Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano Convention Centre . Milano 18-21 Ottobre, 2009 Myelodysplastic Syndromes: WHO 2008
Transcript
Attilio Orazi, M.D., FRCPath. (Engl.)
Weill Medical College of Cornell University
New York, NY
Congresso Nazionale SIE - Società Italiana di Ematologia - MICMilano Convention Centre . Milano 18-21 Ottobre, 2009
Myelodysplastic Syndromes: WHO 2008
MDS are clinically heterogeneous: Classification/Scoring Systems
FAB plus dysplasia (10% rule; uni vs. multi), and cytogenetics (5q-)
Values higher than these are not exclusionary of adiagnosis of MDS, if definitive morphologic and/orcytogenetic findings consistent with MDS are present
Morphologic Guidelines for theDiagnosis and Classification of MDS:
• Dyserythropoiesis, dysgranulopoiesis:>10% of cells on the BM aspirate smear
• Dysmegakaryopoiesis >10% of cellsevaluated on 30 megakaryocytes at least(BM aspirate smear or biopsy)
• Ring sideroblasts (iron stain of aspirate)• Blast percentage• Correlate the findings with marrow biopsy
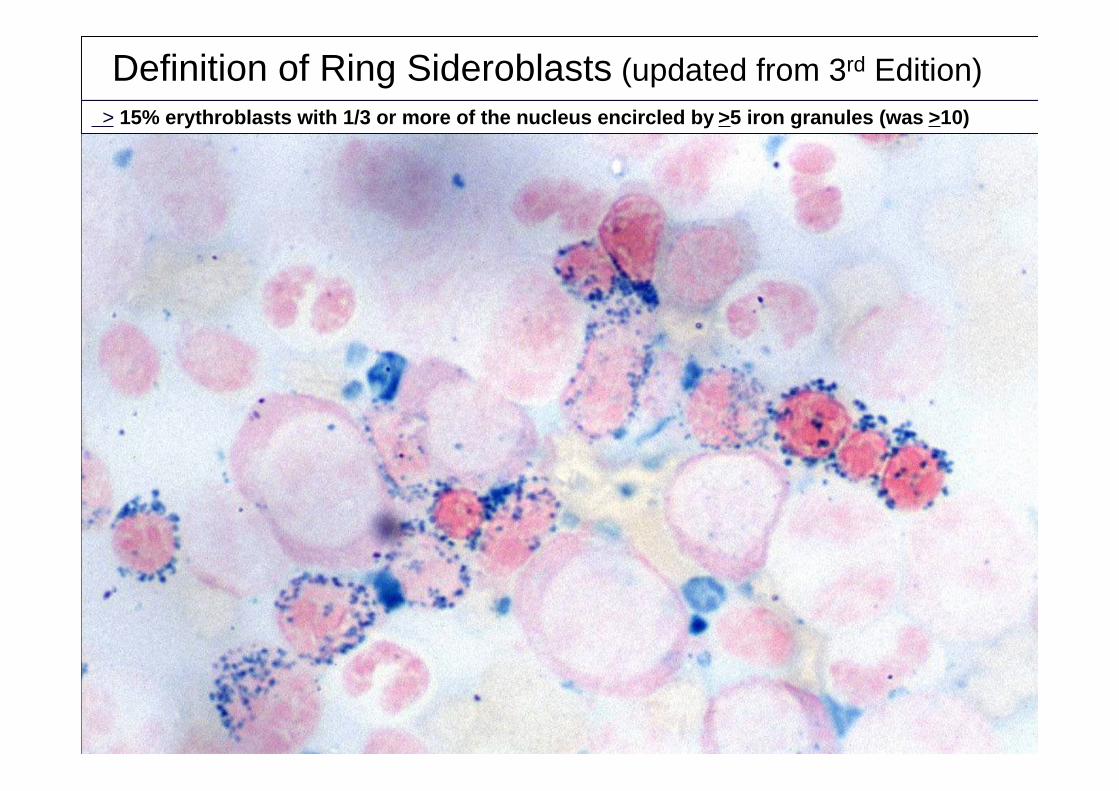
Definition of Ring Sideroblasts (updated from 3rd Edition) > 15% erythroblasts with 1/3 or more of the nucleus encircled by >5 iron granules (was >10)
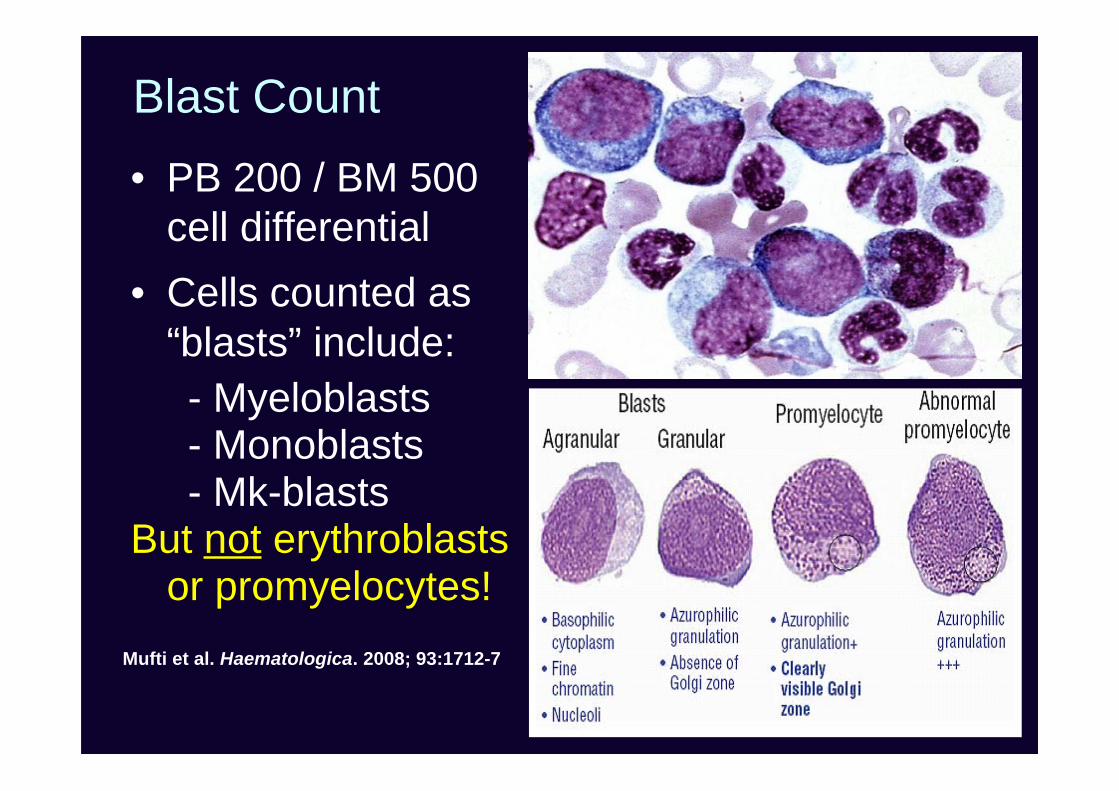
Blast Count• PB 200 / BM 500
cell differential• Cells counted as
“blasts” include: - Myeloblasts - Monoblasts - Mk-blastsBut not erythroblasts
or promyelocytes!Mufti et al. Haematologica. 2008; 93:1712-7
• Quality check for the adequacy of BM aspirate• Provides information on stroma and cellularity
(e.g. fibrosis, fatty marrow)• Yields tissue for a number of studies: - immunohistochemistry
- in-situ hybridization
- molecular procedures (e.g. microdissection)
The role of BM biopsy in MDS is betterdescribed in the 4th edition
Blast count is poorly reproducible particularly in thickparaffin sections. Clusters of blasts more specific.
CD34 pos. cell clusters: 3-5 cells
Blasts and blast clusters identification made easier by immunohistology(e.g. CD34, CD117). Micromegakaryocytes by CD61 or CD42b
CD42b pos. dwarf- / micro- megs.
• Cases with inconclusive morphologic andcytogenetic findings and >3 or more aberrantfeatures by flow cytometry should be re-evaluated over several months for definitivemorphologic or cytogenetic evidence of MDS
• Utility of CD14/CD56 in CMML• Substitution of blast % determined by flow
cytometry for a visual blast count is discouraged
Flow cytometry to demonstrate anabnormal myeloid maturation
(abnormalities in light scatter and antigenic expression)
Interlaboratory variability issues:still work in progress
• Ogata K, et al. Diagnostic utility of flow cytometryin low-grade myelodysplastic syndromes: aprospective validation study. Haematologica. 2009Aug;94(8):1066-74. Epub 2009 Jun 22.
• van de Loosdrecht AA et al. Standardization offlow cytometry in myelodysplastic syndromes:report from the first European LeukemiaNetworking conference on flow cytometry inmyelodysplastic syndromes. Haematologica. 2009Aug;94(8):1124-34.
MDS: WHO 2008
Subtypes and changes
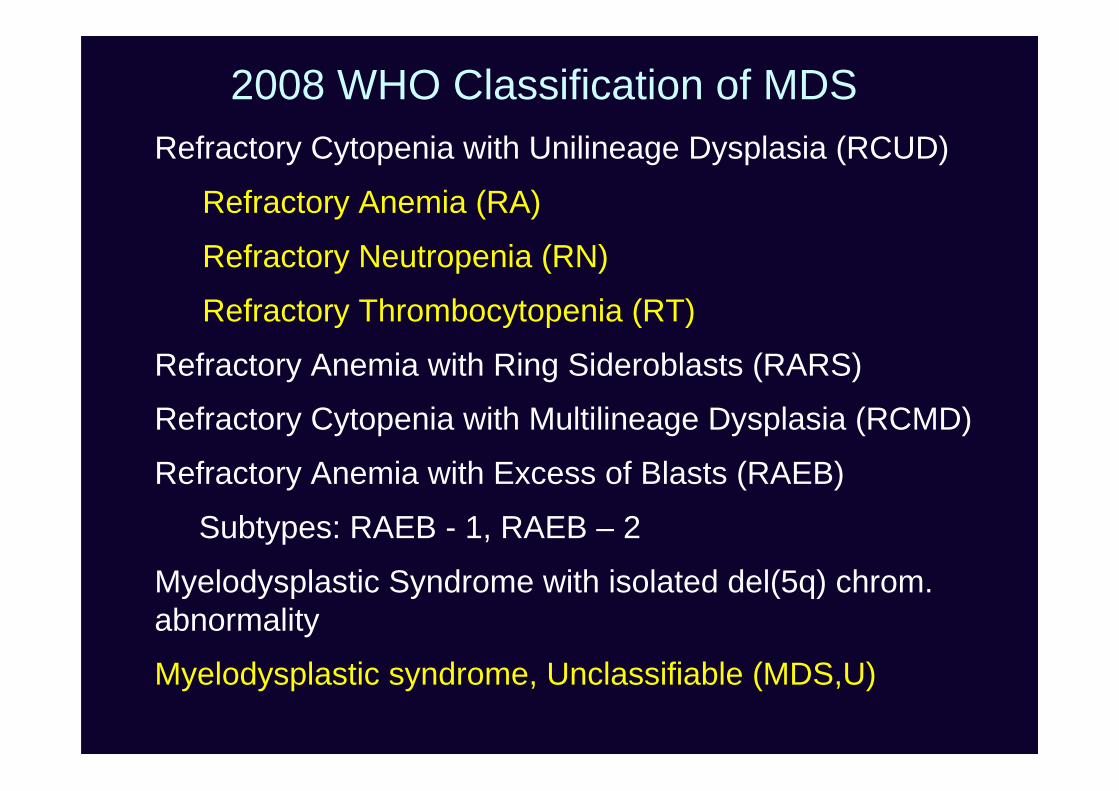
Refractory Cytopenia with Unilineage Dysplasia (RCUD)
Refractory Anemia (RA)
Refractory Neutropenia (RN)
Refractory Thrombocytopenia (RT)
Refractory Anemia with Ring Sideroblasts (RARS)
Refractory Cytopenia with Multilineage Dysplasia (RCMD)
Refractory Anemia with Excess of Blasts (RAEB)
Subtypes: RAEB - 1, RAEB – 2
Myelodysplastic Syndrome with isolated del(5q) chrom.abnormality
Myelodysplastic syndrome, Unclassifiable (MDS,U)
2008 WHO Classification of MDS
Refractory cytopenia with Mono-/bi-cytopenia1 Dysplasia (≥10%) unilineageunilineage dysplasia No or <1% blasts2,3 <5% blasts
<15% ring sideroblasts
Refractory anemia with Anemia Erythroid dysplasia onlyring sideroblasts No blasts <5% blasts
≥15% ring sideroblasts
Refractory cytopenia with Cytopenia(s) Dysplasia in ≥10% of themultilineage dysplasia No or <1% blasts2,3 cells of two or more lineages
<5% blasts< or >15% ring sideroblasts
PB BM
[Note: Monocytes <1 × 109/L; No Auer rods]
(RA, RN, RT)
1 Pancytopenia= MDS,u2 If 1% blasts in PB (<5% blasts in BM)= MDS,u 3 If 2-4% blasts in PB (< 5% blasts in BM)= RAEB-1
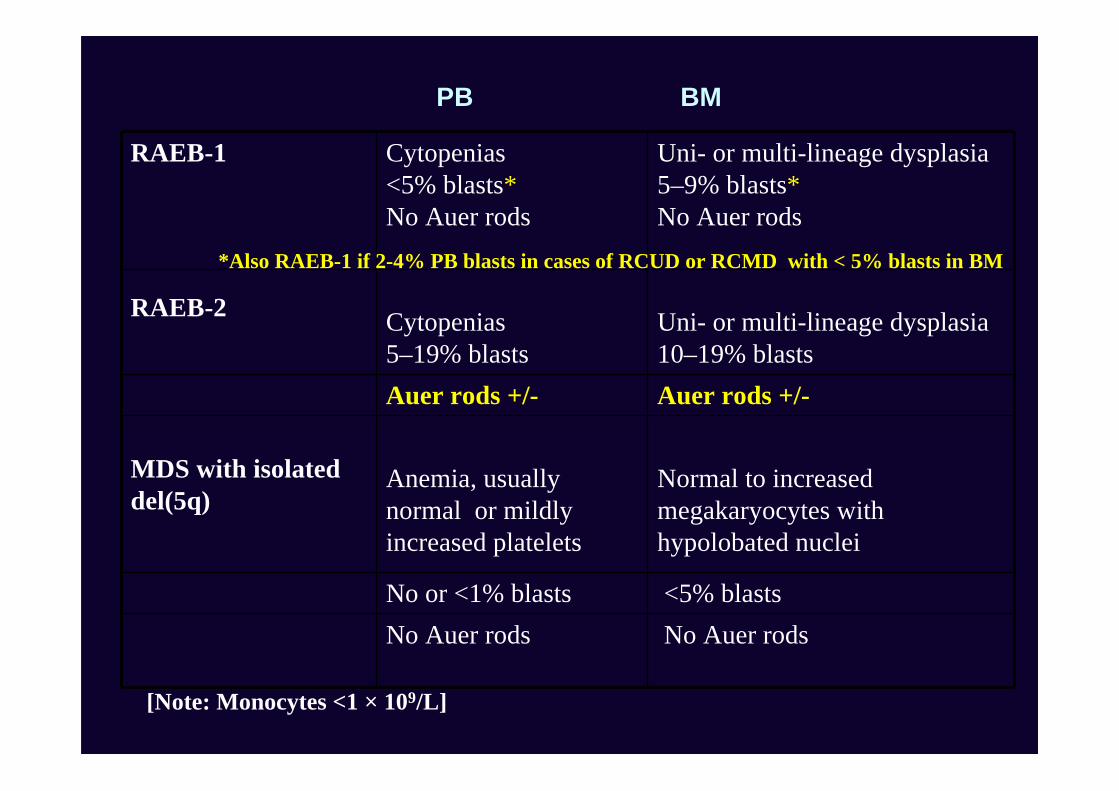
RAEB-1 Cytopenias<5% blasts*No Auer rods
Uni- or multi-lineage dysplasia5–9% blasts*No Auer rods
RAEB-2 Cytopenias5–19% blasts
Uni- or multi-lineage dysplasia10–19% blasts
Auer rods +/- Auer rods +/-
MDS with isolateddel(5q)
Anemia, usuallynormal or mildlyincreased platelets
Normal to increasedmegakaryocytes withhypolobated nuclei
No or <1% blasts <5% blastsNo Auer rods No Auer rods
PB BM
*Also RAEB-1 if 2-4% PB blasts in cases of RCUD or RCMD with < 5% blasts in BM
[Note: Monocytes <1 × 109/L]
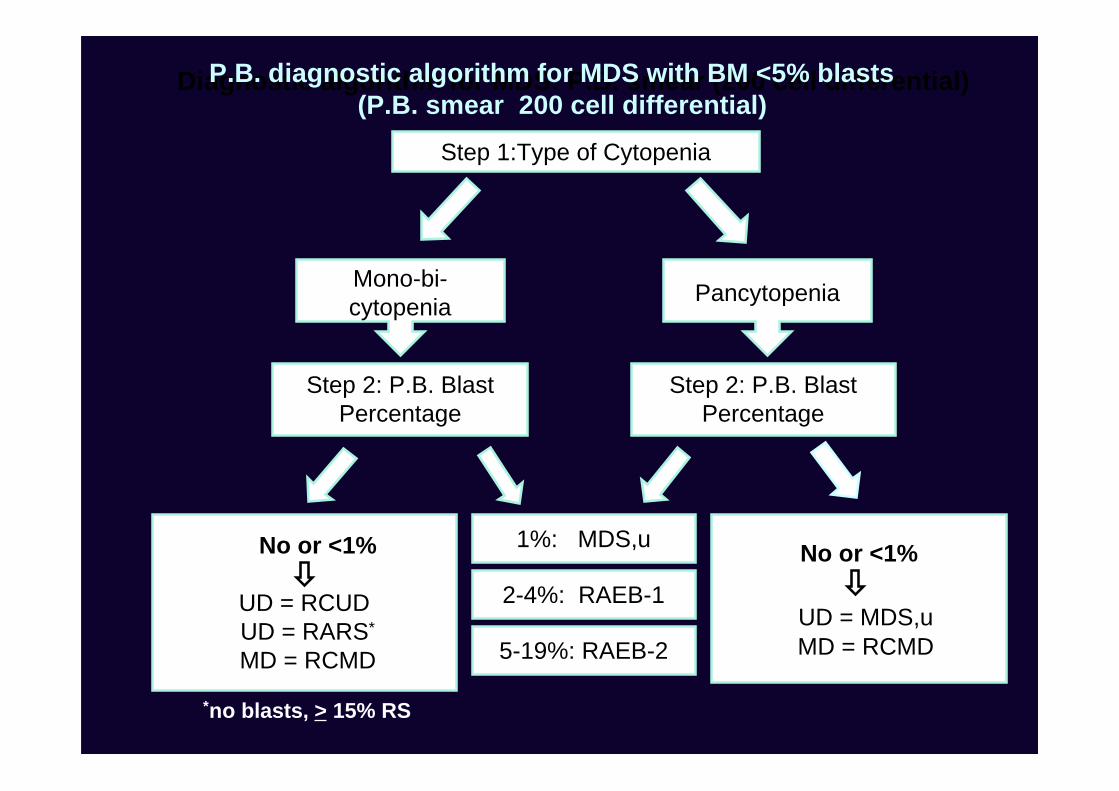
Step 1:Type of Cytopenia
Step 2: P.B. BlastPercentage
No or <1%
UD = RCUD UD = RARS*
MD = RCMD
1%: MDS,u
2-4%: RAEB-1
5-19%: RAEB-2
No or <1%
UD = MDS,u MD = RCMD
*no blasts, > 15% RS
Diagnostic algorithm for MDS: P.B. smear (200 cell differential)
Mono-bi-cytopenia Pancytopenia
P.B. diagnostic algorithm for MDS with BM <5% blasts (P.B. smear 200 cell differential)
(9.0 vs 8.7 g/dL; P=0.272)Ingram et al: Leukemia 2006;20:1319-1321
MDS, unclassifiable (3 settings)
1. Patients with refractory cytopenia withunilineage dysplasia (RCUD) or refractorycytopenia with multilineage dysplasia(RCMD) but with 1% blasts in theperipheral blood
2. Cases of MDS with unilineage dysplasiawhich are associated with pancytopenia.RCUD (in contrast with RCMD) only allowsfor a single cytopenia or bicytopenia
3. Persistent (6 mo.) cytopenia(s) lacking morphologicfeatures of MDS, but with cytogenetic abnormalities
presumptive for MDS*• +8*• -7 or del(7q)• -5 or del(5q)• del(20q)*• -Y*• i(17q) or t(17p)• -13 or del(13q)• del(11q)• del(12p) or t(12p)• del(9q)• idic(X)(q13))
• t(11;16)(q23;p13.3)
• t(3;21)(q26.2;q22.1)
• t(1;3)(p36.3;q21.2)
• t(2;11)(p21;q23)
• inv(3)(q21q26.2)
• t(6;9)(p23;q34)
* As single cytogenetic abnormality, inthe absence of morphologic findings,is insufficient evidence for MDS
Subtypes of MDS difficult todistinguish from other myeloid
neoplasms (discussed in the 4th edition)• Hypoplastic MDS from acquired
aplastic anemia
• MDS with fibrosis from other fibroticmyeloid neoplasms (e.g. PMF)
• MDS with > 50% erythroblasts fromacute erythroid leukemia
hypo-MDS
AA
CD34: h-MDS vs. AA: p=.001
Maschek H,et al. Ann Hematol 1993; 66: 117–122. Orazi et al. Am J Clin Pathol 1997; 107:268-74. Bennet & Orazi. Haematologica 2009; 94:264-8
MDS, hypoplastic(Cellularity <30% in patients <70 years old, and <20% in >70 years old)
hypo-MDS
• Lim ZY, et al. Low IPSS score and bone marrowhypocellularity in MDS patients predict hematologicalresponses to antithymocyte globulin. Leukemia.2007;21:1436-41.
• Sloand EM, et al. Factors* affecting response andsurvival in patients with myelodysplasia treated withimmunosuppressive therapy. J Clin Oncol.2008;26:2505-11.
*Younger age & HLA-DR15 were the most significant factors favoring response totherapy
MDS with fibrosis (>2+ fibrosis)
100
80 % MDS fibrosis <2
Survival 60
40 p < .0005
20
0 1 6 12 18 24 30 36 42 mo
I
III
II
Lambertenghi-Deliliers G, Orazi A, Lucks R, et al.: Br J Haematol, 1991
MDS fibrosis > 2
• Scott BL, et al. Marrow fibrosis as a risk factor forposttransplantation outcome in patients withadvanced myelodysplastic syndrome or acutemyeloid leukemia with multilineage dysplasia. BiolBlood Marrow Transplant 2007;13:345-54
• Buesche G, et al. Marrow fibrosis predicts earlyfatal marrow failure in patients withmyelodysplastic syndromes. Leukemia 2008;22:313-22
• Della Porta MG, et al. Clinical relevance of bonemarrow fibrosis and CD34-positive cell clusters inprimary myelodysplastic syndromes. J Clin Oncol2009;27:754-62
Erythroid-rich MDS: when the erythroidcells are > 50% of all the nucleated cells
• A second count for the non-erythroidcells:
– AML, if the blasts are > 20% of the non-erythroid cells (erythroleukemia)
– MDS, if the blasts are less than 20% of thenon-erythroid cells
• If MDS, then use the original blast %for further MDS subtyping
• Chronic myelomonocytic leukemia (CMML)
• Atypical chronic myeloid leukemia* (aCML)
• MDS/MPN, unclassified (MDS/MPN,u)
–– Refractory anemia with ring sideroblastsRefractory anemia with ring sideroblastsand thrombocytosis (RARS-T)and thrombocytosis (RARS-T)
(Hematopoietic malignancies with hybrid features both of MDS and MPN)
*BCR-ABL1 negative
*May resemble CMML or aCML.Include cases formerly termed CMMLwith t(5;12)
In all cases the presence of• Ph’ chromosome/BCR/ABL1 fusion gene
plus, in cases with eosinophilia• PDGFR Alpha abnormalities
• PDGFR Beta abnormalities*
Diagnosis of MDS/MPN: WHO requiresto exclude
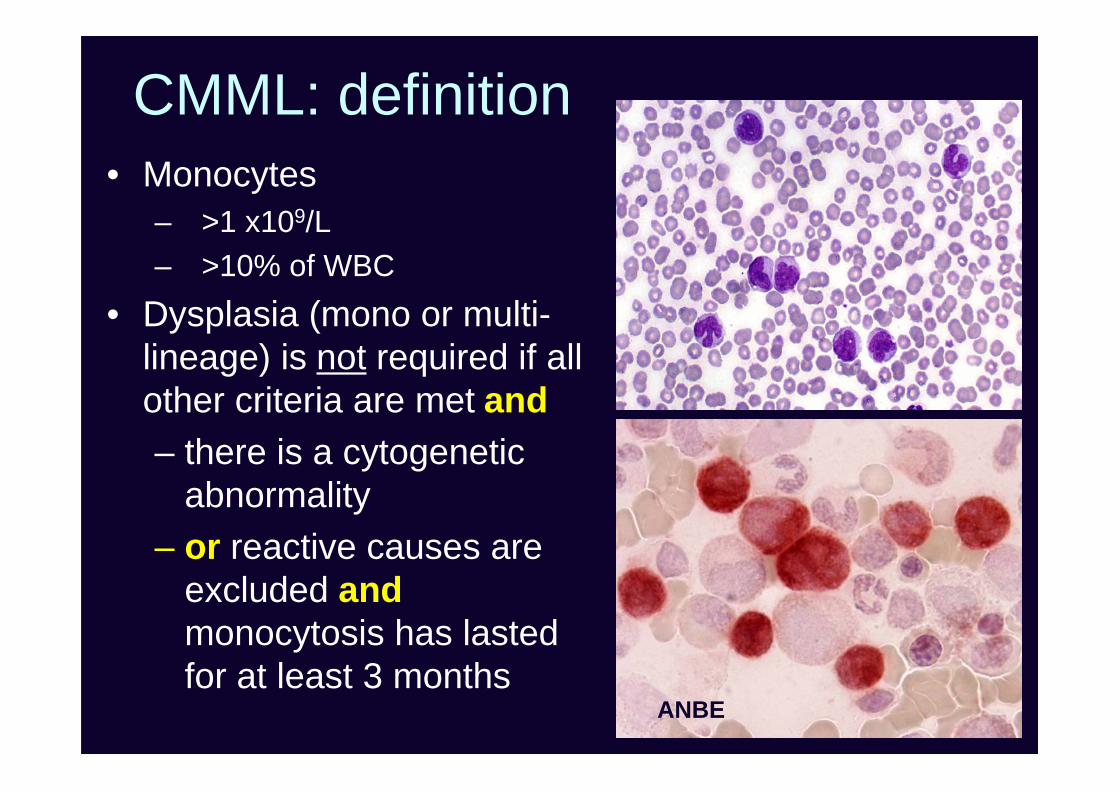
CMML: definition• Monocytes
– >1 x109/L– >10% of WBC
• Dysplasia (mono or multi-lineage) is not required if allother criteria are met and– there is a cytogenetic
abnormality– or reactive causes are
excluded andmonocytosis has lastedfor at least 3 months
ANBE
Monoblasts
Promonocytes
Abnormal monocytes (immature) Adapted from WHO Classification of Tumors of Haematopoieticand Lymphoid Tissues. IARC: Lyon 2008. Fig.1-04 (p. 21).
MonoblastsLarge cells with abundantcytoplasm minimallyvacuolated round nuclei withfine chromatin and nucleoli
PromonocytesIrregular or folded nuclei, smallindistinct nucleoli, finechromatin and a morevacuolated and/or granularcytoplasm
Abnormal monocytesMore condensed chromatin,convoluted nuclei and moregranulated
RARS-T• Its incidence is rare (underdiagnosed?)• JAK2 positive in approx. 60% of cases• MPL W515K/L (very rare)• RARS-T has a worse outcome than ET• Is controversial
Wardrop D, Steensma DP. Is RARS-T a necessary or usefuldiagnostic category? Br J Haematol. 2009;144:809-17
BM Biopsy
• Massachusetts General Hospital, Boston, MA1
• U. Mass Memorial Med. Center, Worcester, MA2
• Brigham and Women’s Hospital, Boston, MA3
• Weill Cornell College of Medicine, New York, NY4
• Genzyme, Inc, New York, NY5
• Baystate Med. Center, Springfield, MA5
Hasserjian RP1, Soupir CP1, Wang Sa A2, VergilioJoA3, Orazi A4 , Dong H5
RARS-T study (44 cases)
Karyotype (40 patients)
• 31 (78%) had a normal karyotype
• 9 cases (22%) with abnormal karyotypewhich included:
• JAK2(+) cases had a significantly higher PLTand WBC counts, and a trend towards a higherHB level
• JAK2(+) cases had more prevalent large Megsoften with staghorn or bulbous nuclearmorphology while small and normal-sized Megs.were predominant in the JAK2(-) cases
• No differences in reticulin fibrosis andmorphologic dysplasia in other lineages
Additional issues
• Prognosis
• Molecular pathogenesis
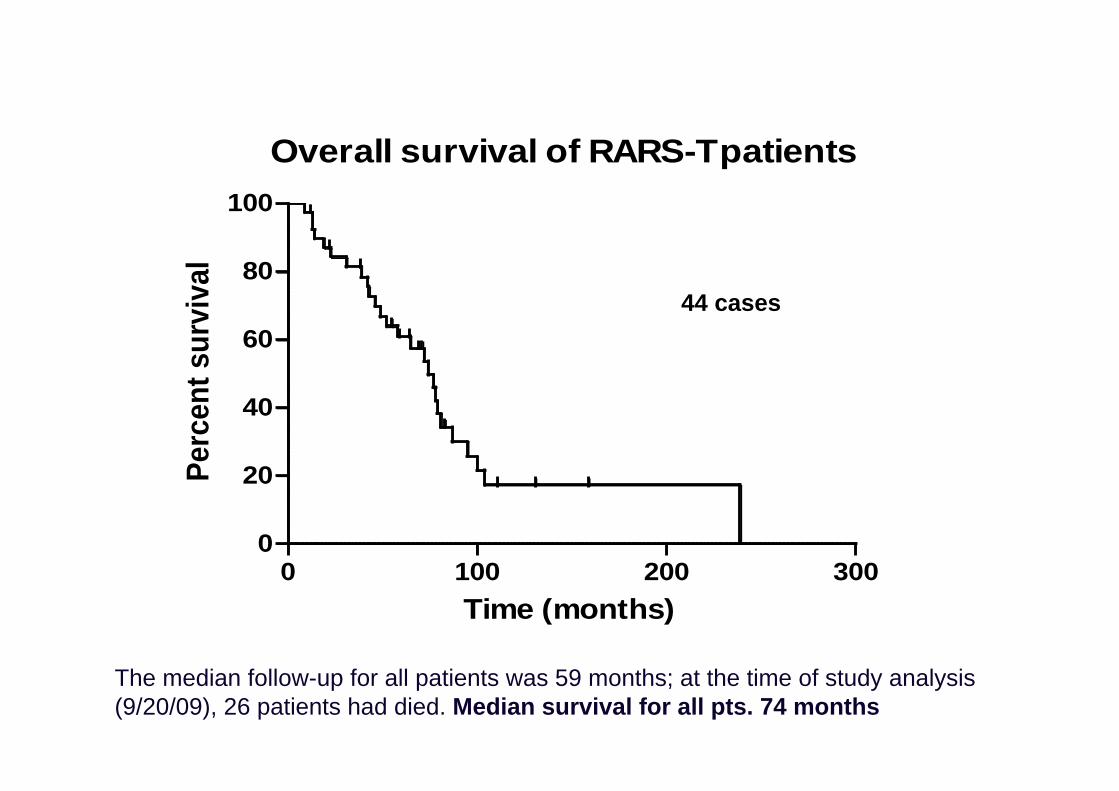
Overall survival of RARS-Tpatients
0 100 200 3000
20
40
60
80
100
Time (months)
Perc
ent s
urvi
val
The median follow-up for all patients was 59 months; at the time of study analysis(9/20/09), 26 patients had died..Median survival for all pts. 74 months
44 cases
Transformation to AML• Our series: 4/27 (15%)
cases with follow up
• Pich A, Godio L. RARS-T associated withJAK2V617F mutationtransformed to AML withchromosomal evolutionincluding monosomy 7.Leuk Res (2009). Inpress.
Schmitt-Graeff A et al. Haematologica 2008
23 cases
Prognostic role for JAK2
Prognostic role for JAK2?
Suggested by: Atallah E, et al. Leukemia. 2008; 22:1295-8
Not confirmed by: Wang SA, et al. Leukemia. 2006;2 0:1641-4
Raya JM, et al. Int J Hematol. 2008; 88:387-95
Hasserjian RP, et al. our current study
Molecular pathogenesis: Malcovati L, et al.Blood. 2009 Aug 19. [Epub ahead of print]
• 19 RARS-T defined according to WHO 2008• Like in RARS, up-regulation of ALAS2 and down-
regulation of ABCB7 in CD34+ cells, i.e. RARS-T hasdistinctive “sideroblastic” features at the molecularlevel.
• X-chromosome inactivation shows that JAK2 pos. cellsare only a fraction of clonal granulocytes
• 3 RARS pts. with low or normal plts. progressed toRARS-T (2/3 acquired JAK2). It may develop fromRARS through the acquisition of somatic mutations ofJAK2, MPL or other as-yet-unknown genes
Summary• Morphology is still very important for diagnosis• Perform always iron and reticulin stains• Look out for monocytes in PB and BM and use
cytochemistry and flow to confirm monocytosis• Bone marrow biopsy supplemented by
immunohistology (particularly useful in cases withfibrosis or fatty BM)
• Karyotype is mandatory. FISH may supplement• BCR-ABL1 and, in cases with eosinophilia, PDGFR
rearrangements• Test for JAK2 when appropriate (e.g. RARS-T, 5q-)