21
MYASTHENIA GRAVIS SARA SEALS AND RYAN PHILLIPS IMMUNOLOGY Picture taken from http:// naturalcureproducts.wordpress.com/tag/myasthenia-gravis-cure
| Date post: | 18-Dec-2015 |
| Category: |
Documents |
| Upload: | logan-webb |
| View: | 241 times |
| Download: | 2 times |

MYASTHENIA GRAVIS
SARA SEALS AND RYAN PHILLIPS
IMMUNOLOGY
Picture taken from http://naturalcureproducts.wordpress.com/tag/myasthenia-gravis-cure
SYMPTOMS AND ANALYSISSymptoms
Ptosis
Diplopia1
Muscle weakness
Myasthenic crisis
Dysphonia2
Thymoma/thymic hyperplasia
Analysis
Electrodiagnostic testing
Presence of Anti-AChR Ab
Edrophonium challenge2
Picture taken from http://naturalcureproducts.wordpress.com/tag/myasthenia-gravis-cure/

EPIDEMIOLOGY
Most common NMJ disease3
Up to 150 per million
Prevalence has been increasing1
Mid- to late adulthood
Incidence increases with age3
Prevalence in women4
Rarely inheritable3
Picture from http://mgakc.org/newly-diagnosed/sample-page/ocular-mg

RISK FACTORS AND TRIGGERS
Risk Factors
Possible genetic factors
HLA B8, DRw3, and DQw22
Down-regulation of miR320a3
Triggers
Infections3
Stress
Sometimes drug-induced4
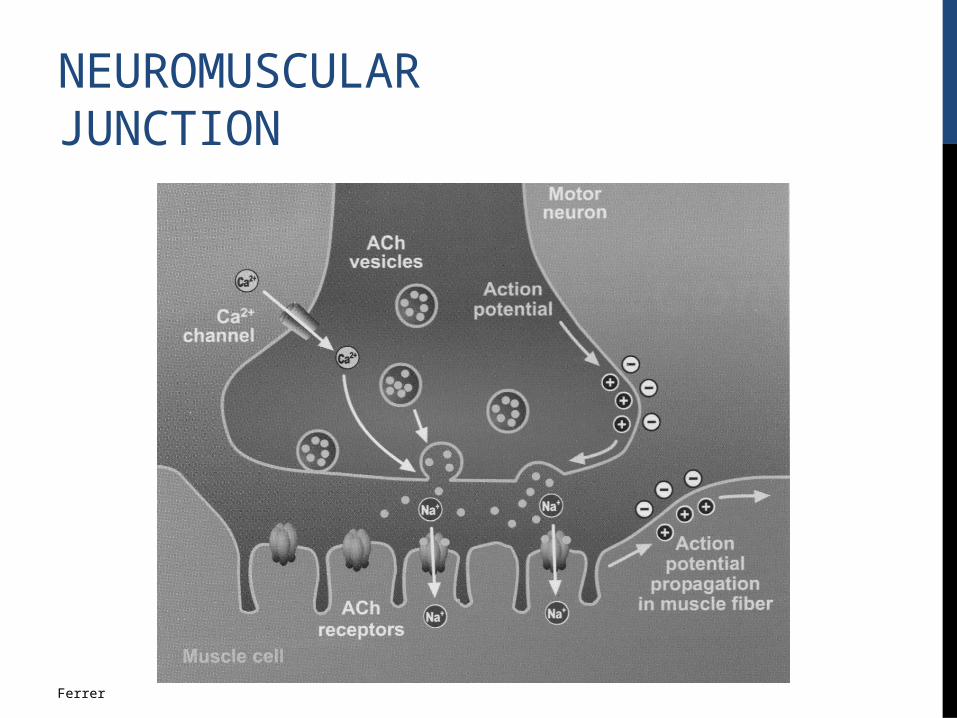
Ferrer
NEUROMUSCULAR JUNCTION
PATHOPHYSIOLOGYAntibodies against:
AChR – most common
Muscle-specific kinase (MuSK)
Seronegative types (LRP4, agrin, clustered AChR)5
Reduction of AChRs at the NMJ in anti-AChR2
Decreased AChR clustering in other types6
Pathophysiological mechanisms for anti-AChR:
AG presentation
T-cell recognition and activation of B cells
Ab activation of complement
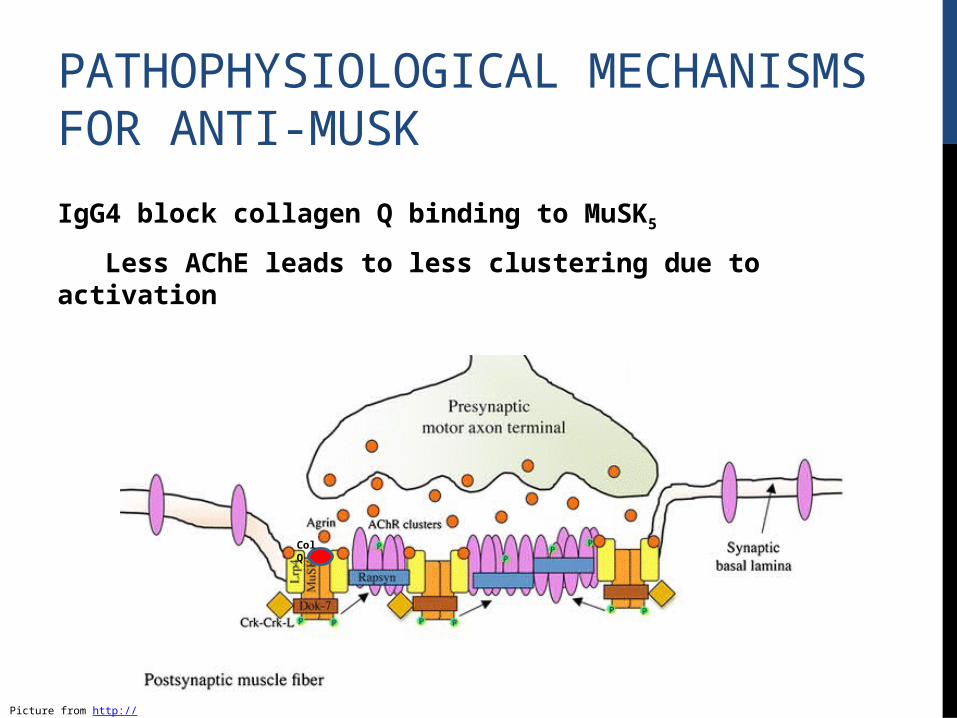
PATHOPHYSIOLOGICAL MECHANISMS FOR ANTI-MUSK
Col Q
IgG4 block collagen Q binding to MuSK5
Less AChE leads to less clustering due to activation
Picture from http://www.jcsm.info/index.php/en/57-fullarticlesvolume2/v2number4december-20113/191-molecular-control-of-neuromuscular-junction-development44

ACHR CLUSTERING PATHWAY
Picture from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2835321/

IMMUNOLOGICAL MECHANISMS
Polymorphisms in FOXP3
Reduces Treg cell number and function
Increased CD28 activity
Active proinflammation cytokines3
More Tfh cells in the peripheral blood
More circulating anti-AChR Ab
Picture from http://neuromuscular.wustl.edu/mtime/modulation.htm

MOST COMMON TREATMENTS
Immunosuppressive therapy—most common7
Prednisone2
Corticosteroids, azathioprine, cyclosporine
Reversible cholinesterase inhibitors2
Helps reduce muscle weakness
Counterproductive in MuSK-MG8
Thymectomy – beneficial in ~96% of patients9
Usually high remission rates
Pictures from http://info.agscientific.com/blog/bid/175925/4-IMPORTANT-USES-OF-IMMUNOSUPPRESSANTS and http://www.lkhtc.com/cms/features/surgery/minimal-access-surgery/thymectomy-for-myasthenia-grevis.html

LESS CONVENTIONAL TREATMENTS
Short-term immunomodulation
Plasmapheresis and intravenous immunoglobulin
Crisis intervention
Rituximab (monoclonal Ab therapy)
Possible use early on in drug-resistant cases
Controversial3
Targets CD208
Eculizaumab/complement inhibitors3
Still in the testing phase
Monoclonal Ab prevents enzymatic cleavage of C5
Picture from http://myrome.org/portal/plasmapheresis-multiple-sclerosis

OPTIMISTIC PROGNOSIS WITH TREATMENT
Long-term natural course is highly variable4
Death (20-30%)10
Current treatment lowers mortality to <4%10
Maximal weakness is usually achieved within the first 3 years4
Picture from http://southtees.nhs.uk/news/hospitals/surgeon-performs-regions-first-vats-thymectomy/

QUESTION 1
How do anti-AChR Ab arise?
A. Activation of B cells via mitogens
B. Polymorphisms in FOXP3 causing a reduction in Treg numbers and function
C. B cell activation via crosslinking
D. Similarities of the AG to bacterial AG cause memory cell activation

QUESTION 2
What role does MuSK play in the neuromuscular junction?
A. Triggers clustering of AChR
B. Signals opening of sodium channels
C. Breakdown of AChR
D. Increases AChE production

QUESTION 3
What treatment is used during myasthenic crisis?
A. Immunosupressants
B. Thymectomy
C. Complement inhibitors
D. Filtration/donation of plasma (plasmapheresis)

QUESTION 4
Who is most likely to be diagnosed with MG?
A. 15-year-old male
B. 15-year-old female
C. 35-year-old male
D. 35-year-old female
ESSAY TIME!!!
A) Where does agrin usually fit in the pathway?
B) How would antibodies against agrin result in myasthenia gravis?

QUESTION ANSWERS
1: B
2: A
3: D
4: D
Essay: A) It’s a ligand for LRP4, which dimerizes MuSK so that AChR will cluster.
B) AChR has to cluster in order to function. Without AChR, the muscle will not receive the signal from the neuron
and will not contract.

REFERENCES1. Saeed S, Patel S. 2011. Use of non invasive ventilation to avoid re-intubation in myasthenia gravis; a case report and review of literature. J Pak Med Assoc. 61(3): 293-295.
2. Mackey JR, Desai S, Larratt L, Cwik V, Nabholz J-M. 1997. Myasthenia gravis in association with allogenic bone marrow transplantation: clinical observations, therapeutic implications and review of literature. Bone Marrow Transplantation. 19: 939-942.
3. Querol L, Illa I. 2013. Myasthenia gravis and the neuromuscular junction. Wolters Kluwer Health. 26(5): 459-465.
4. Tormoehlen LM, Pascuzzi RM. 2008. Thymoma, myasthenia gravis, and other paraneoplastic syndromes. Hematology/oncology Clinics of North America. 22(2008): 509-526.
REFERENCES
5. Cavalcante P, Bernasconi P, Mantegazza R. 2012. Autoimmune mechanisms in myasthenia gravis. Wolters Kluwer Health. 25(5): 621-629.
6. Wu H, Xiong WC, Mei L. 2010. To build a synapse: signaling pathways in neuromuscular junction assembly. Development. 137(7): 1017-1033.
7. Auriel E, Regev K, Dori A, Karni A. 2011. Safety of influenza and H1N1 vaccinations in patients with myasthenia gravis, and patient compliance. Muscle & Nerve. 893-894.
8. Sieb JP. 2013. Myasthenia gravis: an update for the clinician. Clinical and Experimental Immunology. 175: 408-418.

REFERENCES
9. Barrons RW. 1997. Drug-induced neuromuscular blockade and myasthenia gravis. Pharmacotherapy. 17(6): 1220-1232.
10. Ferrer E, Moral A, Bozzo J. 2007. Myasthenia gravis. Drugs of the Future. 32(7): 615-624.

















