70
Methodology and tools NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016 MINISTRY OF HEALTH AND SOCIAL PROTECTION OF THE REPUBLIC OF TAJIKISTAN
| Date post: | 11-Sep-2018 |
| Category: |
Documents |
| Upload: | nguyentruc |
| View: | 216 times |
| Download: | 0 times |

Methodology and tools
NATIONAL MICRONUTRIENT STATUS SURVEY
IN TAJIKISTAN 2016
MINISTRY OF HEALTH AND SOCIAL PROTECTION OF THE
REPUBLIC OF TAJIKISTAN

Methodology and tools
NATIONAL MICRONUTRIENT STATUS SURVEY
IN TAJIKISTAN 2016
MINISTRY OF HEALTH AND SOCIAL PROTECTION OF THE
REPUBLIC OF TAJIKISTAN

Acknowledgment
The National Micronutrient Status Survey in Tajikistan, 2016 was implemented by the Ministry of Health and Social Protection of Population of the Republic of Tajikistan and supported by UNICEF and World Bank with the financial contribution of Japan Scaling up Nutrition Trust Fund. Technical support for the preparation, implementation, and analysis of the survey was provided by the Swiss Tropical and Public Health Institute.
Table of Contents
1 Introduction ....................................................................................................................... 4
2 Demographic and geographical context ........................................................................ 4
3 Study design and sampling ............................................................................................. 5
4 Sample size ........................................................................................................................ 6
5 Primary and secondary endpoints .................................................................................. 8
6 Field data collection .......................................................................................................... 8
6.1 Field teams and piloting ............................................................................................ 9
6.2 Day-to-day work organization, supervision and quality control ........................... 9
6.3 Household inclusion and identification ................................................................. 11
6.4 Questionnaire and ODK forms ................................................................................ 12
6.5 Anthropometric measurements of children (0-59 months) and women
(15-49 years) ............................................................................................................. 13
6.6 Biological sampling ................................................................................................. 14
6.7 Salt iodization ........................................................................................................... 14
7 Data management and analysis .................................................................................... 15
7.1 Data entry and analysis ........................................................................................... 15
7.2 Anthropometric analysis ......................................................................................... 15
7.3 Minimum Dietary Diversity for Women .................................................................. 17
7.4 Haemoglobin ............................................................................................................. 17
7.5 Laboratory analysis ................................................................................................. 18
7.5.1 Iron status indicators ........................................................................................... 19
7.5.2 Inflammation ........................................................................................................ 21
7.5.3 Retinol binding protein ........................................................................................ 21
7.5.4 Vitamin D ............................................................................................................. 22
7.5.5 Folate .................................................................................................................. 22
7.5.6 Urinary iodine concentration ............................................................................... 23
8 Ethics approval and consent to participate ................................................................. 23
Annex 1: List of Clusters included in the survey ................................................................ 24
Annex 2: Study team .............................................................................................................. 29
Annex 3: Questionnaire ......................................................................................................... 30
Annex 4: Participant information and informed consent ................................................... 46
Annex 4.1 Participant information and informed consent - Women ............................. 46
Annex 4.2 Participant information and informed consent – Children .......................... 49
Annex 5: Roles of participating institutions and field team members ............................. 52
Annex 6: Fieldwork procedures ............................................................................................ 54
6.1 Overview of daily schedule and activities ............................................................. 54
6.2 Detailed explanation of activities............................................................................ 55
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
1 Introduction
The purpose of the 2016 National Micronutrient Status Survey in Tajikistan was to perform a
national and regional representative survey to obtain valid and reliable data on the
anthropometric status, levels of anaemia, iron status, inflammation, vitamin A deficiency and
iodine intake in non-pregnant women of reproductive age (15-49 years) and in children (aged 6-
59 months). In addition the survey assessed Vitamin D levels of children aged 6-59 months and
folate levels in non-pregnant women of reproductive age.
The 2016 survey was intentionally closely modelled on the Micronutrient Status Survey
conducted by the Ministry of Health and Social Protection and UNICEF in Tajikistan with
support from the Swiss Tropical and Public Health Institute (Swiss TPH) in 2009. The survey
covered the whole of Tajikistan in order to collect representative data at national and regional
level (dividing the country into five regions: Khatlon, Districts of Republican Subordination
(DRS), Sughd, Gorno-Badakhshan Autonomous Oblast (GBAO) and Dushanbe). A total of
2,145 children aged six to 59 months and 2,149 non-pregnant women aged 15-49 were finally
included in the survey analysis, in representative numbers for each of the regions. Data
collection took place in November 2016. Research methods included respondent interviews,
household observations, anthropometric assessments (weight and height measurements) of all
study participants, and the laboratory testing of blood and urine samples to determine anaemia
and micronutrient content. The results of the 2016 survey are presented in a companion
publication to this one.
2 Demographic and geographical context
In 2016, Tajikistan’s population was estimated to be slightly over 8.5 million people. The country
is divided into four oblasts (regions): Sughd in the northwest, Khatlon in the southwest, Districts
of Republican Subordination (DRS) in the centre and west, and Gorno-Badakhshan
Autonomous Oblast (GBAO) in the east (Figure 1). The capital, Dushanbe, in the DRS, is a
separately administrated area and was considered as a separate region for the purpose of this
study. Oblasts are divided into rayons (districts). Rayons are further subdivided into Mahallas
(communities) in urban areas, and Jamoats (villages) in rural areas. Tajikistan's population is
concentrated in the lowlands, and 90 per cent of its inhabitants live in valleys, often in densely
concentrated urban centres.
TABLE 1:
Estimated population size in 2016 by administrative divisions of Tajikistan
(extrapolation from 2010 census)
Estimated population on
1 January 2016 Percentage of national population
Administrative divisions Urban Rural Total Urban Rural Total
Dushanbe 802,700 0 802,700 9.4% 0% 9.4%
DRS 262,316 1,709,984 1,972,300 3.1% 20.0% 23.1%
Sughd 620,217 1,890,783 2,511,000 7.3% 22.1% 29.4%
Khatlon 548,604 2,499,196 3,047,800 6.4% 29.9% 36.3%
GBAO 29,349 188,051 217,400 0.3% 2.2% 2.5%
Tajikistan 2,263,186 6,288,014 8,551,200
Source: State Statistical Committee of the Republic of Tajikistan
4
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
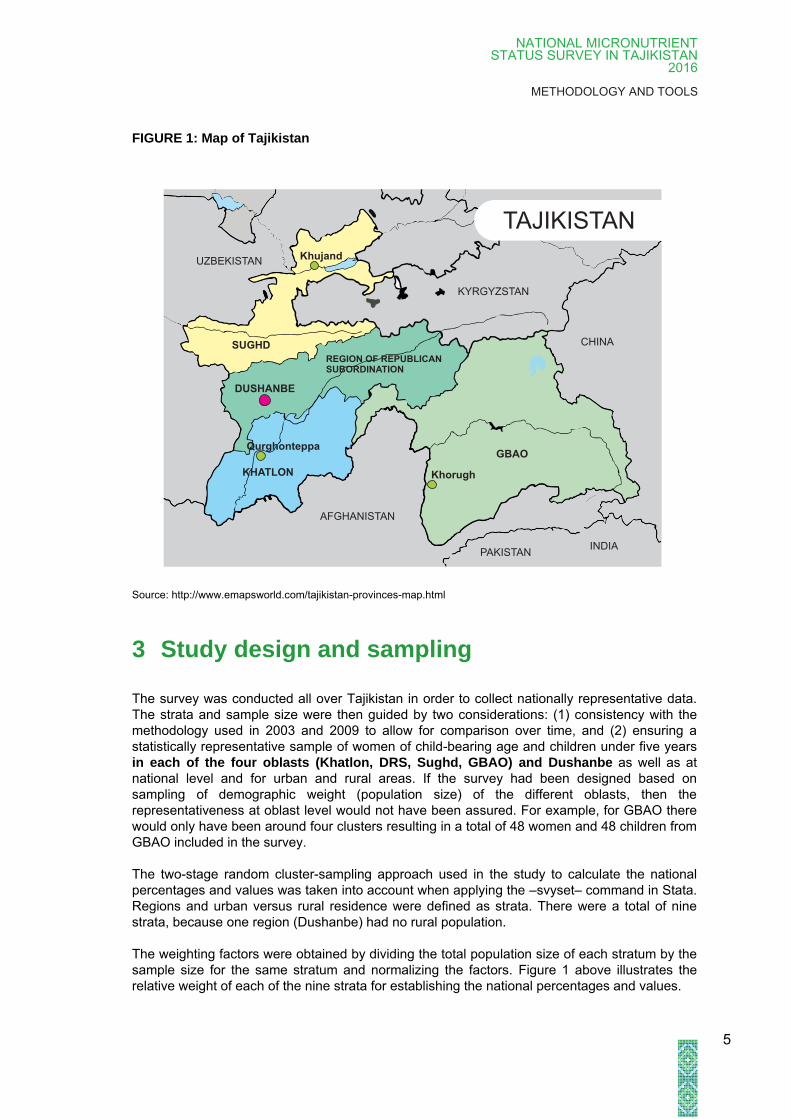
FIGURE 1: Map of Tajikistan
Source: http://www.emapsworld.com/tajikistan-provinces-map.html
3 Study design and sampling
The survey was conducted all over Tajikistan in order to collect nationally representative data.
The strata and sample size were then guided by two considerations: (1) consistency with the
methodology used in 2003 and 2009 to allow for comparison over time, and (2) ensuring a
statistically representative sample of women of child-bearing age and children under five years
in each of the four oblasts (Khatlon, DRS, Sughd, GBAO) and Dushanbe as well as at
national level and for urban and rural areas. If the survey had been designed based on
sampling of demographic weight (population size) of the different oblasts, then the
representativeness at oblast level would not have been assured. For example, for GBAO there
would only have been around four clusters resulting in a total of 48 women and 48 children from
GBAO included in the survey.
The two-stage random cluster-sampling approach used in the study to calculate the national
percentages and values was taken into account when applying the –svyset– command in Stata.
Regions and urban versus rural residence were defined as strata. There were a total of nine
strata, because one region (Dushanbe) had no rural population.
The weighting factors were obtained by dividing the total population size of each stratum by the
sample size for the same stratum and normalizing the factors. Figure 1 above illustrates the
relative weight of each of the nine strata for establishing the national percentages and values.
CHINA
INDIA
KYRGYZSTAN
UZBEKISTAN
AFGHANISTAN
PAKISTAN
TAJIKISTAN
SUGHD
KHATLON
REGION OF REPUBLICANSUBORDINATION
GBAO
Khujand
Qurghonteppa
Khorugh
DUSHANBE
5
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
For example, the results from Dushanbe were weighted to contribute 9.4 per cent of the national
percentage or value. Given the larger population size of Khatlon and Sughd, these regions were
weighted higher and their relative contributions to the national percentages and values were
35.6 per cent and 29.4 per cent respectively. In other words the results from the
demographically large strata/regions contributed more to the national percentage or value.
The survey sampling was based on a national cross-sectional cluster sample design, using
population estimates from the 2010 census extrapolated to 2016. This cluster design was used
because the taking a simple random sample for individuals across Tajikistan is inappropriate.
Therefore a two-stage cluster sampling design was applied (for more detailed information, see
Section 4 Sample size and Section 6.3 Household inclusion and identification):
1. In the first stage, the primary sampling units, i.e. the clusters (usually villages or
mahallas in urban areas), were selected, with a probability proportional to the
population size of the primary sampling unit (region);
2. In the second stage, a random sample was selected in each village (as determined in
the first stage) of a fixed number of individuals (children aged 6-59 months and non-
pregnant women aged 15-49 years).
4 Sample size
The sample size was determined to allow reliable estimation of micronutrient and nutrition
indicators based on a representative probability sample at the level of:
Tajikistan as a whole, stratified along urban and rural areas; and
The five main administrative regions (oblasts) of the country (Dushanbe, DRS, Sughd,
Khatlon and GBAO)
The sampling estimates and the sampling procedures remained consistent with the 2009
Micronutrient Status Survey in Tajikistan, using the following formula:
c = ((( t² x p (1-p)) / m²) x D) / nh + 10% where
c = required number of clusters
t = confidence level at 95% (standard value of 1.96)
p = estimated prevalence of micronutrient deficiencies (50% (maximum)
was used for both 2009 and 2016 surveys)
m = margin of error at 6.5%
D = design effect (1.75 was used for both 2009 and 2016 surveys)
nh = number of households by cluster
6
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
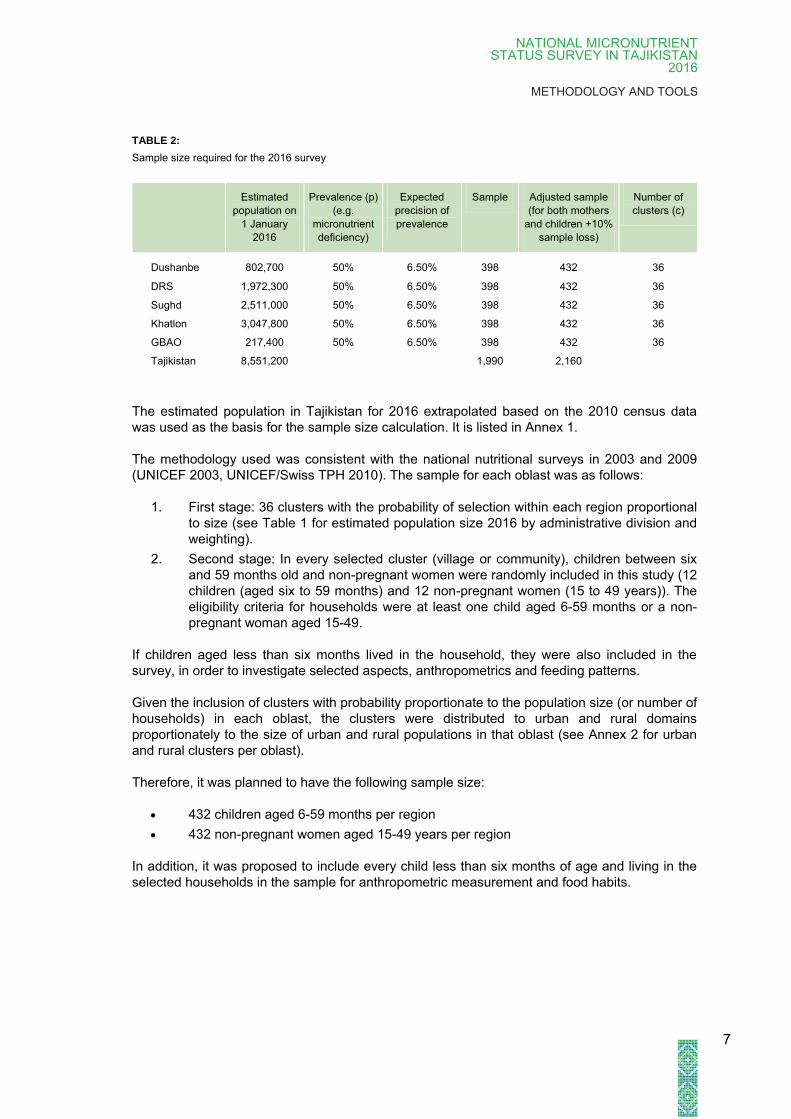
TABLE 2:
Sample size required for the 2016 survey
Estimated
population on
1 January
2016
Prevalence (p)
(e.g.
micronutrient
deficiency)
Expected
precision of
prevalence
Sample Adjusted sample
(for both mothers
and children +10%
sample loss)
Number of
clusters (c)
Dushanbe 802,700 50% 6.50% 398 432 36
DRS 1,972,300 50% 6.50% 398 432 36
Sughd 2,511,000 50% 6.50% 398 432 36
Khatlon 3,047,800 50% 6.50% 398 432 36
GBAO 217,400 50% 6.50% 398 432 36
Tajikistan 8,551,200
1,990 2,160
The estimated population in Tajikistan for 2016 extrapolated based on the 2010 census data
was used as the basis for the sample size calculation. It is listed in Annex 1.
The methodology used was consistent with the national nutritional surveys in 2003 and 2009
(UNICEF 2003, UNICEF/Swiss TPH 2010). The sample for each oblast was as follows:
1. First stage: 36 clusters with the probability of selection within each region proportional
to size (see Table 1 for estimated population size 2016 by administrative division and
weighting).
2. Second stage: In every selected cluster (village or community), children between six
and 59 months old and non-pregnant women were randomly included in this study (12
children (aged six to 59 months) and 12 non-pregnant women (15 to 49 years)). The
eligibility criteria for households were at least one child aged 6-59 months or a non-
pregnant woman aged 15-49.
If children aged less than six months lived in the household, they were also included in the
survey, in order to investigate selected aspects, anthropometrics and feeding patterns.
Given the inclusion of clusters with probability proportionate to the population size (or number of
households) in each oblast, the clusters were distributed to urban and rural domains
proportionately to the size of urban and rural populations in that oblast (see Annex 2 for urban
and rural clusters per oblast).
Therefore, it was planned to have the following sample size:
432 children aged 6-59 months per region
432 non-pregnant women aged 15-49 years per region
In addition, it was proposed to include every child less than six months of age and living in the
selected households in the sample for anthropometric measurement and food habits.
7
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
5 Primary and secondary endpoints
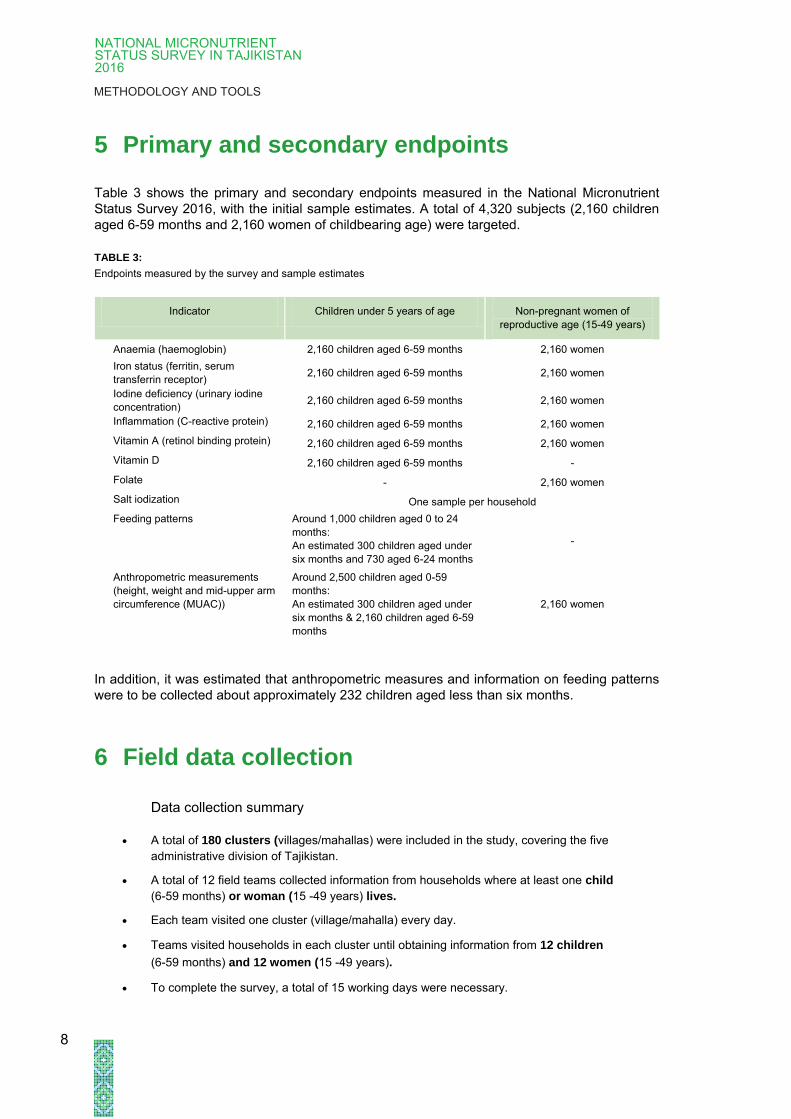
Table 3 shows the primary and secondary endpoints measured in the National Micronutrient
Status Survey 2016, with the initial sample estimates. A total of 4,320 subjects (2,160 children
aged 6-59 months and 2,160 women of childbearing age) were targeted.
TABLE 3:
Endpoints measured by the survey and sample estimates
Indicator Children under 5 years of age Non-pregnant women of
reproductive age (15-49 years)
Anaemia (haemoglobin) 2,160 children aged 6-59 months 2,160 women
Iron status (ferritin, serum
transferrin receptor) 2,160 children aged 6-59 months 2,160 women
Iodine deficiency (urinary iodine
concentration) 2,160 children aged 6-59 months 2,160 women
Inflammation (C-reactive protein) 2,160 children aged 6-59 months 2,160 women
Vitamin A (retinol binding protein) 2,160 children aged 6-59 months 2,160 women
Vitamin D 2,160 children aged 6-59 months -
Folate - 2,160 women
Salt iodization One sample per household
Feeding patterns Around 1,000 children aged 0 to 24
months:
An estimated 300 children aged under
six months and 730 aged 6-24 months
-
Anthropometric measurements
(height, weight and mid-upper arm
circumference (MUAC))
Around 2,500 children aged 0-59
months:
An estimated 300 children aged under
six months & 2,160 children aged 6-59
months
2,160 women
In addition, it was estimated that anthropometric measures and information on feeding patterns
were to be collected about approximately 232 children aged less than six months.
6 Field data collection
Data collection summary
A total of 180 clusters (villages/mahallas) were included in the study, covering the five
administrative division of Tajikistan.
A total of 12 field teams collected information from households where at least one child
(6-59 months) or woman (15 -49 years) lives.
Each team visited one cluster (village/mahalla) every day.
Teams visited households in each cluster until obtaining information from 12 children
(6-59 months) and 12 women (15 -49 years).
To complete the survey, a total of 15 working days were necessary.
8
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
6.1 Field teams and piloting
The field data collection was conducted between 2 and 20 November 2016 by 12 teams of three
collaborators from the Ministry of Health and Social Protection (MoHSP), the Republican
Research Centre on Paediatrics and Child Surgery and the Research Laboratory of Preventive
Medicine of the Republic of Tajikistan (laboratory technicians). In other words, 36 field workers,
including 12 interviewers, 12 clinicians and 12 laboratory technicians were engaged in field data
collection. Each team also included a driver (including the drivers there were 48 persons in the
teams). Therefore every team included a head of team specifically trained on anthropometric
assessments of children and adults, a person with specific training in interview techniques, and
a laboratory technician with experience of capillary blood collection and maintenance of cold
chain procedures.
Prior to the field data collection the MoHSP and UNICEF organized a one-week training course
from 24 to 28 October 2016, for the field teams to standardize the data collection. The Swiss
TPH quality control manager guided this. The first days of training focused on sampling
methodology (how to complete the questionnaire, using Open Data Kit (ODK) software,
interview techniques, anthropometric assessment and blood sample collection procedures). In
order to identify problems with the survey methodology and design, a pilot study was carried out
on days four and five. The team members were instructed on principles of informed consent and
how to obtain it, interview technique, anthropometric measurement of children, basic knowledge
on nutrition, capillary blood collection, coding and labelling of biological samples, safe handling
and transport of samples. The pilot survey also tested the daily workload and allowed for
validation of the survey questionnaire, assessment of the duration of the interviews and testing
of the capillary blood collection and the modalities of its transportation to the central laboratory
in Dushanbe.
6.2 Day-to-day work organization, supervision
and quality control
The First Deputy Minister of the MoHSP was responsible for coordination of the overall survey.
Day-to-day work organization was the responsibility of the head of the Republican Research
Centre for Paediatrics and Child Surgery (Paediatric Research Centre) team, who acted as the
contact point for the field teams and had to ensure that the field teams arrived and conducted
fieldwork every day at the assigned villages (clusters).
Table 4 describes the roles expected from each field team member.
9
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
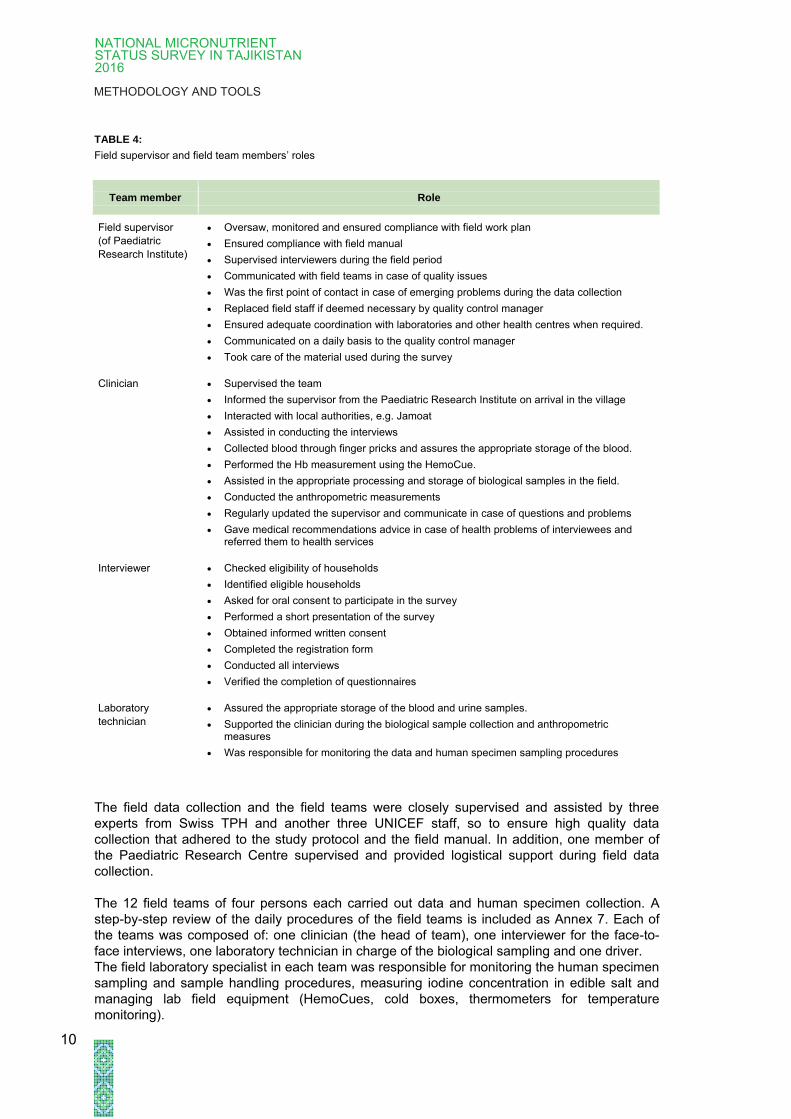
TABLE 4:
Field supervisor and field team members’ roles
Team member Role
Field supervisor
(of Paediatric
Research Institute)
Oversaw, monitored and ensured compliance with field work plan
Ensured compliance with field manual
Supervised interviewers during the field period
Communicated with field teams in case of quality issues
Was the first point of contact in case of emerging problems during the data collection
Replaced field staff if deemed necessary by quality control manager
Ensured adequate coordination with laboratories and other health centres when required.
Communicated on a daily basis to the quality control manager
Took care of the material used during the survey
Clinician Supervised the team
Informed the supervisor from the Paediatric Research Institute on arrival in the village
Interacted with local authorities, e.g. Jamoat
Assisted in conducting the interviews
Collected blood through finger pricks and assures the appropriate storage of the blood.
Performed the Hb measurement using the HemoCue.
Assisted in the appropriate processing and storage of biological samples in the field.
Conducted the anthropometric measurements
Regularly updated the supervisor and communicate in case of questions and problems
Gave medical recommendations advice in case of health problems of interviewees and referred them to health services
Interviewer Checked eligibility of households
Identified eligible households
Asked for oral consent to participate in the survey
Performed a short presentation of the survey
Obtained informed written consent
Completed the registration form
Conducted all interviews
Verified the completion of questionnaires
Laboratory
technician
Assured the appropriate storage of the blood and urine samples.
Supported the clinician during the biological sample collection and anthropometric measures
Was responsible for monitoring the data and human specimen sampling procedures
The field data collection and the field teams were closely supervised and assisted by three
experts from Swiss TPH and another three UNICEF staff, so to ensure high quality data
collection that adhered to the study protocol and the field manual. In addition, one member of
the Paediatric Research Centre supervised and provided logistical support during field data
collection.
The 12 field teams of four persons each carried out data and human specimen collection. A
step-by-step review of the daily procedures of the field teams is included as Annex 7. Each of
the teams was composed of: one clinician (the head of team), one interviewer for the face-to-
face interviews, one laboratory technician in charge of the biological sampling and one driver.
The field laboratory specialist in each team was responsible for monitoring the human specimen
sampling and sample handling procedures, measuring iodine concentration in edible salt and
managing lab field equipment (HemoCues, cold boxes, thermometers for temperature
monitoring).
10
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Within this survey, various measures were taken to ensure high quality field data collection. The
following steps were part of the quality assurance:
During the field data collection, according to the fieldwork plan, all field teams had to
report to the head of the Republican Research Centre for Paediatrics and Child
Surgery team upon arrival at the field destination. The teams were closely assisted
and followed up by supervisors from the Swiss TPH and UNICEF.
The Swiss TPH quality control manager and two dedicated local field supervisors
made unannounced visits throughout the data collection period.
Further quality control measures included quality checks of the collected electronic
data. The quality measures also included field progress monitoring.
The MoHSP and UNICEF Tajikistan both also conducted unannounced visits to the
field and conducted quality assessments.
6.3 Household inclusion and identification
A household was considered eligible for survey inclusion if:
It included at least one non-pregnant woman aged 15-49 years and/or at least one
child aged six to 59 months;
The non-pregnant woman and/or the respective carer of the child/children aged six to
59 months and the child/children were available was/were available for the interview;
and
At least one non-pregnant woman (aged 15-49 years) or carer of a child (aged 6-59
months) signed an informed consent form.
The selection of households was partially aligned to the “Poverty Diagnostic of Water Supply,
Sanitation and Hygiene Sector in Tajikistan (WASH)” survey conducted under the leadership of
the World Bank. As a consequence, and based on the sampling frame (see Section 3), the
selection of households relied on two main mechanisms depending on whether the cluster was
or was not aligned to the WASH survey.
1. When collecting data within a “joint” cluster the field teams were given the household
list prepared by the World Bank for the “Poverty Diagnostic of Water Supply,
Sanitation and Hygiene Sector in Tajikistan (WASH)” survey. The field teams were
then expected to locate the exact households indicated in the list until achieving the
required number of participants per cluster (12 non-pregnant women aged 15-49
years and 12 children aged 6-59 months). If after visiting all 20 households the teams
did not reach the number of participants, then the teams were instructed to select
additional households by a random walk.
2. When collecting data within a cluster that was not in the WASH survey, the teams
were instructed to contact Jamoats for a list of households included in the local
census and then to randomly select 20 households from the Jamoat list. Alternatively,
if the Jamoat list was not available, the teams used household lists from local health
centres.
11
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
INTEGRATION WITH WATER SANITATION AND
HYGIENE SURVEY (THE WORLD BANK):
The World Bank conducted a Water Sanitation and Hygiene Survey (WASH) in Tajikistan covering the same oblasts.
Partially, the Tajik National Micronutrient Status Survey 2016 took place in the same villages (125 villages) as WASH. Consequently TNSS visited and surveyed the same households as the Water Sanitation and Hygiene (WASH).
Analysis of the integrated samples (overwrapping with WASH survey) is underway and the results and methodology will be presented in a separate document.
For those 22 clusters in Dushanbe that were not in the WASH survey, the field teams conducted
a random walk to select households. This was because the 2010 census household information
was outdated and the Jamoat list was not available or was too complex to use.
In most clusters, the teams had support from staff members of the local health centres to
identify the households.
Once a household was identified, the field data collection team checked for the eligibility criteria.
If the eligibility criteria were not fulfilled or consent was not obtained the team identified the next
eligible household. This procedure was repeated until each field study team had identified 12
children and 12 non-pregnant women per village/community.
In cases where very small villages were selected with insufficient numbers of households, other
geographically proximate villages were added to reach the fixed number of subjects per cluster.
6.4 Questionnaire and ODK forms
The survey instrument was developed based on the questionnaire used in 2009. Some
additional and new questions were added and some others were modified. The final version
was reviewed and approved by the MoHSP and UNICEF. The instrument used can be found in
Annex 4 (Questionnaire).
The data collected for the nutritional assessment was in six sections:
1. Household characteristics (type of dwelling, numbers of rooms)
2. Food security of the household
3. Child health issues: morbidity of diarrhoea, nutritional habits
4. Infant feeding related questions: duration of exclusive breastfeeding, complementary
feeding (children aged 6-59 months), infant care and development (only children aged
6-24 months). The questions were then followed by:
Anthropometric measurement in children (6-59 months)
Biologic sampling – anaemia measurement, blood and urine collection for
children’s laboratory examination (6-59 months)
12

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
5. Nutrition habits of non-pregnant women (15-49 years). The questions were then
followed by:
Anthropometric measurement of non-pregnant women (15-49 years)
Biologic sampling – anaemia measurement, blood and urine collection for non-
pregnant women’s laboratory examination (15-49 years)
6. Infant feeding relevant questions (children aged zero to 24 months): duration of
exclusive breastfeeding, complementary feeding, infant care and development. The
questions were then followed by:
Anthropometric measurement of children (less than six months)
The questionnaire was translated into Tajik and then back-translated into English in order to
check misinterpretations.
Questionnaire data was collected with electronic tablets using open data kit (ODK) software.
The questionnaire was organised along four ODK forms.
TABLE 5:
Structure of questionnaire sections in Open Data Kit
ODK Structure Questionnaire sections Respondent/participant
Form 1 - Part I: Household characteristics (type of dwelling,
numbers of rooms)
- Part II: Food security of the household
Carer or non-pregnant women
Form 2 - Part III: Child health issues: morbidity of diarrhoea,
nutritional habits
- Part IV: Infant feeding questions (0-24 months):
duration of exclusive breastfeeding, complementary
feeding, care and development
- Part IV: Anthropometric measurement in children (6-59
months)*
- Part IV: Biologic sampling - children’s laboratory
examination (6-59 months)*
Carer of child(ren) / child(ren) (6-59
months)
Form 3 - Part V: Nutrition habits of non-pregnant, non-lactating
women (15-49 years)
- Part V: Anthropometric measurement among non-
pregnant women (15-49 years) *
- Part V: Biologic sampling - women’s laboratory
examination (15-49 years)*
Non-pregnant women (15-49 years)
Form 4 - Part VI: Infant feeding questions (less than 6 months):
duration of exclusive breastfeeding, complementary
feeding, care and development
- Part VI: Anthropometric measurement in children (less
than 6 months)*
Carer of child(ren) < 6 months
* only documentation; no answers required from respondents
6.5 Anthropometric measurements of children (0-59 months)
and women (15-49 years)
After completing the interview, the paediatrician/clinician took anthropometric measurements.
For the measurements, UNICEF-standardized electronic scales and height boards were used
for both children and mothers. The scales were calibrated regularly using a standard weight and
then checked regularly by supervisors from the Swiss TPH and UNICEF. For infants (aged zero
13

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
to 24 months), the length was measured supine. Children aged two to five years and women
were measured in an upright position. See Annex 7.2 for the anthropometric measurement
methodology.
6.6 Biological sampling
The laboratory technician collected blood and urine samples assisted by the clinicians.
From each child aged 6-59 months and each non-pregnant women of reproductive age (15-49
years), 400 µl of capillary blood were collected using serum separating gel tubes (Microvette®,
Sarstedt). The blood was stored in a cooling box until centrifugation at the nearest district or
oblast hospital. Centrifugation was conducted within a day of onset of collection. Then the
serum was transferred in light protected tubes (Microtainer™, Sarstedt). Immediately after
centrifugation, the samples were placed in a minus 20°C freezer and transported within 24-72
hours in frozen condition to a central storage facility in Dushanbe overseen by the Research
Laboratory of Preventive Medicine of the Republic of Tajikistan, where they were stored at
minus 20°C until analysis. Haemoglobin was measured on the spot using a HemoCue device
(HemoCue AB, Ängelholm, Sweden).
To measure iodine concentration, 5 ml urine samples were collected, using plastic containers,
which were distributed to the women or the carers. Urine sampling from children (6-59 months)
was done whenever possible from the traditional cradle (gavora: the urine is traditionally
collected in a pot under the cradle). The urine samples were transferred to a labelled storage
tube and also placed in a minus 20°C freezer and transported in frozen condition within 24-72
hours to a central storage facility at the Dushanbe Laboratory of Preventive Medicine. In some
instances there was not sufficient space in the freezers so the urine samples were stored in
refrigerators and transported in cooling boxes within 48-72 hours to Dushanbe, where they were
frozen at minus 20°C until analysis.
The clinician in each field team provided clinical feedback regarding the iron status
(haemoglobin value) of tested individuals, and provided advice if it was necessary to seek
further medical advice. Anaemic women and children were referred to a nearby health services.
No other treatment was given, and nor was money or transport to hospital.
6.7 Salt iodization
Fortified salt that contains 15 parts of iodine per million of salt (15ppm) is considered adequate
for the prevention of iodine deficiency (WHO 2014). The iodine content of the salt used in the
households was evaluated by testing for potassium iodate or potassium iodide content using the
MBI rapid test kit for salt fortified with potassium iodate (UNICEF supply catalogue product
number S0008193). A drop of the indicator solution was applied to one spoonful of salt,
flattened on a dish. The colour that immediately developed from the reaction was interpreted
against the coloured scale on the back of the test solution’s packaging. The result was then
registered as coloured (iodine present) or not coloured (no iodine present).
14

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
7 Data management and analysis
7.1 Data entry and analysis
The questionnaire data were collected using electronic tablets and open data kit (ODK)
software. Hence, additional data entry was not necessary.
Data from the biochemical analysis were recorded at the Dushanbe Laboratory of Preventive
Medicine using Excel.
All statistical analysis was conducted using Stata (version 14 Stata Intercooled, Stata Corp.,
College Station, Texas). Data were checked for outliers and normal distribution (using visual
examination of histograms and normality tests), and data not following normal distribution was
log transformed (serum ferritin, transferrin receptor, C-reactive protein, vitamin D and A, retinol
binding protein and urinary iodine concentration).
To calculate the national percentages and values the cluster-sampling approach used in this
study was taken into account by applying the –svyset– command in Stata and defining the 180
primary sampling units (usually villages or mahallas). Regions and urban or rural residence
were defined as strata. There were a total of nine strata, because one region (Dushanbe) had
no rural population. Weighting factors were obtained by dividing the total population size of each
stratum by the sample size for the same stratum and normalizing the factors.
New variables were calculated for the following: z-scores for the definition of stunting, wasting,
and underweight as well as body mass index (BMI) in women (see Section 6.5 for further
details). In addition, categorical variables for anaemia, iron deficiency, iron deficiency anaemia,
body iron stores, vitamin A and D deficiency as well as folate deficiency were defined.
Furthermore adjustments were made for the haemoglobin values of study participants living at
high altitudes, and for serum ferritin and retinol binding protein values for study participants with
inflammation.
Data analysis was conducted following standard epidemiological approaches. Firstly the data
was summarized (e.g. means and percentages) and the associations between outcomes and
explanatory variables were explored while considering confounders. Pearson’s chi-square tests
were conducted for associations of categorical variables and independent t-tests for
relationships of means (continuous variables) between groups. Analysis of variance (ANOVA)
was used to compare several means across groups, and the post-hoc Scheffe's test used to
evaluate which pairs of means were significant. Bartlett's test was used to verify the assumption
of equal variances across groups. P values less than 0.05 were considered as statistically
significant.
7.2 Anthropometric analysis
Anthropometric measurement procedures were standardized following guidelines published by
the United Nations (UN 1989) and WHO (1995). Values were calculated using WHO Anthro
software (version 3.2.2) and analysed in Stata.
For children, four anthropometric indicators were used to monitor nutritional status:
prevalence of underweight, using weight-for-age z-score (WAZ)
WAZ <-2SD and ≥ -3SD for moderate underweight
WAZ <-3SD for severe underweight
15
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
prevalence of stunting, using height-for-age z-score (HAZ)
HAZ <-2SD and ≥ -3SD for moderate stunting
HAZ <-3SD for severe stunting
prevalence of wasting, using weight-for-height z-score (WHZ)
WHZ<-2SD and ≥ -3SD for moderate wasting
WHZ<-3SD for severe wasting
mid-upper arm circumference (for children aged 6-59 months only)
Cut-off was defined as a MUAC<115mm
(based on WHO Standards: www.who.int/childgrowth/standards)
For women, BMI was calculated (BMI = weight(kg)/[height(m)]2) and used to define chronic
energy deficiency (<18.5), normal BMI (18.5 to >25), overweight (25 to >30) and obesity (≥30).
Data collection took place in November 2016, often at temperatures around or below zero.
Consequently study participants were weighed wearing clothes. In this context, in some
instances some field teams corrected the measured weights by between 100g and 200g for
children and by 300-500g for women depending on the weight of the participants’ clothes, as
estimated by the field teams. Since these corrections were not conducted uniformly and
consistently, and the procedures were stopped once uncovered in monitoring, weight data were
not corrected during the analysis.
Data were checked for plausibility to uncover typing errors and mix-ups of variables, as well as
extreme outliers. Obvious recording mistakes were corrected (wrong decimal points, weight and
height exchanged). During the analysis we verified for the influence of extreme outliers and
extreme z-scores for each indicator using the Emergency Nutrition Assessment software of
Standardized Monitoring and Assessment of Relief and Transitions (for further information
please consult:
http://smartmethodology.org/survey-planning-tools/smart-emergency-nutrition-assessment/).
Along international recommendations of WHO
(http://www.who.int/childgrowth/software/WHOAnthro2005_PC_Manual.pdf,
last accessed April 26, 2017), the following cut-offs were used:
Weight-for-age WAZ (underweight): z-score < - 6SD or z-score > 5SD
Height-for-age HAZ (stunting): z-score < - 6SD or z-score > 6SD
Weight-for-height WHZ (wasting): < - 5SD or z-score > 5SD
Overall, 18 of these extreme outliers were detected. Subsequently we calculated prevalence
with extreme values and without extreme values. The results without extreme values were used
as the official final data, though both sets of results are included in the annex of result book.
In addition, the following value was considered as an extreme outlier for women: BMI above
60kg/m2. Overall, only three of these extreme outliers were detected and taken out.
Though the field teams were well trained on MUAC measurement, the precision and accuracy
of their measurement skills was not standardized before the survey.
The limits of using mid-upper arm circumference (MUAC) strips under field conditions are well
known, and repeated analyses from standardization exercises for nutrition surveys indicate that
the MUAC strip measures may result in substantial variations. This is often explained, among
other factors, as being due to the lack of a standard tension applied to the strip at the time of
measurement. During the data analysis, MUAC data quality was checked, and it was concluded
that the accuracy and precision of MUAC measures for this survey was relatively low, and
consequently, it has been decided that data be omitted from the analysis.
16

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
7.3 Minimum Dietary Diversity for Women
To calculate dietary consumption within the past 24 hours, the approach and methodology
described in “Minimum Dietary Diversity for Women - A Guide to Measurement” (FAO 2016)
was used.
The ten food groups included and analysed were: (1) Grains, white roots and tubers, and
plantains, (2) Pulses (beans, peas and lentils), (3) Nuts and seeds; (4) Dairy, (5) Meat, poultry
and fish, (6) Eggs, (7) Dark green leafy vegetables, (8) Other vitamin A-rich fruits and
vegetables, (9) Other vegetables, and (10) Other fruits.
Following the guidance of FAO (2016), the analysis was interested in women who had
consumed a higher proportion of food items from at least five of the ten food groups within the
last day. The analysis also covered the average (mean) diversity score and urban-rural
differences. Thus the 10 minimum dietary diversity groups were first summed into a score
ranging from 0 to 10. Each woman was coded “yes” or “no” for scoring ≥ 5, followed by a
calculation of the proportion of women who scored from 5 to 10.
7.4 Haemoglobin
Haemoglobin is the iron-containing oxygen-binding protein of the red blood cells (Riggs 1965). It
is the best determinant for assessing the prevalence of anaemia. However, to define iron status,
sensitivity of haemoglobin is poor, as the impact of iron deficiency on haemoglobin levels is
marginal and large losses of body iron are needed to develop anaemia. In addition, specificity is
low in countries with high prevalence of poverty, malnutrition and infections that contribute to
anaemia of chronic disease, also called anaemia of inflammation (Cook et al. 2003, Cook
2005).
In the 2016 Micronutrient Status survey, haemoglobin measurements among children aged 6-59
months and women relied on the HemoCue™ field haemoglobin analyser. The cut-off points
used to determine anaemia prevalence followed the recommendations by WHO shown intable 6
TABLE 6:
Haemoglobin thresholds used (WHO 2011)
Haemoglobin threshold (g/dl)
Children (0.5-4.9 years) 11.0
Non-pregnant women (≥15 years old) 12.0
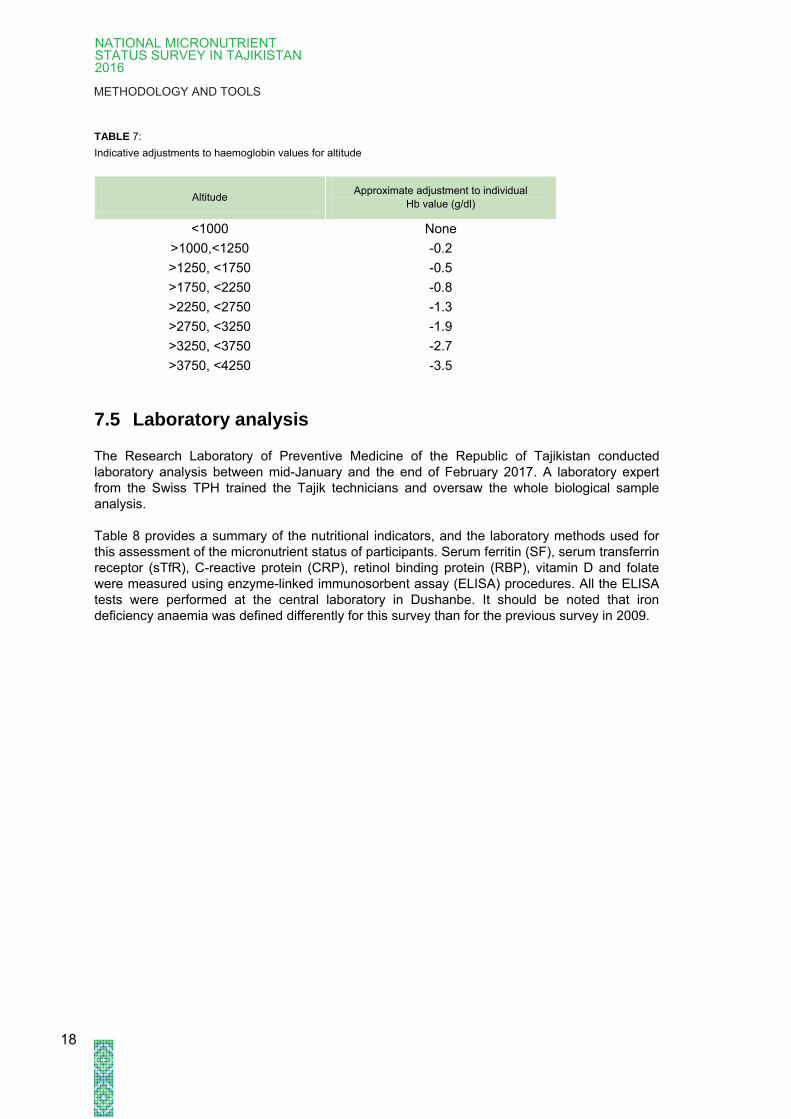
At elevations above 1,000m, haemoglobin concentrations increase as an adaptive response to
the lower partial pressure of oxygen and reduced oxygen saturation of blood. The
compensatory increase in red blood cell production ensures that sufficient oxygen is supplied to
tissues. Haemoglobin values measured in the field were recorded uncorrected. Altitudes were
obtained using the GPS coordinates of the clusters and in complement crosschecking by using
Google Earth (http://www.advancedconverter.com/map-tools/find-altitude-by-coordinates). In
order to correctly estimate the prevalence of anaemia and the values of haemoglobin in clusters
situated above 1,000m, the haemoglobin values were adjusted using the formula set down by
Sullivan et al. (approximate adjustments can be found in Table 7): adjusted Hb(g/dl)=Hb-(-
0.032*(altitude*0.0032808)+0.022*(altitude*0.0032808)2) (Sullivan et al. 2008).
17
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
TABLE 7:
Indicative adjustments to haemoglobin values for altitude
Altitude Approximate adjustment to individual
Hb value (g/dl)
<1000 None
>1000,<1250 -0.2
>1250, <1750 -0.5
>1750, <2250 -0.8
>2250, <2750 -1.3
>2750, <3250 -1.9
>3250, <3750 -2.7
>3750, <4250 -3.5
7.5 Laboratory analysis
The Research Laboratory of Preventive Medicine of the Republic of Tajikistan conducted
laboratory analysis between mid-January and the end of February 2017. A laboratory expert
from the Swiss TPH trained the Tajik technicians and oversaw the whole biological sample
analysis.
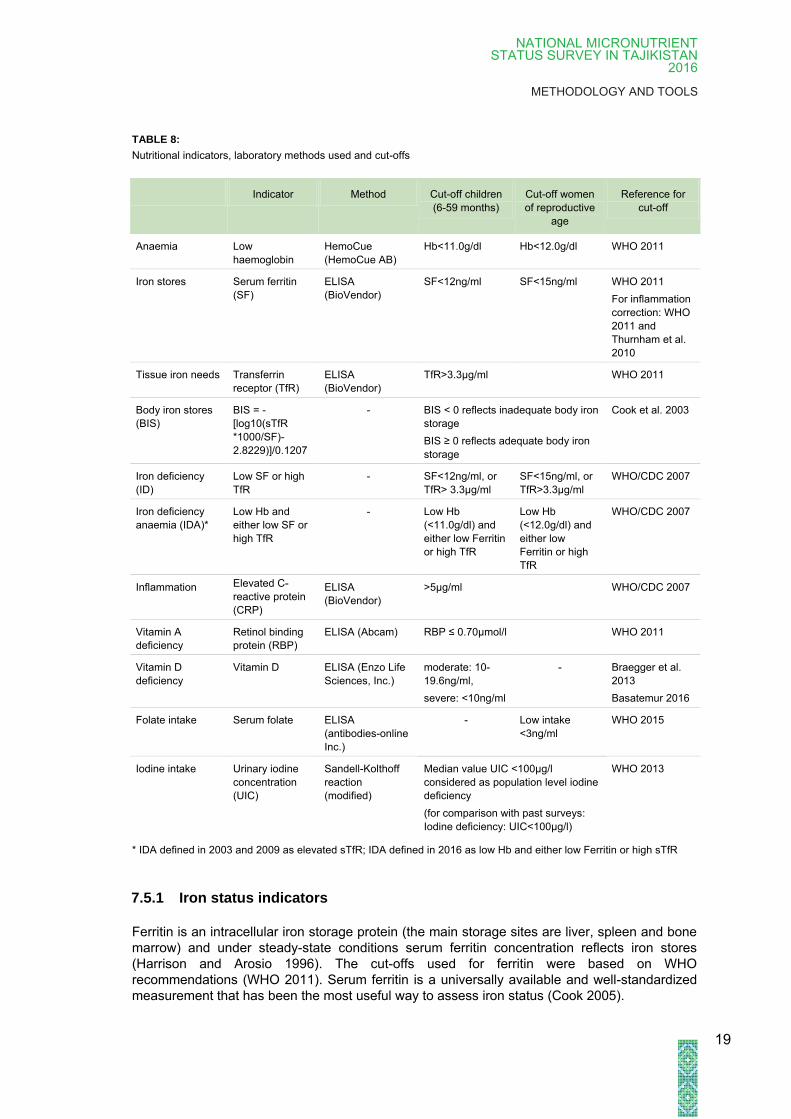
Table 8 provides a summary of the nutritional indicators, and the laboratory methods used for
this assessment of the micronutrient status of participants. Serum ferritin (SF), serum transferrin
receptor (sTfR), C-reactive protein (CRP), retinol binding protein (RBP), vitamin D and folate
were measured using enzyme-linked immunosorbent assay (ELISA) procedures. All the ELISA
tests were performed at the central laboratory in Dushanbe. It should be noted that iron
deficiency anaemia was defined differently for this survey than for the previous survey in 2009.
18
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
TABLE 8:
Nutritional indicators, laboratory methods used and cut-offs
Indicator Method Cut-off children
(6-59 months)
Cut-off women
of reproductive
age
Reference for
cut-off
Anaemia Low
haemoglobin
HemoCue
(HemoCue AB)
Hb<11.0g/dl Hb<12.0g/dl WHO 2011
Iron stores Serum ferritin
(SF)
ELISA
(BioVendor)
SF<12ng/ml SF<15ng/ml WHO 2011
For inflammation
correction: WHO
2011 and
Thurnham et al.
2010
Tissue iron needs Transferrin
receptor (TfR)
ELISA
(BioVendor)
TfR>3.3μg/ml WHO 2011
Body iron stores
(BIS)
BIS = -
[log10(sTfR
*1000/SF)-
2.8229)]/0.1207
- BIS < 0 reflects inadequate body iron
storage
BIS ≥ 0 reflects adequate body iron
storage
Cook et al. 2003
Iron deficiency
(ID)
Low SF or high
TfR
- SF<12ng/ml, or
TfR> 3.3μg/ml
SF<15ng/ml, or
TfR>3.3μg/ml
WHO/CDC 2007
Iron deficiency
anaemia (IDA)*
Low Hb and
either low SF or
high TfR
- Low Hb
(<11.0g/dl) and
either low Ferritin
or high TfR
Low Hb
(<12.0g/dl) and
either low
Ferritin or high
TfR
WHO/CDC 2007
Inflammation Elevated C-
reactive protein
(CRP)
ELISA
(BioVendor)
>5μg/ml WHO/CDC 2007
Vitamin A
deficiency
Retinol binding
protein (RBP)
ELISA (Abcam) RBP ≤ 0.70µmol/l WHO 2011
Vitamin D
deficiency
Vitamin D ELISA (Enzo Life
Sciences, Inc.)
moderate: 10-
19.6ng/ml,
severe: <10ng/ml
- Braegger et al.
2013
Basatemur 2016
Folate intake Serum folate ELISA
(antibodies-online
Inc.)
-
Low intake
<3ng/ml
WHO 2015
Iodine intake Urinary iodine
concentration
(UIC)
Sandell-Kolthoff
reaction
(modified)
Median value UIC <100μg/l
considered as population level iodine
deficiency
(for comparison with past surveys:
Iodine deficiency: UIC<100μg/l)
WHO 2013
* IDA defined in 2003 and 2009 as elevated sTfR; IDA defined in 2016 as low Hb and either low Ferritin or high sTfR
7.5.1 Iron status indicators
Ferritin is an intracellular iron storage protein (the main storage sites are liver, spleen and bone
marrow) and under steady-state conditions serum ferritin concentration reflects iron stores
(Harrison and Arosio 1996). The cut-offs used for ferritin were based on WHO
recommendations (WHO 2011). Serum ferritin is a universally available and well-standardized
measurement that has been the most useful way to assess iron status (Cook 2005).
19
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Serum ferritin is an acute phase protein and its concentration is increased during inflammation.
Thurnham et al. proposed correcting serum ferritin values during subclinical inflammation using
a correction factor of 0.77 during incubation (elevated CRP), 0.53 during early convalescence
(elevated CRP and AGP), and 0.75 during late convalescence (elevated AGP) (Thurnham et al.
2010). In this survey only CRP was measured and therefore a correction factor of 0.77 was
used in cases of elevated CRP.
The Ferritin ELISA (BioVendor, RCD012R) used in this survey is a one-step capture or
“sandwich” assay. The assay makes use of two highly specific monoclonal antibodies: A
monoclonal antibody specific for Ferritin is immobilized onto the microwell plate and another
monoclonal antibody specific for a different region of Ferritin is conjugated to horse radish
peroxidase (HRP). Ferritin from the sample and standards are allowed to bind simultaneously to
the plate and to the HRP conjugate. The washing and decanting steps remove any unbound
HRP conjugate. After the washing step, the enzyme substrate is added. The enzymatic reaction
is terminated by addition of the stopping solution. The absorbance is measured on a microtiter
plate reader at 450 nm. The intensity of the colour formed by the enzymatic reaction is directly
proportional to the concentration of Ferritin in the sample. A set of standards is used to plot a
standard curve from which the amount of Ferritin in patient samples and controls can be directly
read.
Transferrin receptor (TfR) is the cellular entry point for plasma iron, and reflects overall tissue
iron need, but especially in erythrocyte precursors in the bone marrow. The circulating soluble
transferrin receptor (sTfR) is a cleaved form of the entire molecule and reflects total body TfR
(Skikne 2008). The two main determinants of sTfR are erythropoietic activity and tissue iron
deficiency, which increase sTfR (Skikne et al. 1990, Beguin 2003). In iron-replete subjects sTfR
is a marker of erythropoiesis and becomes an iron status indicator in subjects with tissue iron
deficiency, with or without adequate iron stores (Beguin 2003). The lack of international
standardization of the sTfR immunoassays, which all use different standards and reference
ranges, is the main limitation when using sTfR as an iron status indicator (Speeckaert et al.
2010).
The human sTfR ELISA (BioVendor, RD194011100) used in this survey uses microplate wells
pre-coated with monoclonal anti-human sTfR antibody in which standards, quality controls and
samples are incubated. After incubation and washing, monoclonal anti-human sTfR antibody,
conjugated with HRP is added to the wells and further incubated with captured sTfR. Following
another washing step, the remaining HRP conjugate is allowed to react with the substrate
solution (TMB). The reaction is stopped by the addition of acidic solution, and absorbance of the
resulting yellow product is measured at 450 nm. The absorbance is proportional to the
concentration of sTfR. A standard curve is constructed by plotting absorbance values against
concentrations of standards, and concentrations of samples are determined using this standard
curve.
A more recently suggested indicator for iron status is the estimation of body iron based on the
ratio of TfR to SF (Cook et al. 2003). The concentration of SF is directly proportional to body
iron stores in healthy adults and can be estimated as 1 μg/l SF=8-10mg body iron stores.
However, in infants and children body size should be taken into consideration using the formula
1 μg/l SF=120μg storage iron/kg body weight (Finch et al. 1986). Cook et al. established an
estimation of body iron through a series of repeated phlebotomies in healthy adult subjects
(Skikne et al. 1990). The amount of storage iron at baseline was calculated from the amount of
haemoglobin iron removed to reduce SF co microplate wells pre-coated with monoclonal anti-
human sTfR antibody concentration to less than 12ìg/l (Cook et al., 2003). The amount iron
removed at each bleeding was corrected for the absorption of dietary iron and body iron (mg/kg
body weight) and was calculated from the ratio of TfR to SF according to the following equation:
body iron (mg/kg)=-[log10(TfR*1000/SF)-2.8229)]/0.1207. Positive body iron values depict
storage iron, whereas negative values indicate tissue iron deficiency.
20

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
7.5.2 Inflammation
C-reactive protein (CRP) is an acute-phase protein produced exclusively in the liver. CRP is
present in the serum of normal persons at concentrations ranging up to 5-8 µg/ml. Serum
concentration of CRP increases significantly in cases of both infectious and non-infectious
inflammation, tissue damage and necrosis, and in the presence of malignant tumours.
Furthermore, CRP is present in the active stages of inflammatory disorders. The CRP level
increases dramatically following microbial infections. Because the biological half-life of this
protein is only 24 hours, CRP accurately parallels the activity of the inflammation process
(Gewurz et al. 1982).
The literature refers to different cut-off values for CRP when using ELISA testing. A serum CRP
threshold of 3 to 10 μg/ml is recommended when using an immunoassay such as ELISA
(WHO/CDC 2007). In consultation with UNICEF and CDC this survey used a cut-off of 5 μg/ml.
The human CRP ELISA (BioVendor, RAP001) used in this survey consists of microplates
coated with anti-CRP antibodies, which were incubated with diluted standard and study serum
samples. After incubation CRP is bound to the wells and unbound serum proteins are removed.
The antigen-antibody complex in each well is detected with specific peroxidase-conjugated
antibodies, showing a blue colour when in contact with tetramethylbenzidine (TMB) and
hydrogen peroxide. The enzymatic reaction is stopped and the absorbance values are
determined at 450nm. A standard curve was obtained by plotting the absorbance values versus
corresponding standard values and the specific concentration of CRP in the serum samples
were determined by interpolation from the standard curve.
7.5.3 Retinol binding protein
Retinol is the predominant circulating form of vitamin A in the blood. In response to tissue
demand, it is released from the liver at a 1:1 ratio with its carrier protein, retinol-binding protein
(RBP). According to WHO guidelines (WHO, 2011), a prevalence of low serum retinol (<0.70
µmol/l) and therefore vitamin A deficiency (VAD) of 2-9 per cent in a population corresponds to
a mild public health problem, 10-19 per cent to a moderate, and 20 per cent or more to a severe
public health problem (WHO 2011). In children and women, the cut-off for severe vitamin A
deficiency is suggested to be ≤0.48 µmol/l (Gamble 2001) and moderate VAD 0.70 µmol/l
(Gamble et al. 2001, West 2003).
Retinol binding protein is reduced during inflammation, and adjustments were made using
correction factors for retinol binding protein values of 1.14 in the case of elevated CRP
(Thurnham et al. 2003).
The human RBP4 ELISA (Abcam, ab196264) used in this survey employs an affinity tag
labelled capture antibody and a reporter conjugated detector antibody which immunocapture the
sample analyte in solution. This entire complex (capture antibody/analyte/detector antibody) is
immobilized via immunoaffinity of an anti-tag antibody coating the well. To perform the assay,
samples or standards are added to the wells, followed by the antibody mix. After incubation, the
wells are washed to remove unbound material. TMB substrate is added and during incubation is
catalysed by HRP, generating blue coloration. This reaction is then stopped by addition of a
stop solution completing any colour change from blue to yellow. Signal is generated
proportionally to the amount of bound analyte and the intensity is measured at 450nm. A
standard curve was obtained by plotting the absorbance values against corresponding standard
values, and the specific concentrations of RBP in the serum samples were determined by
interpolation from the standard curve. The RBP concentrations retrieved from the ELISA kits
were converted from µg/ml to µmol/l (1µg/ml=0.048µmol/l) (Gamble et al. 2001).
21
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
7.5.4 Vitamin D
Vitamin D regulates calci un exposure to form parent vitamin D3. Alternatively, vitamin D can be
ingested as um and phosphate metabolism and is essential for the maintenance of bone health
(Grossman et al. 2017). Vitamin D requirements can be met by adequate s parent vitamin D2
from food. These parent compounds are transported to the liver and undergo hydroxylation to
25(OH) vitamin D. This metabolite is then transported to the kidney where it undergoes a
second hydroxylation to 1,25(OH)2 vitamin D, the biologically active form of vitamin D. The
levels of vitamin D metabolites increase proportionately with increased uptake of parent vitamin
D. This combined with the greater half-life and stability of 25(OH) vitamin D in circulation versus
the active form are the reasons why detection of the 25(OH) vitamin D metabolite is used as the
best indicator for total vitamin D concentration (Weydert 2014). However, considerable
variability exists among the various assays available, and among laboratories that conduct the
analysis (Mimouni 2010).
Widely accepted cut-offs for the definition of vitamin D deficiency are a serum 25(OH) vitamin D
value of <25nmol/l (<10ng/ml) (Basatemur 2016) for severe and 25-49nmol/l (10-19.6ng/ml) to
indicate moderate vitamin D insufficiency (Braegger et al. 2013).
The 25(OH) vitamin D ELISA Kit (Enzo Life Sciences, Inc., ADI-900-215) used in this survey
employs the competitive inhibition enzyme immunoassay technique. The microplate has been
pre-coated with donkey anti-sheep IgG antibody. Standards and samples are added to the plate
wells and dissociation of 25(OH) vitamin D from vitamin D binding protein allowed to occur. A
solution of alkaline phosphatase-conjugated 25(OH) vitamin D3 is then added, followed by a
solution of sheep monoclonal antibody to 25(OH) vitamin D. During incubation at room
temperature the antibody binds the 25(OH) vitamin D from the sample, standard or conjugate in
a competitive manner and is itself captured by the anti-sheep IgG antibody. After washing,
leaving a complex with bound 25(OH) vitamin D from samples or the alkaline phosphatase
conjugate. A p-nitrophenyl phosphate substrate solution is added initiating an alkaline
phosphatase catalysed reaction that generates a yellow colour in the solution. Stop solution is
added to stop the substrate reaction and the resulting yellow colour is read at 405 nm using a
microplate reader. The amount of signal is inversely proportional to the level of 25(OH) vitamin
D in the sample. A standard curve was obtained by plotting the absorbance values versus
corresponding standard values and the specific concentrations of RBP in the serum samples
were determined by interpolation from the standard curve.
7.5.5 Folate
Folate is important for the prevention of birth defects and other diseases of women of
reproductive age (Obeid et al. 2016). Serum folate is considered an indicator of recent folate
intake, while red blood cell folate concentrations are useful to indicate long-term folate status.
Values indicative of folate deficiency are <3ng/ml (<6.8nmol/l) in serum (WHO 2015).
The human Folic Acid ELISA (antibodies-online Inc., ABIN857086) used in this survey employs
the competitive inhibition enzyme immunoassay technique. The microtiter plate has been pre-
coated with an antibody specific to folic acid (FA). Standards and samples are added to the
appropriate microtiter plate wells with HRP conjugated FA. The competitive inhibition reaction is
launched with HRP-conjugated FA and FA in samples. A substrate solution is added to the
wells and the colour develops inversely to the amount of FA in the sample. The colour
development is stopped and the intensity of the colour is measured at 450 nm using a
microplate reader. A standard curve was obtained by plotting the absorbance values versus
corresponding standard values and the specific concentration of RBP in the serum samples
were determined by interpolation from the standard curve.
22
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
7.5.6 Urinary iodine concentration
An estimated 35 per cent of the world’s population has insufficient iodine intake and continues
to live at risk of iodine deficiency and associated iodine deficiency disorders. Urinary iodine is a
well-accepted, cost-efficient and easily obtainable indicator for iodine status. Since the majority
of the iodine absorbed by the body is excreted in urine (Nath et al. 1992), it is considered a
sensitive marker of current iodine intake and can reflect recent changes in iodine status
(WHO/ICCIDD/UNICEF 2007). A median urinary iodine level of 100 μg/l or less is proposed for
classifying iodine deficiency in the population (Zimmermann 2008). Day-to-day variations for
individual urinary iodine levels have to be kept in mind (Andersen et al. 2008). Thus, the present
survey was primarily interested in the median urinary level.
The method applied in the Tajikistan National Micronutrient Status Survey 2016 was adapted
from the “ammonium persulfate digestion with the use of a microtiter plate to carry out a
Sandell-Kolthoff reaction (Sandell and Kolthoff 1937) and the use of microplate reader for
reading optical density”. Urine samples were digested with ammonium persulfate on a heating
block. Then, after the addition of arsenious acid solution, ceric ammonium sulphate solution was
added and the absorbance of yellow complex was read in a spectrophotometer at 405 nm. The
concentration was calculated by extrapolating from a standard curve. All the glass and plastic
ware used were acid-washed prior to use.
8 Ethics approval and consent to participate
All interviewees gave written The study underwent ethical review by the “Ethikkommission
Nordwest- und Zentralschweiz (Ethical Committee of Northwest and Central Switzerland)” and
was granted approval under Swiss law in October 2016 (ref EKNZ BASEL UBE-req 2016-
00543).
In addition, on 24 October 2016 the Ministry of Health and Social Protection of the Republic of
Tajikistan granted written approval for conducting the National Micronutrient Status Survey and
collecting field data.
Participants were given a participant information and informed consent form. It was pointed out
that participation is voluntary and that individuals may withdraw from the survey at any time.
informed consent before the interview. Informed consent was obtained in writing from all study
participants and/or the parents/legal guardians of children between 0-59 months. (Informed
consent form (ICF), Annex 5). The age of legal majority in Tajikistan is 18 years. For minor
women participating in the survey (15-17 years) consent was secured both from herself and a
parent/legal guardian.
Participation was uncompensated.
23
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
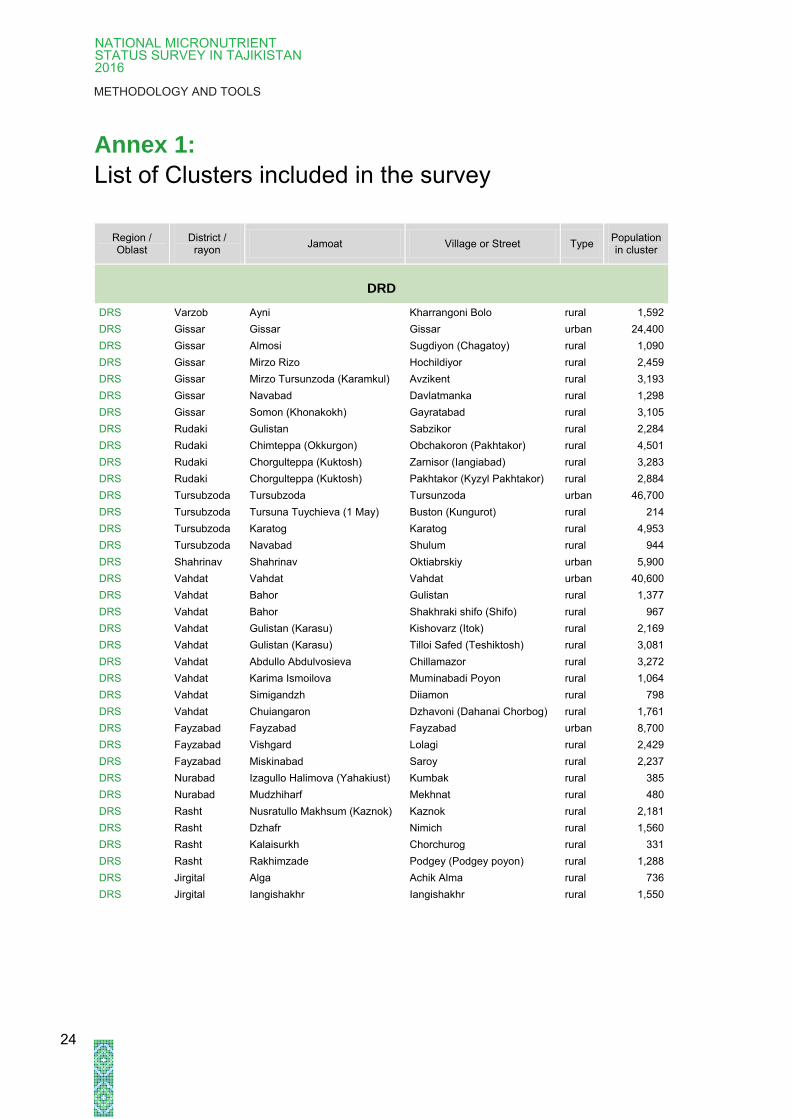
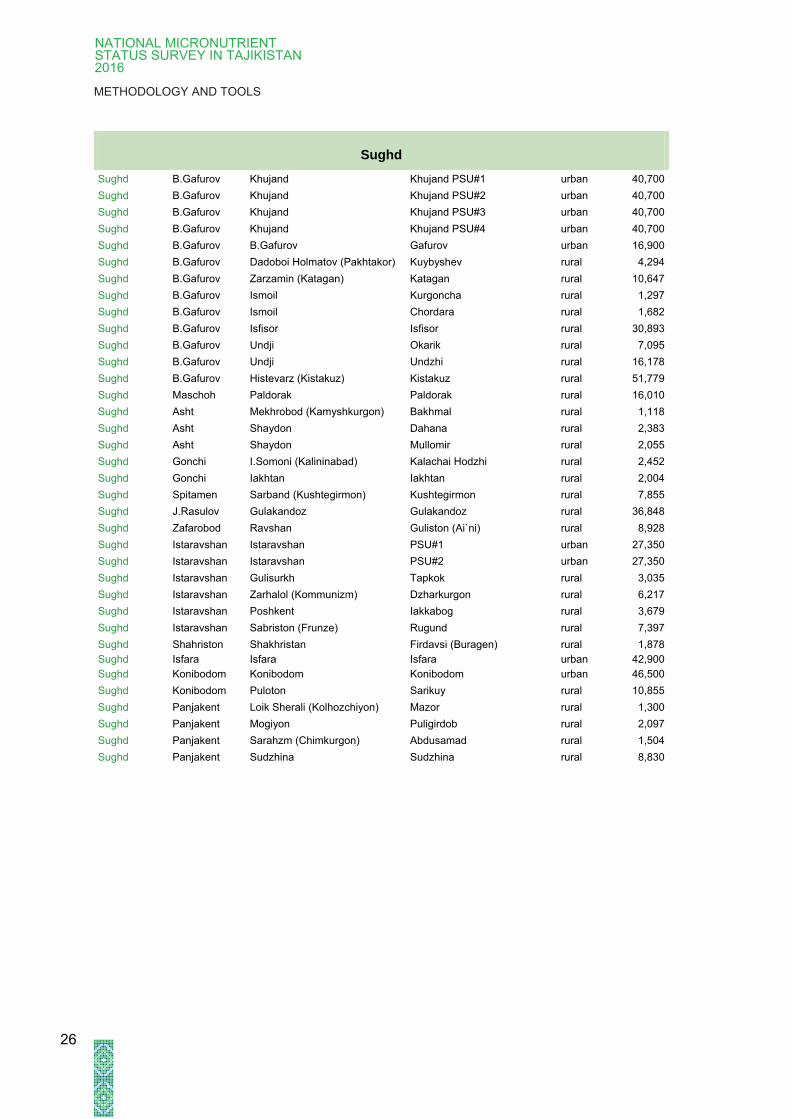
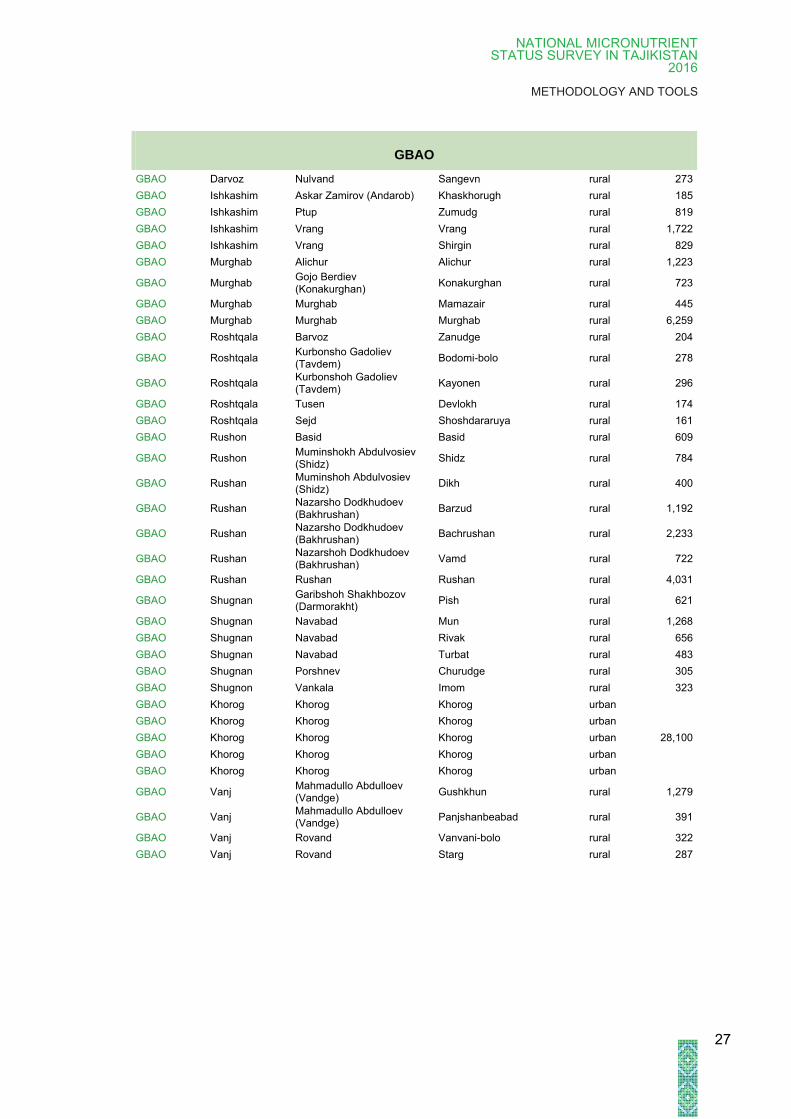
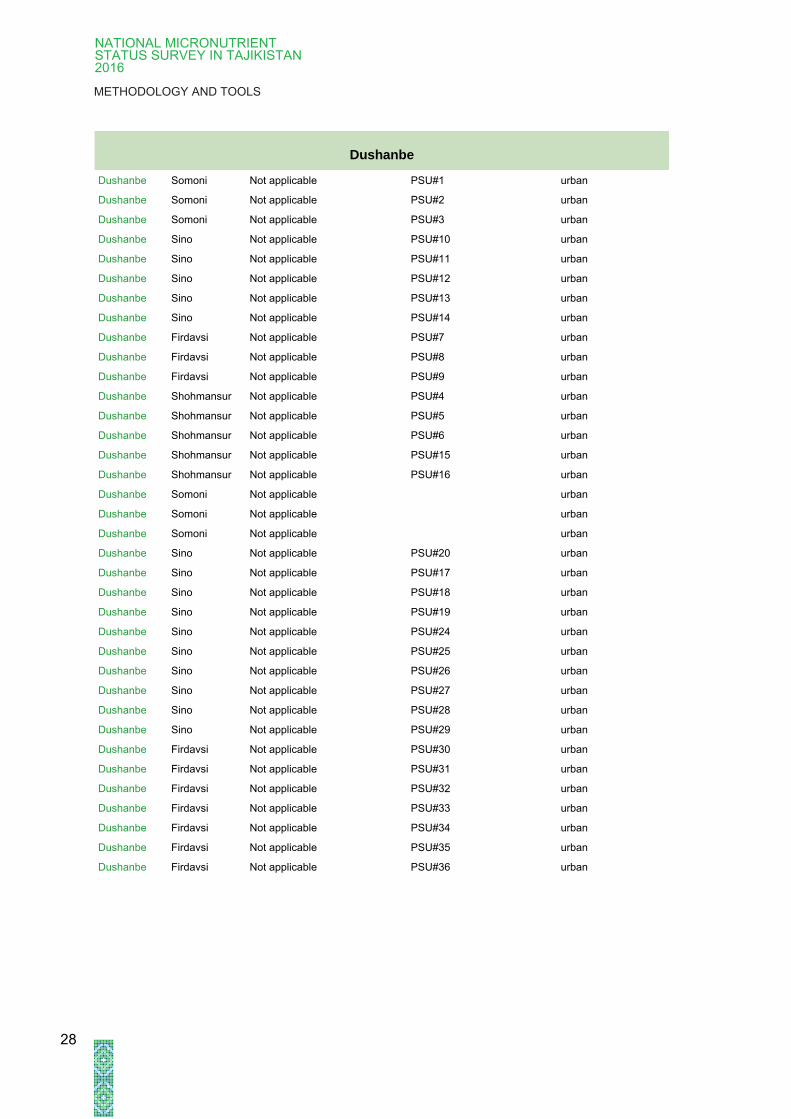
Annex 1:
List of Clusters included in the survey
Region / Oblast
District / rayon
Jamoat Village or Street Type Population in cluster
DRS Varzob Ayni Kharrangoni Bolo rural 1,592
DRS Gissar Gissar Gissar urban 24,400
DRS Gissar Almosi Sugdiyon (Chagatoy) rural 1,090
DRS Gissar Mirzo Rizo Hochildiyor rural 2,459
DRS Gissar Mirzo Tursunzoda (Karamkul) Avzikent rural 3,193
DRS Gissar Navabad Davlatmanka rural 1,298
DRS Gissar Somon (Khonakokh) Gayratabad rural 3,105
DRS Rudaki Gulistan Sabzikor rural 2,284
DRS Rudaki Chimteppa (Okkurgon) Obchakoron (Pakhtakor) rural 4,501
DRS Rudaki Chorgulteppa (Kuktosh) Zarnisor (Iangiabad) rural 3,283
DRS Rudaki Chorgulteppa (Kuktosh) Pakhtakor (Kyzyl Pakhtakor) rural 2,884
DRS Tursubzoda Tursubzoda Tursunzoda urban 46,700
DRS Tursubzoda Tursuna Tuychieva (1 May) Buston (Kungurot) rural 214
DRS Tursubzoda Karatog Karatog rural 4,953
DRS Tursubzoda Navabad Shulum rural 944
DRS Shahrinav Shahrinav Oktiabrskiy urban 5,900
DRS Vahdat Vahdat Vahdat urban 40,600
DRS Vahdat Bahor Gulistan rural 1,377
DRS Vahdat Bahor Shakhraki shifo (Shifo) rural 967
DRS Vahdat Gulistan (Karasu) Kishovarz (Itok) rural 2,169
DRS Vahdat Gulistan (Karasu) Tilloi Safed (Teshiktosh) rural 3,081
DRS Vahdat Abdullo Abdulvosieva Chillamazor rural 3,272
DRS Vahdat Karima Ismoilova Muminabadi Poyon rural 1,064
DRS Vahdat Simigandzh Diiamon rural 798
DRS Vahdat Chuiangaron Dzhavoni (Dahanai Chorbog) rural 1,761
DRS Fayzabad Fayzabad Fayzabad urban 8,700
DRS Fayzabad Vishgard Lolagi rural 2,429
DRS Fayzabad Miskinabad Saroy rural 2,237
DRS Nurabad Izagullo Halimova (Yahakiust) Kumbak rural 385
DRS Nurabad Mudzhiharf Mekhnat rural 480
DRS Rasht Nusratullo Makhsum (Kaznok) Kaznok rural 2,181
DRS Rasht Dzhafr Nimich rural 1,560
DRS Rasht Kalaisurkh Chorchurog rural 331
DRS Rasht Rakhimzade Podgey (Podgey poyon) rural 1,288
DRS Jirgital Alga Achik Alma rural 736
DRS Jirgital Iangishakhr Iangishakhr rural 1,550
24
DRD

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Khatlon
Khatlon Bokhtar Kurgan-Tube Kurgan Tube urban 75,500
Khatlon Bokhtar Oriyon (Avangard) Komintern rural 3,943
Khatlon Bokhtar Navbahor Navdidor (Navobod) rural 1,052
Khatlon Vakhsh Tajhikabad Havaskor rural 1,640
Khatlon Vakhsh Kirov Chorgulteppa rural 531
Khatlon A.Jomi Dusti (Oktiabr) Galaba rural 3,144
Khatlon A.Jomi Iakkatut Krasnaia Zvezda rural 2,879
Khatlon Yavan Norin 1 Maia rural 4,554
Khatlon Yavan Obimuki Obimuki rural 4,356
Khatlon Yavan Obimuki Parchasoy rural 5,025
Khatlon J.Rumi Uzun Telman (Gandzhina ) rural 1,091
Khatlon Qumsangir Qumsangir Dusti urban 14,500
Khatlon Qumsangir Piandzh Pioner rural 4,724
Khatlon Panj Mekhvar (Kuldiman) Burhiyon (Iukoritemez) rural 1,360
Khatlon Panj Nuri Vakhdat (Tugul) Gulabad rural 2,048
Khatlon Panj Ozodagon (Sarmantoy) Turdishaykh rural 1,548
Khatlon Shahrituz Shahrituz Shahrituz urban 14,700
Khatlon Shahrituz Saiyod Saiyod rural 3,764
Khatlon Shahrituz Pakhtaabad Sultonabad rural 4,405
Khatlon Jillikul Garavuti Shakhrinav rural 4,551
Khatlon Kubodien imeni Nosira Hisrava Hishtkupruk rural 3,201
Khatlon Kulob Kulob Kulob urban 95,000
Khatlon Kulob Dahana Oltovul rural 2,595
Khatlon Kulob Zarbdor I.Ibrohimova rural 1,223
Khatlon Kulob Zarbdor Sariosiyo rural 2,018
Khatlon Voce Voce Vose urban 20,600
Khatlon Voce Gulistan Kurbonshahid rural 8,647
Khatlon Voce Mirali Makhmadalieva (Aral) Hulbek rural 4,746
Khatlon Shuronod Shuroobod Shuroobod* rural 1,136
Khatlon Muminobod Balhobi Bogihabib rural 1,661
Khatlon Farkhor Farkhor Farkhor urban 21,500
Khatlon Farkhor Watan Sebisurkh rural 1,531
Khatlon Norak Dukoni Chashma rural 1,026
Khatlon Temurmalik Karakamish Dahaninamak rural 1,277
Khatlon Temurmalik Karakamish Karakamish rural 1,502
Khatlon Temurmalik Kushkiya Mooreodbakhsh rural 530
25
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Sughd
Sughd B.Gafurov Khujand Khujand PSU#1 urban 40,700
Sughd B.Gafurov Khujand Khujand PSU#2 urban 40,700
Sughd B.Gafurov Khujand Khujand PSU#3 urban 40,700
Sughd B.Gafurov Khujand Khujand PSU#4 urban 40,700
Sughd B.Gafurov B.Gafurov Gafurov urban 16,900
Sughd B.Gafurov Dadoboi Holmatov (Pakhtakor) Kuybyshev rural 4,294
Sughd B.Gafurov Zarzamin (Katagan) Katagan rural 10,647
Sughd B.Gafurov Ismoil Kurgoncha rural 1,297
Sughd B.Gafurov Ismoil Chordara rural 1,682
Sughd B.Gafurov Isfisor Isfisor rural 30,893
Sughd B.Gafurov Undji Okarik rural 7,095
Sughd B.Gafurov Undji Undzhi rural 16,178
Sughd B.Gafurov Histevarz (Kistakuz) Kistakuz rural 51,779
Sughd Maschoh Paldorak Paldorak rural 16,010
Sughd Asht Mekhrobod (Kamyshkurgon) Bakhmal rural 1,118
Sughd Asht Shaydon Dahana rural 2,383
Sughd Asht Shaydon Mullomir rural 2,055
Sughd Gonchi I.Somoni (Kalininabad) Kalachai Hodzhi rural 2,452
Sughd Gonchi Iakhtan Iakhtan rural 2,004
Sughd Spitamen Sarband (Kushtegirmon) Kushtegirmon rural 7,855
Sughd J.Rasulov Gulakandoz Gulakandoz rural 36,848
Sughd Zafarobod Ravshan Guliston (Ai`ni) rural 8,928
Sughd Istaravshan Istaravshan PSU#1 urban 27,350
Sughd Istaravshan Istaravshan PSU#2 urban 27,350
Sughd Istaravshan Gulisurkh Tapkok rural 3,035
Sughd Istaravshan Zarhalol (Kommunizm) Dzharkurgon rural 6,217
Sughd Istaravshan Poshkent Iakkabog rural 3,679
Sughd Istaravshan Sabriston (Frunze) Rugund rural 7,397
Sughd Shahriston Shakhristan Firdavsi (Buragen) rural 1,878
Sughd Isfara Isfara Isfara urban 42,900
Sughd Konibodom Konibodom Konibodom urban 46,500
Sughd Konibodom Puloton Sarikuy rural 10,855
Sughd Panjakent Loik Sherali (Kolhozchiyon) Mazor rural 1,300
Sughd Panjakent Mogiyon Puligirdob rural 2,097
Sughd Panjakent Sarahzm (Chimkurgon) Abdusamad rural 1,504
Sughd Panjakent Sudzhina Sudzhina rural 8,830
26
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
GBAO
GBAO Darvoz Nulvand Sangevn rural 273
GBAO Ishkashim Askar Zamirov (Andarob) Khaskhorugh rural 185
GBAO Ishkashim Ptup Zumudg rural 819
GBAO Ishkashim Vrang Vrang rural 1,722
GBAO Ishkashim Vrang Shirgin rural 829
GBAO Murghab Alichur Alichur rural 1,223
GBAO Murghab Gojo Berdiev (Konakurghan)
Konakurghan rural 723
GBAO Murghab Murghab Mamazair rural 445
GBAO Murghab Murghab Murghab rural 6,259
GBAO Roshtqala Barvoz Zanudge rural 204
GBAO Roshtqala Kurbonsho Gadoliev (Tavdem)
Bodomi-bolo rural 278
GBAO Roshtqala Kurbonshoh Gadoliev (Tavdem)
Kayonen rural 296
GBAO Roshtqala Tusen Devlokh rural 174
GBAO Roshtqala Sejd Shoshdararuya rural 161
GBAO Rushon Basid Basid rural 609
GBAO Rushon Muminshokh Abdulvosiev (Shidz)
Shidz rural 784
GBAO Rushan Muminshoh Abdulvosiev (Shidz)
Dikh rural 400
GBAO Rushan Nazarsho Dodkhudoev (Bakhrushan)
Barzud rural 1,192
GBAO Rushan Nazarsho Dodkhudoev (Bakhrushan)
Bachrushan rural 2,233
GBAO Rushan Nazarshoh Dodkhudoev (Bakhrushan)
Vamd rural 722
GBAO Rushan Rushan Rushan rural 4,031
GBAO Shugnan Garibshoh Shakhbozov (Darmorakht)
Pish rural 621
GBAO Shugnan Navabad Mun rural 1,268
GBAO Shugnan Navabad Rivak rural 656
GBAO Shugnan Navabad Turbat rural 483
GBAO Shugnan Porshnev Churudge rural 305
GBAO Shugnon Vankala Imom rural 323
GBAO Khorog Khorog Khorog urban
28,100
GBAO Khorog Khorog Khorog urban
GBAO Khorog Khorog Khorog urban
GBAO Khorog Khorog Khorog urban
GBAO Khorog Khorog Khorog urban
GBAO Vanj Mahmadullo Abdulloev (Vandge)
Gushkhun rural 1,279
GBAO Vanj Mahmadullo Abdulloev (Vandge)
Panjshanbeabad rural 391
GBAO Vanj Rovand Vanvani-bolo rural 322
GBAO Vanj Rovand Starg rural 287
27
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Dushanbe
Dushanbe Somoni Not applicable PSU#1 urban
Dushanbe Somoni Not applicable PSU#2 urban
Dushanbe Somoni Not applicable PSU#3 urban
Dushanbe Sino Not applicable PSU#10 urban
Dushanbe Sino Not applicable PSU#11 urban
Dushanbe Sino Not applicable PSU#12 urban
Dushanbe Sino Not applicable PSU#13 urban
Dushanbe Sino Not applicable PSU#14 urban
Dushanbe Firdavsi Not applicable PSU#7 urban
Dushanbe Firdavsi Not applicable PSU#8 urban
Dushanbe Firdavsi Not applicable PSU#9 urban
Dushanbe Shohmansur Not applicable PSU#4 urban
Dushanbe Shohmansur Not applicable PSU#5 urban
Dushanbe Shohmansur Not applicable PSU#6 urban
Dushanbe Shohmansur Not applicable PSU#15 urban
Dushanbe Shohmansur Not applicable PSU#16 urban
Dushanbe Somoni Not applicable
urban
Dushanbe Somoni Not applicable
urban
Dushanbe Somoni Not applicable
urban
Dushanbe Sino Not applicable PSU#20 urban
Dushanbe Sino Not applicable PSU#17 urban
Dushanbe Sino Not applicable PSU#18 urban
Dushanbe Sino Not applicable PSU#19 urban
Dushanbe Sino Not applicable PSU#24 urban
Dushanbe Sino Not applicable PSU#25 urban
Dushanbe Sino Not applicable PSU#26 urban
Dushanbe Sino Not applicable PSU#27 urban
Dushanbe Sino Not applicable PSU#28 urban
Dushanbe Sino Not applicable PSU#29 urban
Dushanbe Firdavsi Not applicable PSU#30 urban
Dushanbe Firdavsi Not applicable PSU#31 urban
Dushanbe Firdavsi Not applicable PSU#32 urban
Dushanbe Firdavsi Not applicable PSU#33 urban
Dushanbe Firdavsi Not applicable PSU#34 urban
Dushanbe Firdavsi Not applicable PSU#35 urban
Dushanbe Firdavsi Not applicable PSU#36 urban
28

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Annex 2: Study team
Position Name and organisation Role
Survey Implementer Dr. Saida Umarzoda, First Deputy
Minister of Health and Social Protection
of the Population (MHSPP)
Overall supervision and steering of
National Micronutrient Statusal Survey
Survey implementer Dr. Zoir Nabiev, Director of Paediatric
Research Institute, Tajikistan
Supervision and steering of field
activities. ethical and regulatory aspects
Survey Implementer Dr. Sherali Rahmatulloev, Head of
Maternal and Child Health departments,
MHSPP
Supervision and steering of field
activities. ethical and regulatory aspects
Survey Implementer Dr. Samariddin Aliev, Director of Public
Health Institute
Supervision and steering of labaratory
activities
Survey implementer Dr. Bunafsha Kholova Tagoybekovna,
Research Laboratory of Preventive
Medicine
Oversight of transport, storage and
analysis of biological samples
Survey implementer Dr. Obidjon Aminov, Paediatric Research
Institute, Tajikistan
Supervision and steering of field
activities. ethical and regulatory aspects
Sponsor Lucia Elmi, Representative of UNICEF in
Tajikistan
Technical expert Dr. Amir Yarparvar, UNICEF Contributions to survey data analysis and
quality assurance
Technical expert,
coordinating researcher
Yuki Suehiro, UNICEF Coordination of survey (including
sampling) and contributions to planning,
analysis and dissemination.
Technical expert,
coordinating researcher
Dr Safina Abdulloeva, UNICEF Coordination of survey (including
sampling) and contributions to planning,
analysis and dissemination
Technical expert Dr. Mutribjon Bahruddinov, UNICEF Contributions to survey planning
Project Leader, coordinating
researcher, principal
investigator
Prof Dr. Kaspar Wyss, Swiss TPH Overall coordination of planning of survey
(including sampling) and data analysis.
Report writing.
Quality assurance manager Sabine Kiefer, Swiss TPH Technical support, preparation of field
activities, backstopping during field data
collection
Quality assurance manager Dr Adrian Verbel, Swiss TPH Technical support, preparation of field
activities, coordination and supervision of
field data collection, quality assurance
National supervisor Usmon Musoev, Swiss TPH Preparation of field activities, coordination
and supervision of field data collection,
translation
National supervisor Dr. Sanavbar Rakhmatullaeva, Swiss
TPH
Coordination and supervision of field data
collection
Laboratory and nutrition
specialist & epidemiologist
Dr. Tanja Barth-Jaeggi Planning and conception of laboratory
analysis. Data analysis
Laboratory and nutrition
specialist
Dr Lizelle L. Zandberg Planning and supervision of laboratory
analysis
Epidemiologist/statistician Dr Helena Greter, Swiss TPH Data analysis
29

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Annex 3: Questionnaire
1. HOUSEHOLD IDENTIFICATION NUMBER
OBLAST CLUSTER HOUSEHOLD
|__| |__|__|__| |__|__|__|
1.1. Type of dwelling 1= Communal flat; 2= House;
88=Other → specify: |__|__|__|__|__|__|__||__|__|
|__|__|
1.2. How many people live in this household? |__|__|
1.3. Ethnic group 1=Tajik; 2=Uzbek; 3=Russian; 4=Kyrgyz;
88= Other → specify: |__|__|__|__|__|__|__|__|__|
|__|__|
1.4. Gender of the household head? 1=male; 2=female |__|
1.5. What is the household head’s highest
level of education?
1 = none
2 = primary (Grades 1-9)
3 = secondary (Grades 10-11)
5 = vocational/technical education
6 = higher
education (e.g.
university)
99 = don’t know
|__|__|
1.6. What is your household’s main source
of cash income?
1 = private business;
2 = salary;
3 = pension/social assistance;
4 = farming/livestock;
5 = remittances
7 = no cash
income;
88= other
99 = don’t know
|__|__|
1.7. Do you grow food or animals for your own consumption? 1=yes; 2=no;
IF NO GO TO 1.10 |__|
1.8. What do you grow for your own consumption? 1=yes; 2=no;
1.8.1. Wheat, rice |__|__|
1.8.2. Beans, peas, lentils, nuts |__|__|
1.8.3. Potatoes or other routs or tubers |__|__|
1.8.4. Yellow or orange coloured vegetables (pumpkins, carrots) or fruits
(yellow plums or apricots)
|__|__|
1.8.5. Green leafy vegetables |__|__|
1.8.6. Other vegetables and fruits |__|__|
1.9. Do you keep animals for meat and milk production for your own
consumption?
1=yes; 2=no
1.9.1. Cows |__|
1.9.2. Sheep |__|
1.9.3. Goats |__|
1.9.4. Chickens / poultry |__|
1.9.5. Horses |__|
1.10. Are there any children under five years of age in this household
with disabilities?
1=yes; 2=no; 99=don’t know
IF NO OR DON’T KNOW GO TO
1.11
Which of the following disabilities does the children under five
years of age in this household have?
1=yes; 2=no; 99=don’t know
1.10.1. Blindness |__|__|
1.10.2. Deafness |__|__|
1.10.3. Motor disability |__|__|
1.10.4. Mental disability |__|__|
1.11. Have you ever heard about iodization of edible salt? 1=yes; 2=no; |__|
1.12. What kind of edible salt do you usually use? 1= iodized salt;
2= non-iodized salt
99 = don’t know
|__|__|
30
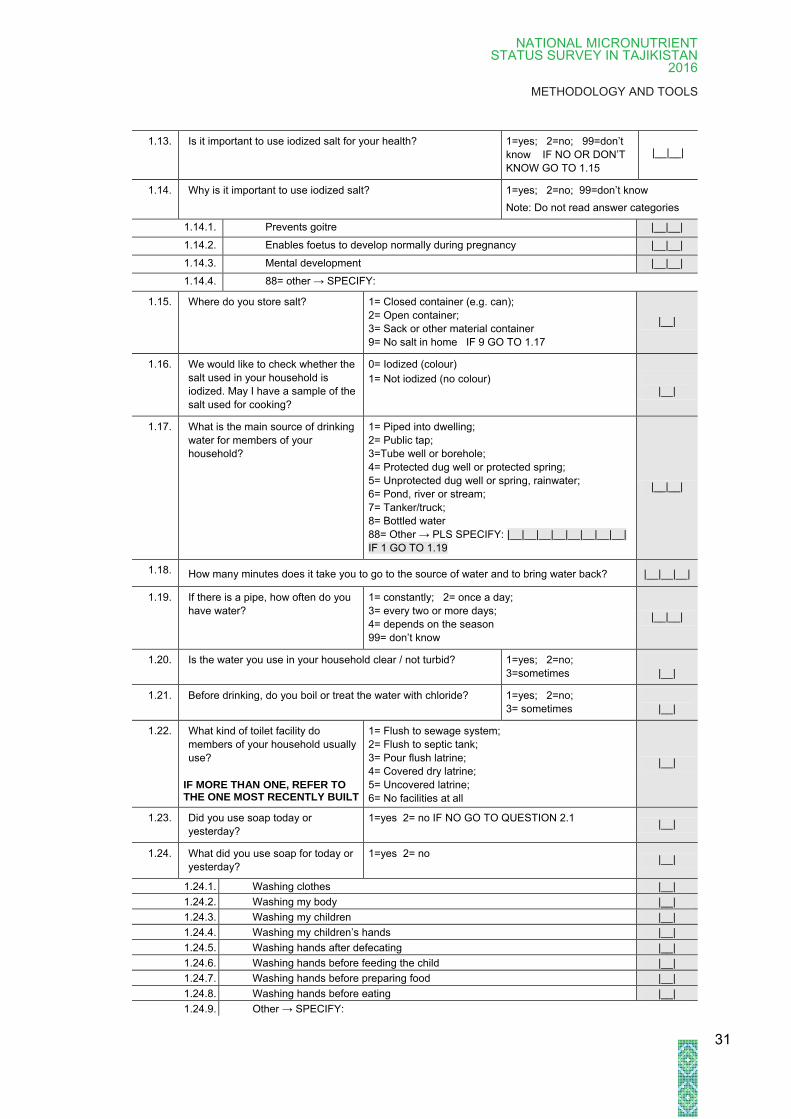
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
1.13. Is it important to use iodized salt for your health? 1=yes; 2=no; 99=don’t
know IF NO OR DON’T
KNOW GO TO 1.15
|__|__|
1.14. Why is it important to use iodized salt? 1=yes; 2=no; 99=don’t know
Note: Do not read answer categories
1.14.1. Prevents goitre |__|__|
1.14.2. Enables foetus to develop normally during pregnancy |__|__|
1.14.3. Mental development |__|__|
1.14.4. 88= other → SPECIFY:
1.15. Where do you store salt? 1= Closed container (e.g. can);
2= Open container;
3= Sack or other material container
9= No salt in home IF 9 GO TO 1.17
|__|
1.16. We would like to check whether the
salt used in your household is
iodized. May I have a sample of the
salt used for cooking?
0= Iodized (colour)
1= Not iodized (no colour)
|__|
1.17. What is the main source of drinking
water for members of your
household?
1= Piped into dwelling;
2= Public tap;
3=Tube well or borehole;
4= Protected dug well or protected spring;
5= Unprotected dug well or spring, rainwater;
6= Pond, river or stream;
7= Tanker/truck;
8= Bottled water
88= Other → PLS SPECIFY: |__|__|__|__|__|__|__|__|
IF 1 GO TO 1.19
|__|__|
1.18. How many minutes does it take you to go to the source of water and to bring water back? |__|__|__|
1.19. If there is a pipe, how often do you
have water?
1= constantly; 2= once a day;
3= every two or more days;
4= depends on the season
99= don’t know
|__|__|
1.20. Is the water you use in your household clear / not turbid? 1=yes; 2=no;
3=sometimes
|__|
1.21. Before drinking, do you boil or treat the water with chloride? 1=yes; 2=no;
3= sometimes
|__|
1.22. What kind of toilet facility do
members of your household usually
use?
IF MORE THAN ONE, REFER TO THE ONE MOST RECENTLY BUILT
1= Flush to sewage system;
2= Flush to septic tank;
3= Pour flush latrine;
4= Covered dry latrine;
5= Uncovered latrine;
6= No facilities at all
|__|
1.23. Did you use soap today or
yesterday?
1=yes 2= no IF NO GO TO QUESTION 2.1 |__|
1.24. What did you use soap for today or
yesterday?
1=yes 2= no |__|
1.24.1. Washing clothes |__|
1.24.2. Washing my body |__|
1.24.3. Washing my children |__|
1.24.4. Washing my children’s hands |__|
1.24.5. Washing hands after defecating |__|
1.24.6. Washing hands before feeding the child |__|
1.24.7. Washing hands before preparing food |__|
1.24.8. Washing hands before eating |__|
1.24.9. Other → SPECIFY:
31
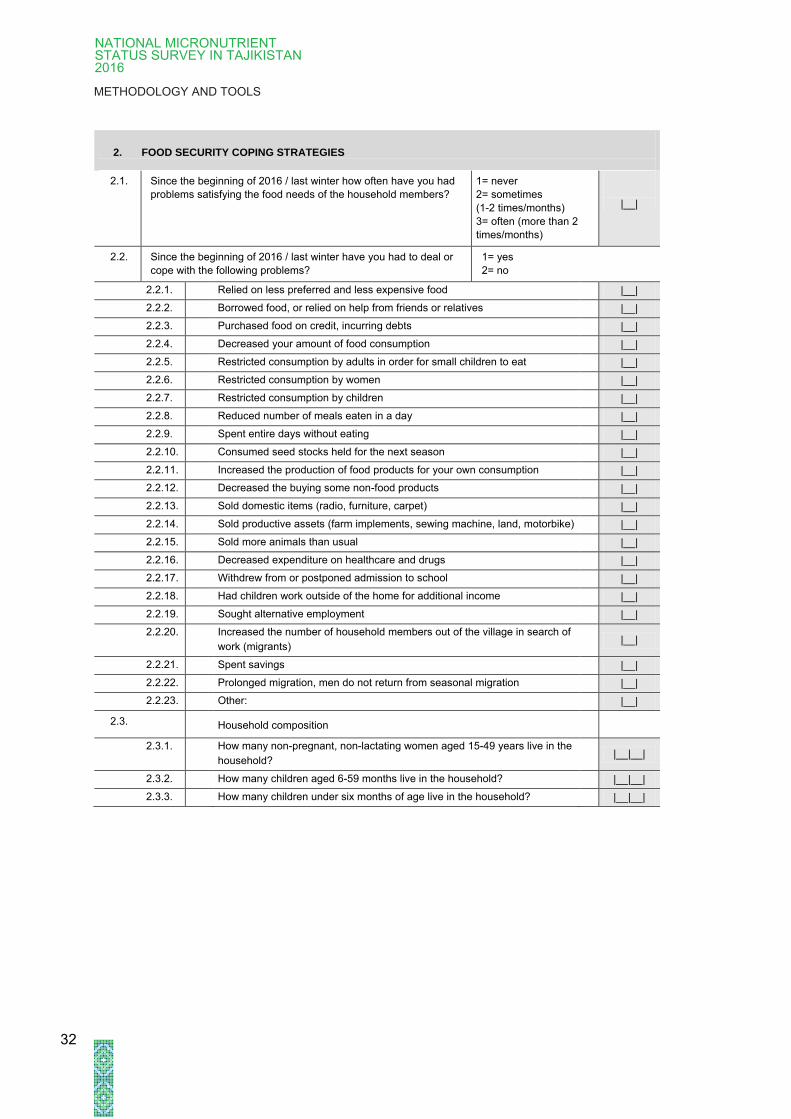
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
2. FOOD SECURITY COPING STRATEGIES
2.1. Since the beginning of 2016 / last winter how often have you had
problems satisfying the food needs of the household members?
1= never
2= sometimes
(1-2 times/months)
3= often (more than 2
times/months)
|__|
2.2. Since the beginning of 2016 / last winter have you had to deal or
cope with the following problems?
1= yes
2= no
2.2.1. Relied on less preferred and less expensive food |__|
2.2.2. Borrowed food, or relied on help from friends or relatives |__|
2.2.3. Purchased food on credit, incurring debts |__|
2.2.4. Decreased your amount of food consumption |__|
2.2.5. Restricted consumption by adults in order for small children to eat |__|
2.2.6. Restricted consumption by women |__|
2.2.7. Restricted consumption by children |__|
2.2.8. Reduced number of meals eaten in a day |__|
2.2.9. Spent entire days without eating |__|
2.2.10. Consumed seed stocks held for the next season |__|
2.2.11. Increased the production of food products for your own consumption |__|
2.2.12. Decreased the buying some non-food products |__|
2.2.13. Sold domestic items (radio, furniture, carpet) |__|
2.2.14. Sold productive assets (farm implements, sewing machine, land, motorbike) |__|
2.2.15. Sold more animals than usual |__|
2.2.16. Decreased expenditure on healthcare and drugs |__|
2.2.17. Withdrew from or postponed admission to school |__|
2.2.18. Had children work outside of the home for additional income |__|
2.2.19. Sought alternative employment |__|
2.2.20. Increased the number of household members out of the village in search of
work (migrants)
|__|
2.2.21. Spent savings |__|
2.2.22. Prolonged migration, men do not return from seasonal migration |__|
2.2.23. Other: |__|
2.3. Household composition
2.3.1. How many non-pregnant, non-lactating women aged 15-49 years live in the
household?
|__|__|
2.3.2. How many children aged 6-59 months live in the household? |__|__|
2.3.3. How many children under six months of age live in the household? |__|__|
32

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
FORM 2: TO BE ANSWERED BY CARER OF CHILD (AGED 6-59 MONTHS)
3. CHILD HEALTH FOR ALL CHILDEN AGED 6-59 MONTHS (START WITH THE YOUNGEST) RESPONDENT: CARETAKER
HOUSEHOLD IDENDIFICATION NUMBER OBLAST
|__|
CLUSTER
|__|__|__|
HOUSEHOLD
|__|__|__|
3.1. ID CODE of the CHILD (AGED 6-59 MONTHS) FROM REGISTRATION FORM |__|__|
3.2. Date of birth of child DD/MM/YY |__|__| / |__|__| /
|__|__|
3.3. Does your child have a birth certificate? 1= yes; 2= no |__|
3.4. What was your child’s birth weight? Enter child’s birth weight in
Lg
99=don’t know
|__| ,|__||__|
|__|__|
3.5. Has the child had diarrhoea (more than three loose
stools per day) in the past 2 weeks?
1=yes; 2=no;
99=don’t know |__|__|
3.6. In general, when your child has diarrhoea does the
child drink any of the following items
1=yes; 2=no
99=don’t know
|__|__|
3.6.1. Breast milk |__|__|
3.6.2. Soup |__|__|
3.6.3. Herbal tea (camomille, fennel, hibiscus) |__|__|
3.6.4. Tea (black or green) |__|__|
3.6.5. ORS packet solution |__|__|
3.6.6. Other milk or infant formula |__|__|
3.6.7. Water, with feeding during some parts of the day |__|__|
3.6.8. Water alone |__|__|
3.6.9. Soft drinks (with gas) |__|__|
3.6.10. Sugary water or fruit juices |__|__|
3.6.11. Antibiotics/anti-diarrheal drugs |__|__|
3.6.12. other → PLS SPECIFY:
3.7. In general when your child has diarrhoea does
he/she drink much less, about the same, or more
than usual?
1= Much less or none
2= About the same
3= More
99= Don’t know
|__|__|
3.8. Has your child been diagnosed with severe
malnutrition?
1=yes; 2=no;
99=don’t know
IF NO OR DON’T KNOW GO
TO 3.11
|__|__|
3.9. Did your child receive or is your child receiving any
medical treatment for severe malnutrition?
1= yes; 2=no;
99=don’t know IF NO OR
DON`T KNOW GO TO 3.11
|__|__|
3.10. Where did you receive medical treatment for severe
malnutrition?
1= Health house
2= Rural health centre
3= Polyclinic
4= Rayon hospital
5= Oblast hospital
88= Other (specify)
|__|__|
3.11. Does your child have vision problems at night?
(vision adaptation to darkness – night blindness)
1= yes; 2= no;
99= don’t know |__|__|
3.12. Did your child have or have had a goiter? 1= yes; 2= no;
99= don’t know |__|__|
33
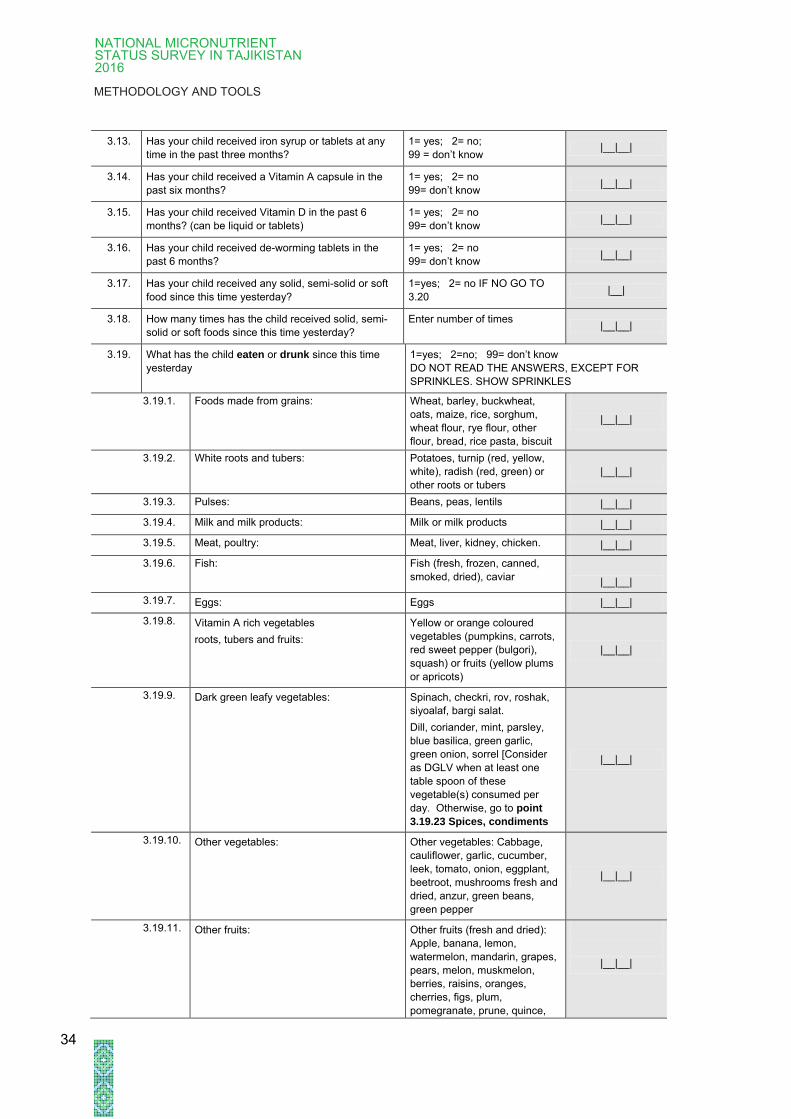
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
3.13. Has your child received iron syrup or tablets at any
time in the past three months?
1= yes; 2= no;
99 = don’t know |__|__|
3.14. Has your child received a Vitamin A capsule in the
past six months?
1= yes; 2= no
99= don’t know |__|__|
3.15. Has your child received Vitamin D in the past 6
months? (can be liquid or tablets)
1= yes; 2= no
99= don’t know |__|__|
3.16. Has your child received de-worming tablets in the
past 6 months?
1= yes; 2= no
99= don’t know |__|__|
3.17. Has your child received any solid, semi-solid or soft
food since this time yesterday?
1=yes; 2= no IF NO GO TO
3.20 |__|
3.18. How many times has the child received solid, semi-
solid or soft foods since this time yesterday?
Enter number of times |__|__|
3.19. What has the child eaten or drunk since this time
yesterday
1=yes; 2=no; 99= don’t know
DO NOT READ THE ANSWERS, EXCEPT FOR
SPRINKLES. SHOW SPRINKLES
3.19.1. Foods made from grains: Wheat, barley, buckwheat,
oats, maize, rice, sorghum,
wheat flour, rye flour, other
flour, bread, rice pasta, biscuit
|__|__|
3.19.2. White roots and tubers: Potatoes, turnip (red, yellow,
white), radish (red, green) or
other roots or tubers
|__|__|
3.19.3. Pulses: Beans, peas, lentils |__|__|
3.19.4. Milk and milk products: Milk or milk products |__|__|
3.19.5. Meat, poultry: Meat, liver, kidney, chicken. |__|__|
3.19.6. Fish: Fish (fresh, frozen, canned,
smoked, dried), caviar
|__|__|
3.19.7. Eggs: Eggs |__|__|
3.19.8. Vitamin A rich vegetables
roots, tubers and fruits:
Yellow or orange coloured
vegetables (pumpkins, carrots,
red sweet pepper (bulgori),
squash) or fruits (yellow plums
or apricots)
|__|__|
3.19.9. Dark green leafy vegetables: Spinach, checkri, rov, roshak,
siyoalaf, bargi salat.
Dill, coriander, mint, parsley,
blue basilica, green garlic,
green onion, sorrel [Consider
as DGLV when at least one
table spoon of these
vegetable(s) consumed per
day. Otherwise, go to point
3.19.23 Spices, condiments
|__|__|
3.19.10. Other vegetables: Other vegetables: Cabbage,
cauliflower, garlic, cucumber,
leek, tomato, onion, eggplant,
beetroot, mushrooms fresh and
dried, anzur, green beans,
green pepper
|__|__|
3.19.11. Other fruits: Other fruits (fresh and dried):
Apple, banana, lemon,
watermelon, mandarin, grapes,
pears, melon, muskmelon,
berries, raisins, oranges,
cherries, figs, plum,
pomegranate, prune, quince,
|__|__|
34
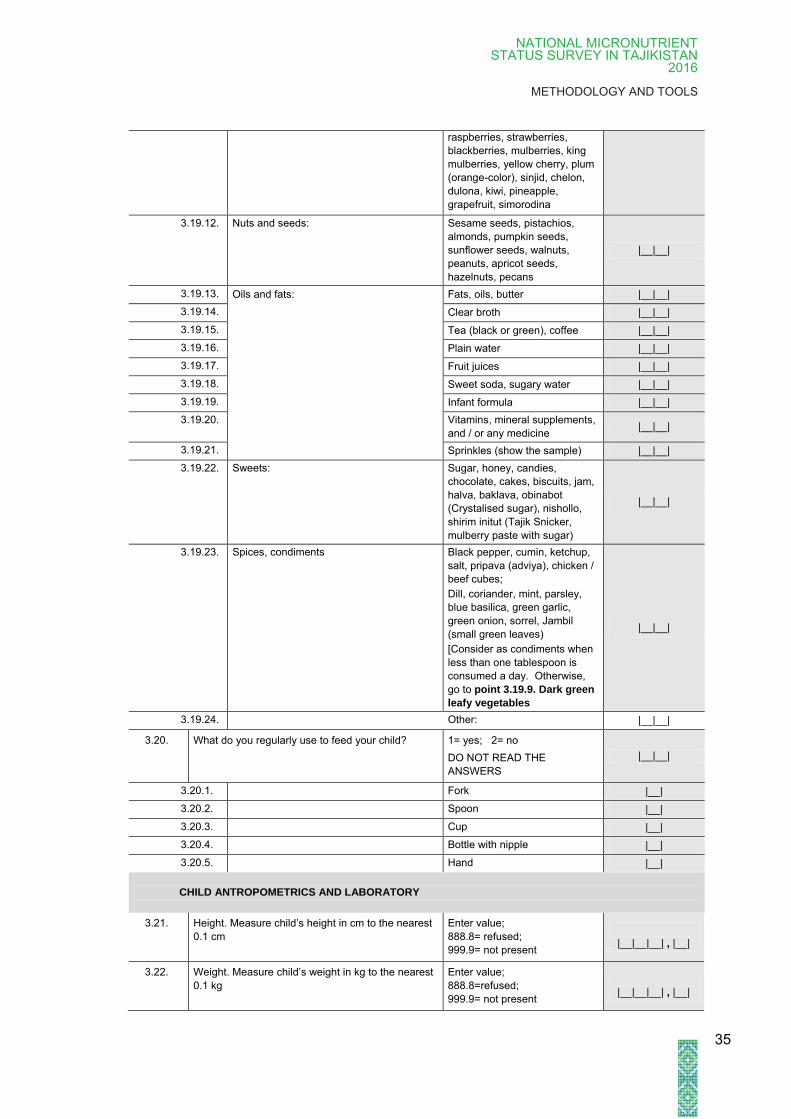
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
raspberries, strawberries,
blackberries, mulberries, king
mulberries, yellow cherry, plum
(orange-color), sinjid, chelon,
dulona, kiwi, pineapple,
grapefruit, simorodina
3.19.12. Nuts and seeds: Sesame seeds, pistachios,
almonds, pumpkin seeds,
sunflower seeds, walnuts,
peanuts, apricot seeds,
hazelnuts, pecans
|__|__|
3.19.13. Oils and fats: Fats, oils, butter |__|__|
3.19.14. Clear broth |__|__|
3.19.15. Tea (black or green), coffee |__|__|
3.19.16. Plain water |__|__|
3.19.17. Fruit juices |__|__|
3.19.18. Sweet soda, sugary water |__|__|
3.19.19. Infant formula |__|__|
3.19.20.
Vitamins, mineral supplements,
and / or any medicine |__|__|
3.19.21. Sprinkles (show the sample) |__|__|
3.19.22. Sweets: Sugar, honey, candies,
chocolate, cakes, biscuits, jam,
halva, baklava, obinabot
(Crystalised sugar), nishollo,
shirim initut (Tajik Snicker,
mulberry paste with sugar)
|__|__|
3.19.23. Spices, condiments Black pepper, cumin, ketchup,
salt, pripava (adviya), chicken /
beef cubes;
Dill, coriander, mint, parsley,
blue basilica, green garlic,
green onion, sorrel, Jambil
(small green leaves)
[Consider as condiments when
less than one tablespoon is
consumed a day. Otherwise,
go to point 3.19.9. Dark green
leafy vegetables
|__|__|
3.19.24. Other: |__|__|
3.20. What do you regularly use to feed your child? 1= yes; 2= no
DO NOT READ THE
ANSWERS
|__|__|
3.20.1. Fork |__|
3.20.2. Spoon |__|
3.20.3. Cup |__|
3.20.4. Bottle with nipple |__|
3.20.5. Hand |__|
CHILD ANTROPOMETRICS AND LABORATORY
3.21. Height. Measure child’s height in cm to the nearest
0.1 cm
Enter value;
888.8= refused;
999.9= not present
|__|__|__| , |__|
3.22. Weight. Measure child’s weight in kg to the nearest
0.1 kg
Enter value;
888.8=refused;
999.9= not present
|__|__|__| , |__|
35

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
3.23. Mid-Upper Arm Circumference (MUAC) in cm Enter value;
888.8=refused;
999.9= not present
|__|__|__| , |__|
COLLECT BLOOD & URINE samples
3.24.
Anaemia. Record haemoglobin value (from
HemoCue) to the nearest 0.1 g/dL
Enter value;
88.8=refused;
99.9= not present
|__|__| , |__|
3.25. Blood taken and placed in Microtainer 1 = yes; 2 = no;
88= refused |__|__|
3.26. Urine collected and placed in Tube 1 = yes; 2 = no;
88=refused |__|__|
36

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
FILTER: FOR CHILDREN BETWEEN 6 and 24 MONTHS THE FOLLOWING
ADDITIONAL QUESTIONS WILL BE ASKED TO THE CARETAKER
4. INFANT FEEDING INTERVIEW: RESPONDENT CARER (ONLY FOR CHILDREN AGED 6–24 MONTHS)
4.1. Has your child ever been breastfed? 1= yes; 2= no; IF NO GO TO 4.11 |__|
4.2. How long after birth was the child put to the breast
for the first time?
1 = within the first 30 minutes from
delivery;
2 = within the first 6 hours;
3 = more than 6 hours after delivery;
99 = don’t know
|__|__|
4.3. Who helped you with breastfeeding, in the first
week?
1 = health professional;
2 = relatives: SPECIFY:
|__|__|__|__|__|__|__|__|__|
3 = mother’s support group
4 = nobody
|__|
4.4. How do you or did you breastfeed your child? 1 = on demand; 2 = at fixed intervals |__|
4.5. Are you still breastfeeding? 1= yes; 2= no; IF NO GO TO 4.7 |__|
4.6. Since this time yesterday, has your child been
breastfed and, if yes, how many times?
0= if no;
WRITE NUMBER= if yes.
THEN GO TO 4.9
|__|__|
4.7. After how many months did you stop breastfeeding
completely?
Write number of months
|__|__|
4.8. Why did you stop breastfeeding? 1 = not enough milk;
2 = mother‘s illness;
3 = baby’s illness;
4 = baby was not gaining enough
weight;
5 = no time;
6 = mother became pregnant;
7 = health worker’s recommendation
8 = relative’s recommendation
88= other; specify
99 = don’t know
|__|__|
4.9. For how long did you exclusively breastfeed your
child?
Write number of months
77= still exclusively breastfeeding
99= don’t know
If 77 then go to 4.16
COMMENT: Exclusive breastfeeding
implies that the child is or has only been
fed with breast milk and has not
received any other food or liquid,
including water or milk.
|__|__|
4.10. How old was your child the first time you fed
him/her with water or cow’s milk?
Write number of months
77= the child has never received water
or cow’s milk
99= don’t know
|__|__|
4.11. How old was your child the first time you fed
him/her with the following food or liquids?
READ POSSIBLE ANSWERS
Write age in months
Write 0. If it has not been given yet
|__|__|
4.11.1. Foods made from grains: Wheat, barley, buckwheat, oats, maize,
rice, sorghum, wheat flour, rye flour,
other flour, bread, rice pasta, biscuit
|__|__|
37
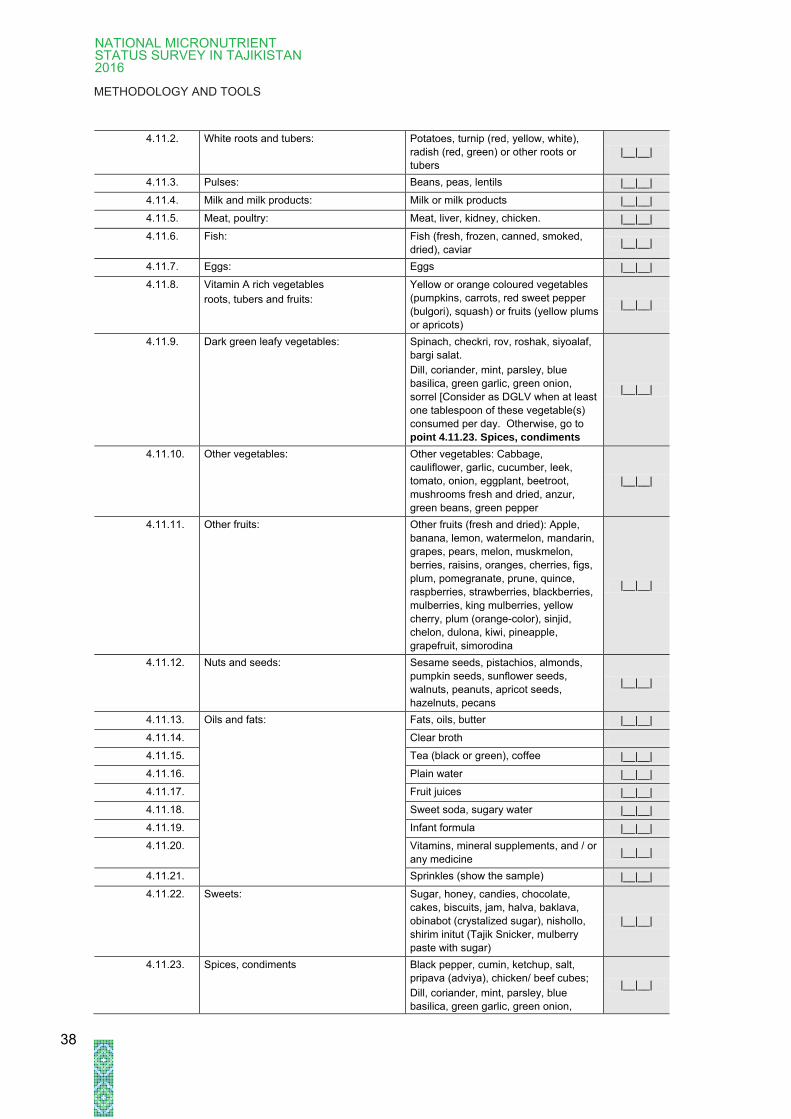
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
4.11.2. White roots and tubers: Potatoes, turnip (red, yellow, white),
radish (red, green) or other roots or
tubers
|__|__|
4.11.3. Pulses: Beans, peas, lentils |__|__|
4.11.4. Milk and milk products: Milk or milk products |__|__|
4.11.5. Meat, poultry: Meat, liver, kidney, chicken. |__|__|
4.11.6. Fish: Fish (fresh, frozen, canned, smoked,
dried), caviar |__|__|
4.11.7. Eggs: Eggs |__|__|
4.11.8. Vitamin A rich vegetables
roots, tubers and fruits:
Yellow or orange coloured vegetables
(pumpkins, carrots, red sweet pepper
(bulgori), squash) or fruits (yellow plums
or apricots)
|__|__|
4.11.9. Dark green leafy vegetables: Spinach, checkri, rov, roshak, siyoalaf,
bargi salat.
Dill, coriander, mint, parsley, blue
basilica, green garlic, green onion,
sorrel [Consider as DGLV when at least
one tablespoon of these vegetable(s)
consumed per day. Otherwise, go to
point 4.11.23. Spices, condiments
|__|__|
4.11.10. Other vegetables: Other vegetables: Cabbage,
cauliflower, garlic, cucumber, leek,
tomato, onion, eggplant, beetroot,
mushrooms fresh and dried, anzur,
green beans, green pepper
|__|__|
4.11.11. Other fruits: Other fruits (fresh and dried): Apple,
banana, lemon, watermelon, mandarin,
grapes, pears, melon, muskmelon,
berries, raisins, oranges, cherries, figs,
plum, pomegranate, prune, quince,
raspberries, strawberries, blackberries,
mulberries, king mulberries, yellow
cherry, plum (orange-color), sinjid,
chelon, dulona, kiwi, pineapple,
grapefruit, simorodina
|__|__|
4.11.12. Nuts and seeds: Sesame seeds, pistachios, almonds,
pumpkin seeds, sunflower seeds,
walnuts, peanuts, apricot seeds,
hazelnuts, pecans
|__|__|
4.11.13. Oils and fats: Fats, oils, butter |__|__|
4.11.14. Clear broth
4.11.15. Tea (black or green), coffee |__|__|
4.11.16. Plain water |__|__|
4.11.17. Fruit juices |__|__|
4.11.18. Sweet soda, sugary water |__|__|
4.11.19. Infant formula |__|__|
4.11.20. Vitamins, mineral supplements, and / or
any medicine |__|__|
4.11.21. Sprinkles (show the sample) |__|__|
4.11.22. Sweets: Sugar, honey, candies, chocolate,
cakes, biscuits, jam, halva, baklava,
obinabot (crystalized sugar), nishollo,
shirim initut (Tajik Snicker, mulberry
paste with sugar)
|__|__|
4.11.23. Spices, condiments Black pepper, cumin, ketchup, salt,
pripava (adviya), chicken/ beef cubes;
Dill, coriander, mint, parsley, blue
basilica, green garlic, green onion,
|__|__|
38

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
sorrel, Jambil (small green leaves)
[Consider as condiments when less
than one tablespoon consumed a day.
Otherwise, go to point 4.11.9. Dark
green leafy vegetables
4.11.24. Other: |__|__|
4.12. Since this time yesterday, has your child received
any of the following drinks?
1= yes; 2= no; IF NO GO TO 4.14
99= don’t know
4.12.1. Plain water |__|__|
4.12.2. Herbal tea |__|__|
4.12.3. Tea (black or green) |__|__|
4.12.4. Fruit juices |__|__|
4.13. Did you add sugar to the above drinks? 1= yes; 2= no; |__|
4.14. Since this time yesterday, did you give animal milk
to your child?
1= yes; 2= no
IF NO GO TO 4.16 |__|
4.15. Did you dilute the animal milk? 1 = yes; 2 = no; |__|
CARE AND DEVELOPMENT (ONLY FOR CHILDREN 6 – 24 MONTHS)
4.16. Did you have a visit from health workers (e.g.
patronage nurse) for your child’s health and
development in the past six months?
1 = yes; 2 = no;
IF NO → FINISH
|__|
4.17. Where did you meet the health worker? 1 = health centre;
2 = at home |__|
4.18. Why did you meet the health worker? 0 = growth monitoring
1 = child was sick
2 = for prevention (vaccination)
3 = for advice on care & development
|__|
|__|
|__|
|__|
4.19. Did the health workers ask you questions or give
you advice about the following?
1 = yes; 2 = no;
99= don’t know
4.19.1. Did s/he ask you about breastfeeding? |__|__|
4.19.2. Did s/he ask you about what foods you were giving your child or how you were
feeding your child? |__|__|
4.19.3. Did s/he ask you about what your child was able to do (e.g., talking, walking,
understanding)? |__|__|
4.19.4. Did s/he give you advice on how to feed your child? |__|__|
4.19.5. Did s/he give you advice on how to help your child to learn more? |__|__|
4.19.6. Did s/he give you advice on child discipline, care and sleep? |__|__|
4.19.7. Did you receive any other advice? |__|__|
4.19.7.1 PLEASE SPECIFY:
4.20. In the past three months, has your child’s weight
been measured?
1 = yes; 2 = no;
IF NO → GO TO 4.22 |__|__|
4.21. How many times has your child’s weight been
measured in the past three months?
PLEASE ENTER NUMBER OF TIMES |__|__|
4.22. In the past three months, has your child’s height
been measured?
1 = yes; 2 = no;
IF NO → FINISH |__|__|
4.23. How many times has your child’s height been
measured in the past three months?
PLEASE ENTER NUMBER OF TIMES |__|__|
4.24. Did you receive counselling after measurement of
weight or height?
1 = yes; 2 = no |__|__|
39
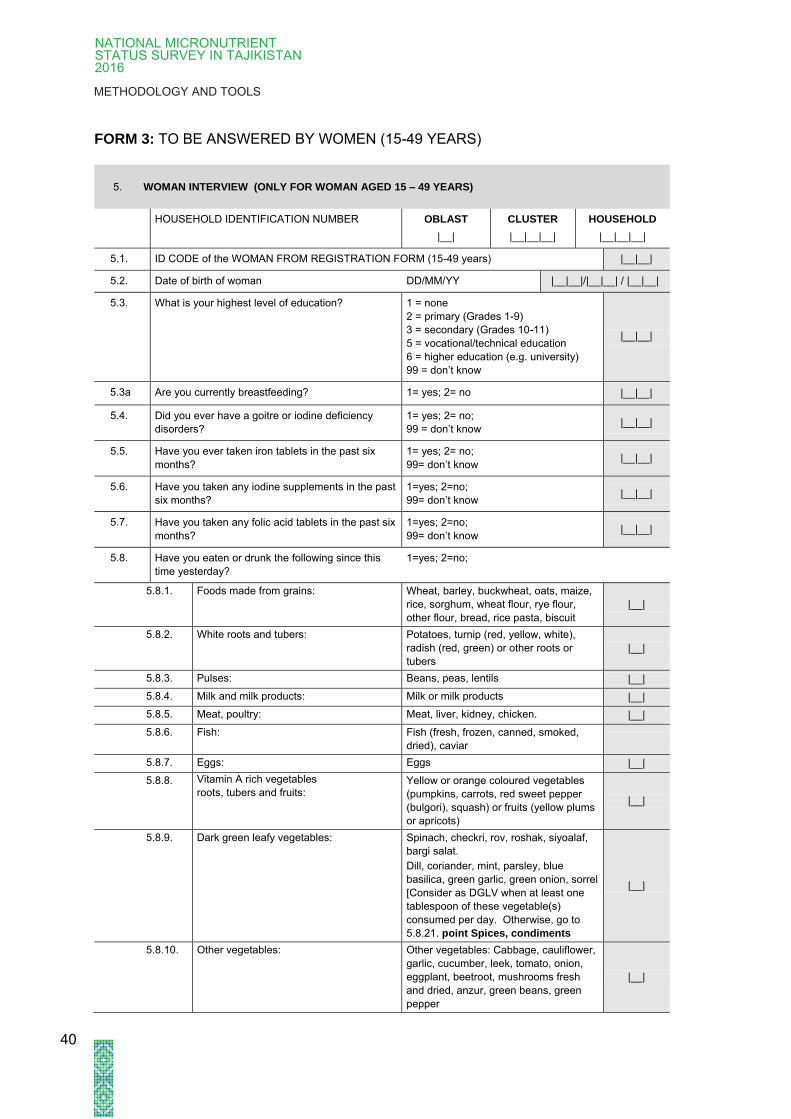
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
FORM 3: TO BE ANSWERED BY WOMEN (15-49 YEARS)
5. WOMAN INTERVIEW (ONLY FOR WOMAN AGED 15 – 49 YEARS)
HOUSEHOLD IDENTIFICATION NUMBER OBLAST
|__|
CLUSTER
|__|__|__|
HOUSEHOLD
|__|__|__|
5.1. ID CODE of the WOMAN FROM REGISTRATION FORM (15-49 years) |__|__|
5.2. Date of birth of woman DD/MM/YY |__|__|/|__|__| / |__|__|
5.3. What is your highest level of education? 1 = none
2 = primary (Grades 1-9)
3 = secondary (Grades 10-11)
5 = vocational/technical education
6 = higher education (e.g. university)
99 = don’t know
|__|__|
5.3a Are you currently breastfeeding? 1= yes; 2= no |__|__|
5.4. Did you ever have a goitre or iodine deficiency
disorders?
1= yes; 2= no;
99 = don’t know |__|__|
5.5. Have you ever taken iron tablets in the past six
months?
1= yes; 2= no;
99= don’t know |__|__|
5.6. Have you taken any iodine supplements in the past
six months?
1=yes; 2=no;
99= don’t know |__|__|
5.7. Have you taken any folic acid tablets in the past six
months?
1=yes; 2=no;
99= don’t know |__|__|
5.8. Have you eaten or drunk the following since this
time yesterday?
1=yes; 2=no;
5.8.1. Foods made from grains: Wheat, barley, buckwheat, oats, maize,
rice, sorghum, wheat flour, rye flour,
other flour, bread, rice pasta, biscuit
|__|
5.8.2. White roots and tubers: Potatoes, turnip (red, yellow, white),
radish (red, green) or other roots or
tubers
|__|
5.8.3. Pulses: Beans, peas, lentils |__|
5.8.4. Milk and milk products: Milk or milk products |__|
5.8.5. Meat, poultry: Meat, liver, kidney, chicken. |__|
5.8.6. Fish: Fish (fresh, frozen, canned, smoked,
dried), caviar
5.8.7. Eggs: Eggs |__|
5.8.8. Vitamin A rich vegetables
roots, tubers and fruits: Yellow or orange coloured vegetables
(pumpkins, carrots, red sweet pepper
(bulgori), squash) or fruits (yellow plums
or apricots)
|__|
5.8.9. Dark green leafy vegetables: Spinach, checkri, rov, roshak, siyoalaf,
bargi salat.
Dill, coriander, mint, parsley, blue
basilica, green garlic, green onion, sorrel
[Consider as DGLV when at least one
tablespoon of these vegetable(s)
consumed per day. Otherwise, go to
5.8.21. point Spices, condiments
|__|
5.8.10. Other vegetables: Other vegetables: Cabbage, cauliflower,
garlic, cucumber, leek, tomato, onion,
eggplant, beetroot, mushrooms fresh
and dried, anzur, green beans, green
pepper
|__|
40
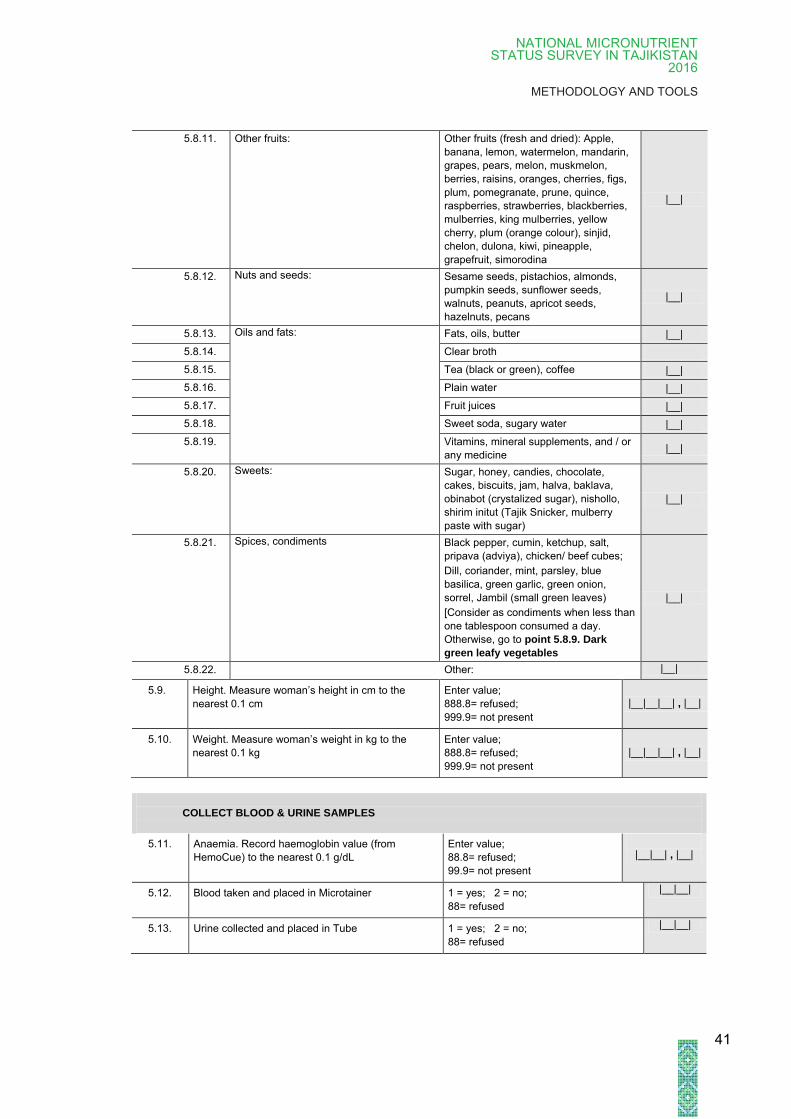
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
5.8.11. Other fruits: Other fruits (fresh and dried): Apple,
banana, lemon, watermelon, mandarin,
grapes, pears, melon, muskmelon,
berries, raisins, oranges, cherries, figs,
plum, pomegranate, prune, quince,
raspberries, strawberries, blackberries,
mulberries, king mulberries, yellow
cherry, plum (orange colour), sinjid,
chelon, dulona, kiwi, pineapple,
grapefruit, simorodina
|__|
5.8.12. Nuts and seeds: Sesame seeds, pistachios, almonds,
pumpkin seeds, sunflower seeds,
walnuts, peanuts, apricot seeds,
hazelnuts, pecans
|__|
5.8.13. Oils and fats: Fats, oils, butter |__|
5.8.14. Clear broth
5.8.15. Tea (black or green), coffee |__|
5.8.16. Plain water |__|
5.8.17. Fruit juices |__|
5.8.18. Sweet soda, sugary water |__|
5.8.19. Vitamins, mineral supplements, and / or
any medicine |__|
5.8.20. Sweets: Sugar, honey, candies, chocolate,
cakes, biscuits, jam, halva, baklava,
obinabot (crystalized sugar), nishollo,
shirim initut (Tajik Snicker, mulberry
paste with sugar)
|__|
5.8.21. Spices, condiments Black pepper, cumin, ketchup, salt,
pripava (adviya), chicken/ beef cubes;
Dill, coriander, mint, parsley, blue
basilica, green garlic, green onion,
sorrel, Jambil (small green leaves)
[Consider as condiments when less than
one tablespoon consumed a day.
Otherwise, go to point 5.8.9. Dark
green leafy vegetables
|__|
5.8.22. Other: |__|
5.9. Height. Measure woman’s height in cm to the
nearest 0.1 cm
Enter value;
888.8= refused;
999.9= not present
|__|__|__| , |__|
5.10. Weight. Measure woman’s weight in kg to the
nearest 0.1 kg
Enter value;
888.8= refused;
999.9= not present
|__|__|__| , |__|
COLLECT BLOOD & URINE SAMPLES
5.11. Anaemia. Record haemoglobin value (from
HemoCue) to the nearest 0.1 g/dL
Enter value;
88.8= refused;
99.9= not present
|__|__| , |__|
5.12. Blood taken and placed in Microtainer 1 = yes; 2 = no;
88= refused
|__|__|
5.13. Urine collected and placed in Tube 1 = yes; 2 = no;
88= refused
|__|__|
41
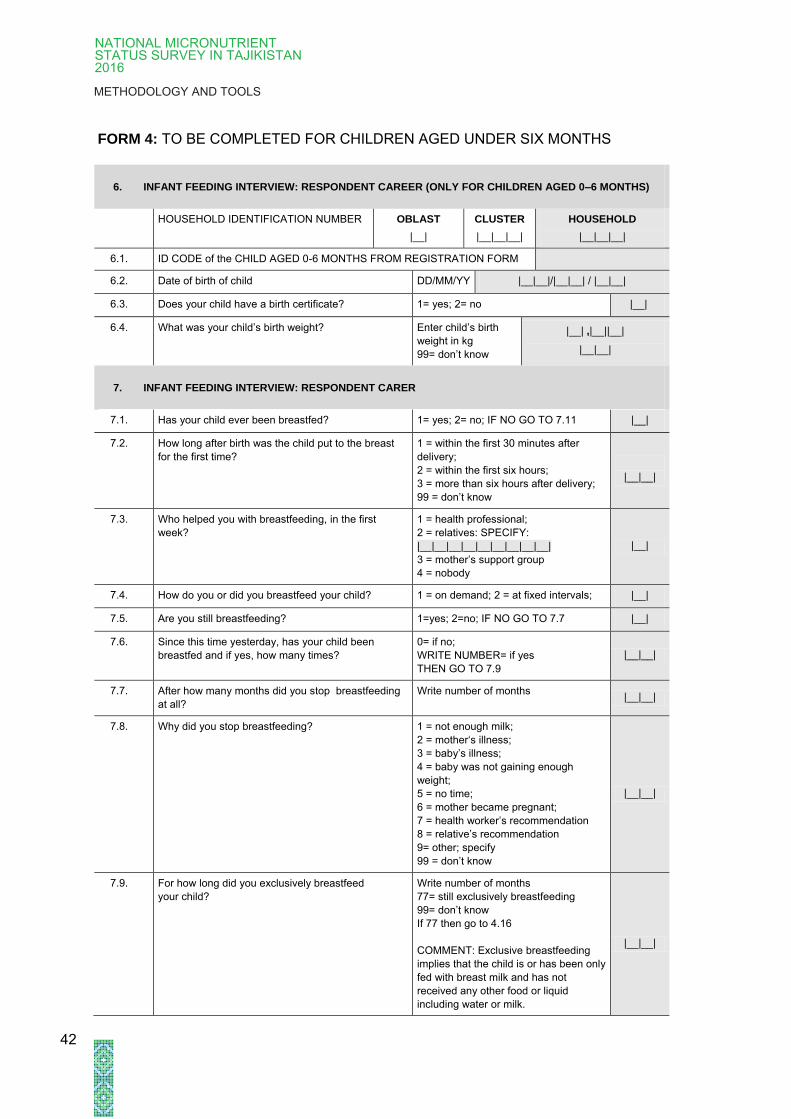
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
FORM 4: TO BE COMPLETED FOR CHILDREN AGED UNDER SIX MONTHS
6. INFANT FEEDING INTERVIEW: RESPONDENT CAREER (ONLY FOR CHILDREN AGED 0–6 MONTHS)
HOUSEHOLD IDENTIFICATION NUMBER OBLAST
|__|
CLUSTER
|__|__|__|
HOUSEHOLD
|__|__|__|
6.1. ID CODE of the CHILD AGED 0-6 MONTHS FROM REGISTRATION FORM
6.2. Date of birth of child DD/MM/YY |__|__|/|__|__| / |__|__|
6.3. Does your child have a birth certificate? 1= yes; 2= no |__|
6.4. What was your child’s birth weight? Enter child’s birth
weight in kg
99= don’t know
|__| ,|__||__|
|__|__|
7. INFANT FEEDING INTERVIEW: RESPONDENT CARER
7.1. Has your child ever been breastfed? 1= yes; 2= no; IF NO GO TO 7.11 |__|
7.2. How long after birth was the child put to the breast
for the first time?
1 = within the first 30 minutes after
delivery;
2 = within the first six hours;
3 = more than six hours after delivery;
99 = don’t know
|__|__|
7.3. Who helped you with breastfeeding, in the first
week?
1 = health professional;
2 = relatives: SPECIFY:
|__|__|__|__|__|__|__|__|__|
3 = mother’s support group
4 = nobody
|__|
7.4. How do you or did you breastfeed your child? 1 = on demand; 2 = at fixed intervals; |__|
7.5. Are you still breastfeeding? 1=yes; 2=no; IF NO GO TO 7.7 |__|
7.6. Since this time yesterday, has your child been
breastfed and if yes, how many times?
0= if no;
WRITE NUMBER= if yes
THEN GO TO 7.9
|__|__|
7.7. After how many months did you stop breastfeeding
at all?
Write number of months
|__|__|
7.8. Why did you stop breastfeeding? 1 = not enough milk;
2 = mother‘s illness;
3 = baby’s illness;
4 = baby was not gaining enough
weight;
5 = no time;
6 = mother became pregnant;
7 = health worker’s recommendation
8 = relative’s recommendation
9= other; specify
99 = don’t know
|__|__|
7.9. For how long did you exclusively breastfeed
your child?
Write number of months
77= still exclusively breastfeeding
99= don’t know
If 77 then go to 4.16
COMMENT: Exclusive breastfeeding
implies that the child is or has been only
fed with breast milk and has not
received any other food or liquid
including water or milk.
|__|__|
42

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
7.10. How old was your child the first time you fed him/her
with water or cow’s milk?
Write number of months
77= the child has never received water
or cow’s milk
99= don’t know
|__|__|
7.11. How old was your child the first time you fed him/her
with the following food or liquids?
READ POSSIBLE ANSWERS
Write age in months
Write 0. If it has not been given yet
|__|__|
7.11.1. Foods made from grains: Wheat, barley, buckwheat, oats, maize,
rice, sorghum, wheat flour, rye flour,
other flour, bread, rice pasta, biscuit
|__|__|
7.11.2. White roots and tubers: Potatoes, turnip (red, yellow, white),
radish (red, green) or other roots or
tubers
|__|__|
7.11.3. Pulses: Beans, peas, lentils |__|__|
7.11.4. Milk and milk products: Milk or milk products |__|__|
7.11.5. Meat, poultry: Meat, liver, kidney, chicken. |__|__|
7.11.6. Fish: Fish (fresh, frozen, canned, smoked,
dried), caviar |__|__|
7.11.7. Eggs: Eggs |__|__|
7.11.8. Vitamin A rich vegetables
roots, tubers and fruits:
Yellow or orange coloured vegetables
(pumpkins, carrots, red sweet pepper
(bulgori), squash) or fruits (yellow plums
or apricots)
|__|__|
7.11.9. Dark green leafy vegetables: Spinach, checkri, rov, roshak, siyoalaf,
bargi salat.
Dill, coriander, mint, parsley, blue
basilica, green garlic, green onion,
sorrel [Consider as DGLV when at least
one tablespoon of these vegetable(s)
consumed per day. Otherwise, go to
point 7.11.23. Spices, condiments
|__|__|
7.11.10. Other vegetables: Other vegetables: Cabbage,
cauliflower, garlic, cucumber, leek,
tomato, onion, eggplant, beetroot,
mushrooms fresh and dried, anzur,
green beans, green pepper
|__|__|
7.11.11. Other fruits: Other fruits (fresh and dried): Apple,
banana, lemon, watermelon, mandarin,
grapes, pears, melon, muskmelon,
berries, raisins, oranges, cherries, figs,
plum, pomegranate, prune, quince,
raspberries, strawberries, blackberries,
mulberries, king mulberries, yellow
cherry, plum (orange-color), sinjid,
chelon, dulona, kiwi, pineapple,
grapefruit, simorodina
|__|__|
7.11.12. Nuts and seeds: Sesame seeds, pistachios, almonds,
pumpkin seeds, sunflower seeds,
walnuts, peanuts, apricot seeds,
hazelnuts, pecans
|__|__|
7.11.13. Oils and fats: Fats, oils, butter |__|__|
7.11.14. Clear broth
7.11.15. Tea (black or green), coffee |__|__|
7.11.16. Plain water |__|__|
7.11.17. Fruit juices |__|__|
7.11.18. Sweet soda, sugary water |__|__|
7.11.19. Infant formula |__|__|
7.11.20. Vitamins, mineral supplements, and / or
any medicine |__|__|
43
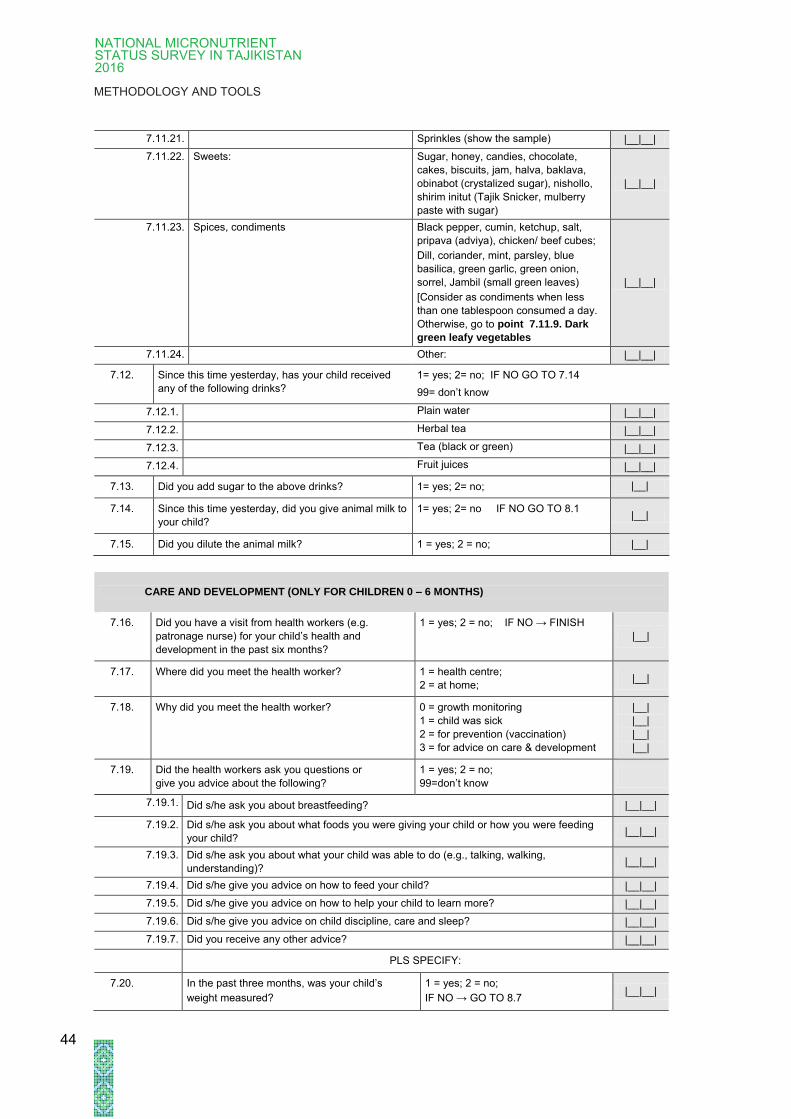
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
7.11.21. Sprinkles (show the sample) |__|__|
7.11.22. Sweets: Sugar, honey, candies, chocolate,
cakes, biscuits, jam, halva, baklava,
obinabot (crystalized sugar), nishollo,
shirim initut (Tajik Snicker, mulberry
paste with sugar)
|__|__|
7.11.23. Spices, condiments Black pepper, cumin, ketchup, salt,
pripava (adviya), chicken/ beef cubes;
Dill, coriander, mint, parsley, blue
basilica, green garlic, green onion,
sorrel, Jambil (small green leaves)
[Consider as condiments when less
than one tablespoon consumed a day.
Otherwise, go to point 7.11.9. Dark
green leafy vegetables
|__|__|
7.11.24. Other: |__|__|
7.12. Since this time yesterday, has your child received
any of the following drinks?
1= yes; 2= no; IF NO GO TO 7.14
99= don’t know
7.12.1. Plain water |__|__|
7.12.2. Herbal tea |__|__|
7.12.3. Tea (black or green) |__|__|
7.12.4. Fruit juices |__|__|
7.13. Did you add sugar to the above drinks? 1= yes; 2= no; |__|
7.14. Since this time yesterday, did you give animal milk to
your child?
1= yes; 2= no IF NO GO TO 8.1 |__|
7.15. Did you dilute the animal milk? 1 = yes; 2 = no; |__|
CARE AND DEVELOPMENT (ONLY FOR CHILDREN 0 – 6 MONTHS)
7.16. Did you have a visit from health workers (e.g.
patronage nurse) for your child’s health and
development in the past six months?
1 = yes; 2 = no; IF NO → FINISH
|__|
7.17. Where did you meet the health worker? 1 = health centre;
2 = at home; |__|
7.18. Why did you meet the health worker? 0 = growth monitoring
1 = child was sick
2 = for prevention (vaccination)
3 = for advice on care & development
|__|
|__|
|__|
|__|
7.19. Did the health workers ask you questions or
give you advice about the following?
1 = yes; 2 = no;
99=don’t know
7.19.1. Did s/he ask you about breastfeeding? |__|__|
7.19.2. Did s/he ask you about what foods you were giving your child or how you were feeding
your child? |__|__|
7.19.3. Did s/he ask you about what your child was able to do (e.g., talking, walking,
understanding)? |__|__|
7.19.4. Did s/he give you advice on how to feed your child? |__|__|
7.19.5. Did s/he give you advice on how to help your child to learn more? |__|__|
7.19.6. Did s/he give you advice on child discipline, care and sleep? |__|__|
7.19.7. Did you receive any other advice? |__|__|
PLS SPECIFY:
7.20. In the past three months, was your child’s
weight measured?
1 = yes; 2 = no;
IF NO → GO TO 8.7 |__|__|
44

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
7.21. How many times was your child’s weight
measured in the past three months?
PLEASE ENTER NUMBER OF TIMES |__|__|
7.22. In the past three months, was your child’s height
measured?
1 = yes; 2 = no;
IF NO → FINISH |__|__|
7.23. How many times was your child’s height
measured in the past three months?
PLEASE ENTER NUMBER OF TIMES |__|__|
7.24. Did you receive counseling after measurement
of weight or height?
1 = yes; 2 = no |__|__|
CHILD ANTROPOMETRICS AND LABORATORY
7.25. Height. Measure child’s height in cm to the
nearest 0.1 cm
Enter value;
888.8= refused;
999.9= not present
|__|__|__| , |__|
7.26. Weight. Measure child’s weight in kg to the
nearest 0.1 kg
Enter value;
888.8= refused;
999.9= not present
|__|__|__| , |__|
45

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Annex 4:
Participant information and informed consent
Annex 4.1
Participant information and informed consent - Women
Title of study: National Micronutrient Status Survey 2016 Tajikistan
Institutions involved: UNICEF Tajikistan, Ministry of Health and Social Protection of the
Republic of Tajikistan (including the Paediatric and Child Surgery
Scientific and Research Institute and the Research Laboratory of
Preventive Medicine of the Republic of Tajikistan), Swiss Tropical
and Public Health Institute.
The number identifying this study is No. [to be determined] (approval letter from MoHSP
Tajikistan).
Why are we giving you this form?
We are giving you this form to provide you information about this research study. After you have
learned more about the study, you can decide if you would like to participate.
Who can participate?
Children aged 0-59 months with their carers and non-pregnant, non-lactating women of
reproductive age (15-49 years).
Purpose of this research study.
Malnutrition among children and women remains a major challenge for Tajikistan. With this
survey we aim to assess the nutritional and micronutrient status of children and women,
determine risk factors for deficiencies and determine possible strategies to improve the general
nutrition situation in Tajikistan. Therefore, we are conducting this study.
We will evaluate the severity of micronutrient deficiencies among children between six and 59
months and non-pregnant women of child-bearing age (18-49 years) in all five geographical
areas of Tajikistan (Khatlon Oblast, the Rayons of Republic Subordination (RRS), Sughd
Oblast, Gorno-Badakhshan Autonomous Oblast (GBAO), and Dushanbe) such as iron, iodine
and vitamin deficiencies. We expect that more than 4,000 persons will participate in the study.
46

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Procedures
If you decide to participate in this study, the following procedures will be followed:
1 We will ask you some questions about your household situation and food security and
your nutrition.
2 We will then measure your weight and height.
3 We will then collect one urine sample from you to examine the level of iodine excretion.
4 An experienced clinician will take 10 drops of blood (0.4 ml) from a finger prick.
We will assess and tell you directly your haemoglobin level. The other analysis will be done in a
laboratory in Dushanbe. In addition, we will examine the salt you commonly use for cooking for
iodine content. The interview and sample collection will last about 20 minutes.
Possible Risks and Discomforts
You may feel some local pain during the blood collection. This will not cause any risk. The urine
provided by you in plastic cups will not cause any risk.
Benefits
Your participation in this study may contribute to benefits for the health of the population in
Tajikistan. It improves understanding of the severity of national micronutrient nutrition
deficiency. UNICEF can initiate activities at national level to reduce the burden of this
deficiency.
If we suspect any anaemia-related deficiencies we will inform you and – if needed – provide you
with required supplements or direct you further. We will immediately give you an answer about
the iodine content of your salt.
Confidentiality voluntary participation
Your participation in the survey is entirely voluntary and will not be compensated for. Our study
has been examined and approved by the Ministry of Health and Social Protection of the
Republic of Tajikistan and the ethics commission in Switzerland. If you agree to participate in
this study the study team will follow the procedures outlined above.
Information from you and your data will of course be treated confidentially. The results will only
be evaluated and represented anonymously. Data will be coded before analysis. Coded means
that your name will not appear anywhere and that your identity will be replaced by an
identification code so that it will not be possible to link the reports to your person. Only the study
team has access to your data. In addition, experts from relevant authorities can have access to
your data for test and control purposes. You can stop the interview and participation at any time
and without giving reasons, or you may withdraw completely from the study. Data and biological
samples collected before your withdrawal may be used for analysis. The collected data may
also be used for further investigations.
If you do not participate in the survey, decide not to complete the interview, decide not to give
biological samples or withdraw completely from the survey, you will not be disadvantaged in any
way.
If you have any questions or concerns, please talk to the study team visiting you today. If you
have any questions about the study after they leave, you can contact our in-country coordinator
at + [to be determined] or your provincial health director.
We would very much appreciate your support and participation in our study.
47
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Title of Study: National Micronutrient Status Survey
• I have been informed about the goals of the study.
• I have read and understand the information provided.
• I know that my personal data will remain confidential and will
only be used in a coded form for research purposes, and that
links to my person will not be possible from the reports.
• I am participating in this study voluntarily. I may revoke my
consent to participate at any time and without giving any
reasons.
• I understand that data and biological samples collected from
me before my withdrawal may be used for analysis.
Name (please print)
Place, Date
Signature
In case of minor participants (15-18 years) please obtain consent from carer in
addition to participant’s consent.
Name (please print)
Place, Date Signature of adult carer (if target person is 15-18
years)
48

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Annex 4.2
Participant information and informed consent – Children
Title of study: National Micronutrient Status Survey 2016 Tajikistan
Institutions involved: UNICEF/Tajikistan, Ministry of Health and Social Protection of the
Republic of Tajikistan (including the Scientific and Research Institute
of Pediatric and Child Surgery, Research Laboratory of Preventive
Medicine of the Republic of Tajikistan), Swiss Tropical and Public
Health Institute/Switzerland.
The number identifying this study is No. [to be determined] (approval letter from MoH
Tajikistan).
Why are we giving you this form?
We are giving you this form to provide you with information about this research study. After you
have learned more about the study, you can decide if you as a carer would like the child to
participate.
Who can participate?
Children aged 0-59 months with their carers and non-pregnant, non-lactating women of
reproductive age (15-49 years).
Purpose of this research study
Malnutrition among children and women remains a major challenge for Tajikistan. With this
survey we aim to assess the nutrition and micronutrient status of children and women,
determine risk factors for deficiencies and determine possible strategies to improve the general
nutrition situation in Tajikistan. Therefore, we are conducting this study.
We will evaluate the severity of micronutrient deficiency among children aged between six and
59 months and non-pregnant women of child-bearing age (18-49 years) in all five geographical
areas of Tajikistan (Khatlon Oblast, Rayons of Republic Subordination (RRS), Sughd Oblast,
Gorno-Badakhshan Autonomous Oblast (GBAO), and Dushanbe) such as iron, iodine or vitamin
deficiencies. We expect that more than 4,000 persons will participate in the study.
Procedures
If you agree for the child (aged 6-59 months) to participate in this study the following procedures
will be applied:
1 We will ask you some questions about the household situation, food security, child
health, health seeking for child health, infant feeding and the child’s nutrition.
2 We will measure the child’s weight, height and mid-upper arm circumference.
3 We will then collect one urine sample from the child to examine the level of iodine
excretion. If possible, we will take it from the traditional cradle (Gavora).
4 An experienced clinician will take 10 drops (0.4 ml) of blood from a finger prick of the
child.
49

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
We will assess and tell you directly the child’s haemoglobin level. Other analysis will be done in
a laboratory in Dushanbe. In addition, we will examine the salt you commonly use for cooking
for iodine content. The interview and sample collection will last about 30 minutes.
If you have a child under the age of six months we would also like to include him/her in the
study but only ask about feeding practices and measure the weight and height. The questioning
and measurements should not take more than 10 minutes. If you agree that the child (aged 0-6
months) can participate in this study the following procedures will be applied:
1 We will ask you some questions about infant feeding practices of the child
2 We will measure the weight and height of the child.
Possible Risks and Discomforts
The child may feel some local pain during the blood collection. This will not cause any risk. The
urine provided by the child in plastic cups will not cause any risk and can alternatively be
sampled from the traditional cradle (Gavora).
Benefits
Your and the child’s participation in this study may contribute to benefits to the health of the
population in Tajikistan. It improves understanding of the severity of national micronutrient
nutrition deficiency. UNICEF can initiate activities at national level to reduce the burden of this
deficiency.
If we suspect any anaemia-related deficiencies in the child we will inform you and – if needed –
provide you with required supplements for the child or direct you further. We will immediately
inform you about the iodine content of your salt.
Confidentiality voluntary participation
Your and the child’s participation in the survey is entirely voluntary and will not be compensated
for. Our study has been examined and approved by the Ministry of Health and Social Protection
of the Republic of Tajikistan and the ethics commission in Switzerland. If you agree that your
child and you participate in this study the study team will follow the procedures outlined above.
Of course, information and data from you and the child will be treated confidentially. Results will
only be evaluated and represented anonymously. Data will be coded before analysis. Coded
means that your name or the name of the child will not appear anywhere and that your and the
child’s identity will be replaced by an identification code. It will not be possible to link the reports
to your person or the child. Only the study team has access to the data. In addition, experts
from relevant authorities can have access to the data for test and control purposes. You can
stop the interview and the participation of your child at any time and without giving reasons, or
you may withdraw completely from the study. Data and biological samples collected from you or
the child before your withdrawal may be used for analysis. The data collected may also be used
for further investigations.
If you do not agree for the child to participate in the survey, decide not to complete the
interview, decide not to give biological samples from the child or withdraw completely from the
survey, no disadvantages will arise for you or your child.
If you have any questions or concerns, please talk to the study team visiting you today. If you
have any questions about the study after they leave, you can contact our in-country coordinator
at + [phone to be determined] or your provincial health director.
We would very much appreciate your support and participation in our study.
50
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Written declaration of consent to participate in the National Micronutrient Status Survey
Tajikistan 2016
Title of Study: National Micronutrient Status Survey
• I have been informed about the goals of the study.
• I have read and understand the information provided.
• I know that my personal data and the data of the child will
remain confidential and will only be used in a coded form for
research purposes, and that links to my person or the child
will not be possible from the reports.
• I and my child participate in this study voluntarily. I may revoke
my consent to participate at any time and without giving any
reasons.
• I understand that data and biological samples collected from
me and the child prior to withdrawal may be used for analysis.
Name of child (please print)
Relation of carer to child
Name of carer (please print)
Place, Date
Signature of carer
51

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Annex 5:
Roles of participating institutions and field team
members
Ministry of Health and Social Protection (MoHSP)
• Initiated the study and required the information to plan interventions
• Supported and facilitated the study administratively
• Oversaw the study as a whole, including field procedures
UNICEF
• Acted as Principal Investigator
• Contributed to planning the study and had managerial oversight.
• Provided all necessary logistical support for the field work
• Conducted unannounced visits to the field and conducted quality assessments
Paediatric Research Institute / Field supervisor:
• The Paediatric Research Institute (PRI) oversaw and managed the 12 field teams and was
responsible for logistics and organizing the fieldwork. The contact person at the PRI acted
as field supervisor and national coordinator.
• The field supervisor ensured that the field teams arrived and conducted fieldwork each day
at the assigned villages.
• The field supervisor was the first line of contact for the heads of each field team and for the
quality control manager from the Swiss Tropical and Public Health Institute (Swiss TPH).
• The PRI appointed additional field supervisors for field monitoring, who conducted
unannounced visits to the field.
Swiss Tropical and Public Health Institute (Swiss TPH) / Quality supervisors
• The Swiss TPH quality control manager and dedicated national supervisors performed
unannounced visits throughout the data collection period.
• Additional quality control measures included quality checks of the electronic data and on
the collection, storage and transport of blood and urine samples. The quality
measures also included field progress monitoring.
Logistics company
• Was responsible for smooth logistics of the field operations.
• Assured the timely transport of field teams and blood and urine samples according to the
schedule defined for field data collection.
52

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Field teams
• 12 field teams, of four people each, conducted data and blood and urine sample collection.
All teams were composed of:
one clinician (the head of team),
one interviewer for the face-to-face interviews,
one laboratory technician in charge of the biological sampling, and
one driver (from logistics company).
• Each team collected information from 12 children (6-59 months) and 12 women (15-49
years) every day.
53

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
Annex 6:
Fieldwork procedures
Annex 6.1:
Overview of daily schedule and activities
I. BEFORE FIELD WORK
1. STEP PREPARING FIELD WORK FOR NEXT DAY: The field supervisor and the team leader were
responsible for verifying the availability of all items and supplies required to conduct the
fieldwork.
2. STEP TRANSPORTATION OF FIELD TEAMS: The head of the team arranged transport to the
villages or mahallas and or household with the logistics company, according to the defined
fieldwork plan.
II. DURING DATA COLLECTION IN THE FIELD
3. STEP REPORTING INITIATION OF FIELD WORK: Once the FIELD TEAM was in the village, the
head of the field team contacted the field supervisor by phone and reported on the time of
arrival.
4. STEP REPORTING TO JAMOAT: Before starting work in a given village, the head of the team
informed the head of the Jamoat (village) of the objectives of the survey.
5. STEP SELECTING/IDENTIFYING HOUSEHOLDS: FIELD TEAMS began identifying and confirming
households following the established protocol
6. STEP VERIFYING THE INCLUSION CRITERIA FOR EACH HOUSEHOLD: The team verified the
inclusion criteria for including households in the survey. If the household did not fulfil the
criteria, then the team continued to the next household in the list and verify again the inclusion
criteria.
7. STEP PARTICIPATION OF HOUSEHOLD: The interviewer asked for oral consent to participate in the
survey. If the head of the household DID NOT CONSENT to participate, then the team
identified the next household in the list. If oral consent was provided then the team continued
with the next steps.
8. STEP FILLING OUT REGISTRATION FORM: The interviewer filled in the REGISTRATION FORM
and prepared the labelling stickers for the blood and urine samples.
9. STEP ENSURING INFORMED CONSENT: The interviewer explained the INFORMED CONSENT,
allowed the participant to read the informed consent, answered questions from the participants
and asked the participants to sign the informed consent form.
10. STEP CONDUCTING INTERVIEW: The interviewer conducted the questionnaire following the
recommendations and steps described in the manual.
11. STEP TAKING ANTHROPOMETRIC MEASURES: The clinician measured height, weight and mid-
upper arm circumference (MUAC) in children aged 6-59 months, and height and weight in
children 6-59 months and women (15-49 years).
12. STEP MEASURING IODINE IN SALT: The laboratory technician collected and measured the iodine
content in salt using the Rapid Test Kid.
13. STEP COLLECTING, LABELLING AND STORING BIOLOGICAL AND SALT SAMPLES: The
clinician, in collaboration with the laboratory technician, collected and labelled the blood and
urine samples. The urine samples were transported in labelled transport tubes and fully sealed.
Both blood and urine samples were labelled and immediately placed into cooling boxes until
further processing at the regional laboratory. Salt samples were packed and labelled according
to protocol.
54
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
14. STEP VERIFYING THE INFORMATION: All the team members verified that all the information was
completed and ensured that all blood, urine and salt samples were correctly labelled
15. STEP HEALTH RECOMMENDATIONS AND REFERRALS: The clinician provided health
recommendations or referrals to health centres in specific cases.
16. STEP THANKING PARTICIPANTS: The field team thanked the participant(s) for participating in the
survey.
STEPS 3-16 WERE REPEATED UNTIL THE NUMBER OF PARTICIPANTS WAS REACHED: The field team
identified the next household in the village and repeated the procedure above until information was
obtained about 12 children (6-59 months) and 12 women (15 -49 years)
III. AFTER DATA COLLECTION IN THE FIELD (SAME DAY)
17. STEP TRANSPORTING, CENTRIFUGING AND STORING SAMPLES: The blood samples were
transferred in a cooling box to the regional laboratory to be centrifuged and separated and the
serum transferred into the correctly labelled storage tube. Urine samples were transported in
labelled transport tubes. All samples were transported in cooling boxes to Dushanbe within
specific dates. Biological waste was disposed of appropriately and according to protocol in
laboratories or health centres. The Head of Team reports to the Field Supervisor once this step
was completed.
18. STEP PREPARING FIELD WORK FOR NEXT DAY: The head of the team and the FIELD TEAM
verified the PROCUREMENT CHECKLIST for the next day (including freezing ice packs and
charging tablets).
Annex 6.2:
Detailed explanation of activities
Before field work
Step 1 - PREPARING FIELD WORK FOR NEXT DAY
• The procurement checklist was gone through the day before and confirmed every
morning by the field team members.
• The field supervisor and the head of the team ensured the availability of all items and
supplies required to conduct the fieldwork.
• Before starting the fieldwork, the teams ensured that tablets and mobiles phones were
fully charged. Similarly ice packs were frozen and copies of all the documents required
were made available.
• Ensuring the availability of required supplies was critical to ensure successful fieldwork and
to avoid delays that could put field data collection at risk.
Step 2 - TRANSPORTATION OF FIELD TEAMS
• The head of the team arranged transportation to the villages or mahallas with the logistics
company, according to the defined fieldwork plan.
During data collection in the field
Step 3 - REPORT INITIATION OF FIELD WORK
• Once the field teams arrived in the village, the heads of the team contacted the Field Supervisor by phone and reported on the time of arrival.
• The Field Supervisor was immediately informed of any problems or delays faced by the field teams during the fieldwork.
55
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
REPORTING TO JAMOAT
• Before starting fieldwork, the Head of Team informed the head of the Jamoat (village) about
the objectives of the survey and showed the authorization from the Ministry of Health and
Social Protection (MoHSP).
• Each field team always carried the authorization letter from the MoHSP.
SELECTION/IDENTIFICATION OF HOUSEHOLDS
• The interviewer was responsible for the identification of households
• Definition of household
A household was defined as all individuals who acknowledge the authority of one
household head and permanently live in the dwelling
• The National Micronutrient Status Survey Tajikistan 2016 had two mechanisms to identify
households in the villages:
a. Villages where a list of 20 households was already available.
b. Villages where no household list was available
a. Villages where a list of 20 households was already available
• In these cases, a list of specific households indicating the village, the name and
address of household and the GPS coordinates (when available), were given to the
field teams.
• The field team were expected to locate the exact households indicated in the
household list.
• If the household was not located, did not fulfil the inclusion criteria or the head
or participants of the household refused to participate in the survey, then the
next household on the list was sought.
• To identify the exact household, the head of the team asked for support from a
member of the local Jamoat or used GPS if equipment and the GPS location were
available
• If household lists were available, the National Micronutrient Status Survey
Tajikistan 2016 and the WASH survey covered the same village and households.
b. Villages where no household list was available
• In these cases, only the village names were given to the field teams
• To identify households the head of the team contacted the Jamoats for the list of
households included in the local census.
• The field teams chose the households randomly, as follows:
20 households were selected per cluster.
The field team located the exact households as they were selected.
If the household was not located, did not fulfill the inclusion criteria or the
head or participants in the household refused to participate in the survey,
then the next household was sought.
56
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
To identify the exact household, the head of the team asked for support from
a member of the local Jamoat
• This meant that the Tajik National Micronutrient Status Survey 2016 identified and
surveyed villages and households that were not included in the WASH survey.
• The field plan clearly specified if the villages had a household list available
(sampling a) or if households need to be selected from the Jamoat list (sampling
b).
VERIFYING THE INCLUSION CRITERIA FOR HOUSEHOLDS
• The interviewer contacted the head of the household and presented him/herself and made a
short presentation of the survey. The short presentation of the survey included the following
information:
• This Micronutrient Status survey is conducted by UNICEF and MOHSP
• The purpose of the survey is to evaluate the nutrition status among children
and women and your participation in the survey will be very important in order
to provide information representing all people of the Republic
• Households were selected at random
• There is no connection between this survey and taxes or any other
government services or data base
• All information is strictly confidential.
• Afterwards, the interviewer verified the criteria for the inclusion of household in the survey.
Inclusion criteria for households
• The household has at least 1 non-pregnant non-lactating woman 15-49 years
AND/OR at least 1 child 6 to 59 months
• Non-pregnant non-lactating women are available AND/OR a carer of child(ren)
6 to 59 months and child(ren) available
• At least one non-pregnant non-lactating woman (15-49) or carer of a child (6-59
months) has signed an informed consent form
A household was excluded if any of the above mentioned inclusion criteria were
not met
• If the household did not fulfil any of the inclusion criteria, then the field teams continued
to the next household in the list until they found a household that fulfilled the criteria.
• If the household fulfilled the inclusion criteria then the team entered the household.
IMPORTANT: The field teams entered the households together and remained in the
household together until all eligible participants had been questioned and all biological
samples collected.
57
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
PARTICIPATION OF HOUSEHOLD MEMBERS
• Any household members who were eligible and lived in the household could be enrolled in
the survey.
• The interviewer provided information on the survey to all eligible and available non-
pregnant, non-lactating women (15-49 years) or carers of children aged 6-59 months. For
this purpose the interviewer handed over the information letter.
• The interviewer asked if the respondent has any questions regarding the survey or his/her
participation.
• If, after sufficient information was provided, any of the non-pregnant non-lactating women
(15-49) or the carers of children (6-59 months) did not consent to participate, then the
team stopped the procedure and identified the next household in the list.
• If after providing sufficient information, any of the non-pregnant non-lactating women (15-
49) or the caretakers of children (6-59 months) did consent to participate, then the team
continued with the registration form.
COMPLETING REGISTRATION FORM
• All household members eligible for participation were registered.
• For household members who lived and worked abroad, the following applied: if the
household member had lived in the household for at least three months in the previous 12
months she was also listed as a household member. Visitors (such as daughters and
grandchildren who normally lived with husbands and parents-in-law) were only included if
they had permanently lived in this household later than March 2016.
• The three sections of the registration form of households were completed on paper:
1 Assessment of eligibility criteria
2 General information on interview situation (date and time)
3 Listing of eligible household members including the assignment of unique anonymising
identifiers
• To identify all household members that needed to be included, the interviewers (1) asked
for the household head and (2) counted and listed all non-pregnant, non-lactating women
(15-49 years) or children (6-59 months) that permanently lived in the dwelling. If children
aged under six months were also living in the household they were also listed.
• Labels for salt, blood and urine samples were identified and prepared.
COMPLETING INFORMED CONSENT FORM
• The interviewer ensured that ALL respondents (non-pregnant non-lactating women aged
15-49 years or carers of children aged 0-59 months) agreed and signed the informed
consent form (Annex 4).
• The need for informed consent was explained and the respondents assured that their
identities and responses would be fully confidential.
• The respondents were allowed to read the informed consent forms and answer questions.
• If the respondent(s) agreed to give informed consent, the interviewer filled in the required
information and asked the respondent(s) to sign it. If none of the respondents in the
household agreed to participate in the survey, then the procedure was terminated and the
next household in the list identified.
58
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
• The signed informed consent of the respondent was kept and stored in a folder, and
subsequently handed over to the study team in Dushanbe.
CONDUCTING INTERVIEW
• The survey for micronutrient and nutritional assessment consisted of four forms (see Table
1: the full forms are available as Annex 3).
• Table 1: Survey forms, respondent and content
Form # Respondent Content Instruction
Form 1 To be answered by
carer of child aged 6-
59 months or non-
pregnant women
aged 15-49 years.
Included information on household
characteristics, household food security and
the test for salt iodization and salt sampling.
Fill out Form 1 once per
household
Form 2 To be answered by
carer of child aged 6-
59 months
Included information related to child health
issues: diarrhoea, nutritional habits,
breastfeeding, complementary feeding, care
and development, measure of height,
weight, mid-upper arm circumference and
the collection of blood and urine samples.
Fill out Form 2 for each
eligible child (even if the
mother or carer of the
child is the same)
Form 3 To be answered by
women aged 15-49
years.
Included information related to nutrition
habits, measure of height and weight, and
the collection of blood and urine samples
Fill out Form 3 for each
eligible women
Form 4 To be completed with
career of child aged
under six months.
Included information related to nutrition
habits, breastfeeding, complementary
feeding, care and development, measure of
height and weight.
Fill out Form 4 for each
eligible child (even if the
mother or caretaker of the
child is the same)
• HOUSEHOLD IDENTIFICATION NUMBER AND ID CODE OF PARTICIPANTS
• The team always began with Form 1: Household information (which needed to be fill out
only once per household) and continued in numerical order with the other forms.
• The interviewer completed one Form 2 for every child aged 6-59 months participating in the
survey, starting with the youngest child. Form 2 was filled out for each child even if the carer
was the same person.
• The interviewer then filled out one Form 3 for every woman aged 15-49 years participating,
starting with youngest woman.
• Finally, one Form 4 was completed for every child aged under six months living in the
household, starting with the youngest child.
• The order of questions as presented in the survey was followed.
• All the questions and information required in the survey were obligatory. If the respondent
refused to answer a question, the surveyors made a note at the end of the survey in the
Comments section.
• If the survey was not complete the software displayed an alert message informing the
interviewer that the information was not complete.
• Once the form was finished and saved, the information registered in the survey could not be
modified, so the teams always ensured that the information registered was correct before
finishing a form.
59

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
The following guiding principles for asking questions were observed:
• The interviewer tried, as much as possible, to interview the respondent privately, so as to
prevent other people from interfering in the responses.
• The interviewer spoke in a polite and respectful way so that the respondents were
comfortable answering questions.
• The interviewers were patient and gave the respondents time to answer the questions
without pressurizing them for replies.
• The interviewers asked the question as written. They avoided changing the content of the
question in any way to prevent errors in the responses.
• If the respondents did not understand questions after they were repeated the interviewer
registered an answer option “No” or “Don’t know.
• The interviewer read the question to the respondent, but not the answers (unless instructed
so by the survey form). Answers were not offered to questions even if asked by the
participant.
• The interviewers avoided judging the responses or reacting to them, either negatively or
positively.
MEASURING ANTHROPOMETRIC STATUS1
The clinician, with the collaboration of laboratory technician, performed the anthropometric
measures. The clinician measured:
1 height and weight in women (15 -49 years);
2 height, weight and mid-upper arm circumference (MUAC) in children aged 6-59
months; and
3 height and weight in children aged 0-6 months.
Weighing
• The scales were calibrated using a standard weight every day before starting the field visits.
• When weighing participants, the clinician ensured that the scales were placed on a flat and
even surface.
• The child’s or women’s weight was always measured in kg to the nearest 0.1 kg
• To weigh children under two years, first the mother or carer was weighed alone. After-
wards, the mother or the carer was weighed carrying the baby in her arms as in Figure1.
• For children two years or older: if they stood still, the children were weighed alone(Figure 2). If they did not stand still, the procedure described as for children less than
two years old was used (Figure1).
• Weighing women: The procedure for weighing women is the same as that described for
children aged two or older (Figure 2).
1 All the pictures and recommendations described in this section for weighing and measuring a child were taken from
the World Health Organization Training course on child growth assessment.
60
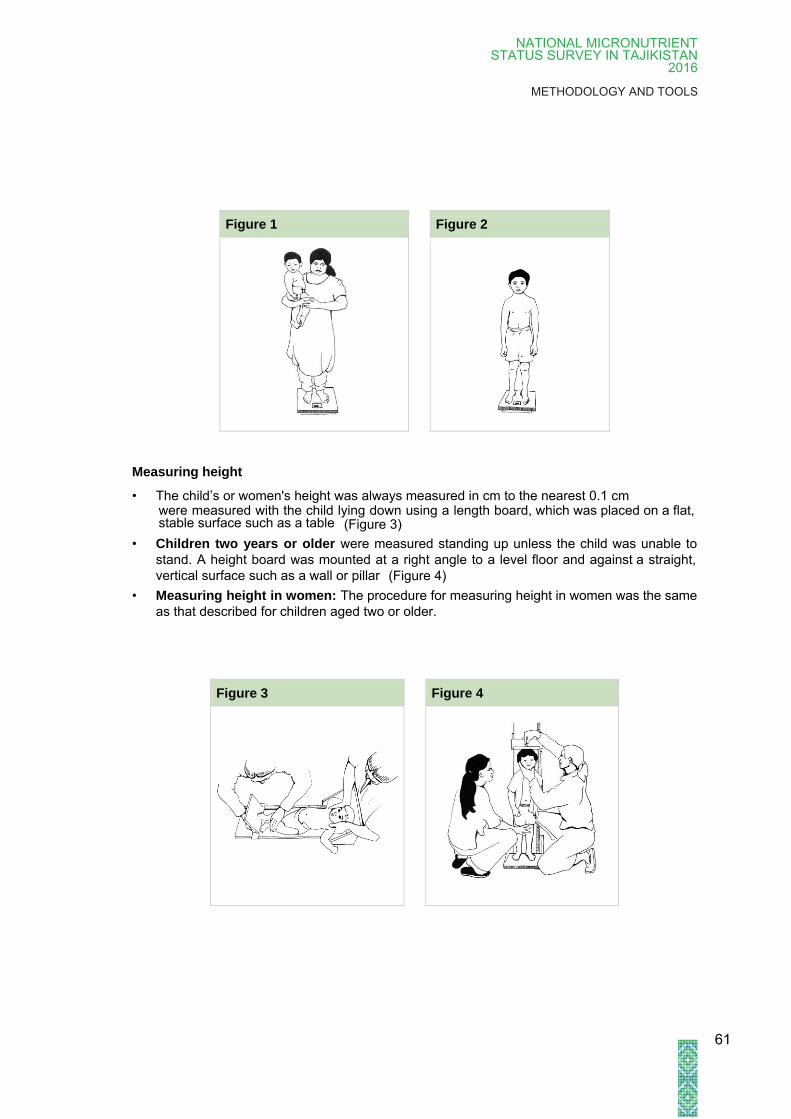
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
Figure 1 Figure 2
Measuring height
• The child’s or women's height was always measured in cm to the nearest 0.1 cm
(Figure 4)
• Children two years or older were measured standing up unless the child was unable to
stand. A height board was mounted at a right angle to a level floor and against a straight,
vertical surface such as a wall or pillar
• Measuring height in women: The procedure for measuring height in women was the same
as that described for children aged two or older.
Figure 3 Figure 4
61
were measured with the child lying down using a length board, which was placed on a flat, stable surface such as a table (Figure 3)
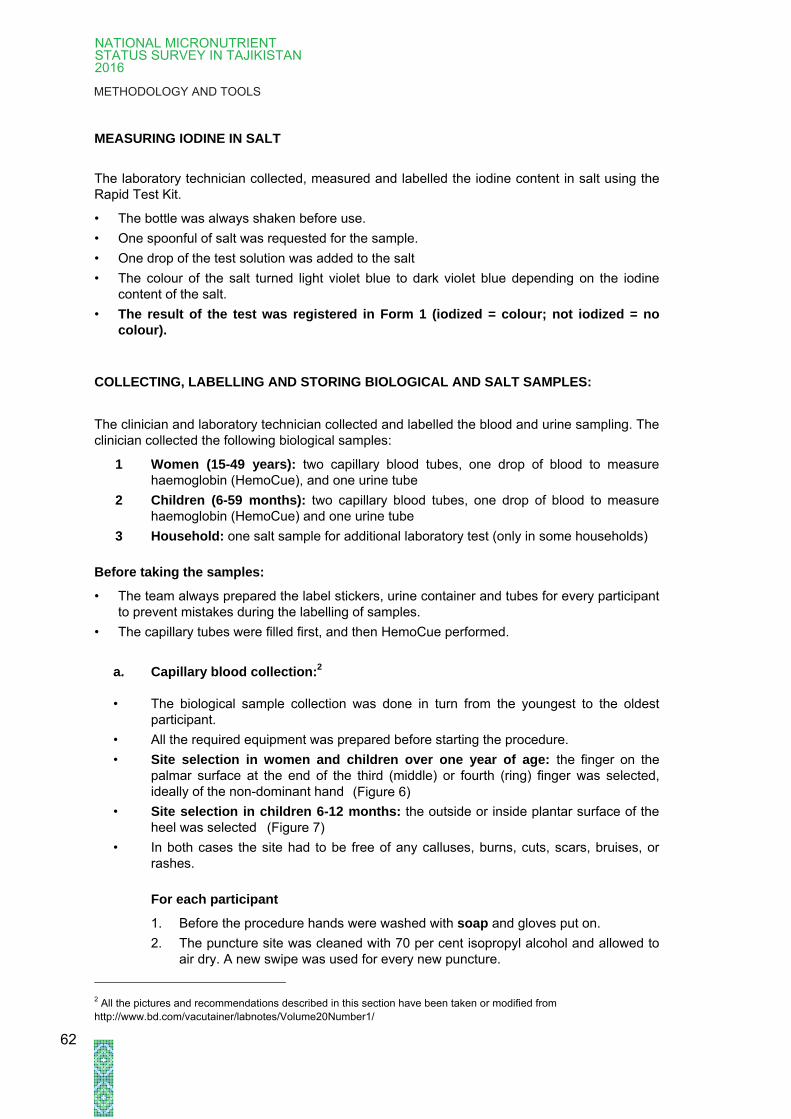
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
MEASURING IODINE IN SALT
The laboratory technician collected, measured and labelled the iodine content in salt using the
Rapid Test Kit.
• The bottle was always shaken before use.
• One spoonful of salt was requested for the sample.
• One drop of the test solution was added to the salt
• The colour of the salt turned light violet blue to dark violet blue depending on the iodine
content of the salt.
• The result of the test was registered in Form 1 (iodized = colour; not iodized = no
colour).
COLLECTING, LABELLING AND STORING BIOLOGICAL AND SALT SAMPLES:
The clinician and laboratory technician collected and labelled the blood and urine sampling. The
clinician collected the following biological samples:
1 Women (15-49 years): two capillary blood tubes, one drop of blood to measure
haemoglobin (HemoCue), and one urine tube
2 Children (6-59 months): two capillary blood tubes, one drop of blood to measure
haemoglobin (HemoCue) and one urine tube
3 Household: one salt sample for additional laboratory test (only in some households)
Before taking the samples:
• The team always prepared the label stickers, urine container and tubes for every participant
to prevent mistakes during the labelling of samples.
• The capillary tubes were filled first, and then HemoCue performed.
a. Capillary blood collection:2
• The biological sample collection was done in turn from the youngest to the oldest
participant.
• All the required equipment was prepared before starting the procedure.
• Site selection in women and children over one year of age: the finger on the
palmar surface at the end of the third (middle) or fourth (ring) finger was selected,
ideally of the non-dominant hand
• Site selection in children 6-12 months: the outside or inside plantar surface of the
heel was selected
• In both cases the site had to be free of any calluses, burns, cuts, scars, bruises, or
rashes.
For each participant
1. Before the procedure hands were washed with soap and gloves put on.
2. The puncture site was cleaned with 70 per cent isopropyl alcohol and allowed to
air dry. A new swipe was used for every new puncture.
2 All the pictures and recommendations described in this section have been taken or modified from
http://www.bd.com/vacutainer/labnotes/Volume20Number1/
62
(Figure 6)
(Figure 7)
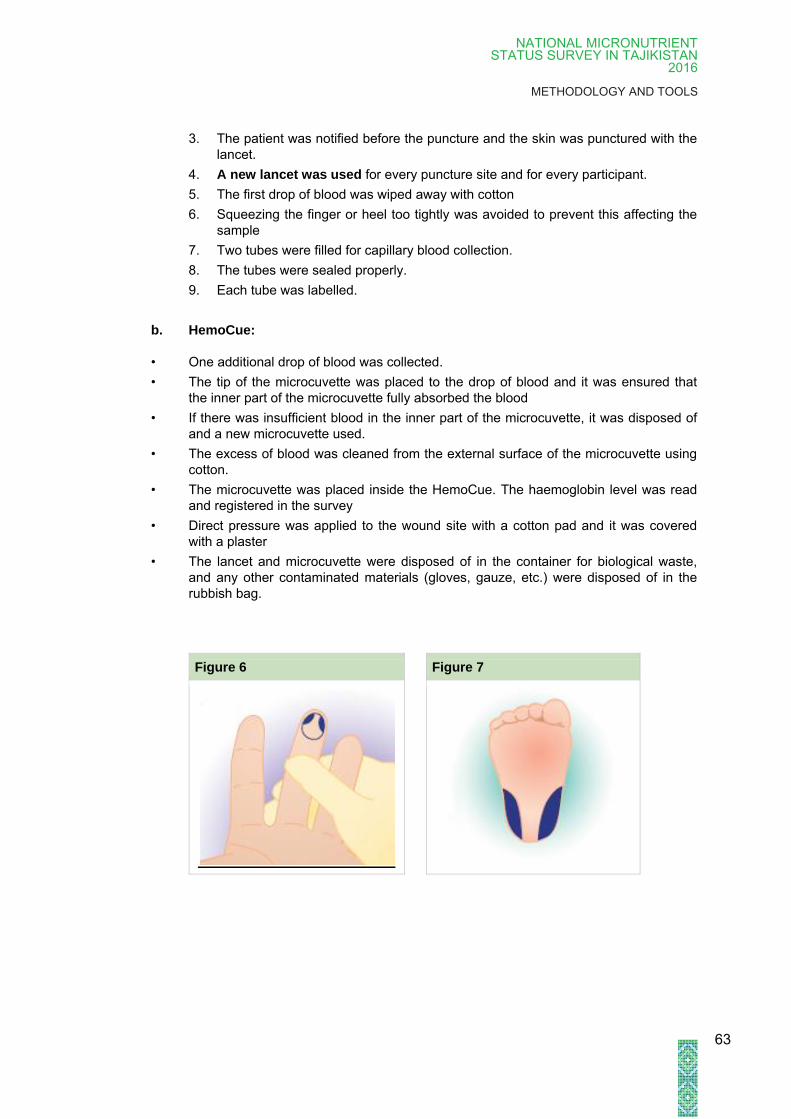
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
3. The patient was notified before the puncture and the skin was punctured with the
lancet.
4. A new lancet was used for every puncture site and for every participant.
5. The first drop of blood was wiped away with cotton
6. Squeezing the finger or heel too tightly was avoided to prevent this affecting the
sample
7. Two tubes were filled for capillary blood collection.
8. The tubes were sealed properly.
9. Each tube was labelled.
b. HemoCue:
• One additional drop of blood was collected.
• The tip of the microcuvette was placed to the drop of blood and it was ensured that
the inner part of the microcuvette fully absorbed the blood
• If there was insufficient blood in the inner part of the microcuvette, it was disposed of
and a new microcuvette used.
• The excess of blood was cleaned from the external surface of the microcuvette using
cotton.
• The microcuvette was placed inside the HemoCue. The haemoglobin level was read
and registered in the survey
• Direct pressure was applied to the wound site with a cotton pad and it was covered
with a plaster
• The lancet and microcuvette were disposed of in the container for biological waste,
and any other contaminated materials (gloves, gauze, etc.) were disposed of in the
rubbish bag.
Figure 6 Figure 7
63

NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
c. Urine sample collection:
• A urine container was given to every woman or child (who could go to the toilet) and
they were asked to fill the container with urine. The participants started urinating and
collecting samples of urine "mid-stream".
• For children cared for in Gavoras (traditional cradles), urine samples were taken from
the receptacle if urine was available, but not if the urine was contaminated with stool.
• The laboratory technician transferred the urine from the container in the tube.
• The tubes were properly closed to avoid spills.
• Each tube was labelled.
IMPORTANT:
• The blood and urine samples were stored in a cooling box at 4°C until transportation
to the district laboratory. The cool boxes were only opened if necessary.
d. Salt sample3
• A salt sample was taken from one household per village.
VERIFYING THE INFORMATION:
• The team verified that all the information in the registration form and Forms 1-4 was
completed.
• They ensure that all blood, urine and salt samples were correctly labelled.
• They saved and finalized the questionnaire.
HEALTH RECOMMENDATIONS AND REFERRALS:
• Health recommendations were provided using template forms, and patients were directed to
the nearest health centre in case of:
• obesity, overweight and underweight participants; or
• anaemia.
• Diagnostic criteria for nutrition problems and anaemia are described in Table 2.
• Table 2: Diagnostic criteria
Participant Diagnosis Criterion
Children 0 to 59 months Anaemia Haemoglobin < 11g/dl
Women of reproductive age Anaemia Haemoglobin < 12g/dl
Obese BMI* ≥30
Overweight BMI 25 - 29
Normal weight BMI 18.5-24.9
Underweight BMI < 18.5
*BMI: Body mass index
3Instructions in this section were taken or modified from
http://www.himedialabs.com/HML/images/literature/pdf/100000021/24.pdf
64
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN
2016
METHODOLOGY AND TOOLS
THANKING PARTICIPANTS
• At the end of the interview, the field team thanked the household heads and the
respondents for their participation.
REPEATING STEP NUMBER 6-16 UNTIL THE NUMBER OF PARTICIPANTS was
REACHED:
• The field team identified the next household in the village and repeated the described
procedure (Step 3 to Step 16) UNTIL INFORMATION WAS RECEIVED ABOUT 12
children (6-59 months) and 12 women (15-49 years)
• The next household in the village was identified and the described procedure repeated until
information was received from a total of 12 children (6-59 months) and 12 women (15 -49
years)
After field data collection (same day)
REPORTING END OF FIELD WORK:
• Once the fieldwork was completed the head of the team reported to the field supervisor by
phone at the time of departure from the village.
TRANSPORTING, CENTRIFUGING AND STORING SAMPLES
• The blood, urine and salt samples were transported, processed and stored as established in
the fieldwork plan. The places of centrifuge and the procedures for storage of samples
differed according to the conditions in every region. However, all field teams followed
certain general procedures:
a. The LABORATORY TECHINICIAN was responsible for processing, storage and
transportation of biological and salt samples.
b. During the transportation and storage of samples the cool chains was always kept.
c. Blood samples:
• Blood samples were centrifuged on collection day at the end of the field work
• Blood tubes were centrifuged for five minutes using 10.000g or 10 minutes
using 4.000-10.000g
• After centrifugation, the serum was extracted from the two tubes (two tubes
per participant) using the pipette and into light protected amber tubes.
• Before every new sample a new pipette tip was put on the pipette and
afterwards the tip was disposed of.
• The new tube was sealed and labelled using the same identification number
used in the collection tubes for this participant.
• The samples were stored in storing boxes and placed in cool boxes or fridges
at a temperature of ≥4-7 C. If power cuts were expected, additional ice or gel
packs were used in the cool boxes in order to maintain the cold chain.
65
NATIONAL MICRONUTRIENT STATUS SURVEY IN TAJIKISTAN 2016
METHODOLOGY AND TOOLS
d. Urine samples
• Urine samples were stored at 4-7 C.
• It was ensured that the tubes were properly closed to avoid spills.
e. Biological waste
• Biological waste was appropriately disposed in the laboratory or health
facilities.
• The head of the team reported to the Field Supervisor once the biological samples had
been processed and stored.
• The samples were transported in cold boxes using sufficient cold packs to the Laboratory of
Preventive Medicine Dushanbe on specific days, where they were frozen at minus 20°C
until further analysis. The samples were not transported using PUBLIC TRANSPORT
• The laboratory technician and the logistics company were responsible for transporting the
biological samples to Dushanbe, assuring the cold chain. The laboratory technician
included a remission note, with the following information:
Date:
Time:
Place:
Name of the sender
Number of blood tubes:
Number of urine tubes:
Number of salt samples
Destination address: Laboratory of the Preventive Medicine Institute
Shevchenko street 61, Dushanbe, -Tajikistan
Person responsible for receiving the sample
• The laboratory technician informed the Field Supervisor the time of departure of the
samples.
• The driver from the logistic company reported to the Field Supervisor once the samples had
been delivered to the Laboratory of the Preventive Medicine Institute.
PREPARING FIELD WORK FOR NEXT DAY
• The head of the team and the field team verified the PROCUREMENT CHECKLIST for the
next day (including freezing ice packs and charging tablets).
66



















