National Health Service Standards for Papua New Guinea 2011-2020 Volume 2 Chapter Four: Quality Standards for Health Services in Papua New Guinea and Health Service Accreditation Program A blueprint A blueprint A blueprint A blueprint for providing safe, quality health services as required by the for providing safe, quality health services as required by the for providing safe, quality health services as required by the for providing safe, quality health services as required by the National Health Plan 2011 National Health Plan 2011 National Health Plan 2011 National Health Plan 2011-2020 to transform our health system 2020 to transform our health system 2020 to transform our health system 2020 to transform our health system Government of Papua New Guinea June 2011
Transcript
National Health Service Standards
for Papua New Guinea
2011-2020
Volume 2
Chapter Four: Quality Standards for Health
Services in Papua New Guinea and Health
Service Accreditation Program
A blueprint A blueprint A blueprint A blueprint for providing safe, quality health services as required by the for providing safe, quality health services as required by the for providing safe, quality health services as required by the for providing safe, quality health services as required by the National Health Plan 2011National Health Plan 2011National Health Plan 2011National Health Plan 2011----2020 to transform our health system2020 to transform our health system2020 to transform our health system2020 to transform our health system
Government of Papua New Guinea
June 2011
Volume 2:
Table of Contents:
National Department of Health: National Health Service Standards 2
Table of Contents:
Volume Two
Volume Two ..................................................................................................................................... 2
National Department of Health: National Health Service Standards 5
Introduction
“Accreditation is a formal process to ensure delivery of safe, high quality health care based on
quality standards and processes devised and developed by health care professionals for health care
services. It is public recognition of achievement by a health care organisation, of requirements of
national health service standards”.1
Hospital standards were established in Papua New Guinea in 1997 to promote the best possible
quality of health care and continuous quality improvement of public health services. This was crucial
to the mission of serving “the rural majority and the urban poor”. The further development of the
standards and progress towards achieving them by all hospitals was a major contribution to the
development of health services.
The standards were later amended, and their title changed to “Quality Standards for Health Services
in Papua New Guinea”, to make them applicable for all health services, including hospitals, Health
Centres, Urban Clinics and Aid Posts and also to make the quality standards appropriate for
government organisations, Non-Government Organisation (NGOs), church or private organisations.
The wisdom of this approach benefits our health care system now as we plan for accreditation of
safe quality health care of Provincial Health Authorities. Adoption of these updated quality
standards by a health service shows its willingness to have its compliance with the quality standards
assessed by a team of trained, experienced and practising health care professionals.
This Quality Standards for Health Services in Papua New Guinea – Health Service Accreditation
Program User Guide is intended to assist all involved in the use of the Quality Standards for Health
Services in Papua New Guinea and in the accreditation process, i.e. Health Service Managers,
National Department of Health Personnel and the Quality Standards and Accreditation Surveyors.
Standards for Hospital Services in Papua New Guinea were developed in the late 1990s and have
been used since as the standards for accreditation of Provincial Hospitals and some NGO-run
hospitals.
In 2010, with the release of the National Health Plan 2011-2020, these Standards were amended to
make them suitable for application in all health services, i.e. Provincial Health Authorities, Referral
Hospitals, Regional Hospitals, Provincial Hospitals, District Hospitals, Health Centres and Community
Health Posts.
It is expected that all health services will strive to achieve these quality standards. The voluntary
accreditation process for health services gives public recognition that a health service is meeting the
Quality Standards. Health services undergo an accreditation survey every two years and more
frequently if they are found not be complying with mandatory quality standards (relating to infection
control, fire and emergency planning, occupational health or safety and waste management).
Accreditation is awarded jointly by the Minister for Health and the Secretary of the National
Department of Health.
1 Australian Council on Healthcare Standards
Volume 2:
Introduction
National Department of Health: National Health Service Standards 6
The National Department of Health, especially through the Medical Standards Division, also reserves
the right to inspect health services which do not have current accreditation to ensure that they are
achieving a satisfactory degree of compliance with the Quality Standards.
The Quality Standards are reviewed, usually every year, by trained Accreditation Surveyors who
recommend amendments to the Quality Standards to the National Department of Health through
the Medical Standards Division.
The accreditation process and the rules and policies which govern it are described in more detail in
the Guide to Quality Standards Accreditation which is available from the National Department of
Health Medical Standards Division and on their website.
Background
It is important that all stakeholders have a shared understanding of the quality standards that is
expected for our health services to achieve in accessibility, safety and effectiveness. The Quality
Standards for Health Services in Papua New Guinea help achieve this shared understanding. The
Quality Standards step from the National Health Plan’s 2011-2020 Key Result Areas and from many
other authoritative sources; they are developed in consultation with those who provide health
services throughout the country.
The Quality Standards reflect the contemporary ideals for health executives practising in health
services management. As much as possible they focus on the core business of patient care and are
based in evidence about what works best. They serve as minimum quality standards to underpin safe
care but they also promote continuous quality improvement. They do not set out in detail all the
standards to which health services should aspire but, by referring to other, more detailed standards;
they aim to promote high quality in all that a health service does i.e. infection control guidelines,
treatment manuals, etc.
Accreditation is one important way of monitoring and promoting compliance with the quality
standards that must be achieve in health services. It draws on the skills of experienced Health
Services Managers and Clinicians to assess compliance of health services with the Quality Standards
for Health Services in Papua New Guinea and it is a valuable process of peer review and networking.
Accreditation is a high level process which tests policies, processes and systems to ensure that they
are working and supporting compliance with more detailed clinical and other standards. It also
encourages health services to monitor their own compliance with the quality standards and report
to the National Department of Health as required.
Purpose of the Quality Standards for Health Services in Papua New Guinea:
It must be the objective of all those who provide clinical and primary health care services, or who
govern or manage them, to achieve safe, high quality outcomes for their patients and their
communities. Health services must also be efficient, effective, accessible, appropriate and
acceptable to those who use them. All these requirements are set out in more detail in the Quality
Standards for Health Services in Papua New Guinea.
The Quality Standards are flexible to apply and can apply to both large and small health services. A
small rural health service is not expected to provide the same range of services as a regional referral
Volume 2:
Introduction
National Department of Health: National Health Service Standards 7
or teaching health service but, where it does provide a service, it must meet the nationally
prescribed standard for quality and safety.
The Quality Standards are continually refined and developed to establish a minimum standard of
safety and also promote continuous improvement in our health services.
Role of Accreditation in Achieving Quality Standards – Health Service
Accreditation Program in Papua New Guinea:
Quality standards accreditation is intended to:
� Promote a uniformly high level of compliance with the Quality Standards for Health Services
in Papua New Guinea;
� Promote continuous improvement of the performance of health services; and
� Build a national consensus about what is good practice.
The Quality Standards and the accreditation process can be applied to any health service, i.e.
Referral Hospital, Provincial Hospital, District Hospital, NGO Hospital, Church Hospital, Health
Centre, Aid Post and Provincial Health Authority.
The quality standards accreditation process involves a team of trained Surveyors visiting a health
service to assess its compliance with the Quality Standards for Health Services in Papua New Guinea.
The Surveyors rate the health service as being fully compliant, partially compliant or not compliant
with each of the Quality Standards and write recommendations for achieving improved compliance.
Standards accreditation is voluntary and the objective of the survey team is to support the health
service in improving its performance; not to punish shortfalls in achievement. Health service
accreditation is also a process of peer review, with Surveyors and the staff of the health service
learning from each other. An accreditation survey can help identify activities that are not adequately
resourced but it is primarily about ensuring that the health service is doing the best it can with the
available resources.
Accreditation Surveyors are experts in interpreting the Quality Standards and applying of them in
different health care settings. Surveyors and health services use the ‘annotations’ to the Quality
Standards for Health Services in Papua New Guinea to help them interpret the Quality Standards and
conduct the survey.
Organisation-wide quality standards accreditation surveys are carried out only every four years and
limited surveys are carried out two years after the Organisation-Wide Survey (OWS). Therefore,
accreditation cannot provide the routine and frequent assurance that a health service is meeting all
its performance targets and other performance monitoring processes are established for this
purpose.
Scope of Quality Standards for Health Services in Papua New Guinea:
A ‘health service’ is all those services and facilities under the control of the Board of Management.
Therefore, the quality standards and accreditation surveys apply to outreach services provided by
the health service but not to the activities of other bodies, such as university departments or
research institutes, which are not controlled by the Board.
Volume 2:
Introduction
National Department of Health: National Health Service Standards 8
Quality Standards either specify, at a high level, what should be done or they refer to other
standards, i.e. Standard Treatment Manuals, Clinical Standards, legislation, regulations, policies and
guidelines. They also support and promote reporting to, and monitoring by, other authorities such
as the National Department of Health. In the era of heightened awareness of the need for good
clinical governance, there has been increased emphasis in accreditation on patient safety and clinical
care more generally, i.e.:
� Credentialling and defining the scope of practice of clinicians and competence of all staff;
� Clinical record keeping; as well as
� Selected clinical issues including:
o Infection control,
o Appropriate use of blood,
o Safe use of medications,
o Obtaining informed consent for procedures,
o Assessment of patients and
o Care planning and discharge planning.
Application of Quality Standards for Rural Health Services in Papua New
Guinea:
As indicated later in Preparing for Survey (p.19), The Coordinating Surveyor and the CEO of the
health service will negotiate any criteria which are not applicable for a survey of a health service.
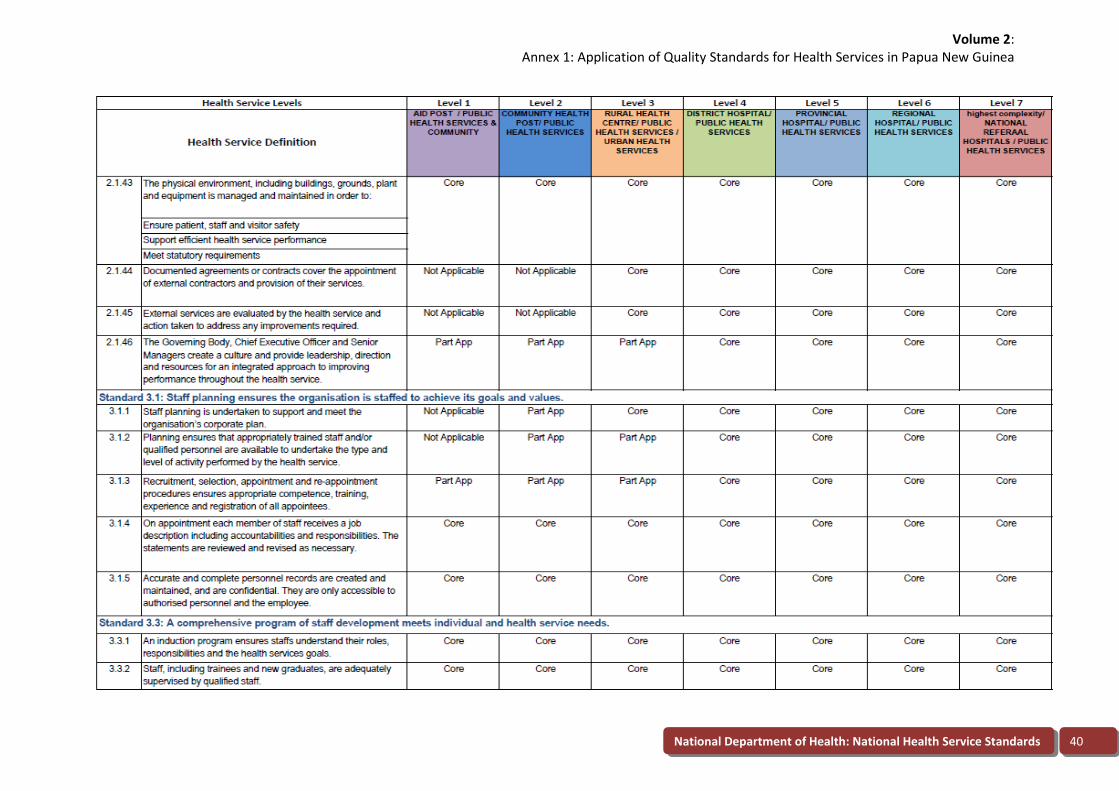
The spreadsheet Application of Quality Standards for Health Services in Papua New Guinea (Annex 1)
will serve as a guide to which criteria are usually fully applicable (core), partly applicable or not
applicable for various levels of health service. For example:
• Criterion 5.4.10 (A designated person is responsible for implementing radiation safety) will
be not applicable in delineated Level 1-3 health services.
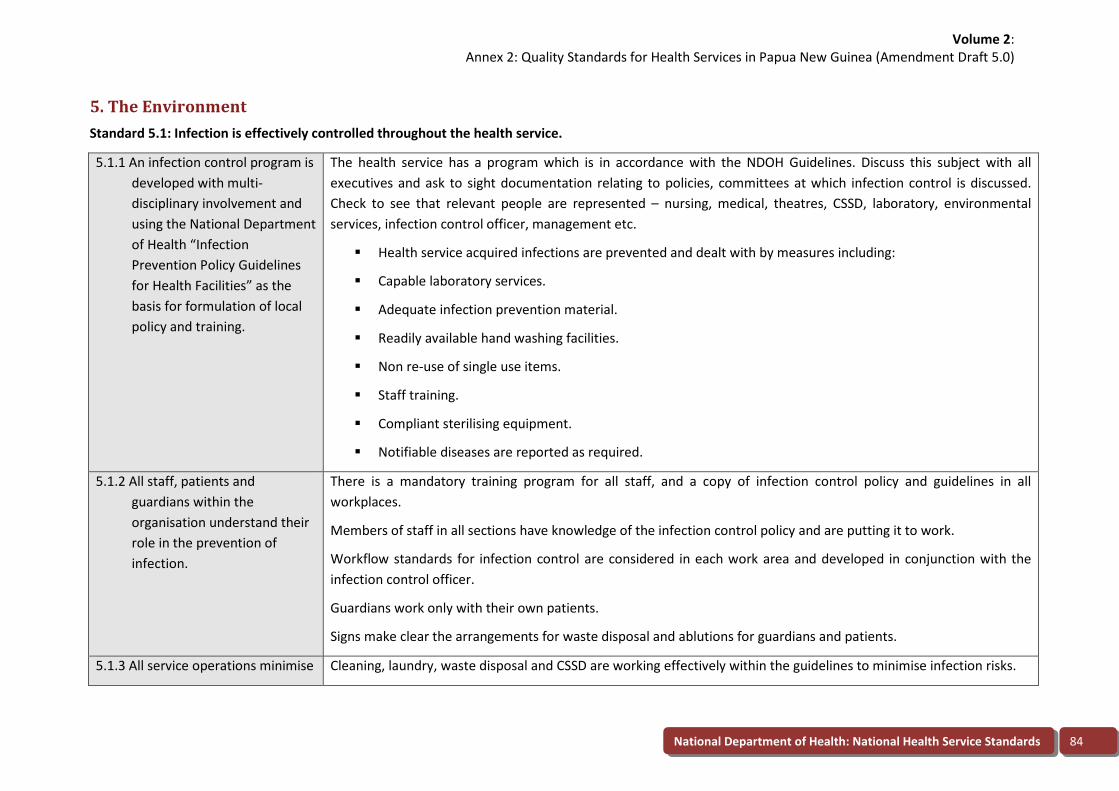
• Criterion 5.1.1 (An infection control program is developed with multi-disciplinary involvement
and using the National Department of Health “Infection Prevention Policy Guidelines for
Health Facilities” as the basis for formulation of local policy and training) will be partially
applicable in Level 1-3 services. If they are part of a Provincial Health Authority, it would be
expected that there would be an infection control program in accordance with the criterion.
If they are operated by the Provincial Government, it would be acceptable for them to have
more informal processes but to comply with the infection control standard as shown in the
Application of Quality Standards for Health Services in Papua New Guinea spreadsheet.
• Criterion 5.1.3 (All service operations minimise any infection risk in accordance with the
infection control program) would be expected to be a core criterion for all health services.
If a criterion is applicable to a health service and it is practical for the health service to comply, it is
expected to fully comply with the criterion, regardless of its size or level of complexity. In other
Volume 2:
Introduction
National Department of Health: National Health Service Standards 9
words, if a health service undertakes any activity, it is expected to comply fully with the National
Health Service Standards 2011-2020.
Surveyors are trained to know how to interpret the standards in health services of different size or
complexity.
Mandatory Quality Standards for Health Services:
The Quality Standards for Infection Control, Waste Management, Emergency and Disaster
Preparedness and Fire Safety are mandatory. This means that 80% compliance in each of those
areas is the ‘pass mark’ for accreditation of those hospitals which have already had a survey.
Substantial compliance would be required at a health service undergoing its first survey.
If a health service fails to achieve 80% for a mandatory quality standard, they may ask for a single
Surveyor to review compliance in a mandatory quality standards review2 between 90 and 120 days
after the initial survey. If 80% or more is achieved in the relevant mandatory quality standard, the
score in the previous survey report will be re-calculated and accreditation stars awarded in
accordance with the section on ‘Awards’ (refer to page 18).
Annex 2 illustrates how the mandatory quality standards are scored.
Development of Quality Standards for Health services:
The Quality Standards which describe the performance expected of health services come from many
authoritative sources. They may be required by legislation or developed by professional societies or
expert bodies or they may represent a consensus of experienced experts. They may also simply
reflect the wishes of the community.
The Quality Standards for Health Services in Papua New Guinea are developed by the Quality
Standards and Accreditation Secretariat within the Medical Standards Division, National Department
of Health in consultation with professional bodies, Accreditation Surveyors and health services.
At each of the annual surveyor updates, the Surveyors will elect a Quality Standards Development
Chair from among their number. The Quality Standards Development Chair will convene and chair
the meetings at which Surveyors contribute their suggestions for amendment of the Quality
Standards and will represent the Surveyors to revise the standards. These meetings may be held in
conjunction with surveyor updates. Any surveyor updates are approved by the Senior Executive. It is
important to note that Quality Standards are being continually revised to promote continuously
improving quality in Papua New Guinea’s health services.
Quality Standards for Health services – Health Service Accreditation User
Guide:
Compliance with the Quality Standards for Health Services in Papua New Guinea is mandatory for all
government health services. Compliance is assured through:
� The voluntary Quality Standards Accreditation process; or
� Operational Reviews conducted by the National Department of Health.
2
Volume 2:
Introduction
National Department of Health: National Health Service Standards 10
Accreditation provides a guarantee to the community that the health service is committed to
achieving the Quality Standards and to continuous improvement. Much of the value of accreditation
is in the critical self-scrutiny that an organization undertakes as it prepares for a quality standards
accreditation survey. The survey is also a peer review process in which experienced Surveyors draw
on their experience to advise their colleagues in the health service being surveyed. If accreditation is
granted to a health service, it is current for four years, after which another survey will be
undertaken.
The Quality Standards Accreditation Survey Report is a report to the health service and it is owned
by the health service. It is confidential to the health service, the survey team, and the National
Department of Health, Medical Standards Division.
Role of the Health Service Accreditation Surveyor:
The role of the Surveyor requires:
� Team work;
� Diplomacy and tact;
� Objectivity and impartiality;
� Expertise; and
� Knowledge.
Surveyors are ambassadors for the Papua New Guinea Health Services Quality Standards process.
The credibility of the Quality Standards depends on the conduct and performance of Accreditation
Surveyors. Another important responsibility of the Surveyor is to serve as a sounding board and
working partner to his or her surveyor colleagues. Therefore Surveyors must be able to evaluate and
offer comment on other areas being surveyed besides their own specialty areas.
Surveyors are consultants and educators during the survey. They offer advice to help identify and
resolve quality-related difficulties. They offer informal on-site education to help prevent future
problems developing and to set health services on the right path towards achieving the Quality
Standards.
Accreditation Surveyors must also continually assess their ability to carry out their role of evaluator
in an environment where increasing complexity and diversity is the norm and change is continual.
The Benefits of Being an Accreditation Surveyor:
The benefits of being an Accreditation Surveyor are as follows:
� The opportunity to keep knowledge up-to-date through studying the Quality Standards and
contact with other Surveyors and peers in health services being surveyed.
� The opportunity to observe firsthand the different organisation structures and processes of
health services.
� The observation of good initiatives which may enhance services in their own organisations.
� The capacity to tap into a network of health services.
Volume 2:
Introduction
National Department of Health: National Health Service Standards 11
� The educational experience of sharing and attempting to resolve problems and difficulties
facing facilities in the delivery of health care.
� The professionally rewarding experience of being part of a survey team, with members of
other professions, and providing health services with a report, drawing on experience in
provision of health care.
� The privileged experience of being invited to enter any area of a facility or health service
being surveyed, to talk to staff, patients or visitors and to review the way in which services
are organised and provided.
� The opportunity to see how people work in health services of all sizes and types and to help
the different groups understand their counterparts in other areas, i.e. people from small
rural and remote health services understanding their counterparts in large teaching health
services and vice versa.
� The benefit of being continually reminded of the performance that the Surveyor's own
organisation should be achieving and observing how different facilities meet the quality
standards within their resources.
Eligibility to be an Accreditation Surveyor
Any health service Chief Executive Officer, Director of Medical Services or Director of Nursing
Services, District Health Manager, District Program Manager are eligible to train to be a quality
standards Accreditation Surveyor. A Chief Executive Officer may also nominate any other suitably
senior and experienced member of his or her staff to be a Surveyor, i.e. Director of Finance and
Administration, Quality Coordinator, Infection Control Officer, Chief Pharmacist, etc.
Suitably senior and experienced officers of the National Department of Health and Provincial Health
Authorities may also be nominated for Surveyor training. The Medical Standards Division, National
Department of Health, should consult the Preceptors about the suitability of any nominees who are
not currently employed in a health service before confirming that they will be trained as Surveyors.
Responsibilities of an Accreditation Surveyor
� Undertake an observation survey.
� Commitment to the implementation of the quality standards.
� A commitment of two surveys per year if required.
� Approval from your employer to participate in surveys.
� Understanding and applying the quality standards in a variety of health services.
� Using up-to-date knowledge of management and clinical practices.
� Participation in Surveyor updates.
� Agreement to be involved in continuing assessment of Surveyor's performance.
� Agreement to submit survey reports at the completion of the survey.
� Agreement to be involved with education and advisory activities or quality standards
development.
Volume 2:
Introduction
National Department of Health: National Health Service Standards 12
� Agreement to be a coordinating Surveyor once adequately experienced.
Summary of the Accreditation Surveying Task
The primary responsibility of the Surveyor is to conduct surveys of health services and to provide
comprehensive, relevant and timely reports of the surveys so that the health service has a prompt
indication of the outcome of its survey. Surveyors are responsible for keeping themselves up-to-date
with quality standards, surveying techniques and procedures. At orientation, all new Surveyors
receive a copy of A Guide to Quality Standards for Health Services in Papua New Guinea – Health
Service Accreditation Program, which details policies and procedures for the conduct of surveys and
the survey process.
Health professionals will be selected as Surveyors on the following requirements:
� Understanding of the Quality Standards and the philosophy that underpins them.
� Suitability based on present employment responsibilities.
� Commitment to the quality standards accreditation process.
� Competence to write reports.
� Time management.
� Acceptance of criticism and self correction.
� Understanding of quality activities and quality in health care.
� Credibility among his or her peers.
� Ability to work in a team.
� Interpersonal skills.
Accreditation Surveyor Education
There are four main components in Surveyor education. They include:
� An orientation workshop for all new Surveyors;
� Observation surveys undertaken by new Surveyors;
� Annual Surveyor updates; and
� Continuing education.
All Surveyors must attend an annual update and, if unable to do so, they should attend the annual
Surveyor orientation. Surveyors will not be eligible to undertake surveys unless they have attended
an orientation, an update or undertaken an observation survey within the last 24 months.
Surveyor orientation
A workshop for new Surveyors will usually be held once each year.
The aims of Surveyor orientation are to:
� Familiarise Surveyors with the Quality Standards;
� Provide Surveyors with the knowledge, skills and attitudes that they will need; and
Volume 2:
Introduction
National Department of Health: National Health Service Standards 13
� Provide Surveyors with a supervised opportunity to observe and participate in a survey.
At the completion of the workshop, Surveyors will be able to:
� Explain the purpose of the Quality Standards for Health Services in Papua New Guinea; the
benefits to the health service of being surveyed; and the effect of a Quality Standards
Accreditation Survey on the community and providers of health services.
� Describe the Quality Standards and the intent of them, their application within health
services and health centres and the Quality Standards Accreditation Survey process.
� Describe the role and functions of the Surveyor.
� Survey a health service or health centre effectively.
Observation Surveys
Trainee Surveyors will be invited to participate in a survey as an observer. The role of an observer is
explained in more detail.
Annual Surveyor Updates
Surveyor updates will usually be held once each year.
Continuing Education
From time-to-time the Medical Standards Division, National Department of Health, will give Surveyors and
health services the opportunity to participate in continuing education activities relevant to the Quality
Standards Accreditation process.
Gratuities
Health services may extend reasonable hospitality to the survey team and it is reasonable – but
certainly not expected – that they give the Surveyors a souvenir of their time at the health service.
However Surveyors must not accept a gift of any significant cash value from the health service.
The Coordinating Surveyor
As well as ensuring the smooth management of the survey and the production of the Survey Report,
the Coordinating Surveyor is the spokesperson for the surveying team. In this important role, the
Coordinating Surveyor must make the initial contact with the organisation, establish leadership of
the survey itself, and throughout the survey be alert to any potential problems and try to defuse
difficult situations before they escalate.
On rare occasions, problems arise during the survey. The Coordinating Surveyor should act
responsibly to resolve any dispute and maintain the good standing of the survey team and process.
Advice may be sought from the Preceptors in regard to any issue, before or during the survey or at
the report writing stage. Advice may also be sought from Preceptors on any aspect of the survey,
interpretation of the quality standards or report writing.
The Coordinating Surveyor is also free to seek assistance from the National Department of Health,
Medical Standards Division at any time during, before or after the survey.
Volume 2:
Introduction
National Department of Health: National Health Service Standards 14
Preceptors
A ‘Preceptor’ is a teacher or instructor. Senior Surveyors (nominated at the Surveyor update
meeting) will serve as Preceptors for the Quality Standards Accreditation Survey Program in the
initial stages.
A Preceptor may:
• Accompany a survey team undertaking a survey in some circumstances;
• Be contacted by Surveyors at any time to discuss aspects of the program and any issues
relating to the Quality Standards; and
• Provide advice to the Quality Standards and Accreditation Secretariat within the National
Department of Health’s Medical Standards Division, on administrative matters relating to
accreditation.
New Surveyor Observer
New Surveyors may be attached to a survey team as observers for practical experience after they
have participated in a new Surveyor training program. The observation survey is designed to enable
new Surveyors to observe how compliance with the Quality Standards is assessed during the course
of a survey. Permission for an Observer to be present on a survey is arranged by the Secretariat with
the health service and the Coordinating Surveyor prior to the survey. In general, only one Observer
should participate in a survey.
The Coordinating Surveyor may delegate a component of the survey to an Observer, such as writing
a section of the report, but an Observer may participate in interviews only under the direct
supervision of an experienced Surveyor.
The new Surveyor’s activities as an Observer are determined by the Coordinating Surveyor within
the following framework. The Observer is expected to:
� Share in the preparation of a plan for surveying the services within a health service.
� Report to other members of the survey team on observations made during the survey.
� Attend the whole survey including both the pre-survey conference and the summation
conference. The Observer may be asked to take an active part in the summation
conference.
� Formulate an opinion on the level of compliance of one or more services with the Standards
and report to the survey team. The objective here is both to add to the education of the
observer but also to improve inter-rater reliability by providing an independent score for
one or more services.
� Write a portion of the Survey Report for submission to the responsible Surveyor.
� Be evaluated by the survey team.
Conflict of Interest for Surveyors
Surveyors should not survey where there is a conflict of interest. Should a conflict of interest arise a
Surveyor should inform the Secretariat promptly. Cases of a conflict of interest include:
Volume 2:
Quality Standards for Health Services – Accreditation Program:
National Department of Health: National Health Service Standards 15
� Health care organisation where they have previously worked in a senior post.
� Health care organisations with which they have a close professional or personal relationship.
� Health care organisations they have surveyed within the last five years.
� A healthcare organisation with which the Surveyor's affiliated organisation is in a
competitive situation.
� Any other situation where a conflict of interest would exist, i.e. prospective employment,
employment as consultant within five years.
The health service may appeal against a particular Surveyor being included in the survey team to the
the National Department of Health, Medical Standards Division if it believes that a conflict of interest
exists. A change of Surveyor may be made at the discretion of the Secretariat.
Quality Standards for Health Services – Accreditation Program:
The objectives of the Quality Standards Accreditation Survey are to:
� Assess the quality of services provided by health services against the quality standards.
� Provide a team of Surveyors to serve as consultants and educators for health services.
� Make recommendations for self improvement.
There are three kinds of survey:
� An OWS every four years.
� A Periodic Review (PR), two years after the OWS.
� A mandatory quality standards review (MSR) -refer to Mandatory Quality Standards on page
9.
Organisation-Wide Survey:
Star ratings are allocated at the OWS every four years. Compliance of the health service with all the
Quality Standards for Health Services in Papua New Guinea is assessed by a full survey team. The
first step a health service takes when seeking accreditation for the first time is an internal survey or a
baseline OWS.
A self-assessment is usually carried out by members of staff of the organisation who have been
trained in the Quality Standards and survey methods. They write a report, including
recommendations, to help the health service prepare for an external accreditation survey by a team
of independent Surveyors. The internal survey helps the organisation to assess its own strengths
and weaknesses.
A baseline survey is one carried out by members of staff from other health services. Again, they
prepare a report to help the organization prepare for an external accreditation survey.
A team of trained Surveyors will visit and provide a report on a health service. The survey team
examines documents, facilities, equipment and services and interviews members of staff and
patients to assess compliance with the Quality Standards.
Volume 2:
Quality Standards for Health Services – Accreditation Program:
National Department of Health: National Health Service Standards 16
The survey team usually comprises a Chief Executive Officer, a Director of Nursing Services and a
Director of Medical Services but can include a Director of Finance and Administration, a Provincial
Health Adviser or District Health Manager for urban and rural health services. In certain health
services, a Clinical Surveyor may also assist with surveying clinical units. These peer representatives
spend from two to five days on site.
At the conclusion of the survey, there is a summation conference to discuss the team’s findings with
the senior management and governing body of the health service.
The Surveyors then complete their report, which contains an assessment of each service and
commendations and recommendations. The report remains the property of the health service,
although a copy is also provided to the Executive Manager Medical Standards Division.
The final phase of the process is the presentation of the Certificate of Accreditation to the health
service. The Certificate can be presented by a member of the Department of Health at a ceremony
at the health service. Accreditation is also announced at the annual National Health Conference.
Periodic Review
A PR will be conducted approximately two years after an OWS. Its purpose is to ensure that quality
standards do not slip in the interval between OWSs.
A PR will be conducted by two Surveyors who will assess compliance with the mandatory quality
standards and progress in dealing with recommendations from the previous OWS.Usually at least
one of the Surveyors at PR will be from the most recent OWS team.
The PR team will write a report, using the relevant sections of the Work Book. In their comments on
each previous recommendation they will:
� Close a recommendation; or
� Amend a recommendation; or
� Confirm that a recommendation remains outstanding.
Accreditation star ratings will not be changed at PR.
Mandatory Quality Standards Review (MSR)
When a health service fails to achieve 80% compliance for any of the mandatory quality standards
(infection control, waste management, emergency and disaster preparedness and fire safety) it will
not be accredited. The health service may request an MSR between 90 and 120 days after the OWS
and, if it has rectified the problems in the mandatory quality standards, the OWS survey report will
be re-scored and stars allocated accordingly.
Internal Survey
A health service which is preparing for its first survey, or the first survey after a long time, may seek
support from the Medical Standards Division for an Internal Survey. An Internal Survey will usually
involve:
� One or two days training about quality standards and accreditation for a group from the
staff of the health service, followed by;
Volume 2:
Quality Standards for Health Services – Accreditation Program:
National Department of Health: National Health Service Standards 17
� An Internal Survey, conducted by the members of staff of the health service over two or
three days.
The training will be conducted by a member of the Medical Standards Division or a senior Surveyor
nominated. The trainer will then assist with the Internal Survey and the scoring of the outcome. The
published Quality Standards, workbook and report format will be used so that the health service has
a record of recommendations for improvement and the recommendations that emerge from the
Internal Survey.
One Internal Survey for a health service preparing for its first accreditation survey will usually be
funded by the Medical Standards Division.
Baseline Survey
A health service which is preparing for a formal accreditation survey may choose to undergo a
Baseline Survey which will be conducted by trained Surveyors, perhaps six to twelve months before
the formal survey is scheduled. To minimise the cost of the Baseline Survey, it will usually be carried
out by Surveyors from within the same Region and they may even be from the health service itself.
A Baseline Survey will usually be organised by the health service itself but the Medical standards
Division can usually assist. The cost of a Baseline Survey will usually be met by the health service;
this will depend on the availability of funds.
Benefits of a Quality Standards Accreditation Survey
A survey is a catalyst for change and a conscious and active demonstration to both the health
service's peers and the public of the effort to maintain high professional standards of care. It is a
valuable learning experience and a health service’s benefits for the participation in the quality
standards accreditation process lie in the preparation and self evaluation that precede survey.
Typical benefits include:
� A structured and comprehensive analysis of a health service’s performance.
� Improvement in the quality of patient care and in the efficiency of a health service's
operations.
� Enhancement of teamwork and staff morale.
� Reflection and challenge to tradition.
� Introduction of new techniques.
� A broadly based improvement in a health service's performance.
It also encourages debate amongst health professionals about the best ways of measuring and
encouraging high performance.
Awards
Awards may be granted and will remain in effect for four years from the date of survey. The
categories of awards are:
� Five stars (�����) are awarded to health services which substantially comply with the
quality standards and which achieve a total rating of 90 - 100%.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 18
� Four stars (����) are awarded to health services that achieve a total rating of 80 - 90%.
� Three Stars (���) are awarded to health services that achieve a total rating of 65 - 79%.
� Two Stars (��) are awarded to health services that achieve a total rating of 50 to 64 %.
� One Star (�) is awarded to health services that achieve a total rating of less than 50 %.
� No accreditation if a health service fails to achieve 80% on any of the four mandatory quality
standards.
It must be understood that the star rating indicates the level of compliance with the Quality
Standards for Health Services in Papua New Guinea achieved by the health service. The rating
should not be interpreted as giving an indication of the range of services provided by the health
service.
Structure and Organisation of the Accreditation Survey
Scope of survey:
All beds and services provided by a health service should be included in the survey. It will be
necessary to check which services located on a health service campus actually belong to the health
service and includes outreach or community health services. In some cases, provincial health or
education facilities may not be part of the health service.
Normally, an OWS is carried out every four years. A PR is carried out within the four year cycle of
accreditation, usually about two years after the OWS.
A Review of Mandatory Quality Standard is carried out approximately 90 days after an OWS to
assess progress when a health service has been scored at less than 80% for a mandatory quality
standard. Following a RMS, the most recent survey report the score will be re-calculated and, if 80%
is achieved for all mandatory quality standards, accreditation will be awarded.
Length of survey:
The length of surveys could range from one to four days, depending on the size, complexity and
geographical spread of the health service to be surveyed.
Numbers of Surveyors:
For a typical health service, the survey team will comprise three members:
� An Administrative.
� A Nurse.
� A Medical Surveyor.
A Finance and Administration Surveyor and/or a clinical Surveyor may be included for surveys of
large organisations.
Preparing for Survey
The Medical Standards division Secretariat will:
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 19
� Identify dates for survey two to six months ahead in consultation with the health service.
� Appoint the Coordinating Survey and, if appropriate, the Preceptor.
� Identify Surveyors in conformance with the rules for assignment of Surveyors to surveys and
given at least two month’s notice of their participation in a survey. It is important to note
that there may be times when a Surveyor has to withdraw from the survey team and it’ll be
necessary to call on a replacement at short notice. The health service can object to a
Surveyor being on a team if it believes that the Surveyor would have a conflict of interest so
check that the health service is comfortable with the survey team.
� Confirm that it is acceptable to have an observer, or observers, on the survey team the if it is
planned or necessary.
� In writing confirm the membership of the survey team and the dates of survey to the
Coordinating Surveyor, Surveyors and the health service.
� Arrange travel, accommodation and travel allowances for the survey team.
� Provide survey materials to the survey team, i.e.:
o Pre-survey questionnaire and attachments.
o Computer and printer.
o Work Books, with pages printed for each service or department to be surveyed in
the particular health service.
o Stationery and name badges.
The Health Service will:
� Undertake a baseline or an internal survey; approximately 12 months before the external
OWS is due.
� Approximately one month before surveying a health service, the Surveyor should receive a
completed questionnaire from the health service, providing background data on its
organisation and services. This should be studied carefully so that the Surveyor is able to
embark on the survey with a reasonable knowledge and understanding of the scope and
dimensions of the health service’s services. Complete the Pre-survey Questionnaire and
send it, with attachments (i.e. annual report) to the Medical Standards Division.
� List the services to be surveyed. This will usually be all departments, sections or services
controlled by the Board of Management.
� Arrange the survey time-table with the Coordinating Surveyor.
The Coordinating Surveyor will:
� Contact the CEO of the organisation to be surveyed at least 14 days before the survey to:
o Decide the scope of the survey and where criteria are “not applicable.”
o Arrange the time-table.
o Ask if there are any particularly sensitive issues that the survey team needs to be
aware of, i.e. industrial relations problems.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 20
o Confirm the arrival time of the survey team at the health service.
o Decide if the health service will give presentations at the initial meeting.
o Contact other survey team members at least 10 days prior to the survey.
o Confirm travel arrangements and make sure Surveyors have tickets etc.
� Confirm accommodation arrangements.
� Conduct a pre-survey meeting of Surveyors usually the evening before the survey. This
meeting is compulsory and each Surveyor must attend. The meeting should:
o Discuss the Pre-survey Questionnaire;
o Confirm areas of responsibility; and
o Work out the time-table.
A Coordinating Surveyor who is new to the role will find it helpful to consult a Preceptor about how
to approach the role. The Coordinating Surveyor should also consider travelling to the health service
a day or more ahead of the rest of the team if intensive consultation with the health service is
required to develop the time table, confirm which criteria are “not applicable” or for other reasons
related to planning the survey.
Surveyors and Observers:
It is essential for Surveyors to be familiar with the content, interpretation and intent of the quality
standards. This knowledge can only be achieved by carefully studying and understanding the Quality
Standards for Health Services in Papua New Guinea. The Annotated Quality Standards have been
prepared to guide Surveyors and organisations being surveyed in interpreting the quality standards.
In particular, each Surveyor should be very familiar with the quality standards for which they are
individually responsible throughout the survey. Before a survey, Surveyors may like to confirm their
knowledge and interpretation of the quality standards by discussing them with a Preceptor. This will
involve:
� Read the Pre-survey Questionnaire and attachments.
� Review the report of the most recent survey, especially recommendations.
� Inform the Secretariat or the Coordinating Surveyor of any problems.
The Preceptor will:
� Provide advice to the Coordinating Surveyor or members of the team when it is requested.
A typical survey day
The first day of survey usually commences at 0800 hours. The survey day is generally completed
around 1600-1700 hours. It concludes with a team conference to verify findings and
recommendations, especially where more than one Surveyor participated in some elements of the
survey. As a general rule, the team conference should commence around 1500 -1530 hours. The
time at which work is concluded each day has to be reasonably flexible but it needs to take into
account the requirement for a night visit.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 21
The Coordinating Surveyor will usually meet with the Chief Executive Officer of the health service at
the end of each day of the survey to report on any important or potentially controversial matters
and to foreshadow any major recommendations.
Night visits
At least one night visit should be included on each Survey. The coordinating Surveyor should discuss
with the organisation's executive the most appropriate time for night visits to take place and the
mode of access. The purpose of this visit is to enable:
� Night staff to be involved in the Survey.
� The Surveyors to interview night staff regarding involvement in emergency procedures,
continuing education, quality activities and safety.
� The Surveyors to examine how safety, security and other matters are managed after hours.
Coordinating a Survey
Before each survey, the Medical Standards Division will nominate one suitably experienced Surveyor
to coordinate the survey. The Coordinating Surveyor may be any one of the Surveyors but a
Coordinating Surveyor may not necessarily have this role each time he or she participates in a
survey. Special attention is needed in the conduct of the initial meeting with the organisation's
representatives. The Coordinating Surveyor must allow adequate time for the summation
conference and adequate time beforehand for the survey team to plan what is to be presented at
this conference, (refer to checklist of points to be covered in the summation conference). It is
expected that up to two hours may be required for the survey team meeting and one - two hours for
the Summation Conference itself. The Coordinating Surveyor must take responsibility for the content
and timely delivery of the survey report to the Secretariat. The Coordinating Surveyor will also write
a page of General Comments at the beginning of the survey report.
It is important that the coordinating Surveyor is alert to any potential problems that may occur.
Examples of problems include:
� Open hostility towards the ideas and principles of the Quality Standards Accreditation
Survey process by members of.
� Reluctance to make medical records or potentially contentious administrative records
available to Surveyors by the organisation, on the grounds of confidentiality.
� A rift between senior executives of the health service or between the Board Chair and the
executive staff of the health service.
� Hostility towards questioning by board members.
� Surveyors exceeding their responsibilities in pursuing information from staff.
Secretarial Support
A Secretary is allocated to the survey team to type reports as they are completed and attend to
logistical matters relating to the survey such as air ticket confirmation, hotel arrangements etc.
The Coordinating Surveyor must make sure that completed sections of the survey are handed to the
Secretary for typing in a timely manner.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 22
After the Survey
It is important for the Coordinating Surveyor to ensure that the other Surveyors return any final,
completed contentforthe Survey Report within 14 days from the time of the survey and in
accordance with the discussions at the pre-survey meeting. Contact can be made with any late
Surveyors if necessary.
Once the survey is complete it is important for the Coordinating Surveyor to read the collated survey
report to make sure that it is:
� Accurate,
� Unambiguous,
� Comprehensive,
� Consistent in comment.
The Coordinating Surveyor must check that all recommendations are relevant, clear and feasible,
and that every item rated Partially Complies (PC) or Not Complies (NC) has a comment and
recommendation. The Coordinating Surveyor must arrange for the completed Survey Report to be
sent to the Medical Standards Division within 21 days of the survey. After the Survey, individual
Surveyors are not to engage in correspondence about aspects of the survey process with the
organisation. Writing letters to the organisation which may later turn out to be at variance with the
final report can cause difficulties.
The survey approach
For the period of the Survey, Surveyors will work very closely as a team. They should arrange to
meet before the Survey to determine the format of the Survey. Surveyors may agree that an
individual Surveyor will visit a number of departments alone, therefore accepting the major
responsibility for assessment in these areas. Where a department includes matters relevant to more
than one member of the team, two or more Surveyors may visit the department, with one being
nominated to write the assessment. This is often the case in meetings with the Chair and the Quality
Assurance Coordinator; and some complex clinical services may be surveyed in this manner.
The initial approach of the Surveyor to health service staff should be to create a good climate for
discussion and learning. The Surveyor should keep in mind that health services will judge the Quality
Standards Accreditation Survey process by the impression made by the Surveyors and by the way
the survey is conducted. It is therefore of paramount importance that Surveyors are mindful of the
need for diplomacy and tact at all times.
The Coordinating Surveyor is responsible for ensuring that each service of the health service is
covered. He or she will act as spokesperson for the survey team; and should thank the health service
and the Chair of the Board for their invitation to survey. Remember, accreditation Surveys are not
compulsory and the survey team is there by invitation. The Coordinating Surveyor is also
responsible for ensuring that the summation conference proceeds smoothly.
Surveying Techniques
There is no single, required way to conduct a survey. The Surveyors should see most of the health
service and assess the scope and work of all departments and services.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 23
Time constraints may become a problem, so it is essential to obtain an appropriate balance between
delving more deeply into areas which require further assessment, and observing necessary
courtesies and making people feel at ease. The Surveyor should try to avoid having a large number
of points which require additional information towards the end of the survey. Being well prepared
for the survey is often the key to successful time management and a smooth survey.
One of the most important issues facing the Surveyor is the ability to apply the generalist approach
to quality standards across the broad range of health care organisations. Each Surveyor should be
able to survey each kind of organisation with a clear understanding of the intent of the quality
standards and without relying entirely on the literal meanings.
During a survey the Surveyors should:
� Arrive on time.
� Drive or walk around the health care facility.
� Gain a general impression of the institution and its environment.
� Note the condition of things such as the grounds, the external buildings, garbage disposal,
parking accessibility and signposting.
� Upon arrival, take notice of the attitude of personnel, your reception and your first general
impression (i.e., cleanliness, atmosphere and odours).
The Initial Meeting
A meeting will be held at the facility before the survey commences. This may be attended by the
survey team, board members, and senior executive staff of the facility. Morning tea is generally
served at these "getting to know you" encounters.
At some health services, entire Boards may be present for the first and last meetings; at others, the
Board Chair may be the only Board representative present. By agreement of the Chief Executive
Officer with the Coordinating Surveyor, the health service may give the survey team presentations,
i.e. on action taken to deal with previous recommendations, development plans, and innovative
quality improvement initiatives.
It is important that the survey teammeet at a predetermined time and place at the health care
facility. Areas to be covered in the initial meeting between the survey team and representatives of
the organisation to be surveyed are:
� A welcome (usually) is given by a representative of the health service.
� The coordinating surveyor should thank the organisation for the invitation to be surveyed.
� Short discussion on matters requiring explanation or clarification in the documentation
(including Pre-Survey Questionnaire) provided by the health service.
� A brief tour of the health service. (This should be a "walk-through" not a "meet-the-people"
tour).
� Presentations by the health service. This is optional and should be agreed by the Chief
Executive Officer and the Coordinating Surveyor before the survey.
� Examination, discussion and finalising of survey timetable.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 24
� Identification of person/s allocated by the organisation to coordinate timetable details.
� Agreement by the Surveyors and the health service about the time to be set aside, especially
for routine team meetings during the survey.
� Finalisationon special matters, i.e. night visit, meal arrangements, Surveyors start time and
finish time by the survey team and facility.
� General agreement to permit Surveyors to meet and talk to staff members, visitors and
patients at any time during the survey and to review relevant documents.
� Introduction of any Observer and the role of the Observer.
� General agreement for more than one Surveyor to sit in on special meetings, i.e. with
medical board representatives where the medical Surveyor of the team considers this to be
desirable.
� Clear agreement on the following areas of concern for the summation conference:
o Location and time.
o Number of persons attending.
o The format as stated by the Coordinating Surveyor.
o Non-use of tape recorders, video recorders or similar during the summation
conference or attendance of the news media.
� Identification of a contact person who can assist with directions and information. The Chief
Executive Officer’s secretary is usually a good choice.
Care should be taken by the survey team to leave no questions unanswered at this point. Once a
survey commences, time is very limited.
Assessment and Verification
The survey team should visit as many wards, departments and service areas and its health services
as possible and talk to as many members of staff and patients as possible. If the staff have been
involved in preparing for Survey they will be disappointed if Surveyors do not visit their area. In
large institutions it may not be possible to visit all areas without neglecting some other aspect of the
Survey. Therefore, one ward unit which is representative of each of the major clinical activities
should be selected. All service areas should be visited. It will be important to check with the Chief
Executive Officer on any department which has worked exceptionally hard and ensure you visit this
department by the end of the Survey.
The Surveyors should be encouraged to carry notes with them as reminders on matters which must
cover. Similarly, they should feel comfortable to ask probing questions, but be courteous at all times
and avoid being seen as a "know-all", aggressive or overly critical. Surveyors should be conscious of
the need to cross-check statements made to them. If they are unsure about the accuracy of
information given to them, they should check by asking similar questions of others.
Surveyors should discuss any major problems identified with the Chief Executive Officer during the
course of the survey so that these issues are not a surprise at the summation conference. In some
cases the Chief Executive Officer can resolve an apparent problem during the course of the survey.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 25
Surveyors may survey some departments individually and work as a team in others and it is
recommended that all Surveyors pay attention to key areas such as Medical Records, Special Care
Areas, and Governing Body and Management, Infection Control, Waste Management, Improving
Performance.
It is important that the survey team spends at least an hour initially, and thereafter whenever
possible, examining documents related to the roles and functions being examined, i.e. board and
committee structure and minutes, medical board structure, financial and accounting systems,
policies and the general administration of the facility. Matters properly documented in board and
administrative records will tell a story that can later be verified in wards and departments. Do not
rush through the examination of committee, sub-committee and departmental reports. They should
provide a picture of how well a health service operates.
Surveyors should not at any time press their views on a Department Head or Ward Supervisor or
Program Managers during survey. Opinions should be kept for the team and, if necessary, for the
written Survey Report. Surveyors should adopt a kind, reasonable and supportive approach.
Surveyor should progressively write up the first draft of the report with specific attention being
given to each of the standards which requires an answer in the Survey Report. Deal decisively with
the standards one at a time. At the conclusion of the survey, prepare your section of the Survey
Report as quickly as possible.
Each Surveyor should prepare a report covering his or her section of Survey and pass it immediately
to the Secretary for typing. A draft report must be finalised before leaving the health service.
The Summation Conference
Purpose of the Summation Conference:
The purpose of the summation conference is to inform the health service, in general terms, of the
major findings of its survey. All areas of concern and all major recommendations and
commendations must be reported to the organisation so that there are no surprises when it receives
the Survey Report. The summation conference also gives the opportunity for the Surveyors to
receive any comments from representatives of the organisation that might lead to the Surveyor's
comments being qualified, or even altered.
Before summation:
It is important for the survey team to meet before the summation conference so that they
consolidate their own positions and develop consensus. At least two hours should be set aside for
this purpose.
Duration of summation:
The duration of summation will vary according to the size and complexity of the organisation. Where
there are many recommendations to be made, or sensitive issues to be discussed, more time may be
required. An approximate time is 45-90 minutes.
Attendance at summation:
The persons to attend the summation should be the subject of prior discussion between the Chief
Executive Officer and the Coordinating Surveyor. As a guide, the summation conference usually
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 26
includes the Board Chair, members of the Executive, Medical Board Chair and selected heads of
department.
Some health services like to invite all their staff along to the summation conference. Surveyors may
not consider this appropriate particularly where they know a number of sensitive issues will be
raised. Again, this is a matter for discussion and agreement between the Chief Executive Officer and
the Coordinating Surveyor before the summation conference.
Recording of summation conferences:
Summation conferences should not be audio or video-taped or have representatives of the media
present.
Spokesperson:
The Coordinating Surveyor should be the team spokesperson for general statements and individual
Surveyors should report on special areas covered by them. By way of introduction to the summation
conference, the Coordinating Surveyor should inform those present that, while the main
recommendations and findings will be commented upon in the summation session, there may be
some finer points or suggestions also included in the Survey Report.
Summary of the survey process:
Where the Surveyors believe that the organisation did not perform at a high level they should,
tactfully and as helpfully as possible, convey to the CEO and the Board the nature of the major
deficiencies, at all times relating performance to actual standards.
Recommendations must always be referred directly to the Quality Standards and be worded to help
the organisation achieve full compliance with the Quality Standards. Surveyors may also make
suggestions based on their own views and experience but these must be presented in a way that
ensures that they are not confused with the formal recommendations.
Areas which may be addressed in the general overview include:
• Physical condition of facility;
• Attitude of staff;
• Morale of staff;
• Communication;
• Documentation;
• Highlights and commendations; and
• Recommendations.
It is important to remind the organisation that an objective of accreditation is to promote
continuous quality improvement. The quality standards, and the interpretation of them, are being
continually revised and the organisation will not necessarily achieve the same rating at its next
survey unless it can demonstrate further improvement.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 27
Recommendations:
The major recommendations should be outlined and the opportunity given for the health service to
respond. There should be major recommendations in the final Survey Report other than those
reported in the summation meeting.
Survey result:
The Chief Executive Officer and others should be told that Surveyors cannot indicate the
accreditation status that will be awarded until the overall calculations are completed. This is to
account for the possibility of Surveyors after further reflection, changing their mind when compiling
the final report. Surveyors should give the Chief Executive Officer and other senior personnel some
impression of the health service’s general status as seen by them.
Questions:
Surveyors should invite questions and comments from the organisation's representatives,
particularly if there are any points requiring clarification.
Closure of session:
Surveyors should always leave the premises on a friendly note, thanking the staff for their health
service’s hospitality, mentioning specific personnel if warranted. Finally, Surveyors should be
supportive and encouraging in manner, even though the message may be that the organisation has
not reached a high standard for Accreditation. It is important to encourage the organisation to look
upon the survey process as an opportunity for learning and improvement.
After the Survey:
Once the survey is completed a checklist of actions should be developed. Surveyors are to agree on
the way each will write their sections of the report, including:
• Sections requiring "shared" reporting, i.e. Infection Control, Environmental Services, medical
staff matters and patient care matters, Governing Body and Management.
• How the report will initially be typed, i.e. on computer disk or manually using the blank
report supplied.
• Ability to conform to deadlines for completing reports. Problems must be discussed
promptly with the Secretariat.
• Checking arrangements for exchange of material by telephone, fax, email or mail and
contact between Surveyors.
• Completion of the draft report by the Coordinating Surveyor and dispatch to the Medical
Standards division.
Time will be allocated, before the Surveyors disperse, to write up the report so that they are ready
to hand to the Coordinating Surveyor.
Processing of the Survey Report:
Members of the survey team will work individually on the areas covered by them and prepare their
parts of the report. Team members will provide completed reports by the end of the survey and
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 28
edits must be done within 14 days. The Medical Standards Division Secretariat undertakes the final
reading and formatting of the report.
Copies are also sent to each Surveyor (including observers) who are asked to phone or fax any
changes to the Secretariat within seven days. If recommendations are to be added or changed, the
coordinating Surveyor is also consulted. The final report is then sent to the health service.
It is important that Surveyors keep their rough notes taken on a Survey until the Survey is cleared by
the Medical standards Division. Surveyors are also advised that unless there are special reasons or
circumstances, the writing of letters to the health service following a Survey should be left to the
Medical Standards Division.
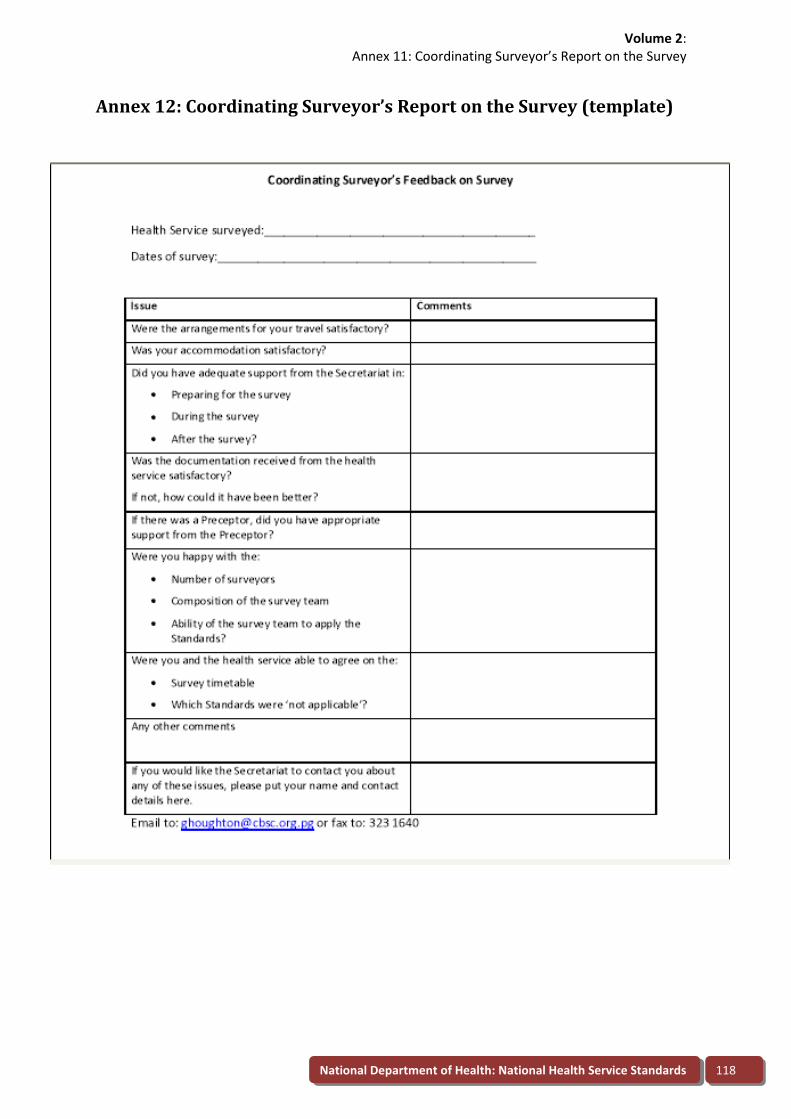
Feedback on surveying technique:
There is a need to continually assess the surveying program. As part of this assessment, health
services will be asked to complete a questionnaire on surveying techniques. The completed
document is forwarded by the Medical Standards Division to each member of the survey team.
Applying the scores: categorisation and definition of scores
Substantially Complies = 2
A long series of Substantially Complies scores with no comments is unhelpful to the health service.
Explanatory comments should be provided wherever possible. Substantially Complies does not
necessarily denote total compliance. On occasions Surveyors may make a recommendation or
comment where it would assist the facility.
Partially Complies = 1
A Partially Complies score must be accompanied by an explanatory statement in the comments
column; a comment in the General Assessment/Commendation page; and an appropriate
recommendation. A Partially Complies score means that, in the opinion of the Surveyor, there is a
substantial part of the criterion with which the health service does not comply.
Does Not Comply = 0
A Does Not Comply score must be accompanied by an explanatory statement in the comments
column; a comment in the General Assessment / Commendation page; and an appropriate
recommendation. Does Not Comply is used when the facility does not comply with the quality
standard.
Not Applicable = n/a
Survey items which are Not Applicable should be accompanied by a comment in the comments
column where it would assist the health service. Not Applicable is used where the criterion or
standard is not relevant to the facility.
Determining Not Applicable services:
If an entire service is Not Applicable this means there is no service provided either internally or
externally. Services which are provided by external consultants or therapists are to be assessed and
recorded in the appropriate area of the Survey Report. It is important to complete the General
Assessment / Commendation page as well as the recommendations page for all external services, i.e.
Laboratory, X-ray, Allied Health Services, Security, Accounting, Maintenance. Give an outline of the
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 29
service provided and the involvement of the provider in the facility's quality activities. It is not
necessary to visit external service providers' facilities but the links between the facility and the
provider are subject to survey.
The Final Report:
The report must be written and typed before the survey team leaves the health service that it is
surveying. Each Surveyor is responsible for the quality of their contributions to the Survey Report but
the Coordinating Surveyor is responsible for the content, style and accuracy of the final report. The
report is from the survey team and the writing style should reflect this. The Survey Report is
available to all Surveyors on computer disk.
The completed report is sent to the Medical Standards Division Secretariat immediately after the
survey. An independent reader must review the contents and inform the Secretariat of any
alterations which are necessary. Any corrections (other than grammar or spelling) suggested by the
reader will be discussed with the Coordinating Surveyor.
The completed report must be sent to the health service within two weeks of the survey and any
concerns managed by the Secretariat in consultation with the Coordinating Surveyor and, if
necessary, the other Surveyors. When the final report is prepared, two copies will be sent to the
health service, one copy will be sent to the Executive Manager of Medical Standards Division for
information.
The Certificate of Accreditation:
The Certificate of Accreditation, signed by the Minister for Health and the Secretary of the National
Department of Health will be sent to the health service as soon as it is available. A duplicate
Certificate will also be presented to the health service at the National Health Conference.
Managing the Health Service Accreditation Process
Responsibility:
The responsibility for the management of the Health Service Accreditation Process lies with the
Medical Standards Division. This will occur in consultation with Surveyors, Chief Executive Officers
and, other standard setting bodies.
Quality Standards and Accreditation Medical Standards Division Secretariat:
The Quality Standards and Accreditation Secretariat is within Medical Standards Division of the
National Department of Health. Its functions are:
1. Coordinate further review and updates for the Quality Standards for Health Services in
Papua New Guinea in consultation with the Quality Standards Development Chair, Surveyors
and the Executive Manager Medical Standards Division.
2. Annually update Surveyors on quality standards.
3. Recruit and train 12 new accreditation surveyors annually in consultation with current
surveyors.
4. Schedule approximately five accreditation surveys each year, especially by managing:
a. Identification of Surveyors.
Volume 2:
Structure and Organisation of the Accreditation Survey
National Department of Health: National Health Service Standards 30
b. Self assessments.
c. Accreditation surveys.
d. Ceremonies and publicity for accreditation awards.
e. Travel and accommodation bookings.
f. Provision of a secretarial service for survey teams.
5. Periodically update the Guide to Quality Standards in Health Services – Health Service
Accreditation Program.
6. Write an annual report on accreditation.
7. Present annual report at the National Health Conference.
8. Organise presentation ceremonies and publicity for accreditation awards.
9. Administration of recruitment and training of accreditation surveyors.
10. Administration of further development of Quality Standards for Health Services in Papua
New Guinea.
11. Maintain a data base of surveys.
12. Maintain a data base of surveyors, including training and participation in surveys.
Volume 2:
Glossary
National Department of Health: National Health Service Standards 31
Glossary
Acronym Full term Definition
Accreditation N/A
ACHS Australian Council on Healthcare
Standards
The body which accredits most health
care services in Australia (and some
internationally)
ACSQHC Australian Commission on Safety and
Quality in Health Care
The statutory body responsible for
leading quality and clinical risk
management in Australia
AHFG Australasian Health Facility Guidelines Specifications for health facilities
developed by the Centre for Health
Assets Australia at the University of New
South Wales.
BPR Business process re-engineering A method for redesigning the way work is
done to better support the organization's
mission and reduce costs.
CQI Continuous quality improvement The process of continuously improving
quality, e.g. we are working to reduce
surgical wound infection rates below our
own best performance, and then below
the best in our Region and then the best
in the nation etc…..
CSF Critical success factor Something that an organisation must do
within a key result area, e.g. timely
emergency care, high quality maternity
care, timely elective surgery
DALY Disability adjusted life year A year of life adjusted for illness or
disability, e.g. a year of life with a severe
disability or illness is of less value than a
year free from disability or illness. It is
used for evaluating the value for money
of health care interventions.
DOTS Directly Observed Therapy, Short-course A major initiative in the WHO
international TB eradication program
EQuIP Evaluation and Quality Improvement
Program
The accreditation process of ACHS
FBO Faith-based organisation
GoPNG Government of PNG
IC Infection control
IHI Institute for Healthcare Improvement An organisation based in the USA which
provides education and leadership in
improving quality and managing clinical
Volume 2:
Glossary
National Department of Health: National Health Service Standards 32
Acronym Full term Definition
risk
ISO International Standards Organisation The principle international body that sets
standards, e.g. for processes and
manufactured products. Other
organisations are licensed to apply the
ISO standards in accreditation
JCAHO Joint Commission on Accreditation of
Healthcare Organisations
The principle accrediting body for health
services in the USA (and for some
internationally)
KM Knowledge Management A system for providing current, evidence-
based information, especially to clinicians
to aid clinical decision-making
KPI Key performance indicator A measure that indicates whether a
critical success factor is being successfully
achieved, e.g. wound infection rate,
immunisation rate, maternal mortality
rate
KRA Key result area One of a small number of things that are
important elements of the role of an
organisation, e.g. emergency care,
elective surgery, outpatient care
NDoH National Department of Health
NGO Non-government organisation
NHP National Health Plan 2011-20
PDSA Plan, do, study, act “The quality cycle”
Preceptor A senior accreditation Surveyor elected
by the Surveyors to provide guidance in
development of the accreditation process
and in accreditation surveys
QA Quality assurance The process of ensuring that a specified,
minimum level of quality is achieved, e.g.
no-one waits longer than 30 minutes to
be assessed in an emergency
department.
QALY Quality adjusted life year A year of life adjusted for the quality of
life of an individual, e.g. a year of life with
a severe disability or illness is of less
value than a year free from disability or
illness. It is used for evaluating the value
for money of health care interventions.
QC Quality control The process of rejecting faulty products.
It has been largely superseded by CQI and
has little application in contemporary
Volume 2:
National Department of Health: National Health Service Standards 33
Acronym Full term Definition
health care except perhaps in rejecting
faulty products such as instrument trays,
sterile packs, pharmaceuticals
RCA Root cause analysis A technique for identifying all the
contributing factors to an adverse event
RCT Randomised controlled trial A technique for comparing the
effectiveness of two courses of action
TQM Total Quality Management A philosophy of quality management
which has been superseded by CQI
VQC Victorian Quality Council The body in the Australian state of
Victoria which leads quality improvement
and management of clinical risk
WHO World Health Organisation The international body, affiliated with the
United Nations, that sets many standards,
objectives and processes for improving
health, especially in developing countries
Annexes
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 34
Volume 2:
Annexes
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 35
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Heal
National Department of Health: National Health Service Standards 36
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 37
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 38
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Healt
National Department of Health: National Health Service Standards 39
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 40
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 41
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health
National Department of Health: National Health Service Standards 42
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 43
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 44
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health
National Department of Health: National Health Service Standards 45
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 46
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 47
Volume 2:
Annex 1: Application of Quality Standards for Health Services in Papua New Guinea
National Department of Health: National Health Service Standards 48
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
1. Patient Care
Standard 1.1: The health service accessibility to the Community.
Criteria Classification objectives
1.1.1 The community that the health
service serves is defined and
information is gathered on its
requirements.
The health service has identified the geographical area and catchment population that it serves including those
referred from other areas. Prevalence rates for significant communicable and non-communicable diseases
affecting the catchment population are identified. These demographic and morbidity profiles of the catchment
population are used to guide service development and provision.
1.1.2 The community is made aware of
services that the health service
provides.
The health service uses a range of strategies to communicate with its community such as notices, pamphlets, radio
sessions, school visits, annual general meeting and open days.
Services are actively promoted and any service closures are made known to the community.
At Health Services with a limited role, i.e. levels 1-4, the services which are available are displayed for the
information of the community.
Temporary disruptions to service resulting from law and order problems, lack of services or supplies or other
causes are communicated to the community through bodies such as schools, churches and local level government
and are logged in a register.
1.1.3 The health service and services
within it can be easily located.
Road signs, internal directional signs, notice boards and helpful staff members assist people to locate services.
There are local language notices where appropriate.
1.1.4 Services are appropriate to the
needs of the community and are
in accordance with the Service’s
delineated role.
Services meet the immediate needs of the local population and are available as advertised.
Referral to higher level Health Services are provided where appropriate. In level 1-3 services, the distance to the
nearest level 4-7 services is displayed.
The services provided by the Health Service are consistent with the National Department of Health’s Role
Delineation statement
National Department of Health: National Health Service Standards 49
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
1.1.5. The hours of operation and fee
schedules are made known to
the community.
Notices inform the public of hours of operation for each section, applicable fee schedules, visiting hours etc.
1.1.6 If emergency services are not
available, or are restricted,
instructions guide clients on
how to obtain a service.
There are signs or notices informing people how to access emergency services if the section closes for any period
during the day. They state where to go or what to do, i.e. “Ring Bell for Service”. ‘Call (Tel Number) for advice’ etc.
Unavailability of service and contingency plans are made known to the public.
1.1.7 There is no discrimination on any
basis in relation to access to
services.
There is equity of access and clients are not turned away because of inability to pay, ethnicity, place of origin or
any other form of discrimination.
There is a register of patients which records their place of origin.
1.1.8 The health service actively
supports the Rural Outreach
Program
The health service has an active program of rural outreach which may include radio consultation, radio ward
rounds, health patrols, clinical visits, emergency response and referrals.
1.1.9 The health facility actively
supports a program of health
promotion.
There is a health promotion program which is delivered in all areas of operation and focuses on priority health
issues such as immunisation, HIV/AIDS, TB and malaria.
It may use health talks, posters or distribution of free material such as condoms.
There is an antenatal program and records of visits are kept in antenatal cards.
The health service uses and promotes distribution of health promotion materials such as:
Posters and promotional materials.
Mosquito nets, condoms etc.
Media dissemination of preventative information
Pamphlets on outbreaks and endemic disease burden.
National Department of Health: National Health Service Standards 50
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
Family screening and contact tracing for TB/HIV.
Epidemic response unit and action plans
1.1.10 The health service
demonstrates progress towards
achieving the national health plan
goals for priority areas.
There are effective programs to promote safe motherhood, immunisation, family planning, VCT and to promote
prevention and effective treatment of malaria, tuberculosis and HIV.
There are facilities for rapid diagnostic tests and, in level 1-3 health services, sputum slide examination for
diagnosis of TB.
National Department of Health: National Health Service Standards 51
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Standard1.2: Each clinical department or unit provides a high standard of clinical care to the patients that it serves.
Patient Care
Criteria Classification objectives
1.2.1 Suitable provision is made for the
personal comfort and safety of
patients and guardians.
There are comfortable beds, clean linen and adequate airflow, i.e. fans.
Adequate hand washing facilities in the ward.
Clean toilets / showers are accessible.
Lights are turned off or down at night.
Waiting rooms are clean and provide adequate seating for outpatients and guardians
Adequate security arrangements exist for the personal safety of patients, guardians and their personal
possessions.
1.2.2 Patient privacy and dignity are
assured and protected within the
constraints of the individual
treatment plan
There is a policy on confidentiality and privacy.
Separate facilities are provided for the examination, treatment and accommodation of adult male and female
clients. Privacy screens are available and used.
There is a suitable private area for triaging upon presentation and discussing private issues with patients and
relatives.
Patients are greeted on arrival and treated with courtesy
1.2.3 Policies and procedures ensure
continuity of care particularly in
regard to communication with
other services and / or the
referring doctor.
Clinical forums (conferences) are used to provide a multidisciplinary approach and good communication between
health care providers.
There are policies for the discharge of patients to their home. They include processes for issue of drugs on
discharge, follow up appointments, or follow up by other health workers, i.e. TB clinic, Mental Health Worker or
rural health staff or private practitioner.
There are policies about referral of patients to other, more appropriate health services to ensure that they receive,
for example, adequate investigative, diagnostic and allied health support and access to critical care services when
National Department of Health: National Health Service Standards 52
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
clinically indicated.
Referrals and discharge arrangements are confirmed in medical records.
There are documented arrangements to deal with patients of visiting medical officers (private practitioners).
1.2.4 Waiting lists, cancellation rates,
and the use of physical facilities
are systematically reviewed and
problems are managed.
Clinics, theatre and surgical wards each have a waiting list for elective procedures. It is reviewed regularly by
management to assess the need for additional services and the efficiency of the service.
Theatre utilisation rates are regularly monitored to ensure effective utilisation
Cancellations for procedures are recorded and monitored.
The time that patients wait to be admitted to a ward after receiving initial treatment in A & E and/or OPD is
recorded and monitored.
Performance is reported to Executive Meeting and Board Meeting and action is recorded in the minutes.
Clinics and units have regular, documented audit or review meetings.
1.2.5 Waiting times in critical care areas
are regularly reviewed to ensure
that patients are prioritised to
ensure that treatment is based
upon clinical need rather than
time of arrival.
There is a triage system to assess patients for urgency of care upon arrival at the facility and to help ensure that
they receive care appropriate to their needs.
Turnaround times for diagnostic services such as pathology, x-ray etc. are regularly reviewed.
Waiting times are regularly reviewed and they are not compromising patient outcomes.
1.2.6 Where Accident and Emergency
services are provided, a system of
triage ensures that patients are
treated in order of medical need.
There is a written policy that describes the triage process to be followed and staff are allocated to this duty.
Effective implementation of the triage system is evident.
1.2.7 Statistics of basic departmental
functions / services are kept and
Statistics are kept of at least the number of admissions and discharges, deaths, births, occupied bed days,
National Department of Health: National Health Service Standards 53
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
form part of the overall
management information system.
outpatient attendances, numbers of client contacts during patrols and the broad classification of diseases treated.
This information is used by staff working in the area with a view to improving services.
Records are available to confirm maintenance of cold chain (where it is available), maternal and child health
program activity, registration of births.
1.2.8 Clinical Indicators as agreed by
the Department of Health are
collected and form part of the
health facility’s monitoring
program and this data is
submitted to the national clinical
indicator monitoring body.
The clinical indicators approved by the National Department of Health are being collected and collated into useful
formats (tables, graphs etc.).
Management, Board and clinical groups use the indicators to review the care that they deliver.
There is evidence of changes made as a result of review of the indicators.
1.2.9 Care is evaluated by health care
providers and when appropriate
with the consumer / patient and
carer.
Clinicians participate in morbidity and mortality review and outcomes of reviews are documented and used to
improve clinical practice.
Critical incidents and adverse outcomes are identified and investigated in order to learn how to prevent
recurrence.
Outcomes of care are explained to patients and guardians.
1.2.10 There are processes for
monitoring the stocks of drugs
and medical and surgical supplies
and re-ordering so that supplies
are available when required.
All wards and patient care areas have access to appropriate drugs and medical and surgical supplies for their role.
Records are maintained of stock used during outreach patrols. There is a stock control system that ensures that
supplies are re-ordered in a timely manner.
In level 3-7 health services, relevant members of staff are trained in standard operating procedures for drug supply
and, in level 4-7 health services, there is a functioning imprest stocking system in patient care areas.
National Department of Health: National Health Service Standards 54
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Staff
Criteria Classification objectives
1.2.11 Adequate numbers of
appropriately qualified and
trained staff are available to
meet the needs of patient care.
Staff numbers meet the current national ‘Staffing Standards’ for these facilities
Staffing levels are monitored and staff members are deployed according to patient load.
Arrangements for staff cover, rosters and contact arrangements are clearly displayed. Sufficient staff are rostered
for evening and night shifts to ensure both staff and patient safety.
There are guidelines and sufficient accredited staff available to provide safe obstetric care.
Where National standards are not met, the facility has initiated actions to meet the requirements such as
restructuring, creating positions, pooling and temporary redeployment of staff etc.
1.2.12 Lines of responsibility within the
service and in relation to related
services are clearly established.
There are organisation charts for the section.
Policies and individual position descriptions clearly set out authorities and responsibilities, i.e. admitting patients,
prescribing drugs, ordering tests, initiating treatment in an emergency etc. This applies to health service staff and
visiting staff, i.e. General Practitioners where applicable.
There are job allocations or duty rosters for each shift (daily, weekly, monthly).
1.2.13 Where the range and volume of
clinical services so requires, the
clinical staff is organised into a
departmental / divisional system
for effective delivery of clinical
services.
Where there are specialists in individual disciplines clinical services are organised along these lines. There is an
organisation structure which reflects this.
Policies, treatment protocols have been developed and are available.
Registrars and interns – where appointed – work within the policies set down.
1.2.14 Suitable continuing education is
available for all staff, including
medical practitioners.
There is a program of regular in-service training available for all staff. Records of training and attendance for
individuals are maintained.
All medical personnel participate in reviews of cases, journal clubs etc. Where there are separate sub specialties,
there is evidence that each sub specialty undertakes review of its cases and reports clinical audit results to the
National Department of Health: National Health Service Standards 55
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Executive and senior staff.
Nurses, Allied Health, Clerical and Support Services Staff also participate in relevant regular in-service training.
Rural based staff have regular access to in-service training and clinical rotation
1.2.15 Creative endeavours including
research, publications and
representation on committees
of professional organisations are
undertaken as appropriate.
All ward or treatment areas are involved in the examination of data collected for the ward and in researching
better ways of treating patients.
Staff members are encouraged to participate in activities of their relevant professional bodies within the limit of
resources.
Where appropriate, staff members participate in formal research programs.
1.2.16 Staff of the Service/ Ward /
Department participate in
regular meetings, team
conferences and quality
improvement activities.
Regular team meetings are held with all staff participating at the ward level. Clinical audit, grand rounds, death
audits are included in this. Minutes are kept and are available to all staff.
In small rural health services there is evidence of regular staff meetings to discuss service delivery and
management issues
Staff members participate in quality improvement activities which are recorded.
1.2.17 There is a plan for provision of
service twenty-four hours per
day.
There is a policy which describes how service will be provided over the 24 hour period.
There are on call rosters etc. There is a mechanism for calling staff, i.e. radio, phone, runner.
National Department of Health: National Health Service Standards 56
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Physical Facilities and Equipment
Criteria Classification objectives
1.2.18 Facilities and equipment are
adequate for the needs of the
service and are maintained in a
safe condition.
Equipment complies at least with the “‘Minimum Equipment Standards’ relevant to the delineated role of the
Service.
There is evidence (stickers or reports) that the Bio-medical Technician has serviced medical equipment or that a
contractor has attended to the servicing requirements.
Medical equipment that has failed is reported to management by way of a special report.
Personnel are trained in the use of equipment, in particular new equipment.
1.2.19 Facilities and equipment are
appropriately located in relation
to patient areas.
Equipment is kept in the patient area in such a location so that it is easily accessible.
There is safe and efficient access to diagnostic, procedural and critical care facilities.
There is efficient/convenient access to toilets, showers, treatment areas, hand washing facilities.
1.2.20 Safe and efficient practice is
ensured through the provision
of appropriate equipment and
supplies.
There is a sufficient stock of all necessary supplies, including drugs, vaccines and clinical consumables such as
syringes, sutures, dressings.
A stocked Emergency Trolley is available.
Stock has not passed its “use by” date.
There are effective purchasing arrangements for non-catalogue and special items.
A cervicograph or partigarm for monitoring progress of women in labour is available in level?
1.2.21 Critical supplies, including a
range for both adults and
children, are readily available for
whenever an emergency arises.
Critical supplies, including emergency trolley drugs and equipment, pain killers, antibiotics, anti malarials, are
available in children and adult sizes and doses as appropriate.
Separate equipment, appropriately sized, is available for use in nursery and Children’s Ward and Children’s
Outpatient Department.
National Department of Health: National Health Service Standards 57
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
1.2.22 Items designated by the
manufacturer for single use are
not reused.
There is a policy on use of items designated for ‘single use’ and there is evidence of compliance with it.
1.2.23 There is adequate storage space
.
There are appropriate secure storage areas for all equipment not in use, i.e. wheel chairs, IV poles, trolleys.
There is secure storage for drugs and medical supplies which is easily accessible and has shelves or storage bins.
There are cool areas or refrigeration for storage of drugs.
All storage areas are clean and tidy.
There are separate storage areas for clean and dirty items.
1.2.24 Steps are taken to reduce noise
in and near patient areas.
Patient areas are kept as quiet as possible.
National Department of Health: National Health Service Standards 58
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Communication and records
Criteria Classification objectives
1.2.25 Patient consent based on
adequate information is
obtained.
Consent forms are held in patient records.
Consent forms are available in the local language or tok pisin as well as English.
Written consent is obtained for all proposed surgical and/or invasive procedures before treatment proceeds.
Patients confirm that they were given an explanation and understood the risks associated with proposed
procedures or treatments before being asked to sign the consent form.
1.2.26 There is effective
communication within the
department and with other
services.
Effective communication within wards and patient care units and with other clinical support areas is effective as
evidenced by comments of staff.
There are areas available for staff communication meetings.
Measures such as nurse call systems, phones, email, PA systems, notice boards, staff meetings, communication
books and newsletters may be used to facilitate communication.
Meetings between clinical staff and management are used to ensure that issues from the clinical level are dealt
with promptly by administration.
1.2.27 Manuals of investigative and
treatment procedures and
protocols are available and are
used.
There are appropriate manuals available within each service area of the health service for treatment protocols or
procedures.
The following documents are available within the relevant service area, there is evidence that they are being used,
and complied with in Provincial Hospitals. Depending on the role of the health service, some of them should be
available and used in level 1-4 health services:
Standard Treatment for Common Illnesses of Adults
Anaesthetic Guidelines for Papua New Guinea.
A&E Procedure and Practice Manual
National Department of Health: National Health Service Standards 59
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
ENT Surgical Audit
Manual of Family Planning
WHO Family Planning
Infection Prevention Policy Guide.
ICU Procedure Manual
Mental Health Care for PNG
Nurses Standard Procedure Manual
Standards of Patient Care
Emergency Obstetric Care
Manual of Standard Management in O&G
Cancer Management Surgical
Guidelines for Treatment of Cancer
Eye Care Standard Proc. Manual
Primary Eye Care: A Simple Guide
Oral Health Services Proc. Manual
Oral Health Services: Min Standards
Paediatrics for Doctors in PNG
Standard Treatment for Common Illnesses of Children
General Laboratory Manual
National Department of Health: National Health Service Standards 60
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
Media
Laboratory Procedure Manual
Waste Management
Radiography Proc. and Practice Manual
Standard Management of STIs
Minimum Standards for STI Services
Post Exposure Prophylaxis to Prevent HIV
Rapid Advice: ARV Therapy
STI Clinic Standards
HEO and Nurses Surgical Handbook
Operating Theatre Procedures
Standard Tray for Operating Theatre
Surgery for Prim. Health Care Workers
Traditional Medicine Policy
1.2.28 The results of investigative
procedures are made available
in a timely manner.
Results and reports for x-rays and urgent pathology requests are quickly available. Routine pathology results are
generally available on the day of ordering the test and x-ray examinations are done on the day of request.
Results are filed on the patient record.
1.2.29 There is a formal process of
patient education, particularly in
regard to medication and
disease prevention.
There are policies regarding the provision of patient education.
There is health education material available in patient care areas.
There is evidence that patients/guardians/parents are educated about the need for medication compliance at the
National Department of Health: National Health Service Standards 61
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
time of discharge
There is evidence that staff provide education to patients and guardians about matters such as TB Treatment, STI
prevention, malaria prevention, infant nutrition, immunisation, and family planning and antes natal care and
prevention and treatment of common childhood diseases.
There is educational material about promotion of breast feeding and good nutrition, exclusive breastfeeding for all
to six months of age including HIV breast feeding mothers.
IEC materials on these matters are clearly displayed for general awareness
Health Education is made available to both mother and father and maternal health awareness information is
readily available.
Information about family planning methods is readily available
National Department of Health: National Health Service Standards 62
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Standard 1.3: Care delivery is monitored by the health care team to ensure that care meets the needs of patients and to assist in the improvement of
care.
Criteria Classification objectives
1.3.1 Indicator data are collected and
used for the evaluation of patient
care and the management of
services.
Data are collected about the patients treated, success and failure rates, i.e. neo natal deaths, maternal deaths,
infection rates, other adverse events and length of stay (NDoH Clinical Indicator Data Set is maintained and used).
Total activity, i.e. admissions, is recorded.
Data are collected about patient and community education and public health measures such as immunisation,
Susu Mama activity, and distribution of family planning information.
The data are used to inform staff meetings, education sessions and relevant committees.
1.3.2 Comparative analysis is
undertaken and the health care
team ascertains reasons for
variance.
Data collected for 3.1 are analysed and information is reported to relevant staff.
Trends are identified and issues evident from trend analysis are addressed in the appropriate forum.
There is evidence that the data and the analyses are reported to meetings of Patient Care Committee etc. There
are adequate resources for this task.
1.3.3 Action is taken to address any
improvements required.
Minutes of staff meeting and relevant committees demonstrate that decisions were made in response to data and
information received.
There is evidence that decisions have been implemented and that staff are aware of any changes made and the
Board has appropriate information through the committee system.
National Department of Health: National Health Service Standards 63
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
2. Leadership and Management
Standard 2.1: The organisation is effectively and efficiently governed and managed, in accordance with its goals and values, to ensure quality of care.
Governing Body
Criteria Classification objectives
2.1.1 The governing body, its officers
and members of its committees
are appointed according to
current legislative requirements
and terms of office.
There are letters or copies of the relevant Gazette available to confirm appointments to the governing body.
Chairpersons and Deputy Chairpersons are appointed in accordance with the relevant legislation. Minutes of the
governing body verify appointments to committees in accordance with the By-laws
2.1.2 Newly appointed members of the
Governing Body are given an
orientation to the health service
so that they understand their
responsibilities.
There is evidence of an orientation program for new members of the governing body. It will include the provision
of acts, bylaws and at least a tour of the health service and introduction to key staff.
2.1.3 Members of the Governing Body
participate in ongoing education
to assist them fulfil their role.
There is evidence that members of the governing body have attended relevant seminars, conferences, lectures.
2.1.4 The governing body specifies why
the health service exists (mission)
and what it wants to achieve
(goals).
The governing body has adopted a Mission Statement and Objectives consistent with the relevant legislation and
they are communicated appropriately to inform the staff, the community, patients and guardians. The Mission
and Objectives may be communicated via the letterhead, information given to patients, flyers and newsletters.
2.1.5 The governing body provides
leadership and has overall
responsibility for the
organisation’s achievements, the
There is evidence that the governing body provides leadership in:
� The health service’s mission and direction;
National Department of Health: National Health Service Standards 64
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
quality of care and the
organisation’s resources.
� The development and quality of patient care; and
� The custody and development of financial, human and other resources.
2.1.6 The governing body ensures that
there are effective working
relationships within the health
service and with the community,
with other relevant health care
providers and other stakeholders.
There is evidence that the governing body ensures that there are effective working relationships within the health
service and with other organisations.
There are memoranda of agreement (or memoranda of understanding) with relevant bodies, including other
health services.
2.1.7 The governing body meets
regularly and ensures
arrangements for continuity of
governance between meetings.
Minutes confirm that the governing body meets in accordance with the Bylaws or its policy
There are delegations to the Chairman or the Chief Executive Officer to make decisions between meetings.
Delegations from the governing body to the Chief Executive Officer/most senior Manager are consistent with
legislation and confirmed in writing
2.1.8 Appropriate committees help the
governing body to fulfil its
responsibilities and assess the
health service’s performance.
The governing body has established the committees specified in the Bylaws and there is evidence that those
Committees are active.
2.1.9 Terms of reference, membership
and procedures are defined for
the meetings of the governing
body and all its committees.
There are terms of reference approved by the governing body covering membership and meeting procedures for
all committees of the governing body.
2.1.10 All committee minutes are
referred to and dealt with by the
governing body.
Minutes of the governing body confirm that all minutes of committees are referred to the governing body.
National Department of Health: National Health Service Standards 65
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
2.1.11 Minutes record the activities and
decisions of the governing body
and all its committees .
Minutes record the activities and decisions of the governing body and minutes have been signed at the
subsequent meeting.
2.1.12 All decisions of the governing
body are communicated in
writing to staff or individuals as
appropriate and the governing
body monitors implementation of
its decisions.
There is evidence that all decisions of the governing body are communicated to the relevant persons in writing.
There is evidence that implementation of decisions is monitored at subsequent meetings
2.1.13. The Governing Body periodically
reviews its own performance to
actively enhance its
achievements and to ensure
improvement in the quality of
care and effective and efficient
management of the Health
service.
The governing body has reviewed its own performance and any appropriate changes were made as a result of the
review.
2.1.14. The governing body ensures the
attendance of executive staff at
governing body and committee
Meetings.
The governing body in level 5-7 health services has a policy requiring its principal advisers, i.e. DNS, DMS and DFA
or equivalent, to attend meetings of the governing body and its committees and they are recorded as “in
attendance.”
In level 4 health services, the policy is that the CEO will attend meetings of the governing body and in level 1-3
facilities; the facility manager will attend meetings of the governing body.
National Department of Health: National Health Service Standards 66
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Chief Executive Officer and Senior Managers
Criteria Classification objectives
2.1.15. The governing body delegates
necessary authority to the Chief
Executive Officer and other
senior managers and they act in
accordance with corporate
policies, delegated authority and
instructions from the governing
body.
There is evidence that executive staff are acting in accordance with the policy and directives of the governing
body.
There are documented delegations to the CEO and other executive staff which define the extent of their authority.
2.1.16. Duties of the Chief Executive
Officer are defined by the
governing body.
There is a documented statement of duties for the CEO set by the governing body.
There are also statements of duties for the DNS, DMS and DFA.
2.1.18. The governing body
recommends an individual to act
for the Chief Executive Officer
when required.
There is evidence that the governing body has duly recommended a particular person to act as the CEO on each
occasion of the CEO’s absence and that recommendation has been forwarded to the appointing Authority.
2.1.19. The governing body reviews the
Chief Executive Officer’s
performance at least annually.
There is evidence of a regular, formal review of the CEO’s performance.
2.1.20. The Chief Executive Officer
reviews the performance of
other senior managers at least
annually.
There is evidence of regular, formal review of the performance of the DMS, DNS, DFA and relevant others.
National Department of Health: National Health Service Standards 67
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Development Plans
Criteria Classification objectives
2.1.21. The health services mission
statement and goals are used
to direct activities of the health
service.
Plans reflect the Mission Statement, Goals and Objectives of the Health Service.
2.1.22. The health services Corporate
Plan is produced in consultation
with and made known to staff,
the community, other relevant
health service providers and
other stakeholders.
The health service’s plans are known to members of staff.
Members of staff are consulted in the development of the plans.
The health service’s plans were made known at the annual meeting, public meetings or open days and formally
distributed to other stakeholders.
2.1.23. Individual services or
departments show evidence of
planning and implementation
of activities consistent with the
Corporate Plan.
Steps are being taken to implement the health service’s development plan.
2.1.24. The Corporate Plan is
implemented and revised as
necessary. The achievement of
the plan is monitored and
action taken to address
improvements required.
Corporate Plans are reviewed by the governing body and, if appropriate, revised at least every three years.
National Department of Health: National Health Service Standards 68
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Organisational Structure
Criteria Classification objectives
2.1.25. Established lines of
responsibility, authority and
communication support
leadership, teamwork and the
integration of services.
There is a documented organization structure showing all levels from the Governing Body down. The staff is
informed about the structure.
The structure supports leadership, teamwork and integration of services.
There are policies for communication, i.e. all correspondence addressed to the CEO, handling of complaints.
2.1.26. The organisation structure is
reviewed at least each three
years or when there is a
significant change, such as
alteration of the role of the
health service or its services.
All organisation charts are dated.
There is evidence of timely restructuring when it is required.
By-laws, Policies and Procedures
Criteria Classification objectives
2.1.27. The health service’s By-laws
and the policies and procedures
are consistent with the
organisation’s goals, accepted
standards, statutory
requirements and regional
responsibilities.
By-laws and policies and procedures are consistent with the mission statement, goals, statutory requirements and
health service responsibilities.
Policies and procedures reflect current standards, i.e. infection control.
Public Hospital By-laws are approved by the Governor General.
2.1.28. Compliance with the policies
and procedures occurs
throughout the health service.
Policies and procedures are implemented throughout the health service and compliance with them is monitored.
Copies of all policies and procedures are available in each work area and members of staff understand and use the
National Department of Health: National Health Service Standards 69
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
policies.
2.1.29. All policies and procedures are
reviewed and revised as
necessary.
All Policies and procedures should be reviewed at least every three years and dated.
Rights and Responsibilities of Patients
Criteria Classification objectives
2.1.30. Rights and responsibilities of
patients are clearly addressed
through policy set by the
Governing Body and there is a
protocol to deal with matters of
complaint.
The rights and responsibilities of patients are the subject of a Governing Body policy and it is available to all
patients, i.e. publicly displayed.
There is a policy regarding the handling of complaints from patient, staff, suppliers and other clients.
The Governing Body is informed about the numbers and subjects of patient complaints and litigation.
2.1.31. Respect for patients/clients is
evident throughout the
organisation.
It is evident that staff members treat patients/clients with respect, are polite and helpful and patients confirm this.
Ethics
Criteria Classification objectives
2.1.32. The Governing Body ensures
that there is a mechanism for
considering ethical issues by an
appropriate ethics committee.
There is a policy for dealing with ethical issues.
The Medical Research Advisory Committee serves as the National Ethical Advisory Clearing Committee – is there a
link to this committee?
2.1.33. All activities are consistent with
recognised clinical
Treatment being used and research being conducted is within recognised clinical practices of the particular
profession. Check by observation in the wards and by talking with professionals.
National Department of Health: National Health Service Standards 70
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
requirements of the profession
and the health service.
2.1.34. Research projects are
approved and regularly
reviewed by the appropriate
ethics committee
Ask if there are any research projects?
Sight approvals by Governing Body and Medical Research Advisory Committee.
Human Resources
Criteria Classification objectives
2.1.35. Human resource policies and
practices comply with statutory
requirements and include
statements on at least,
recruitment and selection,
industrial relations,
performance appraisal,
contractual arrangements,
occupational health and safety,
anti-discrimination and equality
in employment.
There are policies and procedures that have been approved by the Governing Body that address the human
resource issues of this standard.
There is evidence that the policies have been implemented. General Orders are applicable
2.1.36 There is processes for
credentialing and defining the
scope of practice of clinicians
and clinical support staff to
support high quality health care.
The Health Service defines the scope of practice of all clinical staff consistent with the delineated role of the service
and the experience and competence of the individual clinical staff member.
There are policies and procedures and evidence that they are followed.
All managers have qualifications that are appropriate to the work that they do and the service provided.
Risk Management
National Department of Health: National Health Service Standards 71
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
2.1.37 The Governing Body creates a
culture and provides leadership
and resources to improve
performance and ensure
effective management of
corporate and clinical risks.
There are policies and procedures relating to identification and management of risks.
Corporate and clinical risks are identified and rated for likelihood and consequences and risk management
measures are applied.
Relevant Committees monitor areas of enhanced corporate and clinical risk such as financial management, asset
security, the extent of medico legal litigation, outcomes of complex clinical activities, causes and responses to
adverse clinical events and consent to invasive procedures etc.
Financial Management
Criteria Classification objectives
2.1.38. Financial reports are prepared
and presented to the Governing
Body monthly or as appropriate
and the Board satisfies itself
with the quality of the
information provided.
Financial reports are prepared and presented to the Finance Committee and/or Governing Body at the intervals
specified in the By Laws, Acts or Procedure Manuals. .
The Governing Body minutes confirm that it has received and noted them.
2.1.39 The Governing Body ensures
that a financial audit is
conducted not less than
annually and the report is dealt
with at a meeting of the Board.
An annual audit has been conducted by the Auditor General or an approved private auditor.
There is evidence that the report has been received and acted upon by the Governing Body.
2.1.40 There is documented policies
and procedures for all
accounting procedures.
The health service has adopted written policies and procedures for the accounting function which are consistent
with the Financial Management Manual under Public Finance Management Act.
2.1.41 There is an accounting system
that produces information
The accounting system provides accurate, current financial reports for the health service.
National Department of Health: National Health Service Standards 72
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
reflecting the past experience
and the current financial
position of the facility.
It also provides reports on the past position.
It reports payments made as personal emoluments.
2.1.42 There is an appropriate and
effective system of assets
control, including debtors,
inventory and equipment.
There is an up-to-date assets control system.
Debtors and Creditors ledgers are maintained
Information Management
Criteria Classification objectives
2.1.43 Relevant information
Management systems meet the
health services needs.
The health service uses information derived from its management information systems to guide planning and
service delivery.
These include finances, patient statistics, human resource statistics, and operational statistics.
National Department of Health: National Health Service Standards 73
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Environment
Criteria Classification objectives
2.1.44 The physical environment,
including buildings, grounds,
plant and equipment is
managed and maintained in
order to:
� Ensure patient, staff and
visitor safety
� Support efficient health
service performance
� Meet statutory requirements
The health service is clean, neat, tidy and well maintained.
There are fire extinguishers in appropriate locations.
There are no hazards which will affect patients and staff.
There are preventive maintenance programs for buildings, plant and equipment.
There is evidence that the health service is aware of and adopts statutory requirements.
External Services
Criteria Classification objectives
2.1.45 Documented agreements or
contracts cover the
appointment of external
contractors and provision of
their services.
There are current, written contracts with any contractors who provide any services, i.e. security, cleaning, fees
collection, maintenance of equipment, ambulance services, universities and other institutions.
2.1.46 External services are evaluated
by the health service and action
taken to address any
improvements required.
The health service ensures that services are provided in accordance with the contract and that it is getting value for
money.
There is a regular meeting with contractors to resolve issues relating to the improvement of the service.
National Department of Health: National Health Service Standards 74
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Improving Performance
Criteria Classification objectives
2.1.47 The Governing Body, Chief
Executive Officer and Senior
Managers create a culture and
provide leadership, direction
and resources for an
integrated approach to
improving performance
throughout the health service.
The Governing Body receives and acts upon regular reports on Improving Performance (Quality Management).
The Governing Body regularly reviews its own performance.
National Department of Health: National Health Service Standards 75
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
3. Human Resources Management
Standard 3.1: Staff planning ensures the organisation is staffed to achieve its goals and values.
Criteria Classification objectives
3.1.1 Staff planning is undertaken to
support and meet the
organisation’s corporate plan.
There is a staff development plan and it is relevant to the health service and health needs.
The health service can demonstrate that it is taking action to support the level and type of staffing identified in the
development plan.
3.1.2 Planning ensures that
appropriately trained staff
and/or qualified personnel are
available to undertake the type
and level of activity performed
by the health service.
There is a plan or sub-plan which identifies staff training needs and sets the course of action to provide that training.
Appropriate training is taking place.
Affordable measures are implemented to optimise staff recruitment and retention.
Standard 3.2: Staff are appointed through a recruitment, selection and appointment procedure that is consistent with human resources
policy
Criteria Classification objectives
3.2.1Recruitment, selection,
appointment and re-
appointment procedures
ensures appropriate
competence, training,
experience and registration of all
appointees.
The health service demonstrates that it is taking steps to recruit appropriate staff, that it has innovative ideas to
attract staff.
Staff recruitment procedures are in accordance with policy and are fair and based on merit.
There is no bias based on gender or other form of discrimination.
Department and section managers are appropriately qualified and, if necessary registered.
All managers have qualifications and experience appropriate to the work that they do and the service provided.
3.2.2 On appointment each member
of staff receives a job
Members of staff have dated job descriptions and they are available in the workplace.
National Department of Health: National Health Service Standards 76
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
description including
accountabilities and
responsibilities. The statements
are reviewed and revised as
necessary.
Members of staff have acknowledged receipt of their job descriptions.
3.2.3 Accurate and complete
personnel records are created
and maintained, and are
confidential. They are only
accessible to authorised
personnel and the employee.
There are personnel files for each employee and they are up to date.
They can be stored confidentially.
General Orders are followed.
Standard 3.3: A comprehensive program of staff development meets individual and health service needs.
Criteria Classification objectives
3.3.1 An induction program ensures
staffs understand their roles,
responsibilities and the health
services goals.
There is a standard induction program (orientation plan) for all employees that introduces them to the health
service and tells them about its mission, goals, policies and procedures, who’s who, and general expectations.
There is also an orientation at department / section level that is specific to the job to be done.
3.3.2 Staff, including trainees and
new graduates, are adequately
supervised by qualified staff.
All staff and trainees are supervised by an appropriate person. Supervision covers the work that they do and how it
is done, their behaviour at work, arrival and departure etc. Supervision is available on all shifts where new graduates
and trainees are rostered for duty.
3.3.3 Staff are subject to an appraisal
at the end of any probationary
period or at least annually.
The probationary period will usually be the first three months of an appointment.
Appraisals are documented.
There is evidence that the health service and the employee take action in response to the appraisal, i.e. modify job
National Department of Health: National Health Service Standards 77
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
There are links between staff appraisals, the needs of the health service and the training that it provides.
The health service management makes decisions about all training offered to employees and conferences or
workshops attended.
3.3.5 Staff development programs are
assessed and improved to
ensure that they meet the
health service and individual
needs.
The health service reviews its staff development programs from time to time to see whether there is any need for
change.
Staff training is evaluated.
Standard 3.4: Effective workplace relations are facilitated through the use of industrial relations practices.
Criteria Classification objectives
3.4.1 Industrial relations policies and
practices, in line with statutory
requirements, are
implemented and action is
taken to address any
improvements required.
The health service has an industrial relations policy that is consistent with General Orders.
It meets statutory requirements but also plays a part in providing for good relationships with staff and unions.
It includes a mechanism by which staff can bring their concerns to management and receive a fair hearing.
3.4.2 Active consultation about
employment issues occurs
between management,
employees and where
applicable, their
Executive staff meet regularly with staff about employment issues (local conditions, pay issues, security, safety etc.),
and there is a dialogue between the Executive and the unions.
National Department of Health: National Health Service Standards 78
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
representative unions.
4. Management Information Systems
Standard 4.1: Management information systems meet the health services internal and external needs.
Criteria Classification objectives
4.1.1 There is a plan, which identifies
the health services
management information
system needs and enables a
coordinated approach to the
development and use of
information systems.
There is a plan (or part of the development plan) which identifies what the health service hopes to do in management
information. This includes a statement about what is to be collected, how it is to be analysed and who should get
copies. It also has statements about the use and future use of computers to do this work. Information relative to
clinical core indicators, assets, finance, human resource management.
Monthly reports are made available to NDOH where this is appropriate
4.1.2 Management information
systems are routinely
evaluated and improved to
ensure that needs are met.
There should be evidence that the health service is reviewing the management information system regularly (1–2
years) and that the system meets current needs.
4.1.3 There is a system for validation
and protection of data and
information.
There is evidence of regular data audits to confirm the accuracy of data entry, the integrity of systems, the security of
systems and the reliability of computer hardware.
Data stored in computers are backed up.
National Department of Health: National Health Service Standards 79
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Standard4.2: Patient care, management of services, education and research are facilitated by the timely collection and analysis of data.
Data Collection
Criteria Classification objectives
4.2.1 Patient Data is collected in a
timely and efficient manner
and is used for the planning
and delivery of patient care
and management of services.
Other management
information (Human
Resources, Finance,
operational statistics etc.) are
maintained in a separate
system.
There is evidence that data are collected and reported in a timely fashion. This includes the National Health
Information System and reporting ICD10 (Modified) codes for all medical records. It also includes locally collected
statistics. All these must be up to date and available within the health service.
There is evidence that this information is regularly used to evaluate and improve clinical care.
The collection of data is adequately resourced.
Medical Record Data
Criteria Classification objectives
4.2.2 Every patient has a medical
record, which is sufficiently
detailed to enable continuity
of care, education and
research and to facilitate
clinical coding.
Every patient has a record which includes at least an identification page, diagnostic reports, drug prescription sheet,
nursing, medical and allied health notes, theatre sheet and consent forms, blood transfusion record and a final
diagnosis recorded and coded. Check records in the wards.
Where the ‘Helt Buk’ is used as the primary patient record the Health Service maintains supplementary records which
identify, at least, the date of presentation, patient’s name, treating clinician and some detail about the presenting
condition.
4.2.3 All patients, (including
newborn infants only if the
newborn infant is ill), are
Every patient has a unique identifier which is used to identify their records.
National Department of Health: National Health Service Standards 80
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
allocated a unique
identification within the health
service.
4.2.4 Persons who provide care or
authorize care document the
details in the patient
record/chart. All entries are
legible, dated and signed with
designation.
Nurse, medical and allied health staff all record details of orders / treatment in the notes and sign and date those
notes or orders. They must be clearly written.” White out” is not permitted. Check the records in the ward.
4.2.5 Originals, where possible, of all
documents are filed in the
patient record.
Originals of all letters to the health service, x-ray reports, pathology reports, blood cross match report etc are filed on
the record immediately they are available. Check wards and in medical records.
4.2.6 Patient records are made
available upon re-admission.
Medical records are made available to doctors, nurses and other clinical staff on re-admission. There is a procedure
for this in the medical records department.
The key is accessible if medical records are closed after a certain hour.
Reporting Systems
Criteria Classification objectives
4.2.7 Information is made available
to staff in user-friendly format,
which will assist in patient care
and management of services.
Information that is collected is made available to staff in such a way that it will assist with patient care. This includes
statistics about the number and type of patients. It should be made available to all clinical staff. Check to find out
what is available. See also 4.2.8 below.
4.2.8 Statistics consisting of basic
departmental functions are
kept and form part of the
Wards and departments (pathology laboratory in particular) collect information about their functions, i.e. number
admitted, number died and from what cause.
National Department of Health: National Health Service Standards 81
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
overall management
information system.
Pathology collects information about disease patterns, i.e. number of positive STDs or typhoid tests. These can be
analysed to identify disease patterns or an increase in a disease.
Standard 4.3: Patient records are kept secure and safe.
Criteria Classification objectives
4.3.1 Medical records are managed
in such a way that they are
accessible and able to be
found quickly.
There are adequate shelves, a filing system that uses the Unit Record method, and an index system that allows easy
retrieval of records.
The area is tidy, clean and up to date.
There is adequate staff to allow records to be retrieved quickly and staff should be familiar with the system.
The area is secure and limited to medical record staff or those authorised to access it after hours.
4.3.2 The treating medical officer, or
HEO or NO where there is no
medical officer on the staff,
completes medical records
within seven days of
discharge.
The final diagnosis is completed within 7 days.
4.3.3 Medical record data is coded
to allow the production of
quality patient care
information.
Medical record data are coded locally if there are trained staff and recorded in some way so that information from
the coded records can be achieved (spreadsheet or data base) or the coding records are completed and sent to the
National Department of Health for coding.
National Department of Health: National Health Service Standards 82
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Standard 4.4: Medico-legal requirements for information are met.
Criteria Classification objectives
4.4.1 Confidentiality of the patient is
preserved.
There are policies about confidentiality approved by the Governing Body. These are available in the wards and
departments and members of staff know where they are.
4.4.2 Access to patient information
adheres to relevant
professional and statutory
requirements.
Access to patient information (personal details, notes, diagnosis etc) is limited to those people who have a “need to
know”. This will usually be doctors and nurses treating the patient and may include pathology staff, x-ray and
physiotherapy etc. Some of these will have limited need, i.e. pathology.
There is a policy on the production and reproduction of medical records. No copies of any individual’s medical
records are provided to any legal or medical practitioner or insurance agency without the written consent of the
patient or his/her legal guardian.
Information is released only with the approval of the CEO or DMS.
Where the health service uses computerised systems for recording information about individual patients/clients such
systems must have restricted access (password protection/secured access)
4.4.3 Statutory notifications are
reported to the appropriate
authorities within required
time frames.
Infectious diseases which must be notified to the Department of Health are notified within required times.
STANDARD 4.5: Information technology (computers) enhances the health services ability to gather, store and analyse information and to communicate.
Criteria Classification objectives
4.5.1 There is an integrated plan for
the use of computers and
communications technology
within the health service.
The health service has a plan which makes the best use of computers within the health service and also effectively
collects and analyses and publishes information. It should include statements on the use of internet and email etc.,
and will identify standard software to be used.
In level 1-3 health services, the plan may be simple but it is consistent with the amount and complexity of information
National Department of Health: National Health Service Standards 83
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
and communications technology employed.
4.5.2 An information technology
plan is available which covers
at least the following areas:
� Use of licensed software
versions.
� Copies of data are kept
separate from the main
system on backup disk or
tape.
� Standardised computers and
software.
� Management of ongoing
costs.
� The introduction of
computers to support
clinical management.
There are policies on back-up of data and there is evidence that it is followed.
The health service has addressed the continuing costs of computer systems. This might cover patient management
software, accounting, general office use of spreadsheets, word processors etc.
4.5.3 Computer systems are
protected from access by
unauthorised persons.
Computers are in secure area and passwords are used to access the systems and to change data.
National Department of Health: National Health Service Standards 84
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
5. The Environment
Standard 5.1: Infection is effectively controlled throughout the health service.
5.1.1 An infection control program is
developed with multi-
disciplinary involvement and
using the National Department
of Health “Infection
Prevention Policy Guidelines
for Health Facilities” as the
basis for formulation of local
policy and training.
The health service has a program which is in accordance with the NDOH Guidelines. Discuss this subject with all
executives and ask to sight documentation relating to policies, committees at which infection control is discussed.
Check to see that relevant people are represented – nursing, medical, theatres, CSSD, laboratory, environmental
services, infection control officer, management etc.
� Health service acquired infections are prevented and dealt with by measures including:
� Capable laboratory services.
� Adequate infection prevention material.
� Readily available hand washing facilities.
� Non re-use of single use items.
� Staff training.
� Compliant sterilising equipment.
� Notifiable diseases are reported as required.
5.1.2 All staff, patients and
guardians within the
organisation understand their
role in the prevention of
infection.
There is a mandatory training program for all staff, and a copy of infection control policy and guidelines in all
workplaces.
Members of staff in all sections have knowledge of the infection control policy and are putting it to work.
Workflow standards for infection control are considered in each work area and developed in conjunction with the
infection control officer.
Guardians work only with their own patients.
Signs make clear the arrangements for waste disposal and ablutions for guardians and patients.
5.1.3 All service operations minimise Cleaning, laundry, waste disposal and CSSD are working effectively within the guidelines to minimise infection risks.
National Department of Health: National Health Service Standards 85
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
any infection risk in
accordance with the infection
control program.
There is adequate supply and flow of clean water.
Physical design and layout of CSSD and laundry facilities comply with infection control guidelines. Find out what
happens about sanitising of bed pans, urinals, drainage bags. Check use of body bags in mortuaries, preparation of
bodies for transport etc.
The infection control system provides for isolation and containment of infections when required.
5.1.4 A designated person, suitably
trained, is responsible for
implementing infection
control policies and
developing a method of
reviewing practices to
minimise the incidence of
infection.
A person is designated as the “infection control officer”. This is usually a nurse but may also be any other person with
knowledge of infection, i.e. laboratory staff, medical officer. This person may be part time or full time.
The infection control officer is responsible for developing internal policy and implementing it. Suitably trained means
post graduate training or adequate experience acquired under supervision by a post graduate qualified officer. Cross
training with OH&S Officer may be appropriate
5.1.5 Responsibility for coordinating,
monitoring and evaluating the
infection control program is
delegated by management to
a group of relevant staff.
Responsibility for organisation-wide infection control is delegated to a group (Infection Control Committee) which
monitors infection rates, takes appropriate action and evaluates all aspects of the health service’s infection risks. This
responsibility can be taken on by the Patient Care Committee in a small level 4-5 health service but generally requires
a separate group to be effective. Effectiveness will be evidenced by declining/controlled infection rates.
In a level 1-3 health service, the role of the infection control committee and the Infection Control Officer may be
provided by a level 4-7 health service or as a District-wide service.
5.1.6 Process indicators focusing on
compliance with infection
control policies and outcome
measures are collected,
reviewed and actioned as
required.
Indicators are collected and reported in accordance with national definitions and collection processes as required by
NDoH.
National Department of Health: National Health Service Standards 86
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
5.1.7 Cleaning, disinfecting, drying,
packaging and sterilising of
equipment and maintenance
of associated environments
conforms to the guidelines
contained in the “Infection
Prevention Policy Guidelines
for Health Facilities”.
Sterilising is carried out in accordance with the Infection Prevention Policy – Chapters 6, 7, 8 & 9.
These guidelines are available at ward and CSSD level.
Where sterilising services are provided by a third party compliance with Chapters 6, 7, 8 & 9 at that Facility should be
confirmed
5.1.8 The health service has a policy
or educational program to
promote effective
antimicrobial stewardship.
The health service and those who prescribe antibiotics are aware that careless use can promote the development of
resistant micro-organisms.
Standard5.2: Appropriate physical facilities, equipment and supplies assist the health service to fulfil its role and to function safely and efficiently.
Planning and Purchasing
Criteria Classification objectives
5.2.1 The planning of health services,
buildings and plant and the
selection of equipment and
supplies involves relevant staff
and is in consultation with
appropriately qualified
personnel.
When planning new wards, departments etc. the staff who work in those areas are involved in the design and
planning.
The designs take into account the special needs of patients in health services, i.e. access.
Special needs of the area, i.e. pathology, disabled patients, privacy, need to be taken into account. The infection
control officer must be consulted about design.
5.2.2Planning and purchasing
equipment or accepting
donated equipment, must be in
compliance with policy and
New facilities are planned, and new equipment is procured, in consultation with the users and the infection control
officer.
Operating cost, infection control, occupational health and safety, biomedical servicing capabilities and waste
National Department of Health: National Health Service Standards 87
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
consideration is given to at
least:
� Infection control
� Occupational health and
safety
� Waste creation and disposal
creation and disposal are considered.
There are appropriate facilities for hand washing (for staff, patients and guardians), bathrooms, guardians’ toilets
and washing areas, CSSD, kitchen, laundry and isolation of infectious patients.
Facilities and equipment are appropriate to the level of the health service.
Equipment should be standardised where appropriate in accordance with national policy on medical equipment.
User-friendliness and patient comfort should be considered. Operator and Maintenance Instructions must be
supplied. As specified in the National Policy on Medical Equipment, donated equipment must have:
All necessary accessories and attachments for immediate operation
Operation and Service Manuals in English and, where appropriate, availability of user training
Spare parts and consumables for one year's normal operation
Information about the availability of consumables for at least five years
Certification of both electrical safety and correct operation by a competent Biomedical Engineering Service
organization immediately prior to shipment.
PNG standard 240V 50Hz mains power supply, for equipment designed to operate on mains power supply.
Building requirements, Functional Design and Layout
Criteria Classification objectives
5.2.3 The design and layout of all
services allows for safe,
effective and efficient practices
and meet the special
requirements of individual
Wards and clinical areas have sufficient space their function. Space per patient should be about nine square metres
(3mx3m). There is adequate room to get patients in and out.
Functional relationships are reflected in the design of facilities.
All the services of power, light, sinks, oxygen, suction etc are available.
National Department of Health: National Health Service Standards 88
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
services. Privacy of the patient is protected.
5.2.4 Whatever the design or purpose
of the unit, sufficient space is
provided for routine and
emergency care of the patient.
There is sufficient space for routine treatment of the patient – space to manoeuvre trolleys, x-ray machines, space
for theatre team or birth attendants, etc
5.2.5Appropriate storage of
equipment and supplies
enables safe and efficient work
practices.
There is adequate secure storage for supplies needed in the ward or work area. There should be cupboards, shelves,
benches or store rooms that meet the needs of the area.
There is a cool area or refrigeration for storage of drugs.
Ward equipment such as wheel chairs, trolleys, IV poles, crutches all have a place.
Provisions
Criteria Classification objectives
5.2.6 The environment within the
health service is clean and safe
for patients, guardians, visitors
and staff.
The health service and its grounds are clean, there are no hazards and it meets environmental health standards
Utilities (Water, Gas, Electricity)
Criteria Classification objectives
5.2.7 Where water is obtained from a
source other than a public water
supply it is periodically tested for
microbiological safety.
If water is pumped from a well or river to the health service water system, it is tested to ensure that it is
microbiologically safe. Some health service laboratories can carry out water tests. If they cannot then a sample must
be sent by the health service to the Central Public Health
Laboratory that can do the test. Sight the results.
National Department of Health: National Health Service Standards 89
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
Verify the status of essential backup tanks and reservoirs- quality must meet WHO standard for potable water.
5.2.8 There is provision for a
continuous water supply.
The alternative water supply in times of water disruption may be a tank, reservoir, etc.
5.2.9 Emergency light and / or power
supply is available and is regularly
tested.
There is an emergency generator and there is evidence that it is tested at least weekly and is topped up with fuel.
There are battery powered portable lights or solar powered lights where appropriate.
Standard 5.3: Buildings, grounds, plant and equipment is regularly maintained to ensure a safe environment.
Criteria Classification objectives
5.3.1 Buildings, grounds, plant and
equipment are maintained in
accordance with
manufacturer’s instructions or
good practice.
Buildings, grounds, plant & equipment are well maintained.
Maintenance staff have the manufacturers’ manuals and there is evidence that servicing is carried out in accordance
with them.
Good practice is applied, i.e. what might be accepted by the industry, and i.e. painting is done in accordance with
the paint manufacturer’s instructions or in accordance with trade practices.
5.3.2 Equipment is maintained in a
clean and safe working
condition at all times.
All equipment (including bio-medical equipment) is clean, safe and in working condition.
There is an asset management system and a preventive maintenance program for routine servicing of biomedical
equipment, motor vehicles static plant and computer hardware.
National Department of Health: National Health Service Standards 90
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
5.3.3 Equipment is serviced only by
people trained in the
maintenance of that
equipment.
Equipment is serviced only by people qualified to do so. This is particularly important with bio-medical equipment.
Contractors supply qualification details of all staff working on the health service site. The health service checks these
to ensure that it is getting a qualified technician and that work is done in a safe manner.
There are stickers indicating when items were last serviced and when they are due for their next service.
There is a biomededical planned preventative maintenance program.
There is equipment care and operation training for clinical staff.
5.3.4 Current information and
scientific data from
manufacturers concerning their
products are available for
reference and guidance, and for
the operation and maintenance
of plant and equipment.
The health service keeps manuals, operating instructions, product data sheets for all plant and equipment and
products that it uses. Original instructions are kept in the maintenance department with copies at the operator level.
There are product data sheets for all chemicals used in case of poisoning, i.e. cleaning chemicals. These are
sometimes called Material Safety Data Sheets (MSDS).
Asset registers record essential detail about equipment and record maintenance and disposal of unservicable
equipment.
Standard5.4: The safety and welfare of all persons in the health service is protected. THIS IS A MANDATORY STANDARD
Criteria Classification objectives
5.4.1 Occupational Health and Safety
practices are in accordance
with the health services policy
and meet any statutory
requirements.
The health service has a policy on Occupational Health and Safety. There is evidence that practices within the health
service meet the requirements of this policy and any statutory requirements of the Industrial Safety, Health and
Welfare Act and national standards.
There is a workplace policy on HIV/AIDS and post-exposure prophylaxis
5.4.2 Hazards are identified, assessed
and rectified.
The health service has a method of regularly identifying hazards. This can be a reporting notice, regular inspections
& “walk around”.
National Department of Health: National Health Service Standards 91
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
There is evidence that action is taken on the issues identified.
5.4.3 Where hazards are unable to be
eliminated, adequate warning
and protection devices are
used.
Warning signs make known to patients, staff and visitors those hazards that cannot be completely eliminated, i.e.
wet floors.
Personal Protective Equipment is available for all staff.
5.4.4 A safety officer has
responsibility for occupational
health and safety related
activities throughout the health
service and where relevant,
sectional heads of departments
that handle hazardous
materials oversee specific
safety issues.
The health service has a designated safety officer. This is not usually a full time position but additional duties added
to those of a suitable officer. In level 1-3 health services, the safety officer may be provided by a level 4-7 service.
This position continually monitors and promotes safety. OICs of areas that have particular hazards responsibility for
monitoring those hazards, i.e. pathology laboratory, x-ray.
5.4.5 An occupational health and
safety committee comprised of
management and staff,
develops policies, monitors
occupational health and safety
performance and makes
recommendations to
management for appropriate
action to be taken.
There is a committee that takes the lead in occupational health and safety matters. It helps the CEO to develop
policy, monitor the situation in the workplace and make recommendations to management.
In a level 1-3 health service, the committee may be provided by a level 4-7 health service.
It is representative of the workforce.
National Department of Health: National Health Service Standards 92
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Security
Criteria Classification objectives
5.4.6 Security of patients, guardians,
visitors and staff and the assets
of the health service are
protected.
There is a system of providing security for all at the health service. It includes appropriate locking doors and grills for
areas that handle cash or other valuable items, security for drugs, access to phones or alarm systems in the case of
an incident, a guard service (if necessary) provided by a registered, contracted security service or appropriately
trained staff.
There is provision for safe travel during call-outs, evening/night shift changes, There is security for vehicles.
There are Incident reporting systems and information is analysed and used to improve security.
National Department of Health: National Health Service Standards 93
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Fire Safety. THIS IS A MANDATORY STANDARD
Criteria Classification objectives
5.4.7 Fire risk is minimised through:
� Complying with statutory
requirements for fire
standards
� Ensuring that fire hazards are
eliminated, minimised or
performed in a safe manner
� First aid fire equipment is
available and regularly
serviced.
� Fire exits are always kept free
of obstruction.
� Ensuring that an emergency
plan is provided and is
rehearsed.
� Training staff in emergency
fire response and use of
extinguishing equipment
The health service complies with the statutory requirements (building code and/or fire standards) and the
recommendations of the fire brigade. This includes planning buildings and facilities to meet standards.
The health service asks the Fire Brigade to provide an annual inspection which identifies the risks.
The health service is taking action to implement the recommendations of the fire brigade. Many of the
recommendations will involve money that the health service may not have. Others will relate to changed practices
which cost nothing. Do not accept the “no money” answer as a reason to do nothing.
Rubbish, flammable materials are safely stored and handled and safe practices are observed. No smoking policies
are enforced.
There are fire extinguishers and hose reels as recommended by the fire brigade. They have current service tags and
are appropriately located.
Fire exits are free of obstruction, i.e. beds, wheelchairs, boxes, rubbish.
Doors open from the inside and are not locked from the inside. There may be an exception in the case of Psychiatric
Wards, but in this case all staff should have ready access to a key (preferably on their person).
The health service has an emergency fire plan which details what to do in case of a fire and it is rehearsed regularly.
There are records of the training for the plan and all staff members have adequate knowledge of the plan.
There is an annual evacuation drill.
Staff are given at least annual training in the response to a fire in accordance with the Fire Plan.
Staff are trained in use of extinguishers
National Department of Health: National Health Service Standards 94
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Emergency Planning. THIS IS A MANDATORY STANDARD
Criteria Classification objectives
5.4.8 There is an emergency plan for
external and internal disasters
and the plans are known to all
staff and practised at least
annually.
There is an emergency plan (disaster plan) for external disasters (airport crash, bus crash, eruption, etc) and internal
disaster (water failure, building collapse, fire etc). The plans are known to staff and responses are practised annually.
5.4.9 Emergency plans address at
least the following:
� cardiac arrest / medical
emergency
� personal threat including
armed hold-up
� Fire
� Internal emergencies,
including failure of vital
services such as electricity,
water, medical gases and
communications
� Responses to external
disasters, i.e. aircraft crash or
industrial accident
� Responses to natural
disasters, i.e. flood, volcanic
eruption, tsunami, epidemics
The health service has plans to deal with the items included against this criterion. They are available in all areas, are
known to staff and are practised.
Responses to such disasters include a component of co-operation with other bodies such as police and level 4-7
health services will cooperate with the National Disaster Response Unit.
The health service has plans to deal with the items included against this criterion. They are available in all areas, are
known to staff and are practised.
Staff have knowledge of the plans and how to activate them.
An annual drill is held.
Responses to such disasters include a component of co-operation with other bodies such as police, National Disaster
Response Unit, and the Provincial Disaster Response Unit
National Department of Health: National Health Service Standards 95
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Radiation Safety
Criteria Classification objectives
5.4.10 A designated person is
responsible for implementing
radiation safety
A designated person (usually the OIC Radiographer) is responsible for implementing radiation safety practices. This
includes ensuring that staff, patients and the public are not subjected to excessive radiation.
5.4.11 Monitoring and evaluation of
radiation safety is conducted
by a designated person, with
access to appropriate
laboratory resources.
All staff in the x-ray department wear a radiation safety monitor badge.
There is evidence that badges are processed at the specified intervals and the results made known to the staff.
Standard 5.5: Waste is handled, contained and disposed of safely and efficiently. THIS IS A MANDATORY STANDARD
CRITERIA
Criteria Classification objectives
5.5.1 The use of appropriate
procedures and equipment that
conform to relevant statutory
requirement / guidelines
ensure the safe and efficient
handling, collection and
disposal of waste.
There are procedures for the handling of waste and safe disposal of it. They are based upon the Infection Prevention
Guidelines and Environmental Legislation.
Procedures identify how infectious waste and sharps, drugs and cytotoxic wastes and other hazardous substances
are to be separated from other waste and how sharps are to be handled. The procedures also outline the collection
and disposal arrangements with local level government or a contractor.
Expired drugs are disposed of in accordance with NDoH guidelines.
5.5.2 The Infection Control Officer
has a close working relationship
with staff responsible for waste
The infection control officer has a very close link with the waste disposal process and makes regular inspections
(even as often as weekly).
National Department of Health: National Health Service Standards 96
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
management.
6. Improving Performance
Standard 6. 1: A culture of improving performance is created throughout the health service, with leadership, direction and resources from the Governing
Body, Chief Executive Officer and senior managers.
Performance Improvement System
Criteria Classification objectives
6.1.1. The Governing Body is
responsible for ensuring that
there is a system of performance
improvement and that regular
reports are made to the
Governing Body.
There is evidence that the Governing Body accepts ultimate responsibility for ensuring that there is a system by
which performance of the health service is continually improved (also called quality improvement or quality
assurance). This extends across all functions of the health service including medical, nursing, allied health,
management and support services such as cleaning, catering & maintenance.
The Governing Body has this as a standing agenda item, and may receive reports through one of the committees
(usually Patient Care Committee).
There is evidence that the Governing Body acts upon recommendations and generally supports improvement
processes.
The Governing Body sets the policy to ensure that quality improvement is pursued throughout the Health service.
There is evidence of continual improvement.
6.1.2. The Chief Executive Officer is
responsible for coordinating and
evaluating the performance
improvement system.
The CEO coordinates and supports the performance improvement activities.
The CEO receives monthly reports from all areas of the health service and there is evidence that he or she acts upon
the information provided.
There is evidence that the Governing Body’s policy is being implemented.
National Department of Health: National Health Service Standards 97
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
6.1.3. A designated person (where
appropriate) is responsible for
the day to day management of
the performance improvement
system.
There is a designated person responsible for day to day management of the performance improvement activities.
This may be a part time or full time position.
This person knows of all quality activities in the health service and co-ordinates and promotes them and has
adequate authority to promote continuous quality improvement.
6.1.4. All services and staff are
involved in quality activities to
improve performance.
The performance improvement system and the ways that they can be involved in it are understood by the staff.
6.1.5. The performance improvement
system specifies a plan and
identifies resources for quality
activities to ensure a
coordinated approach.
There are plans for the performance improvement activities and resources (money, staff, training, equipment etc)
have been allocated to it.
Performance Improvement Methodology
Criteria Classification objectives
6.1.6. Quality activities enable
continuous performance
improvement and must
incorporate the following
elements:
� monitoring, assessing,
analysing and evaluating
activities
There are records confirming that the elements of this criterion are present, i.e. monitoring, assessing, analysing,
and evaluating.
Timely action is taken to remedy problems.
National Department of Health: National Health Service Standards 98
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
� taking appropriate and timely
action to remedy
deficiencies found
� evaluating the effectiveness
of any action taken
� feeding back results
6.1.7. Quality activities include at
least:
� outcome indicators
� internal and external
customer feedback
� quality control and assurance
� Inspections, external reviews
and other surveys.
� Planned preventive
maintenance activities
Wards and departments use some or all of the activities of this criterion, i.e.:
Clinical indicators/morbidity/mortality rates
Satisfaction surveys, complaints, suggestion box, interviews, focus groups which allow clients to participate in the
review of patient care
Calibration checks etc.
Audits, fire service inspections etc.
6.1.8. The health service
demonstrates improvement
resulting from quality activities.
The health service demonstrates that it is continually improving and not sitting still (and doing nothing about
improving its service).
Refer to 6.1.7.
There is evidence of managed improvement in at least some of the Key Result Areas of the National Health Plan, i.e.
maternal & infant mortality rates, reductions in health service acquired infection rates, reduced rates of client
complaint,
National Department of Health: National Health Service Standards 99
Volume 2:
Annex 2: Quality Standards for Health Services in Papua New Guinea (Amendment Draft 5.0)
Criteria Classification objectives
6.1.9. Confidentiality of both patients
and staff is protected in quality
activity documentation.
Policies and procedures ensure that confidentiality of patients and staff is protected in data and reports.
Patients included in any clinical or management audit data and reports are anonymous or coded.
National Department of Health: National Health Service Standards 100
Volume 2:
Annex 3: Scoring the Mandatory Quality Standards
Annex 3: Scoring the Mandatory Quality Standards
The mandatory quality standards are all in the Environment section of the Quality Standards for
Health Services in Papua New Guinea. They are Infection Control, Waste Management, Emergency
and Disaster Preparedness and Fire Safety. Some of the mandatory quality standards are assessed
on an organisation-wide basis, i.e. “1.1 An infection control program is developed with multi-
disciplinary involvement and using the National Department of Health “Infection Prevention Policy
Guidelines for Health Facilities” as the basis for formulation of local policy and training.”
Others must be assessed in several departments or clinical units, i.e. “1.3 All service operations
minimise any infection risk in accordance with the infection control program.” An example of the
scoring of Standard 1 is:
Quality Standard 1: Infection is effectively controlled throughout the health service
Org
Wide
O&G Paed Pharmacy Blood
Bank
Anaes-
thesia
Path-
ology
Total
1.1 2 2
1.2 2 2 2 2 2 2 12
1.3 2 1 1 2 2 2 10
1.4 2 2
1.5 2 2
1.6 1 1
Total 29
Rating:
Total score x 100
2900
Total score: 29 ------------------------------
Adjusted possible score
------
32
= 90.6%
Possible score: 32
Less: not applicable and not scored 0
Adjusted possible score 32
Therefore, the health service scores 90.6% for this standard and exceeds the 80% score required for
a mandatory quality standard.
National Department of Health: National Health Service Standards 101
Volume 2:
Annex 4: Summation Conference Checklist
Annex 4: Summation Conference Checklist
Matters to be covered by the survey team
Before the summation conference, the Coordinating Surveyor should consult other team members
and decide:
• The time and location of the summation conference.
• The composition (and numbers) of persons from the organisation who will attend. It is wise
to control the size of the group attending the summation conference to allow for frank and
open discussion at senior levels.
• The format of the meeting, i.e.:
o The Coordinating Surveyor to lead off and make appropriate, general comments
about the performance of the health service.
o The "order of appearance" by the individual survey team members.
o The matter of questions, comments and explanations, and when these should be
dealt with, i.e. at the end of the report on each standard or at the conclusion of the
summation conference.
The final summary by the Coordinating Surveyor will include:
• A request for any questions to individual Surveyors or the team on matters covered during
the Survey and at the summation conference.
• A comment to the effect that any major recommendations appearing in the final Survey
Report will have been made at the summation conference.
• A reasonable explanation of the processes to occur following the survey. This will include an
estimate of the time within which the final report can be expected, taking into account
preparation by the Surveyors, the checking, reviewing by Coordinating Surveyor and the
Secretariat.
• A final thanks on behalf of the team
National Department of Health: National Health Service Standards 102
Volume 2:
Annex 5: The Survey Report
Annex 5: The Survey Report
Guiding principle
� Aim for a readable, comprehensive and accurate report. Provide sufficient information,
clearly written and presented, to help the various readers and users of the Survey Report.
� The report is from the survey team but responsibility for approving the final content lies with
the Coordinating Surveyor.
Guidelines on Survey Report Writing
The report writing stage is vital to the success of the Quality Standards Accreditation Survey. The
health service expects to receive a Survey Report which is useful to them.
The comments and recommendations in the Survey Report are based on the criteria in the Quality
Standards.
� The Survey Report has four major purposes:
� To serve as a self-assessment tool for a health service prior to survey.
� To record the observations and findings of the Surveyors.
� To facilitate the accreditation award process.
� To serve as a management tool for the health service to use in the continuing improvement
of its service.
The Survey Report should accurately and objectively reflect a health service's compliance with the
quality standards.
� The following points are to be observed when completing the Survey Report:
o The title page is to include:
o Full name of the health care facility being surveyed.
o Dates of the survey, i.e. 12/11/2010 - 15/11/2010
o Alphabetical list of the names of the Surveyors with the exception of the
Coordinator Surveyor who should be listed first and the words “Coordinating
Surveyor” written beside the name. Where an Observer is present, the Observer's
name is to be written last and the word 'Observer' noted beside it.
� Summary of Survey Assessment page, including the individual scores for each section of the
survey.
� All survey items must be answered with the appropriate compliance score.
� You are writing on behalf of the survey team so the style in which findings should be
expressed is “The survey team found that……”
� The style in which recommendations should be expressed is “It is recommended that…..”
National Department of Health: National Health Service Standards 103
Volume 2:
Annex 5: The Survey Report
� The style in which commendations should be expressed is “Nambawan General Hospital/the
Intensive Care Unit/the Maintenance Department is commended for…..” or “The survey
team commends….”
� Only one answer is to be given for each survey item. Comments made must be in full
sentences. The answer 'yes' is not sufficient nor phrases such as 'meets quality standards'.
� Designations such as 'Director of Nursing' or ‘External Contractor’ should generally be used
in preference to proper names or trade names.
� Do not be coloured or limited by your own experience.
� Scores, comments and recommendations must relate to the words and the intent in the
Quality Standards or the annotations. Commendations can be based on the Surveyor’s own
judgement and experience.
� Review and report on action taken in response to recommendations from a previous Survey,
where applicable.
� Discuss any controversial issues with other members of the survey team to obtain
consensus, before the summation conference, on how to report findings.
� Provide an explanatory statement and an appropriate recommendation for all PC or NC
ratings.
� A page of SC ratings without comments can be unhelpful so try to provide some explanatory
comments which will help the health service to understand the thinking of the Surveyor.
� Record commendations about the service in the Commendation/ Recommendation page.
Also include any potentially useful suggestions for improvement or change which do not
constitute a formal recommendation.
General guidelines on expression and writing style
� Use simple language.
� Write objectively using the third person. Do not refer to trade names or identify the names
of individual people.
� Write in the active voice whenever possible for clear and direct communication, i.e. 'Staff
indicated satisfaction with the new facilities' instead of 'Satisfaction with the new facilities
was indicated by staff.
� Correct spelling, grammar and punctuation are vital. The Survey Report is a formal report.
Use of colloquialisms is not appropriate. Use complete sentence structure. Avoid long
sentences or paragraphs.
� Use the Oxford Dictionary as a guide to correct spelling or the Australian English spell
checker on a computer.
� Use lower case unless referring to proper names or official titles, i.e. Mr Michael Green,
Chief Executive Officer. Use lower case for such references as nursing staff, medical
personnel, cleaning staff, committee members.
� Avoid using hyphens unless an accepted spelling or necessary to avoid ambiguity.
National Department of Health: National Health Service Standards 104
Volume 2:
Annex 5: The Survey Report
� As a general rule, do not use symbols, i.e. the ampersand (&). The exception is the per cent
symbol (%) which, for the sake of consistency and space saving, should always be used in the
Survey Report.
� As a general rule, minimise the use of abbreviations. Spell the word(s) in full followed by the
accepted abbreviation in brackets for the first reference in the text, i.e. quality activities
(QA).
National Department of Health: National Health Service Standards 105
Volume 2:
Annex 6: Other Standards and Guidelines that a Health Service Should Use
Annex 6: Other Standards and Guidelines that a Health Service Should
Use
� Standard Treatment for Common
Illnesses of Adults
� Anaesthetic Guidelines for PNG
� A&E Procedure and Practice Manual
� ENT Guide
� Australasian Health Facility Guide.
� Gender Equity – Training Manual
� Manual of Family Planning
� WHO Family Planning
� Infection Prevention Policy Guide
� ICU Procedure Manual
� Mental Health Care for PNG
� Nurses Standard Procedure Manual
� Standards of Patient Care
� Emergency Obstetric Care
� Manual of Standard Management in
O&G
� Cancer Management Surgical
� Guidelines for Treatment of Cancer
� Eye Care Standard Proc. Manual
� Primary Eye Care: A Simple Guide
� Oral Health Services Proc. Manual
� Oral Health Services: Min Standards
� Paediatrics for Doctors in PNG
� Standard Treatment for Common Illnesses
of Children
� Waste Management
� Radiography Proc. and Practice Manual
� Post Exposure Prophylaxis to Prevent HIV
� Rapid Advice: ARV Therapy
� STI Clinic Standards
� HEO and Nurses Surgical Handbook
� Operating Theatre Procedures
� Standard Tray for Operating Theatre
� Surgery for Primary Health Care Workers
� Traditional Medicine Policy
National Department of Health: National Health Service Standards 106
Volume 2:
Annex 7: Surveying the Improving Performance Standard
Annex 7: Surveying the Improving Performance Standard
A health care facility must be able to demonstrate that it has improved the quality of care or service
in significant areas of its operations, especially major aspects of clinical care. Therefore the
Improving Performance section is very important.
Performance improvement is often referred to by other names, such as Quality Assurance, Quality
Improvement, Best Practice, Continuous Quality Improvement, QAT etc. The name is not important
for survey purposes – what is important is that the health service demonstrates (by whatever
method) that it is continually trying to improve its performance.
General Principles
Familiarise yourself with the “Improving Performance” section of the quality standards.
Ensure you understand the all embracing nature of the term "improving performance," i.e. no one
quality method is prescribed or expected.
Be prepared to recognise the different terminology and approaches to quality which you will find in
use in health services.
Remember the need for all services and staff to be committed to, and involved with, Improving
Performance.
Apply the ‘reasonable person’ test to a health service's individual situation. Do not be prescriptive.
Interpretation of the Quality Standard
Difficulty may be experienced in interpreting a number of the terms used in and elements of the
Improving Performance Standard and its associated criteria. Consider the following points for
clarification:
� "a culture of improving performance is created". Observe and check to see that generally
staff are aware of the health service’s program of improving performance, that they know
what their department / section is doing and why and generally they know what else is
happening to improve performance in the health service.
� “continuous performance improvement” simply means that the efforts continue, i.e. the
health service has systems for systematic quality monitoring and improvement rather than
piecemeal, ad hoc projects. All major departments and services should be incorporated in
the quality activities program and that a whole of health service perspective on quality is
taken.
� Health services must be able to provide evidence of health service-wide improvement if they
are to be high achievers in this standard.
� “All services and staff are committed to and involved ….”Consider the size and role of the
health service. Quality activities should be relevant to the health service’s service priorities.
Check that key performance areas - major aspects of care and service - are monitored.
National Department of Health: National Health Service Standards 107
Volume 2:
Annex 7: Surveying the Improving Performance Standard
� In general, each department or service area should be involved in quality activities. Staff
should generally be aware of quality activities – not just the bosses. Some judgment will be
necessary on the part of the Surveyor to apply interpret this.
� “Governing body is responsible for…”. Although the governing body's role is usually an
indirect one, it is important that it supports and facilitates the health service's quality goals.
In order to assess the governing body's role in leadership and direction and its interest in the quality
standards of care and service delivered:
� Look for a planned health service-wide approach to quality with commitment from the
Governing body which includes resources (i.e. personnel).
� Check that the Board is setting policy, providing resources, kept informed, providing
informed feedback.
� Consider interviewing the Board Executive and / or the Patient Care Committee Chair rather
than just the Chair of the Board. Also interview at least two Board members and ask about
quality activities which have led to change.
� Where applicable, request the Board to give examples of achievements.
� Discuss with the Board how they determine quality activity within their facility and their
level of involvement, especially in relation to results.
� Check to see that the health service collects the Department of Health NHIS and hospital
clinical data as required by monthly reporting. Ask to see how this information is dealt with
by the Board and by Management, Sections etc, i.e. What do they do with it?
What else should you look for?
Check that quality is a regular agenda item on Board and senior management meetings to verify
extent of commitment, leadership and direction shown by governing body and management. Check
agenda and minutes.
Check the terms of reference of the health service-wide quality committee or alternatively check
that responsibility for health service-wide quality program is a regular item on another appropriate
multidisciplinary committee.
Review the organisation chart which identifies how quality activities are coordinated across the
organisation, i.e. specifying lines of responsibility and reporting mechanisms for committees and
Quality Coordinator if appointed. Check the reporting mechanism to the Board.
Assess whether there is sufficiently representative involvement of all staff in quality activities across
the health service, including multidisciplinary or inter-departmental activity.
Check that the health service-wide quality program includes mechanisms for setting priorities,
providing feedback and reviewing and evaluating effectiveness regularly, i.e. annually.
Implementation and reporting
Health services must have more than plans. They must demonstrate action in conformance with
their plans and have a system of reporting that assures management that quality issues are being
addressed.
National Department of Health: National Health Service Standards 108
Volume 2:
Annex 7: Surveying the Improving Performance Standard
Action should deal effectively with problems and lead to continuing improvement in the quality of
care and service provided.
Check that the reporting system demonstrates, not only that quality activities are undertaken, but
also that progress is reported to an appropriate authority, either an individual or a properly formed
group.
Check that agendas and minutes of relevant committee meetings show evidence that the health
service-wide program is operating according to plan.
Adequacy of resources
Criterion 1.5 refers to the identification of resources. It is not prescriptive. The test should be
whether resources enable a health service to meet the performance improvement standards and are
supplied in conformity with its size, complexity and quality plans.
Look for evidence that the health service’s performance improvement program is being adequately
resourced to bring about effective health service -wide quality improvement. Identify links between
education and quality activities.
Look at how the governing body handles the situation where the planned range of quality activities
is not undertaken because of inadequate resources. Seek an explanation from Board members and
senior management for any shortcomings.
Seek feedback from key personnel as to whether they consider their quality activities program is
adequately resourced.
Quality activities resource personnel
The intention of criterion 1.3 is that health service staff have access to resource personnel (Quality
Coordinator, however named) able to help them to be involved in quality activities pertinent to their
areas of work. The number of resource persons and their level of expertise will vary according to the
size and role of the facility.
Look for evidence that these resource personnel are accessible to and utilised by all levels of staff.
Look at how effectively these personnel carry out their resource role, i.e. participation in
committees, committee reports, feedback from staff.
External contracts
Some health services engage contractors to provide services, i.e. cleaning, security, catering,
accounting, fee collection, maintenance of buildings and equipment. A contractor should deliver
services at a specified level of quality which can be assessed by the health service at the point of
delivery. It is for the health service to determine the standards of service it requires and to establish
appropriate means of monitoring, reporting on and responding to that information.
Generally speaking, those aspects of the service which are "invisible" to the health service are not
covered by the survey. Check that contracts or letters of agreement with providers of external
services specify quality issues relevant to the service and contain the requirement for quality
activities to be consistent with the policies of the health service.
Check that contractors understand the requirement for quality activities.
National Department of Health: National Health Service Standards 109
Volume 2:
Annex 7: Surveying the Improving Performance Standard
Interview staff affected by the contract to assess the quality of contracted service and compliance
with the contracts.
Check that health service has dealt with any problems affecting the contracted service.
Where relevant, look at the contractor's involvement in the health service's quality program, i.e.
committee involvement, participation in formal quality activities, in-service education.
Elements of quality activities
Criterion 1.6 is quite explicit.
� Check that quality activities have moved beyond monitoring, auditing and assessment to
ensure appropriate action and follow-up.
� Ask staff to identify significant outcomes of completed quality activities in which they were
involved over last 12 months.
� Check for supporting documentation.
� Look for evidence of change in policy or procedure as a result of quality activities, i.e. the
application of results in the maintenance and improvement of clinical practice or service
delivery.
� Identify issues which the facility is currently addressing, look for all elements of the quality
cycle, including a timetable for action.
� Find evidence of use of data. What has changed due to analysis of data, i.e. change in
staffing of casualty based upon a survey of times of presentation. Check that data are used
to assess and improve patient care or service delivery.
� Check for evidence of feedback to staff, for example, by talking to staff and viewing minutes,
newsletters and other documentation.
Feedback from customers
There needs to be a mechanism to ascertain the opinions of customers of the health service.
The intent is to ensure that a facility makes a significant attempt to establish and respond to
customer opinion. It is not necessary for every customer or every department to be included but
customer satisfaction should be regularly assessed through the health service quality program.
Check that the health service as a whole and individual departments have identified customers of
their service, both internal and external. Look for evidence that they have made a significant
attempt to establish and respond to customer opinion, i.e. changes in services in response to
customer feedback.
Relevant information systems
A health service should define the information it requires to implement its quality activity plan.
Relevant information systems include both the information needed to support quality activities, i.e.
clinical indicator data, and the information which should be reported on quality activities
undertaken and results achieved.
National Department of Health: National Health Service Standards 110
Volume 2:
Annex 7: Surveying the Improving Performance Standard
View the quality plan and identify information requirements, i.e. utilisation and financial data. Check
whether timely and accurate data are available on key service/performance areas to support quality
activities, i.e. infection control rates, infant mortality rate.
Review quantifiable results of quality activities.
Method of Survey
A health service’s level of compliance with the Improving Performance standard is judged on the
evidence gleaned at survey. The Quality Standard emphasises the importance of improved outcomes
as a result of quality activities and of regularly seeking feedback from customers.
Consider the following methods for obtaining evidence:
� Early in the survey, interview a range of people from individual departments through to
senior management. Discuss their understanding of the quality activities program, the
reporting and management structure and where it fits into their day-to-day work. Assess
their knowledge of relevant facility-wide and department plans and their participation in
quality activities.
� Ensure that all survey team members are included in the interview with the quality activities
coordinator.
� Peruse appropriate documents, particularly the quality plan, minutes of quality-related
committees and data resulting from quality activities and assess their relevance to ensuring
a safe and caring environment for patients, staff and visitors.
� Examine how feedback is sought from customers of the service and what is done with it,
both health service-wide and within individual departments.
� Look for evidence of completed quality projects to assess whether the quality cycle is
followed in practice and activities have progressed beyond monitoring and assessment
through to continuing improvement, i.e. problems are acted upon, staff can identify changes
in policies, and/or procedures, and improvements in outcome are identified.
� Look to see what the quality committee (however named) does with the data presented to
it.
� Look to see the extent to which resources are made available to support quality activities,
including personnel, education and equipment.
� Include discussion of the Board’s commitment to quality when speaking to the Chair and
other Board representatives.
National Department of Health: National Health Service Standards 111
Volume 2:
Annex 8: Surveying the Environmental Standard
Annex 8: Surveying the Environmental Standard
The Environment Standards encompasses patient safety, occupational health and safety, accident
and incident reporting, security, fire safety, emergency planning, infection control and waste
management. This is where the mandatory quality standards are found.
This section provides a consolidated focus on all environmental and safety issues. In some areas
covered by this standard, considerable reliance is placed on compliance with external standards or
reviews, i.e. fire safety. This represents a need to rely upon the expert opinion of specialists in the
various fields covered by this standard. In the following discussion, some suggestions are made to
Surveyors on key issues that need to be watched during surveys.
Fire Safety
In the section on fire safety, an inspection report by an appropriate fire authority each year is the
standard requirement. The standard places the emphasis on the fire authority's report and
Surveyors need to evaluate progress in implementing the fire authority's recommendations when
assessing compliance with the standard.
Some towns may not have fire brigades, in this case it will be necessary to determine whether the
health service has sought the advice of the Fire Service from another area or a private consultant.
Occupational health and safely
Surveyors will be aware that occupational health and safety legislation is not widely known or used
in the health industry yet the health services have a high level of potential danger to staff and
patients.
See the section on occupational health and safety and become familiar with the check list which is
included in that document.
Emergency planning
The Standard on Emergency Planning requires health service to have both internal and external
disaster plans. This includes cardiac arrest / medical emergency, fire, personal threat / hold-up,
internal failures of health service systems (i.e. water supply or electricity) as well as external
disasters.
When surveying external disaster plans check that there is a link with the local airport disaster plan
as well as any plans established in the province under the National Disaster Response group.
See the section containing example emergency plans.
Infection Control
Infection control is a major issue for health services. The guidelines produced by the Department of
Health should be used to survey this section.
See the section containing the guidelines and the checklist.
National Department of Health: National Health Service Standards 112
Volume 2:
Annex 8: Surveying the Environmental Standard
Waste Management
Waste Management and Infection Control go hand in hand. When surveying this section use the
Infection control guidelines and also see the example waste management policy.
National Department of Health: National Health Service Standards 113
Volume 2:
Annex 9: Survey Check List (template)
Annex 9: Survey Check List (template)
Quality Standards Accreditation Survey Check List
Health Service:
Survey Dates:
Travel Accommodation Travel
Allowance
Booked Tickets
issued
Informed Booked Paid Informed Paid
Coordinating
Surveyor
Medical
Surveyor
Nursing
Surveyor
Clinical Surveyor
Secretary
Observer
National Department of Health: National Health Service Standards 114
Volume 2:
Annex 9: Survey Check List (template)
Budget prepared
Funding source
Pre-survey questionnaire completed
Health Service has current standards
Survey timetable drafted
Distribution to Surveyors:
� Previous survey report
� Self assessment
� Badges
� Work Books:
o 1 copy of organisation wide
criteria for each Surveyor on
white paper
o 20 copies of Clinical
Departments and Services on
paper of a second colour.
o 10 copies of Environmental or
Non-clinical Service /
Department on paper of a
third colour.
Secretary has Work Book and Survey
Report templates
Computer and printer arranged
Survey time table negotiated by
Coordinating Surveyor and hospital
Feedback questionnaires distributed to:
� health service
� coordinating Surveyor
� Surveyors
Report
� Draft written
� Final copy written
Electronic report distributed to health
service for comment
Report Distributed to:
� NDoH
� Health service
Certificate distributed to health service
Award ceremony
National Department of Health: National Health Service Standards 115
Volume 2:
Annex 10: Coordinating Surveyor Check List (template)
Annex 10: Coordinating Surveyor Check List (template)
Before the Survey
1. Discuss the travel and accommodation arrangements and the composition of the survey
team and secretarial support with the Secretariat in NDoH.
2. Contact the CEO of the health service which is to be surveyed:
• Ensure that the scope of the survey is agreed, especially any outreach or remote
services, academic or research institutes that are – or are not – part of the survey.
• Confirm which criteria will be “not applicable” for the survey. To ensure a consistent
approach for different surveys, the “non applicable” criteria must also be confirmed by
the Secretariat.
• Ask who will be the main contact for organisation of the survey. This will often be the
Quality Coordinator.
• Ask if there are any sensitive or especially complex issues that the survey team needs to
be aware of. These could be industrial relations, inter-personal, inter-professional or
tribal problems.
3. Contact each of the Surveyors and ensure that:
• They know which parts of the survey and the Standards they will be responsible for.
• Their travel arrangements are in hand.
• Any observers are assigned to appropriate criteria and are accompanied by an
experienced Surveyor at all times.
• They know where and when the pre-survey meeting of the survey team will be held.
4. Contact the person at the health service who is responsible for organising the survey to:
• Ensure that they understand what pre-survey information needs to be distributed to
the Surveyors.
• Arrange the time table for the survey. The time table will list all the visits, interviews
and meetings for each surveyor but must also allow time for each Surveyor to
undertake unscheduled verification of compliance with the Standards and time for
the team to meet to discuss their progress.
At the Survey
5. Serve as spokesperson for the survey team at the meeting with health service personnel on
the first day of the survey and at the summation meeting.
6. Give the Organisation’s Feedback on Survey form to the CEO.
7. Meet the CEO at the end of each day of the survey to:
• Report on any difficult issues
National Department of Health: National Health Service Standards 116
Volume 2:
Annex 10: Coordinating Surveyor Check List (template)
• Seek feedback from the CEO on the health service’s view of the survey and the
Surveyors.
8. Inform the Secretariat immediately if any problems arise on the survey which the
Coordinator cannot resolve.
9. Ensure that the survey report and all ratings, scores and recommendations are written
before the survey team leaves the health service.
National Department of Health: National Health Service Standards 117
Volume 2:
Annex 11: Organisation’s Feedback on Survey (template)
Annex 11: Organisation’s Feedback on Survey (template)
National Department of Health: National Health Service Standards 118
Volume 2:
Annex 11: Coordinating Surveyor’s Report on the Survey
Annex 12: Coordinating Surveyor’s Report on the Survey (template)
National Department of Health: National Health Service Standards 119