24
Comparative genomic hybridization in PGD Dmytro Mykytenko, M.D.,Ph.D. 2012

Comparative genomic hybridization in PGD
Dmytro Mykytenko, M.D.,Ph.D.
2012

Embryo aneuploidy
• Platteau P., Staessen C.et all, 2004 – 40,5-60% (depends on pathology)
• NADIYA (total index)
– aCGH – 49,7%
– FISH – 59%
2

3
The main causes of chromosomal anomalies
• The inheritance of the parental pathology- true inheritance (e.g.: parental translocation)
- Chromosomal nondisjunctionduring gametogenesis
(80-85% of causes relate to oocytes
10-15% - relate to spermatozoa)
• Mitotic errors in the zygote

Abnormal oocytes
4Gianaroli, L, Magli, C, et al, Glob. libr. women's med., 2008

• PDG – is the only one method of detection of embryos without chromosomal / genetic pathology.
• The transfer of the embryos without chromosomal imbalances allows us to increase the performance of ART cycles and to prevent the chromosomal pathology of the embryo.
5
Preimplantation genetic testing
Indications to PGS / PGD
•Matermal age > 38-42 y.o.•Multiple IVF failure•RPL•High level of sperm aneuploidy•The carriage of the gene defects / chromosomal rearrangements
Methods of PGD/PGS
• PCR-based
– PCR, real-time-PCR
– QF-PCR
• Sequencing, mini-Sequencing, next-gen sequencing
• F.I.S.H.
• array-CGH
• SNP-array
6

PGD TimeLine
1970 1980 1990 2000 2010
Implementation of the FISH into the cytogenetics
First PCR - PGD
FISH – sex selection
Implementation of the CGH into the cytogenetics
arrayCGH reported for clinical genetics
CGH- PGD
aCGH- PGD
PCR -PGD for Fresh ET
SNP-array PGD
First delivery after aCGH-PGS
aCGH
First aCGH-delivery
8
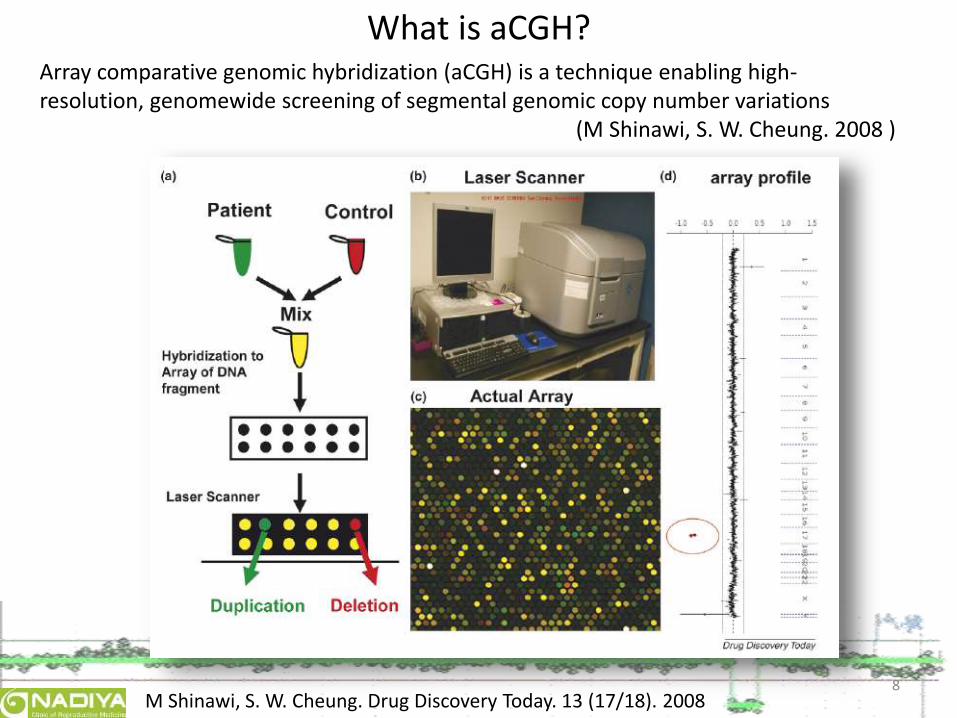
What is aCGH?
M Shinawi, S. W. Cheung. Drug Discovery Today. 13 (17/18). 2008
Array comparative genomic hybridization (aCGH) is a technique enabling high-resolution, genomewide screening of segmental genomic copy number variations
(M Shinawi, S. W. Cheung. 2008 )

9

Advantages of the array-CGH
• Microscopic chromosomal rearrangements– Aneuploidy (with limited mosaicism detection)
– imbalanced rearrangements
– Marker chromosomes
• Submisroscopic alterations– Subtelomeric imbalanced rearrangements
– Micro-deletion/duplication syndromes
10

Disadvantages and limitations• Balanced rearrangements
– Reciprocal translocation
– Inversions
– Robertson translocations
– Reciprocal insertions
• Imbalanced rearrangements below the diagnostic resolution– Point mutations
– Three nucleotide expansions
– Deletions / Duplications in not covered regions
11
•Limited ability to detect polyploidy•Limited ability to detect mosaicism•The method needs a great quantity of DNA

Whole genome amplification (WGA)• Methods
– Primer extension preamplification (PEP)– Degenerative oligonucleotide primed-PCR (DOP-PCR)– Ligation type PCR– Tagget PCR (T-PCR)– Multiple displasement amplification (MDA)– GenpmePlex
• Disadvantages– Sensitivity to quality and purity of the input material– Formation of the 100-1000 bp fragments (mean – 400 bp).– Amplification of the 60-80% of the genome only– Effect of the preferential amplification– Secondary DNA structures cause nonspecific amplification– Presence of the active polymerase after the end of the reraction
causes subsequent degeneration of the products– Allele drop-out phenomenon not excluded if works with single cell
12

aCGH platforms
13
Technologies:
•BAC (1-2 Mbp)
•Oligo (10-140kpb)

What? Where? and When?
14
Исследуемый материал:
• PB 1 & 2
• Blastomere (cleavage stage -day 3)
• Trophectoderm (blastocyst – day 5)
Features
PB biopsy Blastomere biopsy TE biopsy
•Indirect data about the oocyte genotype•Male factor is not taken into account
•Mosaicism is not excluded•Decreasing the embryo viability•Subsequent self-correction of trisomic embryos is not excluded
•More cells = more DNA = more accurate diagnostics•Less mosaicism•Reduced impact of embryo biopsy•Economic factor: less embryos to be analized•Facilitates the selective embryo transfer•Allows to modify endometrium if needed•Ability to blastocyst cultivation and vitrification are needed

12h BlueGnome
15

16
PGD-aCGH (own results)
Euploid embryo46, XY Aneuploid embryo
47, XY, +7
Euploid embryo46, XX
Aneuploid embryo45, XY, -16
arr CGH 22q11.1-q.ter x 1
arr 20q13.32-q.ter x 1

17
The comparative analysis of aCGH and FISH PGS (own data) for patients with multiple IVF failure
CGH-PGS * FISH-PGS No PGS
Cycles total 21 41 134
Main Age 33,9±5,4 33,45±5,1 34,3±4,3
Oocytes retrieved 16,7±8,2 13,6±5,1 12,8±4,2
Previously failed cycles 3,9 ±0,7 3,8±0,6 3,2±0,4
Embryos per ET 1,7±0,5 2,1±1,1 2,6±1,3
ET total 12 (+6 expected) 32 132
Completed cycles 84.4% 78,0% 98,5%
Pregnancies total 6 9 18
Pregnancies / OR 40% 22,0% 13,4%
Pregnancies / ET 50% 28,1% 13,6%
* - frequency of aCGH-PGS cancelation – 34,4%Mykytenko DO, Zukin VD. 1st BRM meeting, 2012

Low Y signal
18

Low Y signal
19

aCGH-PGS for different groups of patients
20
Pro
gno
sis
for
ET a
nd
pre
gnan
cyaf
ter
aCG
H-P
GS
Good
Poor
Egg donors
Young women with good ovarian response
Couples with male factor
Women with age factor
Poor ovarian response
Carriers of the chromosomal rearrangements

PGD/PGS: aCGH vs other technologies
Criterion aCGH SNP array Next-Gen Sequencing
QF-PCR/PCR
FISHPGS
Comprehensive chrom. screening
+ + + - -
Balancedaberrations
- - ? - Limited
Nonbalancedabberations
+ + + + +
Microdeletionsyndromes
Limited + + + +
UPD - + + - -
Single Gene disorders
- +/- + + -
21

Future directions• arrayCGH will compete with SNP-arrays and next-
gen. sequencing-based methods in the range of the same indications to testing
• FISH-method will not die out (at least in close and middle future) due to different indication to testing
22
• Further investigations will be directed to:•comparison of the arrayCGH results with embryo morphokinetics and ‘–omics’ characteristics•development of the accurate criterions for the selective ET

Conclusions
• PGS/PGD testing allows us to increase the performance of ART technologies and to reduce the amount of unsuccessful ET.
• Among all similar PGS-methods, array-Comparative Gnomic Hybridization seems to be the most suitable approach to detect the embryo aneuploidy.
• Performing of aCGH-PGS with the number of embryos less than 3 is inappropriate.
• aCGH should not be the cause of ungrounded rejection of the normal embryo!
23


















