30
APPROACH TO MYOPATHIES
| Date post: | 15-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | dr-arun-mathai-mani |
| View: | 58 times |
| Download: | 1 times |
APPROACH TO MYOPATHIES
CLINICAL FEATURES
Proximal, symmetric limb weakness (arms or legs)
Normal sensations
Preserved reflexes
Muscles are normal in size , without atrophy and fasciculations
Muscle pain or discomfort with palpation ( myalgia )
Muscle stiffness or cramps
Fatigue
Myoglobinuria

LABORATORY EVALUATION
Serum Enzymes - CK is the preferred muscle enzyme to measure in the evaluation of
myopathies
Electrodiagnostic Studies - EMG, repetitive nerve stimulation, and nerve conduction studies are
essential methods for evaluation
DNA Analysis
Forearm Exercise Test – Metabolic myopathies
Muscle Biopsy - usually obtained from a quadriceps or biceps brachii muscle
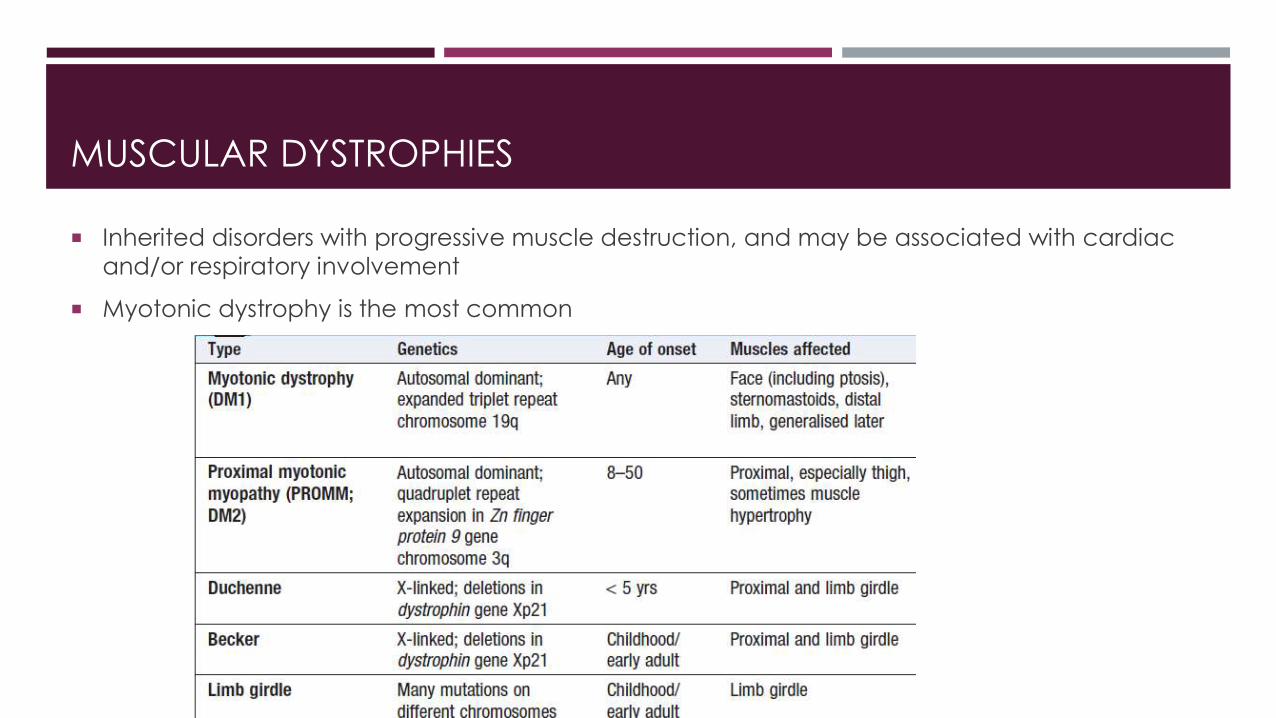
MUSCULAR DYSTROPHIES
Inherited disorders with progressive muscle destruction, and may be associated with cardiac
and/or respiratory involvement
Myotonic dystrophy is the most common
MYOTONIC DYSTROPHY
Myotonia - prolonged muscle contraction followed by slow muscle relaxation
typical "hatchet-faced" appearance due to temporalis, masseter, and facial muscle atrophy
and weakness
Frontal baldness is also characteristic
Myotonia, which usually appears by age 5 years
Cardiac disturbances occur commonly, ECG abnormalities include first-degree heart block
and more extensive conduction system involvement, Complete heart block and sudden death
can occur
Other associated features include intellectual impairment, hypersomnia, posterior subcapsular
cataracts, gonadal atrophy, insulin resistance, and decreased esophageal and colonic
motility

DUCHENNE'S MUSCULAR DYSTROPHY
incidence of 30 per 100,000 live-born males
becomes apparent between ages 3 and 5 years
On getting up from the floor, the patient uses his hands to climb up himself - Gowers' manoeuvre
By age 12 years, most patients are wheelchair dependent
By age 16–18 years, patients are predisposed to serious respiratory failure, sometimes fatal pulmonary infections
presence of a cardiomyopathy in almost all patients
Intellectual impairment is common
diagnosis can be made by Western blot analysis of muscle biopsy specimens
prednisone in a dose of 0.75 mg/kg per day, significantly slow progression for up to 3 years

BECKER'S MUSCULAR DYSTROPHY
less severe form
incidence of about 3 per 100,000 live-born males.
Hypertrophy of muscles, particularly in the calves, is an early and prominent finding
Onset is between ages 5 and 15 years
reduced life expectancy, but most survive into the fourth or fifth decade.
Mental retardation may occur
Cardiac involvement occurs and may result in heart failure
Diagnosis requires Western blot analysis of muscle biopsy

LIMB-GIRDLE MUSCULAR DYSTROPHY
Classification is based on autosomal dominant (LGMD1) and autosomal recessive (LGMD2)
inheritance
Both males and females are affected
onset ranging from late in the first decade to the fourth decade
typically manifest with progressive weakness of pelvic and shoulder girdle musculature
Respiratory insufficiency from weakness of the diaphragm may occur, as may cardiomyopathy

OTHERS
Emery-Dreifuss Muscular Dystrophy
Congenital Muscular Dystrophy
Facioscapulohumeral (FSH) Muscular Dystrophy
Oculopharyngeal Dystrophy
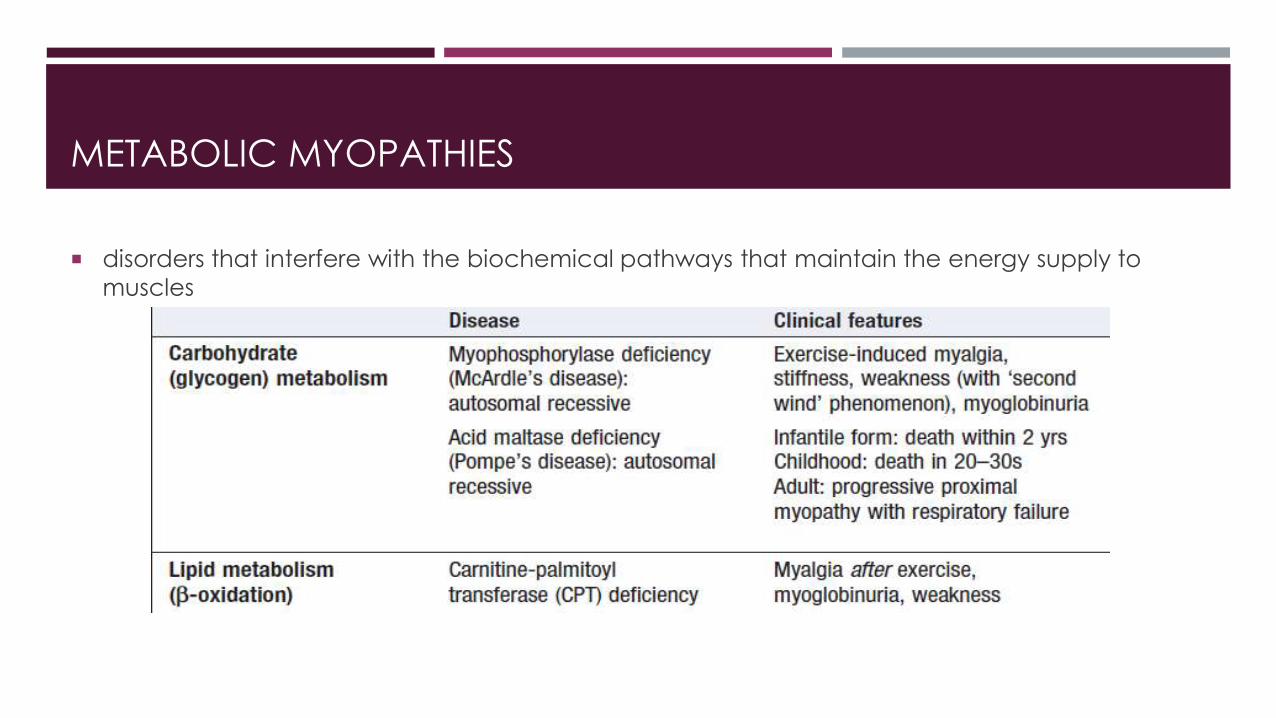
METABOLIC MYOPATHIES
disorders that interfere with the biochemical pathways that maintain the energy supply to
muscles

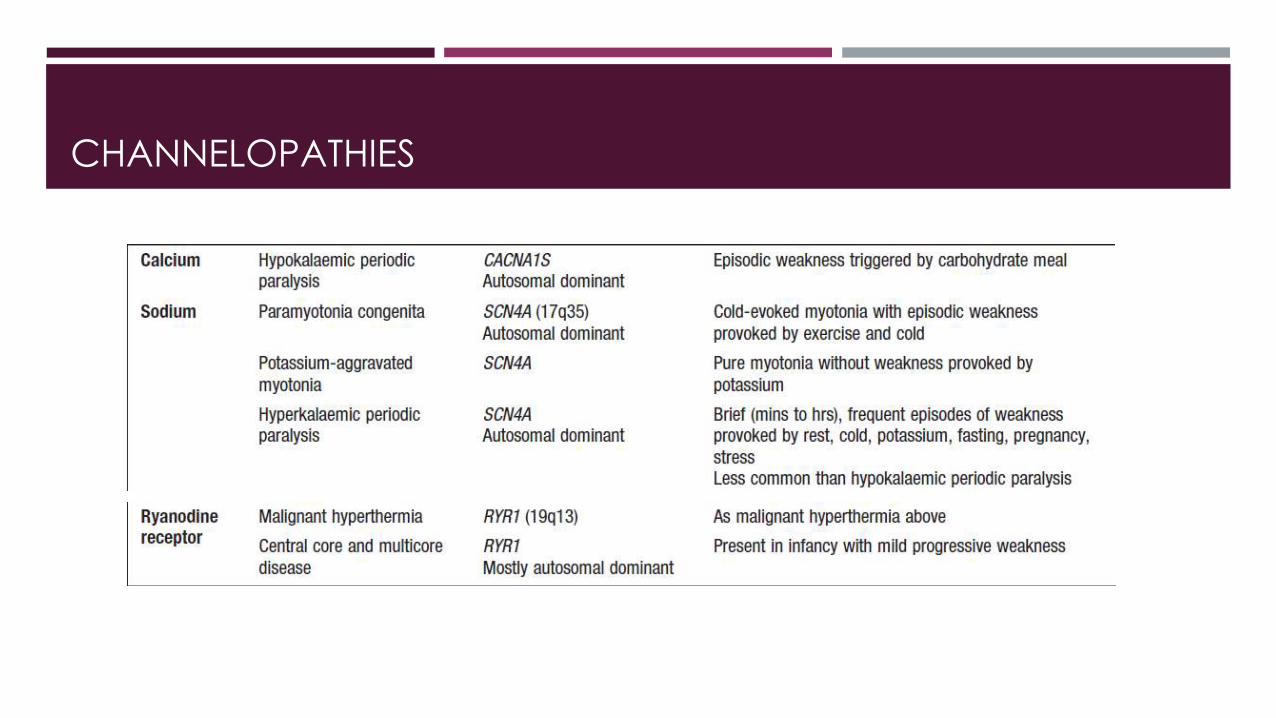
CHANNELOPATHIES

HYPOKALEMIC PERIODIC PARALYSIS (HYPOKPP)
Onset occurs at adolescence
Attacks are often provoked by meals high in carbohydrates or sodium
Ocular and bulbar muscles are less likely to be affected, Respiratory muscles are usually spared
Weakness may take as long as 24 hours to resolve
low serum potassium level during an attack establishes the diagnosis
acute paralysis improves after the administration of potassium, Oral should be given every 30
minutes
low-carbohydrate, low-sodium diet
Prophylactic administration of acetazolamide (125–1000 mg/d in divided doses) reduces or
may abolish attacks
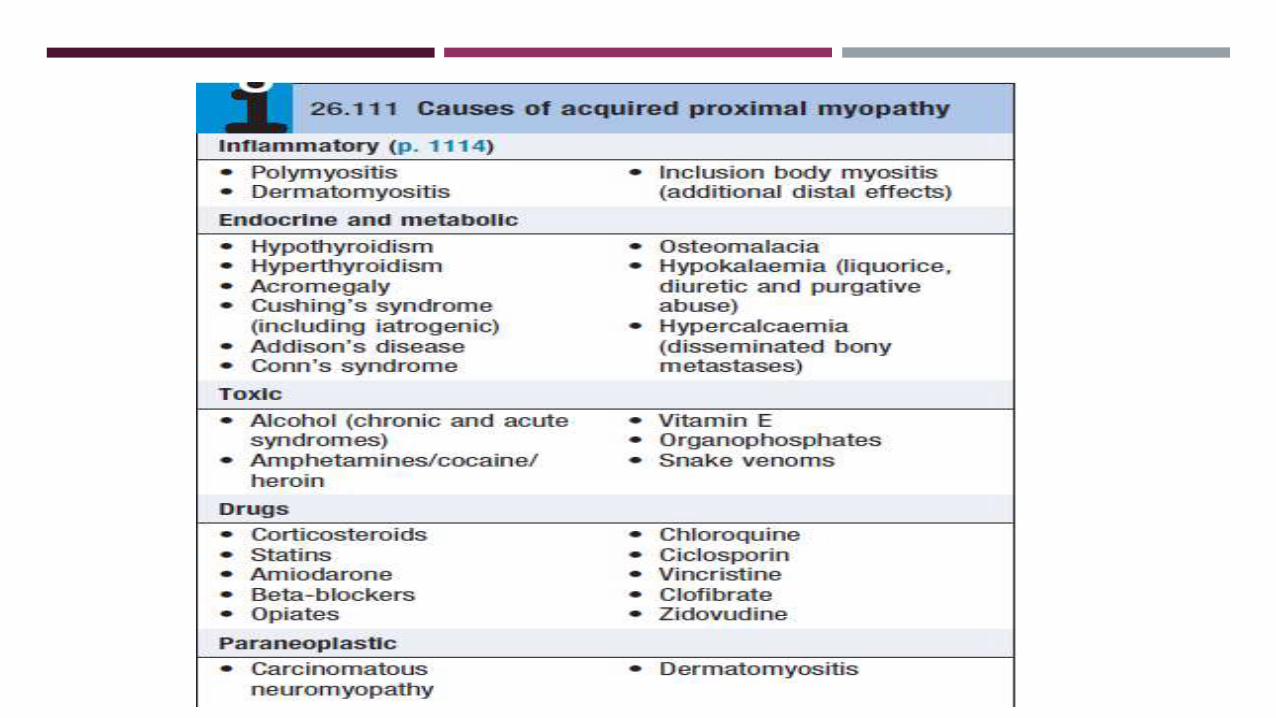

HYPOTHYROIDISM
frequent muscle complaints, and proximal muscle weakness occurs in about one-third
Muscle cramps, pain, and stiffness are common
Some patients have enlarged muscles
Features of slow muscle contraction and relaxation occur in 25% of patients
the relaxation phase of muscle stretch reflexes is characteristically prolonged and best
observed at the ankle or biceps brachii reflexes
HYPERTHYROIDISM
proximal muscle weakness and atrophy on examination
Activity of deep tendon reflexes may be enhanced
Bulbar, respiratory, and even esophageal muscles may occasionally be affected, causing
dysphagia, dysphonia, and aspiration
Other neuromuscular disorders occur in association - acquired hypokalemic periodic paralysis,
myasthenia gravis, and Graves' ophthalmopathy

MYOPATHY FROM LIPID-LOWERING AGENTS
All classes of lipid-lowering agents have been implicated in muscle toxicity, including fibrates,
statins, niacin, and ezetimibe
Myalgia, malaise, and muscle tenderness are the most common manifestations
Varying degrees of muscle necrosis are seen, and in severe reactions rhabdomyolysis and
myoglobinuria occur
Elevated serum CK is an important indication of toxicity
Severe myalgias, muscle weakness, significant elevations in serum CK (>three times baseline),
and myoglobinuria are indications for stopping the drug

GLUCOCORTICOID-RELATED MYOPATHIES
occurs with chronic treatment or as "acute quadriplegic" myopathy secondary to high-dose IV
glucocorticoid use
chronic use of prednisone at a daily dose of 30 mg/d is most often associated with toxicity
fluorinated glucocorticoids (triamcinolone, betamethasone, dexamethasone) appear to be at
especially high risk for myopathy
serum CK is usually normal
critical illness myopathy - high-dose IV glucocorticoids for status asthmaticus, chronic
obstructive pulmonary disease, organ transplantation, or other indications may develop severe
generalized weakness, can also occur in the setting of sepsis
use of glucocorticoids in combination with nondepolarizing neuromuscular blocking agents
potentiate this complication

INFLAMMATORY MYOPATHIES
largest group of acquired and potentially treatable causes of skeletal muscle weakness
classified into three major groups: polymyositis (PM), dermatomyositis (DM), and inclusion body
myositis (IBM)
present as progressive and symmetric muscle weakness
except for IBM, which can have an asymmetric pattern
Ocular muscles are spared, even in advanced, untreated cases
Facial muscles are unaffected in PM and DM, but mild facial muscle weakness is common in
patientswith IBM
They can occur in isolation or in association with other autoimmune diseases, such as SLE,
systemic sclerosis and Sjögren’s syndrome

DERMATOMYOSITIS
DM affects both children and adults and women more often than men
characteristic rash accompanying, or more often preceding, muscle weakness
heliotrope rash - blue-purple discoloration on the upper eyelids with edema
Gottron's sign - erythema of the knuckles with a raised violaceous scaly eruption
erythematous rash can also occur on other body surfaces, including the knees, elbows, malleoli, neck and anterior chest (often in a V sign), or back and shoulders (shawl sign), worsen after sun exposure
Dilated capillary loops at the base of the fingernails are also characteristic
mechanic's hands - palmar areas of the fingers may become rough and cracked, with irregular, "dirty" horizontal lines
muscle biopsy - significant perivascular and perimysial inflammation and perifascicular atrophy is seen


POLYMYOSITIS

INCLUSION BODY MYOSITIS
most likely to affect persons aged >50 years
three times more frequent in men than in women
Weakness and atrophy of the distal muscles, especially foot extensors and deep finger flexors
Dysphagia is common, occurring in up to 60% of IBM
20% of cases, IBM is associated with systemic autoimmune or connective tissue diseases

EXTRAMUSCULAR MANIFESTATIONS
Systemic symptoms, such as fever, malaise, weight loss, arthralgia, and Raynaud's
phenomenon
Dysphagia and gastrointestinal symptoms, due to involvement of oropharyngeal striated
muscles and upper esophagus, especially in DM and IBM
Cardiac disturbances, including atrioventricular conduction defects, tachyarrhythmias, dilated
cardiomyopathy, a low ejection fraction, and congestive heart failure
Pulmonary dysfunction, due to weakness of the thoracic muscles, interstitial lung disease
Subcutaneous calcifications, in DM

ASSOCIATION WITH MALIGNANCIES
incidence of malignant conditions appears to be specifically increased only in patients with
DM and not in those with PM or IBM
most common tumors associated with DM are ovarian cancer, breast cancer, melanoma,
colon cancer, and non-Hodgkin lymphoma
Screening for underlying malignancy should be undertaken routinely, and should include CT of
chest/ abdomen/pelvis, upper and lower gastrointestinal endoscopy, and mammography in
women

DIAGNOSIS
The most sensitive enzyme is CK, level usually parallels disease activity
Muscle biopsy - most sensitive and specific test for establishing the diagnosis of inflammatory
myopathy


MANAGEMENT
Oral corticosteroids (prednisolone 1 mg/kg daily) are the mainstay of initial treatment
high-dose intravenous methylprednisolone (1 g/day for 3 days) may be required in patients
with respiratory or pharyngeal weakness
many need additional immunosuppressive therapy.
MMF, Azathioprine and methotrexate are the agents of first choice


![Version 2 Please don’t nore this - Blood · Inflammatory myopathies – inclusion body myositis (IBM) (formerly Inflammatory myopathies: polymyositis [PM], dermatomyositis [DM]](https://static.documents.pub/doc/80x56/602246494e545541c973d779/version-2-please-donat-nore-this-blood-inflammatory-myopathies-a-inclusion.jpg)














