22
Phillip O. Coffin, MD MIA San Francisco Department of Public Health University of California San Francisco Naloxone for Opioid Safety

Phillip O. Coffin, MD MIA
San Francisco Department of Public Health University of California San Francisco
Naloxone for Opioid Safety
Gilead, Donated ledipasvir-sofosbuvir, Study, 2016-present Alkermes, Donated ER-naltrexone, Study, 2014-2015
Disclosure Information
1. Role / Effectiveness of Lay Naloxone
2. Potential impact of OTC status
3. Research gaps

Source: Darke S, Mattick RP, Degenhardt L. The ratio of non-fatal to fatal heroin overdose. Addiction. 2003 Aug;98(8):1169-71.
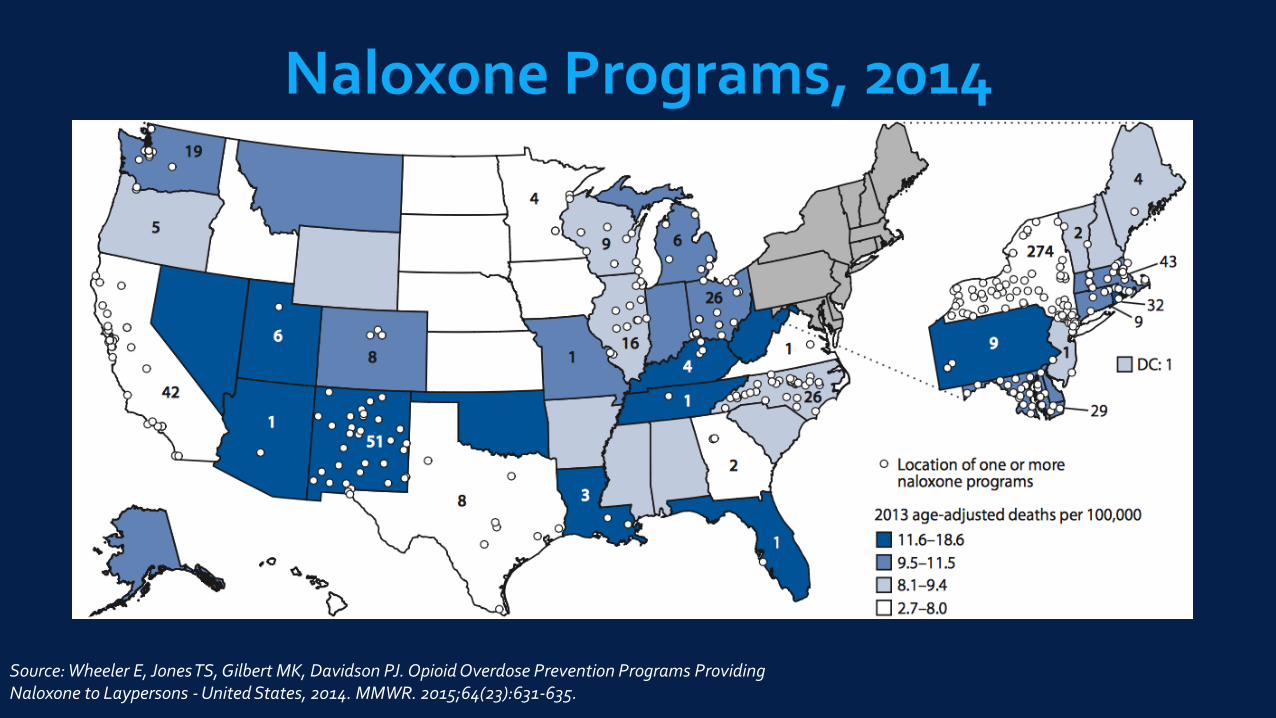
Source: Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid Overdose Prevention Programs Providing Naloxone to Laypersons - United States, 2014. MMWR. 2015;64(23):631-635.

Naloxone is not a controlled substance
States on this map have added legal protections, such as authorizing:
Prescribing/dispensing to potential bystanders Third-party administration by lay bystanders Prescribing/dispensing by standing order or directly from pharmacies
States in green also have laws protecting from prosecution when help is sought
Source: www.lawatlas.org
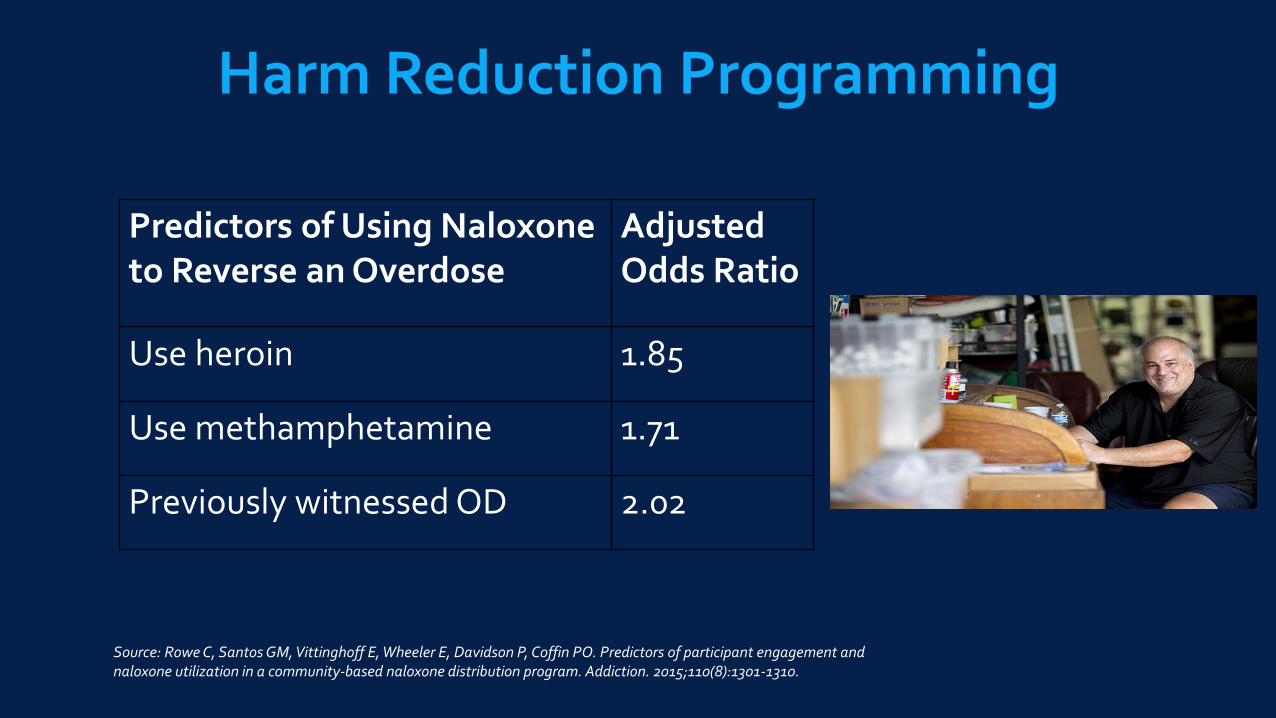
Predictors of Using Naloxone to Reverse an Overdose
Adjusted Odds Ratio
Use heroin 1.85
Use methamphetamine 1.71
Previously witnessed OD 2.02
Source: Rowe C, Santos GM, Vittinghoff E, Wheeler E, Davidson P, Coffin PO. Predictors of participant engagement and naloxone utilization in a community-based naloxone distribution program. Addiction. 2015;110(8):1301-1310.

Sources: Walley et al., Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. BMJ. 2013;346:f174; Davidson et al., Naloxone distribution to drug users in California and opioid-overdose death rates. Drug & Alc Dep. 2015; 156: e54.

Source: Coffin PO, Sullivan SD. Cost-effectiveness of distributing naloxone to heroin users for lay overdose reversal. Ann Intern Med. 2013;158:1-9.

0
1
2
3
4
5
6
7
0
20
40
60
80
100
120
140
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Fe
nta
ny
l-R
ela
ted
De
ath
s
La
y N
alo
xo
ne
Re
vers
als
Fentanyl powder
Counterfeit “Xanax”
Source: Drug Overdose Prevention/Education Project, San Francisco

Source: Binswanger IA, Blatchford PJ, Mueller SR, Stern MF. Mortality after prison release: opioid overdose and other causes of death, risk factors, and time trends from 1999 to 2009. Ann Intern Med. 2013;159(9):592-600.
Deaths / 1000py
Out of Treatment ~4.3
Residential Treatment
In 3.9
1-28 days out 18.8
Source: Pierce M, Bird SM, Hickman M, et al. Impact of treatment for opioid dependence on fatal drug-related poisoning: a national cohort study in England. Addiction. 2016;111(2):298-308.
Scottish Naloxone Program, Pre-Release - 36% reduction in opioid-related deaths in the 4 weeks post-
release - At least 1 death averted per 285 kits distributed
Source: Bird SM, McAuley A, Perry S, Hunter C. Effectiveness of Scotland’s National Naloxone Programme for reducing opioid-related deaths: a before (20076-10) versus after (2011-13) comparison. Addiction. 111:883-891.

“Overdose prevention, including prescribing or dispensing naloxone, is an essential complement to both detoxification services as well as medically supervised withdrawal”

Source: Coffin PO, Behar E, Rowe C, et al. Nonrandomized intervention study of naloxone coprescription for primary care patients receiving long-term opioid therapy for pain. Ann Intern Med. 2016.
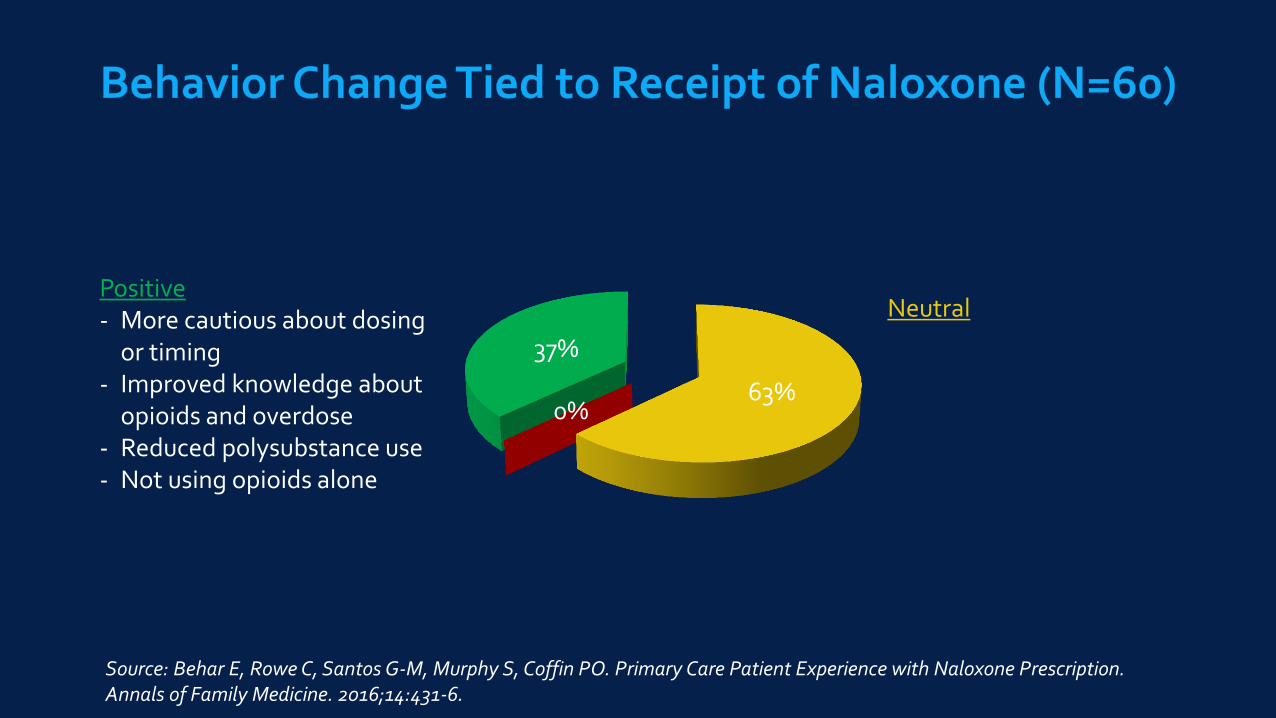
63% 0%
37%
Neutral Positive - More cautious about dosing
or timing - Improved knowledge about
opioids and overdose - Reduced polysubstance use - Not using opioids alone
Source: Behar E, Rowe C, Santos G-M, Murphy S, Coffin PO. Primary Care Patient Experience with Naloxone Prescription. Annals of Family Medicine. 2016;14:431-6.
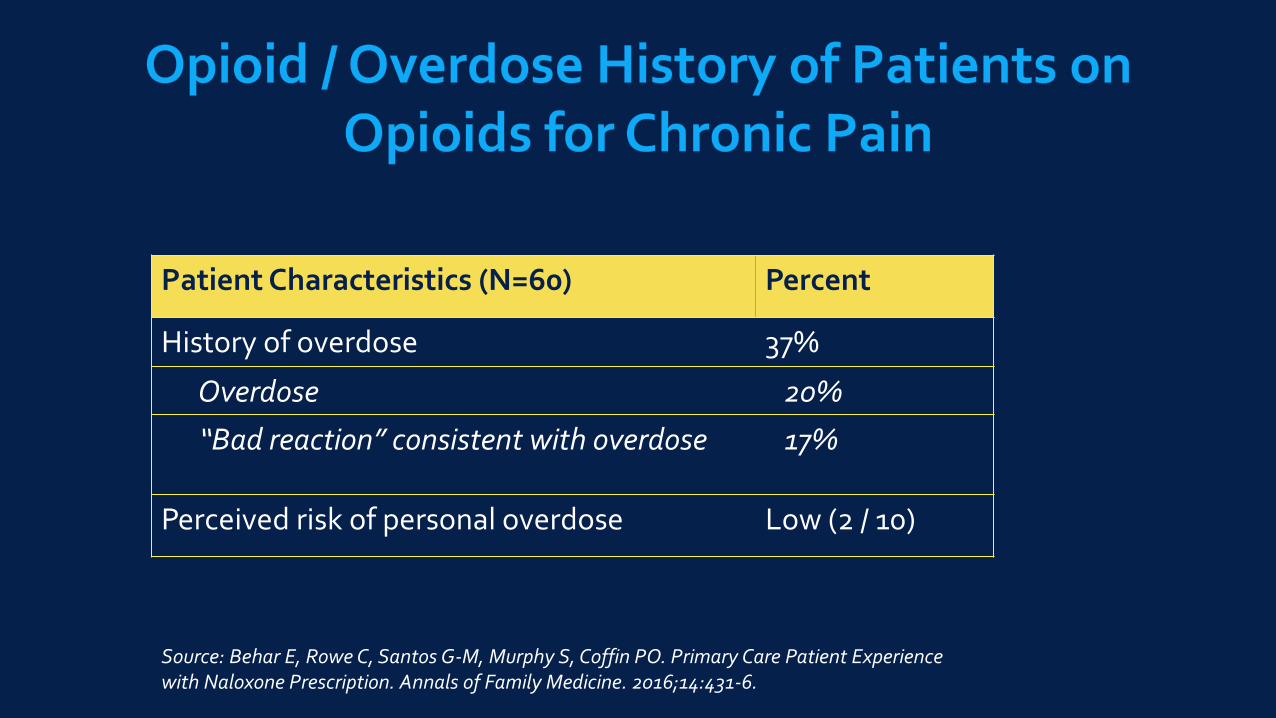
Patient Characteristics (N=60) Percent
History of overdose 37%
Overdose 20%
“Bad reaction” consistent with overdose 17%
Perceived risk of personal overdose Low (2 / 10)
Source: Behar E, Rowe C, Santos G-M, Murphy S, Coffin PO. Primary Care Patient Experience with Naloxone Prescription. Annals of Family Medicine. 2016;14:431-6.

Interviewer: How many times would you say you’ve had these bouts of
delirium, or you’ve stopped breathing because of
opioids?
Patient: Ever? 8-10 times.
Interviewer: And how many times has [naloxone] been used on you?
Patient: Oh boy. That would be really hard to answer. I’d say
somewhere in the neighborhood of 12-15 times.
Interviewer: So, around 12-15 times someone has given you [naloxone]
because you’ve stopped breathing because of opioids?
Patient: Yes. Medical staff each time. Because of the opioids, I’ve
stopped breathing.
Interviewer: Over what period of time?
Patient: Over 1 year.
Source: Behar E, Rowe C, Santos G-M, Murphy S, Coffin PO. Primary Care Patient Experience with Naloxone Prescription. Annals of Family Medicine. 2016;14:431-6.

“Clinicians should incorporate into the management plan strategies to mitigate risk, including considering offering naloxone when factors that increase risk for opioid overdose, such as history of overdose, history of substance use disorder, higher opioid dosages (>50 MME/day), or concurrent benzodiazepine use, are present.”

OTC Access Prescription Only
Insurance coverage
Standing orders
Some products OTC?
No need for clinicians

New terminology for overdose
Indications for co-prescribing
Naloxone in treatment programs / relapse risk
Implementation strategies
Optimal dosing regimen

0.53 0.61 0.58 0.55
0.37 0.32 0.37 0.38
0%
20%
40%
60%
80%
100%
2013 2014 2015 2016
Pe
rce
nt
of A
ll N
alo
xo
ne
Re
vers
als
% reversed with 1.5-2 doses
% reversed with 1 dose
% OD deaths involving fentanyl
Source: Prevention Point Pittsburgh

Source: Santa Fe Mountain Center; North Carolina Harm Reduction Coalition, DOPE Project
0%
10%
20%
Santa Fe (N=95) North Carolina (N=6) San Francisco (N=702)

People who use drugs are in best positioned to utilize lay naloxone
While OTC access would partly alleviate logistic barriers, the major barrier is cost
Co-prescribing naloxone with opioids is feasible and may have ancillary benefits
More research is needed regarding overdose terminology, naloxone in SUD treatment settings, dosing strategies, and implementation.

















