cardionursing.com 21
• Measured by mixed venous oxygen saturation (SVO2)
• Normal 60-80% (75%)
• Tissues were delivered 1000 ml / min (DO2)
• Tissues uses 250 ml / min (VO2)
• This leaves a 75% reserve in venous blood
• Oxygen Extraction Ratio (O2ER) = 25%
42
• Oxygen delivery and oxygen consumption are independent until a critical point of oxygen delivery is reached
• Tissues will extract the amount of oxygen needed independent of delivery because delivery exceeds need
43
Cynthia Webner www.cardionursing.com 22
DO2
VO2 (extraction is
independent of delivery)
SVO2(SV02 will improve when you increase
delivery)
44
1000 cc 250 cc (25%) 75%
750 cc 250 cc (33%) 67%
500 cc 250 cc (50%) 50%
• When oxygen delivery reaches a critical level then consumption will depend on delivery
• SVO2 will not increase with increased delivery while you are in this dependent state
• Anaerobic metabolism occurs here because you have an oxygen deficit
45
Cynthia Webner www.cardionursing.com 23
46
• SVO2 < 60% – Decreased delivery
– Increased consumption
• SVO2 > 80%– Increased delivery
– Decreased demand
– Sepsis (tissues cannot extract)
– Wedged catheter
• Clinically significant change is +or – 5 to 10% over 3 to 5 minutes
• SVO2 < 40%
– Represents limits of compensation
– Lactic acidosis will occur
• Oxygen demand is greater than oxygen delivery and reserve can be depleted = oxygen debt
47
Cynthia Webner www.cardionursing.com 24
• CENTRAL venous oxygenation saturation• Reflects oxygen saturation of blood returning to
right atrium from– Superior vena cava.
• Can be obtained without a pulmonary artery catheter– Modified central venous catheter with fiberoptic
technology.
• Normal value is > 70%.– Values normally a bit higher than SVO2
– Trends the same as SVO2
48
49
• Due to decrease in delivery of oxygen to tissues
– Misdistribution of oxygen to tissues
– System attempts to provide oxygen to vital organs
– Decreased oxygen extraction in some areas
• Elevated lactate levels
– Oxygen consumption is no longer independent of oxygen delivery
• Key parameter in treating sepsis
– Marker of hypoperfusion
Cynthia Webner www.cardionursing.com 25
50
The condition of insufficient perfusion of cells and vital
organs causing tissue hypoxia
DO2= Cardiac Output x Hemoglobin x Arterial Oxygen
Saturation
The Body Knows the Algorithm
• When perfusion to the tissues decrease for whatever reason the body launches a response
• The body begins to adjust to improve cardiac output
• Two primary responses
– Sympathetic nervous system
– Renin angiotensin aldosterone system
51
Cynthia Webner www.cardionursing.com 26
Signs and Symptoms of Shock Stages
• Sub clinical Hypoperfusion
• CI 2.2-2.5 – No clinical indications of
hypoperfusion yet something seems different or not right
• Compensatory with SNS Stimulation
• CI 2.0 – 2.2 – Tachycardia
– Narrowed pulse pressure
– Tachypnea
– Cool Skin
– Oliguria
– Decreased Bowel sounds
– Restlessness / confusion
52
Signs and Symptoms of Shock Stages
• Shock: Progressive with hypoperfusion (CI < 2.0)– Dysrhythmias – Hypotension – Tachypnea – Cold, clammy skin – Anuria – Absent bowel sounds– Lethargy to coma
• Shock: Refractory with profound hypoperfusion (CI < 1.8) – Life threatening dysrhythmias – Hypotension despite
Treatment Goal: Maximize the delivery of oxygen to the tissue
– Remember: Cardiac Index, Hemoglobin, SaO2
• CI– Volume replacement
• Isotonic crystalloids first (0.9NS or Lactated Ringers)
• Colloids if crystalloids not effective
• Hemoglobin– Replace blood loss if necessary for tissue oxygenation
• Need hemoglobin to carry oxygen
– Treat cause of loss
• SaO2– Oxygen
– Intubation and mechanical ventilation if needed
61
Cynthia Webner www.cardionursing.com 31
Volume Replacement
Crystalloids Colloids Blood
Products
Isotonic- Solution stays in vascular
bed
NS, LR (D5NS, D5LR)
Hypotonic
- Solution moves from
vascular bed to cells
.45NS, (D5.45NS), D5W
Hypertonic - Solution pulls volume from
cells in to the vascular bed
3%NS, TPN
Albumin (costly)
Dextran 70/75
Hetastarch (Hespan)
Whole Blood
Packed red cells
Fresh Frozen
Plasma
62
Crystalloids and Colloids
Isotonic Crystalloids
• Osmolality close to blood osmolality
• Stay in vascular space better than other crystalloids
• Safe, effective and inexpensive; usually first line
Colloids • Large molecule solutions
(either protein or starch)
• Stay in vascular space better than crystalloids
• Support intravascular colloidal oncotic pressure to help pull more fluid into the vascular space
• Consider in hypovolemic shock when crystalloids are not effective
63
Cynthia Webner www.cardionursing.com 32
More About Fluid Replacement
• Hypovolemic and Neurogenic Shock
– Crystalloids and Colloids may be used
– Blood for hemorrhagic
• Septic and Anaphylactic Shock (and early burns) “leaky states” with increased capillary permeability
– Crystalloids only (at least initially)
• Require replacement of 3 cc per 1 cc fluid loss
• Fluid challenge of 250 –500 cc over 5 minutes
• Then: 200cc every 5 minutes until an increase in BP or signs of fluid overload
64
Sepsis / Septic Shock New Definitions
• Sepsis: life-threatening organ dysfunction due to a dysregulated host response to infection (SCCM 2016)– Organ dysfunction can be identified as an acute change in total
SOFA score > 2 points consequent to the infection.
• Septic Shock: a subset of sepsis in which underlying circulatory, cellular, and metabolic abnormalities substantially increases mortality more than with sepsis alone.
• Treatment Goal: Maximize the delivery of oxygen to the tissue Remember: Cardiac Index, Hemoglobin, SaO2
– Prevention – hand hygiene
– Treat the cause • Antibiotics within first 30-60 minutes of presentation (mortality increases after 1st hour)
• Antibiotics should cover all likely organisms (Gram-positive organisms most common)
• Source control: wound debrdement
• CI– Volume replacement
• Crystalloids 4-8 liters
– Vasopressors
– May need inotropes
• Hemoglobin– Transfuse as necessary to support tissue oxygenation
• SaO2– Oxygen
– Intubation and Mechanical Ventilation 69
Cynthia Webner www.cardionursing.com 35
70
Early Goal-Directed Therapy (EGDT)
Attempts to adjust
cardiac preload, afterload and contractility
to balance systemic oxygen delivery
with oxygen demand.
Six hour window
Bundles of Care: Surviving Sepsis Campaign
1st 3 Hours • Measure lactate level
• Obtain blood cultures
• Administer broad spectrum antibiotics
• Administer 30 ml/kg crystalloid if: – Hypotension
– Lactate > 4 mmol/L
1st 6 Hours • Start vasopressor if MAP not >
65 mmHg with initial fluids
• Reassess lactate if initial level elevated
• If persistent hypotension or initial lactate > 4 mmol/L reassess volume status– Physical examination
– CVP or ScVO2
– Cardiac ultrasound
– Dynamic assessment of fluid responsiveness with passive leg raise test
71
Cynthia Webner www.cardionursing.com 36
Goals for Initial 6 Hours of Resuscitation
• Central venous pressure (CVP) 8 to 12 mmHg
• CVP of 12 to 15 mmHg in intubated patients and patients with reduced left ventricular compliance
• MAP > 65 mmHg
• Urine output > 0.5 ml/kg/hr
• Mixed venous oxygen saturation (SVO2) 65% or
• Superior vena cava oxygen saturation (ScVO2) 70%
• Normalization of serum lactate 72
Multiple Organ Dysfunction Syndrome (MODS)
• Clinical syndrome characterized by the development of progressive and potentially irreversible physiologic dysfunction in 2 or more organs or organ systems that is induced by a variety of acute insults including sepsis.
• Process not a single event• Various stages of organ functions from mild to
irreversible• Often the clinical continuum of SIRS → sepsis →septic
shock →MODS• Treatment: Treat the shock and offending agent• Mortality with MOD arising from sepsis ranges from
40-75%
73
Cynthia Webner www.cardionursing.com 37
Nonspecific Vasodilatory Shock (Distributive)
• Newer category - Arterial Vasodilation
• May be seen post operative CABG
• Loss of response to catecholamines
• Wide pulse pressure with tachycardia
• Decreased preload, stroke volume secondary to vasodilation
• Treated with IV vasopressin
74
Obstructive Shock
• Obstruction of ventricular filling or obstruction of blood flow through the heart or great vessels resulting in decreased cardiac output– Pulmonary embolus
– Cardiac tamponade
– Pneumothorax
– Dissecting aortic aneurysm
Treatment Focus
• Removing obstruction to flow– Fibrinolytic therapy
√ Decrease preload √ Decrease afterload (think IABP) √ May need to support contractility
√ Fill up container √ Use vasopressors to restore vascular tone √ Treat underlying cause
77
Cynthia Webner www.cardionursing.com 39
Outcome Indicators for Shock States
• Stoke Volume Variation < 15%
• ScVO2 > 70%
• Heart Rate < 90 BPM
• Lactic acid < 2.0 mMOL
• Others: – Mentation
– Urine Output
78
79
Cynthia Webner www.cardionursing.com 40
• 359,400 EMS assessed out-of-hospital cardiac arrests in the US annually (Heart Disease and Stroke Statistics, 2013).
• Approximately 60% of out-of-hospital cardiac deaths are treated by EMS personnel.
• 25% of those EMS-treated out-of-hospital cardiac arrest have no symptoms prior to arrest.
80
• If bystander CPR is not provided, a sudden cardiac arrest victim’s chances of survival fall 7% to 10% for every minute of delay until defibrillation
• The adult survival rate to hospital discharge after EMS treated out-of-hospital cardiac arrest with any first recorded rhythm is 9.8%.
• The survival rate for adults after bystander witnessed VF arrest is 28.4% (57.1% for children).
81
Cynthia Webner www.cardionursing.com 41
82
Immediate Care After ROSC (Return of Spontaneous Circulation)
• Optimize ventilation and oxygenation
– Maintain oxygen saturation >94%
– Do not hyperventilate
• Target PETCO2 of 35-40 mm Hg
• Treat hypotension
• Coronary Reperfusion
– If STEMI or high suspicion of acute MI
• TTM – if does not follow commands
83
Cynthia Webner www.cardionursing.com 42
Coronary Angiography Post Cardiac Arrest
• Coronary angiography should be performed emergently for OHCA patients with suspected cardiac etiology of arrest and ST elevation on the ECG. (COR I, LOE B)
• Emergency coronary angiography is reasonable for select (eg, electrically or hemodynamically unstable) adults who are comatose after OHCA of suspected cardiac origin but without ST elevation on the ECG. (COR IIa,B-NR)
• Coronary angiography is reasonable in post-cardiac arrest patients for whom coronary angiography is indicated, regardless of whether the patient is comatose or awake. (COR IIa, LOE C-LD)
COR: Class of recommendation. LOE: Level of Evidence. B-R: Randomized Studies. B-NR: Non-randomized studies. C-LD: Limited Data. C-EO: Expert Opinion
84
Targeted Temperature Management
• Recommend that comatose (ie, lacking meaningful response to verbal commands) adult patients with ROSC after cardiac arrest should have TTM.
– For VF/VT Out of Hospital Arrest (COR I, LOE B-R)
– For non-VF/VT and in-hospital cardiac arrest (COR IIb, LOE C-EO)
• Recommend selecting and maintaining a constant target temperature between 32°C and 36°C (COR I, LOE B-R)
• It is reasonable that TTM be maintained for at least 24 hours after achieving target temperature (Class IIa, LOE C-EO).
• It may be reasonable to actively prevent fever in comatose patients after TTM (Class IIb, LOE C-LD)
• Routine prehospital cooling of patients with rapid infusion of cold IV fluids after ROSC is not recommended. (COR III: No benefit, LOE A)
COR: Class of recommendation. LOE: Level of Evidence. B-R: Randomized Studies. B-NR: Non-randomized studies. C-LD: Limited Data. C-EO: Expert Opinion
85
Cynthia Webner www.cardionursing.com 43
Circulatory collapse impairs flow of oxygen to the brain Oxygen stores depleted in 20 seconds after loss of
circulation Anaerobic metabolism begins
Glucose and adenosine triphosphate (ATP) dependent cellular pumps are interrupted This results in excessive calcium and glutamate excretion
Leads to hyper-excitability of brain cells and further oxygen debt and cell death Cellular death contributes to the development of cerebral edema.
“No-reflow phenomenon” After ROSC there is a brief period of initial hyperemia
followed by decreased cerebral blood flow due to microvascular dysfunction
86
• Mismatch of cerebral blood flow and amount of O2 required for cerebral metabolism further complicates cerebral metabolism
–Release of excitatory molecules (glutamate and aspartate) from damaged brain cells which increase cerebral metabolic rate
87
Cynthia Webner www.cardionursing.com 44
• Impairs function of energy dependent cellular ionic pump
• Increases intracellular osmolality causing influx of Na+, Cl, Ca++ into the brain
• Cerebral edema, breakdown of lipid membrane and increase in ICP
This increased
metabolism causes a further
mismatch in O2 supply
and demand
88
Key Phases of TTM
• Cooling– Rapid 4-6 hours of arrest– Various methods but none stand out as superior– Target 32-36°C
• Maintenance– 24 hours from achievement of target temperature
• Rewarming– 0.25 to 0.33°C per hour – slower is perceived to be better
• Post rewarming – 48 hours– Avoid hyperthermia
• Neurologic Prognostication– Avoid for minimum of 72 hours post rewarming
• Invasive– Iced lavage–Cooled IV saline (4°C)• Hemodynamically well tolerated, but will not keep temp down• Provides a good “head start” until other methods available
– Intravascular catheter based cooling equipment
90
• Cool environment – turn down heat, turn off lights, calm, quiet and cool.
• Adequately sedate to achieve target temperature
• Large patients take longer to cool
• Neuromuscular blockade is recommended during cooling– Prevents shivering (which interferes with cooling)
– Masks seizures
• Up to 44% have seizures during cooling
• Consider continuous EEG
• Increased IV fluids while cooling – Require higher filling pressures.
91
Cynthia Webner www.cardionursing.com 46
Shivering
• Occurs in approximately 25% of patients (Tomte et al., 2011).
• Shivering occurs as a part of normal thermoregulation. – Decrease in temperature
activates thermoregulatory response of vasoconstriction and shivering
• Increases systemic metabolism.
• Shivering is associated with reduction in brain tissue oxygenation and cerebral blood flow.
Subjective: • Observe for piloerections
(goosebumps)• Bedside Shivering
Assessment Scale – Goal < 1– Palpate pectoralis muscle and
neck and mandible – Humming or vibration is early
sign
Objective • Bispectral index monitoring
(BIS monitoring) • Water temperature of
cooling device92
Bedside Shivering Assessment Scale
Score Assessment
0: No Shivering No detection of shivering on palpation
1: Mild Shivering Localized to neck and / or chest
2: Moderate Shivering Involves arms and neck or chest
3: Severe Shivering Intermittent and generalized involving all 4 extremities.
93
Cynthia Webner www.cardionursing.com 47
Baseline Interventions for Shivering
• Skin counter warming
– Socks
– Head wrap
– Warm packs to hands
Prevention of Shivering During TTM: The Columbia Antishivering Protocol. Choi HA, et al. Neurocrit Care. 2011;14(3):389-394 94
Baseline Interventions for Shivering
• Acetaminophen – 650-1000 mg Q 4-6 h– Lowers the hypothalamic set point
• Magnesium sulfate – 0.5 G/h IV Goal– Increase patient comfort– Decreased time to goal temperature– Causes peripheral vasodilation
Prevention of Shivering During TTM: The Columbia Antishivering Protocol. Choi HA, et al. Neurocrit Care. 2011;14(3):389-394 95
Cynthia Webner www.cardionursing.com 48
Step 1-4 Interventions for Shivering
Step 1 (Mild sedation) • Dexmedetomidine OR opioid • Meperidine
– Lowers shivering threshold – Can also lower seizure
threshold
• Fentanyl – Less antishivering properties
Step 2 (Moderate Sedation) • Dexmedetomidine AND opioid • Dexmedetomidine
– Off label in shivering– Lowers shivering threshold– Monitor for bradycardia and
hypotension
Step 3 (Deep Sedation) • Propofol
– Lowers shivering threshold– Good for seizure activity– Monitor for hypotension
• Step 4 (Neuromuscular Blockade)
Prevention of Shivering During TTM: The Columbia Antishivering Protocol. Choi HA, et al. Neurocrit Care. 2011;14(3):389-394 96
General Considerations
• Neurologic assessment findings invalid – decreased reflexes, muscle tone
• The neurologic findings of either absent motor movements or extensor posturing should not be used alone for predicting a poor neurologic outcome (FPR, 10%; 95% CI, 7%–15% to FPR, 15%; 95% CI, 5%–31%; Class III: Harm, LOE B-NR).
Guidelines
• An EEG for the diagnosis of seizure should be promptly performed and interpreted, and then should be monitored frequently or continuously in comatose patients after ROSC (Class I, LOE C-LD).
• The same anticonvulsant regimens for the treatment of status epilepticus caused by other etiologies may be considered after cardiac arrest (Class IIb, LOE C-LD). 97
Cynthia Webner www.cardionursing.com 49
Cooling
• Bradycardia and ↑ SVR occur as temperature drops
• Bradycardia refractory to atropine
• QT may prolong with bradycardia
• May require BP support– SBP > 90 mm Hg– MAP > 65 mm Hg
• Require higher filling pressures – more IV fluids–Consider CVP 12-14
• LV Function could decrease when cool
Rewarming
• During rewarming, vasodilation may unmask hypovolemia and cause shock
– IVF while polyuric and replete well prior to/during rewarming
98
Look at SvO2 and lactate for signs of shock.
Lactate should decrease in straight lineIf blip, look for acute abdomen, early
sepsis, ischemia, etc.
General Considerations
• Hypoventilation occurs
• ↓ cough reflex
• ↑ airway secretions
• Paralysis of mucociliarymechanisms
• High risk for pneumonia and ARDS
• If hyperventilated
– Cerebral vasoconstriction may further ↓ cerebral blood flow & ↑ cerebral ischemia
–Vasodilation can increase ICP
Guidelines
• Maintain PaCo2 within a normal physiological range, taking into account any temperature correction (Class IIb, LOE B-NR).
• It is reasonable to use the highest available oxygen concentration until the arterial oxyhemoglobin saturation or the partial pressure of arterial oxygen can be measured (Class IIa, LOE C-EO).
• Titrate the Fio2 and maintain oxyhemoglobin saturation to maintain at > 94% (Class IIa, LOE C-LD). 99
Cynthia Webner www.cardionursing.com 50
• Gastrointestinal–Hypomotility while cold
–↓ hepatic metabolism
–↓ insulin resistance from the pancreas
–Stress ulceration
–Ileus
• Tube feedings
• GI prophylaxis
• Follow LFT’s/amylase if suspect pancreatitis
100
• Renal–Impaired renal tubular transport causing ↓ in Na+ &
H2O reabsorption–↓ anti-diuretic hormone response• Massive diuresis during cooling• Must match fluid volume
–Fluid shift from vascular compartment to interstitial spaces
• Follow electrolytes closely (K, Mg, Phos)– Will be low during cooling / maintenance – Correct to low normal
101
Cynthia Webner www.cardionursing.com 51
• Anticipate during rewarming
–Prior to rewarming, correct an elevated K to normal
• If elevated K and/or acute kidney injury
– Normalize before rewarming
–May need hemodialysis
102
• Hematologic–Shift to the left• ↓ O2 delivery to tissues
–↑ blood viscosity–Coagulopathy caused
by inhibition of enzyme reactions to coagulation cascade and splenic sequestration of platelets
• Coagulopathies or the need for systemic anticoagulation is not a contraindication to TTM– Only active, uncontrolled
bleeding• Correct coagulopathies only if
bleeding• If TTM has begun and patient
is bleeding– Correct coagulopathies
and platelet abnormalities– target to 35°C (36°C ) to
minimize impact on platelet and coagulation factors – correct temp slowly
103
Cynthia Webner www.cardionursing.com 52
• ↓ basal metabolic rate
•↓ tissue perfusion–Good skin care
• Altered drug metabolism
–Watch closely for drug accumulation
–Dose paralytics based on Train of Four
–May need decreased drug doses if cleared hepatically
• Treat hyperglycemia with insulin drip per ICU Protocols
• BS increases with cooling
• BS decreases with rewarming
• Watch glucose closely during rewarming, may drop fast
– Consider decreasing or stopping drip prior to rewarming
104
• Hypervigilence for infection
– Signs may be masked
– Inspect lines/tubes, skin, routine CXR
• Low threshold for early antibiotics
105
Cynthia Webner www.cardionursing.com 53
Seen in hypothermia with temperatures < 32°C. Also seen in
hypercalcemia, brain injury, vasopsastic angina, or VF
106
107
Cynthia Webner www.cardionursing.com 54
108
• Initiate rewarming 24 hours after target temperature achieved.
• Prior to rewarming – Assess volume status
– Assess hemodynamics
– Hold all potassium containing medications immediately before and during rewarming if potassium level is > 3.5 mEq/L. - will increase during rewarming
– If potassium is > 4.5 mEq/L cautiously consider rewarming – some suggest waiting until < 4.0
– Assess blood sugar – will drop during rewarming 109
Cynthia Webner www.cardionursing.com 55
110
Post Rewarming Temperature Management
• Administer acetaminophen
• Reinstitute cooling blanket / device
• Iced saline
111
Cynthia Webner www.cardionursing.com 56
Neurologic Prognostication
• No neurologic prognostication for minimum of 72 hours after rewarming has been achieve.
• The absence of pupillary reflex to light at 72 hours or more after cardiac arrest is useful to predict poor neurologic outcome in comatose patients treated with TTM.
• The findings of either absent motor movements or extensor posturing should not be used alone for predicting a poor neurologic outcome.
• The presence of myoclonus, which is distinct from status myoclonus, should not be used to predict poor neurologic outcomes.
112
Other Considerations
• Family
• Clergy Support
• Organ Donation
113
Cynthia Webner www.cardionursing.com 57
Outcomes
• 5445 Cardiac Arrest• 2823 (51.8%) had ROSC • 1081 (19.9%) Survived to Discharge• 816 (15.5%) discharged neurologically intact• Of the cooled (C) vs. non-cooled (NC)patients
with ROSC and not demonstrating purposeful movement– Did not survive to discharge 63% (C) vs 81% (NC)– Discharged neurologically impaired 6% (C ) vs 5% (NC)– Discharged neurologically intact 30% (C) vs 14% (NC)
PATH Data Base – Penn Alliance for Therapeutic Hypothermia Summer 2016114