Journal of Medical Genetics (1973). 10, 309. Myoglobin in Primary Muscular Disease I. Duchenne Muscular Dystrophy and II. Muscular Dystrophy of Distal Type A. E. ROMERO-HERRERA,* H. LEHMANN,* B. E. TOMLINSON,t and J. N. WALTONt Summary. Skeletal myoglobin from two cases of muscular dystrophy, one of Duchenne muscular dystrophy, and one of muscular dystrophy of distal type, have been examined and no differences from normal human myoglobin were found. The opportunity has been taken to discuss the nature of minor fractions of myoglobin- like material which are found when human skeletal myoglobin is isolated. Those which have been observed in the present study have been artefacts and it was pos- sible to demonstrate that they were due to deamidation of certain glutamine and asparagine residues. In recent years we have purified and analysed the skeletal myoglobin of man to complete its amino- acid sequence (Romero-Herrera and Lehmann, 1971a and b; 1972a), where it had not already been described by Hill et al (1969). This knowledge has supported: (1) The identifi- cation of mutants of human skeletal myoglobin found by Huntsman and Boulton in an electro- phoretic survey of 10,000 human muscle samples (Boulton et al, 1969; Boulton et al, 1971a, b, and c) of which the second is presumably identical with one described by Boyer, Fainer, and Naughton (1963). (2) The comparison of man's skeletal and cardiac myoglobin and to show that they were identical (Romero-Herrera and Lehmann, 1971a). (3) An evolutionary study of primate myoglobins (Romero-Herrera and Lehmann, 1971b, 1972a and b; 1973a, b, and c). (4) An investigation in detail of the myoglobin of two patients who had died of primary muscular disease, which is the subject of this paper. Received 6 June 1973. * Medical Research Council Abnormal Haemoglobin Unit, Uni- versity of Cambridge, Department of Biochemistry, Addenbrooke's Hospital, Cambridge CB2 2QR. t Department of Pathology, Newcastle General Hospital, New- castle upon Tyne NE4 6BE. $ Regional Neurological Centre, Newcastle General Hospital, Newcastle upon Tyne NE4 6BE. This last quest followed logically from the experi- ence with abnormal haemoglobin. Nearly 200 haemoglobin variants are known (Lehmann, 1972). Most of them are compatible with the normal func- tion of the erythrocytes. An increasing number, however, are found to be, associated with some change in the function of the haemoglobin molecule which causes a haematological disorder. The most important abnormal variant is sickle-cell haemoglo- bin whose solubility is abnormally low in the deoxy- genated state; other abnormal haemoglobins are permanent methaemoglobin, others show ab- normally high or abnormally low oxygen affinities, and still others cause haemolytic anaemia by their tendency to denature easily into Heinz bodies which affect the life span unfavourably (Morimoto, Lehmann, and Perutz, 1971). The rate of synthesis is below normal in a number of variants (White, 1972). Most of these pathological haemoglobins show more than one of the abnormalities listed. The importance of myoglobin for the function of the muscle is not as obvious as that of haemoglobin for the red blood cell. There can, however, be no doubt of its physiological role as a short and long term oxygen store and its help in facilitating the diffusion of oxygen (Wittenberg, 1959 and 1965; Scholander, 1960a and b, and 1965); the first is indisputable when one considers the metabolism of diving mammals (Scholander, 1961/1962). 09 copyright. on December 28, 2019 by guest. Protected by http://jmg.bmj.com/ J Med Genet: first published as 10.1136/jmg.10.4.309 on 1 December 1973. Downloaded from
Transcript
Journal of Medical Genetics (1973). 10, 309.
Myoglobin in Primary Muscular DiseaseI. Duchenne Muscular Dystrophy
and
II. Muscular Dystrophy of Distal TypeA. E. ROMERO-HERRERA,* H. LEHMANN,* B. E. TOMLINSON,t and
J. N. WALTONt
Summary. Skeletal myoglobin from two cases of muscular dystrophy, one ofDuchenne muscular dystrophy, and one of muscular dystrophy of distal type, havebeen examined and no differences from normal human myoglobin were found. Theopportunity has been taken to discuss the nature of minor fractions of myoglobin-like material which are found when human skeletal myoglobin is isolated. Thosewhich have been observed in the present study have been artefacts and it was pos-sible to demonstrate that they were due to deamidation of certain glutamine andasparagine residues.
In recent years we have purified and analysed theskeletal myoglobin of man to complete its amino-acid sequence (Romero-Herrera and Lehmann,1971a and b; 1972a), where it had not already beendescribed by Hill et al (1969).
This knowledge has supported: (1) The identifi-cation of mutants of human skeletal myoglobinfound by Huntsman and Boulton in an electro-phoretic survey of 10,000 human muscle samples(Boulton et al, 1969; Boulton et al, 1971a, b, and c)of which the second is presumably identical withone described by Boyer, Fainer, and Naughton(1963). (2) The comparison of man's skeletal andcardiac myoglobin and to show that they wereidentical (Romero-Herrera and Lehmann, 1971a).(3) An evolutionary study of primate myoglobins(Romero-Herrera and Lehmann, 1971b, 1972a andb; 1973a, b, and c). (4) An investigation in detailof the myoglobin of two patients who had died ofprimary muscular disease, which is the subject ofthis paper.
Received 6 June 1973.* Medical Research Council Abnormal Haemoglobin Unit, Uni-
versity of Cambridge, Department of Biochemistry, Addenbrooke'sHospital, Cambridge CB2 2QR.
t Department of Pathology, Newcastle General Hospital, New-castle upon Tyne NE4 6BE.
$ Regional Neurological Centre, Newcastle General Hospital,Newcastle upon Tyne NE4 6BE.
This last quest followed logically from the experi-ence with abnormal haemoglobin. Nearly 200haemoglobin variants are known (Lehmann, 1972).Most of them are compatible with the normal func-tion of the erythrocytes. An increasing number,however, are found to be, associated with somechange in the function of the haemoglobin moleculewhich causes a haematological disorder. The mostimportant abnormal variant is sickle-cell haemoglo-bin whose solubility is abnormally low in the deoxy-genated state; other abnormal haemoglobins arepermanent methaemoglobin, others show ab-normally high or abnormally low oxygen affinities,and still others cause haemolytic anaemia by theirtendency to denature easily into Heinz bodieswhich affect the life span unfavourably (Morimoto,Lehmann, and Perutz, 1971). The rate of synthesisis below normal in a number of variants (White,1972). Most of these pathological haemoglobinsshow more than one of the abnormalities listed.The importance of myoglobin for the function of
the muscle is not as obvious as that of haemoglobinfor the red blood cell. There can, however, be nodoubt of its physiological role as a short and longterm oxygen store and its help in facilitating thediffusion of oxygen (Wittenberg, 1959 and 1965;Scholander, 1960a and b, and 1965); the first isindisputable when one considers the metabolism ofdiving mammals (Scholander, 1961/1962).
The myoglobin concentration increases with ageand exercise (Whipple, 1926; Lawrie, 1953) and itslevel is twice as high in hunting than in domesticdogs. Altitude favours a rise in myoglobin con-centration (Hurtado et al, 1937; Poel, 1949; Clark,Criscuolo, and Coulson, 1952; Vaughn and Pace,1956; Tappan and Reynafarje, 1957; Anthony,Ackerman, and Strother, 1959; Reynafarje andMorrison, 1962), but it has been suggested that thismostly represents a change in muscle hydration(Anthony et al, 1959), and even a decrease of myo-globin at high altitude is explained by the lowmuscular activity (Poel, 1949); the opposite hap-pens if the animals are exercised during acclimatiza-tion (Clark et al, 1952). One might expect thathibernation might cause the myoglobin to fall; how-ever, it has been reported to rise in the snowshoehare (Rosenmann and Morrison, 1965), and thenorthern red-backed vole (Morrison, Rosenmann,and Sealander, 1966). At present, it is difficult tointerpret a report that the myoglobin of rats keptfor one to three months at an altitude of 6000 m,changes its equilibrium constant by a factor of two(Strother et al, 1959), however, not so long ago,so would such an observation on haemoglobinwhich would now be understood more easily(Benesch and Benesch, 1969; Perutz, 1970; Arnone,1972).The myoglobin of some molluscs has been re-
ported to form dimers and to exhibit slight haem-haem interaction (Manwell, 1960) and to containcysteine which combined into dimers linked bydisulphide bonds (Terwilliger and Read, 1970).Mammalian myoglobins, most of which do not con-tain cysteine, have nevertheless been shown to formdimers in vitro (van der Oord et al, 1969).Perhaps a powerful argument for the physiological
need for normal myoglobin is that no case has everbeen seen of an obvious myoglobin deficiency. Also,no permanent methaemoglobin caused by a globinabnormality has been described, although newobservations of human 'haemoglobin M' regularlyoccur, with a proportion of these being almostcertainly new mutations (Farmer, Lehmann andRaine, 1969). Mutations of myoglobin likely tocause primary muscular disease would have tocause subtle changes which would not be expectedto alter the myoglobin molecule too obviously and,whilst impairing its normal efficiency, would yetpermit some residual function. These changeswould resemble those that are found in somehaemoglobins with high or low oxygen affinity and/or mild instability. They are mutations whichaffect amino-acid side chains in the interior of themolecule, but the resulting difference from the
normal molecule is not very obvious and wouldperhaps merely be an alteration in the size of a sidechain but not in its polarity or charge. Such adifference would not be easily detected by routinesurveys using electrophoresis and chromatography.The identification of such mutants would thereforerequire a detailed determination of the amino-acidcomposition of the molecule broken up into frag-ments not larger than about 20 residues.
Case ReportsCase 1. J.L., a male born on 23 November 1955, was
first seen by one of us (J.N.W.) on 11 July 1960. Hewas the second child of healthy, unrelated parents andthere was no family history of muscle disease. An eldersister, then aged 8 years, was perfectly normal. Theparents said that ever since this boy had walked at theage of 15 months, he had been unable to run and couldnot climb stairs properly. When he was seen at the ageof 4 he still climbed stairs on his hands and knees andhis parents said that he tried to run like a long-distancewalker walking at speed. He frequently fell and haddifficulty in rising from the floor. His parents had notbeen aware of any weakness of the arms. He had,however, shown some delay in the development ofspeech.On examination there was evidence suggesting some
degree of mild mental retardation, but this was not con-firmed by later psychological testing which gave an IQ of100. The patient walked with a markedly accentuatedlumbar lordosis and with a waddling gait. There wasenlargement of the calves. In the upper limbs there wasbilateral winging of the scapulae with weakness of thepectorals and biceps. In the lower limbs the quadriceps,hip flexors and anterior tibial muscles were particularlyweak. The knee jerks were diminished, the ankle jerkswere brisk, and the plantar responses were flexor.
Estimation of the serum aldolase at that stage gave aresult of 110 units/ml. Electromyography and musclebiopsy were refused. In 1964 the patient was includedin a series of cases receiving a trial of treatment withLaevadosin but obtained no benefit from this. By 1965he required a wheelchair as he was then unable to walk.In 1963 two estimations of the serum creatine kinasegave results of, 230 and 172 units/ml, respectively; afirm diagnosis ofDuchenne type muscular dystrophy wasmade. In 1968, because of increasing scoliosis, he wasprovided with a spinal support. In 1970 he developed amoderately severe endogenous depression which re-sponded to treatment with phenelzine. Despite the pro-vision of a brace, he went on to develop a severe kypho-scoliosis. In June 1971 he was seen to be deterioratingrapidly and by September ofthe same year had developedsevere respiratory insufficiency. On 11 October 1971 hedied suddenly while being transferred from an ambulanceto a wheelchair on his way to attend hospital clinic.
Necropsy showed extreme wasting (total body weight36 kg) of all the musculature, marked contractures oflimbs, and extreme kyphoscoliosis with the anterior pelvicbrim as high as the lower ribs anteriorly.A little clear frothy fluid was present in the trachea and
main bronchi accompanied by a small amount of oedemaof both lungs. The heart was considerably enlarged,weighing 380 g. The pericardial cavity containedapproximately 20 ml of clear, slightly yellow fluid andthe surface of the left and right ventricles showed markedfibrous striations, these running in the lines of the super-ficial cardiac fibres, an appearance which we have cometo regard as typical of the so-called cardiomyopathywhich commonly terminates long surviving cases ofDuchenne muscular dystrophy. All parts of the leftand right ventricles and the interventricular septum wereinvolved by fibrosis, this being particularly severe in thesub-epicardial layers of the left side. The papillarymuscles of the mitral valve were both somewhat thinnedand showed small patches of fibrosis. The other heartvalves and the atria and auricles showed no abnormality.The coronary arteries were thin walled, entirely patentvessels showing only minimal traces of subintimalatheroma.No abnormalities were present in the peritoneal cavity
apart from the very gross distortion produced by thekyphoscoliosis.The scalp, skull, and brain appeared normal, the latter
both to the naked eye and in sample sections. Skeletalmuscles varied greatly in appearance; the lumbar, theanterior, and posterior muscles of the neck were pale butotherwise not grossly abnormal. The muscles of bothpelvic and shoulder girdles and, to the naked eye,the distallimb muscles were reduced largely to small masses of fat,delineated by muscle sheaths.
Histologically all the numerous limb muscles examinedshowed severe dystrophic changes. There was massivereplacement of the majority of muscles by fat with con-
siderable production of fibrous tissue often enclosing orseparating surviving islands of individual muscle fibres.Marked variation in muscle fibre size was present, manygiant fibres showing central nuclei as well as extremelysmall atrophic muscle fibres. Very occasional baso-philic muscle fibres were present and occasional fociwhere degenerating fibres appeared to be associated withactive phagocytosis. No suggestion of grouped fibreatrophy was seen in any section from any muscle.The myocardium showed extensive patchy fibrosis,
particularly severe throughout the left ventricle.The spinal cord was examined at all levels, and the
entire lumbosacral cord in great detail. The motorneurones throughout the lumbosacral enlargement werecounted in serial sections in the manner described byTomlinson, Irving, and Rebeiz (1973), thus establishingthat limb motor neurones were present in normal num-
bers.
Case 2. (D.W.) This man, who was born in 1927,was well until the age of 25 years when he began to sufferfrom progressive weakness of the distal muscles of boththe upper and lower limbs. Weakness first affected the
anterior tibial and calf muscles in the legs, giving initi-ally a moderate degree of footdrop, and some two orthree years later the patient noted weakness of the longfinger flexor and extensor muscles in the upper limbs. Hisfather suffered from a similar progressive neuromusculardisease beginning at approximately the age of 25 years,but suffered an attack of subarachnoid haemorrhage atthe age of 34 years and died after a further attack at theage of 39 years. The patient's patemal grandfather hadalso been similarly affected and had died while in hisfifties from a condition then diagnosed as progressivemuscular atrophy; at this age he had still been able towalk, though with some difficulty. There was noevidence that any other members of the family had beenaffected.When first seen by one of us (J.N.W.) in 1958, there
was evidence of distal weakness of muscles in both theupper and lower limbs involving the long flexors andextensors ofthe fingers in the upper limbs but sparing thesmall hand muscles. In the lower limbs the anteriortibial muscles and those of the calves were selectivelyinvolved, but there was some evidence of weaknessextending to involve quadriceps and hamstrings in thelower limbs and biceps and triceps in the upper limbs.The clinical picture was thought tobe one suggestive ofanatypical form of peroneal muscular atrophy, though theproximal muscle involvement was not compatible withthis diagnosis. At that time an electromyogram showedevidence of many short-duration and polyphasic poten-tials in the distal muscles of both the upper and lowerlimbs, and nerve conduction velocity measurement wasnormal. No sensory loss was evident and the diagnosiswas revised to one of muscular dystrophy of the distalvariety.
Subsequently the patient's condition showed slow butintermittent deterioration; despite his disability he con-tinued to work as a land agent for the National CoalBoard. In 1963 he became unable to walk and was con-fined to a wheelchair. On admission to hospital on 23October 1967 he was an intelligent and energetic man.The facial and bulbar musculature was entirely normal.The stemomastoids were, however, weak and wasted andthere was generalized proximal and distal weakness of allthe upper limb muscles, involving particularly deltoids,infraspinati and the flexors and extensors of the fingers.The tendon reflexes in the upper limbs were, however,present. In the lower limbs there was generalizedweakness of all muscle groups with some minimal pre-servation of toe movement, but all tendon reflexes andthe plantar responses were absent. Again there was nosensory loss. The heart was normal on examination.
Investigations at that time showed Hb 15-9 g/100 ml,PCV 50%, leucocytes 7200/mm3, ESR 8 mm/i hr,serum electrolytes normal, SGOT 31 units/ml, SGPT32 units/ml, serum aldolase 2-8 milli-units/ml, serumcreatine kinase 75 IU/l; the blood uric acid, alkalinephosphatase, calcium phosphate, and total protein wereall normal. An electrocardiogram showed a slightlyincreased PR interval with some ST segment depressionand therewere episodes of sinoatrial block. A repeat elec-tromyogram showed evidence of myopathy in proximal
limb muscles, together with fibrillation potentials,pseudomyotonic discharges and occasional possiblefasciculation potentials. In the distal muscles therewas some evidence of large motor units with a reducedinterference pattern suggesting neurogenic atrophy. Anintravenous pyelogram on this admission showed acalculus at the lower end of the left ureter with normalrenal function and structure, and this was subsequentlyremoved on cystoscopy.A muscle biopsy on 30 October 1967 was taken from
the right extensor digitorum brevis muscle and was re-ported upon by Dr P. Hudgson. The fascicular archi-tecture of the muscle was generally well preserved andthe individual fibres, though showing very marked vari-ation in diameter, showed no necrosis or phagocytosis.There was a gross increase in the amount of both peri-mysial and endomysial fibrous connective tissue, so thatthe surviving fibres were embedded in a sea of connectivetissue. There was no evidence of fatty infiltration. Afew fibrotic muscle spindles were seen and there werenumerous intramuscular nerves in the transverse sec-tions, but these appeared to be normal histologically.The only abnormality therefore was the widespreadperimysial and endomysial fibrosis. The variation inmuscle fibre diameter was regarded as being probablysignificant. Dr Hudgson commented that the changeswere undoubtedly myopathic, but at this late stage it wasimpossible to determine whether the primary diseasewas a myopathy or whether one was dealing with a long-standing neurogenic atrophy with secondary myopathicchange.
In the light of the somewhat equivocal findings oninvestigation in this case, the diagnosis at this stage wasrevised to one of spinal muscular atrophy showing someresemblance to the scapuloperoneal variety.The patient was re-admitted to hospital in February
1968 because of an attack of left lower lobe pneumoniabut made a good recovery. In 1970 he became nolonger able to drive his car and was provided with anelectrically-operated wheelchair. In 1971 for the firsttime he was showing some evidence of mild bilateralfacial weakness, and in March of that year was beginningto show evidence of respiratory insufficiency with ortho-pnoea. He was provided with POSSUM equipment.In September of that year he had an episode of profoundhypotension with transient loss of consciousness afterdrinking two glasses of gin. A repeat electrocardiogramshowed frank ST depression in lead 2 and AVF withdeeply inverted T waves, but there was no evidence ofrecent myocardial ischaemia. In October 1971 it wasfound that the patient was waking at night with frequentepisodes of CO2 retention and breathlessness. Hishaemoglobin was found to be 17-3 g/100 ml with a PCVof 51-6%. A repeat electrocardiogram in late October1971 showed an intermittently wandering pacemakerwith prolonged atrioventricular conduction and occa-sional ventricular ectopic beats. The P wave was broadand bifid, indicating left hypertrophy, and there waswidespread ST segment depression and T wave changesall compatible with cardiac ischaemia, but many of thefeatures were also regarded as being compatible with a
cardiomyopathy. The blood was normal, but the bi-carbonate was elevated to 34 mEq/l, which was thoughtto be a reflection of the respiratory alkalosis. At thisstage the possibility ofassisted respiration was considered,but the patient preferred to try to manage at home with-out such help for the time being. However, he diedsuddenly at home during the night on 9 November 1971,presumably as a result of respiratory insufficiency.At necropsy he appeared a well nourished man, 178 cm
tall and weighing 76 kg, with marked rounding of thelimbs through which actual muscle shape could not bediscerned. Apart from the diseased muscles the majorabnormality at necropsy was in his heart. This weighed370 g and throughout all parts of the left ventricle (whichaveraged 1-6 cm in thickness) and the left side of theinterventricular septum, small foci of fibrosis, poorlydelineated but present in very large numbers and measur-ing up to 5 mm across could be seen. The valves,atria, and right ventricle appeared normal and no massivescarring was present. The coronary arteries were patent,thin walled vessels showing only minute flecks of athe-roma and the rest of the major arteries and the aorta,except in the lower abdomen, were strikingly free ofatheroma.To the naked eye, voluntary muscles were largely
replaced by fat; only the major muscles of the neck andthe temporalis appearing normal. The trunk and proxi-mal limb muscles were unrecognizable as muscle tissue,and the distal limb muscles only slightly better preserved.Multiple muscle sections showed extensive myopathicchanges with severe fat replacement and in some musclesconsiderable fibrosis; many muscles, however, showedchanges entirely consistent with a primary dystrophy.Marked variation of fibre size with many minute fibresand numerous hypertrophied, rounded fibres with cen-tral nuclei constituted the most prominent features;occasional vacuolated or basophilic fibres and some areasof macrophage accumulation were present. Only in asection from sternomastoid were there clusters of atro-phic fibres which might have raised the possibility of anelement of neuronal atrophy.The spinal cord, which appeared normal to the naked
eye was again extensively examined, and the numbers oflimb motor neurones in the lumbosacral enlargementcounted, and established as being at the lower limit ofnormal compared with a small group of controls. Thisfinding entirely eliminated the possibility that this casewas one ofmotor neurone disease.
ConclusionThe first case was therefore one of Duchenne
dystrophy both clinically and pathologically. Thesecond, though presenting a difficult diagnosticclinical problem, was established at necropsy to be acase of muscular dystrophy of distal type. Thesecases are included in an account of the spinal cord inmuscular dystrophy to be published by Tomlinson,Walton, and Irving (1974).
MethodsThe identification of the myoglobin followed tech-
nically the method described briefly in our first publica-tion on the amino-acid sequence of parts of human myo-globin (Romero-Herrera and Lehmann, 1971a), whichwas extended in our reports of some primate myoglobin,notably those of Old World monkeys (Romero-Herreraand Lehmann, 1972b). To summarize: the muscle washomogenized in a blender with 1-5 mM KCN at 4° C.After filtering through muslin the residue was extractedtwice more and the combined filtrates mixed at roomtemperature with 1-5 v/v saturated ammonium sulphate;after one hour the precipitate was filtered off throughWhatman paper No. 1. The filtrate was concentratedand the ammonium sulphate removed by pressure filtra-tion through an Amicon PM30 membrane and applied toa Sephadex G25 column, eluted with 0 05 M TRIS HC1buffer, pH 8-5, followed by the separation of myoglobinby chromatography on a DEAE Sephadex A50 columnwith a linear gradient, pH 8-5-6-0; the buffer used was0 05 M TRIS-HCI (Huisman and Dozy, 1965), with thestarting buffer containing 2mM KCN. The myoglobinfraction was collected, concentrated under vacuum, andsubmitted to repeated discontinuous paper electro-phoresis (Graham and Grunbaum, 1963), until therewas no other protein seen after staining the paper with'light green'. The purified myoglobin was then elutedwith 1-5 mM KCN, concentrated in vacuo in a sartoriouscollodion bag until it was approximately 10%. Thehaem was removed, and the globin precipitated (Ingramand Stretton, 1962). The two globin samples were theninvestigated differently.
Case 1. The globin was first treated with cyanogenbromide (CNBr) following the method of Gross andWitkop (1962) and thereby split into four fragments atthe three methionine residues. These were then submit-ted to.chymotryptic digestion (Sick et al, 1967), and the
resulting peptides were separated by two-dimensional,high voltage paper electrophoresis and chromatography(fingerprinted). Small amounts of globin (1-4 mg) wereused to prepared 'diagnostic' fingerprints. They werefirst examined under ultraviolet light to locate trypto-phan containing peptides and stained with 0 2% nin-hydrin in acetone (v/v) to visualize all peptides present,they were then stained specifically for methionine, argi-nine, histidine, tyrosine, andtryptophan (Romero-Herreraand Lehmann, 1972b). This made it possible to ascer-tain that only peptides belonging to myoglobin werepresent. Preparative fingerprints, from which thesepeptides were to be used for analysis, were made from5 mg of globin, examined under the ultraviolet light, andstained lightly with 0-02% ninhydrin in acetone (v/v)to indicate the location of the peptides which were thencut out and eluted with 6N HC1. The eluates werehydrolysed in sealed tubes heated at 1080 C for 24 hours.For one peptide which contains an Ile-Ile sequencehydrolysis was also carried out for 72 hours. Thehydrolysates were dried in a vacuum desiccator, and theircomposition determined in an automatic amino-acidanalyser.
Case 2. The globin was aminoethylated (Clegg,Naughton, and Weatherall, 1966), digested with trypsin(Sick et al, 1967), and those tryptic peptides which wereinsoluble were treated with pepsin. Both tryptic andpeptic peptides were fingerprinted and analysed asdescribed above for case 1.
ResultsFigs. 1 and 2 show the DEAE Sephadex elution
pattern of the preparation from which most of thenon-haem proteins had been removed by ammoniumsulphate precipitation, followed by the removal ofthis salt by pressure filtration.
FIG. 1. Elution pattern (DEAE Sephadex, pH 8 8-7-5) of an extract of normal humanskeletal muscle from which a large amount of non-haem proteins have been removedpreviously by treatment with saturated ammonium sulphate 6:4 v/v. Fraction 1 ismyoglobin. (For other details see text.)
FIG. 2. Elution pattern as in Fig. 1 of material from skeletal muscleof case 1. A = myoglobin; D = haemoglobin A; E = haemoglobinKoellicker. (For details see text.)
Minor Fractions. Fig. 1 shows the patternobtained from normal muscle, and Fig. 2 that fromthe muscle of patient 1. (The DEAE Sephadexelution pattern from patient 2 had the same
characteristics.) Fractions 2 and 3 in Fig. 1 and Bin Fig. 2 represent small amounts of contaminatingnon-haem proteins. Fractions 1 and A, respectively,are the major myoglobin fractions, 5 and D are
haemoglobin A, and 6 and E haemoglobin Koellicker(Marti, Beale, and Lehmann, 1967). This is a
degradation product derived from normal haemo-globin on post-mortem haemolysis, by the removalof the C-terminal arginine of the a-chain by theenzyme carboxy-peptidase B of the plasma.Fractions 4 and C, though red in colour, containsome non-haem protein plus some deamindatedmyoglobin which is an artefact. There is presentyet another artefact from deamidation of myoglobinwhich by this method (but not others) is eluted withhaemoglobin Koellicker.To complete the purification of the myoglobin, a
non-haem protein has to be removed which elutestogether with myoglobin by DEAE Sephadex chro-matography. This is done by concentrating theeluate and submitting it to discontinuous paperelectrophoresis at pH 8-6 cathode-9 1 anode. Bythis method the non-myoglobin protein moves
behind the myoglobin towards the positive pole.At the same time small amounts of deamidatedmyoglobin appear as minor fractions (Fig. 3),and for their chemical characterization repeatedelution of the main fraction from paper, followed by
FIG. 3. Paper electrophoresis of the myoglobin band isolated byDEAE Sephadex chromatography (see Fig. 2) of case 1. Twoelectrophoreses are shown.
(1) First electrophoresis, on the left the unstained myoglobin, on
the right part of the same strip stained for proteins. In addition to
the myoglobin other proteins are present. (A indicates the most im-portant of these.)
(2) Re-electrophoresis of the myoglobin band of strip 1. Inaddition to the original myoglobin (B) a new red coloured fraction (C)has been formed on elution and concentration of band (B) from strip1. It now moves faster towards the anode than normal myoglobin,and was not present in the original specimen.
concentration and re-electrophoresis was required toobtain enough artefactual material.From the retention time of the DEAE Sephadex
deamidated myoglobin which elutes with haemo-globin Koellicker, it can be concluded that it hasacquired additional negative charges. One of thesewas identified, but the other was in the insolubleprecipitate left after tryptic digestion. This materialcould only be obtained in adequate amounts by re-
peated electrophoresis.
Minor Fractions arising as Artefacts fromDeamidations.
Not all deamidations were found in all prepara-tions. The artefact with the change 152 Gln-÷Glu,only appeared on DEAE Sephadex chromatography.As mentioned above, on chromatography, anotherartefact was obtained. It was at very low concen-tration, and its retention time indicated thepresence of two deamidations. One of these was91 Gln-+Glu, the other had to be the insoluble pre-cipitate left after tryptic digestion, presumably atresidues 12 or 116, but not enough material wasobtained for identification.On paper, one of the deamidations was at residue
91 Gln--Glu (see Fig. 3, band C). In fact anotherband more negatively charged than band C, and atverylowconcentration,which from its electrophoreticmigration should have contained two deamidationsshowed, on fingerprinting, three 91 Gln- Glu,and two in the insoluble core: 12 Asn->Asp and116 Gin--Glu. Presumably this minor fraction was
NOWtAL
79-96 80-96DEAtDATED91OLN-GLU
a mixture of two degradations 91 Gln-+Gly plus12 Asn--Asp, and 91 Gln->Glu plus 116 Gln-+Glu.This was substantiated by the complete absence ofthe tryptic peptide containing 91 Gln, and the partialabsence of the peptic peptide containing 12 Asn and116 Gln in this fraction. Hence although therewere three deamidations found in this fast myoglo-bin band, only two positions 91 and 12 and 91 and116 respectively were affected in one molecule at onetime (see Figs. 4a and 4b).
Main Myoglobin Fractions. Fig. 5 shows thefingerprint of the chymotryptic peptides of themyoglobin previously treated with CNBr, from thepresent case 1. By this method all myoglobinpeptides including those from the insoluble coreremaining after tryptic digestion are present, be-cause partial conversion of the cysteine at position110 into cystic acid during CNBr treatment allows
NORMAL148-153
pH 6.5 +
DEAMIATED1L8-153
152 GLN-vGLU
-Y0
FIG. 4a. Composite chromatogram (fingerprint) of tryptic peptides showing the exact position of the newartefactual peptides which contain deamidated residues at positions 91 and 152.
NORMAL12-16
NORMAL114-118\ -
NORMAL116-11 '-
.
oO
0
DEAMDATED12-16aH12ASN-ASPO
DEAMIDATED114 118 O
116 GLN-GW DEADT( 116-118
116GLN-vGLU
pH 6.5 +
FIG. 4b. Composite fingerprint of the peptic peptides made from insoluble material left after tryptic digestion.The position of peptic peptides which arose as a result of deamidation at residues 12 and 116 are shown. (Fordetails see text.)
FIG. 5. Fingerprint of the chymotryptic peptides from the myoglobin from case 1, which had previously beentreated with CNBr. The specific staining reactions are indicated. * is the point of application.
17-31ARG
515-56
oQ78140
HISMET- \119-133
FIG. 6. Fingerprint of the tryptic peptides of the myoglobin from case 2 which had previously been anino-ethylated. The specific staining reactions are indicated. * is the point of application.
the peptide residues 104-115 to be soluble. Thefingerprint pattern and the staining reactions were
the same as those found for normal myoglobin.Nineteen selected peptides accounting for the 153residues of the whole myoglobin molecule, were
eluted, hydrolysed, and their amino-acid composi-tion determined. The results are shown in Table I.
No differences from normal myoglobin in theiramino-acid composition were found.
Fig. 6 shows the fingerprint of the soluble trypticpeptides of myoglobin from case 2, which had beenpreviously modified by aminoethylation. The pep-tide chromatogram pattern and staining reactionswere indistinguishable from those of normal myo-
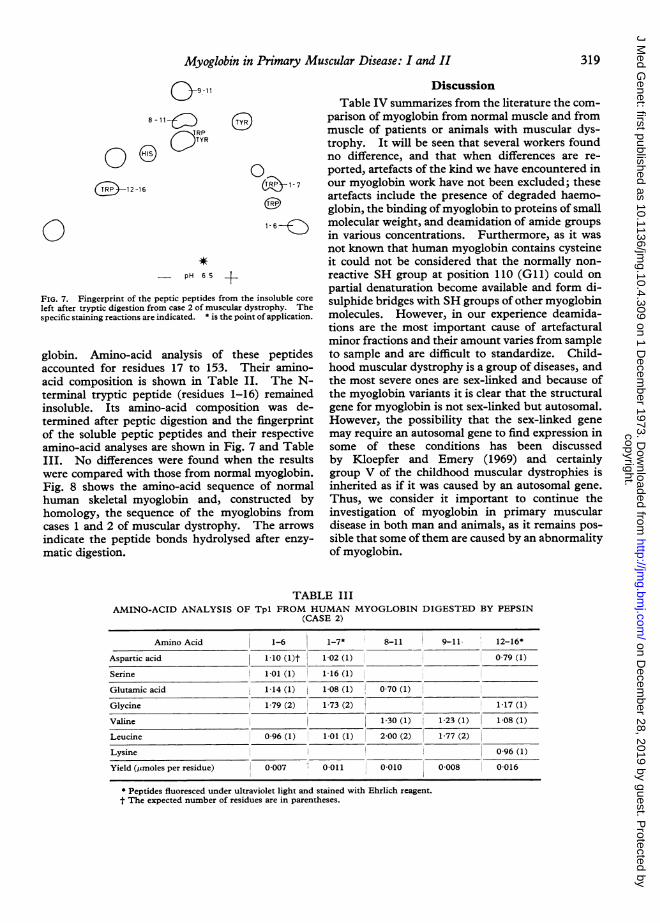
FIG. 7. Fingerprint of the peptic peptides from the insoluble core
left after tryptic digestion from case 2 of muscular dystrophy. Thespecific staining reactions are indicated. * is the point of application.
globin. Amino-acid analysis of these peptidesaccounted for residues 17 to 153. Their amino-acid composition is shown in Table II. The N-terminal tryptic peptide (residues 1-16) remainedinsoluble. Its amino-acid composition was de-termined after peptic digestion and the fingerprintof the soluble peptic peptides and their respectiveamino-acid analyses are shown in Fig. 7 and TableIII. No differences were found when the resultswere compared with those from normal myoglobin.Fig. 8 shows the amino-acid sequence of normalhuman skeletal myoglobin and, constructed byhomology, the sequence of the myoglobins fromcases 1 and 2 of muscular dystrophy. The arrows
indicate the peptide bonds hydrolysed after enzy-matic digestion.
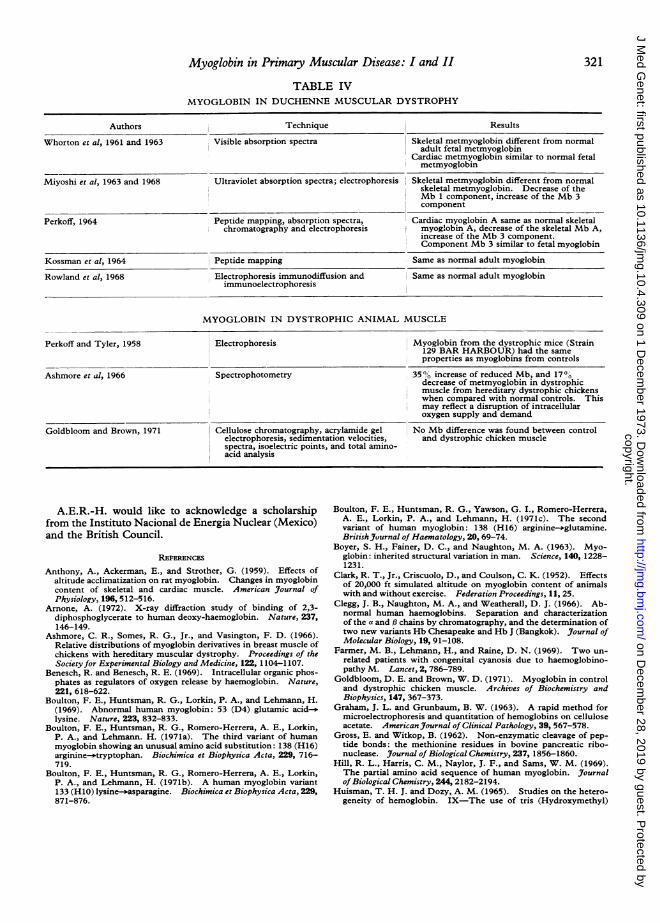
DiscussionTable IV summarizes from the literature the com-
parison of myoglobin from normal muscle and frommuscle of patients or animals with muscular dys-trophy. It will be seen that several workers foundno difference, and that when differences are re-
ported, artefacts of the kind we have encountered inour myoglobin work have not been excluded; theseartefacts include the presence of degraded haemo-globin, the binding of myoglobin to proteins of smallmolecular weight, and deamidation of amide groups
in various concentrations. Furthermore, as it wasnot known that human myoglobin contains cysteineit could not be considered that the normally non-
reactive SH group at position 110 (Gll) could on
partial denaturation become available and form di-sulphide bridges with SH groups of other myoglobinmolecules. However, in our experience deamida-tions are the most important cause of artefacturalminor fractions and their amount varies from sampleto sample and are difficult to standardize. Child-hood muscular dystrophy is a group of diseases, andthe most severe ones are sex-linked and because ofthe myoglobin variants it is clear that the structuralgene for myoglobin is not sex-linked but autosomal.However, the possibility that the sex-linked gene
may require an autosomal gene to find expression insome of these conditions has been discussedby Kloepfer and Emery (1969) and certainlygroup V of the childhood muscular dystrophies isinherited as if it was caused by an autosomal gene.
Thus, we consider it important to continue theinvestigation of myoglobin in primary musculardisease in both man and animals, as it remains pos-
sible that some ofthem are caused by an abnormalityof myoglobin.
TABLE IIIAMINO-ACID ANALYSIS OF Tpl FROM HUMAN MYOGLOBIN DIGESTED BY PEPSIN
Myoglobin in Primary Muscular Disease: I and II 321
TABLE IVMYOGLOBIN IN DUCHENNE MUSCULAR DYSTROPHY
Authors Technique Results
Whorton et al, 1961 and 1963 Visible absorption spectra Skeletal metmyoglobin different from normaladult fetal metmyoglobin
Cardiac metmyoglobin similar to normal fetalmetmyoglobin
Miyoshi et al, 1963 and 1968 Ultraviolet absorption spectra; electrophoresis Skeletal metmyoglobin different from normalskeletal metmyoglobin. Decrease of theMb 1 component, increase of the Mb 3component
Perkoff, 1964 Peptide mapping, absorption spectra, Cardiac myoglobin A same as normal skeletalchromatography and electrophoresis jmyoglobin A, decrease of the skeletal Mb A,
increase of the Mb 3 component.Component Mb 3 similar to fetal myoglobin
Kossman et al, 1964 Peptide mapping Same as normal adult myoglobin
Rowland et al, 1968 Electrophoresis immunodiffusion and Same as normal adult myoglobinimmunoelectrophoresis
MYOGLOBIN IN DYSTROPHIC ANIMAL MUSCLE
Perkoff and Tyler, 1958 Electrophoresis Myoglobin from the dystrophic mice (Strain129 BAR HARBOUR) had the sameproperties as myoglobins from controls
Ashmore et al, 1966 Spectrophotometry 35"% increase of reduced Mb, and 17%Odecrease of metmyoglobin in dystrophicmuscle from hereditary dystrophic chickenswhen compared with normal controls. Thismay reflect a disruption of intracellularoxygen supply and demand
Goldbloom and Brown, 1971 Cellulose chromatography, acrylamide gel No Mb difference was found between controlelectrophoresis, sedimentation velocities, and dystrophic chicken musclespectra, isoelectric points, and total amino-acid analysis
A.E.R.-H. would like to acknowledge a scholarshipfrom the Instituto Nacional de Energia Nuclear (Mexico)and the British Council.
REFERENCES
Anthony, A., Ackerman, E., and Strother, G. (1959). Effects ofaltitude acclimatization on rat myoglobin. Changes in myoglobincontent of skeletal and cardiac muscle. American Journal ofPhysiology, 196,512-516.
Arnone, A. (1972). X-ray diffraction study of binding of 2,3-diphosphoglycerate to human deoxy-haemoglobin. Nature, 237,146-149.
Ashmore, C. R., Somes, R. G., Jr., and Vasington, F. D. (1966).Relative distributions of myoglobin derivatives in breast muscle ofchickens with hereditary muscular dystrophy. Proceedings of theSociety for Experimental Biology and Medicine, 122, 1104-1107.
Benesch, R. and Benesch, R. E. (1969). Intracellular organic phos-phates as regulators of oxygen release by haemoglobin. Nature,221, 618-622.
Boulton, F. E., Huntsman, R. G., Lorkin, P. A., and Lehmann, H.(1969). Abnormal human myoglobin: 53 (D4) glutamic acid>-.lysine. Nature, 223, 832-833.
Boulton, F. E., Huntsman, R. G., Romero-Herrera, A. E., Lorkin,P. A., and Lehmann. H. (1971a). The third variant of humanmyoglobin showing an unusual amino acid substitution: 138 (H16)arginine-*tryptophan. Biochimica et Biophysica Acta, 229, 716-719.
Boulton, F. E., Huntsman, R. G., Romero-Herrera, A. E., Lorkin,P. A., and Lehmann, H. (1971b). A human myoglobin variant133 (H10) lysine-easparagine. Biochimica et Biophysica Acta, 229,871-876.
Boulton, F. E., Huntsman, R. G., Yawson, G. I., Romero-Herrera,A. E., Lorkin, P. A., and Lehmann, H. (1971c). The secondvariant of human myoglobin: 138 (H16) arginine-.glutamine.British Journal of Haematology, 20, 69-74.
Boyer, S. H., Fainer, D. C., and Naughton, M. A. (1963). Myo-globin: inherited structural variation in man. Science, 140, 1228-1231.
Clark, R. T., Jr., Criscuolo, D., and Coulson, C. K. (1952). Effectsof 20,000 ft simulated altitude on myoglobin content of animalswith and without exercise. Federation Proceedings, 11, 25.
Clegg, J. B., Naughton, M. A., and Weatherall, D. J. (1966). Ab-normal human haemoglobins. Separation and characterizationof the a and P chains by chromatography, and the determination oftwo new variants Hb Chesapeake and Hb J (Bangkok). journal ofMolecular Biology, 19, 91-108.
Farmer, M. B., Lehmann, H., and Raine, D. N. (1969). Two un-related patients with congenital cyanosis due to haemoglobino-pathy M. Lancet, 2, 786-789.
Goldbloom, D. E. and Brown, W. D. (1971). Myoglobin in controland dystrophic chicken muscle. Archives of Biochemistry andBiophysics, 147, 367-373.
Graham, J. L. and Grunbaum, B. W. (1963). A rapid method formicroelectrophoresis and quantitation of hemoglobins on celluloseacetate. American_Journal of Clinical Pathology, 39, 567-578.
Gross, E. and Witkop, B. (1962). Non-enzymatic cleavage of pep-tide bonds: the methionine residues in bovine pancreatic ribo-nuclease. Journal of Biological Chemistry, 237, 1856-1860.
Hill, R. L., Harris, C. M., Naylor, J. F., and Sams, W. M. (1969).The partial amino acid sequence of human myoglobin. Journalof Biological Chemistry, 244, 2182-2194.
Huisman, T. H. J. and Dozy, A. M. (1965). Studies on the hetero-geneity of hemoglobin. IX-The use of tris (Hydroxymethyl)
amino methane HCI buffers in the anion-exchange chromato-graphy of hemoglobins. Journal ofChromatography, 19,160-169.
Hurtado, A., Rotta, A., Merino, C., and Pons, J. (1937). Studies ofmyohemoglobin at high altitudes. American Journal of the Medi-cal Sciences, 194, 708-713.
Ingram, V. M. and Stretton, A. 0. W. (1962). Human haemoglobinA2. 1: comparison of haemoglobins A2 and A. Biochimica etBiophysica Acta, 62,456-474.
Kloepfer, H. W. and Emery, A. E. H. (1969). Genetic aspectsof neuromuscular disease. In Disorders of Voluntary Muscle,2nd ed., ed. by J. N. Walton, pp. 683-712. Churchill, London.
Kossman, R. J., Fainer, D. C., and Boyer, S. H. (1964). A study ofmyoglobin in disease with comments concerning the myoglobinminor components. Cold Spring Harbor Symposia on Quanti-tative Biology, 29, 375-385.
Lawrie, R. A. (1953). Effect of enforced exercise on myoglobin con-centration in muscle. Nature, 171, 1069-1070.
Lehmann, H. (1972). Die Primarstruktur des Hamoglobins undihre Funktion die Hamoglobin-varianten. In Synthese, Struk-tur und Funktion des Hdmoglobins, ed. by H. Martin and L.Nowicki, pp. 359-379. J. F. Lehmanns Verlag, Munich.
Manwell, C. (1960). Heme-heme interactions in the oxygen equi-librium of some invertebrate myoglobins. Archives of Bio-chemistry and Biophysics, 89, 194-201.
Marti, H. R., Beale, D., and Lehmann, H. (1967). HaemoglobinKoellicker: A new acquired haemoglobin appearing after severehaemolysis-a2 minus 141 Arg 92. Acta Haematologica, 37, 174-180.
Miyoshi, K., Saijo, K., Kuryu, Y., and Oshima, Y. (1963). Abnor-mal myoglobin ultraviolet spectrum in Duchenne type of progres-sive muscular dystrophy. Science, 142, 490-491.
Miyoshi, K., Saijo, K., Kuryu, Y., Oshima, Y., Nakano, M., andKawai, H. (1968). Myoglobin subfractions: abnormality inDuchenne type of progressive muscular dystrophy. Science, 159,736-737.
Morimoto, H., Lehmann, H., and Perutz, M. F. (1971). Molecularpathology of human haemoglobin: stereochemical interpretationof abnormal oxygen affinities. Nature, 232,408-413.
Morrison, P., Rosenmann, M., and Sealander, J. A. (1966). Seasonalvariation of myoglobin in the northern red-backed vole. Ameri-can Journal of Physiology, 211, 1305-1308.
Oord, A. H. A. van der, Wesdorp, J. J., Dam, A. F. van, and Verheij,J. A. (1969). Occurrence and nature of equine and bovine myo-globin dimers. European Journal of Biochemistry, 10, 140-145.
Perkoff, G. T. (1964). Studies of human myoglobin in severaldiseases of muscle. New England Journal of Medicine, 270, 263-269.
Perkoff, G. T. and Tyler, F. H. (1958). Creatine metabolismin the Bar Harbour 129 strain dystrophic mouse. Metabolism:Clinical and Experimental, 7, 745-750.
Perutz, M. F. (1970). The Bohr effect and combination withorganicphosphates. Nature, 228, 734-739.
Poel, W. E. (1949). Effect of anoxic anoxia on myoglobin concen-tration in striated muscle. American Journal of Physiology, 156,44-51.
Reynafarie, B. and Morrison, P. (1962). Myoglobin levels in sometissues from wild Peruvian rodents to high altitude. Journal ofBiological Chemistry, 237, 2861-2864.
Romero-Herrera, A. E. and Lehmann, H. (1971a). Primary struc-ture of human myoglobin. Nature New Biology, 232, 149-152.
Romero-Herrera, A. E. and Lehmann, H. (1971b). The myoglobinof primates. I Hylobates agilis (gibbon). Biochimica et Bio-physica Acta, 251, 482-488.
Romero-Herrera, A. E. and Lehmann, H. (1972a). The myoglobinof primates. II Pan troglodytes (chimpanzee). Biochimica etBiophysica Acta, 278, 62-57.
Romero-Herrera, A. E. and Lehmann, H. (1972b). The myoglobinof primates. III Cercopithecidae (Old World monkeys): Papio anubts
(olive baboon) and Macaca Fascicularis ( = irus, crab-eatingmonkey). Biochimica et Biophysica Acta, 278,465-481.
Romero-Herrera, A. E. and Lehmann, H. (1973a). The myoglobinof primates. IV New World monkeys (Cebidae). 1. SaimiriSciureus (squirrel monkey). 2. Lagothrix lagothicha (Humboldt'swoolly monkey). Callitrichidae: Callithrix jacchus (commonmarmoset). Biochimica et Biophysica Acta, 317, 65-84.
Romero-Herrera, A. E. and Lehmann, H. (1973b). The myoglobinof primates V. Prosimians: Galago crassicaudatus (thick-tailedgalago) and Lepilemur mustelinus (sportive lemur). Biochimicaet Biophysica Acta. (In press.)
Romero-Herrera, A. E. and Lehmann, H. (1973c). N-terminalchain elongation as evidence for duplication of myoglobin in threeSouth American monkeys. FEBS letters, 31, 175-180.
Rosenmann, M. and Morrison, P. (1965). Seasonal augmentation ofmyoglobin in the snowshoe hare. Journal of Biological Chemistry,240, 3353-3356.
Rowland, L. P., Dunne, P. B., Penn, A. S., and Maher, E. (1968).Myoglobin and muscular dystrophy. Archives of Neurology, 18,141-150.
Scholander, P. F. (1960a). Oxygen transport through hemoglobinsolutions. Science, 131, 585-590.
Scholander, P. F. (1960b). Oxygen diffusion. Science, 132, 368.Scholander, P. F. (1961/1962). Physiological adaptation to diving inanimals and man. Harvey Lectures, 57,93-110.
Scholander, P. F. (1965). Tension gradients accompanying accele-rated oxygen transport in a membrane. Science, 149, 876-877.
Sick, K., Beale, D., Irvine, D., Lehmann, H., Goodall, P. T., andMacDougall, S. (1967). Haemoglobin G Copenhagen and haemo-globin J Cambridge. Two new chain variants of haemoglobinA. Biochimica et Biophysica Acta, 140, 231-242.
Strother, G. K., Ackerman, E., Anthony, A., and Strickland, E.Hardin (1959). Effects of altitude acclimatization on rat myoglo-bin. Effect of viscosity and acclimatization on myoglobin reactionrates. American Journal of Physiology, 196, 517-519.
Tappan, D. V. and Reynafarje, B. D. (1957). Tissue pigmentmanifestations of adaptation to high altitudes. American Journalof Physiology, 190,99-103.
Terwilliger, R. C. and Read, K. R. H. (1970). The radular musclemyoglobins of the amphineuran molluscs, Katherina tunicataWood, Cryptochiton stelleri Middendorf, and Mopalia muscosaGould. InternationalJournal ofBiochemistry, 1, 281-291.
Tomlinson, B. E., Irving, D., and Rebeiz, J. J. (1973). Total numberof limb motor neurones in the human lumbosacral cord and ananalysis of the accuracy of various sampling procedures. Journalof the Neurological Sciences, 20, 313-327.
Tomlinson, B. E., Walton, J. N., and Irving, D. (1974). The spinalcord in muscular dystrophy. Journal of the Neurological Sciences.(In press).
Vaughn, B. E. and Pace, N. (1956). Changes in myoglobin contentof the high altitude acclimatized rat. American Journal of Physio-logy, 185, 549-556.
Whipple, G. H. (1926). The haemoglobin of striated muscle. IVariations due to age and exercise. American Journal of Physio-logy, 76, 693-707.
White, J. M. (1972). The synthesis of abnormal haemoglobins.Biochimie, 54,657-663.
Whorton, C. M. Hudgins, P. C., Conners, J. J. (1961). Abnormalspectrophotometric absorption spectrums of myoglobin in twoforms of progressive muscular dystrophy. New England Journalof Medicine, 265, 1242-1245.
Whorton, C. M., Hudgins, P. C., Conners, J. J., and Nadas, A. S.(1963). The myoglobin molecule and its possible structuralalterations in diseased states of skeletal and cardiac muscle.Southern MedicalJournal, 56,583-587.
Wittenberg, J. B. (1959). Oxygen transport: a new function pro-posed for myoglobin. Biological Bulletin, 117,402.
Wittenberg, J B (1965). Myoglobin-facilitated diffusion of oxygen.Journal of General Physiology, 49, no. 1, pt. 2, 57-74.