NORTHWEST AIDS EDUCATION AND TRAINING CENTER CROI 2015: Hot Topics in HIV Primary Care Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, NW AETC ECHO March 5, 2015
Transcript
NORTHWEST AIDS EDUCATION AND TRAINING CENTER
CROI 2015: Hot Topics in HIV Primary Care
Brian R. Wood, MDAssistant Professor of Medicine, University of WashingtonMedical Director, NW AETC ECHO
March 5, 2015
ECHO CROI Reviews 2015
3/5/15 3/12/15 3/19/15
Brian Wood: Primary Care
Shireesha Dhanireddy: New Treatments
Nina Kim: HCV Coinfection
Ruanne Barnabas: Prevention Issues
CROI 2015: Primary Care Topics
• Cancer risk and lung cancer screening• Benefits of statins beyond cholesterol reduction
“Cancers in Young and Old and Lung Cancer in HIV”
CROI 2015
Cancer Risk in HIV+ Over 65 Years Old
• Case-cohort study• 5% Medicare
registry sample • All cancers in people
over 65 in large cancer registry
• Association between HIV and cancer incidence
• Adjusted for age, race, sex, calendar year
Yanik El et al. Abstract 725.
Cancer Type Hazard Ratio Comparing HIV+ to HIV- (95% CI)
Kaposi sarcoma 79.2 (42.9-146)
Non-Hodgkin lymphoma 3.01 (2.24-4.05)
Diffuse large B cell 5.56 (3.69-8.39)
Burkitt lymphoma 21.8 (6.91-68.5)
Other specified 1.16 (0.67-1.99)
Unspecified 6.78 (3.93-11.7)
Anus 32.4 (21.6-48.5)
Hodgkin lymphoma 9.96 (4.89-20.3)
Liver 3.83 (2.46-5.97)
Lung 1.52 (1.21-1.91)
Colorectal 0.97 (0.69-1.36)
Breast 0.96 (0.56-1.65)
Prostate 0.78 (0.61-0.99)
Total cancer
Prostate
Lung
NHL
Colorectal
Anal
0 2 4 6 8 10 12
Cancer Risk in HIV+ Over 65 Years Old
5-year cumulative incidence (%)
CD4 Count as a Predictor of Lung Cancer Risk and Prognosis
• 26,065 HIV+ in VACS• Incident non-small cell lung
cancer cases• Cox regression models for
lung cancer risk, CD4 count• Adjusted for: age, sex,
race, smoking, h/o pneumonia or COPD
• Compared survival based on HIV status, CD4 +/- 200
Sigel K et al. Abstract 728.
CD4 Analysis Hazard Ratio (95% CI)
12-month lagged value
<200 1.6 (1.2-2.2)
200-500 1.2 (0.9-1.5)
12-month moving average
<200 2.0 (1.4-2.7)
200-500 1.4 (1.1-1.8)
24-month moving average
<200 1.7 (1.2-2.4)
200-500 1.3 (1.1-1.7)
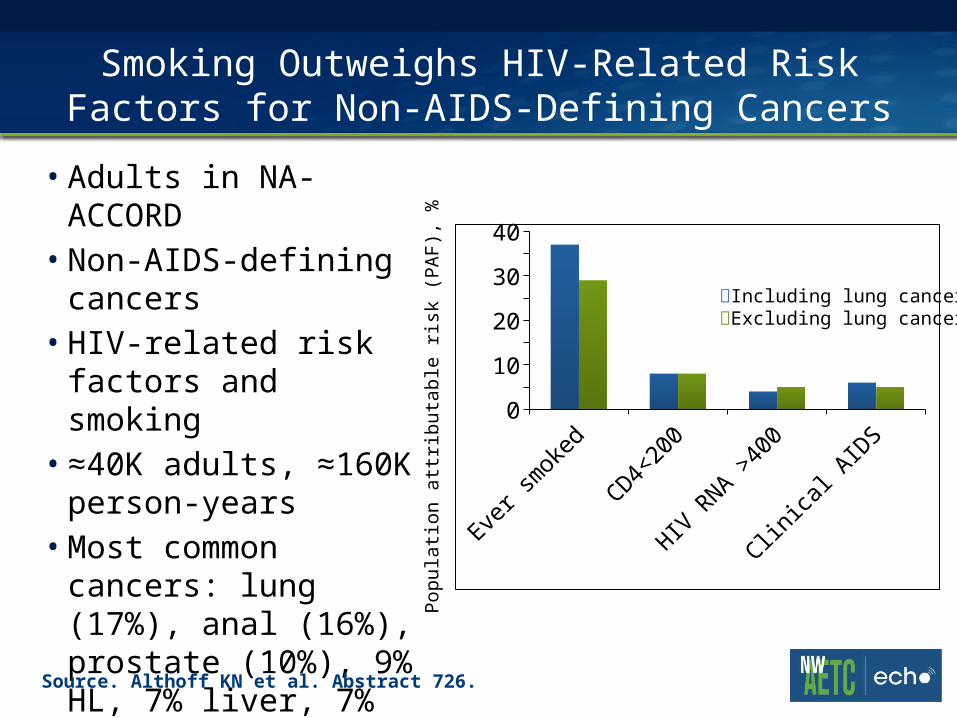
Smoking Outweighs HIV-Related Risk Factors for Non-AIDS-Defining Cancers
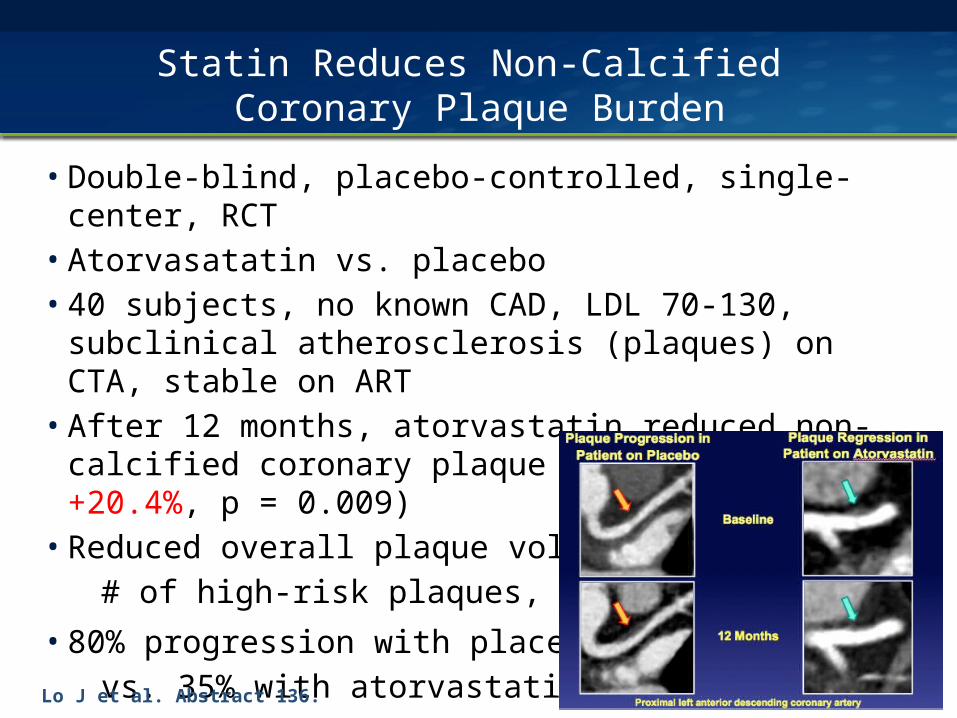
• Double-blind, placebo-controlled, single-center, RCT• Atorvasatatin vs. placebo• 40 subjects, no known CAD, LDL 70-130, subclinical
atherosclerosis (plaques) on CTA, stable on ART• After 12 months, atorvastatin reduced non-calcified
coronary plaque volume (-19.4% vs. +20.4%, p = 0.009)• Reduced overall plaque volume,
# of high-risk plaques, Lp-PLA2
• 80% progression with placebo
vs. 35% with atorvastatin
Lo J et al. Abstract 136.
More Potential Statin Benefits
• Rosuvastatin arrests progression of carotid intima media thickness (Longenecker CT et al. Abstract 137)
• Simvastatin protects human aortic endothelial cells from oxidative damage (Panigrahi S et al. Abstract 298LB)
• Atorvastatin partially reverses the HIV-mediated reduction of heme oxygenase (HO-1) in macrophages and may have benefit in HAND (Duncan MR et al. Abstract 502)
• Statins improve SVR and reduce fibrosis progression and HCC among HCV+ persons (Butt AA et al. Abstract 643)
• Statins have initial benefit for BMD over placebo but benefit doesn’t persist at 96 weeks and has detrimental effects on insulin resistance (Erlandson KE et al. Abstract 771)
Weigh benefits against risks: hepatotoxicity, myopathy, drug interactions, polypharmacy, cost
Justice A et al. Lancet HIV, January 2015.
Conclusions
• HIV infection raises risk of non-AIDS-defining malignancies, though smoking outweighs HIV-related risk factors
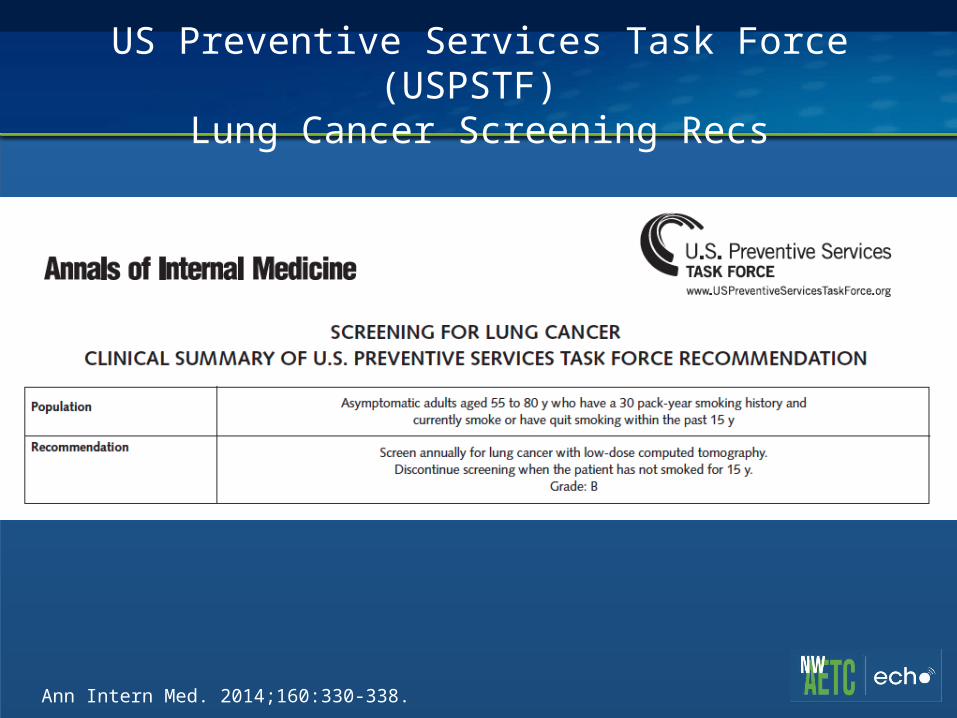
• Lung cancer screening should be considered for those at high risk, but need to define best criteria for HIV+
• Statins have many potential benefits, including reduced progression of subclinical high-risk coronary plaques
• We need better guidelines for assessing CAD risk and statin initiation for HIV+ persons