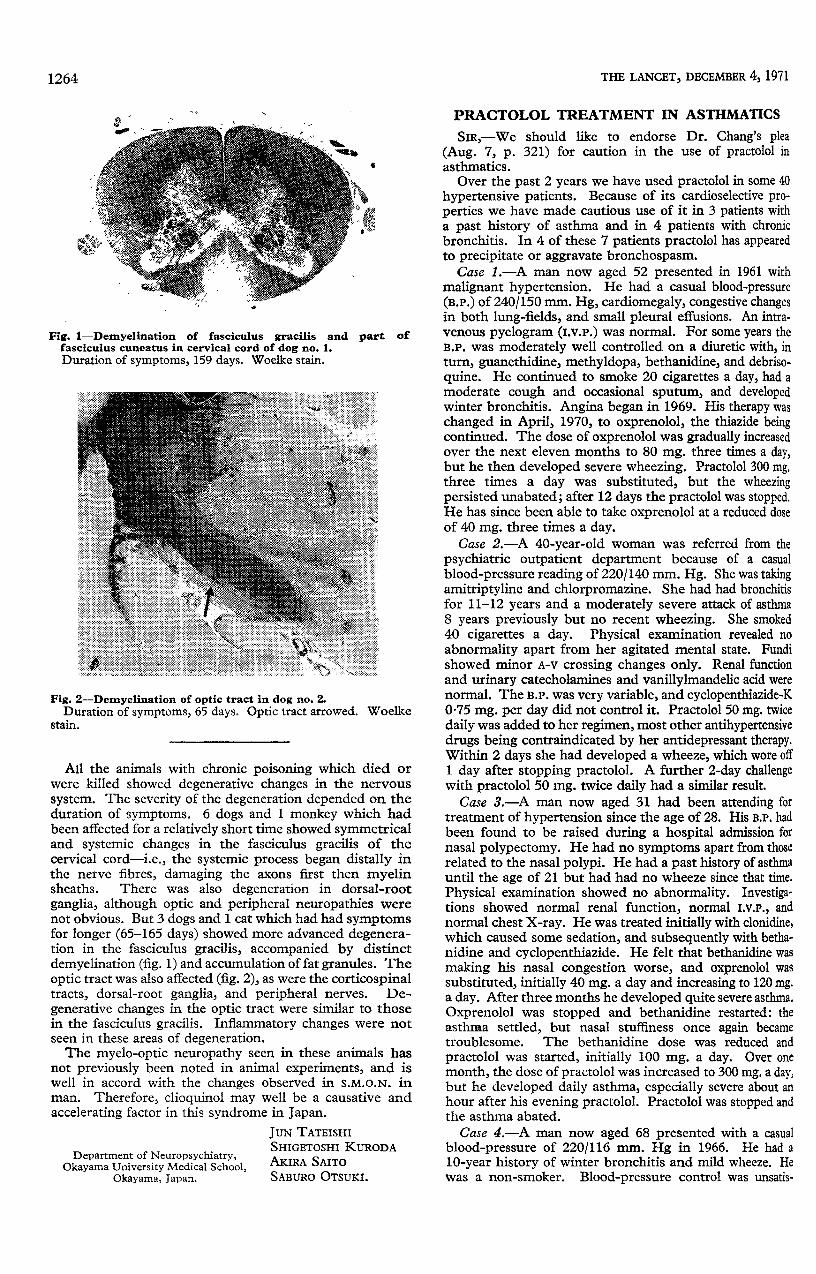
2
1263 AID FOR THE ADOLESCENT ANTHONY RYLE. University Health Service, University of Sussex, Falmer, Brighton, Sussex. CLAIRE RAYNER. Petticoat, IPC Magazines Ltd., Fleetway House, Farringdon Street London EC4A 4AD. W. H. ALLCHIN. 66 Old Kennels Lane, Oliver’s Battery, Winchester. SIR,-It is hard to see how Mr. Brinton (Nov. 20 p. 1139), able to describe a youngster as "on the verge of suicide or some other idiocy " and prepared to be so arrogantly dismissive of the professional workers respon- sible for the care of the young, can himself bring much aid to adolescents. He is also guilty of seriously under- valuing what they do for themselves, failing to note how far they have been able to contain and limit the dangers posed by the ever-present availability of drugs, an achieve- ment still far short of the ideal, but the more admirable when one considers that all too often the help they are offered by doctors (Brinton’s " heroic psychotropic drugs ") is as irrelevant to their problems as are the drugs which their own peer group can provide. He also seems blind to the ways in which mutual tolerance and caring are far more prevalent in young people today than in the past. Despite this greater mutual support, adolescents can respect and seek help from adults who are able to listen to them and to respect them, and many of them need professionals with the knowledge of psychology and the concern for existential issues which Brinton seems to find so distasteful (or threatening ?). Sir warmly support Mr. Henry Brinton regarding the provision of counselling services for disturbed adoles- cents. I deal with the Problem Page for this teenagers’ magazine, coping with the 4000 to 5000 letters per year all seeking help. A large number can be satisfied by information (sex education, in my experience, is still woefully in- adequate in our society), others by being referred to Brook and F.P.A. clinics, marriage-guidance counsellors, the National Council for the Unmarried Mother and Her Child, reliable " pregnancy advisory services ", and the like. But there remains a sizeable group who need, quite desperately, someone to talk to. Someone who will treat them as worth-while people, who will not sneer, make facile moral judgments, or shrug them away as nuisances; I know they need this because they write to me after having received precisely the opposite treatment from the adults they have already approached, such as parents, general practitioners (often!), and (occasionally) teachers. Where there are local youth counselling services I refer readers, but there are far too few, and such as there are tend to be clustered in the large conurbations like London and Birmingham. For the rest there is, fortunately for them and for the " professional " whose burden is taken up for them, the Samaritans-voluntary workers with good selection and basic training provided by the organisa- tion. They care, and they will listen. Any practitioner faced with an adolescent with whom he cannot come to terms, or who frankly bores and irritates him, could do worse than swallow his professional pride and refer his patient to this splendid organisation. SiRjŅMr. Brinton’s article is certainly an interesting piece, but its tone seemed to me surprisingly negative and even somewhat sneering. And I think it would be fair to comment that it was short of factual matter. However, some facts are available. For example, an up- to-date and concise study, covering the care of 150 adoles- cents over five years, has been carried out in the Wessex region by Dr. Mary Capes and two colleagues, a psycholo- gist and a sociologist. 1 This gives details of some of the resources available to adolescents and their parents. Some of the help given is shown to be useful and effective. The child-guidance clinic seems to be anybody’s Aunt Sally these days, and it may be true that it would fail to pass the " cost/benefit analysis " test. Personally, I doubt whether anyone has the information available to confirm or refute the suggestion. But it might be worth saying that many of the most valuable activities in our community, in social and personal terms, might also fail such an assessment, while some of our most pernicious institutions would pass with flying colours and profits. That we can offer only what often amounts to no more than a first-aid service does not separate the child and adolescent field from that of adult psychiatry. Both these deficiencies are a disgrace to any community which hopes to be regarded as compassionate and humane, and to be- little what little we actually do at the present time does not seem to me to be constructive. TOWARDS EASIER CHILDBIRTH S. M. HALLIDAY. Fordingbridge, Hampshire. SIR,-The article by Mr. Tachi (Nov. 20, p. 1134) makes it evident that he has never sat quietly observing a normal labour and delivery. One of the important dis- coveries he might otherwise have made is that a mother (and a father) is normally able to enjoy her baby within one hour of delivery, often within one minute. Perhaps he is unable to sit quietly watching and listening, in which case he should never have been an obstetrician. MYELO-OPTIC NEUROPATHY INDUCED BY CLIOQUINOL IN ANIMALS SIR,-Concerning the stiology of subacute myelo-optic neuropathy (S.M.O.N.) in Japan, two theories have been reported in The Lancet-the clioquinol theory 2-4 and the virus theory.5,6 We administered clioquinol to dogs, cats, and a monkey orally for approximately six months and succeeded in eliciting a similar syndrome to that in man, clinically as well as pathologically. Of 20 dogs given the substance, 3 did not develop any symptoms, 5 died of acute poisoning with epileptic con- vulsions or general weakness, and 12 showed symptoms indicating chronic poisoning. Clinical symptoms of chronic poisoning began with side-swaying of the hips, followed by muscle weakness and increased tendon-jerks in the hind- legs. The longer administration was continued, the more severe the signs became, until the dogs could not remain standing even to eat. The visual acuity was apparently impaired in 3 dogs, since they could not follow objects properly. 1 dog was incontinent of urine. The dose of clioquinol required to elicit symptoms of chronic intoxi- cation ranged from 60 to 144 mg. per kg. per day. Except in 2 dogs, the symptoms appeared within 7-28 days on the above toxic doses. 1 cat showed the same symptoms under the same conditions. A monkey did not develop full symptoms of chronic poisoning, and died of broncho- pneumonia on the 84th day. As controls, 4 dogs, 3 cats, and 1 monkey were healthy throughout the experiments. 1. Capes, M., Gould, E., Townsend, M. Stress of Youth London, 1971. 2. Tsubaki, T., Honma, Y., Hoshi, M. Lancet, 1971, i, 696. 3. Igata, A. ibid. 1971, ii, 42. 4. Nakae, K., Yamamoto, S., Igata, A. ibid. 1971, ii, 510. 5. Inoue, Y., Nishibe. Y., Nakamura, Y. ibid. 1971, i, 853. 6. Shimada, Y., Tsuji, T. ibid. 1971, ii, 41.