440
KPMG National Monitoring and Evaluation of the Indigenous Chronic Disease Package First Monitoring Report 2010-11

KPMGNational Monitoring and Evaluation of the Indigenous Chronic Disease PackageFirst Monitoring Report2010-11

Online ISBN: 978-1-74186-056-6Publications Approval Number: 10487
Paper-based publications© Commonwealth of Australia 2013This work is copyright. You may reproduce the whole or part of this work in unaltered form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only if you or your organisation do not use the reproduction for any commercial purpose and retain this copyright notice and all disclaimer notices as part of that reproduction. Apart from rights to use as permitted by the Copyright Act 1968 or allowed by this copyright notice, all other rights are reserved and you are not allowed to reproduce the whole or any part of this work in any way (electronic or otherwise) without first being given the specific written permission from the Commonwealth to do so. Requests and inquiries concerning reproduction and rights are to be sent to the Online, Services and External Relations Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to [email protected]. Internet sites© Commonwealth of Australia 2013This work is copyright. You may download, display, print and reproduce the whole or part of this work in unaltered form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only if you or your organisation do not use the reproduction for any commercial purpose and retain this copyright notice and all disclaimer notices as part of that reproduction. Apart from rights to use as permitted by the Copyright Act 1968 or allowed by this copyright notice, all other rights are reserved and you are not allowed to reproduce the whole or any part of this work in any way (electronic or otherwise) without first being given the specific written permission from the Commonwealth to do so. Requests and inquiries concerning reproduction and rights are to be sent to the Online, Services and External Relations Branch, Department of Health, GPO Box 9848, Canberra ACT 2601, or via e-mail to [email protected].
This report has been independently prepared for the Australian Government Department of Health by KPMG Australia, and does not necessarily represent the views of the Australian Government.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The evaluation of the Indigenous Chronic Disease Package was commissioned by the Department of Health. This evaluation report has been prepared by KPMG Australia.The report’s lead authors were the National Health and Human Services Practice, KPMG.The other major contributors to the report were: WinangaliKPMG wishes to acknowledge the following stakeholders for their contribution to the evaluation through giving their time and sharing their experiences: the Department of Health, state and territory health departments, the National Aboriginal Community Controlled Health Organisation and its Affiliates, peak bodies, Indigenous Health Services, Divisions of General Practice/Medicare Locals, the Indigenous Health Partnership Forums, ICDP workers and their fund holder representatives, general practice staff and community members. Please refer to Appendix C for a full list of stakeholders consulted.CitationKPMG 2013, National Monitoring and Evaluation of the Indigenous Chronic Disease Package First Monitoring Report 2010-11, Australian Government Department of Health, Canberra
iKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table of Contents iiDisclaimer viiGlossary viiiExecutive Summary 11. Introduction 102. Contextual influences133. Whole of ICDP 164. National Action to Reduce Indigenous Smoking Rates (A1), and
Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) 25
5. Local Indigenous Community Campaigns to Promote Better Health (A3) 58
6. Subsidising PBS Medicine Co-payments (B1) 677. Higher utilisation costs for MBS and PBS (B2) 988. Supporting Primary Care Providers to Coordinate Chronic Disease
Management (B3a) 1089. Case study: Impact of the PIP Indigenous Health Incentive on the
standard of care provided to Aboriginal and Torres Strait Islander people 128
10. Care Coordination and Supplementary Services Program (B3b) 13711. Case Study: Factors impacting access to the CCSS program 15512. Improving Indigenous Participation in Health Care through Chronic
Disease Self Management (B4) 16413. Urban Specialist Outreach Assistance Program (USOAP) (B5a) 17214. Medical Specialist Outreach Assistance Program – Indigenous
Chronic Disease (MSOAP-ICD) (B5b) 18715. Workforce Support, Education and Training (C1) 20316. Expanding the Outreach and Service Capacity of Indigenous Health
Organisations (C2) 22117. Improving Indigenous Access to Mainstream Primary Care Program
(C3) 23318. Attracting More People to Work in Indigenous Health (C4) 254
iiKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
19. Clinical Practice and Decision Support Resources (C5) 266
iiiKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
List of Figures and TablesFigure 1: Summary of Tackling chronic disease risk factors measures, including the progress of overall implementation, key achievements in 2010-11 and key findings against early results.........................................................................................3Figure 2: Summary of Improving chronic disease management and follow up care measures, including the progress of overall implementation, key achievements in 2010-11 and key findings against early results..................................5Figure 3: Summary of Workforce expansion and support measures, including the progress of overall implementation, key achievements in 2010-11 and key findings against early results.........................................................................................7Figure 4: National Action to Reduce Indigenous Smoking Rates causal pathway. Source: KPMG..............................................................................................................26Figure 5: Helping Indigenous Australians Reduce their Risk of Chronic Disease causal pathway. Source: KPMG...................................................................................27Figure 6: Supply/dispensing of smoking cessation medicines - allocation across CtG and S100 RAAHS initiatives..................................................................................47Figure 7: Smoking cessation prescriptions for May 2007 quarter to May 2011 quarter for PBS, CtG and S100 RAAHS.........................................................................50Figure 8: Local Indigenous Community Campaigns to Promote Better Health causal pathway. Source: KPMG...................................................................................59Figure 9: PBS Co-payment causal pathway. Source: KPMG.........................................68Figure 10: Aboriginal and Torres Strait Islander health assessments August 2008 to May 2011................................................................................................................99Figure 11: Aboriginal and Torres Strait Islander health assessments August 2008 to May 2011 by state/territory. .................................................................................100Figure 12: Aboriginal and Torres Strait Islander health assessments August 2008 quarter to May 2011 quarter by remoteness area.....................................................101Figure 13: Health assessments, services from PNs/AHWs and allied health services for August 2008 quarter to May 2011 quarter.............................................103Figure 14: Per 100 capita utilisation by quarter - Australia: Selected MBS items; and CtG items...........................................................................................................107Figure 15: PIP Indigenous Health causal pathway. Source: KPMG..............................109Figure 16: Possibilities for patient flow through registration to Tier 1 payment.........129Figure 17: CCSS program causal pathway. Source: KPMG.........................................138Figure 18: Chronic Disease Self-Management causal pathway. Source: KPMG..........165Figure 19: USOAP causal pathway. Source: KPMG.....................................................174Figure 20: MSOAP-ICD program causal pathway. Source: KPMG...............................189
ivKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Figure 21: Workforce Support, Education and Training causal pathway. Source: KPMG.........................................................................................................................204Figure 22: Expanding the Outreach and Service Capacity of Indigenous Health Organisations causal pathway. Source: KPMG...........................................................222Figure 23: Improving Indigenous Access to Mainstream Primary Care causal pathway. Source: KPMG.............................................................................................234Figure 24: Attracting More People to Work in Indigenous Health causal pathway. Source: KPMG............................................................................................................255Figure 25: Clinical Practice and Decision Support Resources causal pathway. Source: KPMG............................................................................................................266
vKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 1: Overview of the structure of ‘measure chapters’ in this report......................11Table 2: Assessment of key dependencies of A1/A2 measures...................................28Table 3: Assessment of expected impacts of A1/A2 measures based on implementation progress............................................................................................29Table 4: Actual expenditure, A1 and A2 measures, 2010-11.......................................31Table 5: Number of RTC, TAW and HLW workers recruited, 2010-11...........................33Table 6: Number of FTE funded and recruited RTC, TAW and HLW positions for 2010-11. .....................................................................................................................34Table 7: Remoteness breakdown for number of FTE funded and recruited RTC, and TAW positions for measure A1 2010-11................................................................34Table 8: Remoteness breakdown for number of FTE funded and recruited HLW positions for measure A2 2010-11...............................................................................34Table 9: Summary of types of activities RTSHLTs have undertaken............................40Table 10: Number of smoking cessation CtG scripts dispensed by jurisdiction from August 2010 to May 2011 quarters. ...................................................................46Table 11: Comparison of dispensing of CtG, S100 RAAHS smoking cessation prescriptions in three months to May 2011 by scheme for Aboriginal and Torres Strait Islander smokers................................................................................................48Table 12: Number of full co-payment smoking cessation prescriptions in three months to May 2011....................................................................................................48Table 13: Assessment of key depedencies of the A3 measure....................................60Table 14: Assessment of expected impacts of the A3 measure based on implementation progress............................................................................................61Table 15: Assessment of key dependencies of the B1 measure..................................69Table 16: Assessment of expected and observed impacts of the B1 measure based on implementation progress.............................................................................71Table 17: Distribution of patients and scripts, for main groups: May quarter 2011............................................................................................................................74Table 18: Projected and actual utilisation of CtG scripts 2010-11...............................76Table 19: Comparison of geographical distribution of prescribing practices (as at May 2011) to distribution of Aboriginal and Torres Strait Islander population (2006).........................................................................................................................77Table 20: Number of pharmacies (active in that quarter) by jurisdiction and Aboriginal and Torres Strait Islander people per registered pharmacy. .....................79Table 21: Average number of CtG scripts dispensed per pharmacy per quarter (pharmacies active in that quarter) by jurisdiction. ....................................................81Table 22: Patients dispensed at least one CtG script by patient category and quarter (2010-11)*......................................................................................................83
viKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 23: Number of CtG scripts dispensed over 12 months to 31 May 2011 by patient category and state or territory*. .....................................................................84Table 24: CtG Scripts dispensed by ATC category in 12 months to 31 May 2011 by remoteness.............................................................................................................86Table 25: Proportion of CtG scripts annotated electronically by jurisdiction and quarter. ......................................................................................................................91Table 26: Number of hotline enquiries, 2010-11, by intake type. Source: Department of Health and Ageing...............................................................................93Table 27: MBS follow up items for which detailed data is available and short description. Source: Medicare Benefits Schedule......................................................102Table 28: Total services and May 2011 service and provider statistics at the national level.............................................................................................................104Table 29: Aboriginal and Torres Strait Islander health services by jurisdiction. ........105Table 30: Physiotherapy health services by jurisdiction. ..........................................105Table 31: Podiatry health services by jurisdiction. ....................................................106Table 32: Assessment of the key dependencies of the B3a measure........................110Table 33: Assessment of the expected and observed impacts of the B3a measure based on implementation progress............................................................111Table 34: Practice registrations by Medicare quarter and practice type....................114Table 35: Patients and practices registered in 2010 by type of practice...................115Table 36: Expenditure against PIP Indigenous Health Incentive payments May 2010 to May 2011.....................................................................................................117Table 37: Numbers of registered patients triggering outcome payments and practice type in 2010................................................................................................120Table 38: Practice reach of PIP Indigenous Health Incentive by jurisdiction at May 2011.,........................................................................................................................122Table 39: Estimates of PIP Indigenous Health Incentive reach for the Aboriginal and Torres Strait Islander population aged 15 years and over and with a chronic disease, by jurisdiction, 2010.,,..................................................................................123Table 40: Estimates of PIP Indigenous Health Incentive reach for the Aboriginal and Torres Strait Islander population aged 15 years and over and with a chronic disease, by remoteness, 2010.,,.................................................................................123Table 41: Assessment of key dependencies of the B3b measure..............................139Table 42: Assessment of expected and observed impacts of the B3b measure based on implementation progress...........................................................................140Table 43: Number of Care Coordinators (FTE and headcount) recruited by states and territories, 2010-2011. Source: Department of Health and Ageing.....................142
viiKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 44: Care Coordinators recruited in 2010-11 (FTE and headcount) by urban, regional and remote location.....................................................................................143Table 45: Number of patients who received Care Coordinator services and/or Supplementary Services funding, by state or territory, 2010-11...............................147Table 46: Assessment of key dependencies of the B4 measure................................167Table 47: Assessment of expected and observed impacts of the B4 measure based on implementation progress...........................................................................168Table 48: Number of health services providers trained in Flinders CDSM, target and actual.................................................................................................................169Table 49: Location of Flinders CDSM training, by jurisdiction, to 31 August 2011.....170Table 50: Assessment of key dependencies of the B5a measure..............................175Table 51: Assessment of expected and observed impacts of the B5a measure based on implementation progress...........................................................................176Table 52: Number of USOAP outreach service host organisations contracted, by state and services commenced, at 30 June 2011. Source: Department of Health and Ageing................................................................................................................179Table 53: Number of specialists participating in USOAP in 2010-11, by state...........180Table 54: Location of USOAP service delivery, type of services provided, and number of Aboriginal and Torres Strait Islander patients served, by state or territory, 1 September 2010 to 31 August 2011........................................................181Table 55: Assessment of key dependencies of the B5b measure..............................190Table 56: Assessment of expected and observed impacts of the B5b measure based on implementation progress...........................................................................191Table 57: Specialty and other health professional services delivered by the MSOAP-ICD, by state or territory, 2010-11. Source: Department of Health and Ageing.......................................................................................................................195Table 58: Number of MSOAP-ICD services provided, by outreach service type, 2010-11.....................................................................................................................197Table 59: Number of MSOAP-ICD services provided, and number of patients receiving services, by state and territory, 2010-11. .................................................198Table 60: Assessment of key dependencies of the C1 measure................................205Table 61: Assessment of expected and observed impacts of the C1 measure based on implementation progress...........................................................................208Table 62: Delivery of ATSIOW orientation packages, by jurisdiction, and cumulative number of ATSIOWs oriented, as at 1 June 2011.....................................211Table 63: Number of nursing and midwifery professional development and clinical placement scholarships provided, 2010 and 2011 calendar years, by state or territory........................................................................................................217Table 64: Assessment of key dependencies of the C2 measure................................223
viiiKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 65: Assessment of expected and observed impacts of the C2 measure based on implementation progress...........................................................................225Table 66: Number of C2 workforce FTE, allocated (A) and actual recruitment (R), to 30 June 2011, by jurisdiction.................................................................................227Table 67: Capital works projects funded by the Expanding the Outreach and Service Capacity of Indigenous Health Organisations measure, by jurisdiction, to 30 June 2011.............................................................................................................229Table 68: Assessment of key dependencies of the C3 measure................................235Table 69: Assessment of expected and observed impacts of the C3 measure based on implementation progress...........................................................................239Table 70: ATSIOWs and IHPOs in Divisions and SBOs to 30 June 2011, by jurisdiction.................................................................................................................241Table 71: Assessment of key dependencies of the C4 measure................................256Table 72: Assessment of expected and observed impacts of the C4 measure based on implementation progress...........................................................................258Table 73: Assessment of key dependencies of the C5 measure................................268Table 74: Assessment of likely effects of the C5 measure based on implementation progress..........................................................................................269
ixKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Disclaimer
Inherent LimitationsThis report has been prepared as outlined in the scope section. The services provided in connection with this engagement comprise an advisory engagement which is not subject to Australian Auditing Standards or Australian Standards on Review or Assurance Engagements, and consequently no opinions or conclusions intended to convey assurance have been expressed.
This report has not been prepared on KPMG letterhead and does not contain the KPMG logo, but is presented in an editable format to support web accessibility for the vision impaired. We confirm that the definitive version of this report is that which bears the KPMG logo.
The findings in this report are based on consultation with stakeholders.
No warranty of completeness, accuracy or reliability is given in relation to the statements and representations made by, and the information and documentation provided by the Department of Health personnel and stakeholders consulted as part of the process.
Where appropriate KPMG have indicated within this report the sources of the information provided. We have not sought to independently verify those sources unless otherwise noted within the report.
KPMG is under no obligation in any circumstance to update this report, in either oral or written form, for events occurring after the report has been issued in final form.
The findings in this report have been formed on the above basis.
Third Party RelianceThis report is solely for the purpose set out in the scope section and for the information of the Department of Health, and is not to be used for any other purpose or distributed to any other party without KPMG’s prior written consent.
This report has been prepared at the request of the Department of Health in accordance with the terms of KPMG’s contract. Other than our responsibility to the Department of Health neither KPMG nor any member or employee of KPMG undertakes responsibility arising in any way from reliance placed by a third party on this report. Any reliance placed is that party’s sole responsibility
xKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
GlossaryAcronym DefinitionAGPN Australian General Practice NetworkAH&MRC Aboriginal Health and Medical Research CentreAHCSA Aboriginal Health Council of SAAHMAC Australian Health Ministers’ Advisory CouncilAHW Aboriginal Health WorkerAIHW Australian Institute of Health and WelfareAMS Aboriginal Medical ServiceAMSANT Aboriginal Medical Services Alliance of the Northern
TerritoryAPCC Australian Primary Care CollaborativesATC Anatomical Therapeutic Chemical (ATC) Classification
SystemATSIHP The Aboriginal and Torres Strait Islander Health PartnershipATSIOW Aboriginal and Torres Strait Islander Outreach WorkerCAH Centre for Aboriginal HealthCARIHPC Central Australian Regional Indigenous Health Planning
CommitteeCCSS Care Coordination and Supplementary Services (B3b
measure)CDSM Chronic Disease Self ManagementCEITC Centre for Excellence in Indigenous Tobacco ControlCEO Chief Executive OfficerCOAG Council of Australian GovernmentsCO Central Office (Department of Health and Ageing)CRG Campaign Reference GroupCtG Closing the GapDH Victorian Department of HealthDHHS Tasmanian Department of Health and Human ServicesDoGP Division of General Practice
xiKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Acronym DefinitionDoHA Department of Health and AgeingFaHCSIA Department of Families, Housing, Community Services and
Indigenous AffairsFTE Full Time EquivalentGP General PractitionerGPET General Practice Education and TrainingGPNNT General Practice Network Northern TerritoryGPNSW General Practice New South WalesGPMP General Practice Management PlanGPQ General Practice QueenslandGPSA General Practice South AustraliaGPV General Practice VictoriaHLW Healthy Lifestyle WorkerHPF Health Performance FrameworkICDP Indigenous Chronic Disease PackageIHPF Indigenous Health Partnerships ForumIHPO Indigenous Health Project OfficerIHS Indigenous Health ServiceMBS Medicare Benefits ScheduleMSOAP Medical Specialist Outreach Assistance ProgramMSOAP-ICD Medical Specialist Outreach Assistance Program –
Indigenous Chronic DiseaseNACCHO National Aboriginal Community Controlled Health
OrganisationNATSIHEC National Aboriginal and Torres Strait Islander Health
Equality CouncilNATSISS National Aboriginal and Torres Strait Islander Social SurveyNIRA National Indigenous Reform AgreementNPA National Partnership AgreementNRT Nicotine Replacement TherapyNSW Health New South Wales Department of Health
xiiKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Acronym DefinitionNT DoH Northern Territory Department of HealthNTER Northern Territory Emergency ResponseOATSIH Office for Aboriginal and Torres Strait Islander HealthOWG Operational Working GroupQAIHC Queensland Aboriginal and Islander Health CouncilPIP Practice Incentives ProgramPBS Pharmaceutical Benefits SchemePN Practice NurseQLD Health Queensland Department of HealthQUMAX Quality Use of Medicines Maximised in Aboriginal and Torres
Strait Islander Peoples ProgramRACGP Royal Australian College of General PractitionersRHFs Regional Health ForumsRPBS Regional Pharmaceutical Benefits SchemeRTC Regional Tobacco CoordinatorRTO Registered Training OrganisationRTSHLT Regional Tackling Smoking and Healthy Lifestyle TeamRWAV Rural Workforce Agency VictoriaSAAHP South Australian Aboriginal Health PartnershipS100 RAAHS Supply of pharmaceutical benefits to remote area Aboriginal
Health Services under section 100 of the National Health Act 1953
SBO State Based Organisation of the Divisions of General Practice
SONT Specialist Outreach Northern TerritorySTO State and Territory Office (Department of Health and
Ageing)TAC Tasmanian Aboriginal CentreTAWs Tobacco Action WorkersTCA Team Care ArrangementsTERIHPC Top End Regional Indigenous Health Planning Committee
xiiiKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Acronym DefinitionTRG Technical Reference GroupUSOAP Urban Specialist Outreach Assistance ProgramVACCHO Victorian Aboriginal Community Controlled Health
OrganisationVACKH Victorian Advisory Council on Koori HealthWACHS Western Australian Country Health ServiceWA Health Western Australia Department of Health
xivKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key terms DefinitionCtG scripts Used by service providers and community members to refer
to scripts which have been CtG annotated to provide the patient with access to the PBS co-payment relief (B1 ICDP measure)
Indigenous health service
A primary health care practice/Aboriginal Community Controlled Health Service/clinic providing primary care services to a predominantly Aboriginal and Torres Strait Islander population. In this report IHS may refer to a community controlled health organisation or a different type of entity which primarily provides primary health care services to Aboriginal and Torres Strait Islander people.
Mainstream In this report this refers to private or public services which primarily provide health care services to non-Aboriginal and Torres Strait Islander people. An example is mainstream general practices.
Medicare quarter
Medicare quarter in this report refers to data periods, the four Medicare quarters are:Jun-AugSept-NovDec-FebMar-May
xvKPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Executive SummaryThis document is the First Monitoring Report for the evaluation of the Indigenous Chronic Disease Package (ICDP or the Package). The purpose of the report is to provide information on the second year of implementation of the ICDP (2010-11).The ICDP is the Australian Government’s contribution to the National Partnership Agreement on Closing the Gap in Indigenous Health Outcomes (NPA). The ICDP comprises a set of 14 interrelated measures which fit within one of the three key activity and outcome areas that have been identified for the ICDP: tackling chronic disease risk factors, improving chronic disease management and follow up care and workforce expansion and support.Overview of progressThe continued implementation of ICDP in 2010-11 was largely on track. The delays that did occur were in components of the ICDP that collectively represent a relatively small proportion of the overall investment. This second year of the ICDP saw the consolidation of those measures first launched in 2009-10 and the rollout of most other measures.As noted in the Baseline Report, this represents an important achievement, given the magnitude of implementation activity. In its second year of implementation, the ICDP: required a considerable investment in workforce across a number of
measures, as well as setting up various initiatives to support the new workforce such as training and networking supports;
successfully deployed innovative strategies such as the community based social marketing strategies;
was able to consolidate various incentive programs including Closing the Gap (CtG) scripts, Practice Incentive Program (PIP) Indigenous Health Incentive and access to specialist services;
required substantial and effective collaboration between the mainstream and Aboriginal and Torres Strait Islander health sectors, which is critical to addressing local implementation issues; and
has considerable support amongst all stakeholders for its broad direction.There is continued support for the broad direction of ICDP amongst all stakeholders, who also recognise that it will take time to consolidate the various initiatives that will require on-going and effective collaboration across all levels of government and across the various health service sectors. Overall, the majority of stakeholders believe that the ICDP is sufficiently comprehensive and that it will benefit individuals, communities and enhance
1© 2013 KPMG, an Australian partnership and a member firm of the KPMG network of independent member firms affiliated
with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
the service system in the Indigenous Health Service (IHS) and the mainstream sectors. The potential effectiveness of the ICDP could be impacted by delays in the implementation of some aspects of the Package, such as recruitment delays, and the time it will take for all aspects to be fully operational. There are early indications of issues that will be critical to the long-term effectiveness of the ICDP and that need to be addressed, which otherwise could constrain the effectiveness of the ICDP. These issues relate to the need to improve collaboration between health care sectors and between different levels of government; addressing emerging ICDP workforce requirements; and the sustainability of core components of ICDP such as the workforce.Summary of progress by priority areaThe ICDP has three priority areas as follows: tackling chronic disease risk factors; improving chronic disease management and follow up care; and workforce expansion and support.Progress with the implementation of the various measures that comprise each of these priority areas follows.2010-11 progress - Tackling chronic disease risk factors
This priority area includes three measures: National Action to Reduce Indigenous Smoking Rates (also referred to as
the A1 measure); Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2);
and Local Indigenous Community Campaigns to Promote Better Health (A3).Key activities included substantial research into health promotion strategies that are likely to be effective in the Aboriginal and Torres Strait Islander context; establishment of Regional Tackling Smoking and Healthy Lifestyle Teams (RTSHLTs); additional national supports targeting smoking; and the funding of Local Community Campaigns (LCCs) grant projects to increase healthy lifestyle choices through two rounds of grant applications. The following achievements in 2010-2011 have been noted by the evaluation: substantial progress with the deployment of a new health promotion
workforce, with the funding and recruitment of the RTSHLTs; early indications that the ICDP is influencing many people to think about
and work towards quitting smoking and adopting healthy lifestyle changes,
2© 2013 KPMG, an Australian partnership and a member firm of the KPMG network of independent member firms affiliated
with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
although high smoking rates are still considered to be a significant problem;
the uptake of smoking cessation medicines appears to have increased over 2010-2011; however, this is most likely influenced by a combination of ICDP and non-ICDP initiatives (funded by the Commonwealth and state/territory governments);
the introduction of smoke-free workplace policies (supported by the Office for Aboriginal and Torres Strait Islander Health (OATSIH)) are promoting organisational change in IHSs to support the work of RTSHLTs, and even in the absence of RTSHLTs; and
the mobilisation of the first round of LCCs. The following figure summarises the overall progress and progress with respect to what the Evaluation Framework refers to as (expected) early results.
A1&A2
Establishment of RTSHLTs - recruitment of 68 workers. National Coordinator for Tackling Indigenous Smoking appointed.
Teams have the knowledge and skills to provide smoking prevention and cessation and health lifestyle activities
A3First round of LCCs funded in J une 2011 - 38 campaigns. 'Live Longer!' website & Community Health Action Pack launched
Local Community Campaigns are evidence based
Measure Implementation progress and key achievements Early results
Figure 1: Summary of Tackling chronic disease risk factors measures, including the progress of overall implementation1, key achievements in 2010-11 and key findings against early results.2
2010-11 progress - Improving chronic disease management and follow up care
This priority area includes six measures: Subsidising Pharmaceutical Benefits Scheme (PBS) Medicine Co-payments
(B1); Higher utilisation costs for Medicare Benefits Scheme (MBS) and PBS (B2); Supporting Primary Care Providers to Coordinate Chronic Disease
Management (CDSM) (B3a and B3b);
1 One arrow represents that implementation has just commenced and has a long way to go; two arrows represents that implementation is on track and expected to be completed in years three and four; three arrows represents that the measure is fully implemented and operational.2 As specified in the ICDP Monitoring and Evaluation Framework.
3© 2013 KPMG, an Australian partnership and a member firm of the KPMG network of independent member firms affiliated
with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Improving Indigenous Participation in Health Care through Chronic Disease Self Management (B4);
Increasing Access to Specialist and Multidisciplinary Team Care (B5a and B5b); and
Monitoring and evaluation (B6). Key activities included subsiding the PBS co-payment for Aboriginal and Torres Strait Islander people with or at risk of a chronic disease; implementing the PIP Indigenous Health Incentive (B3a) to enhance access to high quality primary health care; establishing a Care Coordinator workforce; increasing the capacity of the health workforce to provide chronic disease self management training to Aboriginal and Torres Strait Islander people with chronic disease; and funding specialists and allied health professionals to provide services in areas of need. The Sentinel Sites Evaluation (SSE) and the National Monitoring and Evaluation are also activities which fall into this outcome area. The following achievements in 2010-2011 have been noted by the evaluation: the number of patients using CtG scripts exceeded projections in the 12
months to 31 May 2011; uptake of PIP Indigenous Health Incentive exceeded expectations in terms
of expenditure, patient registration payments and Tier 2 payments (majority of patient care); however, Tier 1 incentive payments for practices to provide chronic disease management are less than expected. This does not necessarily mean that patients are not receiving effective care; roll out of the Care Coordinator workforce progressed (B3b), however, this program was still very much in the implementation phase during this year;
training targets for chronic disease self management training were significantly exceeded with a total of 202 workers trained against a target of 57;
implementation of the Medical Specialist Outreach Assistance Program – Indigenous Chronic Disease (MSOAP–ICD) (B5b) program was largely successful and was supported by groundwork laid by the mainstream MSOAP program;
the inclusion of allied health services has been positive, and the greater availability of allied health providers has offset specialist recruitment challenges; and
the SSE project continued to progress and to provide important location based insights into the implementation and early impact of the ICDP.
The following figure summarises the overall progress and progress with respect to what the Evaluation Framework refers to as (expected) early results.
4© 2013 KPMG, an Australian partnership and a member firm of the KPMG network of independent member firms affiliated
with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
B1 79,076 individual Aboriginal and Torres Strait Islander people were dispensed a total of 859,370 CtG scripts
Participating patients have reduced financial barriers to purchasing pharmaceuticals for chronic disease management
B3a Uptake exceeded expectations for practice sign-up and patient registrations
Outcomes payments associated with best practice chronic disease management (Tier 1 payments) commence
B3b 22.1 FTE Care Coordinators recruited and 294 patients received services. 83 patients received Supplementary Services funds
The program aligns with the guidelines, and participating patients are receiving increased access to coordinated multidisciplinary care as recommended in care plans
B4 202 health care professionals trained in CDSM against a target of 57. Puntukurnu Aboriginal Remote Project commenced
A growing number of health care professionals have the knowledge and skills to effectively deliver CDSM sessions
B5aSignificant increases in the number of specialists participating (19) and patients receiving specialist care (380), compared to 2009-10
Patients in urban areas are beginning to have greater access to culturally accessible specialist care
B5b 541 services provided to 6,283 Aboriginal and Torres Strait Islander patients
Patients in regional and remote areas continue to have greater access to accessible multidisciplinary care
Measure Implementation progress and key achievements Early results
Figure 2: Summary of Improving chronic disease management and follow up care measures, including the progress of overall implementation3, key achievements in 2010-11 and key findings against early results.4
3 One arrow represents that implementation has just commenced and has a long way to go; two arrows represents that implementation is on track and expected to be completed in years three and four; three arrows represents that the measure is fully implemented and operational.4 As specified in the ICDP Monitoring and Evaluation Framework.
5KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
2010-11 progress - Workforce expansion and support
This priority area includes five measures: Workforce Support, Education and Training (C1); Expanding the Outreach and Service Capacity of Indigenous Health
Organisations (C2); Engaging Divisions of General Practice to Improve Indigenous Access to
Mainstream Primary Care (C3); Attracting More People to Work in Indigenous Health (C4); and Clinical Practice and Decision Support Resources (C5).Key activities included provision of workplace training and support for ICDP workers; establishment of Indigenous Health Project Officers (IHPOs) and Aboriginal and Torres Strait Islander Outreach Workers (ATSIOWs) in both the IHS and mainstream primary health care sectors; health workforce expansion activities; and the establishment of an on-line clinical resources and tools repository to support better practice care for Aboriginal and Torres Strait Islander people. The following achievements in 2010-2011 have been noted by the evaluation: recruitment of ATSIOWs within IHSs is largely on track, although
recruitment has been slow in some locations, and there is emerging evidence that ATSIOWs are facilitating increased access to health care within IHSs by Aboriginal and Torres Strait Islander people;
recruitment of IHPOs and ATSIOWs in mainstream services is also progressing well, although there have been some challenges around the recruitment and retention of ATSIOWs in this sector, and there is emerging evidence to suggest that IHPOs/ATSIOWs teams have supported increased access to mainstream primary health care services and higher utilisation of MBS items for some Aboriginal and Torres Strait Islander people; and
promotional materials developed to encourage Aboriginal and Torres Strait Islander secondary school students to consider taking up a career in health have been used by stakeholders and are considered valuable in engaging students.
The following figure summarises the overall progress and progress with respect to what the Evaluation Framework refers to as (expected) early results
6KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
C1
84 ATSIOWs commenced orientation or training programs, GP registrars placed in 46 additional Indigenous Health Training Posts, 64 professional development and 60 clinical placement scholarships awarded
No early result outcomes noted in the second year of this measure
C2 37 ATSIOWs, 19.5 Practice Managers, 13.8 other health workforce positions recruited to 47 IHSs across Australia
Participating IHSs have increased capacity and capability to provide services
C380.9 ATSIOWs and 92.9 IHPOs recruited to Divisions of General Practice, SBOs, NACCHO and NACCHO affiliates, exceeding targets
Implementation complies with program guidelines; and Aboriginal and Torres Strait Islander people increase their utilisation of mainstream primary health care services
C4 Development, testing and refining of the Health Heroes and Do Something Real campaigns, using a strong evidence base
The Health Heroes campaign is informed by research and rolled out across schools
C5 Development of first iteration of the web-based primary health care resource – not available for release
Due to implementation delays, there are no early results for this measure
Measure Implementation progress and key achievements Early results
Figure 3: Summary of Workforce expansion and support measures, including the progress of overall implementation5, key achievements in 2010-11 and key findings against early results.6
5 One arrow represents that implementation has just commenced and has a long way to go; two arrows represents that implementation is on track and expected to be completed in years three and four; three arrows represents that the measure is fully implemented and operational.6 As specified in the ICDP Monitoring and Evaluation Framework.
7KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Whole of Package impactsWhile the ICDP comprises individual measures, its potential impact is more than the sum of the effects of the individual measures. There are indications that the Package as a whole has enhanced the service system as a result of the interconnectedness and interdependencies of the individual measures and the collaboration that the ICDP has generated from the extensive support that national and local organisations have for the ICDP. Most notably, the ICDP has achieved over and beyond the effects of individual measures in the following areas: Enhanced the capacity and capability of the service system to engage
Aboriginal and Torres Strait Islander communities through multiple interconnected elements of ICDP.
Enhanced the capability of the existing service system and in particular, improved cultural competency of the mainstream sector through the on-the ground collaborative efforts between various ICDP workforce elements.
Improved access to existing knowledge and information resources relating to chronic disease management guidelines and best practice through networking opportunities created by different aspects of ICDP.
Improved collaboration between the mainstream and the IHS sectors and between different levels of government.
As organisations that are funded by ICDP and other affected organisations better understand how the different components of the ICDP are designed to be complementary to each other, the systems effects of ICDP are likely to grow. There are a number of themes that relate to the Package as a whole that are emerging and that present opportunities to enhance the impact of ICDP and that are critical to the long-term effectiveness of ICDP.Cross measure and priority area themes Within the individual measure chapters ( through ) a number of measure specific facilitators, barriers and opportunities have been identified. There are a number that are in common across multiple measures and that relate to the Package as a whole, listed below. For workforce based measures, organisational leadership, capacity
and support are identified as facilitators (when present) and as barriers (when not optimal). This is of particular relevance for the ICDP positions which represent a new line of business in their organisations – such as RTSHLTs in organisations which have historically focused on acute primary health care, or ATSIOWs and IHPOs in Divisions of General Practice (DoGPs) which have not previously had such a role in Aboriginal and Torres Strait Islander health.
8KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Important linkages between measures have already been established, most notably linking the workforce elements of the National Action to Reduce Indigenous Smoking Rates (A1) and Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) measures. There are other opportunities to maximise potential synergies such as promoting the website resources (C5) to all ICDP workforce, the complementary roles of ATSIOWs and Care Coordinators and the complementary nature of LCCs and RTSHLTs.
The National Health Reform agenda provides further opportunity and risks for the ICDP. While the period of early reform may slow implementation for some measures, the establishment of Medicare Locals also provides an opportunity to maximise the local impact of ICDP and support its sustainability. The department could promote the role of Medicare Locals in the Indigenous Health Partnership Forums (IHPFs) at the national and jurisdictional level as a way of supporting ongoing cross-sector collaboration of ICDP activities and Aboriginal and Torres Strait Islander health more broadly.
The department should continue to pursue and promote flexibility to allow locally appropriate implementation of the measures and to respond to emerging challenges. Examples may include more flexible guidelines for use of the Supplementary Services funds, flexibility in the role of various ICDP workforce types to fit in with existing workforce structures and broadening eligibility criteria for the PBS Co-payment arrangements, to facilitate access for patients not connected with a PIP Indigenous Health Incentive registered practice.
The ICDP workforce values the professional development and networking opportunities that have been provided to date. All ICDP workforce groups expressed a desire for more networking opportunities as an important workforce development activity. Although individual measures have training and networking opportunities in place, development of a strategic approach to promote networking for all workforce components may be warranted.
9KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
IntroductionThis chapter provides an overview of the purpose and scope of the First Monitoring Report, as well as a brief overview of the Monitoring and Evaluation of the Indigenous Chronic Disease Package (ICDP or ‘the Package’), a discussion of the evaluation methodology relevant to the first phase of evaluation work and a description of the structure of this report. Appendix A provides a detailed overview of the ICDP including the policy context, aims, objectives and rationale and information about the individual measures that comprise the ICDP. 1.1 Purpose and scope The purpose of this document is to report on the first phase of evaluation activity, with specific reference to the 2010-11 financial year. This report builds on the Baseline Report, which covered the 2009-10 financial year.7 As with the Baseline Report, this report explores the progress of the Package at three levels - the ‘individual measures’ level, the ‘overall Package’ level and the ‘contextual influences’ level. This report synthesises information collected through various evaluation activities as outlined below, and provides an integrated view of the Package from a number of perspectives. Appendix B provides a detailed overview of the ICDP and the evaluation, including the various phases of work and specific activities undertaken or to be undertaken in each of the phases. 1.2 Methodology Several evaluation activities have informed development of this report, including: ten Regional Forums (or equivalent) which brought together a range of
location based stakeholders ranging from senior staff from health departments to service delivery staff to discuss the implementation of the ICDP at a local level and to explore expectations of the Package, progress of the Package and current challenges and issues;
a selection of eight community site visits which involved a range of interviews and focus groups with staff who are directly funded through ICDP, other staff members and managers of organisations which receive some form of ICDP funding, providers who in some way interact with ICDP measures, and Aboriginal and Torres Strait Islander community members;
semi-structured interviews with the departmental staff responsible for the implementation and ongoing management of the various measures (referred to as measure managers);
7 References to organisations including government departments therefore uses names which were in effect during this year.
10KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
interviews with a range of stakeholders including national peak body representatives, each of the National Aboriginal Community Controlled Health Organisation (NACCHO) affiliates, the relevant state and territory based bodies representing general practice, and other key stakeholders (see Appendix C for a complete list);
analysis of program documentation provided by the department; review of the relevant reports of the Sentinel Sites Evaluation; attendance at key events of interest including the Regional Tackling
Smoking and Healthy Lifestyle Team (RTSHLT) workforce training day held in Canberra in December 2011, and a meeting of the Tasmanian Aboriginal Health Reference Group, also held in December 2011; and
analysis of secondary data, including Practice Incentives Program (PIP) Indigenous Health Incentive data, Medicare Benefits Scheme (MBS) and Pharmaceutical Benefits Scheme (PBS) data, data available based on the Health Performance Framework (HPF) and other national surveys and databases, and ICDP program data.
See Appendix C for a more detailed description of the methodologies. 1.3 Structure of this document This report contains a discussion of contextual factors relevant to the ICDP (the ‘contextual influences’ level), an overview of findings for the ICDP overall (the ‘overall Package’ level) and a series of chapters which consider, in detail, the findings relevant to each measure (the ‘individual measures’ level). The structure of these ‘measure chapters’ (chapters through ) is illustrated in the table below. Table 1: Overview of the structure of ‘measure chapters’ in this report.
Measure chapter
Description
‘At a glance’ Overview of the progress of the measure during the 2010-11 reporting period.
Measure overview Description of the measure including its core components and key stakeholders.
‘Core measure component X’
For each of the core components of the measure, a summary finding relevant to the progress of the core component for 2010-11, details of the information/data on which the finding is based, and a discussion of key activities and progress against identified results, based on available evidence.Note: these sections are based on the indicators and evaluation questions within the Evaluation Framework.
11KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Measure chapter
Description
‘Facilitators and barriers’
List of facilitators and barriers identified for 2010-11.
‘Opportunities’ List of opportunities identified to address the barriers and progress of the measure beyond 2010-11.
Appendices have been used to supplement the material in the main body of the report: Appendix A – provides an overview of the ICDP Appendix B – provides an overview of the evaluation Appendix C – provides a detailed description of the methodologies used to
inform this report and a list of stakeholders consulted as part of this report Appendix D – provides an overview of the findings from the Regional
Forums Appendix E – provides an update of the ICDP data collection table Appendix F – provides more detailed information about data analysis
undertaken in the assessment of the Subsidising PBS Medicine Co-payments (B1) measure
Appendix G – provides more detailed information about data analysis undertaken in the assessment of the Higher Utilisation Costs for MBS and PBS (B2)
Appendix H – provides more detailed information about data analysis undertaken in the assessment of the Supporting Primary Care Providers to Coordinate Chronic Disease Management measure (B3a)
Appendix I – provides information about which indicators from the ICDP Monitoring and Evaluation Framework were addressed in the main report
For many of the expected impacts of the ICDP (early and medium-term results), the Evaluation Framework identifies year four as the most appropriate timeframe for consideration of achievement against the suggested indicators. Wherever possible, this report discusses some of the emerging evidence relating to these expected results.
12KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Contextual influencesThe Baseline Report provided an overview of contextual factors, including historical, social, environmental and service access factors, as well as an overview of national and jurisdictional polices that are likely to impact on the ICDP. This chapter provides a discussion of the additional external contextual factors that were identified during the consultations and other evaluation activities undertaken to date. Contextual factors identified can be considered at three distinct levels: local programs related to chronic disease prevention or management; state and territory level agendas; and health system level reforms. In every location in Australia where the ICDP is being implemented, a range of permanent and time limited interventions are in place aimed at reducing the incidence of chronic disease in the Aboriginal and Torres Strait Islander population, and at diagnosing and managing chronic disease to reduce the impact on individuals and the community. Examples identified during the 2010-11 consultations included: The Access Services for Kooris (ASK) program, which is a partnership
between an Indigenous health service (IHS) and Divisions of General Practice in Victoria. ASK aims to address the gap in life expectancy by increasing access to primary health care, improving the cultural competence of mainstream primary care providers and improving Aboriginal and Torres Strait Islander Australians’ understanding of the health care system and chronic disease management. These aims are identical to some of the core aims of the ICDP.
Connecting Care for Chronic Disease in New South Wales, a mainstream severe chronic disease management program through which care coordinators support people with chronic disease to seek health care and manage their condition. In both locations visited for the evaluation in New South Wales, this program was in place within Divisions/Medicare Locals.
These examples illustrate the complex and multi-faceted nature of providing chronic disease related services at a local level, and the many opportunities for both duplication and service fragmentation, and for partnerships and synergies to be developed. Given that the ICDP is only the Commonwealth Government’s contribution to Closing the Gap, each state and territory is also funding a number of initiatives under the jurisdictional implementation plans. Both the ICDP and the individual state/territory initiatives were still being rolled out in 2010-11. As such during this reporting period, some individual organisations were still
13KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
discovering the inter-relationships and overlaps between these two levels of Closing the Gap. While ICDP and these state/territory initiatives for the most part focus on different aspects of the service system, they invariably intersect at either the funded organisation or at the community level. For example in 2010-11, there were state based initiatives that engaged specific communities to improve health risk factors while concurrently, RTSHLTs employed through the ICDP were engaging the same communities on related matters. The task of avoiding duplication and, as far as possible, ensuring that ICDP and state/territory initiatives complement each other was being addressed in some cases in 2010-11 through the state redeploying its resources to avoid duplication, often in consultation with Indigenous Health Partnership Forums (IHPFs). Examples of complementary investment are the funding of brief intervention training by New South Wales and Queensland governments and by some of the Indigenous Tobacco Control Initiative projects. This complementary activity can be expected to support the desired outcomes of the ICDP measures focused on tackling chronic disease risk factors. Consultations also indicated that, in many cases, coordination happens at the organisation level, where multiple workers funded by different levels of government, agencies or even program areas combine to form a coordinated program unit. Examples identified during the 2010-11 consultations included: Care Coordinators from the ICDP Care Coordination and Supplementary
Services (CCSS) measure and Connecting Care Programs undertaking the same tasks within a team based model; and
Aboriginal and Torres Strait islander Outreach Workers (ATSIOWs) funded under ICDP referring patients to Aboriginal Health Workers (AHWs) funded through core department and state and territory programs.
In the Northern Territory, primary health care service delivery was undergoing significant reform in 2010-11, referred to as regionalisation. This agenda included primary health care system development to improve coordination and integration, expansion of current services, enabling community control and Aboriginal and Torres Strait Islander participation in planning and delivery of services, and delivery of health services at a regional or Health Service Delivery Area level.Stakeholders reported that regionalisation, coupled with other significant activity in the Northern Territory in recent years, including the Northern Territory Emergency Response, have had an impact on the capacity of organisations to respond to additional change. The Northern Territory was also
14KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
experiencing significant workforce shortages during this period. This is one significant example of a number of similar initiatives across Australia aiming to strengthen community control, organisational governance and coordination that were operating in 2010-11. Other examples include strategies at the jurisdictional level such as funding for governance training for Aboriginal and Torres Strait Islander organisations (Victoria), and at the regional or local level such as cross-sectoral networking forums (various states/territories).The National Health Reform agenda, and particularly the establishment of the Medicare Local network, is also of significance to the implementation of the ICDP. The magnitude of the changes being introduced into the mainstream primary health care sector during 2010-11 will inevitably impact on the capacity of that sector to respond to other opportunities and priority areas of interest going forward.Some relevant observations noted during Regional Forums and other consultations included: some State Based Organisations (SBOs) and Divisions were unsure of their
future existence and role, and many Divisions were very busy implementing changes to become Medicare Locals and had limited capacity to focus on other aspects of work;
the role that Medicare Locals have in Aboriginal and Torres Strait Islander health represents a changed landscape. While Divisions have always had a role, it is now one of the core responsibilities of Medical Locals;
some IHSs expressed concern that the department may use Medicare Locals as fund holders for new program funding that historically may have been given directly to IHSs;
there was at least one example given in a Regional Forum of the largest IHS in a region not having had any contact with the Division in its application to become a Medicare Local, adding to the mistrust between the two sectors; and
given the planning role that Medicare Locals now have (under their agreement with the department), they have a major role in discussions with state health departments regarding community needs assessments. However, with regard to ICDP, the IHPFs are the department’s main avenue for discussing resource allocation and issues arising from deployment of ICDP resources. Individual Medicare Locals are not on the IHPF and, in some cases, the SBO is not part of the IHPF. Thus, there appears to be a misalignment between the department’s expectation of Medicare Locals with regard to Aboriginal and Torres Strait Islander health and their role in ICDP governance arrangements.
15KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Whole of ICDPThis chapter reports on those matters that are relevant to the entire Package. This chapter draws primarily on the following sources: findings from each of the measure specific chapters (which draw on a
number of sources relevant to each measure); the Regional Forums – an evaluation activity which provided a significant
opportunity to discuss the ICDP at the whole of Package level with a broad range of stakeholders; and
national and state based stakeholders. 1.4 Implementation progress of the Package in 2010-11During 2010-11, the continued roll out of the ICDP progressed largely as planned. As noted in the Baseline Report, this in itself represents an important achievement, given the magnitude and scale of implementation activity. In its second year of implementation, the ICDP: required a considerable investment in workforce across a number of
measures as well as setting up various initiatives to support the new workforce such as training and networking supports;
successfully deployed innovative strategies such as the community based social marketing strategies;
consolidated key measures which had been implemented in 2009-10 including CtG scripts, PIP Indigenous Health Incentive and access to specialist services;
required substantial and effective collaboration between the mainstream and Aboriginal and Torres Strait Islander health sectors, which is critical to addressing local implementation issues; and
has considerable support amongst all stakeholders for its broad direction.There is continued support for the broad direction of ICDP amongst all stakeholders, who also recognise that it will take time to consolidate the various initiatives that will require on-going and effective collaboration across all levels of government and across the various health service sectors. Overall, the majority of stakeholders believe that the ICDP is sufficiently comprehensive and that it will benefit individuals, communities and enhance the service system in the IHS and the mainstream sectors.
16KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.5 Key findings against the evaluation objectives A summary of key findings in relation to the objectives of the evaluation are provided below. Consistency of the implementation with the Commonwealth Implementation Plan
The ICDP has largely been implemented in a manner consistent with the original intent, except in a few cases where expert advice or emerging evidence has provided a strong rationale for a change in design.Synergies among the measures
There are important interdependencies and linkages across the Package, as identified in the Baseline Report. Findings to date indicate that linkages at the local level continue to strengthen as the various measures have been progressively implemented and as stakeholders have increased their understanding of the various measures and recognised opportunities to maximise linkages and synergies. There are significant opportunities for the different measures to leverage off each other and to leverage off other emerging national primary health care initiatives such as the establishment of Medicare Locals. This will require action from the department across its various divisions, at the local level and from peak bodies such as the National Aboriginal Community Controlled Health Organisation (NACCHO) and Australian General Practice Network (AGPN).Appropriateness of individual measures and the Package
Appropriateness is considered from two perspectives, as follows: Appropriateness of the Package to meet target population and stakeholder
needs as determined by the strength of the evidence to support the need for action and the suitability of the action taken. As reported in the Baseline Report, the need for action on addressing chronic disease for Aboriginal and Torres Strait Islander people is clearly demonstrated by the existing evidence, and supported by stakeholders. The evidence supporting the specific approaches to addressing the various components of need (represented by the individual measures) is also available, but less consistently so. While at the broad level, ICDP has been appropriately designed to address community health care needs; there is the opportunity to improve the targeting of ICDP activities. This includes:- continuing to ensure that the deployment of the remaining workforce
elements is in areas of priority need and do not overlap with other existing initiatives;
17KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
- ensuring that local organisations funded under various ICDP initiatives have sufficient flexibility to use the funds to address local needs in the most appropriate manner, particularly in relation to workforce roles and the use of the supplementary services fund; and
- ensuring that funding is used to address priority needs not just to respond to provider availability (this is particularly relevant to the specialist outreach measures).
Appropriateness, defined as awareness, appreciation and satisfaction of the Package as described to us by stakeholders.The evaluation has found that appreciation of, and support amongst stakeholders is strong. Stakeholders report that their understanding of the overarching design of the ICDP has increased since commencement of the Package, as additional ICDP key activities are implemented and begin to operate effectively and have an impact at the local level. Importantly, funded organisations have greater appreciation of the interconnectedness and interdependencies of various measures that are critical to the whole of Package effectiveness. It is to be expected that over time stakeholder views will move away from a focus on concerns about the design and investment decisions, to consideration of the practical implementation based issues and developing solutions to maximise the benefit of the ICDP.
Effectiveness of individual measures and the Package as a whole in delivering the results and outcomes
2010-11 represents the second year of implementation, and for many measures there has been limited progression towards outcomes for individuals and communities, as is to be expected at this early stge. Some measures which have built on previous programs, such as MSOAP-ICD have been able to proceed quickly through the implementation phase to start having an impact faster than those measures which rely on significant lead in time to build a new workforce or change provider behaviours. There is evidence that ICDP as a whole is benefiting individuals and communities and enhancing the service system. The main impacts evident for individuals and communities are: The PBS Co-payment measure, which in 2010-11 exceeded expectations in
terms of the number of people accessing co-payment relief. The PIP Indigenous Health Incentive, which has seen good progress in
terms of practice sign-up and patient registration. The next challenge for the PIP Indigenous Health Incentive is to consider how usage of the sign-up and patient registration payments interact with uptake of the outcomes payments.
18KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The IHPO and ATSIOW teams in both the IHS and the mainstream sectors, which are working effectively with providers and community members in many locations to increase access to primary health care through: community engagement and practical support (such as transport); improving identification of Aboriginal and Torres Strait Islander patients in the mainstream sector; and promoting engagement in the PIP Indigenous Health Incentive and PBS Co-payment measures.
There is a range of emerging evidence that ICDP has resulted in purposeful engagement of the community to address health risk factors. One of the strongest themes coming out of community focus groups was that many people are thinking and talking about chronic disease risk factors like smoking in a way which demonstrates a collective will to move towards healthier choices.
There is a range of emerging evidence that the ICDP has resulted in some Aboriginal and Torres Strait Islander people re-engaging with their local primary health care service in both the IHS and the mainstream sectors. Stakeholders most frequently identify the PIP Indigenous Health Incentive (along with the IHPO and ATSIOW workforce) and the PBS Co-payment as the measures which have been implemented and are having an impact, and this view is consistent with the findings outlined in this report.
The main impacts evident for the service system are: enhanced service delivery capacity which is a direct result of workforce
investment and practice incentives; enhanced capacity and capability for the service system to engage
Aboriginal and Torres Strait Islander communities predominantly through the investment in new types of workforce;
enhanced capability of the existing service system and in particular, improved cultural competency of the mainstream sector and enhanced chronic disease management skills of clinicians and health workers in the IHS and the mainstream sectors;
improved access to existing knowledge and information resources relating to chronic disease management guidelines and best practice through training and networking opportunities created by different aspects of the ICDP; and
improved collaboration between the mainstream and the IHS sectors and between different levels of government.
The potential effectiveness of the ICDP could be impacted by delays in some aspects of the Package and be impacted by the additional time it will take for all aspects to be fully operational. At this stage of the evaluation it seems
19KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
these impacts are more likely to be to delay the full effects of the ICDP rather than to significantly reduce its long-term effectiveness. There are early indications of the factors that will be critical to the long-term effectiveness of the ICDP and that need to be addressed by individual organisations and/or the system as a whole, which otherwise could constrain its effectiveness. These factors are discussed further below under ‘Whole of Package themes’ and will be monitored and reported on in the Second Monitoring Report.1.6 Whole of Package themesDuring the consultations conducted for this report, a number of themes were raised that are of relevance to the whole of package. Specifically, there are three emerging themes that impact the Package as a whole: improving collaboration; workforce related requirements; and sustainability. Improving collaboration
There is consistent evidence that suggests the ICDP has improved collaboration between providers through some of the mechanisms inherent to ICDP and through necessity to ensure that aspects of ICDP could work on the ground. During consultations and Regional Forums, many stakeholders provided examples of improved collaboration both between the mainstream and IHS sector and within each sector. Examples of collaboration resulting from ICDP include: IHPOs are undertaking a range of tasks, such as facilitating joint training
and professional development events, which have contributed to improved collaboration between IHS and mainstream sector stakeholders. Supporting collaboration is a core role of the IHPOs and as such this activity aligns with expectations.
SBOs in some jurisdictions are engaging with Indigenous Health Partnership Forums and their subcommittees around ICDP planning and implementation. SBOs are also working with IHSs to host Care Coordinators.8
SBOs opting to include IHSs as Care Coordination hosts (as in Queensland), and facilitating networking opportunities for staff from both sectors within their jurisdiction.
8 Commonwealth funding of SBOs will cease from 1 January 2013 as a result of funding of Medicare Locals.
20KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Examples of IHSs providing training opportunities and office space for ATSIOWs who are employed through Divisions of General Practice.
Several stakeholders reported that in some cases local implementation of ICDP measures had required that providers work together to ensure that the nationally prescribed requirement is adapted to meet local needs.
The evaluation has also identified a number of barriers to collaboration which exist in some settings. There is a perception that the ICDP has created direct competition between the mainstream and IHS sectors in relation to funding (for example, for ATSIOW funding or for PIP Indigenous Health Incentive), patients (registering patients under PIP Indigenous Health Incentive), and competition for workforce (e.g., where a health worker in an IHS has been employed by the mainstream sector under ICDP). This ‘competition’ has in some cases been detrimental to relationships. Related to this is the emergence of Medicare Locals who have a mandate to focus on Aboriginal and Torres Strait Islander health that has created some concern amongst some IHSs that Medicare Locals may become fund holders for money previously provided by the Commonwealth directly to the IHS.There is also reluctance amongst some IHSs to engage with mainstream organisations due to ideological and historical factors such as the views held by some that mainstream services do not provide appropriate care for Aboriginal and Torres Strait Islander people. The ICDP is underpinned by two important principles. One is that Aboriginal and Torres Strait Islander health is ‘everyone’s business’ and the other being that Aboriginal and Torres Strait Islander people have the right to exercise choice including the choice to use the mainstream sector, hence, the ICDP investment in the mainstream sector as well as the community controlled sector. Amongst state/territory and national stakeholders, views about the value of cross-sector collaboration vary. While some stakeholders view cross-sector collaboration as an essential element and objective of the ICDP, others are concerned that the department is inappropriately controlling and enforcing the terms of engagement. Workforce related requirements
The ICDP has made a considerable investment in the workforce that has seen new types of workforce established, the expansion of the size of the existing workforce and considerable focus on training and development of both the new and existing workforce. In this context, it is not surprising that workforce related requirements have emerged as an important theme across the measures. The Baseline Report discussed both the importance of recognising progress against the workforce elements of the Package and the need for a longer term workforce development strategy to support the elements of the Package.
21KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
All workforce elements of the ICDP have included training and development support strategies that are valued by the employed workforce and their organisations. These strategies include local and national supports aimed at increasing the skills and knowledge of the new workforce groups and providing them with networking opportunities. A number of issues and opportunities were consistently raised by various stakeholders that relate to the following: the provision of appropriate orientation and training; whether ICDP workers are substituting rather than building upon the
existing health workforce; the highly specific nature of some workforce positions; and the cultural safety of Aboriginal and Torres Strait Islander people working in
mainstream organisations. These matters will be explored further in subsequent evaluation reports.Several of the ICDP measures include funding and other provisions for training the ICDP workforce. The provisions for orientation and training vary by position and location. The following specific issues have been raised by stakeholders: Access to orientation, training and networking opportunities. Orientation
and training was built into the design of ICDP (for example, the orientation provision for ATSIOWs through the Workforce Support, Education and Training (C1) measure). Standardised orientation has not been arranged for all ICDP workforce positions, or has been infrequent and therefore not available when it may be of most use to newly appointed workers. Workers consulted consistently reported that when accessible, the centralised training is useful, even if only for networking purposes.
Funding of orientation and training. Funds for training are not consistently available to all ICDP staff. For example, host organisations have been provided with training funds for the National Action to Reduce Indigenous Smoking Rates (A1) and Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) workforce positions, but ATSIOW host organisations (Expanding the Outreach and Service Capacity of Indigenous Health Organisations (C2) and Engaging Divisions of General Practice to Improve Indigenous Access to Mainstream Primary Care (C3)) must access training funds through proposals to the department (submitted via the NACCHO affiliate or SBOs). The design does not include training provisions for some positions at all (for example, IHPOs and Care Coordinators). While these positions require staff to have formal qualifications, it appears that staff still require (value) orientation and training in relation to, for example, application of models of care coordination to Aboriginal and Torres Strait Islander people. It appears that the department has recognised this
22KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
limitation in setting up arrangements for national coordination and networking such as conferences.
The second theme relates to workforce substitution. Many stakeholders have suggested that to some extent, ICDP workers have been sourced from other positions in the Aboriginal and Torres Strait Islander health sector. There are anecdotal examples of AHWs taking up ATSIOW or Tobacco Action Worker (TAW) positions, partly because the pay rate for these positions is sometimes higher than AHW rates. The Sentinel Sites Evaluation Report suggested that some stakeholders feel that the establishment of ATSIOW positions in mainstream settings may be diverting workers from other positions, rather than expanding the workforce overall.9 Such workforce movement may result in unfilled positions elsewhere in the system, and result in substitution rather than genuine workforce expansion. Simple analysis of consultations with ICDP workers undertaken to date indicates that of the 25 ICDP workers interviewed, 14 reported that they had previously been in a health related role, and of those 14, eight reported that they believed there had been delays or difficulties in filling their previous position. This data will continue to be expanded upon throughout the evaluation. The third matter relates to the need for more flexibility in workforce roles and responsibilities to take into account the knowledge base, skills and background of the individual worker and the context of the organisation that employs the worker. The high degree of ICDP role specificity may result in de-skilling of the Aboriginal and Torres Strait Islander workforce and/or not optimising the value of the worker, where workers have skills in addition to those required for the role. For example, the ATSIOW role does not include clinical work, so an AHW recruited to that role may be in danger of losing valuable clinical skills over time. It should be noted that while this issue was raised by several national and state and territory level stakeholders, the evaluation has identified some examples of potentially detrimental substitution (defined here as a worker taking up a lower skill position) occurring in the field. This will continue to be an area of investigation. It should also be noted that some workers may take up lower skilled roles for a range of personal reasons, such as a transition to semi-retirement. This should not necessarily be viewed as a negative outcome, given that their valuable knowledge and skills are being retained in the sector rather than lost altogether. An example of this is a retired Aboriginal male nurse who has taken up a role as a part-time ATSIOW. The organisations funded to recruit different ICDP workers have varying workforce capacity and service models. Stakeholders consistently commented that the role and duties of additional workers need to be adapted to fit their specific organisational context while maintaining the intent of the role of the 9 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
23KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
new type of worker. Some stakeholders have noted that the design of the ICDP workforce positions are too prescriptive and should be modified to fit within an existing team that has a complementary role. Similarly, these stakeholders considered that there should be more flexibility in the use of training supports particularly where organisations have existing staff fulfilling a role similar to that funded by ICDP. For example, organisations that had an existing health promotion team and who received funding for TAWs and Healthy Lifestyle Workers (HLWs) commented that there has been some tension between the existing staff and ICDP funded positions as training activities are offered only to ICDP staff; allowing all staff involved in health promotion (i.e., RTSHLT staff and other workers in similar roles) to attend training activities may mitigate this issue.Finally, some stakeholders have expressed concerns that Aboriginal and Torres Strait Islander people taking up ICDP positions in the mainstream health services sector (ATSIOWs, IHPOs, and Care Coordinators) may experience a culturally unsafe environment. Preliminary findings indicate that many Aboriginal and Torres Strait Islander workers are very satisfied with their employment in mainstream organisations, while a small number reported an absence of active strategies to create a culturally safe environment within these organisations.Sustainability
Sustainability of the ICDP measures has consistently been the subject of discussion by stakeholders, who have indicated that the uncertainty regarding continuity of funding has impacts for workforce recruitment and retention and ongoing engagement of participants. In some cases, stakeholders have indicated that it has been difficult recruiting and retaining workers given the short term nature of the positions. Reportedly, some ICDP workers have vacated positions in order to secure permanent work elsewhere. Health service providers across both the IHS sector and mainstream reported that it can be difficult to engage community members in new programs as there is a general sense that many programs start up for a short time and then lose funding and cease. Community members similarly reported a level of frustration and fatigue associated with the ongoing rollout of time limited programs. Many stakeholders have emphasised their desire that the ICDP investments continue in order to achieve the desired outcomes. Sustained investment is seen as a sign of good faith in the achievements made to date and the long term nature of the desired improvements to Aboriginal and Torres Strait Islander health.
24KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.7 Opportunities The measure specific chapters ( to ) discuss opportunities that are specific to the individual measure. The following opportunities relate to the Package as a whole.Connectivity within the ICDP. There have already been enhanced linkages between different ICDP measures, with the most notable one being linking the workforce elements of the National Action to Reduce Indigenous Smoking Rates (A1) and Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) measures. There are other examples such as promoting the website resources (C5) to all ICDP workforce and the complementary roles of ATSIOWs and Care Coordinators. The department should ensure that all potential linkages between the measures are explored and formalised.Potential examples include: promotion of the Clinical Practice and Decision Support Guidelines (C5) as
the evaluation found that few ICDP stakeholders were aware of this resource; and
encouraging second round grant recipients for the Local Community Campaigns (A3) to link with other ICDP measures to enhance their local campaigns and maximise impact for the community.
Connectivity and collaboration beyond the ICDP. There may be significant opportunities to improve connectivity between the ICDP and other national primary healthcare initiatives in a way which will support sustainability of the ICDP. The most notable example is Medicare Locals, which in addition to hosting and contributing to several ICDP measures, also have a responsibility for community primary health care planning and Aboriginal and Torres Strait Islander health within defined purview. The department could promote the potential benefits of including Medicare Locals in the IHPFs at the national and jurisdictional level as a way of supporting ongoing cross-sector collaboration of ICDP activities and Aboriginal and Torres Strait Islander health more broadly.Ongoing flexibility. Ongoing flexibility to allow locally appropriate implementation of the measures and to respond to emerging policy dilemmas, examples may include more flexible guidelines for use of the Supplementary Services funds, flexibility in the role of various ICDP workforce types to fit in with existing workforce structures and broadening eligibility criteria for the PBS Co-payment arrangements to allow access to patients who do not attend a PIP Indigenous Health Incentive practice.
25KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Workforce development: The ICDP workforce values the networking opportunities that have been organised as part of the ICDP initiative. All ICDP workforce groups expressed a desire for more networking opportunities as an important workforce development activity. Although individual measures have training and networking opportunities in place, development of a strategic approach to promote networking for all workforce components may be warranted. The strategy should consider options to provide more networking opportunities, ways of sharing local innovations that could have relevance for other regions and options for integrating ICDP workforce groups into the broader Aboriginal and Torres Strait Islander workforce.
26KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
National Action to Reduce Indigenous Smoking Rates (A1), and Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2)This chapter describes the progress of the National Action to Reduce Indigenous Smoking Rates (A1), and Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) measures. In this chapter, we discuss findings against activities, outputs and expected results as described in the Evaluation Framework, and barriers, facilitators and opportunities identified to date. The measures at a glance The evaluation found that the National Action to Reduce Indigenous Smoking Rates and Helping Indigenous Australians Reduce Their Risk of Chronic Disease measures were largely ‘on track’ in 2010-11, and a number of key achievements had occurred, relating to workforce recruitment, implementation of program supports, and establishment of a smoke-free workplaces policy by the department. The key activity relating to these measures in the 2010-11 financial year was the establishment of Regional Tackling Smoking and Healthy Lifestyle Teams (RTSHLT) funding agreements and recruitment of staff for these teams. Recruitment was mostly on schedule at the end of 2010-11, with a small gap between the number of positions funded and recruited. Several of the measure’s program supports were successfully implemented during 2010-11, including the National Coordinator - Tackling Indigenous Smoking, development and distribution of resources for workers and rollout of Regional Tackling Smoking Funds. RTSHLTs appeared to value the training and networking opportunities made available to them, and considered access to ongoing training and support as particularly important. The departmental policy linking smoke-free policies to funding agreements10, implemented in 2010-11, promoted discussion and organisational change around smoke-free workplaces, even in locations where no RTSHLT was in place. Analysis of PBS data indicates that there was an increase in uptake of smoking cessation medicines during 2010-11 through pharmaceutical schemes targeted to Aboriginal and Torres Strait Islander people. This could be due to a combination of ICDP (i.e., RTSHLTs and the PBS Co-payment relief measure) and non-ICDP factors. There is evidence that some RTSHLTs have started to promote the use of smoking cessation medicines, and the impact of this is not yet known.
10 Email to KPMG from the Department of Health and Ageing, 2011.27
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Many of the Aboriginal and Torres Strait Islander community members engaged through the evaluation recognised the importance of quitting smoking and adopting healthy lifestyle changes, but indicated that smoking is still a significant problem in communities. Awareness of RTSHLT initiatives amongst community members was variable, most likely due to the fact that many RTSHLTs have only recently been established. 1.8 Potential effects based on implementation findings and Figure 5 below are the causal pathways for these two measures. The causal pathways illustrate the expected outcomes that should occur as a result of the activities of these measures.
National Action to Reduce Indigenous
Smoking Rates
Increase in knowledge and
understanding of the dangers and risks associated with smoking
Reduced smoking rates through a
reduction in new smokers and an
increase in people quitting smoking
Change in attitudes towards taking up
smoking and quitting smoking
Reduced chronic disease risk factors
Recruitment, retention and
capacity building of the
workforce
Supports are effectively
implemented and evidence
based
Individuals and
communities are receptive
to the messages
Individuals and
communities are motivated
to change
28KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Figure 4: National Action to Reduce Indigenous Smoking Rates causal pathway. Source: KPMG.
Helping Indigenous Australians Reduce
Their Risk of Chronic Disease
Increase in knowledge and
understanding of lifestyle related
chronic disease risk factors
Improved uptake of healthy lifestyle
choices
Change in attitudes towards making healthy lifestyle
choices
Reduced chronic disease risk factors
Recruitment, retention and
capacity building of the
workforce
Activities are effectively
implemented and evidence
based
Individuals and
communities are receptive
to the messages
Individuals and
communities are motivated
to change
Figure 5: Helping Indigenous Australians Reduce their Risk of Chronic Disease causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect11 and the observed impacts.12 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. Table 2 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). The measure was modified from its original design to combine the A1 and A2 workforce into a single team. This is likely to enhance the plausibility of effect in 2010-11. Some of the key dependencies for these measures are in place, but there are emerging issues with the time it takes to recruit workers, with building the skills of the workforce, and with
11 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.12 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
29KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
retention. While there are early signs of community receptivity and motivation to change, these are challenged by variation between individuals and established norms. If these persist / are not addressed in future years, the impact of the measures could be constrained.Table 2: Assessment of key dependencies of A1/A2 measures
Key dependencies
Finding Evidence
Recruitment, retention and capacity building of the workforce
Recruitment is on track, but there are emerging issues with the time it takes to recruit workers and with retention. There are also some constraints to building the skills of the workforce.Delays in recruitment are likely to have impacted the momentum of the RTSHLTs’ role.
Qualitative information gathered from a small group of relevant stakeholders, and analysis of data provided by the department on workforce numbers
Supports/activities are effectively implemented and evidence based
Both measure components (RTSHLTs and program supports) were implemented according to plans in 2010-11.
Qualitative information gathered from a small group of relevant stakeholders, analysis of measure documentation and literature review
Individuals and communities are receptive to messages
There is early indication of community receptivity to healthy lifestyle messages, although this is challenged by widely held community norms about unhealthy lifestyle behaviours.
Qualitative information gathered from a small group of relevant stakeholders
Individuals and communities are motivated to change
There are variable levels of motivation amongst community members (to changing lifestyle behaviours) and organisations (to becoming ‘smoke-free’).
Qualitative information gathered from a small group of relevant stakeholders
30KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Finding Evidence
Contextual considerations
Variation amongst individuals and communities is likely to impact on existing behaviour and receptiveness to change and thus the impact these measures can have across locations. For example, Aboriginal and Torres Strait Islander people living in remote areas are more likely to be smokers.13Further, the availability of supports for healthier lifestyles and smoking, which RTSHLTs can refer to, varies across jurisdictions and remoteness areas.14
Analysis of measure documentation and literature review
Table 3 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above).The evaluation has found preliminary evidence for progress against two of the expected impacts: community knowledge and understanding of chronic disease risk factors; and attitudes to smoking and healthy lifestyles. However, at this stage the evaluation is not able to measure change in knowledge or attitudes. The effectiveness of the measure is likely to be impacted by individual and community variations, and the geographical location in which RTSHLTs are operating.
13 Cancer Council Victoria 2012, Tobacco in Australia. 14 As demonstrated in the ‘Policy Map’ within the KPMG Baseline Report: KPMG 2013, Indigenous Chronic Disease Package National Monitoring and Evaluation Project: Baseline Report, Australian Government Department of Health and Ageing, Canberra.
31KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 3: Assessment of expected impacts of A1/A2 measures based on implementation progress.
Expected impact
Observed impact Evidence
Increase in knowledge and understanding of the risks and dangers associated with smoking/of the lifestyle related chronic disease risk factors
At this stage, the evaluation is not able to measure change in knowledge and understanding. The evaluation found a high level of awareness amongst Aboriginal and Torres Strait Islander community members consulted about the risks of smoking and unhealthy lifestyle behaviours, but the majority had not engaged with a RTSHLT.
Qualitative information gathered from a small group of relevant stakeholders
Change in attitudes towards taking up smoking and quitting smoking / to making healthy lifestyle choices
At this stage, the evaluation is not able to measure change in attitudes. There is emerging evidence that Aboriginal and Torres Strait Islander people consulted want to make changes to their lifestyles/behaviours to become healthier (e.g., quit smoking, eat a better diet) but also significant barriers to doing so, including community norms.
Qualitative information gathered from a small group of relevant stakeholders
Reduced smoking rates through a reduction in new smokers and an increase in people quitting smoking / improved uptake of healthy lifestyle choices
Data is not available for the First Monitoring Report.
Not applicable
Reduces chronic disease risk factors
Data is not available for the First Monitoring Report.
Not applicable
32KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected impact
Observed impact Evidence
Contextual considerations
A number of contextual influencers were identified during consultations: Recruitment of RTSHLTs has
been impacted by broader recruitment challenges associated with the Aboriginal and Torres Strait Islander health workforce.
The evaluation found good awareness of the health risks and benefits associated with chronic disease amongst Aboriginal and Torres Strait Islander community members and amongst some people; willingness to change their lifestyle behaviours – this is likely to support the work of the RTSHLTs. In all focus groups community members were able to provide examples of local services to support behaviour change (i.e., that RTSHLTs can refer to) although the number of and choice in services varied; with fewer in remote areas than in urban.
Qualitative information gathered from a small group of relevant stakeholders
1.9 Measure overviewThe National Action to Reduce Indigenous Smoking Rates measure (A1) and the Helping Indigenous Australians Reduce Their Risk of Chronic Disease measure (A2) contribute to the aims of the ICDP by tackling chronic disease risk factors, including smoking tobacco and other lifestyle choices. To assist in distinguishing between the two measures within this chapter, the measures are sometimes referred to by their letter/number codes. Together, these measures are also referred to as the ‘RTSHLT measures’. The National Action to Reduce Indigenous Smoking Rates (A1) measure comprises: A tackling smoking workforce of Regional Tobacco Coordinators (RTCs) and
Tobacco Action Workers (TAWs) - who work with communities to raise awareness of the health impacts of smoking and of smoking cessation
33KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
options. The activities of this workforce are supported by a National Coordinator for Tackling Indigenous Smoking, a grants-based funding program entitled the Regional Tackling Smoking Fund (RTSF), resources for program delivery, and funding for training/upskilling of the workforce.
National level supports for smoking cessation - these include a smoke free workplace policy for the IHSs sector, training programs for the Aboriginal and Torres Strait Islander tobacco workforce, funding to support the national anti-smoking campaign, Break the Chain, and tobacco cessation research projects.
The Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) measure funds a workforce of Healthy Lifestyle Workers (HLWs) to promote healthy lifestyle choices related to nutrition and physical activity amongst Aboriginal and Torres Strait Islander people. The two measures were originally designed as distinct measures, with Regional Tackling Smoking Teams (RTSTs) comprising the workforce component of A1, and Healthy Lifestyle Workers (HLWs) comprising the workforce component of A2. However, at the local level, HLWs have been integrated with the RTSTs to promote, support and improve collaboration to enhance outcomes. RTSHLTs are now composed of a combination of a Regional Tobacco Coordinator (RTC), Tobacco Action Workers (TAWs) and HLWs. Therefore, these two measures have been addressed together in this report.In 2010-11, the joint expenditure on the RTSHLT measures was $24.781 million.
34KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 4: Actual expenditure, A1 and A2 measures, 2010-11.15
Measure Actual expenditureA1 measure $18.022mA2 measure $6.759m
Total $24.781m
1.10 Research supporting the RTSHLT measuresThe research conducted as part of the RTSHLT measures was undertaken in 2009-10. The evaluation has found that this research strongly influenced the design of these measures.This finding has been informed by review of research and measure documentation provided by the department, and consultations with the department and Ipsos Social Research Institute. During 2009-10, the department contracted Carroll Communications to undertake a literature review and stakeholder consultations on tobacco control social marketing approaches for Aboriginal and Torres Strait Islander communities.16 The department also contracted Ipsos-Eureka (now Ipsos Social Research Institute) and Winangali Pty. Ltd. to conduct and report on ‘Developmental research to inform the National Action to Reduce Smoking Rates Social Marketing Campaign.’17 A number of specific features of the RTSHLT measures were refined as a result of this research, with the majority of changes being made to the A1 measure due to the focus of the research being on tobacco control. For example, in recognition of the research findings that mainstream media is frequently accessed by Aboriginal and Torres Strait Islander people, the social marketing components of the A1 measure now utilise mainstream media in addition to Aboriginal and Torres Strait Islander specific media. In addition, the focus of social marketing under the A1 measure is based on findings about the types of messages which may be most effective in communicating with Aboriginal and Torres Strait islander people, such as emphasising the impact of smoking on family members and negatively impacting on sporting performance. The recommendation to augment other strategies under the measure by
15 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [A1/A2 response].16 Carroll Communications 2009, Health promotion and social marketing interventions addressing tobacco smoking in Indigenous Communities: Time for moving forward, Department of Health and Ageing, Canberra.17 Ipsos-Eureka Social Research Institute 2010, Developmental Research to inform the National Action to Reduce Smoking Rates Social Marketing Campaign, Department of Health and Ageing, Canberra.
35KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
implementing shared smoking cessation activities, including smoke-free workplace initiatives, has also been taken up.18 1.11 Regional Tackling Smoking and Healthy Lifestyle Teams
(RTSHLTs) Recruitment
Recruitment of staff for the RTSHLTs19 was a key focus during 2010-11. The evaluation has found that recruitment is largely on track, with a small gap between the number of funded and recruited workers. Most notably for some jurisdictions and in major cities, some challenges and concerns relating to recruitment were evident that resulted in delays in staff commencing their work as part of the RTSHLT. This finding has been informed by analysis of data and documentation provided to the evaluators by the department, consultations with community and departmental stakeholders, Regional Forums and analysis of the 2010-11 Sentinel Sites Project Report.20
RTSHLT funding agreements
Information provided by the department indicates that 22 organisations were funded for the RTSHLT measures as at 30 June 2011.21 These organisations were identified as priority areas within each jurisdiction, in consultation with the Indigenous Health Partnership Forums (IHPFs). In some cases, there was a staged implementation of the full RTSHLT, with initial recruitment of workers to establish the core team and plans to recruit the balance of the team at a later date. Wherever possible, IHSs (usually community controlled organisations) host the RTSHLTs. However, in some cases the teams are hosted by other organisations with strong links to Aboriginal and Torres Strait Islander communities such as Divisions of General Practice/Medicare Locals. Analysis of the workforce location report indicated that 80 per cent (16 of the 20) of RTSHLT contracted organisations were IHSs in 2010-11. All of the RTSHLTs engaged through community site visits in 2010-11 (three teams in total comprising 9 people) were placed in IHSs.
18 ibid.19 These positions are targeted towards Aboriginal and Torres Strait Islander people, but not ‘identified’ (i.e., Aboriginal and Torres Strait Islander people only) positions.20 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.21 Based on workforce location report provided by the Department of Health and Ageing.
36KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
In 2010-11, some RTSHLTs were placed in organisations with existing tackling smoking and health promotion capacity, such as health promotion staff, allied health workers (with a focus on healthy lifestyles such as nutritionists) and (in IHSs only) GPs who can prescribe smoking cessation medicines.22 Two of the three RTSHLT fund holder organisations engaged through community site visits had either existing health promotion or tackling smoking activities in place when the teams came on board in 2010-11. In the majority of cases, 2010-11 funding was provided as part of the 2010-11 OATSIH core funding agreement, and included funds for staffing, vehicles, training, and rural/remote loading. The RTSHLTs could also access the Regional Tackling Smoking Fund (subject to submission and approval of a business case)23 – another component of the RTSHLT measures. Related to the 2010-11 year, fund holders were expected to deliver a number of plans and reports to the department, identifying their planned and completed activities, and performance against their budget. Business cases for the Regional Tackling Smoking Fund were also required to be submitted in 2010-11.
RTSHLT recruitment
The data provided in the following tables is drawn from workforce data provided by the department. The following points need to be noted when interpreting this data: differences between allocation and recruitment may be due to late
allocation of positions in the financial year; and recruitment numbers may be low due to turnover of staff.Table 5 below summarises the workers recruited in 2010-11, a total of 64 workers. Table 5: Number of RTC, TAW and HLW workers recruited, 2010-11.24
Position Number recruitedRegional Tobacco Coordinators
17
Tobacco Action Workers 17Healthy Lifestyle Workers 30
22 Note – some RTSHLTs are places in Medicare Locals which do not provide GP services as do IHSs.23 A fund that provides up to $100,000 (GST exclusive) annually to fund holders for projects related to tobacco reduction – this is discussed further in section .24 Based on workforce location report provided by the Department of Health and Ageing.
37KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 6 below compares the total number of positions funded in 2010-11 with the total number of positions recruited in the same period. As this table shows, there was a difference of nine Full Time Equivalent (FTE) for the National Action to Reduce Indigenous Smoking Rates (A1) measure (with a total of 43 staff funded and 34 recruited) and 13 FTE for the Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) measure (with a total of 43 staff funded and 30 recruited). Table 6: Number of FTE funded and recruited RTC, TAW and HLW positions for 2010-11.25 26
Measure Funded RecruitedA1 43 35 (17TRC, 17 TAWs)A2 43 30 (HLWs)
The jurisdiction with the most significant gap between funded and recruited positions was New South Wales, where approximately one-third of the positions funded were recruited. The Northern Territory and South Australia also fell short of their funded recruitment by two positions for both the A1 and A2 measures in 2010-11.Table 7 and Table 8 below contain the number of FTE funded and recruited RTSHLT workers broken down by remoteness. The data in these tables show that in 2010-11, 28 per cent of funded positions were in remote and very remote areas and the remaining 72 per cent were in major cities and regional areas (inner and outer).Table 7: Remoteness breakdown for number of FTE funded and recruited RTC, and TAW positions for measure A1 2010-11.27
ASGC Remoteness
2010-11 FTE Funded
2010-11 FTE Recruited
Major Cities 15 11Inner Regional 6 5Outer Regional 10 8Remote 6 4Very Remote 6 6Total 43 34
25 Based on workforce location report provided by the Department of Health and Ageing.26Note: no quarterly data was available to the evaluation to enable analysis of the impact of timing on these gaps between the number of staff funded and recruited.27 Based on the workforce location report provided by the Department of Health and Ageing.
38KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 8: Remoteness breakdown for number of FTE funded and recruited HLW positions for measure A2 2010-11.28
ASGC Remoteness
2010-11 FTE Funded
2010-11 FTE Recruited
Major Cities 15 8Inner Regional 6 4Outer Regional 10 9Remote 6 4Very Remote 6 5Total 43 30
The data on recruitment by remoteness suggests that recruitment, in line with the number of funded positions, was strong in regional (inner and outer), remote and very remote areas in comparison to that in major cities in 2010-11. This contrasts with reports from some stakeholders and literature29 which suggested that recruitment was more difficult in remote locations than urban locations. It also contrasts with the findings of the Sentinel Sites Project which found that, in the Sentinel Sites during 2010-11, “On balance, progress with recruitment to the RTC and TAW positions appeared to be more advanced in remote and urban sites than in regional sites.”30 This issue will be an ongoing area of investigation for the evaluation.
Recruitment challenges
While overall recruitment is largely on track, organisations consulted during the evaluation commented on two issues. The first relates to the time it takes to recruit and the second relates to retaining staff.Some organisations consulted during community site visits reported that they had experienced difficulties in recruiting RTSHLT staff, resulting in delays in the RTSHLT workers coming on board. Most of these stakeholders acknowledged that these recruitment difficulties were likely to be symptomatic of the broader challenges encountered in recruiting to the Aboriginal and Torres Strait Islander health workforce. This view was 28 Based on the workforce location report provided by the Department of Health and Ageing. 29 Australian Institute of Health and Welfare 2010, Aboriginal and Torres Strait Islander health services report, 2008-09, OATSIH Services Reporting – key results, Cat. no. AIHW 31, AIHW, Canberra; Stephens BJ 2010, ‘The Determinants of Labour Force Status among Indigenous Australians’, Australian Journal of Labour Economics, vol. 13, no. 3, pp. 287-312.30 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
39KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
supported by the literature, which showed broad reaching difficulties in recruiting staff to work in Aboriginal and Torres Strait Islander health positions.31 This view was consistent with the difficulties reported in recruitment of workers for other ICDP measures (see chapters , and and specifically). This suggests recruitment difficulties were not specific to the RTSHLT measures. A number of Regional Forum participants and community based stakeholders consulted during 2010-11 raised concerns about sustainability of the ICDP, both in terms of specific measures and the workforce. The main factors often identified by stakeholders as contributing to difficulties recruiting workers were: a lack of long-term certainty about funding and therefore employment
tenure. All positions funded under National Action to Reduce Indigenous Smoking Rates (A1) and Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) measures are based on 12-month contracts (although the intention is that the positions will be funded for the duration of the ICDP); and
movement of the workforce – with the common concern being that the attractiveness of RTSHLT and other ICDP workforce positions (e.g., in terms of their remuneration and benefits), and the resulting movement of existing health workers to these positions, would lead to gaps in the workforce in other areas. While this was raised by organisational representatives as an issue, only one of the 10 RTSHLT workers consulted considered that there had been negative impacts on other programs or workforce groups as a result of the movement of workers to RTSHLTs in 2010-11.
RTSHLT training and capability building
The evaluation found that in 2010-11, the ICDP-sponsored national opportunities for training, networking and skill development for RTSHLTs were highly valued components of the RTSHLT measures. The evaluation is unable to meaningfully report on the generalised experiences of RTSHLTs across Australia in terms of participation in training due to the small number of teams engaged during the 2010-11 site visits, and the fact that program documentation identifying which RTSHLTs had participated in the training was not available. However, based on the available information, it appears that RTSHLT staff have received a mix of local and national training support (the
31 Lyle D & Kerr C 2001, ‘Building capacity in rural health’, NSW Public Health Bulletin, vol. 12, no. 6, pp. 159-161; Australian Institute of Health and Welfare 2011, The health and welfare of Australia’s Aboriginal and Torres Strait Islander people an overview, AIHW, Canberra; Australian Institute of Health and Welfare 2010, Aboriginal and Torres Strait Islander health services report, 2008-09, OATSIH Services Reporting – key results, Cat. no. IHW 31, AIHW, Canberra.
40KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
extent of which is unknown), but there appears to be some constraints that have limited the access that RTSHLT staff had to training in 2010-11. These findings have been informed by consultation with community, national and departmental stakeholders, Regional Forums and analysis of the 2010-11 Sentinel Sites Project Report.32
RTSHLT participation in training and networking
The department has provided fund holders with specific funding and supports for training the RTSHLT workforce. These supports focus on ensuring: RTSHLTs participate in national induction training and other national
workshops to complement organisational induction which fund holders are expected to provide – the department provides national induction and training/networking opportunities for RTSHLTs annually;
fund holders meet the specific requirement for RTSHLTs to obtain certificate level qualifications (RTCs are required to have, or be working towards, a Certificate IV qualification in a relevant discipline while TAWs and HLWs are required to have, or be working towards, a Certificate III qualification in a relevant discipline33) the department has provided specific funding to fund holder organisations to support this; and
RTSHLTs have access to other relevant training to complement their skill needs – again, the department has provided specific funding to fund holder organisations to support this.
The department requires training pathways for each worker to be documented in an individual training plan developed within the host organisation. In 2010-11, the department ran two national forums for the workforce. In December 2010, a national workshop was held in Canberra to provide induction training and build networks across the workforce. The workshop was attended by the new RTSHLT workforce and relevant representatives from the fund holders (e.g., CEOs and Population Health Managers) and was chaired by Dr Tom Calma, National Coordinator - Tackling Indigenous Smoking. Specific training on tobacco cessation was provided at a second forum by the Centre for Excellence in Indigenous Tobacco Control (CEITC, Melbourne University) and on healthy lifestyles by Health Infonet (Edith Cowan University).Only a small number of RTSHLT staff were interviewed as part of community site visits; 10 staff in total working across three RTSHLTs. Workers in two of these RTSHLTs had participated in training since being recruited, which
32 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.33 Relevant disciplines may include courses such as Population Health, Preventative Health, Aboriginal Health Work, Aboriginal and/or Torres Strait Islander Primary Health Care
41KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
included national workshops (e.g., national induction), training focused on smoking cessation (e.g., smoke check, brief interventions training) and training in public health as part of a certificate level qualification. All RTSHLTs had plans to undertake further training in the future. A strong message from consultations with all three RTSHLTs that were consulted was that access to networking and training opportunities was highly valued. The opportunity to meet other workers, share ideas and stories and create relationships, which could be leveraged to exchange ideas and provide support throughout the year, were seen as particularly valuable. Linked to this, most RTSHLT workers engaged through the site visits reported that ongoing support and mentoring from within teams, the organisations they were employed by and at the jurisdictional level (for example, the RTC in the NACCHO affiliate) was critical to the ongoing development of knowledge, skills and, in particular, confidence in their role. Similarly, the Sentinel Sites Project34 found that the team-based deployment of RTSHLT workers was viewed positively.
Training and support requirements
Regional Forum participants commented that insufficient information was available during the ICDP implementation period regarding the roles of ICDP workers including RTSHLTs and, related to this, there were either delays in or insufficient access to training opportunities for newly recruited staff. Consistent with this, no workers within one RTSHLT engaged through the community site visits had undertaken any training despite being in place for nearly nine months. The Sentinel Sites Project35 also found that training had not been made widely available to RTSHLTs due to the workforce still being in the early stages of recruitment in 2010-11. Some of the other RTSHLT workers engaged during the site visits reported experiencing restrictions in the amount of training in which they could participate due to financial constraints within their organisation, and difficulties finding time to attend training due to competing priorities associated with their role.In addition, workers engaged through the site visits identified a number of areas in which they would like further training. Largely these ‘gaps’ were similar to the areas of training RTSHLT workers had already accessed, for example training in smoking cessation, public health, and how to embed smoke-free cultures within workplaces. This suggests that participation in only ‘one off’ training may not be sufficient to address the skill requirements 34 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.35 ibid.
42KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
of some of these entry level positions. All of the RTSHLT workers engaged through the site visits reported that ongoing training opportunities would be welcomed, and some RTSHLT workers thought the additional training would boost their confidence in performing their role. One suggestion was for the creation of a website to share ideas and examples of good practice. This is currently being progressed by the department through the inclusion of a password protected section of the website where workers can engage with one another. The importance of support for Aboriginal and Torres Strait Islander people in these roles was further highlighted by one worker, who reported that working to change deeply entrenched community behaviours (such as smoking) can be personally challenging and can expose the individual to some criticism and a sense of isolation within their community. This has the potential to contribute to poor retention of the workforce over time. Regional Forum participants identified opportunities to improve the training available for staff through ICDP by improving coordination, consistency and targeting future training content to actual needs as identified by the sector (which was based on information available from the site visits included, but was not limited to training in: smoking cessation; public health; embedding smoke-free workplaces; and clinical skills). RTSHLT workforce program supports
The evaluation found that in 2010-11, a number of program supports were successfully implemented for RTSHLTs, namely: the Regional Tackling Smoking Fund; the National Coordinator - Tackling Indigenous Smoking; and development and presentation of resources and support materials relevant
to the teams’ activities. This finding has been informed by a review of documentation provided by the department and consultations with community, departmental and national stakeholders involved in the implementation and operation of these program supports. The Regional Tackling Smoking Fund provides up to $100,000 (GST exclusive) annually to fund holders for projects related to tobacco reduction. Organisations can submit their business cases to access funds from the Regional Tackling Smoking Fund at any time throughout the year.In 2010-11, 13 of the 22 fund holders applied to the National Coordinator Tackling Indigenous Smoking for use of the Regional Tackling Smoking Funds. The funded projects delivered in 2010-11 ranged in their focus. Examples of
43KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
projects or items funded through the Regional Tackling Smoking Fund in 2010-11 included: purchasing localised TV and radio advertising; running smoke-free sporting events that also promote health checks; setting up a trailer for mobile health promotion activities; providing smoke-free healthy living expos with role models; equipment such as Smokey Sue Smokes for Two dolls (a jar with a doll’s
head on top and a foetus inside which can smoke a cigarette and as it burns the fluid around the foetus turns darker); and
development of animations and video clips posted on YouTube and Facebook.
One project considered to be particularly successful by stakeholders engaged through community site visits was the development of the resource guide, “Deadly Choices,” by the Institute for Urban Indigenous Health. This resource is intended to provide guidance for delivery of community based health events, such as those that provide health checks. A number of community stakeholders engaged through the site visits were aware of this resource and/or had used it. The position of National Coordinator - Tackling Indigenous Smoking was established by the department in 2010-11 and is held by Dr Tom Calma. The role of the National Coordinator is to provide strategic and national support and to contribute to increasing the knowledge and skills of the workforce over time, through both leadership and mentoring activities.36 The National Coordinator used a variety of events to network with RTSHLTs to emphasise a number of key messages: the RTSHLT workforce should not be duplicative of existing services and
programs at the organisational level, but should be working with their organisations to identify and delineate activities and responsibility; and
there is a need to maintain key features of the program design to ensure that TAWs are not being absorbed into generalist AHW type activities.
The importance and impact of this national leadership role was evident during the site visits. TAWs at two community site visits emphasised these messages during consultations, and provided examples of how their activities were aligning to the program intent (e.g., delivery of community wide events rather than specific programs).
36 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [A1/A2 response].
44KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The final example of successful implementation of program supports relates to the development of resources for use by the RTSHLT workforce as follows: CEITC was contracted under a three-year funding agreement to provide
supports including development and delivery of induction training for the RTSHLT workforce and organising the biennial symposia on Aboriginal and Torres Strait Islander people tobacco control.
In May 2011 in Adelaide, the department brought together the RTSHLTs with the funding recipients from the Local Indigenous Community Campaigns to Promote Better Health (A3) measure to jointly learn about social marketing and the use of the Community Health Action Pack, a Local Indigenous Community Campaign to Promote Better Health (A3) resource that guides health promotion activities in Aboriginal and Torres Strait Islander communities.
Edith Cowan University was engaged in 2010-11 to prepare resource materials and induction training for the HLWs.37 In late 2010, the “Healthy, Deadly and Strong: Healthy Lifestyle Worker Toolkit” was released by Edith Cowan University.
Finally, in 2010-11, the department provided the workforce with two key materials to enhance their knowledge and to support their skills development. These were the Guidebook on Nicotine Replacement Therapy and the RTSHLT website.
RTSHLT activitiesThe three RTSHLTs engaged in the 2010-11 site visits had undertaken a broad range of activities. While these teams are situated in different areas of remoteness (both urban and regional locations), there was consistency in the types of programs and services being provided across the RTSHLTs, as Table 9 below shows. Table 9: Summary of types of activities RTSHLTs have undertaken.38
Type of activity Examples of programs and servicesSmoking cessation Individual interactions such as brief interventions with
community membersGroup interactions such as anti-smoking workshops
Delivery of healthy lifestyle programs
Group interactions such as walking groups, exercise sessions
37 Department of Health and Ageing, 2010, Commonwealth’s Indigenous Chronic Disease Package Update, 10th edition, Department of Health and Ageing, Canberra.38 Based on information gathered through community site visits.
45KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Type of activity Examples of programs and servicesEvents Attending community events to engage the community
Displays/stalls at events to promote healthy lifestyle messagesRunning sporting events
Resource development Developing and distributing health promotion materialsDeveloping and distributing information brochures about ICDP
Liaison Assist community members with linking to a primary health care provider for health checks and smoking cessation medicines
Working with other organisations
Developing partnerships with local primary health care organisations (e.g., Medicare Locals), local government, and other local organisations (Aboriginal and Torres Strait Islander and mainstream)Working with partners to promote NRT and to deliver common anti-smoking messages
The activities of the three RTSHLTs engaged were focused on both tobacco cessation and healthy lifestyles and included a mix of group/event based activities and individual interactions. Participants in the Regional Forums had strong expectations that RTSHLT activities would result in improved community member understanding of the health risks and benefits associated with chronic disease. Participants also expected that this increased understanding would lead to decreased smoking amongst community members and amongst Aboriginal Torres Strait Islander health workers.In addition to these activities, RTSHLT workers commented that they were forging successful partnerships with other organisations, with one team working to support the uptake of MBS Health Assessments amongst Aboriginal and Torres Strait Islander community members, a specific Key Performance Indicator for HLWs.Data on the number of Health Assessments provided in 2010-11 is presented in Chapter and Appendix G. In summary, the number of MBS Health Assessments for Aboriginal and Torres Strait Islander people (Item number 715) increased significantly between 2009-10 and 2010-11. However, it is not possible at this stage to estimate the extent to which this increase can be attributed to the ICDP, nor specifically the RTSHLT measures. Community participation in RTSHLT activities
No national data was collected on participation in RTSHLT activities by community members in 2010-11, and the three RTSHLTs consulted though the
46KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
community site visits were not collecting site level data at the time these visits were conducted. As such, it is not possible to comment meaningfully on the level of participation in RTSHLT activities by community members during 2010-11.However, two of the three RTSHLTs engaged through the site visits noted that community engagement with their programs and services was increasing. In addition, the same two RTSHLTs noted that there was increasing community interest in their programs and services, as indicated by community members more frequently talking to the team members about smoking/healthy lifestyles, and asking them for information. Improvements in understanding - health risks and benefits
The work of the RTSHLTs is expected to result in improvements in community members’ understanding of both health risks associated with smoking, and health risks and benefits associated with nutrition, alcohol use and physical activity. The evaluation found evidence that community members were generally aware of health risks and benefits associated with chronic disease. However, due to the limited exposure that the community members have of RTSHLTs, this knowledge and awareness cannot be attributed to the RTSHLT measures. This finding has been informed by community consultations, Regional Forums and analysis of the 2010-11 Sentinel Sites Project Report. All community focus groups undertaken during 2010-11 asked participants specific questions about smoking and other lifestyle choices. The vast majority of participants in these focus groups reported that they (and other Aboriginal and Torres Strait Islander people in the community) were aware of the dangers of smoking, poor nutrition and lack of exercise and that, as a result of this understanding, their attitudes (towards smoking in particular) had changed in recent years. There did not appear to be significant differences across urban, regional and remote sites in terms of this broad understanding. The common themes that arose during the focus groups were: smoking was a big problem in the community; less people were smoking, but still too many; more people were trying to quit people perceived the main reasons for
quitting to be the expense (of purchasing cigarettes), health messages and seeing family and friends getting sick;
community smoking rates were reducing somewhat and people were a lot less likely to smoke in homes and cars;
47KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
some people were eating healthy food, but a number of people were still eating too much take-away and junk food;
young people had access to a number of options for sport but there were not as many options for older people (although some sites reported several new programs starting up to address this, none were directly as a result of ICDP); and
the cost of registration fees (for organised sports), gym memberships and equipment was a problem for many families (although similarly, some sites reported new initiatives to address this such as subsidised gym memberships).
The majority of community focus group participants across all areas of remoteness saw smoking as a significant problem amongst Aboriginal and Torres Strait Islander people. There was a general perception that people wanted to make changes to their lifestyles or behaviours to become healthier (e.g., quit smoking, eat a better diet) but that there were barriers to doing so. This perception was common across urban, regional and remote area focus groups.In urban areas, community members discussed barriers around ready availability of junk food and limited access/opportunities to participate in sport and exercise. Distinctly, a common barrier raised in regional and remote areas was difficulties accessing fresh, healthy food, and such food being unaffordable. Access to sporting and exercise opportunities such as organised walking groups and team games, was reportedly easier in regional areas than in urban and remote areas. Participants commonly drew direct links between access to primary health care and the impacts of this on chronic disease. For example, a number of participants articulated the importance of going to the GP for people with a chronic disease to obtain assistance in managing the chronic disease. Many participants also discussed access to medication as important for people with chronic diseases such as diabetes and heart disease. Participants less commonly made specific links between lifestyle behaviours and the impact of these behaviours on chronic diseases. The only common link made across focus groups was between diabetes and ‘sugar’. It is important to note that the community focus groups can only provide limited insight into the impact of RTSHLTs on influencing community understanding of health risks and benefits. This is because participants at only one community focus group were aware of a RTSHLT in their region (this is explained further in the following section) and the fact that RTSHLTs that were engaged during the 2010-11 site visits had not been providing their tackling smoking and healthy lifestyle activities for long period of time.
48KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The above findings are consistent with those of the Sentinel Sites Project that reported there is a high level of interest amongst community members to quit smoking and a high level of awareness that smoking is associated with negative health outcomes. The Sentinel Sites Project further found through the community focus groups that often community members had a good awareness about what constitutes a healthy lifestyle, but were less able to make direct links between healthy lifestyle and chronic disease. 39 Improvements in understanding and access – resources
RTSHLTs are expected to inform community members of, and link them to, relevant resources that would support them to quit smoking and lead healthier lifestyles. The evaluation found that community members were aware of the availability of resources for smoking cessation and healthy lifestyle choices. However, the majority of resources identified were not part of the ICDP. This finding has been informed by consultation with Aboriginal and Torres Strait Islander community members through community focus groups. Participants in all community focus groups conducted in 2010-11 could identify one or more relevant resources available in their local area. However, community focus group participants primarily indentified resources that were not solely associated with the ICDP, such as: smoking cessation pharmaceuticals; support based programs delivered through IHSs (provided by non-RTSHLT
workers); and dieticians who people could see through their IHS or mainstream services
(usually associated with someone being diagnosed with diabetes). Community focus group participants across urban, regional and remote locations were able to identify such resources, and the types of resources identified were fairly consistent across types of locations (i.e., urban, regional, remote). Only one focus group identified the support provided by a TAW as a ‘relevant resource’. This may be reflective of the fact that, of the eight sites visited, RTSHLTs were present in only three. Improvements in assistance seeking – smoking cessation medicines
RTSHLTs are expected to inform community members of, and link them to, relevant resources that would support them to quit smoking. This includes services through which individuals can access smoking cessation medicines. The RTSHLTs have no clinical role in prescribing or dispensing medicines. The
39 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
49KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
evaluation found that in 2010-11, awareness of, and access to, smoking cessation medicines through Aboriginal and Torres Strait Islander targeted pharmacy schemes was increasing. However, it is not possible at this stage to specifically identify the role of RTSHLTs in this increased awareness, and further, this awareness does not necessarily translate to an increased uptake of smoking cessation medicines. This finding has been informed by community site visit consultations, and analysis of secondary data on access to smoking cessation medicines by Aboriginal and Torres Strait Islander people through the PBS Co-payment subsidy (CtG scripts) and Section 100 Remote Area Aboriginal Health Services Program (S100 RAAHS)40 schemes. A broad range of smoking cessation medicines are available to Aboriginal and Torres Strait Islander people, including over the counter NRT such as patches and chewing gum, and prescription only medicines including NRT and other smoking cessation medicines such as Varenicline Tartrate (Champix). An increase in the number of Aboriginal and Torres Strait Islander people who seek assistance through smoking cessation medications is likely to impact on: the sales of over the counter NRT; the number of full co-payment PBS scripts41 for smoking cessation medicines dispensed; and the number of subsidised or free scripts dispensed under subsidisation schemes, such as the CtG scripts and S100 RAAHS. In light of this, trends in the uptake of smoking cessation medicines, and factors potentially influencing this uptake amongst the Aboriginal and Torres Strait Islander population, are discussed below. Specifically, this section presents: a discussion of the range of ways in which Aboriginal and Torres Strait
Islander people who smoke can access smoking cessation medicines and how these have changed over 2010-11;
data on the utilisation of smoking cessation medicines dispensed through schemes that are specifically for Aboriginal and Torres Strait Islander people (S100 RAAHS and CtG scripts);
40 Under the S100 RAAHS, Aboriginal and Torres Strait Islander patients residing in certain areas are able to receive PBS listed medicines free of charge. The S100 RAAHS PBS supply arrangements for Indigenous health services do not require the provision of individual patient medicine dispensing records to Medicare Australia. PBS medicines are supplied in bulk to an approved IHS and are provided to patients with no co-payment charge and without the need for a PBS prescription. See: Department of Health and Ageing (no date), Alternative Arrangements for Medicines, Aboriginal Health Services and Pharmaceutical Benefits Scheme (PBS). 41 This includes PBS and Regional Pharmaceutical Benefits Scheme (RPBS) scripts, which are supplied to both Aboriginal and Torres Strait Islander people and non-Aboriginal and Torres Strait Islander people.
50KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
an assessment of the observed change in use of the above scripts and the extent to which this represents an increase in the use of smoking cessation medicines by Aboriginal and Torres Strait Islander people;
a comparison with the utilisation of smoking cessation medicines by non Aboriginal and Torres Strait Islander people who smoke as a benchmark for rates of uptake of smoking cessation medicines;
a discussion of the factors that could influence any observed change; and a discussion of the limitations of this analysis.
Subsidy schemes for Aboriginal and Torres Strait Islander people
One factor which is likely to influence the uptake of smoking cessation medicines amongst Aboriginal and Torres Strait Islander people is subsidisation schemes. Subsidisation of smoking cessation medicines has been operating independently of the ICDP since 2008 as part of the Smokecheck program 42.
Under this initiative, Aboriginal and Torres Strait Islander people were eligible for two 12 week courses of 15 mg per 16 hours NRT (patches) for free. Free smoking cessation medicines have also been available through the S100 RAAHS scheme since 1999. Through this scheme, PBS medicines are supplied to eligible IHSs and are provided free of charge to Aboriginal and Torres Strait Islander people in remote areas. Since the implementation of the ICDP, subsidisation of smoking cessation medicines has operated in an expanded form whereby people registered for CtG scripts (B1 measure) have access to prescription smoking cessation medicines such as nicotine patches43, Varenicline Tartrate and Bupropion (Zyban) with a full or part subsidy of the co-payment.Data is thus presented below on the dispensing of CtG and S100 RAAHS smoking cessation scripts in 2010-11. Over the 12 months to 31 May 2011, a total of 2,572 smoking cessation scripts were dispensed to patients under the CtG scripts measure (see Table 10 below).
42 National Prescribing Service 2008, In Brief A digest of news items about NPS RADAR, new drugs and changes to PBS listings.43 These include Nicorette 15mg for 16 hours and Nicabate P 21 mg for 24 hours. Source: Department of Health and Ageing 2012, Medicines to Help You Stop Smoking, Commonwealth of Australia, Canberra.
51KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 10: Number of smoking cessation CtG scripts dispensed by jurisdiction from August 2010 to May 2011 quarters.44 45
Jurisdiction Number of smoking cessation CtG scripts
New South Wales / Australian Capital Territory 1,289Queensland 431Western Australia 176Northern Territory 15Victoria 372South Australia 228Tasmania 61Australian Total 2,572
At the national level, the number of smoking cessation CtG scripts dispensed grew from 172 in the August quarter 2010, which was soon after the CtG scripts measure was introduced, to 1,341 in the May quarter 2011. The total number of smoking cessation scripts (2,572) represents four of every 1,000 CtG scripts dispensed over this period. As noted previously, smoking cessation medicines are also supplied free of charge through S100 RAAHS. S100 RAAHS data shows that a total of 4,027 smoking cessation medicines were supplied to Aboriginal and Torres Strait Islander people between June 2010 and May 2011. As the figure below shows, there was a decrease in the number of smoking cessation scripts supplied each quarter through S100 RAAHS since June 2010.This decrease in S100 RAAHS smoking cessation scripts across 2010-11 was accompanied by an increase in CtG scripts dispensed, although the information is not available to determine whether these two changes are related. When CtG and S100 RAAHS scripts are considered in conjunction, a total of 6,599 smoking cessation medicines were supplied and/or dispensed for smoking cessation that can be identified as potentially utilised by Aboriginal and Torres Strait Islander people between June 2010 and May 2011.
44 PBS data, provided by the Department of Health and Ageing.45 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
52KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1,289 1,004 883 851
172 344 715
1,341
0
500
1,000
1,500
2,000
2,500
August 2010 November 2010 February 2011 May 2011
Scrip
ts
S100 scripts CtG scripts
Figure 6: Supply/dispensing of smoking cessation medicines - allocation across CtG and S100 RAAHS initiatives.46 The increase in CtG scripts for smoking cessation over 2010-11 does not necessarily represent the increase in scripts dispensed over this period. Some Aboriginal and Torres Strait Islander community members using CtG scripts might otherwise have used the full co-payment PBS scripts to access smoking cessation medicines, i.e., the CtG scripts measure has replaced access to PBS medicines at full price. Further, some Aboriginal and Torres Strait Islander community members living in remote locations (where S100 RAAHS is in place) may have used CtG scripts instead of accessing medicines through S100 RAAHS, i.e., the CtG scripts measure has replaced (some) access to S100 RAAHS. Other Aboriginal and Torres Strait Islander people who smoke might have increas7ed their over-the-counter NRT use.In summary, there is an observable increase in the use of smoking medicines available from the two schemes CtG scripts and the S100 RAAHS. Whether this represents the increase in the smoking cessation medicines used by Aboriginal and Torres Strait Islander people requires further exploration.
A benchmark for rates of uptake of smoking cessation medicines
It is important to put the above analysis in context by considering data for full co-payment PBS scripts. Table 11 below provides a comparison between the smoking cessation scripts dispensed through CtG scripts and S100 RAAHS, and those dispensed under
46 Section 100 data supplied by the Department of Health and Ageing.53
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
the full co-payment PBS to the broader population of all smokers for the three months to 31 May 2011. It also provides: a ratio of the smoking cessation CtG scripts and S100 RAAHS scripts
dispensed to the Aboriginal and Torres Strait Islander smoking population; and
a ratio of smoking cessation full co-payment PBS scripts dispensed to the broader smoking population.47
Table 11: Comparison of dispensing of CtG, S100 RAAHS smoking cessation prescriptions in three months to May 2011 by scheme for Aboriginal and Torres Strait Islander smokers.48
Scheme Number of smoking cessation scripts
Aboriginal and Torres Strait Islander smokers (2008 NATSISS)
Ratio
CtG Scripts 1,341 153,000 0.9S100 RAAHS scripts
1,092 153,000 0.7
CtG Scripts and S100 RAAHS Scripts
2,433 153,000 1.6
Table 12: Number of full co-payment smoking cessation prescriptions in three months to May 2011.49
Scheme Number of smoking cessation scripts (PBS Online)
Number of smokers (2008 NHS) Ratio
PBS Scripts 221,360 3,332,700 6.6
As Table 11 and Table 12: Number of full co-payment smoking cessation prescriptions in three months to May 2011. show, there were fewer smoking cessation CtG and S100 RAAHS scripts dispensed per Aboriginal and Torres Strait Islander smoker (1.6 per 100 smokers), than there were smoking cessation scripts dispensed per smoker in the broader population (6.6 per 100
47 Population statistics based on the most up to date, available population statistics at the time of drafting.48 PBS data provided by the Department of Health and Ageing and accessed online; Australian Bureau of Statistics 2008, National Aboriginal and Torres Strait Islander Social Survey data and Australian Bureau of Statistics 2008, National Health Survey data.49 PBS data provided by the Department of Health and Ageing and accessed online; Australian Bureau of Statistics 2008, National Aboriginal and Torres Strait Islander Social Survey data and Australian Bureau of Statistics 2008, National Health Survey data.
54KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
smokers) in these three months. This result suggests that the rate of uptake of smoking cessation medicines, and pharmacotherapy, is lower amongst the Aboriginal and Torres Strait Islander population generally, as demonstrated in literature and research studies.50 There are two factors that may have contributed to the observed difference of 1.6 to 6.6 scripts per 100 smokers: not all smoking cessation medicines used by Aboriginal and Torres Strait
Islander people are identified using data on CtG scripts and S100 RAAHS this is discussed on the following page; and
Aboriginal and Torres Strait Islander smokers have a lower rate of uptake, as evidenced above.
If the first explanation were true, full co-payment PBS scripts would represent up to 75 per cent of all the smoking cessation medicines dispensed to Aboriginal and Torres Strait Islander people and S100 RAAHS and CtG scripts would represent the remaining 25 per cent.
Limitations
The data presented above identifies the number of prescriptions known to be dispensed to Aboriginal and Torres Strait Islander people for smoking cessation under the two schemes, CtG scripts and the S100 RAAHS. However, as noted previously, this data does not provide a full picture of the use of smoking cessation medicines amongst Aboriginal and Torres Strait Islander people. In particular: this data does not show all smoking cessation scripts dispensed to
Aboriginal and Torres Strait Islander people in 2010-11, because it is likely some smoking cessation medicine scripts were dispensed outside of these two schemes (i.e., full co-payment PBS scripts); and
purchased over-the-counter smoking cessation medicines, which are likely to present a proportion of smoking cessation medicines accessed by Aboriginal and Torres Strait Islander people, cannot be tracked through any secondary data sources.
The data on these two subsidy schemes therefore cannot be interpreted as an overall increase in access to smoking cessation medicines. What this data does show is that the CtG scripts measure was being increasingly utilised over time during 2010-11.
50 Hayman N 2011, ‘Improving Aboriginal and Torres Strait Islander people’s access to the Pharmaceutical Benefits Scheme’, Australian Prescriber, 34(2) pp. 38-40; Australian Institute of Health and Welfare 2008, Expenditures on health for Aboriginal and Torres Strait Islander peoples 2004-05, Health and welfare expenditure series no. 33. Cat. No. HWE 40, Australian Institute of Health and Welfare, Canberra.
55KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Consistent with this, the community focus groups conducted in 2010-11 showed that there was strong awareness of the availability of subsidised smoking cessation medicines through CtG scripts. Participants in half of all community focus groups explicitly stated they were aware that they could access subsidised smoking cessation medicines, including for some participants, the pharmaceutical Varenicline Tartrate. Similarly, the Sentinel Sites Project found “widespread use and awareness of NRT” amongst Aboriginal and Torres Strait Islander people consulted for this project.51 Some of this awareness may have been reflective of existing awareness of the Smokecheck program. However, participants’ knowledge of Varenicline Tartrate (unique to ICDP) and the fact that participants in all community focus groups were aware they could access subsidised medications generally through CtG scripts, suggested that the ICDP had contributed (at least to some extent) to an increased understanding of smoking cessation pharmaceuticals in 2010-11.
Impact of PBS smoking cessation medicine availability
Another factor influencing the use of smoking cessation medicines is the availability of new and additional smoking cessation medicines over time. The uptake of smoking cessation medicines through the PBS does not generally fit a simple trend over time, partly as a consequence of the changes in the number and types of smoking cessation medicines listed on the PBS over the last five years. For example, in early 2008, Varenicline Tartrate (Champix) was listed for the first time. In late 2008, an additional type of nicotine replacement patch was listed. In early 2011, two further types of nicotine replacement patches were listed. The figure below presents a comparison of the growth in smoking cessation PBS scripts (both CtG and full co-payment) and S100 RAAHS scripts dispensed between September 2009 and May 201152.
51 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.52 Note – this period was chosen as the CtG script data is supplied quarterly, i.e., May 2011 data consists of scripts for May, April and March 2011.
56KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
02004006008001,0001,2001,4001,600
0
50,000
100,000
150,000
200,000
250,000M
ay-07
Aug-0
7No
v-07
Feb-0
8M
ay-08
Aug-0
8No
v-08
Feb-0
9M
ay-09
Aug-0
9No
v-09
Feb-1
0M
ay-10
Aug-1
0No
v-10
Feb-1
1M
ay-11
CtG and S100 ScriptsPBS S
cript
s
PBS Scripts CtG scripts S100 scripts
Champix
Figure 7: Smoking cessation prescriptions for May 2007 quarter to May 2011 quarter for PBS, CtG and S100 RAAHS.This figure shows that there was growth in both CtG and full co-payment PBS smoking cessation scripts between June 2010 and May 2011. For PBS smoking cessation scripts, there was a substantial increase in the first half of 2011 – coinciding with the introduction of two additional nicotine patches to the PBS. This is one example of how changes in the uptake of smoking cessation medicines are influenced by factors outside of community demand for these medicines. The increase in PBS smoking cessation scripts was greater than the growth in CtG scripts over 2010-11. However, the potential substitution of PBS scripts for CtG scripts cannot be determined from the available data; hence, it is again not possible to identify whether the increase in CtG scripts represents an increased uptake of smoking cessation medicine by Aboriginal and Torres Strait Islander people.
Role of RTSHLTs
Another, final influencing factor on the uptake of smoking cessation medicine is likely to be the work of the RTSHLTs in recommending and referring people to these medicines. Using the data presented above, it is not possible to specifically identify the role of RTSHLTs in this increased uptake of smoking cessation medicines via CtG scripts. However, of the three RTSHLTs engaged through the site visits,
57KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
two had promoted or talked to community members about smoking cessation medicines through their activities, and one of these RTSHLTs reported referring community members to GPs to access smoking cessation medicines. This suggests that RTSHLTs may have had a role in building community awareness regarding the availability of smoking cessation medicines in 2010-11, and that the RTSHLT measures are complementary to the CtG scripts measure in terms of access to smoking cessation medicine. Data providing details on the utilisation of Quitline by Aboriginal and Torres Strait Islander people was not available for 2010-11.Reduced smoking and increased healthy lifestyle choices
In 2010-11, the evaluation found some emerging evidence of attitudes and behaviours which may lead to reduced smoking and increased healthy lifestyle choices, amongst Aboriginal and Torres Strait Islander community members consulted.This finding has been informed by focus groups conducted during 2010-11 community site visits. There was no data available on reductions in smoking or increases in healthy lifestyle choices amongst Aboriginal and Torres Strait Islander people for 2010-11 which could be analysed to assess the contribution of the ICDP. Nor could the outcomes reported during community focus groups around understanding and assistance seeking be linked to the work of RTSHLTs, given that participants at only one community focus group knew about a RTSHLT in their region. The community focus groups indicated that many community members wanted to quit smoking, with participants at over half of all focus groups saying that many people in the community wanted to quit. Further, a small number of participants engaged in focus groups had quit, or provided examples of people they knew who have quit smoking. The focus groups also suggest that some community members were making healthier lifestyle choices; one-quarter of all focus groups provided examples of community members making changes to their exercise or eating habits. In addition, two of the three RTSHLTs engaged during the site visits indicated staff in their organisation either wanted to or had quit smoking. Smoke-free workplaces
The evaluation found that the 2010-11 departmental smoke-free workplaces policy53 has promoted discussion and organisational change around smoke-free workplaces, even in locations where no RTSHLT was in place.
53 Email to KPMG from the Department of Health and Ageing 2011.58
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
This finding has been informed by community, departmental and national stakeholder consultations and Regional Forums. In 2010-11, all IHSs received notification that organisations receiving funds through the National Action to Reduce Indigenous Smoking Rates (A1) measure must become smoke-free workplaces by 30 June 2011, and that all other IHSs must be smoke-free by 30 June 2012 as a condition of Department of Health and Ageing future funding.54 Anecdotal examples were provided in Regional Forums of the importance of IHSs (including the leadership group) embracing this policy. Participants commented that this was important to support health workers to give up smoking, and it was difficult for the RTSHLT workers to promote quit smoking messages in the community if IHS staff (and particularly CEOs and Board members) were smokers. All of the IHSs engaged through community site visits were aware of this new policy, and many provided examples of changes that had been made within their organisation to implement smoke-free workplace policies and associated changes. For example, staff in one IHS were asked to cover their uniforms if they went beyond the IHS precinct to smoke and the CEO had committed to give up smoking. In other organisations, one RTSHLT had been working towards enforcing their organisation’s existing smoke-free workplace policy, and another had been working with staff to support them to quit smoking through brief intervention sessions. Together, these examples suggest this policy is leading to some change within organisations. A small number of other stakeholders engaged through the site visits noted that there were challenges for their organisation in being ‘smoke-free’. For example, at one organisation, a doctor reported that there had always been reluctance by the Board to ban smoking because of a perception that it would be unacceptable to ‘tell elders what they can and can’t do’. In this organisation, the TAW had to work very hard to achieve Board support to implement the changes required by the policy.Consultations undertaken with IHSs during the 2010-11 community site visits suggest that many IHSs have been implementing strategies to support workers to quit smoking for many years. For example, two of the four IHSs consulted during the community site visits reported that they had existing smoke-free workplace policies in place prior to the commencement of the departmental policy. In addition, research acknowledges that Aboriginal and Torres Strait Islander organisations and communities have been working to promote smoke-free places for some time (albeit with variable success).55
54 Email to KPMG from the Department of Health and Ageing 2011.55 Centre for Excellence in Indigenous Tobacco Control 2012, Fact Sheet: What do we know about the success of smoke-free workplaces, homes and cars?, Department of Health and
59KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Therefore, the National Action to Reduce Indigenous Smoking Rates (A1) measure may, in some places, act to strengthen existing initiatives, rather than facilitate new initiatives.1.12 National level support for tobacco reduction (A1)Quitline enhancements
Quitline is a free and confidential telephone-based service that offers assessment and information to assist callers to quit smoking. Through the National Action to Reduce Indigenous Smoking Rates (A1) measure, the department is funding Quitline to enhance its capacity to be more culturally sensitive and to provide accessible and appropriate services for Aboriginal and Torres Strait Islander people. These enhancements include (but are not limited to) cultural awareness training for Quitline staff, and employment of Aboriginal or Torres Strait Islander people. In 2010-11, six organisations were provided funding ranging from $94,000 to $254,000 to undertake these enhancements to their Quitline service. In 2010-11, Quitline organisations employed six Aboriginal or Torres Strait Islander staff through the enhancement project.56 This was the only information available on Quitline enhancements undertaken through 2010-11. As noted previously, no data on utilisation of Quitline by Aboriginal and Torres Strait Islander people was available to the evaluation.Brief intervention training
Tobacco brief intervention applies motivational interviewing techniques in opportunistic settings to assist recipients to reduce or eliminate their tobacco use. Health workers trained in this smoking cessation technique are expected to deliver tobacco brief interventions to patients/clients as opportunities arise in the course of service delivery. As part of the RTSHLT measures, the department identified a 2010-11 target to provide brief intervention training in tobacco to 200 health workers, drug and alcohol treatment staff and community youth educators. This target was met through training workshops delivered by Quit Victoria, across Victoria and the Northern Territory. In the Northern Territory, in partnership with the Northern Territory government, training was delivered in three locations in the Northern Territory: Darwin; Katherine; and Alice Springs. In Victoria, in partnership with the Victorian Community Controlled Health Organisation, training was delivered in five locations: Bairnsdale, Morwell, Bendigo, Mildura and Carlton. The workshops averaged 15-20 participants.57
Ageing. 56 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [A1/A2 response].
60KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The department will also fund refresher sessions to ensure that training recipients retain capacity and confidence to deliver brief interventions. The evaluation found evidence that workers within some ICDP funded organisations had participated in brief interventions training during 2010-11, but that this was not necessarily the training funded under the ICDP. Two of the three RTSHLTs engaged through the community site visits reported that at least one of their workers has participated in brief interventions training. In the sites without RTSHLTs, only one other stakeholder reported that workers (in this case midwives) at their organisation had undertaken the training and were using the technique in their interactions withclients. These sites were in jurisdictions outside of Victoria and the Northern Territory (i.e., where the ICDP funded training was delivered). Further, during one Regional Forum (Brisbane), other ICDP workers discussed training of a similar nature which was being undertaken by workers in their organisations. These reports suggest that at least some of the brief intervention training accessed is not ICDP specific, and it is thus likely that the ICDP is complementing existing activity in this area.Data is not currently being collected on the delivery of brief interventions to patients due to the opportunistic nature of the service. ‘Break the Chain’
Break the Chain is the first national anti-smoking campaign targeted to Aboriginal and Torres Strait Islander people, and is part of the National Tobacco Campaign. Break the Chain provides an anti-smoking message that is expected to supplement the work of the RTSHLTs. Break the Chain was launched in March 2011 with a budget of $5.1 million. As announced by the Ministers on 31 May 2011, the Break the Chain campaign included a partnership with Aboriginal Hostels Limited, which is a Commonwealth organisation that provides temporary accommodation for Aboriginal and Torres Strait Islander people. The campaign provided funding to ensure that smoking at hostels is restricted to designated smoking areas, and to ensure that staff provide health education and promotion activities and messages to clients.58 Due to this campaign being released in late 2010-11, it is not plausible to consider the impacts of this campaign on smoking attitudes and behaviours amongst Aboriginal and Torres Strait Islander community members in this report.
57 ibid. 58 70 accommodation facilities sign on to stamp out smoking (31 May 2011), The Hon Warren Snowden MP, Minister for Indigenous Health; The Hon Nicola Roxon MP, Minister for Health and Ageing; The Hon Jenny Macklin MP, Minister for Indigenous Affairs.
61KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Related to Break the Chain, and also during 2010-11, an evaluation of the National Partnership Agreement on Preventative Health Tobacco Social Marketing Campaign was completed, with the release of an Evaluation Report developed by the Social Research Centre. 59 This evaluation considered, in relation to Break the Chain specifically: campaign awareness, message communication and impact on the attitudes, awareness, intentions and behaviour of the target audiences; namely, smokers aged 18 to 40; and recent quitters aged 18 to 40. The evaluation found a higher recognition of the Break the Chain campaign amongst Aboriginal and Torres Strait Islander people than other people (69 per cent versus 55 per cent overall) suggesting the campaign may be effectively targeting its intended audience. It also found an increased proportion of Aboriginal and Torres Strait Islander people intending to quit in the month following the airing of this campaign (35 per cent compared with 19 per cent previously). This suggests that this campaign has potential to impact on smoking rates amongst the Aboriginal and Torres Strait Islander population. 1.13 Facilitators and barriersThe following factors have supported implementation of the measures in 2010-11: Existing supports: placement of new RTSHLTs workers into organisations
which were already running some health promotion based activity, and linking the RTSHLTs to those existing teams was identified as a facilitator by stakeholders. Input from Regional Forums suggests that RTSHLTs achieved gains more quickly in organisations where staff were incorporated into, or had an opportunity to work with, established health promotion or drug and alcohol workers. Some fund holders had not previously provided health promotion services and, in such cases, it is likely that additional time and energy would be required to achieve integration within their organisation.
Organisational support: Regional Forum participants and health workers consulted indicated that the commitment to smoking cessation from organisational CEOs and Board members was important to the credibility of TAWs (and RTCs) in the eyes of the community and to the level of support provided to the TAW in the organisation. Where this support was lacking or was perceived by the community as not existing, the TAWs were more likely to encounter resistance from within the community to engage in smoking cessation activities.
59 Social Research Centre 2011, National Partnership Agreement on Preventative Health Tobacco Social Marketing Campaign Evaluation Report, Department of Health and Ageing, Canberra.
62KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Networking: networking across fund holders and between individual workers was identified as a key facilitator by all RTSHLT workers consulted. This is likely to be particularly true for workers who are operating alone or in small teams at the moment (until others are recruited). Workers reported that meeting others at training had allowed them to initiate ad hoc contact to exchange ideas and mutual support with colleagues around the country.
Complementary activity: both the New South Wales and Queensland governments are providing substantial funding for brief intervention training during 2010-11. Training was also provided for brief intervention through some of the Indigenous Tobacco Control Initiative projects during this period. This complimentary activity to the ICDP can be expected to support the desired outcomes of the National Action to Reduce Indigenous Smoking Rates (A1) and Helping Indigenous Australians Reduce Their Risk of Chronic Disease (A2) measures.
A number of barriers were also identified: Confusion about the roles: a number of stakeholders interviewed
indicated that the confusion regarding the role of TAWs and RTSHLTs made for a “slower start” to this initiative. In some cases, where there were existing similar local initiatives (funded by other programs), the confusion of the role was exacerbated.60 There was a perception that insufficient information was available during the implementation period regarding the roles of ICDP workers including RTSHLTs, which may have resulted in this confusion.
Organisational leadership: Regional Forum participants indicated that where organisational leaders (CEOs, Board members and key workers) were reluctant to personally commit to quit smoking, it affected the credibility of messages that TAWs were delivering to the community. Some IHSs reported that certain members of the community were resistant to changes associated with the move to a smoke-free environment and the more insistent messages promoting lifestyle changes.
Community pressure: some workers reported that there was a level of community and cultural pressure placed on Aboriginal and Torres Strait Islander workers (who are also community members) in the RTSHLT roles due to workers having to deliver messages opposing widespread attitudes and behaviours. This may have had a negative impact on recruitment and retention of RTSHLTs.
Perceived sustainability: uncertainty regarding long-term funding for the ICDP measures and the workforce were identified as barriers for both
60 This issue was raised at Regional Forums and interviews with peak body organisations such as SBOs and NACCHO affiliates.
63KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
these measures specifically and for the ICDP as a whole (see chapter for further discussion). Stakeholders reported that this had a negative impact both on recruitment of workers and community member willingness to engage with new activities and services.
1.14 OpportunitiesThe early stages of implementation have identified several areas that the department may consider in order to improve the implementation and impact of the measures, as outlined below: Support for Aboriginal and Torres Strait Islander workers:
mentoring and support for Aboriginal and Torres Strait Islander workers to manage community based pressures associated with their roles. Consultation findings to date indicate that these community based pressures could have a negative impact on the retention of the workforce over time.
Enhance training: continue to seek opportunities to improve the training available for staff through ICDP by improving coordination, consistency and targeting future training content to actual needs as identified by the sector.
Organisational leadership: consider ways to promote and enhance organisational leadership to support the RTSHLTs. This may be done by sharing examples of good leadership across the sector, or providing communications to CEOs and boards outlining the importance of support and providing examples of ways to support these measures.
Networking: future training and professional development planning for the workforce should emphasise the value of networking, and support national and jurisdictional collaboration both during and beyond formal training opportunities.
Placement of RTSHLTs: when identifying the location of additional workers and resources under the RTSHLT measures, placement of RTSHLTs within organisations with existing health promotion capacity should be considered as a criterion.
Sustainability: commence early work to consider and plan for the sustainability of the measures and the RTSHLTs. Communicate with the sector about the progress of this work on a regular basis.
64KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Local Indigenous Community Campaigns to Promote Better Health (A3)This chapter provides an overview of the Local Indigenous Community Campaigns to Promote Better Health measure (hereafter referred to as the LCC measure). In this chapter, we discuss findings against activities, outputs and expected results as described in the Evaluation Framework, and barriers, facilitators and opportunities identified to date. The measure is the subject of a concurrent evaluation by the evaluation consortium and consequently has a different schedule of deliverables and timeframes to the rest of the evaluation. An Interim Evaluation report is being developed separately. This report covers progress of the LCC measure for much of the 2010-11 financial year. The key findings presented below are a summary of the findings reported in these two deliverables. Local Indigenous Community Campaigns to Promote Better Health at
a glance The LCC measure was in the early stages of implementation in 2010-11, during which time the department completed the planned developmental activities including the production of various resources to support local campaigns, and the first round of targeted funding of local community campaigns.The first round of LCC funding (the ‘targeted’ round) was targeted to organisations with demonstrated capacity and capability to carry out a LCC. The department’s targeted round of funding process was structured and extensive in terms of the criteria applied to select LCCs, ensuring rigorous assessment of grant applications and clarity of process. As a result, a diverse range of campaigns were funded in 2010-11. Funding was predominantly distributed to community-based organisations with governance structures linked to the community and therefore an assumed understanding of community needs.The funding agreements between the department and LCC grant recipients were established in June 2011, towards the end of the 2010-11 reporting period. As such, the evaluation cannot comment on the progress or efficacy of targeted round LCCs as part of 2010-11 reporting.During 2010-11, the LCC measure website went live and Community Health Action Pack (CHAP), a resource for LCC grant recipients, was developed and ready for distribution. The evidence collated for the evaluation during 2010-11 clearly demonstrates that the developmental research conducted in 2009-10 had a significant influence on the design of the measure. Namely, the move to a more local
65KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
campaign strategy rather than a national campaign approach, a more significant focus on young people, and a focus on group activities aligned to positive health behaviours.
66KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Potential effects based on implementation findingsFigure 8 below is the causal pathway for the LCC measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
Local Indigenous Community
Campaigns to Promote Better
Health
Increase in knowledge and
understanding of lifestyle related
chronic disease risk factors
Improved uptake of healthy lifestyle
choices
Change in attitudes towards making healthy lifestyle
choices
Reduced chronic disease risk factors
Increase in community mobilisation
Projects are effectively
implemented and evidence
based
Individuals and communities engage with
and participate in LCCs
Figure 8: Local Indigenous Community Campaigns to Promote Better Health causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect61 and the observed impacts.62 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below.Table 13 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). The measure was modified from the original design, to provide a local grass roots rather than a national campaign model. This is likely to have enhanced the plausibility of effect in 2010-11. As the funding agreements were only executed with LCC grant recipients at the end of the
61 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.62 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
67KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
2010-11 financial year, there is limited evidence in respect of the majority of the key dependencies/assumptions and expected impacts for this measure. Table 13: Assessment of key depedencies of the A3 measure.
Key dependencies
Finding Evidence
Increase in community mobilisation
Data is not available for the First Monitoring Report.
Not applicable
Projects are effectively implemented and evidence based
Data is not available for the First Monitoring Report.
Not applicable
Individuals and communities engage with and participate in LCCs
Data is not available for the First Monitoring Report.
Not applicable
Contextual considerations
Variation amongst individuals and communities is likely to impact on existing behaviour and receptiveness to change, as noted previously in relation to the RTSHLT measures.63 The availability of supports for healthier lifestyles and smoking, which LCCs can link with, also varies across jurisdictions and remoteness areas.64
Analysis of measure documentation and literature review
below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). Data is not available on any of the expected impacts for 2010-11. Two key contextual factors were evident: increased awareness of chronic disease risk factors and variable willingness to change behaviour; and awareness and availability of services to assist in behaviour change.
63 Bond C, Brough M, Spurling G & Hayman N 2012, ‘It had to be my choice’ Indigenous smoking cessation and negotiations of risk, resistance and resilience’, Health, Risk & Society, vol 14, no 6, pp 565-581.64 As demonstrated in the ‘Policy Map’ within the KPMG Baseline Report: KPMG 2013, Indigenous Chronic Disease Package National Monitoring and Evaluation Project: Baseline Report, Australian Government Department of Health and Ageing, Canberra.
68KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 14: Assessment of expected impacts of the A3 measure based on implementation progress.
Expected impacts
Observed impacts Evidence
Increase in knowledge and understanding of lifestyle related chronic disease risk factors
Data is not available for the First Monitoring Report.
Not applicable
Change in attitudes towards making healthy lifestyle choices
Data is not available for the First Monitoring Report.
Not applicable
Improved uptake of healthy lifestyle choices
Data is not available for the First Monitoring Report.
Not applicable
Reduces chronic disease risk factors
Data is not available for the First Monitoring Report.
Not applicable
Contextual considerations
As noted in chapter 4 in relation to the RTSHLT measures, the evaluation found good awareness of the health risks and benefits associated with chronic disease amongst Aboriginal and Torres Strait Islander community members; and amongst some people, willingness to change their lifestyle behaviours. In all focus groups, community members were able to provide examples of local services to support behaviour change (i.e., that LCCs can refer to) although the number of and choice in services varied; with fewer in remote areas than in urban.
Qualitative information gathered from a small group of relevant stakeholders
1.15 Measure overviewThe Local Indigenous Community Campaigns to Promote Better Health (A3) measure represents a series of locally generated and delivered health promotion initiatives that target Aboriginal and Torres Strait Islander people at
69KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
risk of chronic disease, including those who have low engagement with health services. The objective of the LCC measure is to encourage Aboriginal and Torres Strait Islander communities to adopt sustainable healthy lifestyle choices including increased engagement with primary health care services. Delivery of the measure is broadly divided into two components: LCC grant projects to be delivered by local community organisations with
the objective of promoting sustainable behavioural change around chronic disease prevention and management, healthy lifestyle choices and the benefits of accessing primary healthcare; and
a coordinated national communications and program support strategy branded ‘Live Longer!’ and comprised of:- a website (www.livelonger.health.gov.au)65 that is designed to share
information and stories about Aboriginal and Torres Strait Islander chronic disease health promotion activities and events;
- Healthy Community Day events, to raise the awareness of chronic disease, healthy lifestyle choices and local primary healthcare services; and
- a CHAP to support Aboriginal and Torres Strait Islander communities design and deliver health promotion activities including, but not restricted to, those taking part in LCCs.
The Australian Government has allocated approximately $21.3 million (excluding GST) to the LCC measure between 2009-10 and 2012-13.1.16 ResearchThe research activities for the LCC measure were completed in 2009-10. In 2009, the department commissioned Ipsos-Eureka (now Ipsos Social Research Institute) and Winangali Pty Ltd to conduct research in order to inform the department of the best approach to delivering the LCC measure. The research was based on a literature review and consultations with Aboriginal and Torres Strait Islander community members and health care professionals. Specifically, focus group consultations were held with more than 220 community members, and 30 in-depth interviews were conducted with health professionals in 22 locations across all jurisdictions in Australia except the ACT. The consultations with Aboriginal and Torres Strait Islander community members focused on assessing current levels of awareness of chronic disease risk factors, barriers to modifying these risk factors, issues related to accessing health services, and communication preferences. These consultations strongly informed the findings of the research report developed
65 Department of Health and Ageing, Canberra. Live Longer (website), viewed April 2012.70
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
by Ipsos-Eureka and Winangali Pty Ltd in 2010.66 This research report provides a summary of recommendations for effective social marketing campaigns for Aboriginal and Torres Strait Islander communities. The research emphasises that campaigns are most likely to be effective when they: are locally relevant (such as those that include promotion of local health
services, address local health service access issues, and promote preventative approaches to chronic disease among local primary health care providers);
focus on young people; promote group participation; and draw on the link between culture and family. As a result of this research, the department designed a grass roots, rather than national, campaign model for this measure. 1.17 Targeted round LCCs The evaluation has found that in 2010-11, the department ran a successful targeted grant application process to identify and fund appropriate organisations to implement the first round of LCCs. This finding has been informed by consultation with the department, and analysis of documentation provided by the department. The first round of funding was targeted to specific organisations. Specialist Aboriginal and Torres Strait Islander communications consultancy Cox Inall Ridgeway was engaged to assist with the identification of organisations that were likely to have the capacity and capability to implement funded projects, based on the following criteria: established organisations that would benefit from additional funds to
increase their scale, reach and effectiveness; organisations that had delivered a proven program or health promotion
methodology to a community that had not been able to access these type of services in the past;
organisations that had a proven track record in delivering innovative preventative health campaigns;
organisations that had the ability to meet program timeframes; and organisations that had the potential to become model projects to
encourage other communities to bring forward projects in subsequent funding rounds.
66 Ipsos-Eureka Social Research Institute and Winangali Pty 2010, Developmental Research to inform the Local Aboriginal and Torres Strait Islander Community Campaigns to Promote Better Health, Department of Health and Ageing, Canberra.
71KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Cox Inall Ridgeway conducted community consultations across Australia to canvass expressions of interest from potential grant recipient organisations. Over one hundred (105) organisations were invited to apply for grant funding in the targeted round in March - April 2011, including organisations in every state and territory. As a result of the call for applications, the department received 75 applications from 68 organisations. Assessment of applications was conducted by a Central Assessment Committee, with advice from OATSIH state and territory offices. The selection criteria were67: Appropriateness: the project objectives and target group align with the
objectives of the program, including linking to healthcare services as appropriate, demonstrating how to reduce risk factors for chronic disease, promoting healthy living, and building community and/or cultural identity.
Effectiveness: demonstrates appropriate application of resources and method of delivery.
Capacity: demonstrates ability to plan and apply resources to deliver the proposed project.
Community need and readiness: demonstrates need and willingness by the community to engage.
Value for money: demonstrates efficient use of funds and benefits proportional to the size of the grant.
The selection criteria for the LCC measure broadly aligned with the principles within the National Indigenous Reform Agreement (NIRA)68, as the Draft Interim Progress Report describes. The exception is the lack of obvious adherence to the ‘Integration’ principle as written in the NIRA, as there is no explicit collaboration between the department and state/territory governments on the ICDP, including the LCC measure.Thirty-eight campaigns were selected for delivery by 35 organisations across Australia. Funding agreements were signed in June 2011 to a total value of $10 million (GST inclusive). Grants were awarded to deliver campaigns in all states and territories excluding Tasmania and the Australian Capital Territory, with the greatest share of grant funding awarded to the Northern Territory (35
67 Department of Health and Ageing 2011, Local Community Campaigns to promote better Aboriginal and Torres Strait Islander health program: Grant guidelines, Department of Health and Ageing, Canberra.68 Council of Australian Government 2009, National Indigenous Reform Agreement (Closing the Gap), COAG, Canberra
72KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
per cent). Eighty per cent of grant funding was awarded to states and territories with the highest Aboriginal and Torres Strait Islander populations.69
The LCCs funded in the targeted round involved activities falling within five broad ‘categories’. These categories included: healthy lifestyle or wellbeing programs that target at risk individuals; awareness raising communication strategies that target the broader
community; community program style campaigns where a regular schedule of events
are available to all of the target audience; community and school event-driven projects; and strategies that use culture to deliver healthy lifestyle messages.The funded LCCs largely included activities aligning with two or more of these ‘categories’, although in 34 of the targeted round LCCs, there is a predominant alignment with a single campaign style.Five of the 35 grant recipients in the targeted round were media organisations, and the remaining organisations were community organisations which were largely health or community development focused. The organisations and LCCs funded have widespread coverage across Australia. Thirty-four of the 38 funded LCCs are region-specific, and the remaining four are ‘cross-border’ projects covering numerous localities and communities. 1.18 Community involvement and engagement with LCCsThe evaluation has found that, at the end of 2010-11, there was emerging evidence that LCCs were designed to meet local community needs. This finding has been informed by consultation with the department and analysis of documentation provided by the department. As indicated above, the criteria against which targeted round LCC grant applications were assessed required applicants to demonstrate how their proposed LCC met community needs and readiness. Information provided by the department suggests that all of the funded LCCs were assessed as having adequately met this criterion. Further, the selection of targeted round grant recipients appears to have reflected an emphasis on locally designed and delivered campaigns, rather than more widely provided media campaigns.At the time of writing this report, the extent to which funded organisations had consulted with community members prior to submitting their funding applications was not clear. However, the majority of targeted round grant recipients are community-based organisations, many of which are assumed to
69 NSW, QLD, WA and NT.73
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
have existing relationships with communities and governance structures directly linked to the community. These features are potential facilitators to community consultation. Additionally, many of these organisations are staffed by local community members, suggesting that LCC design was informed by first-hand knowledge and experience. Planned consultations post the 2010-11 reporting period and assessment of grant recipients’ progress reports will further inform on the involvement of communities in the LCC design and grant application process. 1.19 Program supports for the LCC measureThe evaluation has found that in 2010-11 two key program supports were implemented for the LCC measure, with implementation largely occurring as planned. This finding has been informed by consultation with the department and analysis of documentation provided by the department. The ‘Get Active, Eat Good Tucker, Live Longer!’ website was developed by Cox Inall Ridgeway in 2010-11, and went live ahead of the call for targeted round grant applications. The website includes resources such as the CHAP, and other information relevant to LCCs such as dates for community events and media releases. The CHAP was also developed in 2010-11. Cox Inall Ridgeway was contracted to lead the development of the CHAP, with input from both Aboriginal and Torres Strait Islander communications and health promotion experts and the department. The CHAP is an instructional resource which contains four parts: ‘Ten steps to planning a health promotion project’, ‘Project planning templates’, ‘Running your project’ and ‘Health promotion resources.’ In May 2011, the department ran a workshop in Adelaide to introduce the CHAP to workers within IHSs, many of whom were engaged in the RTSHLTs (A1 and A2) measures. The department plans to refine the CHAP based on feedback from this workshop. As this workshop occurred prior to the finalisation of the targeted round grant application process, no LCC representatives were in attendance. The CHAP was also made available on the ‘Live Longer’ website in July 201170 but was unavailable to assist LCC organisations with their grant applications. 1.20 Facilitators and barriersThe following factors have supported implementation of the LCC measure in 2010-11:
70 Department of Health and Ageing, Community Health Action Pack workshop, 10 May 2011, viewed 10 May 2012.
74KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Influential research. The developmental research conducted by Ipsos-Eureka and Winangali Pty Ltd influenced the department’s choice to base the measure on local community campaigns.
Targeted invitations. In order to fund organisations likely to achieve and model success, the department chose to invite organisations to apply for the targeted round funding. The selection process was based on community consultations and a subsequent assessment process to identify the strongest applications. This targeted approach appears appropriate to optimise the desired outcomes from the first round of LCCs.
Provision of support to organisations. The department engaged Cox Inall Ridgeway to provide support to the organisations invited to submit an application to receive funding under this measure. While information on the extent to which this support was used by individual organisations was not available for 2010-11, interviews with departmental stakeholders suggest that it was widely used by a number of organisations.
The LCC measure had not faced significant barriers within the 2010-11 timeframe, although at the time of preparing this report, the evaluators were aware of a number of challenges that LCC organisations had faced with the implementation of their local campaigns during 2011-12, which will be the focus of the next Monitoring Report.1.21 OpportunitiesThe early stages of implementation have identified several areas that the department may consider in order to improve the implementation and impact of the LCC measure, as outlined below: Networking. The department may consider providing an effective
networking mechanism to ensure that funded organisations have the opportunity to share implementation experiences. This may enhance use of best practices and support successful outcomes.
Coverage. While targeted round funding reflected the strongest applications, it will be important for the second round of LCC funding to include additional areas that have high numbers and/or concentrations of Aboriginal and Torres Strait Islander people.
75KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Subsidising PBS Medicine Co-payments (B1)This chapter describes the progress of Subsidising PBS Medicine Co-payments measure (hereafter referred to as the PBS Co-payment measure or CtG scripts). In this chapter we discuss findings against activities, outputs and expected results identified within the Evaluation Framework, and barriers, facilitators and opportunities identified to date. PBS Co-payment measure at a glanceThe evaluation found that in 2010-11 the PBS Co-payment measure had significant success in terms of primary health care provider involvement in the measure, and utilisation of CtG scripts. Despite some initial implementation issues, the measure was ‘on track’ to achieving its identified outputs.The PBS Co-payment measure commenced 1 July 2010. In the period to 31 May 2011 (11 months), 79,076 Aboriginal and Torres Strait Islander people were dispensed 859,370 CtG scripts (10.9 per person) through the PBS Co-payment measure; exceeding the department’s documented expectations. 3,278 community pharmacies dispensed at least one CtG script over the three months to 31 May 2011, representing around 65 per cent of all community pharmacies in Australia. During 2010-11, 46 per cent of CtG scripts dispensed were in the Anatomical Therapeutic Chemical (ATC) Classification System categories broadly corresponding to the three key chronic diseases (cardio-vascular, respiratory and diabetes71). The most common ATC outside this group was medicines for the nervous system which represented 22 per cent of total CtG scripts. The range of dispensed medicines reflects the broad range of medicines used by people with or at risk of chronic disease. At this stage the extent to which the successful uptake of this measure has translated to improvements in access to PBS medications has not been assessed. An unknown share of CtG scripts represents direct substitution of PBS scripts that would otherwise have been dispensed under current PBS co-payment arrangements. This will be explored in future evaluation reporting. Implementation of the PBS Co-payment measure throughout 2010-11 underscored a number of issues which created some access challenges for the intended recipients, including lack of provider awareness and buy-in and gaps in coverage (e.g., access through hospitals and other providers). The department responded to some of these issues to overcome access barriers during this 2010-11 reporting period.
71 “Cardiovascular disease, cancer, diabetes and respiratory diseases are the major diseases contributing to an unacceptable gap in life expectancy. Department of Health and Ageing 2009, Closing The Gap: Tackling Chronic Disease - The Australian Government’s Indigenous Chronic Disease Package Booklet p.1.
76KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Qualitative evidence collected in 2010-11 suggests that the measure is highly valued by the majority of stakeholders consulted, who viewed it as a means to enhance access to medication. 1.22 Potential effects based on implementation findingsFigure 9 below is the causal pathway for the PBS Co-payment measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
Figure 9: PBS Co-payment causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect72 and the observed impacts.73 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below.
72 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.73 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
77KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the measure, and despite some initial implementation issues, the measure was ‘on track’ to achieving its identified outputs in 2010-11. All of the key dependencies/assumptions for this measure were in place in 2010-11. The plausibility of effect in 2010-11 is therefore not affected.
Table 15: Assessment of key dependencies of the B1 measure.
Key dependencies
Finding Evidence
Primary health care practices are registered for the PIP Indigenous Health Incentive74
Practices are registered, but there is scope to increase practice participation. As at May 2011 56 per cent of all Indigenous health services had registered for the PIP Indigenous Health Incentive, which is almost double the rate of mainstream general practices (28 per cent). However, there are many more mainstream general practices than IHSs eligible for registration.
Empirical evidence: analysis of Medicare data
Benefits outweigh administrative costs to primary health care practices
The benefits outweigh administrative costs to primary health care practices which have registered. The measure has not resulted in a significant administrative burden on primary health care practices.
Qualitative information gathered from a small group of relevant stakeholders and the department; and empirical evidence from analysis of Medicare data
74 The main group of eligible prescribers of CtG scripts are prescribers located in primary health care practices registered for the PIP Indigenous Health Incentive (B3a measure). As such, there are clear links between the PBS Co-payment (B1) and the PIP Indigenous health Incentive (B3a) measures.
78KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Finding Evidence
Aboriginal and Torres Strait Islander patients participate
There has been a high level of participation in the measure by Aboriginal and Torres Strait Islander patients to date.
Qualitative information gathered from a small group of relevant stakeholders; and empirical evidence from analysis of PBS data
Patients have willingness and support to adhere to medicines regimen
The measure is having a positive impact on patient access to medicines and compliance with medicine regimens.
Qualitative information gathered from a small group of relevant stakeholders.
Approved suppliers participate
A majority (65 per cent) of all community pharmacies in Australia dispensed at least one CtG script in the 12 months to 31 May 2011. There were some initial issues with lack of provider buy in, however these do not appear to be ongoing, and rates have increased over time.
Qualitative information gathered from a small group of relevant stakeholders, and empirical evidence from analysis of PBS data.
Prescribed medicines are required for chronic disease management
Medicines prescribed include those required for chronic disease management. A small majority (54%) of medicines prescribed are those related to conditions other than chronic disease (e.g., analgesics, a range of drugs for mental health conditions, antibacterials and vaccines). The wide range of medicines dispensed is consistent with the eligibility criteria for patient registration.
Empirical evidence from analysis of PBS data
Contextual considerations
Participation in the PBS Co-payment measure (by both primary health care providers and community members) is likely to be influenced by the availability of existing pharmaceutical subsidy schemes. This in includes the S100 RAAHS program in remote and very remote areas.
Analysis of measure, PBS data and S100 RAAHS data and documentation
79KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
80KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 16 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above).The evaluation observed that the measure is reducing financial barriers to accessing pharmaceuticals for many Aboriginal and Torres Strait Islander people. Change in patients’ use of medicines for chronic disease management, or improvements in Aboriginal and Torres Strait Islander peoples’ chronic conditions are yet to be evaluated .The evaluation requires access to relevant empirical evidence to assess whether the success of uptake of this measure has translated to improvements in access to PBS medications. A confounding factor in this evaluation is that an unknown share of CtG scripts represents direct substitution of PBS scripts that would otherwise have been dispensed under current PBS co-payment arrangements. The key contextual factor influencing the effectiveness of this measure is the availability of other existing pharmaceutical subsidy schemes, particularly the provision of PBS listed medications free of charge under the Section 100 Remote Area Aboriginal Health Services Program (S100 RAAHS). Table 16: Assessment of expected and observed impacts of the B1 measure based on implementation progress.
Expected impacts
Observed impacts Evidence
Reduced financial barrier to purchase of pharmaceuticals
The measure is reducing financial barriers to accessing pharmaceuticals for many Aboriginal and Torres Strait Islander people.
Qualitative information gathered from a small group of relevant stakeholders
Increase in patients’ use of medicines for chronic disease management
At this stage, the evaluation is not able to measure change in use of medicines for chronic disease management.
Not applicable
Improvements in Aboriginal and Torres Strait Islander peoples’ chronic conditions
Data is not available for the First Monitoring Report.
Not applicable
81KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected impacts
Observed impacts Evidence
Contextual considerations
The increased presence of the S100 RAAHS program is likely to have contributed to the low uptake of CtG scripts in the Northern Territory compared to other states.
Empirical evidence from analysis of PBS and S100 RAAHS data
1.23 Measure overviewThe PBS Co-payment measure aims to contribute to the improved management of chronic disease by ensuring patients have affordable access to required medications. The measure provides financial subsidy of the co-payment for PBS medicines prescribed by providers at eligible practices for eligible patients and dispensed by approved suppliers. Patients are provided with scripts annotated by eligible prescribers as “CtG” to indicate inclusion within the PBS Co-payment measure. Eligible prescribers of CtG scripts include those located in primary health care practices registered for the PIP Indigenous Health Incentive (B3a measure) and IHSs who are not registered with the PIP Indigenous Health Incentive but who meet certain criteria including being a “provider of Medicare rebated services”. 75 The ‘Special Arrangements’ for non-PIP Indigenous Health Incentive registered IHSs excludes IHSs in remote or very remote locations.76 Medical specialists can also now prescribe under the PBS Co-payment measure, where an eligible patient is referred to the specialist by a practice registered by the PIP Indigenous Health Incentive.77 Changes in separate legislation which came into force in September 201078 mean that authorised nurse practitioners can now prescribe certain PBS medicines and can therefore also annotate these scripts for eligible patients, provided they are located at an eligible location.Patients eligible for the PBS Co-payment are “Aboriginal and Torres Strait Islander people of any age who present with an existing chronic disease or are at risk of chronic disease and in the opinion of the prescriber: would experience setbacks in the prevention or ongoing management of
chronic disease if they did not take the prescribed medicine; and are unlikely to adhere to their medicines regimen without assistance
through the measure.”79
75 Department of Health and Ageing n.d., Special arrangements for Indigenous Health Services not currently participating in the Practice Incentives Program (PIP), p. 1.76 ibid. 77 Medicare Australia 2012, Closing the Gap—PBS Co-payment Measure. 78Department of Health and Ageing n.d., Nurse practitioner PBS prescribing.
82KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
It is important to note that “prescriptions for all of an eligible patient’s PBS medicines are covered under the measure whether or not the medicines are being used to treat chronic or acute medical conditions.”80
The PBS Co-payment measure commenced subsidy of co-payments on 1 July 2010. 1.24 Structure of chapter and corresponding Data Appendix Compared to other measures, the evaluation of the PBS Co-payment measure has a higher reliance on quantitative data. The interpretation of this data is subject to multiple caveats. Each of the 17 broad outcomes specified in the Evaluation Framework for this measure has one to four specific evaluation questions relating to the quantitative data, and each of these questions refers to up to five different quantitative indicators. Each of these quantitative indicators can be interpreted and presented in multiple ways, for example, by characteristics of patients (age and concessional status), location (state and remoteness) and as number of scripts or number of patients who are dispensed CtG scripts. The Data Appendix for this chapter (Appendix F) contains a detailed discussion of each of 13 PBS Co-payment measure evaluation questions as specified in the Evaluation Framework, using quantitative indicators. In a number of cases, the necessary data is not yet available. In some cases, the original evaluation questions cannot be addressed with the specified data sources and alternatives are suggested. The Data Appendix covers some additional areas to enhance understanding of the PBS Co-payment measure. This includes: definition of specific terminology used in relation to the PBS Co-payment subsidy (e.g., PBS price subsidy and CtG Co-payment subsidy);81 and a discussion of the relevance of the Section 100 Remote Area Aboriginal Health Services Program (S100 RAAHS)82 in
79 Medicare Australia 2012, Closing the Gap—PBS Co-payment Measure.80 Department of Health and Ageing June 2010, Fact Sheet - Information for General Practitioners
Pharmaceutical Benefits Scheme (PBS) Co-payment Measure (the measure), Department of Health and Ageing, Canberra.81 For example, the “PBS price subsidy” is available to all Medicare registered patients prescribed PBS listed medications for which that patient is eligible. The Safety Net co-payment subsidy is available to all households of Medicare registered patients who reach a particular level of expenditure on PBS listed items. The CtG co-payment subsidy is available to patients who are registered for the measure on all CtG annotated scripts. See Data Appendix for details of references.82 Under the S100 RAAHS Aboriginal and Torres Strait Islander patients residing in certain areas are able to receive PBS listed medicines free of charge under Section 100 of the National Health Act. The S100 RAAHS PBS supply arrangements for Indigenous health services do not require
83KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
remote areas in relation to interpretation of the impact of the measure. Additional tables that contain more detailed analysis, for example, by age of patient, are also presented.1.25 PBS Co-payment Patient eligibility and registrations
The evaluation found that the inclusiveness of the eligibility criteria for the PBS Co-payment measure is highly valued amongst the majority of stakeholders (including primary health care providers and Aboriginal and Torres Strait Islander community members). The breadth of the measure’s definition of eligibility is reflected in the large number of Aboriginal and Torres Strait Islander people (79,076) who were dispensed at least one CtG script in the 12 months to 31 May 2011. This finding was informed by consultations with national stakeholders (relevant peak and representative organisations), primary health care service providers and Aboriginal and Torres Strait Islander community members, and analysis of PBS data. The patient eligibility criteria for the PBS Co-payment measure have not changed since 2009-10. However, as noted above, the operational model for the measure has changed to allow for additional prescribers. National stakeholders and primary health care providers consulted through interviews and community site visits generally considered the patient eligibility criteria for the PBS Co-payment measure to be appropriate, and valued the inclusion of people less than 15 years of age and those at risk of developing a chronic disease. However, many national stakeholders and primary health care providers reported that the variation between the eligibility criteria for the PIP Indigenous Health Incentive and the PBS Co-payment measure creates confusion for providers. A number of these primary health care providers and national stakeholders reported that the joint registration form adds to this confusion. A small number of other stakeholders felt that having the two sets of eligibility criteria set out together is helpful, as it is convenient to have the one form. The majority of stakeholders engaged through site visits – both service providers and Aboriginal and Torres Strait Islander community members, provided positive commentary on the measure, including the fact that (in their
the provision of individual patient medicine dispensing records to Medicare Australia. PBS medicines are supplied in bulk to an approved IHS and are provided to patients with no co-payment charge and without the need for a PBS prescription. See: Department of Health and Ageing n.d., Alternative Arrangements for Medicines, Aboriginal Health Services and Pharmaceutical Benefits Scheme (PBS).
84KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
understanding) it is available to all Aboriginal and Torres Strait Islander people. Around 70 per cent of stakeholders consulted raised such issues. At only one community focus group, participants indicated a reason why eligible patients might choose not to participate in the measure: their perceived need for the financial benefit. For example, eligible participants may be employed and therefore choose to pay for their medicines as they can afford to do so. In general, community members discussed the fact that many Aboriginal and Torres Strait Islander people are on low incomes, and many also have one or more chronic diseases, requiring multiple medications. This view was held across urban, regional and remote locations. Therefore, they saw the subsidy as beneficial to all Aboriginal and Torres Strait Islander people. Data on the number of patients registered for the PBS Co-payment measure and their distribution across service types was not available for 2010-11. However, at least 79,076 Aboriginal and Torres Strait Islander people registered, as this is the number dispensed at least one CtG script. Data was available on the distribution of patients and scripts by age, concessional status, jurisdiction, and remoteness. Table 17 provides a profile of patients registered for the PBS Co-payment Subsidy measure and those receiving CtG scripts in the May quarter of 2011 within these four main groups.83 This data indicates that in 2010-11 the vast majority of CtG scripts were provided to concession card holders and that approximately half of CtG scripts were provided to patients between the ages of 15 and 55 years. Table 17: Distribution of patients and scripts, for main groups: May quarter 2011.84
Main Group Proportion of patients Proportion of CtG scripts
Concessionary beneficiaries
74% 80%
15 to 55 year olds 58% 52%Outer regional 32% 31%NSW 43% 42%
This distribution of patients is over representative of older age groups as would be expected. It is also under-representative of Northern Territory as a consequence of the high utilisation of the S100 RAAHS in that territory.
83 The full tables are presented in Appendix F.84 Pharmaceutical Benefits Scheme (PBS) data, provided by the Department of Health and Ageing.
85KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Prescribing of CtG scripts
The evaluation found that at least 2,128 practices, including IHSs, had registered for the measure by 31 May.85 At the same time, there were some initial challenges associated with awareness about and reluctance by some GPs to participate in, the PBS Co-payment measure.86
This finding was informed by consultations with national stakeholders (relevant peak and representative organisations), the measure manager, primary health care service providers, Regional Forums, and analysis of PBS data. Consultations conducted through community site visits suggest that there was an initial lack of awareness about the PBS Co-payment measure amongst GPs. In a number of sites visited in 2010-11, community members and ICDP workers (e.g., ATSIOWs, IHPOs) reported initial problems with GPs’ awareness and understanding of CtG scripts (around 65 per cent of stakeholders consulted raised such issues). Specifically, these stakeholders reported that GPs were unclear about patient eligibility, and the types of scripts (medications) that could be annotated as CtG. Participants at Regional Forums seconded this, and provided examples of instances where patients had to explain the measure to GPs. Pharmacists engaged through the community site visits had a range perspectives of GP understanding of and engagement with the measure. Some pharmacists stated that GPs are now largely aware of the measure and understand how it works, and others stated that there is still lack of awareness amongst GPs in some locations. The department advised that these issues around GP awareness are generally restricted to the mainstream primary health care sector, as IHSs have, for the most part, been supportive of the measure and have promoted it within their communities. 87 In addition, many IHSs which are now participating in the PBS Co-payment measure would have been involved in the previous QUMAX program (Quality Use of Medicines Maximised in Aboriginal and Torres Strait Islander Peoples Program) which is similar to the PBS Co-payment measure in intent. 88
85 The number of practices registered for PIP Indigenous Health Incentive was 2,218 and hence, given that some non-PIP IHSs can also register for CtG under the “Special Arrangements”, and all PIP Indigenous health Initiative registered practices are CtG registered, 2,218 represents a minimum number of CtG registered practices. 86 KPMG consultation with measure manager, 28 October 2011.87 KPMG consultation with measure manager, 28 October 2011.88 Pharmacy Guild of Australia n.d., QUMAX Program (webpage).
86KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Despite this apparent lack of awareness, the majority of community stakeholders reported that uptake of the measure by primary health care services has been strong. This is consistent with the data, which shows there has been stronger than expected participation in the measure amongst practices. Table 18 below, provides an overview of projected versus actual patients with at least one CtG script, and CtG scripts dispensed for 2010-11. This data shows that the number of actual patients with at least one CtG script exceeded the projected number of patients more than two-fold. Table 18: Projected and actual utilisation of CtG scripts 2010-11.89
Indicator Projected ActualPatients with at least one CtG script
38,393 79,076
CtG scripts dispensed n/a 859,370Average scripts dispensed per patient
n/a 10.9
Data on the location (distribution of prescribing practices across urban to remote locations) compared to distribution of the Aboriginal and Torres Strait Islander population suggests that there was a high correlation between the two in 2010-11 the exception was remote and very remote locations. Aboriginal and Torres Strait Islander people in many of these locations have existing access to free medicines through the S100 RAAHS arrangements and these are also locations with low numbers of community pharmacies available. For these reasons, it is not surprising to see low numbers of prescribing practices in remote and very remote locations, relative to the Aboriginal and Torres Strait Islander population. Table 19 below shows the exception was remote and very remote locations. Aboriginal and Torres Strait Islander people in many of these locations have existing access to free medicines through the S100 RAAHS arrangements and these are also locations with low numbers of community pharmacies available. For these reasons, it is not surprising to see low numbers of prescribing practices in remote and very remote locations, relative to the Aboriginal and Torres Strait Islander population.
89 The projected and actual number of patients is sourced from PBS data provided by the Department of Health and Ageing. There is no information currently available to the evaluators on the expected number of scripts dispensed.
87KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 19: Comparison of geographical distribution of prescribing practices (as at May 2011) to distribution of Aboriginal and Torres Strait Islander population (2006).
Location Distribution of prescribing practices90
Population distribution91
Major cities 31% 31%Inner regional 27% 22%Outer regional 31% 23%Remote 7% 8%Very remote 3% 16%Unknown 1% N/A
A number of primary health care providers engaged through the 2010-11 site visits, including GPs, noted issues with GPs having to annotate CtG scripts by hand. Specifically, these stakeholders thought that there was room for human error with this process, and reported that sometimes GPs forget to include the CtG annotation, leading to the patient being denied free/reduced price medicines at the pharmacy. One pharmacist engaged through the community site visits said that while the majority of permanent GPs remember to annotate CtG scripts, locums were often forgetting to, or were not aware of this option. One GP engaged during the site visits indicated they were expecting software upgrades to support automatic annotation, but understood this was not yet available. This is despite the fact that “the Department executed funding agreements with PBS prescribing and dispensing software vendors to upgrade their software as specified in the resource document. With the exception of Medical Director, all PBS prescribing software was upgraded with ‘CtG’ functionality by 30 June 2010.”92 Access to CtG scripts outside of primary health care practices was reported as an issue through the 2010-11 consultations. Consulted pharmacists consistently stated that patients being unable to access CtG scripts through hospitals greatly limits patient access particularly in rural and remote areas where the hospitals may be the only source of medicines. One pharmacist also
90 Based on Pharmaceutical Benefits Scheme (PBS) data, provided by the Department of Health and Ageing.91 Australian Bureau of Statistics 2007, Population Distribution, Aboriginal and Torres Strait Islander Australians, 2006, cat. no. 4705.0.92 KPMG 2013, Indigenous Chronic Disease Package National Monitoring and Evaluation Project: Baseline Report, Australian Government Department of Health and Ageing, Canberra.
88KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
noted that some patients are confused by access being limited to only certain practices (i.e., only those registered for the PIP Indigenous Health Incentive).Dispensing of CtG scripts
The evaluation found that around 65 per cent of all community pharmacies in Australia93 dispensed at least one CtG script in 12 months to 31 May 2011. This was in the context of some initial implementation challenges related to pharmacist awareness of this measure. This finding was informed by consultations with national stakeholders (relevant peak and representative organisations), primary health care providers (including pharmacists) and community member consultations conducted through site visits, as well as Regional Forums and analysis of PBS data.An initial lack of awareness of the measure amongst pharmacists was also reported by primary health care providers and community members engaged through the 2010-11 site visits. Specifically, a number of these stakeholders provided examples of patients presenting to community pharmacies and the pharmacist not being aware of what their CtG script was (i.e., the target group, what it entitled the patient to and what the pharmacist was required to do with it). Some community members engaged during focus groups reported that they, or people they knew, were required to explain the CtG script (the purpose and process) to pharmacists. In a small number of cases, Aboriginal people reported that pharmacists had questioned their Aboriginality. Similar experiences were reported through the Sentinel Sites Evaluation.94 Community members at over half of the community focus groups felt that this type of experience was embarrassing and associated with ‘shame’. They also reported that it may or had discouraged people from accessing community pharmacies in the future. Stakeholders participating in the Regional Forums also described the initially poor understanding of the measure among pharmacists, and indicated that these issues seem to have had a negative impact on initial utilisation of CtG scripts by some Aboriginal and Torres Strait Islander community members. Some of the national stakeholders consulted linked this issue to a lack of promotion they had a perception that insufficient printed material was provided to pharmacists. It should be noted that the department promoted the measure to peak organisations through extensive consultations.
93 There are around 5,000 community pharmacies in Australia, according to the fact sheet “Australia’s unique system of community pharmacy”.94 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing. Canberra.
89KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Pharmacists consulted through community site visits said that they heard about the measure from a range of sources, such as newsletters from peak organisations, their PBS contacts and the Pharmacy Guild. No pharmacists discussed formal systems to support participation such as meetings or consultations. Overall, feedback from pharmacists about how they found out about and were encouraged to engage with the measure was mixed. Whilst some were involved in the measure’s developmental process, others only heard of CtG through colleagues or other informal contacts. Some pharmacists had a direct point of contact for information and assistance, whilst others had to proactively seek their assistance through the Pharmacy Guild.A number of ICDP staff (ATSIOWs and IHPOs) engaged through community site visits discussed how they had worked with pharmacists to improve their understanding of the measure, including providing information resources and having discussions with pharmacists. According to both Regional Forum participants and community stakeholders, the initial lack of awareness amongst pharmacists improved over time and the majority of pharmacists reportedly understood the measure at the time the site visits and forums were undertaken (late 2010). This is consistent with the PBS data on CtG scripts, which shows that around 65 per cent of all community pharmacies in Australia95 dispensed at least one CtG script in 12 months to 31 May 2011.As Table 20 shows, the number of pharmacies that dispensed at least one CtG script was 3,278 for the May quarter 2011, increasing from 1,605 for the August quarter 2010. The number of participating pharmacies was 30 per cent higher than the projected rate at June 2011.
95 There are around 5,000 community pharmacies in Australia, according to the fact sheet “Australia’s unique system of community pharmacy”.
90KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 20: Number of pharmacies (active in that quarter) by jurisdiction and Aboriginal and Torres Strait Islander people per registered pharmacy.96 97 98
Quarter NSW QLD WA NT VIC SA TAS ACTTotal
Aug 2010 562 427 150 11 228 133 65 291,60
5
Nov 2010 832 646 259 17 356 225 100 452,48
0Feb2011 990 745 324 20 413 260 107 53
2,912
May 20111,09
9 829 383 30 464 305 111 573,27
8Aboriginal and Torres Strait Islander people per participating pharmacy 150 194 199 2287 79 100 181 83 172
As this table shows, the distribution of CtG dispensing community pharmacies across jurisdictions remained consistent for each quarter, suggesting a consistent rate of uptake across jurisdictions. There were large differences across the states and territories in the numbers of pharmacies and the number of Aboriginal and Torres Strait Islander people per participating pharmacy. For example, of the participating community pharmacies in the May quarter 2011, 34 per cent were in New South Wales and in contrast, just under 1 per cent were in the Northern Territory. The low number of participating pharmacies in Northern Territory is consistent with both the lower number of community pharmacies in the territory, and the existing availability of PBS listed items, free of charge to patients through remote area IHSs as a result of the S100 RAAHS program. The higher number of Aboriginal and Torres Strait Islander people per registered pharmacy in New South Wales, Queensland and Western Australia, compared to South Australia and Victoria may also be explained by 96 Pharmaceutical Benefits Scheme (PBS) data, provided by the Department of Health and Ageing.97 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.98 Australian Bureau of Statistics 2007, Population Distribution, Aboriginal and Torres Strait Islander Australians, 2006, cat. no. 4705.0.
91KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
remoteness. In Western Australia and Northern Territory, 20 and 37 per cent of Aboriginal and Torres Strait Islander people, respectively, live in remote and very remote locations. In these more remote areas, where pharmacies do participate in the PBS Co-payment measure, there are likely to be fewer people per pharmacy. These areas are also likely to have a higher utilisation of S100 RAAHS. Overall, the number of CtG scripts dispensed per pharmacy per quarter increased from 41 in the August quarter 2010 to 106 in the May quarter 2011. The relative growth in scripts dispensed per pharmacy was 159 per cent for Australia overall. The high rate of growth in Tasmania is likely to be a consequence of the more limited number of participating pharmacies accommodating the growth in scripts dispensed. The highest number of CtG scripts dispensed per pharmacy in the May quarter 2011 was 151 for the Northern Territory, as Table 21 shows. This high ratio of scripts per pharmacy for Northern Territory is a probably a consequence of the small numbers of registered pharmacies in the state and one region, Darwin, having the greatest concentration of Aboriginal and Torres Strait Islander people outside the remote and very remote locations (which have access to S100 RAAHS). Table 21: Average number of CtG scripts dispensed per pharmacy per quarter (pharmacies active in that quarter) by jurisdiction.99 100
Quarter NSW QLD WA NT VIC SA TAS ACTAustralia
Aug 2010 48 45 32 58 39 34 17 21 41Nov 2010 98 82 70 131 58 65 31 37 78Feb2011 105 88 84 142 58 79 42 38 86May 2011 134 109 96 151 69 91 60 47 106Ratio of May 2011 to August 2010 2.79 2.42 3.00 2.60 1.77 2.68 3.53 2.24 2.59
Consultations undertaken with pharmacists during 2010-11 provide an update on what was reported in the Baseline Report101 for the 2009-10 year:
99 Based on Pharmaceutical Benefits Scheme (PBS) data, provided by the Department of Health and Ageing.100 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.101 KPMG 2013, Indigenous Chronic Disease Package National Monitoring and Evaluation Project: Baseline Report, Australian Government Department of Health and Ageing, Canberra.
92KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
“research and evaluation of similar programs to the PBS Co-payment have shown that they may be detrimental to organisations (Indigenous Health Services and community pharmacies) due to additional costs102 and the requirement to undertake more administration.”103 No pharmacists engaged during 2010-11 raised issues relating to the burden (administrative or financial) of ongoing reimbursement payments. One pharmacist commented that the process for the PBS Co-payment measure is more user friendly than the previous QUMAX Program. Utilisation of CtG scripts by Aboriginal and Torres Strait Islander people
The evaluation found that utilisation of CtG scripts by Aboriginal and Torres Strait Islander people exceeded the department’s total target for the measure in 2010-11, the first year of implementation of this measure. This finding has been informed by analysis of PBS data and consultations with community members through 2010-11 site visits.
Overview of CtG script utilisation
The department projected that there would be 70,000 patient beneficiaries using CtG scripts for the PBS Co-payment measure; to be achieved by the end of 2012-2013 fiscal year104. Exceeding this, 79,076 Aboriginal and Torres Strait Islander people were dispensed at least one CtG script in 2010-11. The number of patients dispensed at least one CtG script each quarter increased significantly over the 12 months to end May 2011. In the May quarter 2011, 54,628 patients were dispensed at least one CtG script, which represents an increase of 35,434 (2.8 fold) since the August quarter 2011 (see Table 22 below). Of all the CtG scripts dispensed between the August quarter 2010 and the May quarter 2011, 40 per cent were dispensed in the last quarter reflecting the increasing rate of uptake of these scripts over the 12 months. Consistent with this overall strong uptake of CtG scripts, community members at all focus groups (a total of 20 focus groups) conducted during the site visits demonstrated high awareness of the measure including in remote locations,
102 Australian Healthcare Associates 2010, Final Report: Review of the Existing Supply and Remuneration Arrangements for Drugs Listed under Section 100 of the National Health Act 1953, AHA, Melbourne.103 Kelaher M, Dunt D, Taylor-Thompson D, Harrison N, O’Donaghue L, Barnes T & Anderson I 2006, ‘Improving access to medicines among clients of remote area Aboriginal and Torres Strait Islander Health Services’. Australian and New Zealand Journal of Public Health, vol 30, no. 2, pp. 177-183.104 Department of Health and Ageing June 2010, Subsidising PBS medicine co-payments.
93KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
and community members at almost all of these reportedly had utilised it to access pharmaceuticals. With the available data, it is not possible to estimate the proportion of PIP Indigenous Health Initiative registered patients who are also registered for CtG scripts. However, it can be concluded that it is likely that Aboriginal and Torres Strait Islander people registered for the PIP Indigenous Health Initiative represent no more than 70 per cent of people dispensed CtG scripts in the first year.105
Utilisation of CtG scripts by key patient characteristics
Tables presenting a detailed breakdown of CtG scripts dispensed by remoteness area, jurisdiction, age and concessional status are contained in Appendix F. These detailed results are reported for patient numbers, scripts numbers and average scripts per patient. Key points from these tables are summarised below.In 2010-11, 31 per cent of CtG scripts were dispensed in major cities and 10 per cent were dispensed in remote or very remote locations, which is consistent with the existing access to free of charge medicines through the S100 RAAHS and the limited number of pharmacies in remote and very remote locations. The highest proportion of CtG scripts were dispensed in New South Wales (42 per cent), aligning with the high numbers of Aboriginal and Torres Strait Islander people in this state. In contrast, only 1 per cent of CtG scripts were dispensed in the Northern Territory; this is likely to be attributable to the high rates of access to S100 RAAHS scripts in this jurisdiction, as previously noted.A higher proportion of CtG scripts were dispensed to older people than younger people in 2010-11; 6 per cent of CtG scripts were dispensed to people under the age of 15 while 41 per cent were dispensed to people over the age of 55. The proportion of patients dispensed at least one CtG script whose status was concessional ranged from 66 per cent in the November quarter 2010 to 74 per cent in the February quarter 2011. Additionally, 283 RPBS patients were dispensed at least one CtG script in 2010-11. The number of patients dispensed at least one CtG script, by concessional status is presented by in Table 22. 106
105 The number of patients who were dispensed at least one CtG script in the 12 months to the end of May 2011 was 79,076. The number of patients registered for the PIP Indigenous Health Initiative as at 31 May 2011 was 49,741 (see Chapter on B3a measure). The former initiative has broader eligibility criteria compared to the latter; it also includes people at risk of a chronic disease, including people under the age of 15, in addition to people with a chronic disease. Hence, the maximum proportion of CtG script registered patients is 70 per cent if all PIP Indigenous Health Initiative registered are co-registered for PBS Co-payment subsidies.
94KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 22: Patients dispensed at least one CtG script by patient category and quarter (2010-11).107
Patient Category (PC) Aug 2010 Nov 2010 Feb 2011 May 2011Concessional patients
14,276 27,995 31,920 40,610
Ordinary 13,444 25,059 31,761 40,003Safety net 832 2,937 159 607General patients 4,863 10,042 10,788 13,873Ordinary 4,779 9,655 10,771 13,843Safety net 84 387 17 30RPBS patients 55 139 125 145Ordinary NR* 96 NR* NR*Safety net NR* 43 NR* NR*Total 19,194 38,177 42,833 54,628
* For confidentiality reasons, this number is not reported.
The number of scripts dispensed by concessional status and jurisdiction over the 12 months to 31 May 2011 is presented in Table 23. Of these scripts: items dispensed to concessional patients represented 80 per cent of total
dispensed CtG scripts; concessional patients were dispensed 67 per cent and 85 per cent of CtG
scripts in Australian Capital Territory and Victoria respectively; 42 per cent of CtG scripts were dispensed in NSW and 1 per cent in NT as
noted previously;108 and the highest scripts per Aboriginal and Torres Strait Islander person was 2.5
in Victoria and the lowest was 0.2 in Northern Territory where there is the highest utilisation of the S100 RAAHS program.
106 If the numbers in this table are summed, they will not match the total number of patients dispensed at least one script, for two reasons, First, people change their concessional status over the year and therefore can be counted twice (once under each category). Second, this data relates to the number of patients who were dispensed at least one CtG script in each quarter, and hence patients could be counted up to four times in this 12 month period.107 Derived from Pharmaceutical Benefits Scheme (PBS) data, provided by the Department of Health and Ageing.108 Also as noted previously, the low levels of CtG scripts dispensed in Northern Territory need to be considered in conjunction with the higher utilisation of PBS items supplied to IHSs through S100 RAAHS program.
95KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 23: Number of CtG scripts dispensed over 12 months to 31 May 2011 by patient category and state or territory.109,110
PC NSW QLD WA NT VIC SA TAS ACT Total
Conc.289,59
7174,66
068,78
77,523 72,11
955,65
512,12
84,668 685,1
37
Ord.265,46
5161,49
064,46
87,360 65,45
851,64
911,05
34,407 631,3
50
SN24,132 13,170 4,319 163 6,661 4,006 1,075 261 53,78
7
Gen.67,961 52,216 17,65
32,687 12,83
511,85
32,921 2,296 170,4
20
Ord.65,058 50,378 16,87
82,656 12,48
311,36
72,842 2,238 163,9
00SN 2,903 1,838 775 30 352 486 79 57 6,520RPBS 1,787 1,160 256 37 218 93 259 NR* 3,812Ord. 1,521 1,044 241 NR* 199 NR* 218 NR* 3,350SN 266 116 15 NR* 19 NR* 41 NR* 462
Total359,34
5228,03
586,69
610,24
785,17
267,60
115,30
86,966 859,3
70Scripts per capita
2.4 1.6 1.2 0.2 2.5 2.4 0.8 1.6 1.7
Scripts % of Total
42% 27% 10% 1% 10% 8% 2% 1% 100%
Legend: PC Patient Category, Conc Concessional, Ord. Ordinary, SN Safety Net, Gen. General.* For confidentiality reasons, this number is not reported.
As the data in Table 22 and Table 23 shows, the majority of CtG scripts were dispensed to concessional patients and thus most were dispensed free of charge.
Utilisation of CtG scripts by ATC category
393,940 of the CtG scripts dispensed in the 12 months ended 31 May 2011 were in the ATC categories of Cardiovascular system (C), Respiratory system
109 Based on Pharmaceutical Benefits Scheme (PBS) data, provided by the Department of Health and Ageing.110 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
96KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
(R) or Drugs for diabetes (A10). These are the broad categories for medicines to manage and treat three of the four chronic diseases that are “the major diseases contributing to an unacceptable gap in life expectancy”.111 They account for 46 per cent of total CtG scripts dispensed in this period.The following table summarises the ATC of medicines dispensed through the measure in the 12 months to 31 May 2011, by two categories of remoteness (very remote/remote and other). As this table shows, there was a small variation by remoteness, in relation to cardiovascular and nervous system items. There is also significant dispensing outside the three key chronic disease most notably nervous system drugs (which includes analgesics and a range of drugs for mental health conditions) and anti-infectives (which includes antibacterials and vaccines). The wide range of medicines dispensed is consistent with the eligibility criteria for registration (with or at risk of chronic disease) and that “prescriptions for all of an eligible patient’s PBS medicines are covered under the measure whether or not the medicines are being used to treat chronic or acute medical conditions.”112
111 “Cardiovascular disease, cancer, diabetes and respiratory diseases are the major diseases contributing to an unacceptable gap in life expectancy.” Department of Health and Ageing 2009, Closing The Gap: Tackling Chronic Disease - The Australian Government’s Indigenous Chronic Disease Package Booklet, viewed 12 December 2012.112 Department of Health and Ageing 2010, Fact Sheet - Information for General Practitioners
Pharmaceutical Benefits Scheme (PBS) Co-payment Measure (the measure), Department of Health and Ageing, Canberra.
97KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 24: CtG Scripts dispensed by ATC category in 12 months to 31 May 2011 by remoteness.113
Descriptionand (ATC)
Items in major cities, inner and outer regional
% of CTG Scripts
Items in remote and very remote
% of CTG Scripts
Items in Australia
% of CTG Scripts
Alimentary tract and metabolism – drugs used in diabetes (A10)
63,836 8% 9,187 11% 73,023 8%
Alimentary tract and metabolism – other (A ex A10)
55,576 7% 5,903 7% 61,478 7%
Anti-infective for systemic use (J)
86,439 11% 9,067 10% 95,505 11%
Cardiovascular system (C)
227,709
29% 30,220 35% 257,929
30%
Musculo-skeletal system(M)
19,623 3% 2,258 3% 21,881 3%
Nervous system (N)
173,955
23% 14,976 17% 188,931
22%
Respiratory system (R)
57,549 7% 5,439 6% 62,988 7%
Other 87,416 11% 10,218 12% 97,634 11%Subtotal Chronic diseases (A10, C and R)
349,095
45% 44,845 51% 393,940
46%
Total 772,10
3100% 87,267 100% 859,37
0100%
Appendix F presents a series of additional tables that detail types of medicines by geography and patient characteristics. This appendix also presents a number of comparisons of the mix of medicines as specified in Evaluation Framework, including a comparison with the general population dispensing
113 Based on Pharmaceutical Benefits Scheme (PBS), data provided by the Department of Health and Ageing.
98KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
and with S100 RAAHS supply. These comparisons have a number of caveats that need to be considered in their interpretation, which are detailed in that appendix.
Interpretation and data limitations
The number of Aboriginal and Torres Strait Islander people dispensed at least one CtG script in 2010-11 (79,076) is an underestimate of the number who have access to PBS listed medicines with a subsidised or no co-payment. Some Aboriginal and Torres Strait Islander people have access to PBS listed medicines free of charge as a result of the S100 RAAHS program. In the May quarter 2011, 365,683 items were supplied via S100 RAAHS to remote and very remote IHSs and dispensed free of charge to Aboriginal and Torres Strait Islander people. This compares to 347,938 CtG scripts dispensed in the same quarter.114 115 The complementary nature of the S100 RAAHS program and the PBS Co-payment measure needs to be acknowledged as the basis for the low uptake of CtG scripts in the Northern Territory (4,532 in May quarter 2011) compared to other states, for example, New South Wales (147,091 May quarter 2011). It should not be interpreted as indicating that Aboriginal and Torres Strait Islander people residing in Northern Territory had comparatively less access to PBS listed medicines with a subsidised co-payment or free of charge. In the same quarter, IHSs in the Northern Territory were supplied 187,625 PBS medicines whereas NSW IHSs were supplied with 3,417 PBS medicines through the S100 RAAHS program.In addition, the number of CtG scripts dispensed (827,493) is an over estimate of the number of additional PBS scripts dispensed to CtG registered patients, where additional is relative to what would have occurred in the absence of the initiative.While some of these CtG scripts are likely to represent scripts that would not otherwise have been dispensed, others represent scripts that would have otherwise been dispensed to Aboriginal and Torres Strait Islander patients under current PBS co-payment arrangements. This proportion cannot be
114 The number of patients supplied with medicines under the S100 RAAHS program is not available to the evaluators, nor is the number of supplied PBS listed medicines through both the CtG measure and S100 RAAHS program. However, if it is reasonable to assumed that it is unlikely that all patients supplied with PBS listed items through S100 RAAHS have also been dispensed at least one CtG script, then it is possible to conclude that the 79,076 patients supplied at least one CtG script is an underestimate of the number of Aboriginal and Torres Strait Islander people who had the PBS co-payment subsidised and hence access to medicines improved in 2010-11.115 See the Data Appendix (B1) for tables relating to S100 RAAHS supply and CtG utilisation.
99KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
estimated with data currently available. It is expected to be explored in future evaluation reporting. One example of this is as follows: of all dispensed CtG scripts, seven per cent were concessional, general or RPBS safety net and hence had no co-payment or a reduced co-payment independent of the measure. An unknown proportion of these scripts would have otherwise been available at a reduced or no payment. However, the majority (93 per cent) of CtG scripts were not supplied on the Safety Net, and hence represent scripts supplied at reduced or no co-payment compared to what would otherwise have occurred. Finally, the number of PBS scripts (CtG and non-CtG) dispensed to Aboriginal and Torres Strait Islander people registered for CtG is an indicator specified in the Evaluation Framework. The total number of PBS listed medicines dispensed to CtG registered patients is underestimated by the number of CtG scripts dispensed in the 12-month period, for two reasons: the number of people using CtG scripts increased over the period, hence,
some CtG registered patients would have accessed CtG scripts for only some of these 12 months and conventional PBS scripts in other months; and
not all PBS scripts dispensed to a CtG registered patient are CtG annotated, for range of reasons including the prescriber’s assessment of eligibility of the script for subsidy and patient attendance at a non-CtG registered practice. Hence, the average number of CtG scripts per patient for the May quarter 2011 (see Appendix F underestimates the average number of all PBS scripts dispensed per patient.
Data to allow exploration of this issue is expected to be available for future evaluation reporting.Reduced financial barriers and improved patient access and compliance
The evaluation found some emerging evidence that in 2010-11 the PBS Co-payment measure was reducing financial barriers for Aboriginal and Torres Strait Islander people, and there were initial indications that the measure is having a positive impact on patient access to medicines and compliance with medicine regimens. This finding has been informed by consultations with national stakeholders (relevant peak and representative organisations), primary health care providers and community members through site visits and Regional Forums. The PBS Co-payment measure is expected to reduce the financial barriers and thus increase access to medicines by Aboriginal and Torres Strait Islander people for the management of chronic disease.
100KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Stakeholders consulted during 2010-11 commented that the PBS Co-payment measure is a valuable means to reduce the financial barriers faced by Aboriginal and Torres Strait Islander patients in accessing needed medications. Consultation with participants from the national to local levels repeatedly confirmed this sentiment. Community members consulted during site visits frequently said that access to free or reduced price pharmaceuticals reduced the likelihood that patients would share their medication with family members and friends who could not afford their own medication. They also commonly reported a reduction in people prioritising other expenses over medications, such as food and bills. In this context, community members emphasised the importance of the PBS Co-payment for people with low incomes, such as single mothers and older people on a pension. Community members and primary health care providers consulted through site visits also indicated that the PBS Co-payment measure is particularly important for people with chronic disease requiring multiple medications.Pharmacists engaged through community site visits also felt (as previously noted) that the measure allows Aboriginal and Torres Strait Islander people to access to medications they may not have previously been able to access due to affordability issues. One pharmacist commented that in relation to affordability and financial constraints, the measure is an improvement on the QUMAX program.Some participants at Regional Forums indicated that patients’ increased access to free or reduced price pharmaceuticals increased pressure on those patients to share medications with family members and friends who did not have CtG scripts. Medication sharing may be an unintended consequence of the PBS Co-payment measure; the extent of which is unknown. However, as previously noted it was the perception of most community members that sharing medications had decreased rather than increased as a result of the measure.Consistently, staff working within primary health care organisations identified similar benefits associated with the measure. A number of stakeholders made comments such as “this is the single best Indigenous health initiative in the last 20 years.”116 The PBS Co-payment measure was also strongly supported by peak bodies and other state/territory and national stakeholders consulted; all stakeholders engaged provided positive feedback about the intentions of the measure and the impact it could have and in some cases is having in the community. Many of the stakeholders consulted during 2010-11 suggested that the PBS Co-payment measure is improving medication compliance. Various examples
116 Interview with local GP, South Australia, 15 December 2011. 101
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
were given during Regional Forums of patients who were having their medications dispensed on a more regular basis because of the removal of financial barriers, and of patients who were reportedly re-engaging with their local health service because of CtG scripts. Similar examples were provided in community member focus groups; for example, at one focus group, a participant discussed having to choose between buying food for their grandchildren, who were visiting, and their medicines. These findings are echoed in the Sentinel Sites Evaluation which noted that both community members and stakeholders believed the measure was improving medication compliance.117 Stakeholders consistently noted a number of implementation challenges that have impacted the measure, as described previously. Some pharmacists consulted highlighted the limitations of the PBS Co-payment measure in supporting medications compliance; which they suggested could be improved through patient education, greater access to Domiciliary Medications Management Reviews or inclusion of Dose Administration Aid services. CtG patients are in fact eligible for Domiciliary Medications Management Reviews (known as home medication reviews), which facilitate collaboration between a pharmacist and a GP to improve the management of medications for patients living in the community. It is possible that access to CtG scripts has increased the number of medications some patients take, resulting in an increase in requests for home medication reviews. The capacity to provide additional home medication reviews could be limited in some areas. In summary, while the empirical data required to test whether the uptake of CtG medicines is leading to improved access to PBS medicines is not available at this stage, the emerging evidence supports that hypothesis. In addition, the empirical evidence of the high participation in this program by prescribers, patients and pharmacists supports the view that there is an increased focus on medicines for Aboriginal and Torres Strait Islander people with or at risk of chronic disease. 1.26 Program supports for the PBS Co-payment measureSoftware upgrades
Through the PBS Co-payment measure, the department provided incentive payments to software vendors, to support them in upgrading their software to allow electronic CtG annotation. The evaluation found that software upgrades were largely ‘on track’ in 2010-11, however, there was emerging evidence of some lack of health
117 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
102KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
provider awareness of these upgrades, and that CtG ‘hand annotation’ practices continued through 2010-11.This finding has been informed by consultations with the department, primary health care providers and community members (through site visits), review of documentation provided by the department and analysis of PBS data.Pharmacy software products were updated in 2009-10, as were some prescriber software products, as reported in the Baseline Report.118 In 2010-11, remaining prescriber software upgrades were completed; with Minfos upgrades occurring by mid-July 2010, and Medical Director prescribing software upgrades occurring in November 2010. However, software updates aimed at supporting specialists to annotate scripts were not progressed during 2010-11. There was no information available to the evaluation on software specifications and incentives, and the extent of vendor participation and timing of software activity for 2010-11. The proportion of scripts annotated electronically rather than manually increased from 18 per cent to 40 per cent over the 12 months from August quarter 2010 to May quarter 2011. Within this, there was variation across states and territories, with some of the smallest states and territories (i.e., Tasmania, Northern Territory and Australian Capital Territory) having higher proportions in May 2011; most likely a consequence of the smaller number of participating sites. Table 25: Proportion of CtG scripts annotated electronically by jurisdiction and quarter.119 120
Quarter NSW QLD WA NT VIC SA TAS ACTTotal
Aug 2010 7% 22% 46% 1% 26% 6% 86% 30% 18%Nov 2010 13% 28% 48% 6% 24% 10% 89% 59% 23%Feb 2011 26% 36% 53% 19% 28% 17% 84% 61% 32%May 2011 37% 43% 53% 45% 38% 21% 83% 69% 40%
118 KPMG 2013, Indigenous Chronic Disease Package National Monitoring and Evaluation Project: Baseline Report, Australian Government Department of Health and Ageing, Canberra.119 Based on Pharmaceutical Benefits Scheme (PBS) data, provided by the Department of Health and Ageing.120 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
103KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The fact that 60 per cent of CtG scripts were not being annotated electronically in May 2011 is consistent with the reports from stakeholders, noted earlier, that some scripts are still being hand annotated with CtG. Promotion of the PBS Co-payment subsidy
The evaluation found that the initial promotional activities planned and undertaken by the department in late 2009-10 and early 2010-11 did not fully meet pharmacists’ needs for information, thus leading to a range of ad-hoc state/territory and local activities being implemented later in 2010-11. This finding has been informed by review of program documentation and consultations with the department, national stakeholders (relevant peak and representative organisations), and primary health care providers (including pharmacists) through community site visits. An intensive round of presentations was conducted with key stakeholder groups regarding the parameters and implementation of the PBS Co-payment measure in 2010-11. These stakeholders included: the Australian General Practice Network and their State Based Organisations (SBOs); the National Aboriginal Community Controlled Health Organisation and their affiliates; the Pharmacy Guild of Australia; the Pharmaceutical Society of Australia; and Medicare Australia. The intention was that these stakeholders would in turn promote the measure through their networks.Promotional material was provided to the wider membership of these organisations through newsletter articles that were supplied by the department. The department also developed print materials to support awareness of the measure including a Pharmacy Staff Resource Booklet which was developed in consultation with the Pharmacy Guild of Australia and Pharmaceutical Society of Australia, and published in June 2010. This booklet was distributed to all registered Section 90 pharmacies across Australia. In addition to these planned activities, a number of national and local activities to promote the PBS Co-payment measure were undertaken by stakeholders and the ICDP workforce in 2010--2011.In relation to the implementation of the PBS Co-payment measure, the Pharmacy Guild of Australia (the Guild) was expected by the department to resolve issues with non-compliant pharmacies or other pharmacies that needed support for implementation.121 The Guild also distributed pamphlets and responded to enquiries through the QUMAX phone line, and as reported at the Regional Forums; some of the jurisdictional branches of the Guild took on a proactive role in promoting the scheme with pharmacists and addressing issues that patients encountered with pharmacists.122 Divisions of General
121 Consultation with Pharmacy Guild of Australia in 2011.122 Bendigo Regional Forum conducted in 2011.
104KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Practice SBOs also created and distributed posters to inform pharmacy front line staff about the measure. Consultations conducted with pharmacists and national stakeholders suggest there was inconsistency in the conduct of these promotional activities across the states and territories, and that this type of promotion occurred in an ad-hoc rather than systematic fashion.There were also a number of examples provided of local endeavours to promote the measure through the Regional Forums, consultations with SBOs, and though the community site visits. IHPOs are expected to promote the PBS Co-payment measure among prescribers and pharmacists, and emerging evidence suggests that this was occurring in 2010-11. Regional Forum participants noted that IHPOs (and ATSIOWS) had been either promoting the measure directly to primary health care providers, or indirectly by encouraging patients to ask their GP if they are PIP Indigenous Health Incentive registered. The community site visits further provided examples of IHPOs, along with ATSIOWs: conducting visits to pharmacies to explain the initiative and its importance; providing education to pharmacists at network meetings (as well as to GPs
and other general practice staff with the aim of ‘spreading the word’); distributing relevant information resources to pharmacists in the local area;
and brokering arrangements between pharmacists and local GPs, identifying
the pharmacist or pharmacy as ‘safe’ for GPs to refer CtG patients to.123
Further, some Divisions of General Practice reportedly directly promoted the measure amongst their members, such as through newsletters or mail-outs. The evaluation has not measured the extent of such local endeavours for 2010-11; however, both community members and the IHPOs themselves reported that these activities were successful in boosting pharmacists’ awareness of the measure, and willingness to provide CtG script medications to Aboriginal and Torres Strait Islander patients. These ad-hoc national and local promotional activities may have responded to the initial lack of awareness about the measure amongst some pharmacists (discussed previously in this chapter). Pharmacists consulted during the 2010-11 site visits generally expressed that sufficient information about the PBS Co-payment measure was not available to pharmacies prior to implementation.
123 This has reportedly been in response to patients being turned away by pharmacists not understanding the measure, and resulting impacts of shame and reluctance to access medicines using CtG scripts in the future – as noted previously.
105KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
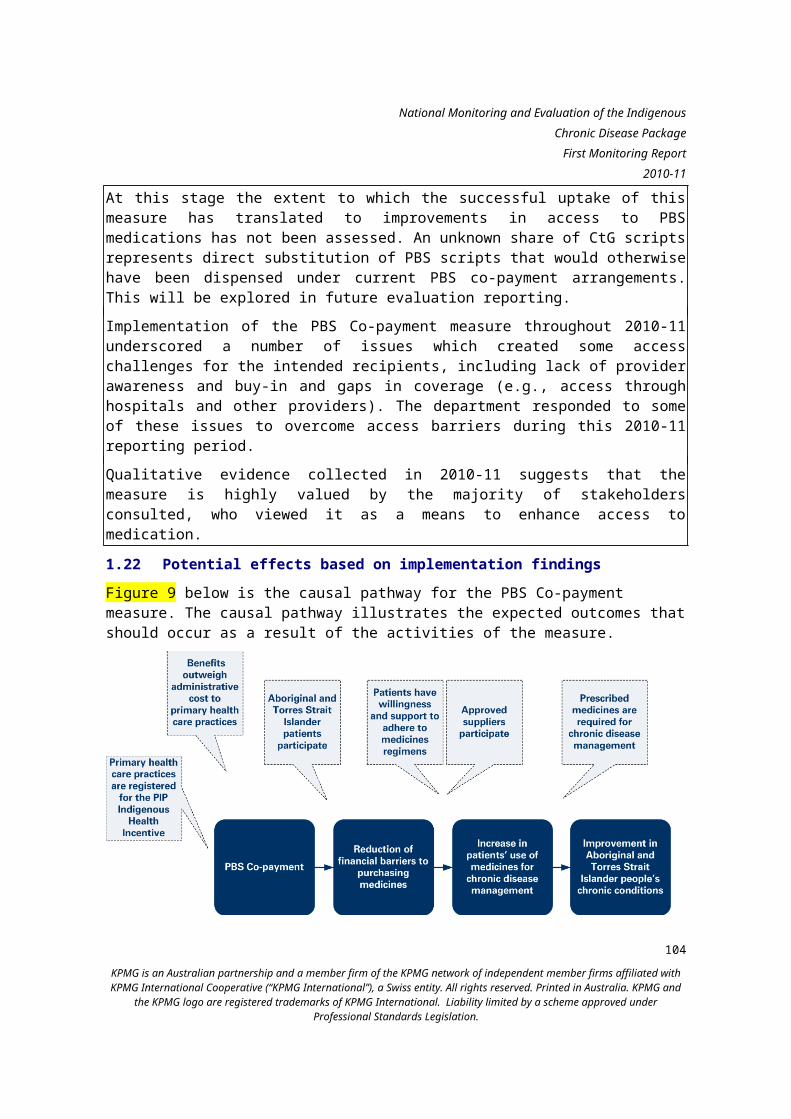
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Many of the national stakeholders engaged in promotional activities had previously been engaged in the PBS Co-payment Technical Reference Group, which was involved in the implementation arrangements for the measure from May 2009 to May 2010. Feedback from national pharmacy stakeholders indicates a missed opportunity in involving the Technical Reference Group in resolving ongoing implementation issues. These stakeholders expressed frustration at not having a vehicle for ongoing dialogue regarding the measure with the department.Finally, pharmacy stakeholders also noted that pharmacists may not have sufficient cultural awareness to provide advice to Aboriginal and Torres Strait Islander clients on issues related to medication use and compliance in a culturally sensitive manner. This may be an area in which further promotion, education and/or support is needed for pharmacists. Note, due to legislated privacy restrictions, the department is not able to provide the public or health care services with a list of PIP Indigenous Health Incentive-registered practices. Stakeholders reported that this constrained their capacity to promote the PBS Co-payment measure to the Aboriginal and Torres Strait Islander population.PBS Co-payment hotline
Beginning in June 2010, the department established a hotline that can be accessed by the general public, prescribers and pharmacies to respond to enquiries about the PBS Co-payment measure. The hotline provides verbal information and additional documentation can be emailed if requested. The department reported that the hotline was well received, particularly by members of the public.Table 26 below provides a count of hotline enquiries received for the fiscal year. Due to database issues experienced by the department, the type of caller or enquiry was not accurately recorded for the hotline. It is not possible, therefore, to report on the extent to which the hotline has been used by the general public (i.e., Aboriginal and Torres Strait Islander people) to gain information about the PBS Co-payment measure. Table 26: Number of hotline enquiries, 2010-11, by intake type. Source: Department of Health and Ageing.
Intake type Number of Hotline enquiries
Phone 4,685Email 1,558Total 6,243
106KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.27 Facilitators and barriersThe number of Aboriginal and Torres Strait Islander people who were dispensed a CtG script and the number of CtG scripts significantly exceeding the department’s expectations. There were still a number of barriers for the PBS Co-payment measure, many of which relate to the issues experienced with implementation, and the linkages with the PIP Indigenous Health Incentive (B3a) measure. It is important to note however, that the department has responded to many of these barriers to date as discussed below: Reliance on PIP Indigenous Health Incentive (B3a) measure. This issue
relates to access to an eligible prescriber/practice. Mainstream practices must be PIP Indigenous Health Incentive registered to provide CtG annotated scripts. IHSs that are PIP Indigenous Health Incentive registered are also eligible to prescribe CtG annotated scripts. When the PBS Co-payment measure was implemented, ‘special arrangements’ were put in place that allowed for participation by non-PIP Indigenous Health Incentive registered IHSs that met certain criteria, including being providers of MBS services and being outside remote and very remote areas.124 Additionally, medical specialists in any location can provide CtG annotated scripts to any eligible patients referred by an eligible prescriber at a registered location.However, CtG scripts are not currently available to some prescribers including hospitals and after hours services (who are not eligible for PIP Indigenous Health Incentive). Thus for example, a GP who works in a PIP Indigenous Health Incentive practice during normal hours could issue a CtG script but the same provider cannot do so when working in an after hours service or working for another health service not registered. Stakeholders reported examples of patients registered with one practice but attending a second practice that is not PIP Indigenous Health Incentive registered and thus not having access to CtG scripts. This could arise for example when a patient in a rural town is registered with a local provider (IHS or GP) and then travels to another location for a period of time (e.g., for sorry business) and the practice they are familiar with in this other location is not PIP Indigenous Health Incentive registered. Another example provided by community members at focus groups is patients who usually visit IHSs, using another local GP (not registered for PIP Indigenous Health Incentive) to avoid the IHS’s waiting list (which can be up to four hours in some locations), and not being able to access CtG scripts. As discussed previously, there is inconsistency in the patient eligibility criteria between the PBS Co-payment (B1) and PIP Indigenous Health Incentive (B3a) measures; the former includes some patients not eligible for the latter. It is possible that as a result of the differing patient eligibility
124 Department of Health and Ageing n.d., Special arrangements for Indigenous Health Services not currently participating in the Practice Incentives Program (PIP).
107KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
between these two measures, “some GPs may decide not to take the time and effort to complete the registration forms”125 for patients who are at risk of a chronic disease or who are under 15 years of age (i.e., those patients that are not otherwise eligible for the PIP Indigenous Health Incentive).
Provider awareness and participation. As noted previously in this chapter there was reportedly an initial lack of awareness amongst pharmacists about the measure which placed patients in the position of self-advocacy when presenting CtG scripts. National stakeholders and service providers reported that patients may be ill equipped to advocate on their own behalf when presenting a CtG script at a pharmacy where staff are unaware of the PBS Co-payment measure. Such situations may cause severe embarrassment to Aboriginal and Torres Strait Islander clients, for example, if they are asked to pay for the medication when they do not have sufficient funds to do so.
Identifying PIP Indigenous Health Incentive registered practices. Restrictions that limit the information that can be published about private businesses have not allowed the department to advertise which primary health care practices are registered to participate in the PBS Co-payment measure (i.e., either through PIP Indigenous Health Incentive or by special arrangement). As a limited remedy, the department’s hotline can respond to individual enquiries regarding local access. Given this restriction, promotional activities have been largely restricted to providers and conducted locally. Partly as a result of this, the PBS Co-payment is limited in the extent to which it can be driven by patient demand. The department is currently seeking permission from General Practices to release information that identifies them as a PIP Indigenous Health Incentive registered practice and is assessing options for the release of this information (e.g., on the web or only through the hotline). At one Regional Forum, participants suggested a role for Divisions / Medicare Locals to obtain consent from local practices to release this information locally.
Patient self-identification. One-time registration is required for a patient’s participation in the PBS Co-payment measure. The department has opted for self-identification (without the need for documentation), as recognition of status as an Aboriginal or Torres Strait Islander person varies from community to community. There are reports from Regional Forums and community site visits to suggest that some patients are self-identifying as an Aboriginal or Torres Strait Islander person, but are not known to the community as such. However at this stage, the small number of
125 Department of Health and Ageing n.d., Special arrangements for Indigenous Health Services not currently participating in the Practice Incentives Program (PIP).
108KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
consultations in which this was raised did not allow the prevalence of this issue to be identified.
Inclusion of non-chronic disease PBS medications. The PBS Co-payment measure is not limited to medications for chronic conditions, and registered patients may receive subsidised medication for treatment of other medical conditions (e.g., acute conditions). The volume of prescribing activity of medicines not directly related to the three chronic conditions of cardiovascular and respiratory disease and diabetes represents 44-54 per cent of all dispensed scripts in the 12 months to 31 May 2011 (see Appendix F for details). As noted above there are a number of reasons why there is extensive prescribing outside of these three conditions including: one risk factor alone is an eligibility criterion for CtG registration; there are chronic diseases other than these three including arthritis and mental health conditions; and people with chronic conditions have acute comorbidities.
Electronic processing. Software upgrades developed through the PBS Co-payment measure have supported electronic processing of scripts with the CtG annotation. Hand-marked scripts are also accepted for pharmacist processing. This flexibility has likely to have enabled greater prescriber participation than would have been achieved through the electronic option alone. However, as noted throughout this chapter, this has also led to some challenges associated with human error (i.e., GPs forgetting to annotate the scripts).
1.28 OpportunitiesThe significant early uptake of the PBS Co-payment measure indicates strong interest in and need for the measure, and the possibility to achieve even greater utilisation for the Aboriginal and Torres Strait Islander population. The early stages of implementation have identified several areas that the department may consider in order to provide the intended recipients with greater access to the PBS Co-payment measure, and continue to build positive outcomes: Further engagement of pharmacists to support improved implementation
and outcomes. The further engagement of pharmacists lends the opportunity to strengthen the implementation and outcomes of the measure. At a national level, the reinstatement of the Technical Reference Group may allow for an ongoing channel of communication between the department and pharmacy peak bodies, who are interested in this opportunity for involvement. At a local level, engagement of pharmacists could be enhanced through further communications from the department (including increased distribution of Pharmacy Staff Resource Booklets), as well as ongoing communications through professional associations.
109KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Engagement of pharmacists to improve correct utilisation of medications. Improved medicine compliance could be supported through pharmacist training of ICDP staff with regular interactions with patients, such as ATSIOWs and Care Coordinators. This pharmacist role would be similar to working with AHWs on the Quality Use of Medicines. Some stakeholders have suggested that home medication review should be included as an additional component of the measure, which would be provided by appropriately qualified pharmacists. In order to improve interactions with Aboriginal and Torres Strait Islander clients, it has been suggested that pharmacists could benefit from cultural awareness training. Ideally, the PBS Co-payment measure allows the interaction between pharmacists and Aboriginal and Torres Strait Islander clients to shift from concern with payment to discussion about use of medication.
Further engagement of GPs. As noted for pharmacists, the department’s engagement of GP practices could be improved with explicit, targeted and ongoing information dissemination about the measure, such as which medications are included.
Taking patient mobility into consideration: The department could consider alterations to the measure design that would better account for patient mobility, in particular in the case where the patient loses access to either S100 RAAHS or their PIP Indigenous Health Initiative registered general practice.
The department could consider arrangements where the eligibility for the PBS Co-payment ‘resides’ with the patient rather than the location or prescriber. For instance, the CtG annotation could be automated for eligible/registered patients, or pharmacists could play a role in deeming eligibility. Such revisions to the measure may also override the confusion created by inconsistent eligibility and registration requirements of the PBS Co-payment measure and PIP Indigenous Health Initiative. This suggestion was supported by the pharmacists engaged through the community site visits.
110KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Higher utilisation costs for MBS and PBS (B2)This chapter provides an overview of the higher utilisation costs for MBS and PBS measure. In this chapter, we discuss findings against activities, outputs and expected results as described in the Evaluation Framework. Higher utilisation costs for MBS and PBS at a glanceThe utilisation of selected MBS and PBS items across Australia increased significantly between 2009-10 and 2010-11. Largely, this increase was consistent across geographical areas. The exception to this was the low utilisation of Practice Nurse (PN) and Aboriginal Health Worker (AHW) follow up items in most jurisdictions apart from Victoria, New South Wales and Queensland. In terms of uptake of Health Assessments (MBS Item 715), there was also some variation across population groups, namely, age with a higher utilisation of Health Assessments amongst older people (aged 15-55 and 55+) than younger people (aged 0-14), and gender with a higher utilisation of Health Assessments amongst females. The increase in utilisation of selected MBS and PBS items must be interpreted with due consideration of the data limitations and contextual factors, which are described in this chapter. 1.29 Measure overviewThe Higher utilisation costs for MBS and PBS measure provides increased funding to the MBS and PBS to meet expected higher utilisation costs by Aboriginal and Torres Strait Islander people accessing complementary programs under the ICDP. Unlike other measures, this measure is not a direct service strategy, but a budget provision in anticipation that other measures will increase use of MBS and PBS. The overall aim of the evaluation of this measure is to estimate the impact of the ICDP on MBS and PBS utilisation. 1.30 Utilisation of MBS itemsThis section presents data on utilisation of selected MBS items which target Aboriginal and Torres Strait Islander patients including Aboriginal and Torres Strait Islander Health Assessments, allied health provider items and PN/AHW follow up items. MBS Aboriginal and Torres Strait Islander Health Assessment (Item 715)
MBS Item 715, Aboriginal Health Assessment, is available to all people of Aboriginal and Torres Strait Islander descent. Prior to 1 May 2010, Items 704, 706, 708 and 710 were used for Aboriginal and Torres Strait Islander Health Assessments. These items were rolled into the single Item 715 on 1 May 2010. The Health Assessment is an annual service. The minimum time allowed
111KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
between services is nine months. This allows flexibility for very remote communities, where medical practitioner visits may be less frequent and may make it more difficult to follow a consistent schedule of Health Assessments.126
An upward trend in the number of Health Assessments has been seen since 2009, since the introduction of the single Item 715. The general trend in the number of Health Assessments by quarter for August 2008 to May 2011 is shown in Figure 10, below. As shown in Figure 10, the number of Health Assessments grew from 10,833 in the May quarter 2009 to 13,378 in the May quarter 2010, an increase of 23 per cent. Across 2010-11, this upward trend continued. In May 2011, there were 20,599 Health Assessments, an increase of 53 per cent from the corresponding quarter in 2010 (and almost double the number of Health Assessments in May 2009).
0
5,000
10,000
15,000
20,000
25,000
Healt
h ass
essm
ents Items 704,706, 708, 710 Item 715
Figure 10: Aboriginal and Torres Strait Islander health assessments August 2008 to May 2011.127
Note, the time series displays seasonal effects (e.g., drop in services between November to February quarters due to shut downs and reductions in service hours over the holiday period).
One question presented by the rollup of Health Assessment items into the single Item 715 is whether this increase in the number of Health Assessments since 2010 is a consequence of reducing the administration involved through 126 Department of Health and Ageing n.d., Medicare Benefits Schedule (MBS) Health Assessment for Aboriginal and Torres Strait Islander People (MBS Item 715) Fact Sheet.127 Based on MBS data, provided by the Department of Health and Ageing.
112KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
combining these Health Assessment items, or as a result of the ICDP which was implemented just prior to this (or a combination of both). This will be explored in the contribution analysis, which will utilise data from the 2011-12 financial year.Figure 11 below shows the number of Health Assessments by jurisdiction by quarter from August 2008 to May 2011. As this figure shows, growth in Health Assessments across jurisdictions was generally consistent, with the four jurisdictions with the largest Aboriginal and Torres Strait Islander populations (NSW, Qld, WA and NT) performing at least 30 per cent more health assessments in the May 2011 quarter compared to the May 2010 quarter. Queensland had the highest number of Health Assessments despite having the second largest Aboriginal and Torres Strait Islander population.
01,0002,0003,0004,0005,0006,0007,0008,000
Healt
hass
essm
ents
NSW QLD WA NT VIC SA TAS ACT
Figure 11: Aboriginal and Torres Strait Islander health assessments August 2008 to May 2011 by state/territory.128 129
In 2010-11, there was also growth in Health Assessments across all remoteness areas: major cities; inner regional; outer regional; and very remote Australia. However, inner and outer regional areas had a greater percentage increase in the number of Health Assessments (180 per cent and 179 per cent, respectively) than major cities and very remote Australia (149 and 118 per cent, respectively), as Figure 12 below shows.
128 Based on MBS data provided by the Department of Health and Ageing.129 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
113KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
01,0002,0003,0004,0005,0006,0007,000
Heal
th a
sses
smen
ts
Major Cities of Australia Inner Regional AustraliaOuter Regional Australia Remote AustraliaVery Remote Australia
Figure 12: Aboriginal and Torres Strait Islander health assessments August 2008 quarter to May 2011 quarter by remoteness area.130 In 2010-11 there was a greater increase in the number of Health Assessments amongst older age groups (15-44 and 55+) compared to younger age groups (0-14). There was also a greater increase in Health Assessments amongst females. This higher number of Health Assessments for females has always been the case. However interestingly, since the introduction of Item 715 the gap appears to have increased, particularly for some age groups (e.g., 15-55). The unique number of providers of Health Assessments also increased over 2010-11 by 44.8 per cent. Appendix G provides a more detailed discussion and data relevant to these variables.Patient Flow through MBS ItemsFor Aboriginal and Torres Strait Islander people with a chronic disease who have a Health Assessment, there are a number of follow on items which can be accessed. These are listed in HWs and allied health services. below. Thus, Health Assessments act as a gateway item to follow up services from PNs/AHWs and allied health services.
130 Based on MBS data provided by the Department of Health and Ageing.114
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 27: MBS follow up items for which detailed data is available and short description. Source: Medicare Benefits Schedule.
Item Number
Short description
10987 Follow up from PN or AHW81300 Aboriginal and Torres Strait Islander Health Service81305 Diabetes education health service81310 Audiology health service81315 Exercise physiology health service81320 Dietetics health service81325 Mental health service81330 Occupational therapy service81335 Physiotherapy health service81340 Podiatry health service81345 Chiropractic health service81350 Osteopathy health service81355 Psychology health service81360 Speech pathology health service
Analysis of the available data shows that follow up services from a PN/AHW grew substantially over the last two years. As Figure 13 below shows, there were four times as many of these services in the May quarter 2010 (1,483 services) compared to the May quarter 2009 (345 services). In the May quarter 2011 (4,293 services), there were almost three times as many services provided than in the May 2010 quarter.
115KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
10,83313,378
20,599
3451,483
4,293
189 5751,353
0
1,000
2,000
3,000
4,000
5,000
0
5,000
10,000
15,000
20,000
25,000Au
g-08
Nov-0
8Fe
b-09
May
-09Au
g-09
Nov-0
9Fe
b-10
May
-10Au
g-10
Nov-1
0Fe
b-11
May
-11
Followup services / allied health
services
Healt
h ass
essm
ents
Health assessments Services from PNs/AHWsAllied health services
Figure 13: Health assessments, services from PNs/AHWs and allied health services for August 2008 quarter to May 2011 quarter.131
As Figure 13 shows, in the May 2011 quarter there were 1,353 allied health services across all service types (e.g., physiotherapy, podiatry). As at May 2011, the volume of allied health services was much lower than that of health assessments or follow up services.For some of the allied health items, there were very few services at the national level. For example, the only allied health services that accounted for more than 1,000 services since November 2008 were Aboriginal and Torres Strait Islander Health Service, Physiotherapy health service and Podiatry health service, as Table 28 below shows.In contrast, there were only 49 osteopathy health services provided between August 2010 and May 2011. Unlike the other allied health items, which generally started flowing through in February 2009, the first osteopathy service was provided in the August 2010 quarter. Other services, such as audiology health service, were not provided at all in the May and February quarters of 2011.
131 Based on MBS data, provided by the Department of Health and Ageing.116
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 28: Total services and May 2011 service and provider statistics at the national level.132
Service Total Services since Nov 2008
Services May 2011
Providers May 2011
Average services per provider May 2011
Aboriginal and Torres Strait Islander Health Service
1,430 372 20 18.6
Diabetes education health service 355 126 13 9.7Audiology health service 16 NR* NR* NR*Exercise physiology health service 262 27 11 2.5Dietetics health service 583 145 19 7.6Mental health service 22 NR* NR* NR*Occupational therapy service 58 NR* NR* NR*Physiotherapy health service 1,192 221 53 4.2Podiatry health service 1,443 322 34 9.5Chiropractic health service 87 20 9 2.2Osteopathy health service 49 NR* NR* NR*Psychology health service 78 16 6 2.7Speech pathology health service 462 91 17 5.4
* For confidentiality reasons, this number is not reported.
While the volume of allied health services was lower than Health Assessments and PN/AHW follow up items, the trend in uptake of these services was rather similar to that of follow up services from a PN/AHW, with more than twice as many allied health services provided in the May 2011 quarter (1,353 services) as there were in the May 2010 quarter (575 services). The low volumes of allied health services do not warrant investigating the distribution by remoteness or state. However for the Aboriginal and Torres Strait Islander Health Service, Physiotherapy health service and Podiatry health service, there were some interesting differences by geography, particularly by jurisdiction.
132 Based on MBS data provided by the Department of Health and Ageing.117
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
For Aboriginal and Torres Strait Islander Health Service, over 98 per cent of services were provided in New South Wales, Victoria and Queensland. Victoria had the highest number of services of all jurisdictions. Essentially, there were no Aboriginal and Torres Strait Islander health services provided by a PN/AHW in all other jurisdictions – this is rather interesting for Western Australia and the Northern Territory considering the size of their Aboriginal and Torres Strait Islander populations. Table 29: Aboriginal and Torres Strait Islander health services by jurisdiction.133 134
State/territory Aboriginal and Torres Strait Islander Health Service
NSW 281VIC 616QLD 505SA/WA/TAS/NT/ACT 28Total 1,430
Note, for physiotherapy health services, the distribution was more broadly reflective of the Aboriginal and Torres Strait Islander population distribution as Table 30 below shows. Table 30: Physiotherapy health services by jurisdiction.135 136
State/territory Physiotherapy health serviceNSW 495VIC 32QLD 299SA 45WA 186NT 93TAS/ACT 42Total 1,192
133 Based on MBS data, provided by the Department of Health and Ageing.134 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.135 Based on MBS data, provided by the Department of Health and Ageing.136 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
118KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
119KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 31: Podiatry health services by jurisdiction.137 138
State/territory Podiatry health serviceNSW 262QLD 384WA 578NT 207VIC/SA/TAS/ACT 12Total 1,443
Data limitations - MBS
It is not possible at this stage to estimate the proportion of change in MBS use that can be attributed to the ICDP. This is because incremental analysis to distinguish the effects of the ICDP specifically on utilisation of the selected MBS items could not be undertaken using the data available for 2010-11. Further, due to the ongoing upward trend in utilisation of the selected MBS items over time, it is likely that some of the increase in uptake of selected MBS items would have occurred in the absence of the ICDP.Incremental analysis to distinguish the effects of the ICDP specifically on utilisation of the selected MBS items will inform the development of the Final Evaluation Report in 2013.1.31 Utilisation of PBSDetailed analysis of the utilisation of the PBS by Aboriginal and Torres Strait Islander people, and specifically utilisation of CtG scripts, is discussed in chapter .In summary, across jurisdictions, a steady rise in utilisation of CtG scripts was observed which was broadly consistent with overall trends in CtG script utilisation for Australia as a whole, and in line with the Aboriginal and Torres Strait Islander population numbers across states and territories (i.e., jurisdictions with higher Aboriginal and Torres Strait Islander populations saw higher numbers of CtG scripts dispensed). The exception to this was the Northern Territory, which had comparatively lower numbers of CtG scripts dispensed, although this was expected due to the high use of S100 RAAHS in that jurisdiction.
137 Based on MBS data, provided by the Department of Health and Ageing.138 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
120KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Some growth in PBS scripts for Aboriginal and Torres Strait Islander people would be expected as a consequence of the growth in attendance at primary health services, implied by the increased MBS items, discussed in the previous section. Figure 14 below shows the per capita utilisation of the selected MBS items and CtG scripts for Australia. This figure shows that there was a larger increase in utilisation of CtG scripts compared to the selected MBS items over the period August quarter 2009 to May quarter 2011. As this figure shows, CtG scripts became available from July 2010 and utilisation has grown significantly since this time.
010203040506070
0
1
2
3
4
5
CtG items per capita per quarterM
BS ite
ms p
er ca
pita p
er qu
arter
MBS items per 100 capita per quarterCtG items per 100 capita per quarter
Figure 14: Per 100 capita utilisation by quarter - Australia: Selected MBS items; and CtG items.139
Data limitations - PBS
It is not possible at this stage to estimate the proportion of CtG scripts that represents additional dispensing of PBS items compared to what would otherwise have occurred. Additionally, the number of CtG scripts dispensed underestimates the total utilisation of PBS items dispensed by community pharmacies to Aboriginal and Torres Strait Islander people. Non-CtG annotated scripts, including those prescribed for chronic disease management, will continue to be dispensed to Aboriginal and Torres Strait Islander people, for a range of reasons. These limitations are discussed in more detail in chapter .
139 Based on MBS and PBS data provided by the Department of Health and Ageing.121
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Appendix G provides a series of tables and figures which support further insight into MBS and PBS utilisation.
122KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Supporting Primary Care Providers to Coordinate Chronic Disease Management (B3a)This chapter describes the progress of the Supporting Primary Care Providers to Coordinate Chronic Disease Management (hereafter referred to as the Practice Incentives Program (PIP) Indigenous Health Incentive measure). In this chapter we discuss findings against activities, outputs and expected results identified within the Evaluation Framework, and barriers, facilitators and opportunities identified to date. PIP Indigenous Health Incentive measure at a glancePayments under the PIP Indigenous Health Incentive commenced in May 2010, and the 2010-11 year saw the widespread implementation of the incentive arrangements. From the commencement of the initiative to May 2011, 2,128 practices signed up for PIP Indigenous Health Incentive, 133 of which were IHSs In 2010 there were 31,646 patient registrations. In 2011, to May 31 there were 15,308 patient registrations, of which 5,517 were re-registrations from 2010. In 2010, seven out of ten registered patients triggered an outcome payment, with the majority of patients triggering Tier 2 outcome payments only.Key findings about the PIP Indigenous Health Incentive measure in 2010-2011: The rapid uptake of the PIP Indigenous Health Incentive has exceeded
expectations in terms of expenditure. The actual expenditure on the measure was $16.7 million with payments for: practice registration (12 per cent), patient registration (67 per cent) and Tier 1 (1 per cent) and Tier 2 (20 per cent) outcome payments. The main driver of the higher than expected expenditure is the higher than expected patient registration per practice; 8,738 patients were expected to benefit from PIP Indigenous Health Incentive in 2009-10 and 2010-2011 combined.
Approximately one out of ten patients triggered a Tier 1 payment in addition to a Tier 2 payment. Consultations identified reasons for the low level of Tier 1 payments including: the perceived or real difficulty undertaking the care required to trigger a Tier 1 payment; and a view that the administrative burden associated with the PIP Indigenous Health Incentive is significant, particularly for smaller practices that tend to have minimal administrative capacity.
Potential effects based on implementation findingsFigure 15 below is the causal pathway for the PIP Indigenous Health Incentive measure. The causal
123KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
PIP Indigenous Health Incentive
Increase in primary health care
providers’ cultural awareness
Increase in better practice care for chronic disease management
Provider motivatio
n to change
Increase in primary health care providers’
willingness to provide better practice care to Aboriginal and Torres Strait
Islander patients
Improved identification of Aboriginal and Torres Strait
Islander patients who require
enhanced chronic disease care and
management
Improvement in Aboriginal and Torres Strait
Islander people’s chronic conditions
Increase in primary health care providers'
knowledge, understanding and
skills
Primary health care practices are registered
for the PIP Indigenous
Health Incentive
Incentive payments and other benefits outweigh the administrative
costs to primary health care practices
Cultural awareness training is
appropriate and effective
Aboriginal and Torres Strait
Islander patients
participate
Figure 15: PIP Indigenous Health causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect140 and the observed impacts.141 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below.
140 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.141 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
124KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 32 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There were no significant changes to the design of the measure; therefore the plausibility of effect remains unchanged. The PIP Indigenous Health Incentive has been fully implemented, and there has been significant uptake from IHSs. All of the key dependencies are present to some extent but scope exists to scale these up in terms of practices and patients registered, and to improve the appropriateness of cultural awareness training. Table 32: Assessment of the key dependencies of the B3a measure.
Key dependencies
Finding Evidence
Primary health care practices are registered for the PIP Indigenous Health Incentive
Practices are registered, but there is scope to increase practice participation. As at May 2011, 56 per cent of all Indigenous health services had registered for the PIP Indigenous Health Incentive, which is almost double the rate of mainstream general practices (28 per cent). However, there are many more mainstream general practices than IHSs eligible for registration.
Empirical evidence from analysis of Medicare data
Incentive payments and other benefits outweigh the administrative costs to primary health care practices
The incentives generally outweigh the costs for the majority of participating practices. There are some indications that the administrative burden may be an issue for smaller practices.
Qualitative information gathered from a small group of relevant stakeholders.
Cultural awareness training is appropriate and effective
There are emerging indications that the online format and minimum number of staff required to complete cultural awareness training are reducing its appropriateness. At this stage, the evaluation cannot assess the effectiveness of cultural awareness training.
Qualitative information gathered from a small group of relevant stakeholders
125KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Finding Evidence
Aboriginal and Torres Strait Islander patients participate
Eligible Aboriginal and Torres Strait Islander patients are participating, but potential remains to expand the patient base, as just over one-quarter of Aboriginal and Torres Strait Islander people with one or more chronic diseases are registered.
Empirical evidence from analysis of Medicare data
Contextual considerations
The uptake of the PIP Indigenous Health Incentive may be limited in IHSs due to variable organisational capacity, which may impact on the capacity to satisfy practice registrations requirements and ongoing requirements for consistent and structured contact with patients.142
Literature review.
Table 33 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). For most of the expected impacts – which relate to provider knowledge, skills and willingness to provide better practice care – there is not yet clear evidence of changes to provider behaviour in relation to increasing proactive management of chronic disease. There are signs of improved awareness and identification of Aboriginal and Torres Strait Islander patients, and of increased activities associated with better practice care. Contextual factors which appear to be impacting on the measure are sector and remoteness. It is apparent that IHSs and mainstream general practices are implementing PIP Indigenous Health Incentive differently, and this may lead to the measure having different impacts in the two sectors. Remoteness influences patient and practice participation.
142 Couzos S & Thiele DD 2010, The new “Indigenous health” incentive payment: issues and challenges’, Medical Journal of Australia, vol. 192, no. 3, p. 156; Urbis Keys Young 2006, Aboriginal and Torres Strait Islander Access to Major Health Programs, Urbis JHD Group, Sydney.
126KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 33: Assessment of the expected and observed impacts of the B3a measure based on implementation progress.
Expected impacts
Observed impacts Evidence
Increase in primary health care providers’ cultural awareness
There is no data available on the impact of training on providers’ cultural awareness at this stage.
Not applicable
Increase in primary health care providers’ knowledge, understanding and skills
At this stage, the evaluation is not able to measure change in the knowledge or skills of providers. There is an indication that registered providers in mainstream general practices have better awareness of who their Aboriginal and Torres Strait Islander patients are; and IHSs have access to additional resources to support chronic disease care.
Qualitative information gathered from a small group of relevant stakeholders
Increase in primary health care providers’ willingness to provide better practice care to Aboriginal and Torres Strait Islander patients
At this stage, the evaluation is not able to measure change in the willingness of providers. The vast majority of outcomes payments were for providing the majority of a patient’s care rather than for specific chronic disease management. However, there is evidence that activities associated with good practice care have increased.
Empirical evidence from analysis of Medicare data; and emerging evidence drawing on qualitative information gathered from a small group of relevant stakeholders, and a case study
Improved identification of Aboriginal and Torres Strait Islander patients who require enhanced chronic disease care and management
The PIP Indigenous Health Incentive together with the C2 / C3 workforce (ATSIOWs and IHPOs) are improving the identification of Aboriginal and Torres Strait Islander patients, primarily within mainstream practices.
Emerging evidence; drawing from qualitative information gathered from a small group of relevant stakeholders
127KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected impacts
Observed impacts Evidence
Increase in better practice care for chronic disease management
At this stage, the evaluation is not able to measure change in the practice care for chronic disease management. However, there is evidence that activities associated with good practice care (health checks and allied health services) have increased.
Empirical evidence from analysis of Medicare data
Improvement in Aboriginal and Torres Strait Islander people’s chronic conditions
Data is not available for the First Monitoring Report.
Not applicable
Contextual considerations
The evaluation found that often, the PIP Indigenous Health Incentive is being implemented differently in mainstream practices compared to IHSs. Largely this is based on existing organisational capacity / readiness. For example in some cases IHSs already have the systems in place to support PIP Indigenous Health Incentive such as those for collecting Aboriginal and Torres Strait Islander status, but do not have well utilised practice management systems. This may have implications for the impact on the organisation, and the impact of the measure overall.Remoteness is cited in this report as one of the factors influencing both patient participation as well as practice participation.
Qualitative information gathered from a small group of relevant stakeholders
1.32 Measure overview The PIP Indigenous Health Incentive is aimed at supporting general practices and Indigenous Health Services (IHSs) to provide better health care for Aboriginal and Torres Strait Islander patients, including best practice management of chronic disease.
128KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The PIP Indigenous Health Incentive has three components: Sign-on Payment ($1,000 per practice): A one-off payment to practices that
agree to undertake specified activities to improve the provision of care to their Aboriginal and Torres Strait Islander patients with a chronic disease.
Patient Registration Payment ($250 per eligible patient per calendar year): A payment to practices for each Aboriginal and Torres Strait Islander patient aged 15 years and over, registered with the practice for chronic disease management.
Outcomes payments (total up to $250):- Tier 1 ($100 per eligible patient per calendar year): A payment to
practices for each registered patient for whom a targeted level of care is provided by the practice in a calendar year; and
- Tier 2 ($150 per eligible patient per calendar year): A payment to practices for providing the majority of care for a registered patient in a calendar year.
In 2010-11 actual expenditure on the PIP Indigenous Health Incentive measure was $16.7 million, significantly higher than allocated. This additional expenditure was driven by a higher than projected number of patients registered per participating practice. Originally 8,738 patients143 were expected to benefit from PIP Indigenous Health Incentive in 2009-10 and 2010-11 combined. However, 31,646 patients were registered in the 2010 calendar year and a further 9,791 new patients had been registered in the February 2011 and May 2011 quarters144 (refer Appendix H for further details). 1.33 Indigenous Health Incentive payments Practice sign-on
To sign-on for the PIP Indigenous Health Incentive, practices are required to meet the eligibility requirements of the Practice Incentives Program (PIP), and: agree to obtain consent to register their eligible Aboriginal and Torres
Strait Islander patients for the PIP Indigenous Health Incentive and/or the PBS Co-payment measure with the Department of Human Services;
establish and use a mechanism to ensure their Aboriginal and Torres Strait Islander patients aged 15 years and over with a chronic disease are followed up;
undertake cultural awareness training; and
143 Email to KPMG from the Department of Health and Ageing 2011, Data for Baseline Report Input from Measure Managers, sent on 2 September 2011.144 PIP data, provided by the Department of Health and Ageing 2011
129KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
annotate PBS prescriptions for Aboriginal and Torres Strait Islander patients participating in the PBS Co-payment measure.
The number of practices registering for PIP Indigenous Health Incentive peaked in May 2010 for both IHSs and general practices. This was the quarter in which practices commenced registering after the Department of Human Services wrote to practices in March 2010 and invited them to join the PIP Indigenous Health Incentive.Table 34: Practice registrations by Medicare quarter and practice type.145
Medicare Quarter
IHS General Practice
Total
May-10 86 767 853Aug-10 24 448 472Nov-10 14 325 339Feb-11 8 228 236May-11 1 227 228Total 133 1,995 2,128
IHPOs interviewed to date reported that practices more likely to embrace sign-on were those that had already clearly identified their cohort of Aboriginal and Torres Strait Islander patients. These practices see a clear link between care they are already providing and the PIP Indigenous Health Incentive requirements. In these instances, the PIP Indigenous Health Incentive is providing guidance, support and (cultural awareness) training, which is highly valued by practices. IHPOs also reported that some practices in their areas have no interest in the PIP Indigenous Health Incentive and once initial information has been provided they are considered to be ‘no go’ practices for follow up. IHPOs have suggested a range of reasons for this including that some practices: genuinely have no Aboriginal and Torres Strait Islander patients and are
unlikely to attract any, perhaps because of their location or the out of pocket fees charged;
do not believe that they have Aboriginal and Torres Strait Islander patients – even though this is sometimes not the case according to IHPOs (this issue was particularly raised in locations where Aboriginal and Torres Strait Islander people may not be easily identified by their appearance); and
some practices do not wish to attract Aboriginal and Torres Strait Islander patients.
145 PIP data, provided by the Department of Health and Ageing 2011130
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Patients registrations
Patient registration payments are annual payments of $250 to practices for each eligible patient that they register for the PIP Indigenous Health Incentive. Patient re-registration is required on an annual basis. The registration and re-registration process involves completion and lodgement of a patient registration and patient consent form, and requires that the patient provides informed consent. During the 2010-11 year, a revised patient consent process was developed, with a new requirement to send patient consent forms to Medicare Australia (previously, they were kept by the primary health care provider). Medicare Australia communicated this change to registered practices through the PIP News Update (Feb 2011 and July 2011); the new requirements were implemented as of 1 July 2011. Of the three available breakdowns relating to patient registrations (the breakdowns being jurisdiction, remoteness and practice type) the most interesting aspect is the difference in registrations by practice type, i.e., IHS and general practice. In 2010 an IHS registered, on average, 169 patients while a general practice registered, on average, seven patients. Table 35: Patients and practices registered in 2010 by type of practice.146
Statistic IHS General PracticePractices registered in 2010
124 1,540
Patients registered in 2010
20,966 10,680
Average patients registered per practice147
169 7
One of the most significant changes required of many practices that participate in the PIP Indigenous Health Incentive sign-on is the imperative to improve the accuracy of identification of their Aboriginal and Torres Strait Islander patients. This applies not only to new patients, but in many cases to existing patients. Various examples were cited during evaluation consultations of strategies being used to improve identification of Aboriginal and Torres Strait islander people such as: using new systems that have automatic and hurdle prompts for reception
staff to improve collection; instigating regular file updates of existing patients; and
146 Based on PIP data, provided by the Department of Health and Ageing 2011147 Average patient figures rounded to the nearest whole number
131KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
encouraging multiple points of collection, for example, both reception staff and GPs may have prompts to ask patients about their Aboriginal and Torres Strait Islander status.
Aboriginal and Torres Strait Islander identification is further discussed below.Generally consistent (though not universal) feedback from stakeholders at the national, state and local levels indicates a perception that the administrative requirements associated with the PIP Indigenous Health Incentive are significant, and that this perceived burden impedes more widespread participation in the measure. Stakeholders felt that the impact of the administrative burden may be particularly felt by small primary health care practices located in regional areas and practices with one or a small number of GPs. This is consistent with findings from the Sentinel Sites evaluation, which found that participation of practices is more challenging in remote areas than urban and regional areas. Sentinel Sites stakeholders in remote sites emphasised barriers such as administrative burden related to participation, and shortfalls in workforce capacity. The Sentinel Sites project has also noted that perception of administrative burden is decreasing over time. 148
As an illustration of the extent of the administrative requirements, a large IHS reported that they reinvested a portion of the income generated through the Indigenous Health Incentive into employment of a junior administrative assistant to manage the administrative requirements. The health service regarded the establishment of a new full time job for a young Aboriginal person in their community as a positive outcome, however, this case also illustrates that there can be significant administrative burden associated with participation in the Indigenous Health Incentive. GPs and practice staff in several locations have reported that the administrative burden associated with re-registration is particularly concerning, given that registered patients will continue to have a chronic condition and hence, unless they no longer attend that practice, they will continue to be eligible.
148 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
132KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Outcome payments
A Tier 1 payment of $100 is made to practices that either: prepare a GP Management Plan (GPMP) (MBS item 721) or coordinate the
development of Team Care Arrangements (TCA) for a registered patient in a calendar year; and
undertake at least one review of the GPMP or the TCA (MBS item 732) during the calendar year.
OR undertake two reviews of a patient’s GPMP or TCA (MBS item 732) during
the calendar year.OR contribute to a review of a multidisciplinary care plan for a patient in a
Residential Aged Care Facility (MBS item 731) on two occasions during the calendar year.
Tier 1 outcomes payments are paid in the quarter following the provision of services based on entries against the MBS schedule.A Tier 2 outcomes payment of $150 is made to the practice that provides the majority of eligible MBS services for a registered patient (with a minimum of five eligible MBS services) in a calendar year. Practices are not obliged to provide specified care items in order to receive a Tier 2 payment. Tier 2 outcomes payments are paid annually in February. provides a breakdown of the PIP Indigenous Health Incentive expenditure from May 2010 to May 2011. Of the four PIP Indigenous Health Incentive payment types, the largest uptake has been patient registration payments. The number of payments and total expenditure is outlined in below. Table 36: Expenditure against PIP Indigenous Health Incentive payments May 2010 to May 2011.149
PIP Indigenous Health Incentive statistics from May 2010 to May 2011
Number Payment Expenditure
Total Practices Registered 2,128 $1,000 $2,128,000Total Patients Registered150 49,741 $250 $12,435,250Tier 1 payments 2,046 $100 $204,600
149 PIP Indigenous Health Incentive data, provided by the Department of Health and Ageing 2012.150 Includes patients that have re-registered in 2011.
133KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
PIP Indigenous Health Incentive statistics from May 2010 to May 2011
Number Payment Expenditure
Tier 2 payments 24,796 $150 $3,719,400Total - - $18,487,25
0
In 2010 approximately 70.3 per cent of registered patients triggered a Tier 1 and/or Tier 2 payment, i.e., seven out of ten patients. There was limited variation across jurisdictions in terms of the numbers of registered patients triggering a payment. The lowest proportion was in Victoria, where 63.8 per cent of registered patients triggered a payment. The highest proportion was in Queensland, where 73.0 per cent of registered patients triggered a payment in 2010 (for details see Appendix H) For general practices about one in four registered patients did not trigger a payment, compared to IHSs where this figure was almost one in three registered patients, see below.The available data on Tier 1 and Tier 2 outcome payments indicates that substantially more payments are related to general care (Tier 2), as opposed to the more specific chronic disease management (Tier 1) as evidenced in. below shows only a very small number of patients triggered a Tier 1 payment only, i.e., if a registered patient triggered a Tier 1 payment then they almost certainly triggered a Tier 2 payment as well. In relation to this, feedback from stakeholders indicates that the time requirements associated with the specified chronic disease management tasks are a disincentive.151 In 2010-11the vast majority of outcome payments provided through the PIP Indigenous Health Incentive were for providing the majority of patients’ care (Tier 2) rather than for providing the required MBS chronic disease management items (Tier 1). Based on this observation it initially appears unlikely that there have been significant changes to the delivery of the prescribed MBS chronic disease management items as intended by the PIP Indigenous Health Incentive. However, there is evidence that activities associated with good practice care have increased. It is unclear, at this stage, whether these increases in health checks and allied health services are associated with the ICDP or other complementary Commonwealth, state or territory or local initiatives. Analysis of this data is outlined in chapter . Consultations have also provided examples of PIP Indigenous Health Incentive changing the way that care is being provided to Aboriginal and Torres Strait Islander patients. For example, one GP engaged during the site visits said the
151 These requirements are not ICDP related but the normal requirements of Medicare Australia of the procedures that GPs must follow in order to receive payment for, e.g., care plans.
134KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
PIP Indigenous Health Incentive provides GPs with an incentive to spend more time with patients during a consultation. Other GPs consulted said the PIP Indigenous Health Incentive provides GPs with an ‘excuse’ to ask patients whether they are Aboriginal or Torres Strait Islander. Nurses at one IHS reported that they are now doing many more health checks (in conjunction with GPs) and that these checks provide opportunities for patients to ‘open up to them’ and to establish a good relationships which in turn lead to better ongoing care and engagement in treatment. For example an IHS reported that this has led to a 10 per cent increase in vaccinations that is now at 90 per cent of the target population Half of the practices consulted stated that they are already providing good practice care to patients, and do not see the need for changed practice. Based on activities undertaken to date it seems that this perception is consistent between IHSs and general practices. Some national and state-level stakeholders expressed a view that the PIP Indigenous Health Incentive lacks a mechanism to promote genuine practice change, and relies solely on the assumption that incentive payments will automatically generate the desired service delivery. However, consideration should be given to the combined effect of the PIP Indigenous Health Incentive and workforce elements of ICDP (IHPOs, ATSIOWs and Care Coordinators in particular) to effect change. A number of site based stakeholders pointed out that the primary benefit of the PIP Indigenous Health Incentive is that it encourages general practitioners to identify and engage with Aboriginal and Torres Strait Islander patients. Many stakeholders feel that improving identification and creating an increased awareness in practices that they do provide services to Aboriginal and Torres Strait Islander people is the first step to improving that care.
135KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 37: Numbers of registered patients triggering outcome payments and practice type in 2010.152
Statistic IHS General practice
Total
IHI Registrants - no payment
6,764(32.3%)
2,640(24.7%)
9,404(29.7%)
IHI Registrants - Tier 1 only
19(0.1%)
29(0.3%)
48(0.2%)
IHI Registrants - Tier 2 only
13,352(63.7%)
7,246(67.8%)
20,598(65.1%)
IHI Registrants - Tier 1 & 2
831(4.0%)
765(7.2%)
1,596(5.0%)
Total IHI Registrants 20,966(100.0%)
10,680(100.0%)
31,646(100.0%)
Community promotion, participation and satisfaction
A number of mechanisms have been used to promote PIP Indigenous Health Incentive to eligible community members including direct encouragement from practice staff and community engagement and education activities undertaken by IHPOs and ATSIOWs. In some locations IHPOs and ATSIOWs have also developed and distributed posters and pamphlets explaining the PIP Indigenous Health Incentive. The effectiveness of these communication materials is likely to be highly variable given the localised nature. The evaluation has not thus far uncovered evidence that eligible patients are declining to participate in PIP Indigenous Health Incentive in substantial numbers. Community consultations have provided no real insight into why an eligible person might choose to decline to participate in the PIP Indigenous Health Incentive. The Sentinel Sites evaluation reported that the need for self-identification was identified by community members as a reason not to participate, particularly in regional areas.153
Emerging evidence suggests that the PIP Indigenous Health Incentive is leading to improvements in access to primary health care in some locations. Examples cited by participants in regional forums included patients re-engaging with their local health service provider. Participants did suggest that this is a combination of the efforts of ATSIOWs as well as primary health care providers who are PIP Indigenous Health Incentive registered.152 Based on PIP data, provided by the Department of Health and Ageing, 2012.153 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
136KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The evidence from MBS service data demonstrates that there have been substantial increases in health assessments and related allied health services provided to Aboriginal and Torres Strait Islander patients between May 2009 and May 2011. For detailed tables and charts see chapter . In several community focus groups individuals expressed views that GPs are so busy that they do not have time to talk to their patients or to build trusting relationships. This view suggests that many Aboriginal and Torres Strait Islander people may value the opportunity to engage in more patient focused care such as health assessments and care planning.Estimating the reach of the PIP Indigenous Health Incentive
It is estimated that there were 7,035 general practices in Australia in 2010-11.154 In 2010-11 there were an estimated 235 IHSs.155 To assess the “reach”156 of the practice sign-on to PIP Indigenous Health Incentive at a jurisdiction level, the total practice registrations as at May 2011 were compared to the total number of practices by jurisdiction. Details of the methodology used to calculate these estimates presented in Appendix H. below provides an indication of the reach, at the practice level, of the PIP Indigenous Health Incentive. There is substantial variation in the proportion of general practices and IHSs registered by jurisdiction. At a national level, the proportion of IHSs registered (56.6 per cent) is substantially higher than the proportion of general practices that have registered (28.4 per cent). Within jurisdictions there is also interesting variation in the reach by practice type. For example, in New South Wales three out of every four IHSs have registered but only one in four general practices registered. In contrast, within Western Australia the proportion of IHSs and general practices that have registered is similar at approximately two out of five primary health care services.
154 Primary Health Care Research Information Services 2011, SBO Key Division of General Practice characteristics 2010-2011, PHCRIS, Adelaide.155 Australian Institute of Health and Welfare 2011, Aboriginal and Torres Strait Islander health services report 2010–11: OATSIH Services Reporting—key results, cat. no. IHW 56, AIHW, Canberra.156 Reach is broadly defined as the number of participating practices divided by the total number of practices
137KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 38: Practice reach of PIP Indigenous Health Incentive by jurisdiction at May 2011.157,158
StatisticNSW/ACT QLD WA NT VIC SA TAS AUS
Mainstream general practices
2,796 1,179 573 105 1,687 537 158 7,035
General practices registered
753 478 223 18 328 140 55 1,995
Proportion Total Registered
26.9% 40.5%
38.9%
17.1%
19.4%
26.1%
34.8%
28.4%
Total IHSs 57 37 35 55 25 15 11 235Total IHSs Registered
43 25 14 22 NR* NR* NR* 133
Proportion IHSs Registered
75.4% 67.6%
40.0%
40.0%
NR* NR* NR* 56.6%
* For confidentiality reasons, this number is not reported.While the above data show the level of penetration or reach of this measure in terms of practice participation, it is also important to consider whether the measure is operating in areas that will benefit Aboriginal and Torres Strait Islander people. Estimates of “patient reach” are outlined below, with the details of the methodology used to calculate these estimates presented in Appendix H. The estimates presented in below. provide a guide to patient reach by state for the first six months of the measure – this data relates to 2010, and payments under the PIP Indigenous Health Incentive commenced in May 2010. At the national level, it is estimated that 26.5 per cent (31,646/119,456) of eligible patients registered for PIP Indigenous Health Incentive in 2010. As evidenced in below. below, there is substantial variation in the reach of the initiative across jurisdictions.
157 Primary Health Care Research Information Services 2011, SBO Key Division of General Practice characteristics 2010-2011, PHCRIS, Adelaide.158 Australian Institute of Health and Welfare 2011, Aboriginal and Torres Strait Islander health services report 2010–11: OATSIH Services Reporting—key results, cat. no. IHW 56, AIHW, Canberra.
138KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The four jurisdictions with the largest Aboriginal and Torres Strait Islander populations (i.e., New South Wales, Queensland, Western Australia and Northern Territory) have substantially different estimates of PIP Indigenous Health Incentive patient reach. In New South Wales it is estimated that 31.7 per cent of Aboriginal and Torres Strait Islanders with a chronic disease have registered, while in the Northern Territory it is estimated that only 10.3 per cent of Aboriginal and Torres Strait Islanders with a chronic disease have registered. In terms of remoteness, it is the inner and outer regional combined area that registered the highest proportion of patients. Further statistics on patient reach for the first six months of the measure are presented in below. and Table 40 below.Table 39: Estimates of PIP Indigenous Health Incentive reach for the Aboriginal and Torres Strait Islander population aged 15 years and over and with a chronic disease, by jurisdiction, 2010.159,160,161
Population (aged 15 years and over)
NSW QLD WA NT VIC SA TAS ACT
Population with one or more chronic diseases
35,491
32,926
16,379
14,714
8,022 6,485 4,407 968
PIP Indigenous Health Incentive Registered patients in 2010
11,244
8,460 5,017 1,518 2,659 2,164 208 376
Percentage of population that is registered
31.7%
25.7%
30.6%
10.3%
33.1%
33.4%
4.7% 38.8%
Note, the period of time this data is relevant to (2010) reflects only the first six months of measure implementation.
159 AIHW 2012, Chronic diseases (webpage), viewed March 2012.160 Australian Bureau of Statistics 2009, Experimental Estimates and Projections, Aboriginal and Torres Strait Islander Australians, 1991 to 2021, ABS cat. no. 3238, ABS, Canberra.161 Based on PIP data, provided by the Department of Health and Ageing 2012.
139KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
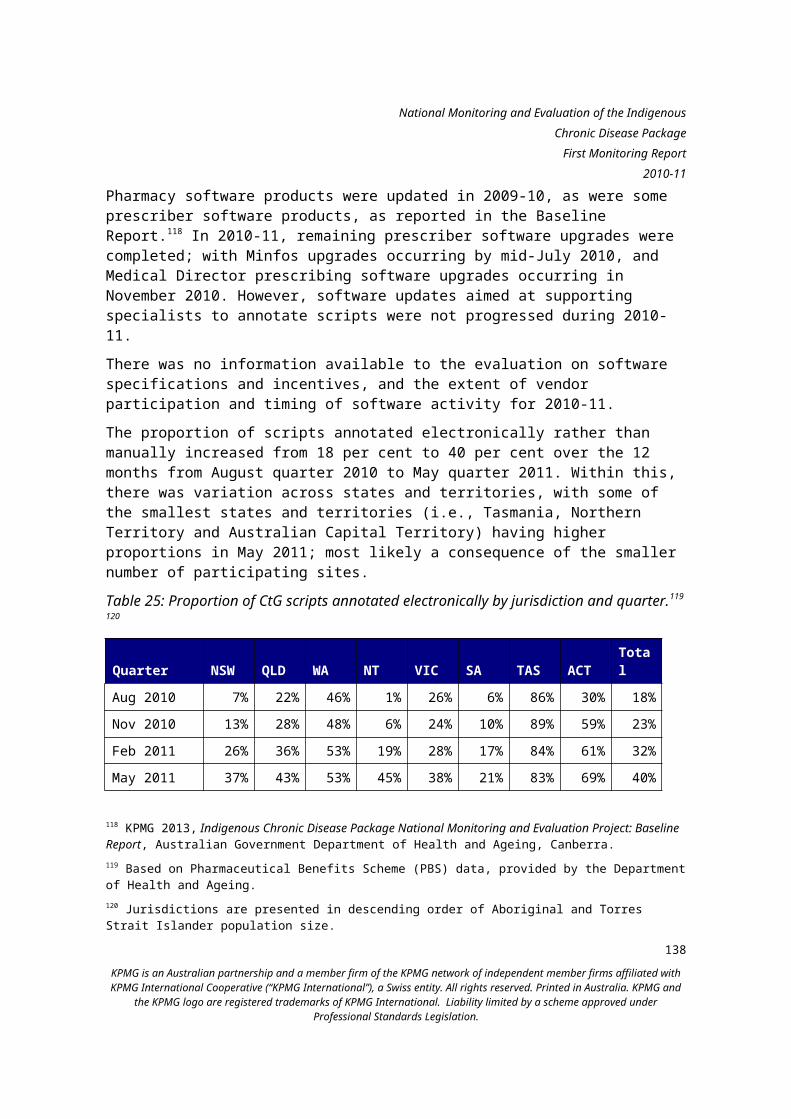
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 40: Estimates of PIP Indigenous Health Incentive reach for the Aboriginal and Torres Strait Islander population aged 15 years and over and with a chronic disease, by remoteness, 2010.162,163,164
Population (aged 15 years and over)
Major Cities
Inner and Outer Regional combined
Remote and Very Remote combined
Australia
Population with one or more chronic diseases
38,635 51,895 28,926 119,456
PIP Indigenous Health Incentive Registered patients in 2010
8,706 17,890 5,050 31,646
Percentage of population that is registered
22.5% 34.5% 17.5% 26.5%
Note, the period of time this data is relevant to (2010) reflects only the first six months of measure implementation.
1.34 Program supportCultural awareness training
In April 2011, the online cultural awareness training package developed by Royal Australian College of General Practitioners became available. Among other acceptable options165, this training meets the requirement for cultural awareness training expected of PIP Indigenous Health Incentive registered practices. Access to the training module is through the RACGP’s ‘gplearning’ platform, and is available free of charge to RACGP members and their general practice teams.166
162 AIHW 2012, Chronic diseases (webpage), viewed March 2012.163 Australian Bureau of Statistics 2009, Experimental Estimates and Projections, Aboriginal and Torres Strait Islander Australians, 1991 to 2021, ABS cat. no. 3238, ABS, Canberra.164 Based on PIP data, provided by the Department of Health and Ageing 2012.
165 Other acceptable options for cultural awareness training are noted in the Program Guidelines. Department of Health and Ageing and Medicare Australia 2010, Practice Incentives Program, Indigenous Health Incentive Guidelines – September 2010, Department of Health and Ageing, Canberra.166 Department of Health and Ageing 2010. Commonwealth’s Indigenous Chronic Disease Package Update, 10th edition, Department of Health and Ageing, Canberra.
140KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
While not funded through the measure, the Australian College for Rural and Remote Medicine has also developed an online cultural awareness module to meet the requirements of the PIP Indigenous Health Incentive.167
Practices that have signed on to the PIP Indigenous Health Incentive since 2010 are expected to complete cultural awareness training within 12 months of signing-on, or by April 2012, whichever is the later (the requirement is that two staff members, including one GP, must complete the training). Many stakeholders participating in regional forums, and consultations with Divisions of General Practice and other national, state and territory level stakeholders indicated that the requirements for cultural awareness training (two staff must complete training; training may be undertaken online) may not be adequate to support enhanced cultural awareness. This sentiment has been confirmed by the SBOs, who have reflected feedback from their membership that online training may be insufficient. Several examples of SBOs and Divisions of General Practice developing their own cultural awareness packages, with a focus on the local context, ongoing training and training to more than two staff members, have been provided to the evaluation during consultations. Stakeholders discussed the importance and value of IHPOs and ATSIOWs engaging directly with providers to deliver training which emphasised cross cultural learning. This was reported to further enhance the work being undertaken by ATSIOWs in the community to promote engagement with primary health care services. At the same time, input received from mainstream general practices at community visits indicate that some GPs prefer online training, and that providing training which GPs can complete in their own time presents one less barrier to participating in the PIP Indigenous Health Incentive. Program advisory support
The purpose of the PIP Advisory Group is to provide timely advice and assistance to the department on the development and implementation of initiatives available through the Practice Incentives Program (PIP). The implementation of the PIP Indigenous Health Incentive was discussed with the PIP Advisory Group in 2009 and 2010. Program guidelines
The Department of Human Services wrote to practices in March 2010 and invited them to join the PIP Indigenous Health Incentive. This mail-out provided practices with a copy of the PIP Indigenous Health Incentive guidelines and relevant forms. The guidelines are now available on the Medicare Australia website. The guidelines describe the various payments, the eligibility criteria, the practice obligations and the appeals process. 167 ibid.
141KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Practices consulted with during site visits reported that they are complying with the guidelines, and discussion of the implementation of PIP Indigenous Health Incentive in these practices reflected consistency with the guidelines. The extent to which this can be extrapolated more broadly is limited at this stage of the evaluation. In section 1.33 above perceived issues associated with the administrative burden of the requirements laid out in the guidelines are discussed. Promotion to practices
Activities for the PIP Indigenous Health Incentive in 2010-11 included ongoing communications and promotions through Medicare Australia’s publications, the PIP News Update (August 2010, November 2010, February 2011 and May 2011) and the Forum. Outside of departmental communication, promotion of the PIP Indigenous Health Incentive relies heavily on NACCHO affiliates, Divisions of General Practice SBOs, and the activities of the ICDP workforce. Some stakeholders have reported that the initial communications from the department were not easy to understand, and thus they invested considerable time in assisting with the preparation and submission of registration materials. IHPOs are intended to fulfil a role in the promotion of the PIP Indigenous Health Incentive to mainstream practices. As indicated earlier, there is evidence that IHPOs have worked with ATSIOWs to support practice staff to implement the system requirements for the PIP Indigenous Health Incentive. 1.35 Barriers and facilitators Barriers and facilitators to the implementation of this measure in 2010-11 relate to the PIP Indigenous Health Incentive as a gateway to the PBS Co-payment and Care Coordination and Supplementary Services (CCSS) measures; the behavioural response to incentives; having an identified cohort of Aboriginal and Torres Strait Islander patients; and PIP Indigenous Health Incentive administrative requirements. The link between the PIP Indigenous Health Incentive and the PBS Co-
payment measure as a facilitator. The PIP Indigenous Health Incentive patient registration form is also the PBS Co-payment registration form, although the eligibility criteria are different; the PBS Co-payment eligibility criteria additionally include Aboriginal and Torres Strait Islander children (under the age of 15) and people at risk of chronic disease. Patients eligible for both can choose to register for either one or both of the measures. Linking these two consent and registration processes is seen to provide an incentive for patients to register for PIP Indigenous Health Incentive where otherwise they may not. This link is reported by many to be the main driving force behind patient consent and registration from the patient’s perspective.
142KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Identified cohort of Aboriginal and Torres Strait Islander patients. IHPOs interviewed to date have reported the practices that are more likely to sign-on are those who have a previously identified cohort of Aboriginal and Torres Strait Islander patients. These practices see a clear link between care they are already providing and the PIP Indigenous Health Incentive requirements. In these instances, the PIP Indigenous Health Incentive is providing guidance, support and (cultural awareness) training which are highly valued by practices.
Administrative requirements as a barrier. Feedback received at Regional Forums indicates that the administrative requirements for participation in the PIP Indigenous Health Incentive may present a significant capacity challenge to primary health care practices, particularly small practices in regional locations. These practices may not find it viable to fully participate in the PIP Indigenous Health Incentive, as it was designed. The Sentinel Sites project identified this same issue as a barrier, along with a lack of availability of cultural awareness training requirement (possibly prior to release of the RACGP on-line training), for health services to be accredited, gaps in practice systems and workforce capacity.168
Unintended consequence of the incentive on provider behaviour. The significant expenditure on the measure above the expectations indicates that the PIP Indigenous Health Incentive has achieved substantial uptake. However, the mix of payments provided suggests that the incentives may be encouraging registration of patients without providing the desired services (to the Tier 1 requirements). It is possible that the low number of Tier 1 payments may be due to the limited time available for patients registered in 2010 to have received the targeted level of care provided by the practice within the 2010 calendar year.
1.36 OpportunitiesGiven the perception held by some stakeholders that the administrative requirements of the PIP Indigenous Health Incentive are unduly burdensome, particularly the re-registration process, the department may wish to consider whether this component should be maintained going forward. The causal model for the measure expects that increased delivery of better practice care will result from the provision of incentives to deliver specific chronic disease management, and the requirement to undertake cultural awareness training. In practice it is unclear whether the PIP Indigenous Health Incentive is having this effect. Evidence suggests that practice change may require a more guided intervention which considers and overcomes barriers to change within a supportive environment.169
168 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
143KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
One way to strengthen practice change may be through connecting participating PIP Indigenous Health Incentive practices with the Clinical Practice and Decision Support Guidelines (C5) measure, which offers materials to support better practice care delivery for Aboriginal and Torres Strait Islander patients. The department should also consider designing a more multi-faceted approach to supporting primary health care practice change in consultation with stakeholders in Indigenous health services and the mainstream primary health care system. Such interventions may potentially follow the format of pilot ‘improvement collaboratives’ such as the Australian Primary Care Collaboratives Program. While incentives may be a logical approach to changing behaviours, the design of the incentive approach should be highly sensitive to the business environment of private general practice. Adjustment of incentive payment regime may be required to encourage the desired level and type of service delivery.
169 National Institute for Health and Clinical Excellence 2007, How to change practice, NIHCE, London.
144KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Case study: Impact of the PIP Indigenous Health Incentive on the standard of care provided to Aboriginal and Torres Strait Islander people From the commencement of the initiative to May 2011, 2,128 practices signed up for PIP Indigenous Health Incentive. In 2010, there were 31,646 patient registrations. Up to May 2011, there had been 15,308 patient registrations. Of these, 5,517 were re-registrations from 2010.The data indicates that only a small proportion of patients who registered for the PIP Indigenous Health Incentive have received the target level of care associated with a Tier 1 outcomes payment. Tier 1 provides incentive for chronic disease management care planning, including the preparation and/or review of a GP Management Plan (GPMP) or Team Care Arrangement (TCA) for patients with chronic disease. In 2010, seven of 10 registered patients triggered an outcome payment, with the majority of patients triggering Tier 2 outcome payments only. Only one of 10 patients triggered a Tier 1 payment (note: almost all of these patients triggered a Tier 2 payment as well).One interpretation of the data is that primary health care practices are signing on and registering patients – largely administrative exercises and are failing to follow through with providing the prescribed MBS chronic disease management items (usually refers to providing or reviewing a GPMP or TCA). However, qualitative information gathered both by the department and through the evaluation indicates that the story is more complex.
145KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Re-registrationsPatients registered for
PIP Indigenous Health Incentive
GPs choose not to do a GPMP or TCA
GPs complete a GPMP, TCA
or review
GPs deem patients do not require a GPMP
or TCA
GPs provide care commensurate with a
GPMP or TCA, but don’t claim
Practices claim items 721, 723 or 732
Figure 16: Possibilities for patient flow through registration to Tier 1 payment. There are a number of reasons which may be contributing to low uptake of Tier 1 payments: GPs determine that not all PIP Indigenous Health Incentive registered
patients require additional services: GPs may determine that TCAs are unnecessary as the patient does not require a multidisciplinary management response. Furthermore, the GP may determine that even a GPMP is not warranted for some patients because their chronic disease is already well managed and they are unlikely to benefit from a more structured management approach. This decision could also reflect the wishes expressed by the patient in discussion with the GP – some people might not want a GPMP or TCA.
GPs may provide care consistent with a GP Management Plan or Team Care Arrangement, but fail to claim for the appropriate MBS item: This may occur as a result of the actions of individual GPs, i.e., GPs may create a care plan that does not conform to the requirements for the specified MBS items (e.g., 721, 723, and 732). Instead, they may bill for a consultation (e.g., Item 36) for providing services commensurate with care planning. Barriers to claiming relevant MBS items include a lack of communication between GPs and practice staff, poor understanding of the items and
146KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
claiming procedures or a perception that the administrative requirements are prohibitive.170
The relative value of payments creates an incentive to focus on patient registrations, rather than outcome payments: It is possible that some practices focus on registrations, which provide a higher per patient payment ($250), and do not consider that the payment for Tier 1 ($150) provides a strong enough incentive to complete the relatively more onerous associated tasks.171
GPs choose not to complete a GP Management Plan or TCA (or provide the commensurate level of care). Considerable research has been undertaken to examine the barriers to uptake of various MBS items.172,173 Reasons may include: - Time pressures: GPs perceive the increased workload imposed by the
requirements of GPMPs and TCAs as a barrier to uptake. In busy practices, GPs also see the opportunity cost (in this case, the cost of foregoing consulting with other patients) as too high to warrant completing GPMPs and TCAs.
- GP personal preference: In many cases, GPs are reluctant to alter their practice to complete GPMPs and TCAs. Some GPs feel that the items reduce autonomy over clinical decision making.
- Practice factors: Lack of appropriate IT infrastructure and poor computer literacy amongst practice staff may inhibit the introduction of GPMPs and TCAs, as practices do not have efficient processes for recording and disseminating information relating to the items. Practices may not invest sufficiently in GP education, meaning that GPMPs and TCAs are not well understood. Finally, the need to coordinate with providers across multiple sites may be a barrier where good communication and information sharing protocols are not in place.
- It is important to note that the number of registrations does include some re-registrations. Up to May 2011, there had been 15,308 patient
170 Preen DB, Bailey BES & Wright A 2006 ,’Willingness of general practitioners to participate in enhanced primary care discharge care planning’, Medical Journal of Australia, vol. 184, no. 2.171 It should be noted that this is additional to other payments associated with MBS billing. 172 Perkins D, Larsen K, Davies GP &Taggart J 2006, Practice level barriers and enablers to the uptake of the Chronic Disease Management Items and Service Incentive Payment for Diabetes, UNSW Research Centre for Primary Health Care and Equity, Sydney, viewed 4 July 2012.173 Wilkinson D, Mott K, Morey S, Beilby J, Price K, Best J, McElroy H, Pluck S & Eley V 2003, Evaluation of Enhanced Primary Care Medicare Benefits Schedule Items and the General Practice Education, Support and Community Linkages Program (GPESCL) Final Report, Department of Health and Ageing, Canberra.
147KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
registrations. Of these, 5,517 were patient re-registrations from 2010, which equates to 36 per cent of patient registrations in 2011.174
1.37 Purpose and scope of the case study Recognising there are alternative explanations for the payments data, this case study is concerned with actual impact on care: the extent to which practices registered for the PIP Indigenous Health Incentive have improved the standard of care provided to their Aboriginal and Torres Strait Islander patients with chronic disease. A number of sub-questions were also identified, and these are specifically addressed below in section 1.39.Due to the small number of practices involved in the cases study interviews, the views presented here are not necessarily generalisable to/representative of all practices registered for the PIP Indigenous Health Incentive. This case study provides important insight into the evaluation questions rather than claiming definitive answers.This case study presents two vignettes which provide alternative experiences of primary health care practices registered for the PIP Indigenous Health Incentive. These vignettes are composite examples which have been developed based on information provided by stakeholders (including GPs, Practice Managers, Practice Nurses, Care Coordinators and others) at multiple practices. It is apparent that implementation of the PIP Indigenous Health Incentive varies to a large degree by practice type, i.e., whether the practice is a general practice or an IHS. These vignettes emphasise that there are significant benefits to participation outside of the Tier 1 outcomes payments that can impact the standard of care. 1.38 VignettesVignette1: A general practice registered for the PIP Indigenous Health Incentive The Town and Country Medical Practice (TCMP)175 is located in an outer regional area and has 40 regular patients who identify as Aboriginal and Torres Strait Islander. This represents around three per cent of all of their patients. The Aboriginal and Torres Strait Islander patients who regularly attend this clinic are by and large employed, have stable housing and have health outcomes comparable with non-Aboriginal and Torres Strait Islander people in the town. Other Aboriginal and Torres Strait Islander people access this practice occasionally and usually go to the large IHS close by.
174 PIP data, provided by the Department of Health and Ageing 2011.175 Practices and individuals referred to in the case study are not actual practices and people.
148KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
TCMP signed up for the PIP Indigenous Health Incentive after six months of discussions with the practice support team from the local Division of General Practice (Division or DoGP). Initially, they had some concerns about the cost of cultural awareness training required by the PIP Indigenous Health Incentive. Then Aboriginal patients started to ask them about free or reduced cost CtG medications (through the PBS co-payment), and the IHPO at the Division was able to organise some training which met the requirements. Eventually, TCMP staff agreed that the likely benefit to their patients was worth the effort. Having participated in the Australian Primary Care Collaborative (APCC), and being an RACGP-accredited practice, TCMP already had a good patient recall system, a chronic disease register and some processes in place to identify Aboriginal and Torres Strait Islander patients.The ATSIOW from the Division, however, pointed out to the Practice Manager that some of their Aboriginal and Torres Strait Islander patients had not been identified. The identification of Aboriginal and Torres Strait Islander patients is also a requirement under RACGP registration, so the TCMP Practice Manager had considerable motivation to review the existing processes. The existing patient identification system required new patients to complete an intake form including a question asking if the patient is of Aboriginal or Torres Strait Islander origin. Periodically, reception staff would ask all patients to confirm their personal information including their Aboriginal or Torres Strait Islander origin. These processes seemed to work well for new patients, but reception staff reported that they did not feel comfortable asking existing patients whether they are of Aboriginal or Torres Strait Islander origin – it seemed rude or embarrassing to them. They often skipped that question, which continues to be an issue in the practice. The Division’s IHPO suggested additional strategies to improve Aboriginal and Torres Strait Islander identification. He provided posters for the waiting room so the practice could advertise their participation in the PIP Indigenous Health Incentive and the benefits of patient registration. He noted that the practice could consider hanging Aboriginal art or providing waiting room reading material like the ‘Koori Mail’.The three GPs at TCMP have so far registered 18 patients for the PIP Indigenous Health Incentive. More Aboriginal and Torres Strait Islander patients – 30 patients -- have been registered for CtG scripts, and GPs think this might be improving medication compliance for at least a few patients. Of the 18 patients registered for the PIP Indigenous Health Incentive, 10 have had health assessments and five have care plans in place. The Practice Nurse does most of the work required for the health assessment and care plans, and the GPs review and finalise these in line with the MBS requirements. Participation in the APCC has further supported TCMP’s participation in the PIP
149KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Indigenous Health Incentive by improving processes to manage timing of health assessments and care plans. The GPs have not changed the nature of the clinical care they provide to Aboriginal and Torres Strait Islander patients in the treatment of acute conditions or even acute exacerbations of chronic disease. They pride themselves on providing high quality care to all Australians. But care planning is now more proactive, and staff are more aware of their Aboriginal and Torres Strait Islander patients. This has brought new attention to service delivery. For instance, the Practice Nurse has found that health assessments are a good opportunity to build rapport with Aboriginal and Torres Strait Islander patients. She feels that patients trust her more as a result and she can more naturally work into a discussion about chronic disease risk factors and management. At the same time, the Practice Nurse is very busy, and there is not a lot of time to fit in health assessments and care plans. She arranges these patient appointments around her other work. Finding an appropriate space in the practice can also be difficult, especially since TCMP now has visiting allied health providers coming in most days. There are other challenges to participation in the PIP Indigenous Health Incentive. One of the most frustrating issues for the Practice Manager is the annual patient re-registration process. In her view, this requirement seems unnecessary given that patients will continue to meet the eligibility criteria. The requirement is also perplexing in its difference from the PBS Co-payment, where patients only need to register once. The other problem with patient registration is that only one practice can ‘own’ the patient. Medicare has rejected some of the patient registration forms submitted by TCMP because some of the regular patients were already registered by the local IHS. Again, this seems to be extra administration for TCMP for no benefit. As is apparent by their participation in the APCC, TCMP is a practice that is dedicated to improved delivery of care. On a small but tangible scale, they have seen benefits from the PIP Indigenous Health Incentive for their Aboriginal and Torres Strait Islander patients. There are benefits to the practice too: when formal care planning occurs at TCMP, they make sure to bill against the relevant MBS item, and have received outcomes payments as a result. This clearly involves a team effort, and that is “how we practice at TCMP”.
Discussion of vignette 1
Many mainstream GPs see only a small number of Aboriginal and Torres Strait Islander patients. In such circumstances, it can be hard to justify significant
150KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
changes to practice. This is the case even where the practice has a dedicated mandate and culture for improvement. Based on stakeholder consultation conducted to date, it appears that mainstream practices are largely complying with registration requirements by increasing their cultural awareness, improving front desk practices, ensuring that their patient recall systems and chronic disease registers are in place or updated and increasingly considering how they can best offer services to local Aboriginal and Torres Strait Islander people. It is also clear from these consultations that target levels of care associated with Tier 1 outcomes payments are most commonly achieved through nurse-led models. An example of this occurs through allocating dedicated time for practice nurses to work with Aboriginal and Torres Strait Islander patients to increase provision of health assessments and organising care planning. For some small practices with limited administrative and nursing support, it can be very difficult to set up systems to process health assessments and care plans at the volume necessary to justify the expense. Moreover, GPs generally state that the number of health assessments and care plans does not necessarily correlate with the quality of care being provided on an ongoing basis.In the mainstream setting, it seems that PIP Indigenous Health Incentive works best when there are other supportive programs and incentives and the right practice culture. Supportive programs may include the APCC, which promotes a team based model of care, connection with other ICDP benefits such as the PBS Co-payment and the CCSS program, and the help of ICDP staff such as IHPOs and ATSIOWs. Vignette 2: A PIP Indigenous Health Incentive registered IHS The Main Street Aboriginal Medical Service (MSAMS) is a large IHS in an outer regional area which provides comprehensive primary health care and some related social services to around 800 Aboriginal and Torres Strait Islander patients and a small number of non-Aboriginal and Torres Strait Islander patients. MSAMS signed on for the PIP Indigenous Health Incentive as soon as it was announced and registered all of their eligible patients. They have used the income generated by incentive payments to support development of a dedicated chronic disease management program. Within the MSAMS approach, an AHW spends a few days a week managing a chronic disease register with over 90 patients, and gets patients in for health assessments and care plans. An ICDP Care Coordinator employed at the IHS has started to support the AHW and works with those patients who need some extra help to manage their chronic disease. A part time position has also been created for an administrative assistant to support the Care Coordinator and
151KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
manage the PIP Indigenous Health Incentive paperwork. MSAMS has converted an office for the chronic disease management program. Since it has gotten off the ground, many patients have been involved and news about the program has spread in the community. One of the challenges for chronic disease management care at MSAMS has been the turnover of GPs. Some doctors do not get to know their patients very well which limits their capacity to build rapport and identify care needs. Some community members do not feel comfortable with the prospect of seeing a new GP and this is one of the reasons they are reluctant to come in for regular care. MSAMS have found that building the chronic disease program around the AHW who knows the community members well can somewhat offset this problem. For MSAMS, the PIP Indigenous Health Incentive has offered significant motivation to build a system that optimises benefits for the clinic and patients. They are more thorough in ensuring that patients with chronic disease are identified, registered, receive health assessments and have care plans. This system has worked well for the registered patients who are willing to come in and receive care. It is difficult to engage some community members and some are worried about the cost or hassle of follow up care.As a result of the PBS Co-payment, MSAMS no longer stocks its own dispensary, which has also lifted a financial and administrative burden. The MBS billing and the Supplementary Services funding process is a lot of work, but they stay on top of it. All of this has not happened immediately, and the additional administrative support and Care Coordinator have helped a great deal in making it happen. As there are many factors that influence the health of community members, it is hard to pinpoint what health outcomes have resulted from the PIP Indigenous Health Incentive at MSAMS. Although with this better resourced and more deliberate approach to chronic disease management at the MSAMS clinic, patients are more likely to get the care that they need.
Discussion of vignette 2
IHSs, and particularly large IHSs, have been able to use the significant income generated through the PIP Indigenous Health Incentive to make complementary staffing and process changes. Like in the MSAMS vignette, this often includes allocation of administrative support to manage the MBS and PIP Indigenous Health Incentive paperwork and clinical staff to drive enhanced chronic disease management. Many of the registration requirements, such as improving identification of Aboriginal and Torres Strait Islander patients and increasing cultural
152KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
awareness, are not as relevant in the IHS setting, though some IHSs have described ‘tightening’ their processes in this regard. 1.39 Summary of findingsThe case study sheds light on the ways that general practices and IHSs have responded to the incentives and offer some insight into the pattern of Tier 1 outcomes payments. We have seen, for instance, that practices need human resources and practice management systems to support service delivery and care planning in accordance with MBS billing requirements. Patients must also be engaged and attend the clinic for care planning – not to mention follow up care for chronic disease management. The vignettes presented in this case study are not representative of all practices registered for the PIP Indigenous Health Incentive, and the findings could be the result of a stakeholder selection process that has favoured highly engaged primary health care practices. In these vignettes, practices state that they are billing for MBS items associated with the PIP Indigenous Health Incentive. This case study offers insight into the sub-questions, as discussed here:1. How have PIP IHI registered practices changed the way they provide
services and care to Aboriginal and Torres Strait Islander patients in relation to the front desk, services capability, patient management, care management and linkages with other health services?
The two vignettes demonstrate that primary health care practices can improve processes that are important in the patient experience and management of care. For general practices, involvement in the incentive program has led to increased cultural awareness and closer examination of processes to identify Aboriginal and Torres Strait Islander people. For IHSs, the PIP Indigenous Health Incentive represents an important new stream of income for the IHS which can allow for reallocation of resources and development of dedicated programs for chronic disease. The information collected to date does not include evidence of increased linkages with other health services as a result of participation in the PIP Indigenous Health Incentive. 2. To what extent and how have any such changes improved the level of care
provided to patients?In these two vignettes, both the mainstream general practice and IHSs are providing an enhanced level of chronic disease care to their Aboriginal and Torres Strait Islander patients. In the story of the general practice, the PIP Indigenous Health Incentive may lead to an increase in health assessments and care plans, but not at a
153KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
significant volume (because of the practice already focused on these matters). From an investment perspective, the number of Aboriginal and Torres Strait Islander patients does not warrant more significant or systemic changes to how care is provided at the practice. Within the IHS example, the increased practice capacity suggests that more community members with chronic disease can be monitored more closely. Considering the limitations of the case study, it is not possible to quantify the extent to which care delivery has changed; however, it appears that engaged practices are making improvements in order to provide care planning services to a greater proportion of their patients. 3. To what extent have care planning practices changed as a result (using
care planning more often, changed the approach to care planning)?It appears that care planning practices for Aboriginal and Torres Strait Islander patients have not changed significantly for the general practices involved in the case study. As shown in vignette 1, the small number of Aboriginal and Torres Strait Islander patients does not warrant systematic practice changes. Practices believe that they provide a high standard of care for all of their patients. IHSs with good practice management may find significant payoff in increasing the volume of care plans for their registered patients. The vignettes in this case study represent successful implementation of the PIP Indigenous Health Incentive; not all primary health care practices have been as successful. Barriers to care delivery (as commensurate with Tier 1 outcomes payments) include absence of practice nurses or similar roles, limited administration capacity, and lack of ability or willingness to navigate the requirements for MBS care items. 4. To what extent do practices adhere to the practice registration (sign-on)
requirements (registration of patients' Indigenous status, recall and reminder system, cultural awareness training and script annotation); and what are the related issues and barriers?
The case study vignettes show that engaged practices are committed to meeting the requirements of registration with the PIP Indigenous Health Incentive. The availability of RACGP and local cultural awareness training provides general practices with options to meet the requirement. It appears that recall and reminder systems and CtG scripts are set up as a matter of course within the practice. Identification of Aboriginal and Torres Strait Islander status may present a more challenging requirement. It appears that some reception staff are uncomfortable asking this question because of the perceived stigma associated with identification.
154KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
5. Can the above changes be attributed to the PIP Indigenous Health Incentive or other ICDP related initiatives?
In both general practices and IHSs, benefits associated with the PIP Indigenous Health Incentive are best achieved through synergies between a number of ICDP measures. For general practices, ICDP teams in Divisions (e.g., IHPOs, ATSIOWs, and Care Coordinators) often play a critical role in supporting practices to implement the PIP Indigenous Health Incentive and other ICDP measures. For IHSs, ATSIOWs and Care Coordinators offer staff capacity to improve current processes and care delivery. In both settings, free or inexpensive medicines (PBS co-payment) are the most significant incentive for patients to consent to participation in the PIP Indigenous Health Incentive, and they offer the most accessible and tangible benefit.6. Do PIP Indigenous Health Incentive registered practices utilise available
MBS items relevant to health checks and chronic disease management in a consistent way. Why or why not?
The primary health care practices interviewed for this case study have indicated that they bill MBS for health checks and care plans. Without an audit of service delivery and billing practices, it is not possible to comment on the precision and consistency of MBS billing practices across practices registered for the PIP Indigenous Health Incentive.
155KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Care Coordination and Supplementary Services Program (B3b)In this chapter, we discuss the implementation of the CCSS Program in 2010-11, the second year of the ICDP, including achievements, activities, facilitators, barriers, signs of progress towards desired outcomes, and opportunities for the future. The CCSS measure at a glance The implementation of the CCSS Program proceeded as planned in 2010-11, in line with the program guidelines and with evidence of appropriate variation in service models and referral pathways. Key achievements included the recruitment of 22.1 FTE positions across Australia, and 192 individual patients receiving care coordination services. Most Care Coordinators (17.6 FTE) were based in mainstream Divisions of General Practice, with the remainder located in IHSs. Forty per cent were based in urban areas, with 10 per cent in remote areas and the remainder in regional areas.There was a National Coordinator position recruited to the Australian General Practice Network (AGPN) to support the CCSS Program. Planning for further recruitment of Care Coordinators in 2011-12 was also commenced in 2010-11. The CCSS Program appears to have been implemented in line with the program guidelines, with evidence of varying service models and referral pathways as intended. In 2010-11, significant attention was given to working through the operational elements of the Care Coordinator roles, which vary by location. The early focus for Care Coordinators has been on identifying referral pathways and delineating roles with other health care providers.A total of 83 individual patients received Supplementary Services funding in 2010-11. Stakeholders identified issues related to the conditions and processes for the use of Supplementary Services funding. However, the department has taken action to improve understanding and support utilisation of Supplementary Services funding. 1.40 Potential effects based on implementation findingsFigure 17 below is the causal pathway for the CCSS Program. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
156KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
CCSS Program Increase in primary health care system capacity to provide coordinated care
Increase in coordinated,
multidisciplinary care
Improvement in Aboriginal and Torres Strait
Islander people’s chronic conditions
Aboriginal and Torres Strait
Islander patients
engage with the CCSS Program
Primary health care providers make referrals
to Care Coordinators
Care Coordinators
have a connection to a registered practice/s
Primary health care practices are registered
for the PIP Indigenous
Health Incentive
Figure 17: CCSS program causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect176 and the observed impacts.177 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the CCSS Program measure and it was implemented according to plan in 2010-11, therefore the plausibility of effect is not affected. All of the key dependencies are in place to a limited extent, and scope exists to scale these up to increase the effectiveness of the measure over time.
176 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.177 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
157KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 41: Assessment of key dependencies of the B3b measure.
Key dependencies
Finding Evidence
Primary health care practices are registered for the PIP Indigenous Health Incentive
Practices are registered, but there is scope to increase practice participation. As at May 2011 56 per cent of all Indigenous health services had registered for the PIP Indigenous Health Incentive, which is almost double the rate of mainstream general practices (28 per cent). However, there are many more mainstream general practices than IHSs eligible for registration.
This is based on analysis of measure documentation, and empirical evidence; analysis of Medicare data
Care Coordinators have a connection to a registered practice/s
The connections between Care Coordinators and registered practices were being established in 2010-11.
Qualitative information gathered from a small group of relevant stakeholders
Primary health care providers make referrals to Care Coordinators
As Care Coordinators build relationships with providers, referrals follow, but this can be further scaled up. Care Coordinators are more likely to use alternative referral pathways where they are not co-located in a primary health care service and bring the patient to the provider for subsequent formal referral.
Qualitative information gathered from a small group of relevant stakeholders
Aboriginal and Torres Strait Islander people engage with the CCSS Program
There has been good uptake of the CCSS Program by Aboriginal and Torres Strait Islander patients.
Data provided by the department, and a case study based on consultations with a small sample of IHSs and mainstream general practices
158KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Finding Evidence
Contextual considerations
A core role of Care Coordinators is to support relevant referrals to other services, to address patients’ chronic condition(s). However, the ability of Care Coordinators to undertake this role may be limited based on the number of relevant services within a location. This is likely to be particularly impacting in rural and remote locations. Supplementary Services funds can be used to facilitate access to transport where a service is not available locally; in locations where this is frequently required Care Coordinators may have to focus their efforts at facilitating access to services, whereas others in better resourced locations may be more able to focus their efforts on other aspects of the role.
Analysis of measure documentation and publicly available policy documentation
Table 42 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). The evaluation is not able to measure change in the expected impacts, but there is some evidence of progress in respect of the measure’s impact on coordinated, multidisciplinary care. Contextual factors which appear to be influencing the measure are the variation in availability of relevant services across different locations; and the different service models adopted for the program.
159KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 42: Assessment of expected and observed impacts of the B3b measure based on implementation progress.
Expected impacts
Observed impacts Evidence
Increase in primary health care system capacity to provide coordinated care
At this stage, the evaluation is not able to measure change in system capacity. Compared with other ICDP workers, the small numbers of Care Coordinators (22.1 FTE) recruited in 2010-11 is likely to limit the extent to which these positions increased system capacity. Further, there is a lag between recruitment and care coordination, as Care Coordinators take time to build relationships with clients, providers and other services. Limits on permitted uses are also likely to have capped the extent to which the measure contributed to increased capacity.
Recruitment data provided by the department, and qualitative information gathered from a small group of relevant stakeholders
Increase in coordinated, multidisciplinary care
At this stage, the evaluation is not able to measure change in coordinated, multidisciplinary care. Where Care Coordinators have been in place for some time, are well connected within the local health care system, and have strong organisational support, they are able to support patients in a way which increases coordinated, multidisciplinary care. However, the extent of impact is likely to have been low in 2010-11 due to the state of implementation.
Recruitment data provided by the department, and qualitative information gathered from a small group of relevant stakeholders
Improvements in Aboriginal and Torres Strait Islander people’s chronic conditions
Data is not available for the First Monitoring Report.
Not applicable
160KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected impacts
Observed impacts Evidence
Contextual considerations
Fund holders have taken a variety of approaches to implementation of the CCSS program to suit local needs. This has resulted in different service delivery models – for instance delivery through IHSs, Medicare Locals/Divisions, or GP private practices, with part time or full time Care Coordinators. A range of approaches to professional networking have also been undertaken. This variation in approaches to implement the program may lead to variable impacts across different settings.
This is based on a case study, drawing on consultations with a small sample of IHSs and mainstream general practices
1.41 Measure overview The CCSS measure establishes a Care Coordinator workforce to support patients with certain chronic diseases and complex care needs in the implementation of their GP-developed care plan. It also provides a pool of funds (Supplementary Services funds) to support access to medical specialist and allied health services relevant to the patient’s care plan, local transport to appointments and other relevant needs associated with the care plan. Funding for the CCSS Program has been provided to the State Based Organisations (SBOs) of the Divisions of General Practice, which in turn have subcontracted the funds to place Care Coordinators in Divisions of General Practice or, in a few cases, in IHSs. In some cases, Divisions of General Practice have then funded individual mainstream general practices to employ or part fund care coordination within their practice. The total budget for the CCSS measure for the duration of the ICDP (from 2009-10 to 2012-13) is $73 million. In 2010-11, the annual budget for the measure was $7.306 million (excluding GST). While the budget has been fully allocated by the department to SBOs, consultations indicate that not all SBOs were able to expend the funds within the financial year. 1.42 Care Coordinators Recruitment of Care Coordinators
The evaluation found that the recruitment of Care Coordinators is largely on track, with filled positions spread across all Australian jurisdictions except Tasmania178; in both mainstream organisations and IHSs, and in urban, regional and remote locations. Recruitment challenges were reported in the 178 Where recruitment had not commenced in 2010-11.
161KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Northern Territory and Queensland, and there is no information available on retention rates. Findings in this section are informed by program documentation and information provided by the department, consultations with the department, stakeholder feedback from Regional Forums, and interviews with the AGPN, fund holders and Care Coordinators.The recruitment of Care Coordinators commenced in 2010-11, with 22.1 FTE staff recruited nationally, including a National Coordinator position (1 FTE) recruited to the AGPN. Table 43 below identifies the number of Care Coordinators recruited in each state or territory. The department did not determine a total target of position numbers, or the allocation of positions for individual locations; rather, each SBO received a pool of funding and allocated funding to Divisions of General Practice (and in some cases IHSs) based on their needs assessments. These needs assessments drew on work undertaken by Divisions of General Practice, under the Engaging Divisions of General Practice to Improve Indigenous Access to Mainstream Primary Care (C3) measure (where this measure is operating).179 A number of stakeholders stated that this is an appropriate approach, because it supports development of locally appropriate service models. Table 43: Number of Care Coordinators (FTE and headcount) recruited by states and territories, 2010-2011. Source: Department of Health and Ageing.180
Jurisdiction
Care Coordinators recruited in 2010-11 (FTE)
Care Coordinators recruited in 2010-11 (number of people)
NSW 8.8 9QLD 4.5 6WA 2.6 5NT 1 1VIC 1.2 2SA 2 2TAS* 0 0ACT 2 2
179 Department of Health and Ageing April 2010, Indigenous Chronic Disease Package, Care Coordination and Supplementary Services, Program Guidelines, April 2010, Department of Health and Ageing, Canberra, p. 12, viewed 15 November 2012.180 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [B3b response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
162KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Jurisdiction
Care Coordinators recruited in 2010-11 (FTE)
Care Coordinators recruited in 2010-11 (number of people)
Total 22.1^ 27* Recruitment had not commenced in 2010-11. ^Includes the national coordinator based at the AGPN.
Most Care Coordinators (16.6 FTE) in 2010-11 were located within Divisions of General Practice, with the balance (4.5 FTE) located in IHSs and 1.0 FTE based in the AGPN to assist with national coordination. Table 44 below presents the breakdown of Care Coordinator positions recruited in 2010-11 by area of remoteness. This shows that 40 per cent of Care Coordinators are based in urban areas, followed by outer regional areas, then inner regional areas. Almost 10 per cent are based in remote areas. Table 44: Care Coordinators recruited in 2010-11 (FTE and headcount) by urban, regional and remote location.181
Geographical classification*
Care Coordinators recruited in 2010-11 (FTE)
Care Coordinators recruited in 2010-11 (number of people)
Proportion of total (%)
Urban (RA1) 8.8 11 40%Inner Regional (RA2) 5.1 6 23%Outer Regional (RA3) 6.2 8 29%Remote (RA4) 2 2 8%Total^ 22.1 27 100%*Based on the Australian Standard Geographical Classification (ASGC). ^Includes the national coordinator based at the AGPN.
The AGPN reported that recruitment was proceeding according to plan in all jurisdictions in 2010-11, apart from the Northern Territory, where limited workforce capacity and a large number of territory based and other department funded positions competing for candidates made recruitment challenging. The Queensland SBO also reported some difficulties in recruiting and retaining Care Coordinators in that jurisdiction, but did not indicate whether this was a statewide issue or relevant to particular regions. Some recruitment and retention issues for Care Coordinators were identified through consultations with Care Coordinators (16 consulted to date, across site visits and case studies), fund holders and organisations and national stakeholders.
181 Based on the workforce location report provided by the Department of Health and Ageing. 163
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Care Coordinators are required to have a clinical background, and fund holders and Divisions reported that this created recruitment challenges. However, Care Coordinators consulted during the evaluation consistently expressed the view that the requirement to have a clinical background is appropriate and necessary for the Care Coordinator role.
Care Coordinators are required to build professional networks, establish referral pathways and develop referral tools to support effective care coordination. Three of the six Care Coordinators consulted reported that this developmental work was very challenging in the absence of clear guidance (from the department, SBO and/or their employer), and the provision of templates (for example, referral tools). Other Care Coordinators reported that they had been provided with sufficient support and were able to successfully establish structures and pathways in the early stages of their role without difficulty.
It is not possible to analyse whether Care Coordinators have been appropriately deployed to meet need. One way to assess this would be to determine the extent to which the deployment of Care Coordinators mirrors the distribution of the PIP Indigenous Health Incentive registered practices (given that these practices are the primary referral source). However, information about the number and location of PIP Indigenous Health Incentive registered practices is not publically available. Funding allocations to SBOs were largely based on the size of the Aboriginal and Torres Strait Islander population in each jurisdiction. The model of allocating Care Coordinators described above – through provision of funding to SBOs to facilitate localised deployment of Care Coordinators in response to local needs assessments – is a process likely to have supported needs-based deployment. Care Coordinators have reported a number of different professional development opportunities available to them, including the Flinders Chronic Disease Self Management (CDSM) training (available through the Improving Indigenous Participation in Health Care through Chronic Disease Self Management measure of the ICDP), state-based Care Coordinator orientation182 and teleconference meetings with professional networks. Although data is currently not available, it appears from consultation with various stakeholders that the majority of Care Coordinators are not of Aboriginal or Torres Strait Islander descent. Cultural awareness training is not a requirement for the role, but some Care Coordinators identified that this training would be beneficial. Care coordination structures and referral pathways
The evaluation has found that establishing service models, referral pathways and networks has been the focus for Care Coordinators recruited in 2010-11, 182 In New South Wales only.
164KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
and is necessary for bedding down the CCSS Program. These findings are informed by data provided by and consultations with the department, consultations with the AGPN, fund holders and Care Coordinators, and the Sentinel Sites Evaluation.183 Care Coordinators provide service delivery to Aboriginal and Torres Strait Islander patients with a chronic disease who are referred by a GP in a general practice or IHS that is participating in the PIP Indigenous Health Incentive.184
Referral pathways
While the CCSS program guidelines describe a referral pathway that starts with the GP, in reality, Care Coordinators have used all manner of strategies to identify patients – both through GPs (referred to by some Care Coordinators as the ‘top down’ approach to patient recruitment) and by identifying patients in the community (the ‘bottom up’ approach). Care Coordinators and other ICDP workers consulted who discussed entry into the CCSS Program were mainly based in urban and regional locations, and described a range of referral pathways. These included referrals from GPs, staff members who conduct health checks, community health organisations, outreach services, Aboriginal and Torres Strait Islander organisations, specialists, discharge and care coordination positions in hospital, and self-referrals. In some organisations, the Aboriginal and Torres Strait Islander Outreach Worker (ATSIOW) plays a role in identifying patients who would benefit from the CCSS Program. Care Coordinators were more likely to use alternative processes where they were not collocated or embedded in a primary health care service with established referral pathways. It is understood that Care Coordinators using alternative referral pathways subsequently seek referrals from PIP Indigenous Health Incentive registered GPs. See also the case study at the end of this chapter for further discussion of referral pathways.The referral pathways established by a Care Coordinator appear to have best gained traction in areas where the Care Coordinators had previously existing relationships with health care providers, usually from their previous roles. Where such established networks have not been present, stakeholders have described the significant effort needed to build awareness, support and uptake of the service from GPs.
183 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.184 It is possible to obtain an exemption to this requirement in areas where a scarcity of PIP Indigenous Health Incentive registered practices is a barrier to obtaining referrals to the CCSS Program.
165KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Based on the limited consultations with Care Coordinators undertaken to date (16 in total across site visits and to inform case studies), it appears that appropriate referrals of patients with complex and multiple needs are being made. This will require further investigation throughout the evaluation.
Service models
The CCSS program guidelines permit a variety of care coordination service models, including supplementing existing or establishing new structures and services – as long as the model takes into account community need, related services, cost efficiency and maximising services to patients.185 Consultations suggest that the extent to which the CCSS program is providing new care coordination structures or augmenting existing structures varies across fund holders. During some community site visits, the Care Coordination model being implemented represented a completely new service (primarily where Care Coordinators were located within Divisions); while in others new workers had been incorporated into existing chronic disease management programs (most commonly where Care Coordinators were located in IHSs and general practices). A variety of service models were described by the AGPN, fund holders and Care Coordinators consulted, for example: a ‘one-stop-shop’ model with Care Coordinators providing services through
a clinic as part of a team of health workers (e.g., GPs, specialists, nurses, AHWs) and providing other ICDP-funded services at the same time (such as USOAP specialist services, PBS co-payment and PIP Indigenous Health Incentive registration);
one person sharing a FTE load between the 0.5 FTE Care Coordinator role and other programs; and
sharing clinical components, implementing care plans and other Care Coordinator activities between an allied health provider and other staff such as AHWs.
The extent to which CCSS is augmenting existing programs will depend to some extent on the location of the service and whether there are similar programs funded by state or territory governments in place. For example, in New South Wales the Connecting Care (Severe Chronic Diseases Management) program provides a very similar service.186 The ICDP Sentinel Sites Evaluation Report commented that there are existing care coordination
185 Department of Health and Ageing 2010, Indigenous Chronic Disease Package, Care Coordination and Supplementary Services, Program Guidelines, April 2010, Department of Health and Ageing, Canberra, p. 9, viewed 15 November 2012.186 New South Wales Government 2012, NSW Chronic Disease Management Program (Connecting Care in the Community) (webpage), viewed 15 November 2012.
166KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
services available in some communities, and that stakeholders are aware of the need to minimise duplication.187
Care coordination services
Care coordination services appear to comply with the program guidelines, which are flexible to allow a variety of service models and approaches to be developed to respond to local needs and conditions. In 2010-11, Care Coordinators were establishing their new role and undertaking a range of activities which vary across locations and settings, including both public health/systems-focused activities and assistance to individual patients in line with their care plan. These findings are informed by program documentation; stakeholder feedback from Regional Forums; consultations with Care Coordinators, other ICDP workers and primary health care providers; and community focus groups.
Care Coordinator activities
Table 45 below identifies the number of patients who received Care Coordinator services in 2010-11, as well as those who have received funds from the Supplementary Services pool. Demographic information about patients receiving services was not available. Data for referrals and episodes of service was not available.Table 45: Number of patients who received Care Coordinator services and/or Supplementary Services funding, by state or territory, 2010-11.188
JurisdictionNumber of Care Coordinators (FTE)
Number of individual patients receiving Care Coordinator services
Number of individual patients receiving Supplementary Services funding
New South Wales 8.8 32 4Queensland 4.5 11 0Western Australia 2.6 24 5
Northern Territory 1 10 10
Victoria 1.2 52 20
187 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.188 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [B3b response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
167KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
JurisdictionNumber of Care Coordinators (FTE)
Number of individual patients receiving Care Coordinator services
Number of individual patients receiving Supplementary Services funding
South Australia 2 19 0Tasmania^ 0 0 0Australian Capital Territory 2* 44 44
Total 22.1 194 83* Includes the national coordinator based at the AGPN.^ Recruitment had not commenced in 2010-11.
The high variability between worker-to-patient ratios is most likely due in part to workers having been employed for varying lengths of time during the financial year. Since the Care Coordinator is a new position in the employing organisations, networks, organisational relationships and referral mechanisms have been a focus of implementation. Fund holders and Care Coordinators have described varying degrees of traction in building demand and utilisation of the service, which appears to depend largely on the awareness and receptivity of referring health care providers. Early indications are that the measure has the potential to fulfil a significant need, with some stakeholders describing the role as indispensible. The exact nature of duties being undertaken by Care Coordinators appears to vary somewhat across locations and settings. For example, there is variation in the type and amount of clinical duties being undertaken. It is understood that Care Coordinators undertake a broad range of activities, depending on the location and setting in which they work. Examples of work being undertaken by Care Coordinators provided during consultations include: public health and organisational or systems-focused activities, such as:
- educating community members about outbreaks of diseases and appropriate medication use;
- developing tools for better information sharing; and- improving the cultural competency of local providers;
assisting individual patients, such as through:- identifying the needs of patients and families, including relevant social
determinants of health;- assisting with care planning;
168KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
- acting as a case manager or liaison point between different services for the patient, including assisting patients to transition between different programs or services;
- supporting patients by scheduling specialist appointments and accessing Supplementary Services funding to help pay for the specialist fee;
- reminding patients about their appointments prior to and on the day of the appointment;
- supporting patients to sign up for programs and services to support their chronic disease management; and
- assisting patients to access transport services available in the community.
The examples of activities provided by Care Coordinators to illustrate their role are not predominantly clinical in nature, even though Care Coordinators are required to have a clinical background. The requirement that Care Coordinators have a clinical background is to enable them to: understand the need for services in a patient’s care plan; operate in accordance with the treating doctor’s instructions; work with specialists, GPs, nurses and allied health professionals, and
negotiate with other service providers; be able identify patients who show signs of a deteriorating condition
between the scheduled times for review of their care plan, and encourage them to return to their GP; and
capture and share clinical information with relevant health care providers.189
Consultations to date indicate that Care Coordinators are using their clinical skills in respect of most of these activities, and particularly through their understanding of “medical jargon” when liaising between GPs and patients.
Awareness of Care Coordinators
Promotion of the CCSS program appears to occur primarily through the activities of the ICDP workforce, including Care Coordinators and ATSIOWs at a site level, and Indigenous Health Project Officers (IHPOs) more broadly as part of their role in promoting all ICDP measures. In consultations with Care Coordinators and their organisations, ATSIOWs were seen as useful in
189 Department of Health and Ageing 2010, Indigenous Chronic Disease Package, Care Coordination and Supplementary Services, Program Guidelines, April 2010, Department of Health and Ageing, Canberra, pp. 7-8, viewed 15 November.
169KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
supporting patient awareness of, and access to, the CCSS care coordination service. Consultations found that stakeholders have varying levels of understanding about the Care Coordinator’s role, and varying perspectives about the utility of this role. For instance, some stakeholders reported that the Care Coordinator role is duplicating existing care coordination mechanisms and that there is little demand for the service. Other stakeholders reported that care coordination is working very well and that the role of the Care Coordinator is essential to ensure chronic disease management for complex patients.The consultations undertaken with other primary health care providers indicate that where the Care Coordinators have been in their role for some time, the service is working effectively to support patients and improve chronic disease management, while recognising that, in most locations visited by the evaluators, the program was still in its infancy. One of the positive outcomes reported by health workers consulted during the evaluation was that patients who are working with a Care Coordinator seem to be more likely to attend their appointments. Consistent and reliable attendance at specialists and allied health appointments is likely to support better health outcomes for patients, and also to reduce waste within the health system through reducing ‘no shows’. Consultations with community members undertaken to date indicate that, while awareness of the role is still limited in most places, many Aboriginal and Torres Strait Islander patients are likely to value the Care Coordinator services. This is illustrated by people identifying concerns (real or perceived) that primary health care providers are often very busy and unable to dedicate sufficient time to engage with them in a way they would like. Concerns about difficulties managing transport to appointments and navigating the health care system were also frequently raised during consultations with community members, and these are also matters which Care Coordinators have the potential to address. 1.43 Supplementary Services funding As described in Table 45 above, the total number of individual patients to receive Supplementary Services funding in 2010-11 was 83. Data was not available on the type of services purchased through the Supplementary Services funding pool. While the rationale for the guidelines on the use of the Supplementary Services funding is clear, there have been reports of challenges operationalising the guidelines which hampered the implementation of this component of the measure in 2010-11.This finding is informed by program documentation, information provided by and consultation with the department; stakeholder feedback from Regional Forums; consultation with AGPN, fund holders, Care Coordinators and other
170KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
staff from organisations in which Care Coordinators are based (such as Team Leaders and CEOs); and the Sentinel Sites Evaluation Report.190 Consistency with the guidelines
The CCSS Guidelines were released by the department in April 2010. A Frequently Asked Questions document was released in November 2011 to provide further clarification.191 The program guidelines provide that Supplementary Services funds can be used to expedite a patient’s access to specialist and allied health services in accordance with their care plan, where a delay to access a publicly funded provider creates a clinical risk. It also allows the funds to assist with the cost of transport to health care services.192 Specifically relating to paying appointments, the guidelines state that “Supplementary service funds may be used to directly pay fees for services by allied health providers (where MBS rebates are not available), or to meet the difference between MBS rebates and fees charged by private specialists or allied health providers”. In some areas, it may be reasonable to pay providers a retainer for making urgent appointments available to care coordination patients or for undertaking sessional work in a particular location. “Panels” of preferred providers and organisations that provide services in a culturally safe way may also be established at the local level.193
The program guidelines note that the Supplementary Services funds are a limited resource and priority should be given to responding to urgent needs. While local arrangements for managing the funding pool may vary, the guidelines state that these need to accommodate rapid approval and access to the funds.194 These requirements were established to limit the Supplementary Services funding being used as an alternative to existing funding streams (i.e., to limit cost shifting).In some locations, advisory committees have been convened to consider allocation of Supplementary Services funding to ensure that best use is made
190 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.191 Department of Health and Ageing 2011, Care Coordination and Supplementary Services (CCSS) Program Frequently Asked Questions, Department of Health and Ageing, Canberra. 192 While the CCSS guidelines note that “The [Supplementary Services] funds may also be used to assist with the cost of local transport to health care appointments” (p. 2), the department notes that Supplementary Services funds can be used for transport outside the local area, where the service is not available locally in a clinically acceptable timeframe.193 Department of Health and Ageing 2010, Indigenous Chronic Disease Package, Care Coordination and Supplementary Services, Program Guidelines, April 2010, Department of Health and Ageing, Canberra, pp.10-11, viewed 15 November 2012.194 Department of Health and Ageing 2010, Indigenous Chronic Disease Package, Care Coordination and Supplementary Services, Program Guidelines, April 2010, Department of Health and Ageing, Canberra, pp.10 11, viewed 15 November 2012.
171KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
of the available resources. This may be particularly important in areas where the Urban Specialist Outreach Assistance Program (USOAP) and Medical Specialist Outreach Assistance Program – Indigenous Chronic Disease (MSOAP-ICD) measures are also operating, to ensure that all needs are met and there is no duplication or confusion across these measures. Consultations undertaken to date indicate that Supplementary Services funds are generally being expended in a manner which is consistent with the guidelines. This assessment is based on information provided to evaluators by the fund holders and does not represent an independent assessment of consistency in the use of these funds. While it appears that funds are generally used to meet the costs of specialist and allied health appointments, and to support travel to appointments, in some jurisdictions fund holders are making use of the option to fund sessional work in locations where access to particular services is especially limited. One example of this is funding a dentist to provide sessions in a remote area, where access to dental services is otherwise extremely limited. The Sentinel Sites Evaluation has suggested that stakeholders feel that the amount of funding is too low, that there may be confusion about eligibility criteria for what the funds can be used for, and that access to specialists in remote areas is a barrier to use of the Supplementary Services funds.195
Challenges
Stakeholders at the national, state and local levels consistently reported that the program guidelines for Supplementary Services funding are overly restrictive in not allowing the purchase of aids or equipment. The most commonly discussed reasons given were limited capacity to use funds to purchase disposable items (for example, dressings for wound care), for purchase or hire of equipment (for example, hire of continuous positive airway pressure or CPAP machines for patients with chronic respiratory illnesses) or to purchase aids to support chronic disease management (such as orthotics for diabetic patients). These stakeholders also considered that there were too many steps in the process required to access funds for permissible uses, when the need is often immediate. They noted that the conditions placed on the funds do not give detailed guidance on what items will be able to be funded, meaning that SBOs are required to spend time determining what existing services a patient can access before applying for Supplementary Services funding, and takes up time that Care Coordinators could otherwise be spending on care management. One of the main sources of frustration identified at Regional Forums was the need to ensure that Supplementary Services were not being allocated to
195 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
172KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
provide access to services already available through existing pathways. Stakeholders reported that sometimes services are available but may not be appropriate due to wait times. For example, organising patient transport through existing mechanisms often requires advanced notice to get approval from patient transport schemes. At times, it may be beneficial to facilitate access to transport funding quickly, however, stakeholders felt that the guidelines would prohibit doing so because an existing (although sub-optimal) mechanism is already in place. Finally, some stakeholders identified a common practical barrier to utilising Supplementary Services funds: when a patient cannot afford a co-payment for a health service, Supplementary Services funding can be used, however, the patient may be required to pay the full amount upfront and then apply for reimbursement. Stakeholders commented that some patients are not in a position to pay the full amount upfront and wait for reimbursement, and consequently they do not use the service. Stakeholders feel that both issues (limits on permissible uses, and the process to access funding for permissible uses) mean funding is not being used in a way that meets the objectives of the measure and respond to individual patient needs in a timely manner. Many of these challenges may have been addressed through the development and distribution of the Frequently Asked Questions document released in November 2011, or have been resolved as fund holders come to understand the guidelines and possible application of the funds. For example, the Program Guidelines state that “when barriers such as these exist, and a delay is clinically inappropriate, the coordinator may use the CCSS Program supplementary services funding to expedite the patient’s access to these services in the private sector.”1.44 Program supports The evaluation found that the program supports for this measure were operating effectively during 2010-11. The National Coordinator role was in place and valued by fund holders and Care Coordinators. This finding is informed by consultation with the department, AGPN, fund holders and Care Coordinators. The AGPN National Coordinator role commenced in May 2011 to ensure consistency and to build networks and linkages across the SBO fund holders, including standardisation of practice. SBOs report that the National Coordinator is a valuable resource, both to support the program at a strategic level, and to act as an advocate for the CCSS program. The AGPN has developed a number of supports for the CCSS Program. These include coordination of information sharing across the Care Coordinator network and setting up a clearinghouse of relevant resources (hosted on the
173KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
AGPN website). Development of a national database (MMex), which provides a minimum reporting data set for SBO reporting to the department, commenced during this period. 1.45 Facilitators and barriers The key facilitators and barriers to the implementation of the CCSS Program are set out below. It should be noted that Care Coordinator recruitment only commenced in 2010-11, and sufficient time may not have elapsed for all stakeholders to fully understand the program and its potential impact. Facilitators: Networks and organisational support. Having strong pre-existing
connections to local health care providers and community members, and working within a team of health care providers can be important facilitators for Care Coordinators. This includes working with other ICDP positions such as ATSIOWs, who can act as cultural brokers and provide complementary services such as transport. As a necessity, Care Coordinators must have good knowledge of the local primary health care system in their area in order to negotiate services for their patients. While models of care coordination will be investigated in further detail in the next stages of the evaluation, the currently available evidence indicates that care coordination works well when the Care Coordinator has a clearly defined role within a team of health care providers, including ATSIOWs, GPs, and specialists.
Trusted relationships with the Aboriginal and Torres Strait Islander community. Relationships with community members are important, as the Care Coordinator role relies on a level of trust from the patient. Care Coordinators have also found it beneficial to involve Aboriginal and Torres Strait Islander family members in the patient journey.
National Coordinator and workforce support. Care Coordinators have valued the access they now have to a range of program supports. In addition to support provided at the state and territory level by the fund holders, funding is also provided for a national coordinator. This role is valued by Care Coordinators and fund holders as a means to enhance the role of Care Coordinators.
Coordination with other ICDP activity. Care Coordinators working with other ICDP positions such as ATSIOWs and IHPOs appears to enhance awareness of and access to the CCSS Program. As these ICDP workforce elements are new, all are still evolving as are their networks, organisational relationships and referral mechanisms. Coordination should continue to strengthen in future years, as the roles, services and organisations work through operational elements including interaction with each other and other parts of the existing service system.
174KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Barriers: Recruitment of Care Coordinators in rural and remote locations. The
requirement that Care Coordinators have a clinical background may limit the pool of potential candidates. Recruitment to the Care Coordinator position has been difficult in the Northern Territory and, to a lesser extent, Queensland. Some expectations of the role, such as the need to build professional networks, establish referral pathways and develop referral tools, were reported to be challenging by some Care Coordinators and may impact on retention in the role. These barriers may be reduced through support from the National Coordinator in the AGPN and the department. For example, national promotion of positions vacant across jurisdictions, sharing what works between Care Coordinators, tool templates and networking opportunities, could increase the confidence, capabilities and retention of Care Coordinators.
Supplementary Services funds. Feedback received from the majority of stakeholders suggests that the permitted uses for the Supplementary Services funds are not broad enough to facilitate the care coordination needs that are being identified through the work of the Care Coordinators. Chiefly, this relates to the need for medical aids and equipment for chronic disease patients, particularly when this is required urgently. These items cannot be covered by the Supplementary Services funds under the program guidelines. For uses that can be covered under the Supplementary Services funding, the approval processes can be a barrier – such as where the Care Coordinator must explore all alternative funding sources before accessing the funds, which creates delays; or where the patient must cover upfront costs and seek reimbursement. As a result, patient needs may not be met in a timely way, program funds may go unspent, and fund holders may continue to be frustrated by the constraints. While this issue was widely reported by a variety of stakeholders in numerous settings, it was not universally identified, which indicates that some fund holders may have managed to work with the existing guidelines in a way which is satisfactory to both providers and patients. A balance will need to be struck between preventing substitution and enabling uses in line with the objectives of the measure.
1.46 OpportunitiesThe primary opportunities for strengthening the implementation of the CCSS Program measure in future years are: Continue to monitor concerns about the Program Guidelines in relation to
Supplementary Services funds, and consider activities to complement the Frequently Asked Questions document such as developing a mechanism for fund holders to share learnings.
175KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Sharing resources, examples, templates and tools across the Care Coordinator network that support the establishment of the care coordination model, referral pathways and service networks. This could better equip new workers to progress developmental work and gain traction quickly.
Ensure that all potential linkages between relevant ICDP measures and the CCSS program are optimised. The evaluation found that ATSIOWs and Care Coordinators are already working together in many places, and also link with other ICDP measures such as the PBS co-payment measure and PIP Indigenous Health Incentive. These connections should be recognised and encouraged through communication from the department, the National Coordinator and NACCHO.
176KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Case Study: Factors impacting access to the CCSS programCare coordination is an important activity in the complex realm of the healthcare system. Care Coordination elicits the idea that clients will experience a supportive patient journey, including care planning for their complex care needs, seamless and timely care delivery between multiple providers, and assistance with self-management. It is clear from organisational literature that care coordination is not a single type of service, and that there are different models of care coordination that may be effective depending on the delivery context. This fact appears to be acknowledged by the department’s CCSS program guidelines196, which offer broad guidance and flexibility for the establishment and delivery of Care Coordinator services. Accordingly, as fund holders for the CCSS program, the Divisions of General Practice Network’s SBOs have taken a variety of approaches to implementation. This has resulted in different service delivery models – for instance delivery through IHSs, Divisions or general practices, with part-time or full-time Care Coordinators, and a range of approaches to professional networking. There have been varying degrees of uptake of CCSS, particularly Supplementary Services funding. In some areas, Supplementary Services funding is being widely applied and in others there has been little or no use of the available resource. The variation in program delivery is perhaps exacerbated in this early stage of the CCSS program, where pre-established structures and relationships have largely determined what implementation looks like. 1.47 Purpose and scope of the case study The purpose of this case study is to examine the factors that influence patients’ access to the CCSS program, including services of Care Coordinators and use of Supplementary Services funding. A number of sub-questions were also identified, and are addressed in section 1.49. In addition to information gathered during the course of the evaluation, some additional interviews have been undertaken with Care Coordinators, primary health care providers, Divisions and SBOs to inform this case study.This case study presents three vignettes that discuss the concept of access from the perspectives of Care Coordinators in the mainstream and IHS sector
196 Department of Health and Ageing 2010, Indigenous Chronic Disease Package, Care Coordination and Supplementary Services, Program Guidelines, April 2010, Department of Health and Ageing, Canberra, viewed 15 November.
177KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
experience in the CCSS program is significantly mediated by these widely differing contexts. Here, two vignettes are dedicated to the experience of the mainstream, where it is apparent that the placement and role of the Care Coordinator can mediate how the program and funds are accessed.These vignettes are composite examples which have been developed from the experience of CCSS implementation in multiple locations, including from the perspective of Care Coordinators, GPs, Practice Managers and other stakeholders.1.48 VignettesVignette 1: CCSS in an IHSShirley197 has worked as a Care Coordinator at the Inner Regional Aboriginal Medical Service (IRAMS) for the past year, where she previously worked as a Practice Nurse. IRAMS serves over 900 Aboriginal and Torres Strait Islander patients at a single location. She enjoys her job and thinks of it as helping patients navigate the health maze. Shirley has not had any trouble getting referrals for patients who need her help. If anything, Shirley is feeling pinched by the time needed to attend to all of their needs. Her caseload is 57 patients, all of them from IRAMS. IRAMS’ three GPs are well acquainted with Shirley’s role in chronic disease care coordination. When they have identified a patient in need, they call Shirley from down the hall or email her to let her know that they have a referral in mind. Some patients need more intensive services that require consultation with other providers. In a flurry of activity, Shirley arranges for patients to attend a series of appointments with specialists and allied health providers. It is convenient that IRAMS has a diabetes clinic and visiting providers including a dietician and dermatologist. Shirley has good relationships with a handful of other specialists where she regularly connects patients; several of these specialists are willing to bulk bill for IRAMS patients which allows Shirley to save the Supplementary Services money she’d otherwise use for gap fees. In other cases, Shirley’s patients are not using a lot of health care services, but still have pressing needs that impact their quality of life. Many of her patients cannot afford to pay for things like glasses, wound dressings, incontinence pads, walking aids, orthotic inserts and certain medications and vitamins not under PBS. These expenses cannot be covered by the Supplementary Services funding and even where other sources of funding are available it can often take months to receive the equipment. Shirley feels frustrated and disheartened when she cannot help patients with these simple needs. 197 Practices and individuals referred to in the case study are not actual practices and people.
178KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
On the whole, Shirley has been quite resourceful in leveraging other options for supporting patients. Lately, she has successfully convinced another specialist to bulk bill, thus avoiding embarrassment (‘shame’) for her patients who are uncomfortable asking for this themselves. She accesses a number of state-run programs for funding and services. She uses the resources and supports that she can muster, and Supplementary Services funds are a last resort. Shirley’s role is fully integrated into the ongoing work of IRAMS where patient care is a team effort. She participates in weekly case conferencing with the practice staff to discuss her patients’ needs and she has access to all patient files. She provides self-management counselling in conjunction with other staff. With support from the AHWs and Outreach Worker she has maintained a close connection with the local Aboriginal and Torres Strait Islander community – most of whom, she thinks, would access IRAMS more often than the local general practices. Shirley recognises though, that even with this web of supports, IRAMS is still only touching the ‘tip of the iceberg’ when it comes to patient needs. Her patient caseload does not even match the 75 patients at IRAMS with diabetes, not to mention a whole lot more on their chronic disease register. There are other patients who need her services that do not currently qualify, such as patients under the age of 15 with diabetes. With different eligibility criteria, she is convinced that many others could benefit from the CCSS program.
Discussion of vignette 1
This vignette highlights a number of factors that impact access to the CCSS program within the context of an inner regional IHS. Most importantly, it is clear that Care Coordinators working in IHSs have roles that are aligned with existing services. In this environment, the Care Coordinator provides additional service capacity and coordination for patients who have complex needs. Similarly, Supplementary Services provides an additional stream of funding that is most valuable for accessing specialist services. Care Coordinators cannot access the Supplementary Services funds until they have exhausted all other funding options (and so long as any delay is not going to have a negative impact on the clients’ clinical outcome), nor can they use the funds for equipment and materials that patients need. In this example, the Care Coordinator role has been absorbed into the organisation and into the existing model of care. The Care Coordinator works closely with GPs and other practice staff who are dedicated to serving Aboriginal and Torres Strait Islander clients. The Care Coordinators have existing relationships with other providers and community members, and have
179KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
a clear understanding of the context of patients’ lives, the type of support they need and the local service system. Vignette 2: CCSS in a DoGP Deborah has been working as a Care Coordinator for the (inner regional) South Bank Division of General Practice (SBDGP) for six months, and was born and raised in the area. She is a member of SBDGP’s ‘Closing the Gap’ team, which includes another Care Coordinator, an IHPO, and an ATSIOW. Deborah is a registered nurse and wants to help Aboriginal people with chronic disease to get the care that they need. It is fortunate that Deborah has had the support of her Closing the Gap team. When she started this job, Deborah felt like she was climbing a sheer cliff in order to establish promotional materials, develop referral pathways, and beg time to speak about CCSS with Practice Managers and GPs. Early on, it felt like she was not getting traction. Not only did it take two months to get her first referrals from general practices, she also tried without success to get engagement of a local IHS. Meanwhile, the other Care Coordinator on her team used an established relationship with a local IHS to develop a significant and growing caseload. Waiting for a GP referral clearly was not working for Deborah, so she decided to change her tactics. Enlisting support from the ATSIOW, Deborah began promoting the CCSS program at Aboriginal community events and community programs. She also visited the hospital where she asked the Aboriginal Liaison Officer and staff at the chronic disease management program to provide CCSS program information to clients that have been admitted more than twice in six months. Deborah checks in with these staff regularly so that they can get to know her and her services. Through these efforts, Deborah began accumulating interested community members for the CCSS program. Unfortunately, she has not been able to help those patients attached to the local IHS. For the others, she arranged appointments and accompanied these patients to visit their GP, where she provided the GP with a referral form awaiting their signature. GPs have been satisfied with this approach and the vast majority in the area are already registered for the PIP Indigenous Health Incentive – one practice has even signed on to the incentive program since they learned about the benefits of Supplementary Services funding. Practices have been prompted to update their care planning in order to meet CCSS requirements and have been able to claim the MBS item to do so. Deborah has achieved good results with her caseload of 16 patients. She is especially proud of the outcomes she has recently achieved with a patient who has just been released from jail. He is a widower with two teenage children, has diabetes, no car and lives a $90 taxi ride from the nearest town
180KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
to access primary health care. He was having difficulty getting the right payment from Centrelink and had no savings. Deborah arranged a series of GP and specialist appointments for him over a few weeks, provided him with an appointment calendar and arranged all of his transportation. She was also able to assist in identifying health issues with his children, who have had health checks, dental work and receive home help funded through the state. Deborah cannot turn a blind eye to client circumstances and does her best to use all available services and funding to meet these basic needs. Most often, Deborah uses Supplementary Services to pay specialist consultation and gap fees. She does not mind applying a little pressure to the ‘heart strings’ to get specialists to bulk bill describing client circumstances usually helps. Supplementary Services has been very useful for transportation too, but Deborah feels that it falls short when it comes to equipment. Deborah feels responsible for her patients, and feels that she is letting them down when she cannot help with something simple that could keep them out of the hospital – like a commode chair for an amputee, or a CPAP machine needed for breathing therapy. She would also like to be able to use Supplementary Services funding for surgeries that her patients cannot afford.Deborah still struggles enlisting the interest of general practices. This is despite the fact that more than 80 per cent of accredited practices in the area are signed on to the PIP Indigenous Health Incentive. She believes that Practice Managers have sometimes been a barrier, noting that some refuse to bulk bill for any patients, have not displayed promotional posters or literature within their practice, and do not have effective self-identification systems (some Practice Managers think that they can identify an Aboriginal or Torres Strait Islander person by their appearance). Some have been unsure about sharing private patient information with Deborah. In her visits to practices, Deborah has learned that some do not like how the CCSS caters only to Aboriginal and Torres Strait Islander people, and in a few cases she has encountered attitudes that are, in her opinion, downright racist. But even with these barriers, Deborah sees the CCSS program as successful. She is just keeping up with the demands of her current caseload, and recognises that the community needs are much greater than what the Closing the Gap team can offer.
Discussion of vignette 2
This vignette highlights the difficulty that some Care Coordinators in Divisions can face in gaining GP engagement. While the CCSS program guidelines describe a referral pathway that starts with the GP, in reality, Care Coordinators have used all manner of strategies to identify patients – both through GPs (referred to by some Care Coordinators as the ‘top down’
181KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
approach to patient recruitment) and by identifying patients in the community (the ‘bottom up’ approach). In the context of a Division, other ICDP workers play a vital role in supporting the Care Coordinator. This includes collegiality and shared workload with other Care Coordinators. ATSIOWs play an important role in identifying community members for the CCSS program and supporting patient appointments. The IHPO provides support with engaging mainstream practices overall. While not discussed in this case study vignette, state-level Care Coordinator networking has been important in launching the program in some locations, by connecting the CCSS to other related initiatives and supporting best practice and professional development. All of these background elements are critical in establishing and maintaining an accessible CCSS program. Vignette 3: CCSS in a General PracticeFor five years, Grace has been a full time Practice Nurse for the Nearby Medical Clinic (NMC), a general practice in an outer regional area. About six months ago, she added ‘Care Coordinator’ to her title. That was when the NMC received ICDP funding through the DoGP for the CCSS program. Grace’s position is now funded under this program for one day each week. In her role as a Care Coordinator, Grace sees patients who have been identified as Aboriginal or Torres Strait Islander and who need chronic disease care. NMC established a process to identify existing patients as part of the PIP Indigenous Health Incentive. Fifty patients are registered with the PIP Indigenous Health Incentive, and Grace sees about 10 of these as a Care Coordinator. Grace’s role is to provide health assessments, care planning, and other clinical services for chronic disease management. These are billed through MBS to generate income for the practice. It is easy for the GPs at NMC to refer patients to Grace. In fact, none of the communication channels in the practice have really changed and the GPs do not distinguish between her role as a Practice Nurse and as a Care Coordinator. Grace does not see too much difference in her role either; she is just able to give extra attention to a certain group of patients. It has been helpful for Grace to attend the Care Coordinator training provided by both the Division and the SBO to better understand her role. She keeps in touch with other Care Coordinators she met at the training to discuss some common issues. One of the main areas of frustration they have discussed is the Supplementary Services funding. Grace has not used the Supplementary Services funding very much. She finds it too time consuming and involved – it means a lot of communication with the service provider to convince them to bulk bill and accept cheques. On top of this she then has to calculate costs, organise the patient’s attendance and
182KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
send payments. She has gone down this road to get access to dental health and allied health services. Still, it makes her wonder whether the fees process could be automated somehow. At the NMC, the main benefit of the CCSS program has increased capacity to deliver services that trigger payments through the PIP Indigenous Health Incentive. Without the dedicated help of the Care Coordinator, practitioners at the NMC would not have the time to deliver care necessary for outcomes payments. The practice recognises that they have lost one day of Grace’s time for other Practice Nurse duties but for now the payoffs are enough to stick with this model.
Discussion of vignette 3
The story of the NMC presents a model whereby the SBO has subcontracted the CCSS program to a DoGP, which has in turn developed a model that funds care coordination services from within a general practice registered for the PIP Indigenous Health Incentive. In practical terms, this means funding a portion of an existing nursing position to provide care coordination. This model ensures an accessible clinical space where Care Coordinators have good access to clients and can regularly see patients. An embedded Care Coordinator/s provides additional capacity to support better practice care, and supports participation in the PIP Indigenous Health Incentive. 1.49 Summary of findingsThis case study provides insight into the factors that constrain and support access to the CCSS program. The vignettes provided in this case study demonstrate the factors that are most important in different contexts – in an IHS, a Division and a general practice. Responses to the sub-questions are provided below:1. What factors constrain access to care coordinators?
As shown by the three vignettes in this case study, there are a number of factors that determine access to the CCSS program. Firstly, the model of CCSS service delivery depends on subcontracting arrangements made by SBO fund holders. In some cases, they have subcontracted directly with IHSs. In other cases, they have subcontracted Divisions which then make arrangements to share the services of Care Coordinators with IHSs. In other instances, the relationships between the IHS sector and Divisions have limited resource sharing. In each case, the model of service delivery determines which patients (those using mainstream services and/or those using IHS services) will have access to CCSS at the funded location.
183KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
CCSS referrals rely on trusting relationships between GPs and Care Coordinators. This is most supported in cases where the Care Coordinator is an embedded part of the clinic environment (as in vignettes 1 and 3). Where Care Coordinators are outside of this structure, they expend significant effort to engage general practices that impacts on the number of patients they can manage.Community engagement is a significant part of patient recruitment. Here, Care Coordinators benefit from a pre-existing relationship with the Aboriginal and Torres Strait Islander community or assistance from an Outreach Worker or AHW. Care Coordinator networks and supports are vital in supporting the CCSS program, thereby boosting capacity and patient access. This includes state level training workshops, the support of other ICDP workers, and clinic-level teamwork in case conferencing patients. Care Coordinators have noted restrictions in program guidelines that limit access to the CCSS. The PIP Indigenous Health Incentive guidelines restrict participation to those aged 15 years and over with a diagnosed chronic disease. Care Coordinators note that this divides Aboriginal and Torres Strait Islander family members – those who can receive services and those that cannot. Clearly, many patients are at high risk for chronic disease and are ‘waiting’ for diagnosis, while children under the age of 15 may also have chronic diseases. As well, only accredited practices can participate in the PIP Indigenous Health Incentive, so patients attached to non-accredited practices cannot access CCSS.
2. Does the requirement to be a PIP Indigenous Health Incentive registered practice work as a barrier to referrals to care coordinators?
This case study has not included the perspective of non-registered practices. Where Care Coordinators are embedded within one practice (IHS or general practice), external referrals are not relevant. Care Coordinators working at the Division level have indicated that they have not received referrals from non-registered practices. In this context, Care Coordinators are expending their efforts engaging with registered practices only. From their perspective, the pool of registered practices is more than enough to occupy their available service capacity.
3. To what extent do practices understand the referral mechanisms and the role of care coordinators?
Again, this question is only relevant where Care Coordinators are located at a Division. An understanding of the referral process itself does not appear to be a barrier to accessing the CCSS program; rather it is the capacity or
184KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
willingness to activate the referral process that may potentially inhibit referrals. GPs do not believe that the referral process is onerous; it simply takes a couple of extra steps for paperwork and communication.
4. What information is provided by practices to care coordinators when a patient is referred? How adequate are the referrals and the care plans for referred patients?
Care Coordinators situated in general practices or IHSs automatically have full access to the required patient information. Information exchange, both through care plans and less formally, is generally very good, and supported by a professional relationship between the Care Coordinator and GP. For Care Coordinators located in Divisions, accessing patient information can at times prove more challenging. Many referring practices are prepared to provide a care plan, and generally agree to update this for the purpose of ensuring the referral is appropriate and informative. In areas where Care Coordinators are struggling for GP referrals, some Care Coordinators with suitable skills may offer to prepare the care plan and provide it for GP approval (and to facilitate MBS billing). Some practices have expressed concern about management of private patient information within the referral process, and while this does not appear to be a significant barrier to participation, it may have a negative impact on the adequacy of referrals.
5. To what extent do care coordinators get referrals from non PIP Indigenous Health Incentive registered practices and if frequent, are there differences in the quality of referral compared to registered practices?
As per (2) above, Care Coordinators have not received referrals from practices that are not registered for the PIP Indigenous Health Incentive.
6. What strategies have fund-holders used to increase awareness of the measure among the primary health care services particularly of the supplementary services funding?
Most awareness raising occurs at the local level, where Divisions and Care Coordinators have played roles in increasing awareness of the CCSS among primary health care services. In the mainstream sector, much of the interaction with practices occurs through the combined efforts of the ‘Closing the Gap’ teams (ICDP-funded workers located in Divisions), and sometimes through practice support teams. Care Coordinators are active in visiting practices to inform staff about the CCSS program. Care Coordinators have indicated that Practice Managers are gatekeepers for GP engagement, and that their attitude or receptivity can determine whether the GP receives information about the CCSS Program. From their perspective, GPs feel that they receive a huge volume
185KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
of information about different programs, and they cannot make effective use of them all. Unsurprisingly, effective engagement appears to occur where there are existing relationships, receptivity to better practice approaches to care delivery, and capacity to participate.
7. How are supplementary services funds being used?
Most often, it appears that Supplementary Services funding is being used to access specialist care – either to pay consultation fees upfront, or gap fees. Care Coordinators have also indicated that they purchase allied health care services. This may include the purchase of sessions or a retainer fee for a regular schedule of care delivery. In at least one state, Divisions are required by the SBO to set up a Supplementary Services reference group (composed of clinical and non-clinical members) to decide on appropriate use of the funds. In their decision making, they consider principles including clinical appropriateness, contribution to self-management and equity.
8. Are fund holders brokering instead of/in addition to accessing supplementary services funding? If so why and how?
As found for this case study, Care Coordinators are diligent in meeting the program guidelines requirement that Supplementary Services should be accessed if no other funds are available in a clinically appropriate timeframe. To this end, Care Coordinators advocate for bulk billing by specialists and allied health providers, connect their patients to public providers, and access state funding where this is available.
9. What are the barriers to the use of the supplementary services funds?
Supplementary Services funding guidelines are considered by many to be overly restrictive, particularly in excluding the purchase of low cost medical aides and equipment. Another barrier is the requirement to use other sources of funding in the first instance (unless any potential delay is deemed to be clinically inappropriate). Where other sources of funding are available, the low use of Supplementary Services funds could give the mistaken impression that Care Coordinators are not meeting patient needs. Finally, depending on local relationships and processes, Care Coordinators have varying levels of administrative requirements to access and pay for services using Supplementary Services funds. These requirements can occupy a significant amount of a Care Coordinator’s time.
186KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Improving Indigenous Participation in Health Care through Chronic Disease Self Management (B4)This chapter describes the progress of the Improving Indigenous Participation in Health Care through Chronic Disease Self Management measure (referred to hereafter as the chronic disease self management measure). In this chapter we discuss the implementation of this measure in 2010-11, the second year of the ICDP, including findings against activities, outputs and expected results as described in the Evaluation Framework, and barriers, facilitators and opportunities identified to date. Chronic Disease Self Management (CDSM) measure at a glanceThe evaluation found that the implementation of the measure in 2010-11 is ahead of schedule in terms of the delivery of training to health professionals, although there was an uneven spread across the country in terms of the locations where training was held. The very limited consultations with workers trained in CDSM, and community members, suggest that workers are likely to see the training as useful, and patients will probably value this type of service. However, empirical findings on the impact of the training for participants and patients are not able to be made, due to limited data collected on the measure. The department is working with Flinders University to support and record the delivery of CDSM sessions by trained staff through employer organisations.The department has set a total target for 400 health care professionals to receive the Flinders University training through the ICDP. Training targets were significantly exceeded in the 2010-2011 year with a total of 202 workers trained against a target of 57 for the year, across 13 locations in Australia. The Puntukurnu Aboriginal Remote Project commenced in the Kimberley and Pilbara regions of Western Australia in this financial year, with the participation of five small, remote IHSs. The expenditure on the measure in 2010-11 was $2.962 million.Having undertaken the CDSM support training, the trained workforce is expected to deliver around 50,000 hours of appropriately designed support sessions or activities to Aboriginal and Torres Strait Islander clients over three years (2010-11 to 2012-13). However, at the time of reporting, the number of CDSM sessions delivered to patients by clinicians trained in CDSM has not been reported.The key barrier and opportunity for this measure is to improve data collection and reporting to inform its ongoing implementation, continuous improvement and evaluation in future years.
187KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.50 Potential effects based on implementation findingsFigure 18 below is the causal pathway for the Chronic Disease Self Management measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
Chronic Disease Self Management
Health care professionals have capability to deliver CDSM sessions to
Aboriginal and Torres Strait
Islander patients
Improvements in patients’ self
management of their chronic
diseases
Improvements in relevant chronic disease clinical
indicators
Aboriginal and Torres Strait
Islander patients have adequate supports to self
manage
Primary health care practices
support staff to deliver CDSM and to view patients
as partners
CDSM is integrated into Aboriginal and Torres Strait
Islander patients’ care
Aboriginal and Torres Strait
Islander patients have capability
and willingness to self manage
CDSM training is appropriate and effective
Figure 18: Chronic Disease Self-Management causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect198 and the observed impacts.199 Both the plausibility and observed
198 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.
188KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
impacts of the measures can be influenced by contextual factors, which are also identified in the tables below.
199 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
189KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 46 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the CDSM measure and it was implemented according to plan in 2010-11. There is an indication that one of the key dependencies requires attention to ensure that trained health workers and clinicians are able to apply their training, namely, organisation support and commitment to the application of CDSM. Consultations suggested that some trainees have been constrained in applying CDSM training in their day-to-day role due to workload pressure arising from the considerable demand for acute care, and time constraints to apply all aspects of the CDSM with patients (these include time constraints for both the provider patients).Table 46: Assessment of key dependencies of the B4 measure.
Key dependencies
Findings Evidence
Chronic Disease Self Management (CDSM) training is appropriate and effective
The training program is based on model that has been in operation for some time prior to the ICDP. This training program was adapted based on consultations with a range of stakeholders to ensure that training meets the needs of health professionals working with Aboriginal and Torres Strait Islander people.Flinders University note that aspects of content and method of training need to be further adapted to ensure relevance of training and applicability of CDSM tools (used by providers with patients).
This is based on analysis of measure documentation, and consultations with Flinders University staff involved in the delivery of the training
Patients are selected to receive CDSM session
Data is not available for the First Monitoring Report.
Not applicable
Patients have capability and willingness to self manage
Data is not available for the First Monitoring Report.
Not applicable
Patients have adequate support to self manage
Data is not available for the First Monitoring Report.
Not applicable
190KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Primary health care organisations support trained staff to deliver CDSM and view patients as partners
Consultations suggested that some trainees have been constrained in applying CDSM training through their care delivery due to workload pressure arising from the considerable demand for acute care, and time constraints to apply all aspects of the CDSM with patients (these include time constraints for both the provider patients).
This is based on qualitative information; consultations with Flinders University staff involved in the delivery of the training (who have followed up with some trainees on an ad-hoc basis)
Contextual considerations
Organisational capacity and commitment to support the application of CDSM is likely to vary and this could lead to variation in the impact of the measure. The plausibility of effect may be diminished depending on the extent to which trainees are constrained by factors which limit their capacity to apply CDSM within their usual setting, and the level of support they receive from their employer/organisation to implement a CDSM based approach.
This is based on literature and information provided by Flinders University staff involved in the delivery of the training
Table 47 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). The evaluation is not able to measure change in the expected impacts. The key contextual factor influencing the measure in 2010-11 is the accessibility of training across different geographical locations.
191KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 47: Assessment of expected and observed impacts of the B4 measure based on implementation progress.
Expected Observed impacts EvidenceHealth care professionals have acquired the capability to deliver CDSM session to Aboriginal and Torres Strait Islander patients
All trainees have been awarded a certificate that now allows them to apply CDSM. Trainees’ feedback information not yet available for evaluation use.
This is based on analysis of measure documentation
Patient’s have improved their self management
Data is not available for the First Monitoring Report.
Not applicable
Relevant chronic disease risk factors have improved
Data is not available for the First Monitoring Report.
Not applicable
Contextual considerations
Accessibility of the training across locations is likely to impact on its uptake. In 2010-11 there was an uneven spread across the country in terms of the locations where training was held.
This is based on analysis of measure documentation
1.51 Measure overviewThe CDSM measure provides CDSM training for health workers to deliver self management sessions to empower Aboriginal and Torres Strait Islander patients with a chronic disease to actively participate in the management of their disease. Chronic disease self management educates patients in how to become active in the management of their own chronic disease. Flinders University is funded to provide the training to primary health care workers including AHWs, GPs, Registered Nurses, Care Coordinators and allied health professionals who deliver health services to Aboriginal and Torres Strait Islander people with chronic disease. Training ranges in time from 1.5 days (for GPs and practice nurses) to four days (for AHWs and allied health professionals).
192KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Flinders University has been funded to provide additional support to the Puntukurnu Aboriginal Remote Project in Western Australia, which will ensure staff at five IHSs receive CDSM training and, in turn, the staff will train their Aboriginal and Torres Strait Islander patients to actively participate in the management of their own chronic diseases. The department funded this project as a means to trial and support the application of self management training in remote settings.Further detail on the measure is given in the Baseline Report.200 In 2010-11, the total expenditure on the measure was $2.692 million.201
1.52 Chronic condition self management trainingChronic Disease Self Management training and sessions
The evaluation found that the measure is ahead of its target in terms of the delivery of training to health professionals, although there was an uneven spread across the country in terms of the locations where training was held. While limited emerging evidence suggests that health professionals and Aboriginal and Torres Strait Islander patients may be interested in gaining the skills of chronic disease self management, the impact of the training on participants’ practice and patient outcomes cannot be empirically assessed at this stage. These findings are based on information provided by the department, consultations with two participants and community focus groups. The department has set a target for 400 health care professionals to receive the Flinders University training through the ICDP. While training targets were not met within the 2009-10 year, they were significantly exceeded in the 2010-11 year, as illustrated in Table 48 below. Table 48: Number of health services providers trained in Flinders CDSM, target and actual.202
Indicator NumberTarget trained by 30 June 2011 57Actual trained to 31 August 2011 102
Four of the health workers trained have also completed the training to become accredited “Closing the Gap” CDSM trainers.203 Training was conducted in 13 200 KPMG 2013, Indigenous Chronic Disease Package National Monitoring and Evaluation Project: Baseline Report, Australian Government Department of Health and Ageing, Canberra.201 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [B4response].202 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [B4response].203 ibid.
193KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
locations across Australia in 2010-11, as shown in Table 49 below. Training was predominantly held in regional locations. No training sessions were held in Tasmania or the Australian Capital Territory. Training was conducted in Western Australia under the Puntukurnu Aboriginal Remote Project.Table 49: Location of Flinders CDSM training, by jurisdiction, to 31 August 2011.204
State/Territory Location of training Number of health professionals trained in CDSM
NSW Sydney 15QLD Cairns
IpswichYarrabah
51
WA - 0NT Alice Springs
Darwin23
VIC BendigoMilduraSwan Hill
75
SA AdelaideCedunaCoober PedyPort Augusta
38
TAS - 0ACT - 0Total N/A 202
Data is not available to identify whether these training recipients are employed in mainstream services or IHSs. Having undertaken the CDSM support training, the trained workforce is expected to deliver around 50,000 hours of appropriately designed support sessions or activities to Aboriginal and Torres Strait Islander clients over three years (2010-11 to 2012-13). At the time of reporting, the number of CDSM sessions delivered to patients by clinicians trained in CDSM has not been reported. The department is working with Flinders University to support and
204 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [B4response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
194KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
record the delivery of CDSM sessions by trained staff through employer organisations.205 In 2010-2011, the Puntukurnu Aboriginal Remote Project commenced in the Kimberley and Pilbara regions of Western Australia, with the participation of five, small remote health services that do not generally have access to new programs: Beagle Bay, Bidyadanga, Balgo, Mulan and Billinluna. The model provides up to 20 hours of one-to-one support on a sessional basis for each patient over a 12 month period. Each service will identify patients on their Chronic Disease Register, aiming for a total of 600 patients in one year, and a total of 24,000 hours of individually tailored support over two years. The Puntukurnu Aboriginal Medical Service is responsible for the management of this project including the collection and reporting of activity data to the department. It will be evaluated through an evaluation conducted by the University of Western Australia. At the time of reporting, further information was not available on activity undertaken within this financial year, or outcomes achieved. In consultations to date, only two health workers had completed the CDSM training but both indicated they found it useful and expected to apply the learning in their role. In consultations with organisations such as Divisions of General Practice and National Aboriginal Community Controlled Organisation (NACCHO) affiliates to date, it has been difficult to elicit information on this measure due to their lack of awareness.
During some community focus groups, people commented on the importance of equipping individuals with the knowledge and skills to better manage their own health. One community member commented that many programs and services are time limited – “they come and go” – which was seen (by the group) to increase the importance of enhancing self management capacity. On the basis of consultations undertaken to date, it is not possible to say whether this view represents a broader community view; however, if it does, it is likely that these services will be highly valued by Aboriginal and Torres Strait Islander people. 1.53 Facilitators and barriers It is difficult to identify facilitators and barriers to the CDSM measure in a comprehensive manner at this stage, given the limited information available. However, the very limited consultations with workers trained in CDSM, and community members, suggest that workers are likely to see the training as useful, and community members will value this type of service. The limited capacity to track the reach and impact of CDSM sessions for patients is a barrier to monitoring, improving and evaluating this measure.
205 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [B4response].
195KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.54 OpportunitiesThe central opportunity for the CDSM measure identified to date is to enhance reporting to allow for continuous improvement of the measure, and a robust evaluation in future years. In particular, collection of data about the number of CDSM sessions provided to clients by health professionals trained in CDSM, and a way to assess the impact of those sessions, is needed.
196KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Urban Specialist Outreach Assistance Program (USOAP) (B5a)This chapter describes the progress of the Increasing Access to Specialist and Multidisciplinary Team Care (hereafter referred to as the Urban Specialist Outreach Assistance Program or USOAP measure). This measure funds the provision of outreach medical specialists to Aboriginal and Torres Strait Islander people in urban communities in need of such services.In this chapter, we discuss the implementation of this measure in 2010-11, the second year of the ICDP, including findings against activities, outputs and expected results described in the Evaluation Framework, and barriers, facilitators and opportunities identified to date. The USOAP measure at a glanceThe evaluation found that the USOAP was largely implemented as planned in line with a deliberately phased approach. There were significant increases both in the number of specialists participating and patients receiving specialist care through this measure, compared with 2009-10. A number of key achievements have been realised in 2010-11, in jurisdictions where the USOAP is operating, including engaging fund holders, contracting outreach service host organisations, recruiting a wide range of specialists and delivering services to almost 400 Aboriginal and Torres Strait Islander patients. There are no indications of difficulties in the operation of fund holding arrangements, or in adhering to program guidelines. The planned staggered implementation of the program means that services are not yet available in almost half the eligible jurisdictions, and this phasing has not completely overcome challenges in recruiting medical specialists to deliver the outreach services. The implementation of USOAP has been phased in over several years, with funding only available in New South Wales, Victoria, Queensland and Western Australia in 2010-11. Fund holders are to be engaged in the remaining eligible jurisdictions (the Australian Capital Territory, South Australia and Tasmania) in 2011-12. By the end of 2010-11, there were 34 outreach service host organisations contracted by USOAP fund holders, and at least 11 where services had commenced. Host organisations were most often IHSs or other community health services. Nineteen (19) specialists were participating in USOAP across the three jurisdictions, with medical specialties comprising paediatrics, endocrinology, dermatology, ophthalmology, cardiology, psychiatry, orthopaedic surgery, renal, and general practice. A total of 380 Aboriginal and Torres Strait Islander patients received USOAP services between 1 September 2010 and 31 August 2011.Some implementation delays have been experienced across jurisdictions despite the planned incremental implementation of USOAP. The delays
197KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
mostly relate to challenges in recruiting specialists. Contributing factors appeared to be fund holders’ lack of pre-existing relationships with urban service providers, insufficient remuneration to attract significant numbers of new specialists to provide an outreach service, and the restriction of the measure to the use of specialist providers only (noting that the Medical Specialist Outreach Assistance Program – Indigenous Chronic Disease (MSOAP-ICD) B5b measure includes multidisciplinary health outreach). It is not clear whether service uptake reflects the full extent of referrals and whether actual USOAP service delivery reflects the availability (and preferences) of specialist service providers, or reflects priority community needs as identified in needs assessments undertaken by fund holders.The USOAP (B5a) and MSOAP-ICD (B5b) measures share the same objective and most of the same fund holders, which may create efficiency, collaboration or other synergies. The implementation of USOAP may benefit from improved coordination with other ICDP measures, such as support from the ICDP workforce, funding from the Supplementary Services fund for specialist follow up care, and referrals from practices registered for the PIP Indigenous Health Incentive. Other opportunities for the future include enhancing mechanisms to ensure that priority community needs have been assessed and that USOAP funding is being directed to meet those needs. Potential effects based on implementation findings Figure 19 below is the causal pathway for the USOAP measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
198KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Aboriginal and Torres Strait
Islander patients engage
with USOAP services
Aboriginal and Torres Strait
Islander patients receive
referrals to USOAP services
Service delivery sites are
appropriate and accessible
Outreach services
respond to identified
community health needs
Increasing Access to Specialist Care -
USOAP
Increase in care providers' cultural
awareness
Increase in urban health system
capacity to provide culturally
appropriate specialist outreach services for chronic
disease management
Improvement in patients’ access to a range of culturally
appropriate specialist outreach services for chronic
disease management
Increase in care providers'
knowledge, understanding and
skills
Improvement in Aboriginal and Torres Strait
Islander people’s chronic conditions
Recruitment and retention of outreach service
providers
Cultural awareness training is
appropriate and effective
Figure 19: USOAP causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility
199KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
of effect206 and the observed impacts.207 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. Table 50 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the USOAP measure. It was largely implemented according to plan in 2010-11, although there were some delays in the recruitment of relevant medical specialists. The evaluation is not able to determine whether all key dependencies are in place and in particular whether medical specialist providers underwent effective cultural awareness training and whether referral mechanisms are working optimally. Table 50: Assessment of key dependencies of the B5a measure.
Key dependencies
Findings Evidence
Recruitment and retention of outreach service providers
Recruitment of service providers was delayed. There were 19 specialists participating in USOAP across three jurisdictions in 2010-11. The staged implementation of the USOAP meant that services were not available in almost half the eligible jurisdictions in 2010-11.
This is based on data provided by the department
Cultural awareness training is appropriate and effective
Data is not available for the First Monitoring Report.
Not applicable
206 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.207 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
200KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Aboriginal and Torres Strait Islander patients receive referrals to USOAP services
Referral mechanisms appeared to be working effectively in many areas; however this appears to have been dependent on existing relationships and arrangements, which varied across locations.
This is based on qualitative information gathered from a small group of relevant stakeholders
Service delivery sites are appropriate and accessible
Data is not available for the First Monitoring Report.
Not applicable
Outreach services respond to identified community health needs
Community needs assessment and planning is a required component of the measure (and is undertaken by fund-holders). However, USOAP services in some cases are more reflective of the availability of service providers than of community needs.
This is based on qualitative information gathered from a small group of relevant stakeholders, and analysis of measure documentation
Aboriginal and Torres Strait Islander patients engage with USOAP services
19 specialists provided services to 380 Aboriginal and Torres Strait Islander patients in 2010-11. Not all jurisdictions funded for the measure provided services in this fiscal year.
This is based on data provided by the department on services provided through USOAP
201KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Contextual considerations
The location of service provision may influence engagement with USOAP services, given the importance of services being located in a culturally safe environment.208 209,210
It is likely that variable capacity to recruit providers across jurisdictions may also impact on the implementation of the program.
Literature review
Table 51 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). The evaluation is not able to measure change in the expected impacts, although 380 Aboriginal and Torres Strait Islander people received services from 19 medical specialists. Contextual factors that have the potential to influence the measure are the availability of GPs to make a referral and the preference of some patients to be seen in an IHS.Table 51: Assessment of expected and observed impacts of the B5a measure based on implementation progress.
Expected Observed impacts EvidenceIncrease in care providers’ cultural awareness
USOAP services providers are required to undergo cultural awareness training. No information is available to confirm the level and nature of training provided, or to assess the impact of this training.
This is based on consultations with the department and review of program guidelines
Increase in care providers’ knowledge, understanding and skills
Data is not available for the First Monitoring Report.
Not applicable
208 Northern Territory Government Department of Health and Families 2009 Revision of the Preventable Chronic Disease Strategy Background Paper: Preventable Chronic Disease in Aboriginal Populations, viewed September 2011.209 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project [C3 response]. 210 Hayman NE, White NE & Spurling GK 2009, ‘Improving Indigenous Patients’ access to mainstream health services: the Inala experience’, Medical Journal of Australia, vol. 190, no. 10, pp. 604-606.
202KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected Observed impacts EvidenceIncrease in urban system capacity to provider culturally appropriate specialist outreach services for chronic disease management
Data is not available for the First Monitoring Report whilst noting that 19 specialists provided services to 380 Aboriginal and Torres Strait Islander patients in 2010-11. Not all jurisdictions funded for the measure provided services in this fiscal year.
Not applicable
Improvement in patients’ access to a range of culturally appropriate specialist outreach services for chronic disease management
Data is not available for the First Monitoring Report whilst noting that 19 specialists provided services to 380 Aboriginal and Torres Strait Islander patients in 2010-11. Not all jurisdictions funded for the measure provided services in this fiscal year.
Not applicable
Improvement in Aboriginal and Torres Strait Islander people’s chronic conditions
Data is not available for the First Monitoring Report.
Not applicable
203KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected Observed impacts EvidenceContextual considerations
The extent to which referrals are supported by existing referral pathways, arrangements or informal relationships between services, is likely to impact on the number of referrals to (and thus access to) USOAP services. The availability and accessibility of existing specialist services may influence the need for outreach – consultations suggest that in areas with an IHS already providing such services, patients may be less in need of USOAP.Consultations also showed that the administrative capacity of organisations may influence their willingness and readiness to run USOAP clinics and the effectiveness (i.e., in terms of the coordination of patients, providers) of the services provided.
Qualitative information gathered from a small group of relevant stakeholders
1.55 Measure overviewThe Urban Specialist Outreach Assistance Program (USOAP) is one of two ICDP measures that provide outreach services. The USOAP provides cultural sensitive medical specialist outreach services that focus primarily on the management and treatment of chronic disease for Aboriginal and Torres Strait Islander people living in urban areas.211 The Medical Specialist Outreach Assistance Program – Indigenous Chronic Disease (MSOAP-ICD) (B5b) measure provides multidisciplinary health outreach services in rural and remote locations.212 Further detail on the measure is given in the Baseline Report.213
The implementation of USOAP has been phased in over several years, with funding only available in New South Wales, Victoria, Queensland and Western Australia in 2010-11. In 2010-11, the expenditure on USOAP was $0.798 million.1.56 Urban specialist outreach servicesThe evaluation found that the USOAP was largely implemented as planned in 2010-11, in line with a deliberately phased approach. There were significant
211 Urban areas are defined by reference to the Australian Standard Geographical Classification - Remoteness Area (ASGC-RA) 1 and 2.212 Rural and remote locations are defined by reference to the Australian Standard Geographical Classification - Remoteness Area (ASGC-RA) 2-5, with a focus on ASCG-RA 4 and 5.213 KPMG 2011, Indigenous Chronic Disease Package National Monitoring and Evaluation Project, Baseline Report, Department of Health and Ageing, Canberra.
204KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
increases both in the number of specialists participating and patients receiving specialist care through this measure, compared with 2009-10. However, the staged implementation of the USOAP means that services were not available in almost half the eligible jurisdictions in 2010-11, and this phasing has not overcome challenges in recruiting medical specialists to deliver the outreach services. While USOAP appears to be attracting patients, it is unclear whether service uptake reflects the full extent of referrals. Data is not available on the delivery or impact of cultural awareness training for providers involved in the USOAP.These findings have been informed by program documentation and data provided by the department, stakeholder feedback at Regional Forums, and consultation with the department and a selection of NACCHO affiliates, USOAP fund holders and host organisations. Fund holding and host organisation arrangements
As planned by the department, USOAP delivery continued throughout 2010-11 with the same fund holders that were engaged in 2009-10 in New South Wales, Western Australia and Victoria (rural workforce agencies) and in Queensland (the SBO). Fund holders are to be engaged in the remaining eligible jurisdictions (the Australian Capital Territory, South Australia and Tasmania) in 2011-12. The Northern Territory does not have areas classified as urban214 (the criteria for USOAP), and so is not eligible for inclusion in this measure. There are no indications of difficulties in the operation of fund holding arrangements. At 30 June 2011 there were 34 outreach service host organisations contracted by USOAP fund holders and 11 where services had commenced (refer Table 52 below). Host organisations are most often IHSs or other community health services.215
214 Using the Australian Standard Geographical Classification - Remoteness Area (ASGC-RA) 1 and 2.215 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, Urban Specialist Outreach Assistance Program, 2010-11 implementation [B5a response].
205KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 52: Number of USOAP outreach service host organisations contracted, by state and services commenced, at 30 June 2011. Source: Department of Health and Ageing.216
Jurisdiction Contracted organisations
Organisations where services commenced
NSW 11 6QLD 7 2WA 8 0VIC 8 3Total 34 11
Medical specialists delivering outreach services
Medical specialties included in USOAP in 2010-11 were: paediatrics, endocrinology, dermatology, ophthalmology, cardiology, psychiatry, orthopaedic surgery, renal, and general practice. As outlined in Table 53 below, there were 19 specialists participating in USOAP across three jurisdictions in 2010-11; while the fund holder and host organisations were in place in Western Australia, provider services had not yet commenced.Table 53: Number of specialists participating in USOAP in 2010-11, by state.217
Jurisdiction NumberNSW 9QLD 5VIC 5
Total 19
In general, fund holders and host organisations have faced challenges in recruiting specialists to provide USOAP services, which have led to implementation delays. Stakeholders identified a number of contributing factors, including:
216 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, Urban Specialist Outreach Assistance Program, 2010-11 implementation [B5a response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.217 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, 2010-11 implementation [B5a response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population.
206KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
the fund holders had no prior experience in the urban arena, and so lacked the networks that would enable them to easily engage with urban providers;
providers who were interested in working in Aboriginal and Torres Strait Islander health were already working in rural and remote areas (i.e., leaving no ready pool of providers to draw from), and that urban outreach lacks the same attraction as providing outreach services in rural and remote settings;
the remuneration available from USOAP was not significant enough to draw new providers; and
provider recruitment was challenged by overlapping service delivery zones for USOAP and MSOAP-ICD (in Remoteness Area 2), which creates competition for specialist resources between the two measures.
USOAP services
For the purposes of the USOAP, an outreach service is defined as a medical specialist visiting and providing a consultation or treatment to an individual patient at a location approved by the department. Specialist services delivered as part of the program are defined as medical specialist services that focus on the management and treatment of chronic conditions.218 Twenty-two specialist services were provided in 2010-11 in New South Wales, Queensland and Victoria. This is the number of particular medical specialties provided to patients in an approved location. Fund holders are not required to report on the number of outreach services provided, and this data is not known. Services did not commence in WA in the 2010-11 year. Table 54 below provides an overview of USOAP service delivery from 1 September 2010 to 31 August 2011, including the location of service delivery, the type of services delivered, and the number of Aboriginal and Torres Strait Islander patients who received these services. Note that all services provided under USOAP must be related to the management and treatment of chronic disease, not chronic disease prevention.219 Unlike the MSOAP-ICD (B5b measure), USOAP services are not accessible by populations other than Aboriginal and Torres Strait Islander people.
218 Department of Health and Ageing 2010, Closing the Gap, Increasing Specialist Follow-up Care, Urban Specialist Outreach Assistance Program: Program Funding Guidelines, March 2010, Department of Health and Ageing, Canberra, viewed 27 November 2012.219 Department of Health and Ageing 2011, Commonwealth’s Indigenous Chronic Disease Package Update, 16th edition (March 2011), Department of Health and Ageing, Canberra.
207KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 54: Location of USOAP service delivery, type of services provided, and number of Aboriginal and Torres Strait Islander patients served, by state or territory, 1 September 2010 to 31 August 2011.220
JurisdictionLocations of service delivery
Type of specialist services delivered
Number of Aboriginal and Torres Strait Islander people receiving services
NSW ArmidaleCampbelltownCoffs HarbourGraftonHamiltonWyong
Physician, geriatricsGeneral PhysicianPaediatricsCardiologyEndocrinologyPsychiatryOphthalmologySurgery, Orthopaedic
133
Queensland Burleigh HeadsIpswich
EndocrinologyDermatologyOphthalmologyPsychiatry
166
Victoria DandenongFootscrayWhittlesea
PsychiatryGeneral PhysicianEndocrinologyRenalPaediatrics
81
Total N/A N/A 380
USOAP differs from the MSOAP-ICD measure in that specialists work as individuals when providing services to patients rather than as part of a formal multidisciplinary team. Care coordination within USOAP relies on liaison between the GP (referrer) and specialist (provider) as well as other relevant members of the patient’s care team. There is no explicit coordinating mechanism inherent in this measure, aside from proximity provided through location at outreach host organisations, which are most often IHSs.
220 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, 2010-11 implementation [B5b response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
208KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Referral pathways, promotional channels and materials
Within USOAP, patients gain access to specialists through referral from a GP. The data and consultations suggest that referral mechanisms are working effectively in many areas, although two issues were raised during the consultations: One fund holder noted that the requirement for GP referrals may inhibit
access in locations where Aboriginal and Torres Strait Islander patients have limited access to primary health care services.
A host organisation said that they undertook a needs assessment to determine which specialists they should host, and tried to secure the involvement of the local hospital and local GP practice but were unsuccessful. They considered this was due to existing referral pathways between the GP practice and specialists at the hospital, and a perception that no further specialist services were needed.
These issues may be specific to the local context rather than being widespread and thus may not be an inherent limitation of this measure. These matters will be explored in subsequent evaluation activities. There are indications of synergy between this and other ICDP measures and most notably with measures that deployed new workforce. Qualitative evidence gathered as part of this evaluation suggests that some ICDP workers have been engaged in promoting outreach services, and facilitating patient access to USOAP. For instance, in one location, the Care Coordinator has set up and attended appointments with patients. The potential for these other ICDP measures to support and be supported by the USOAP measure will be explored in subsequent evaluation activities.
Cultural awareness training
USOAP providers are required to undertake cultural awareness training prior to commencing service delivery. Fund holders are responsible for ensuring this requirement is met, but are not required to report on the results to the department. The department assumes that all health care providers who have provided USOAP services have received cultural awareness training, in line with the program guidelines and funding agreements. Information on this aspect of ICDP is not available.1.57 Program supportsThe evaluation has mixed findings on the effectiveness of USOAP program supports for 2010-11. The evaluation found that there were no significant difficulties in adhering to USOAP program guidelines in 2010-11. Some stakeholders suggested that there is a risk that USOAP will provide services that reflect specialist availability rather than priority community need. These matters are explored further below and are based on program documentation,
209KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
information provided by the department, consultations with select USOAP fund holders and host organisations, and stakeholder feedback at Regional Forums.Program guidelines
The department released program guidelines for the USOAP in March 2010.221 Fund holders have not reported difficulty in adhering to USOAP program guidelines or applying them to local implementation, although one fund holder indicated that host organisations are reluctant to notify them of any challenges they experience, as they fear loss of funding as a repercussion.Program Advisory Committees
The program guidelines require fund holders to establish Program Advisory Committees with representation from relevant stakeholders, including (but not limited to) the Commonwealth, state/territory health departments, Aboriginal health organisations, and medical specialist, general practice and consumer organisations, to assist with development of the implementation plan and provide ongoing advice on the management of the USOAP. The Committees are advisory rather than decision making bodies, and their mandate includes forging links with the Indigenous Health Partnership Forums and planning mechanisms for other programs to explore options for integration. They also provide fund holders with advice on the appropriate types of services to be delivered, whether a proposed service meets an identified gap in specialist services and whether a proposed service location meets the criteria for a service host organisation.222 These bodies may be shared with the MSOAP-ICD (B5b measure) Advisory Forums. The USOAP Program Advisory Committees were not in place in 2009-10, and information has not been provided on progress in establishing them in 2010-11. These Committees have not been the subject of specific stakeholder feedback to date. Accordingly, the function of these Committees in informing the design and delivery of the measure is as yet unclear, including the extent to which the Committees play a role in determining how the USOAP can respond to community chronic disease needs.
Community needs
One of the responsibilities of fund holders is to develop a program implementation plan and budget focusing initially on the delivery of services in priority locations identified by the department in consultation with Indigenous Health Partnership Forums. These should be endorsed by Program Advisory Committees. 221 Department of Health and Ageing 2010, Closing the Gap, Increasing Specialist Follow-up Care, Urban Specialist Outreach Assistance Program: Program Funding Guidelines, March 2010, Department of Health and Ageing, Canberra, viewed 27 November 2012.222 ibid.
210KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Consistent with feedback on the MSOAP-ICD, stakeholders at the Regional Forums expressed concern that USOAP services are more reflective of the availability of service providers than of community needs. This is despite the fact that community health needs assessments are a requirement within USOAP funding applications, and that annual implementation plans must reflect community needs. At the same time, the uptake of services in 2010-11 indicates that delivered services are fulfilling a need.1.58 Facilitators and barriers The following factors have supported implementation of the USOAP measure in 2010-11: Fund holder arrangements. The USOAP and MSOAP-ICD measures share the
same objective: to deliver outreach services in accessible, culturally appropriate settings. For the most part, the measures share the same fund holders, despite the operation of USOAP concentrating on urban areas223 and MSOAP-ICD on rural/remote areas.224 It is possible that these fund holder arrangements create efficiency, collaboration or other gains. This will be investigated in future stages of the evaluation.
Connectivity to other ICDP measures. Access to USOAP services relies on referral from a GP, so other ICDP measures which aim to improve Aboriginal and Torres Strait Islander peoples’ access to the primary health care system are potentially a significant facilitator of the USOAP. Based on preliminary findings, it appears that the USOAP is not fully connected to other relevant ICDP measures that could otherwise enhance USOAP outcomes. For instance, while the evaluation found that Care Coordinators in at least one location facilitate access to the USOAP, there is no evidence that this is the case more broadly. There is scope for the USOAP to better link with other ICDP measures and positions (such as IHPOs and ATSIOWs) to improve GP and patient awareness of, and referral pathway to, the USOAP.
Referral pathway. The uptake of USOAP services depends on an effective referral pathway from GPs to USOAP providers, and the measure does not include provisions to enhance the referral pathway. Rather, this is expected to be provided through the IHPOs, ATSIOWs and Care Coordinators funded through other ICDP measures. However, given the limited connectivity between USOAP and other ICDP measures described above, the role of outreach host organisations may be pivotal in lifting GP awareness of the USOAP and in providing patient access.
223 ASCG-RA 1 and 2 under the Australian Standard Geographical Classification schema.224 ASCG-RA 2 to 5 under the Australian Standard Geographical Classification schema.
211KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Barriers identified included: Specialist recruitment. It is evident from consultations with stakeholders
that the key barrier to the implementation of this measure is the recruitment of specialists to deliver the USOAP services. A number of factors are at play. The fund holders lacked the knowledge of a pre-existing network of providers in the urban setting, and building these connections has taken time. The geographical overlap between the USOAP and MSOAP-ICD measures in relation to locations classified as Remoteness Area 2225, has led to competition between the two programs in recruiting specialists for this area. Stakeholders also suggested that USOAP remuneration is not sufficient to attract specialists who are not already engaged in providing services to Aboriginal and Torres Strait Islander patients, and that providing rural/remote outreach may be more appealing than urban outreach to providers. Challenges with specialist recruitment may mean USOAP services are being driven predominantly by the specialist availability rather than community needs, as was perceived by Regional Forum participants.
1.59 OpportunitiesThe early stages of implementation have identified several areas that the department may consider in order to improve the implementation and impact of the USOAP measure, as outlined below: Priority needs assessments: it is not clear the extent to which funded and
host organisations have been able to effectively identify prior community need for USOAP services that then allows them to target the specialists services required to meet this need. To the extent that this may constrain the effectiveness of the measure, there is an opportunity for the department to consider options to provide additional support to these organisations, for example providing needs assessment training to ICDP workers, or bolstering the role of Program Advisory Committees. IHPOs could also be encouraged to work with fund holders to identify priority needs. In the future, Medicare Locals, given their planned role in community needs assessment, could be linked into this measure to assist with needs identification. It is important for not only the different elements of the ICDP to be working together on such issues, but also for ICDP managers to be working in collaboration with other (non-ICDP) funded initiatives. The department could encourage this collaboration across its various internal divisions, directly with the funded organisations and through the Indigenous Health Forums.
Extending the range of services available: given the general acceptance of the role of multi-disciplinary care for people with chronic and often complex
225 Under the Australian Standard Geographical Classification schema.212
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
care needs, the department may also consider, the inclusion of allied health providers within the USOAP (as in MSOAP-ICD). Such an expansion of the USOAP may offer the added benefit of reducing the pressure on specialist recruitment by sourcing from a broader pool of health care professionals. The department should consider, however, if there are alternate service delivery methods that can effectively facilitate Aboriginal and Torres Strait Islander people’s access to urban allied health providers.
Enhanced coordination: there are a number of opportunities to enhance coordination with other ICDP measures, such as:- Encouraging liaison with Care Coordinators under the ICDP CCSS Program
(B3b measure) to explore use of the Supplementary Services funding pool to bolster USOAP funding. Supplementary Services funds can be used for patients under the CCSS Program to expedite their access to specialist and allied health services in accordance with their care plan, where a delay to access a publicly funded provider is clinically inappropriate. The CCSS Program guidelines226 provide that Supplementary Services funds may be used to meet the difference between MBS rebates and fees charged by private specialists or allied health providers. Funds may be used in some areas to pay providers a retainer for making urgent appointments available to care coordination patients, or undertaking sessional work in a particular location.
- Fostering closer working relationships between specialist providers and ICDP workers, to encourage promotion of the USOAP to GPs and community members, to encourage referrals and greater uptake.
- Improving referral pathways to and from practices registered for the Practice Incentives Program (PIP) Indigenous Health Incentive (B3a measure).
226 Department of Health and Ageing 2010, Indigenous Chronic Disease Package, Care Coordination and Supplementary Services, Program Guidelines, April 2010, Department of Health and Ageing, Canberra, pp.10-11. viewed 15 November 2012.
213KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Medical Specialist Outreach Assistance Program – Indigenous Chronic Disease (MSOAP-ICD) (B5b)This chapter describes the progress of the Increasing Access to Specialist and Multidisciplinary Team Care (hereafter referred to as the Medical Specialist Outreach Assistance Program – Indigenous Chronic Disease, or MSOAP-ICD) measure. This measure funds the provision of medical specialists and multidisciplinary team services to rural and remote communities in need of such services. In this chapter we discuss the implementation of the MSOAP-ICD in 2010-11, the second year of the ICDP, including findings against relevant activities and outputs and expected results as described in the Evaluation Framework, and barriers and facilitators and opportunities identified to date.The MSOAP-ICD at a glanceThe evaluation has found that the implementation of the MSOAP-ICD in 2010-11 is proceeding well, with fund holding agreements in place in almost every jurisdiction, and a very broad range of medical specialist and allied health services being provided to a large number of patients. There is noticeable growth in the uptake and delivery of the measure compared with 2009-10. In 2010-11, changes were made to the MSOAP-ICD program guidelines to include additional types of health professionals as service providers within the MSOAP-ICD measure; this has served to accommodate a wider range of outreach services. Recruitment of providers has been less of a challenge for the MSOAP-ICD than for the USOAP and, like the USOAP, provider availability may be influencing service provision. Fund holding agreements have been established as intended in every state and territory where relevant (i.e., all but the Australian Capital Territory), using organisations that have experience delivering the mainstream MSOAP. Overall, fund holder arrangements appear to be adequate and in line with the program guidelines. Information is not available on the type of organisations engaged as the host organisations and it is unclear how well these arrangements functioned in 2010-11. A wide range of medical specialist and allied health services were provided through the MSOAP-ICD in 2010-11. Over 500 (541) MSOAP-ICD ‘services’ were provided in 2010-11 in all states and the Northern Territory, which is more than triple the number of services provided in 2009-10. Around 80 per cent of these services were allied health. Over seven thousand (7,228) patients, including 6,283 Aboriginal and Torres Strait Islander patients, received MSOAP-ICD services in 2010-11. This was more than an eightfold increase in the number of patients seen in 2009-10. Approximately 87 per
214KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
cent of MSOAP-ICD services nationally were provided to Aboriginal and Torres Strait Islander patients. To a great extent, stakeholders perceive the MSOAP-ICD to be successful in terms of take up by patients in rural and remote locations. The implementation of the measure was facilitated by the prior experience of the fund holders in delivering mainstream MSOAP services. Recruitment issues have not been as significant for the MSOAP-ICD as for the USOAP measure (B5a), partly because the MSOAP-ICD supports both specialist and allied health service delivery, creating a broader pool of providers to draw on. However, specialist and allied health services are not interchangeable and specialist recruitment is still a salient issue in some locations. It has been suggested by some stakeholders at both the national and jurisdictional level that the availability of service delivery providers has driven the selection of MSOAP-ICD services, rather than just priority community needs alone. At the same time, some fund holders and host organisations have asserted that the high uptake of delivered services indicates a close match to community need. The implementation of the MSOAP-ICD may benefit from improved coordination with other ICDP measures, such as support from the ICDP workforce, funding from the Supplementary Services fund for specialist follow up care, and referrals from practices registered for the PIP Indigenous Health Incentive. Other opportunities for the future include enhancing mechanisms to ensure that priority community needs have been assessed and that MSOAP-ICD funding is being directed to meet those needs. Recognising the need for services in the rural and remote locations where MSOAP-ICD is delivered, MSOAP-ICD does not preclude non-Aboriginal and Torres Strait Islander peoples from accessing services, and the proportion of funds being used for these patients is 13 per cent. There is concern from a few stakeholders that the measure is providing benefits outside of the target population in some jurisdictions; however, available evidence suggests that there is unused capacity indicating scope for further uptake of services within the existing budget envelope.Potential effects based on implementation findings Figure 20 below is the causal pathway for the MSOAP-ICD measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
215KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Outreach services
respond to identified
community health needs
Aboriginal and Torres Strait
Islander patients receive
referrals to MSOAP-ICD
services
Aboriginal and Torres Strait
Islander patients engage with MSOAP-ICD services
Service delivery sites are
appropriate and accessible
Increasing Access to Specialist and Multidisciplinary
Team Care - MSOAP-ICD
Increase in care providers' cultural
awareness
Increase in regional and remote health system capacity to provide culturally
appropriate specialist and allied
health outreach services
Improvement in patients’ access to
culturally appropriate
specialist and allied health outreach
services
Increase in care providers'
knowledge, understanding and
skills
Improvement in Aboriginal and Torres Strait
Islander people’s chronic conditions
Cultural awareness training is
appropriate and effective
Recruitment and retention of outreach service
providers
Figure 20: MSOAP-ICD program causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect227 and the observed impacts.228 Both the plausibility and observed
227 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.
216KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the MSOAP-ICD measure and it was implemented according to plan in 2010-11, therefore, the plausibility of effect is not affected. Most key dependencies are in place with some suggestion that insufficient work was undertaken to identify priority needs and that there is a risk that services are provided on the basis of what providers are available, that may meet a need but not necessarily the priority need. Table 55: Assessment of key dependencies of the B5b measure.
Key dependencies
Findings Evidence
Recruitment and retention of outreach service providers
Some stakeholders reported issues with recruitment and the administrative cost and time burden with coordinating sessions for multiple providers.
This is based on stakeholder interviews
Cultural awareness training in appropriate and effective
Data is not available for the First Monitoring Report.
Not applicable
Aboriginal and Torres Strait Islander patients receive referrals to MSOAP-ICD services
Over five hundred (541) MSOAP-ICD services were provided in 2010-11 in all states and the Northern Territory, which is more than triple the number of services provided in 2009-10 (148). A wide range of medical specialist and allied health services were provided to patients.
This is based on data provided by the department
Service delivery sites are appropriate and accessible
Data is not available for the First Monitoring Report.
Not applicable
228 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
217KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Outreach services respond to identified community health needs
Varied perceptions concerning whether specialists recruited and services provided address priority need.
This is based on stakeholder interviews
Aboriginal and Torres Strait Islander patients engage with MSOAP-ICD services
Number of services provided suggests strong engagement but perceptions that some patients prefer services to be provided by IHSs.
This is based on stakeholder interviews
Contextual considerations
The location of service provision may influence engagement with MSOAP-ICD services, given the importance of services being located in a culturally safe environment.229 230,231
It is likely that variable capacity to recruit providers across jurisdictions may also impact on the implementation of the program.
Literature review
below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). The evaluation is not able to measure change in the expected impacts but notes that the level of service delivery has increased substantially in 2010-11. The evaluation is not able to gauge at this stage whether this increase is a net increase or whether there has been some substitution of existing services. The key contextual factors likely to be influencing the operation of the measure are the availability of GPs who can refer to the MSOAP-ICD, and the administrative capacity of host organisations.
229 Northern Territory Government Department of Health and Families 2009 Revision of the Preventable Chronic Disease Strategy Background Paper: Preventable Chronic Disease in Aboriginal Populations, viewed September 2011.230 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project [C3 response]. 231 Hayman NE, White NE & Spurling GK 2009, ‘Improving Indigenous Patients’ access to mainstream health services: the Inala experience’, Medical Journal of Australia, vol. 190, no. 10, pp. 604-606.
218KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 56: Assessment of expected and observed impacts of the B5b measure based on implementation progress.
Expected Observed impacts EvidenceIncrease in care providers’ cultural awareness
MSOAP-ICD services providers are required to undergo cultural awareness training. No information is available to confirm the level and nature of training provided, or to assess the impact of this training.
This is based on consultations with the department and review of program guidelines
Increase in care providers’ knowledge, understanding and skills
Data is not available for the First Monitoring Report.
Not applicable
Increase in regional and remote system capacity to provider culturally appropriate specialist and allied health outreach services
Data is not available for the First Monitoring Report.
Not applicable
Improvement in patients’ access to a range of culturally appropriate specialist and allied health outreach services for chronic disease management
Data is not available for the First Monitoring Report.
Not applicable
219KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected Observed impacts EvidenceImprovement in Aboriginal and Torres Strait Islander people’s chronic conditions
Data is not available for the First Monitoring Report.
Not applicable
Contextual considerations
The availability of GPs who can refer to MSOAP-ICD clinics is likely to impact on the number of referrals to (and thus access to) MSOAP-ICD services. For example if a GP is not available in the community leading up to the clinic, a patient may miss out on a referralLike USOAP, consultations showed that the administrative capacity of organisations may influence their willingness and readiness to run USOAP clinics and the effectiveness (i.e., in terms of the coordination of patients, providers) of the services provided.
Qualitative information gathered from a small group of relevant stakeholders
1.60 Measure overviewThe Medical Specialist Outreach Assistance Program - Indigenous Chronic Disease (MSOAP-ICD) provides Aboriginal and Torres Strait Islander people with improved access to specialist and multidisciplinary healthcare services in culturally appropriate rural and remote environments. MSOAP-ICD is an extension of the mainstream MSOAP provided by the department, which was developed in 2000 to improve rural and remote communities’ access to medical specialist services. The extended ICD program aims to provide further targeted benefits to Aboriginal and Torres Strait Islander communities in rural and remote areas.232 Note that while the primary focus of the MSOAP-ICD is to deliver services to locations where the majority of the population is Aboriginal and Torres Strait Islander, non-Aboriginal and Torres Strait Islander patients are also able to access services through the MSOAP-ICD, recognising that there may be no other services available.233
Similar to the Urban Specialist Outreach Assistance Program (USOAP) (B5a measure), the MSOAP-ICD supports outreach services which focus on the detection, management and prevention of chronic diseases. Unlike the 232 Defined using the Australian Standard Geographical Classification as Remote Areas 2 (inner regional) to 5 (very remote).233 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, 2010-11 implementation [B5b response].
220KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
USOAP, the MSOAP-ICD provides for preventative health services such as those provided by allied health professionals. The MSOAP-ICD expects health professionals funded under the measure to work in a multidisciplinary team to provide treatment and management of chronic conditions for Aboriginal and Torres Strait Islander patients. Funding is able to be used for medical specialists, GPs and allied health professionals. The configurations of the multidisciplinary team may vary depending on the health and treatment needs of communities and individual patients, and it is recognised that it may not be necessary or possible for team members to deliver an outreach service at the same time.234 Further detail on the measure is given in the Baseline Report.235
The department has entered into fund holder agreements with public and private organisations to administer the delivery of outreach services in rural and remote locations. Funds have been distributed among state and territory jurisdictions based on the size of their Aboriginal and Torres Strait Islander population. All fund holders have existing experience with providing mainstream MSOAP services. In 2010-11, the actual expenditure during this year was $6.835 million. 1.61 Rural and remote outreach servicesThe evaluation has found that the implementation of the MSOAP-ICD in 2010-11 is proceeding well, with fund holding agreements in place in every relevant jurisdiction; fund holding arrangements appear to be adequate; and a wide range of medical specialist and allied health services are being provided to a large number of patients. There is noticeable growth in the take up and delivery of the measure compared with 2009-10.The Sentinel Sites Evaluation found that care coordination between team members of MSOAP-ICD providers (delivered by the outreach service host) and the cultural awareness of providers were important features of success for the MSOAP-ICD measure in the Sentinel Sites. There is not sufficient evidence for the evaluation to make broader findings on these matters, nor on the operation of the outreach service host organisation arrangements. Some stakeholders reported issues with recruitment and the administrative cost and time burden with coordinating sessions for multiple providers. These findings have been informed by program documentation and data provided by the department, the Sentinel Sites Evaluation Report236, stakeholder feedback at Regional Forums, and consultation with the
234 Department of Health and Ageing 2010, Medical Specialist Outreach Assistance Program Indigenous Chronic Disease 2009-2013 Guidelines, Department of Health and Ageing, Canberra, viewed 30 November 2012.235 KPMG 2013, Indigenous Chronic Disease Package National Monitoring and Evaluation Project: Baseline Report, Australian Government Department of Health and Ageing, Canberra
221KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
department, and a selection of NACCHO affiliates, fund holders and outreach service host organisations.Fund holding and host organisation arrangements
The nature of MSOAP-ICD fund holders varies from rural workforce agencies, state or territory departments of health to a DoGP SBO. To date, fund holder arrangements appear to be adequate, and in line with the program guidelines.237 Data on the number and location of MSOAP-ICD host organisations is not collected by the department.238 Consultations suggest that these organisations tend to be IHSs or Divisions of General Practice, but stakeholders did not comment on these arrangements.Medical specialists and allied health care providers
A range of specialist and allied health services are supported through the MSOAP-ICD. This is in contrast to the USOAP (B5a measure), which funds only medical specialist outreach service delivery. Table 57 below lists the specialty areas and other health professionals (such as allied health professionals or GPs) who delivered outreach services through the MSOAP-ICD in 2010-11.
236 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.237 Department of Health and Ageing 2010, Medical Specialist Outreach Assistance Program Indigenous Chronic Disease 2009-2013 Guidelines, Department of Health and Ageing, Canberra, viewed 30 November 2012.238 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, 2010-11 implementation [B5b response].
222KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 57: Specialty and other health professional services delivered by the MSOAP-ICD, by state or territory, 2010-11. Source: Department of Health and Ageing.239
JurisdictionType of specialty services delivered
Other health professionals who delivered outreach services
New South Wales
CardiologyEndocrinology (diabetes)NephrologyRespiratoryEndocrinologyOphthalmologyPsychiatry
GP CoordinatorsRegistered NurseAboriginal Health Education OfficerDietician/NutritionistPsychologistDiabetes EducatorAboriginal Health WorkerPodiatristRespiratory ScientistPhysiotherapistClinical Nurse SpecialistSocial WorkerExercise PhysiologistAsthma EducatorSpirometry InstructorGP - Chronic DiseaseCardiac Rehabilitation NurseMental Health Nurse
239 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, 2010-11 implementation [B5b response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
223KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
JurisdictionType of specialty services delivered
Other health professionals who delivered outreach services
Queensland CardiologyGeneral PhysicianRespiratoryEndocrinology (diabetes)OphthalmologyEndocrinologyPaediatricsDermatology
Registered NurseRespiratory ScientistGPGP RegistrarSonographerDiabetes EducatorClinical Nurse SpecialistDietician/NutritionistPodiatristPhysiotherapistExercise PhysiologistSpeech PathologistGP - Chronic DiseasePsychologist
Western Australia
CardiologyEndocrinology (diabetes)General Physician
Registered NurseClinical CoordinatorDietician/NutritionistPhysiotherapistGPAboriginal Health WorkerOrthoptistDiabetes EducatorPodiatrist
Northern Territory
RehabilitationCardiology
Dietician/NutritionistCardiac EducationPodiatristDiabetes Educator
Victoria CardiologyEndocrinologyPsychiatry
Aboriginal Health WorkerGPPodiatristExercise PhysiologistDietician/NutritionistDiabetes Educator
224KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
JurisdictionType of specialty services delivered
Other health professionals who delivered outreach services
South Australia General Physician GPChronic Disease NursePodiatristStudent/RegistrarOccupational TherapistGPPractice NurseDietician
Tasmania Nil Dietician/NutritionistDiabetes EducatorExercise PhysiologistOrthoptist
Australian Capital Territory
Not applicable (not a fund holder)
Not applicable
Preliminary findings indicate that while the measure appears to be using a wide range of service providers, host organisations and fund holders have experienced some recruitment challenges. Outreach service delivery requires a scheduled break from a provider’s regular work, and there are significant logistical challenges in coordinating a fly-in schedule for multiple providers. Host organisations consulted have indicated that there is insufficient funding to cover this significant administrative work. Specialist and allied health outreach medical services
Over five hundred (541) MSOAP-ICD services were provided in 2010-11 in all states and the Northern Territory, which is more than triple the number of services provided in 2009-10 (148). Within the MSOAP-ICD measure, a ‘service’ is defined as a health professional (i.e., an individual medical specialist, GP and/or allied health professional) visiting and providing medical consultation at an approved location, i.e., a ‘service’ does not indicate one consultation with a patient. Table 58 below shows the number of specialist and allied health services provided through the MSOAP-ICD in 2010-11. Around 80 per cent of services were allied health.
225KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 58: Number of MSOAP-ICD services provided, by outreach service type, 2010-11.240
Type of outreach service Number of services provided in2010-11
Specialist services 107Allied health services 434Total 541
As set out in Table 59 below, a total of 6,283 Aboriginal and Torres Strait Islander patients were served by the MSOAP-ICD in each state or territory in 2010-11. This was more than an eightfold increase in the number of Aboriginal and Torres Strait Islander patients seen in 2009-10 (717). Note that given the definition of a ‘service’, multiple patients could be served in one MSOAP-ICD ‘service’. Thus the number of patients served is greater than the number of services provided.As noted in the table, approximately 87 per cent of MSOAP-ICD services were provided to Aboriginal and Torres Strait Islander patients with the remainder provided to non-Aboriginal and Torres Strait Islander patients. In Tasmania, some stakeholders noted that this open eligibility policy may be inappropriately diverting resources away from the intended beneficiaries, Aboriginal and Torres Strait Islander people. However, the department advises that there was an underspend in the program budget in Tasmania in 2010-11, suggesting there was capacity for greater uptake by Aboriginal and Torres Strait Islander clients in Tasmania. Based on the views of stakeholders consulted to date, the MSOAP-ICD appears to provide an increased number of services rather than providing a substitute source of funding for existing services. Appointments appear to be well attended, but patient ‘no shows’ are reportedly an issue in some locations.
240 Department of Health and Ageing 2011, Data request for national ICDP monitoring and evaluation project, 2010-11 implementation [B5b response].
226KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 59: Number of MSOAP-ICD services provided, and number of patients receiving services, by state and territory, 2010-11.241 242
Jurisdiction Number of services provided
All patients receiving services
Aboriginal and Torres Strait Islander patients receiving services
New South Wales
194 1,673 1,473
Queensland 164 2,963 2,438Western Australia
67 781 661
Northern Territory
50 767 767
Victoria 36 198 164South Australia 25 760 760Tasmania 5 86 20Australian Capital Territory
N/A N/A N/A
Total 541 7,228 6,283
Coordinated care
The MSOAP-ICD is premised on a team-based model of care, with the expectation that service providers are willing and able to communicate with each other regarding patient care. Coordination for the team model ultimately rests with the host organisation, which is expected to liaise with team members, including through sharing of patient records. Care coordination may be enhanced by the MSOAP-ICD due to the high degree of interaction within service provider teams. For instance, in Western Australia, teams of healthcare providers travel together in charter planes to deliver health services to remote locations. The host organisation provides administrative assistance, including handling paperwork on site and briefing and debriefing service delivery with the team. Team members may consult with one another during the course of service delivery as warranted. 241 Department of Health and Ageing2011, Data request for national ICDP monitoring and evaluation project, 2010-11 implementation [B5b response]. Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.242 Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
227KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The Sentinel Sites Evaluation Report has noted that effective coordination of the MSOAP-ICD through local primary health care practices is pivotal to the success of the measure.243 Some stakeholders at ICDP Sentinel Sites reported deficiencies in care coordination within the mainstream MSOAP program, including poor communication between specialists and patients and lack of follow up care, and expressed concern that these would also occur within the MSOAP-ICD.There is insufficient evidence for the evaluation to make a broader finding on the effectiveness of care coordination at this stage.Cultural awareness training and cultural appropriateness of outreach services
MSOAP-ICD providers are required to demonstrate that they have participated in cultural awareness training prior to delivery of outreach services, and the MSOAP-ICD supports training costs.244 Fund holders are responsible for arranging and verifying this training, but are not required to report on this to the department. The department assumes that all health care providers who have provided MSOAP-ICD services have received cultural awareness training, in line with the program guidelines and funding agreements. The cultural appropriateness of outreach services relies on the adequacy of the required cultural awareness training to influence the behaviour of MSOAP-ICD service providers, and the orientation or preparation provided by the fund holder or host organisation. This outcome has not been the subject of any substantive feedback from stakeholders consulted through the evaluation. One outreach host observed that a lack of previous experience working with Aboriginal and Torres Strait Islander people, or working in remote locations, will affect the cultural appropriateness of a provider’s service delivery. Findings from the Sentinel Sites Evaluation245 also emphasised the need for cultural awareness training for the service providers in order to help them understand the social and cultural factors impacting on their patients’ health, including the reasons that patients may not attend scheduled appointments (such as to attend funerals and fulfil associated cultural commitments). Promotional channels and materials
Fund holders rely on host organisations (often IHSs) to book patient appointments for outreach services. It is unknown whether patients of other services outside of these host organisations have access to MSOAP-ICD services.243 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.244 Department of Health and Ageing 2010, Medical Specialist Outreach Assistance Program Indigenous Chronic Disease 2009-2013 Guidelines, Department of Health and Ageing, Canberra, viewed 30 November 2012.245 ibid.
228KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Aboriginal and Torres Strait Islander Outreach Workers (ATSIOWs), a new role funded under the ICDP (measure C2 and C3) appear to play a role in promoting patient access to outreach services. Some stakeholders consulted, including an SBO, a fund holder and a host organisation, reported that ATSIOWs (and in some locations the pre-existing position of AHW) have local contacts who promote the service and coordinate patient access. 1.62 Program supportsThe evaluation found that program supports were in place and there were no significant difficulties that organisations had with adhering to the MSOAP-ICD program guidelines. The operation of the MSOAP-ICD state and territory Advisory Forums could be strengthened to improve their understanding of and operation in the outreach service system in each jurisdiction, and to ensure alignment between MSOAP-ICD services and community needs. These findings are informed by program documentation, stakeholder feedback at Regional Forums, and consultation with a selection of NACCHO affiliates, fund holders and outreach service host organisations.State and territory Advisory Forums
The MSOAP-ICD state and territory Advisory Forums are designed to be a consultative mechanism to inform the department and fund holders about how to best deploy resources and determine service priorities for MSOAP-ICD service planning in each jurisdiction. The functions of the Advisory Forums include: making recommendations on service priorities, including considering target
locations for delivery of the MSOAP-ICD, and their relative needs; evaluating all proposals for MSOAP-ICD funding with regards to:
- whether the selected region has the need and capacity to sustain support for a new service;
- gaps in services; and- appropriateness of the types of services to be delivered; and
liaising with the Indigenous Health Partnership Forums and linking with the planning mechanisms of other programs to explore possibilities for integrated program implementation, when appropriate.246
These bodies may be shared with the USOAP (B5a measure) Program Advisory Committees.
246 Department of Health and Ageing 2010, Medical Specialist Outreach Assistance Program Indigenous Chronic Disease 2009-2013 Guidelines, Department of Health and Ageing, Canberra, viewed 30 November 2012.
229KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Feedback on the MSOAP-ICD state and territory Advisory Forums from stakeholders consulted through the evaluation has been minimal. However, the available input indicates that the members of the Advisory Forums have struggled with the complexity of the outreach service system, particularly where there are other outreach programs within the one jurisdiction. An example is in the Northern Territory where MSOAP-ICD service delivery may overlap with the Specialist Outreach Northern Territory (SONT) program. The target communities of the MSOAP-ICD are locations with a majority Aboriginal and Torres Strait Islander population with a high prevalence of complex and chronic health conditions or where a significant proportion of the Aboriginal and Torres Strait Islander community in the location have chronic health conditions. Fund holders are responsible for undertaking a needs analysis in consultation with the Advisory Forums, the Indigenous Health Partnership Forums and local health professionals. The Advisory Forums are responsible for considering the target locations and their relative needs in recommending services under the MSOAP-ICD to the department. All services supported under the MSOAP-ICD are required to be reviewed annually by the fund holder and the Advisory Forum to ensure that services continue to meet the objectives of the measure and the needs of the community.247 The extent to which MSOAP-ICD service delivery is responsive to community health needs appears to vary across jurisdictions. Regional Forum stakeholders considered that the delivery of both MSOAP-ICD and USOAP was not always based on an understanding of needs and good planning processes. A few Advisory Forum and fund holder stakeholders in some jurisdictions considered that the needs assessments submitted in funding proposals were not considered in funding decisions. At the same time, other fund holder and host organisation stakeholders have indicated that good attendance at outreach service appointments reflects a match between service delivery and community health needs. It is possible that, while MSOAP-ICD service delivery may not match priority health needs as identified in the needs assessment, uptake of services reflects relative need. This may reflect fund holders’ practical accommodation of recruitment challenges. Program guidelines
In 2010-11, changes were made to the MSOAP-ICD program guidelines248 to include additional types of health professionals as service providers within the
247 ibid.248 Department of Health and Ageing 2010, Medical Specialist Outreach Assistance Program Indigenous Chronic Disease 2009-2013 Guidelines, Department of Health and Ageing, Canberra, viewed 30 November 2012.
230KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
MSOAP-ICD measure; this served to accommodate a wider range of outreach services. Preliminary stakeholder feedback has not indicated any particular difficulties in conforming to the requirements of the program guidelines, or any significant deviation from the program guidelines. 1.63 Facilitators and barriers Implementation of the MSOAP-ICD has been influenced by a number of factors, including fund holder arrangements, response to community health needs, and adequacy of remuneration for providers. The following factors have supported implementation of the MSOAP-ICD measure in 2010-11: Fund holder arrangements. The implementation of the MSOAP-ICD has
been enhanced by the previous participation of fund holders in the mainstream MSOAP which has enabled healthcare providers to be recruited through existing networks. In general, fund holders appear to be capable of delivering the program according to program guidelines.
The following barriers were also identified: Match to community health needs. Recruitment issues have not been as
significant for the MSOAP-ICD as for the USOAP measure (B5a), partly because the MSOAP-ICD supports both specialist and allied health service delivery, creating a broader pool of providers to draw on. However, specialist and allied health services are not interchangeable and specialist recruitment is still a salient issue in some locations. For instance, MSOAP-ICD services have at times been cancelled or delayed where no service providers are available. As for the USOAP, it has been suggested by some stakeholders at both the national and jurisdictional level that the availability of service delivery providers has driven the selection of MSOAP-ICD services, rather than priority community needs.
Remuneration. Outreach service delivery requires recruitment of health care providers who may require leave from their regular/ongoing duties in order to participate in the MSOAP-ICD. To support provider recruitment, the MSOAP-ICD program guidelines allow for a ‘workforce support’ payment that provides financial support at sessional rates to outreach service providers participating in MSOAP-ICD. Providers may receive either (but not both) the workforce support payments or MBS payments for outreach service delivery at the location. Fund holders have indicated that remuneration available through MSOAP-ICD may not be sufficient to attract new providers who are not already engaged in the Aboriginal and Torres Strait Islander health sector or other outreach services.
231KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.64 OpportunitiesThe implementation of the MSOAP-ICD measure has been successful by most stakeholder accounts. Suggestions are given in section 13.5 on ways in which the needs assessments could be enhanced to ensure that those most in need of care have access to the service. The department may also want to consider the outcomes of MSOAP-ICD in relation to the significant cost of delivering outreach services. See also the opportunities outlined for the USOAP (B5a measure) in section 1.59 above which also hold for the MSOAP-ICD.
232KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Workforce Support, Education and Training (C1)This chapter describes the progress of the Workforce Support, Education and Training (C1) measure in 2010-11, the second year of the ICDP. In this chapter, we discuss the measure’s achievements, activities, facilitators, barriers, signs of progress towards desired outcomes, and opportunities for the future. Workforce Support, Education and Training at a glanceThe evaluation found that the focus of this measure in 2010-11 was on delivering key components, following the preparatory work undertaken in 2009-10, and this has largely been on track. Fifty-nine Aboriginal and Torres Strait Islander Outreach Workers (ATSIOWs) received orientation across five jurisdictions in 2010-11, and overall providers and participants considered the orientation to be relevant to the ATSIOW role and valuable for facilitating networking between outreach workers. Some lags between the recruitment and orientation of ATSIOWs are evident in some jurisdictions, and discussions were underway between the department, NACCHO and affiliates to address these delays. Despite ATSIOW roles being entry-level positions, incumbents have wide variation in skills, experience and qualifications which impacts on the value that stakeholders placed on orientation and there were some challenges in tailoring the content appropriately to the diverse workforce. There is also evidence that training is valued, which is likely to reflect that training is responsive to individual needs identified by workers and their organisation. Links to professional qualifications are important for extending the development of ATSIOWs and developing a career pathway for this new role, and there is an indicative link between the availability of professional development opportunities and sustainability of ATSIOW positions. Nursing scholarships were under-subscribed in 2010-11, and awareness of these scholarships was low amongst stakeholders consulted. The evaluation found that there is substantial uptake of the GP registrar training posts in 2010-11, despite low awareness amongst stakeholders about the availability of these posts. Facilitators for the implementation of this measure were the ability to build on existing national programs for training posts and nursing and midwifery scholarships. The key barriers were delays in ATSIOW recruitment; delays in accessing orientation in some locations; inadequate numbers of qualified GPs in IHSs available to supervise GP registrars; and an indistinct ‘brand’ or identity for the ICDP nursing and midwifery scholarships. There are opportunities to strengthen the Workforce Support, Education and Training measure in the future through developing a coordinated ICDP workforce training strategy; and improving the promotion of ATSIOW individualised
233KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
training, the measure nursing and midwifery scholarships and GP registrar training post opportunities including eligibility requirements, what funding covers and relevant registered training organisations / IHSs available to provide training, placements and posts. . Potential effects based on implementation findings Figure 21 below is the causal pathway for the Workforce Support, Education and Training measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
GPs and nurse trainees have a positive
perception of their placement experience
Benefits of work in IHSs outweighs costs
to GPs and nurses
Workforce Support, Education and Training
Increase in delivery of primary health care services
by GPs and nurses
Improved preparation and development of the ATSIOW workforce to effectively carry
out their duties
Increase in health system capacity and capability to deliver primary health care services to Aboriginal and
Torres Strait Islander people
More ATSIOWs, GPs and nurses choose to sustain their employment in IHSs
GPs and nurses have a greater understanding of the health needs of Aboriginal and Torres Strait Islander
people
ATSIOWs feel supported and satisfied with their roles
Nurses in IHSs have greater opportunities for
professional development
Nurses in IHSs feel supported and satisfied with
their roles
ATSIOW orientation is appropriate and
effective
Employers provide supportive work environments for
ATSIOWs
ATSIOW training is accessible and relevant to work in the health
care sector
Figure 21: Workforce Support, Education and Training causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility
234KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
of effect249 and the observed impacts.250 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. Table 60 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the measure and it was largely implemented according to plan in 2010-11, therefore, the plausibility of effect is not affected. Information is available for some of the key dependencies and which suggests that there is a need to improve the timeliness and relevance of orientation and training of ATSIOWs and to improve the promotion of the scholarships to ensure the long-term effectiveness of this measure.Table 60: Assessment of key dependencies of the C1 measure.
Key dependencies
Findings Evidence
ATSIOW orientation and training support:ATSIOW orientation is appropriate and effective
There were delays in the provision of orientation to ATSIOWs. The literature indicates that where orientation and preparation programs are inconsistent, it can result in inadequate recruitment and high turnover.251
This is based on review of the literature, data provided by the department, program documentation, and qualitative information gathered through consultations with the department, NACCHO and affiliates, Regional Forums, and 11 ATSIOWs across six jurisdictions.
249 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.250 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes. 251 Smith J, O’Dea K, McDermott R, Schmidt B & Connors C 2006, ‘Educating to improve population health outcomes in chronic disease: an innovative workforce initiative across remote, rural and Indigenous communities in northern Australia’, Rural and Remote Health (online), vol 6: 606, pp.1-15.
235KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
ATSIOW orientation and training support:ATSIOW training is accessible and relevant to work in health care sector
Training is valued and may support the sustainability of ATSIOW positions. A few ATSIOWs had difficulties in accessing training due to a perception of cost constraints, which suggests a need to better communicate information on the measure (including that it covers training and travel costs where required). The literature shows that training and education activities are important to enhance the potential productivity and retention of the Aboriginal Health Worker workforce, while discontinuous or insufficient training represent barriers to providing better practice health care.252
This is based on review of the literature, program documentation, and qualitative information gathered through consultations with NACCHO and affiliates, Regional Forums, and 11 ATSIOWs across six jurisdictions
ATSIOW orientation and training support:Employers provide supportive work environments to ATSIOWs
Timely and on-going access to relevant training is an emerging issue.
This is based on qualitative information gathered through consultations with 11 ATSIOWs across six jurisdictions
ATSIOW orientation and training support:Contextual considerations
Research highlights the importance of geographically accessible training for AHWs in rural and remote locations using a variety of teaching methods.253 Therefore, it is likely that the geographic accessibility of the orientation may impact on the uptake of this component.
This is based on analysis of literature
252 Si D, Bailie RS, Togni SJ, D'Abbs PHN & Robinson GW 2006, ‘Aboriginal health workers and diabetes care in remote community health centres: a mixed method analysis’, Medical Journal of Australia, vol. 185, no. 1, pp. 40-45.253 Sutherland A & Billimoria B 2011, Aboriginal and Torres Strait Islander continence training in rural and remote Australia. Conference paper presented at the 11th National Rural Health Conference, March 2011.
236KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
GP registrar training posts and Nursing and midwifery scholarships:GP registrars and nurse trainees have positive perceptions of their placement experience
Data not available for First Monitoring Report.
Not applicable
Benefits of work in IHSs outweighs costs to GPs and nurses
Data not available for First Monitoring Report.
Not applicable
GP registrar training posts and Nursing and midwifery scholarships:GPs registrars, nurses and midwives / nursing and midwifery students are aware of the opportunities for training posts and scholarships
Awareness of the opportunities appears to be variable and in some cases low amongst relevant stakeholders.Lack of adequate promotion was suggested as a reason for this by national stakeholders and health services engaged through the site visits.
This is based on a review of program documentation and qualitative information gathered through consultations with the department, NACCHO and affiliates, the fund holders, Regional Forums, and staff at IHSs
237KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
GP registrar training posts and Nursing and midwifery scholarships:Contextual considerations
Literature shows that health professionals require support and guidance to deliver effective care254, however, it is likely that some types of support (e.g., supervision) may be less accessibly in regional and remote areas due to difficulties recruiting staff to these areas.255
The impact of the measure in part also depends on the willingness and capacity of IHSs to take on a registrar training post or nursing placement.
Literature review
below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). The evaluation is not able to measure change in the expected impacts, but there is some evidence that ATSIOWs have valued the training provided and the support from other ICDP workforce elements. The main contextual factors that appear to be influencing this measure are the wide range in existing skills and backgrounds of ATSIOWs that has impacted on the desire for, perceived need for, and value placed on orientation and ongoing training needs; support from employers to identify ATSIOW training needs and facilitate access to the available training under the measure; and willingness and capacity within Indigenous health services (IHSs) to host GP registrar training placements and nursing / midwifery student clinical placements funded by scholarships.
254 Zwar N, Harris M, Griffiths R, Roland M, Dennis S, Powell Davies G & Hasan I 2006, A systematic Review of Chronic Disease Management, Australian Primary Health Care Research Institute, Canberra. 255 Hays R 2012. Remote supervision of health professionals in areas of workforce need: time to extend the model? Article based on keynote presentation at the inaugural Remote Medical Education Conference held 27-28 July 2012 in Sydney, Australia.
238KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 61: Assessment of expected and observed impacts of the C1 measure based on implementation progress.
Expected impacts
Observed impacts Evidence
ATSIOW orientation and training support:Improved preparation and development of the ATSIOW workforce to effectively carry out their duties
Fifty-nine ATSIOWs across five jurisdictions have received orientation, and overall providers and participants considered it to be relevant to the role and valuable for facilitating networking between outreach workers. Delayed delivery of orientation may have somewhat reduced the effectiveness of their preparation.
This is based on qualitative information gathered through consultations with NACCHO and affiliates, Regional Forums, and staff at IHSs
ATSIOWs feel supported and satisfied with their roles
ATSIOWs feel supported and satisfied with their roles.
This is based on qualitative information gathered through consultations with ATSIOWs, IHPOs and Divisions of General Practice
239KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected impacts
Observed impacts Evidence
ATSIOW orientation and training support:Contextual considerations
While the ATSIOW role was designed to be an entry-level position, in practice the workers have wide variations in previous experience and qualifications. This has impacted on the desire for, perceived need for and value placed on orientation and training. Further, support from employers to identify ATSIOW training needs and facilitate access to the available training under the measure is a key external factor impacting on the implementation of this component of the measure.Some stakeholders consulted for the evaluation raised issues with accessing orientation and training due to their geographical location. Specifically, ATSIOWs in regional and remote areas raised as barriers the costs associated with travelling to main centres for orientation, and having to take time off work around orientation.
This is based on qualitative information gathered through consultations staff at IHSs
Nursing and midwifery scholarships:Nurses and midwives in IHSs have greater opportunities for professional development
The scholarships have broadened the opportunities available for relevant individuals.
This is based on a review of program documentation provided by the fund holder
Nursing and midwifery scholarships:Nurses and midwives in IHS feel supported and satisfied with their roles
Data is not available for the First Monitoring Report.
Not applicable
240KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected impacts
Observed impacts Evidence
Nursing and midwifery scholarships:Nurses and midwives have greater understanding of the health needs of Aboriginal and Torres Strait Islander people
Data is not available for the First Monitoring Report.
Not applicable
Nursing and midwifery scholarships:Increase in delivery of primary health care services by nurses and midwives
Data is not available for the First Monitoring Report.
Not applicable
Nursing and midwifery scholarships:Contextual considerations
None identified.
GP registrar training posts:GPs have greater understanding of the health needs of Aboriginal and Torres Strait Islander people
Data is not available for the First Monitoring Report.
Not applicable
241KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected impacts
Observed impacts Evidence
GP registrar training posts:Increase in delivery of primary health care services by GPs
Data is not available for the First Monitoring Report.
Not applicable
Contextual considerations
None identified.
All components:More ATSIOWs, GPs and nurses choose to sustain their employment in Indigenous Health Services
Data is not available for the First Monitoring Report.
Not applicable
All components:Increase in health system capacity and capability to deliver primary health care services to Aboriginal and Torres Strait Islander people
Data is not available for the First Monitoring Report.
Not applicable
1.65 Measure overviewThe Workforce Support, Education and Training measure provides education and training opportunities for the ICDP ATSIOW workforce, GP registrars, nurses and nursing trainees. The Workforce Support, Education and Training
242KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
measure aims to increase workforce capacity and capability to deliver primary health care services to Aboriginal and Torres Strait islander people. Under this measure, professional development opportunities are provided to ATSIOWs, who can access role orientation support and nationally accredited training, and attend workshops; medical graduates who can apply for GP registrar training posts; and nursing and midwifery students and qualified health workers in the IHS sector who can apply for nursing and midwifery scholarships. The measure has a budget of $17.74 million across the four years of the ICDP (2009-10 to 2012-13). The 2010-11 expenditure was $3.18 million. 1.66 ATSIOW orientation and training supportThe focus of this component of the measure in 2010-11 was on delivering orientation and training, following the preparatory work undertaken in 2009-10. The evaluation found that this component is largely on track. Some lags between the recruitment and orientation of ATSIOWs are evident in some jurisdictions, and discussions were underway between the department, NACCHO and affiliates to address these delays. There were mixed views on the value of orientation and relevance to the ATSIOW role which may reflect these lags, and that despite ATSIOW roles being entry-level positions, incumbents have wide variation in skills, experience and qualifications. Some stakeholders raised issues with accessing orientation and training due to their geographical location, and financial and time costs, but there was strong evidence that, overall, training has been taken up and was valued.These findings are informed by information and data provided by, and consultations with, the department, NACCHO and NACCHO affiliates; feedback from stakeholders at Regional Forums; consultations with SBOs, host organisations and 11 ATSIOWs. Activities undertaken by this measure for ATSIOW professional development in 2010-11 included the development and delivery of ATSIOW orientation packages, commencement of processes to identify and fund training, and a national workshop. All jurisdictions, with the exception of the Northern Territory, Queensland and Tasmania, conducted ATSIOW orientation in 2010-11.256 Delays in these jurisdictions were due to lags in the recruitment of ATSIOWs and the level of consultation required to develop orientation packages. The number of ATSIOWs who have participated in orientation workshops as at 1 June 2011, and the total number of ATSIOWs recruited under the ICDP by 30 June 2011, is presented in Table 62 below.
256 The ATSIOW in the Australian Capital Territory participated in orientation in Victoria coordinated by the Victorian Aboriginal Community Controlled Health Organisation (VACCHO).
243KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 62: Delivery of ATSIOW orientation packages, by jurisdiction, and cumulative number of ATSIOWs oriented, as at 1 June 2011.257
Jurisdiction Number of ATSIOWs recruited FTE258
Number of ATSIOWs who have completed orientation programs
New South Wales 35 18Queensland 39 0Western Australia 19 18Northern Territory 8 0Victoria 13 12South Australia 14 10Tasmania 6 0Australian Capital Territory 2 1Total 136 59
In early 2010-11, a workshop was hosted in the Northern Territory to discuss the orientation and training needs of the Northern Territory ATSIOW workforce. Following this workshop, a funding agreement was executed with the Northern Territory NACCHO affiliate (Aboriginal Medical Services Alliance of the Northern Territory) to develop and deliver an orientation package to IHS and mainstream ATSIOWs located in the Territory. In 2010-11, discussions also commenced between NACCHO and the Tasmanian Aboriginal Centre (TAC) regarding the delivery of orientation for ATSIOWs employed in IHSs in Tasmania, and with the Australian Divisions of General Practice for the delivery of orientation to ATSIOWs working in general practices in Tasmania. However, during 2010-11, ATSIOW orientation was not delivered in Tasmania; with AHW training commitments reducing the capacity of the TAC to deliver ATSIOW orientation.The ICDP focus on workforce and, in particular, building workforce capacity through recruitment and skill development was seen to be important by many stakeholders who acknowledged this as a significant need.ATSIOW orientation
ATSIOWs are an entry-level position recruited under the Expanding the Outreach and Service Capacity of Indigenous Health Organisations (C2) and
257 Department of Health and Ageing 2011, Data request for ICDP national monitoring and evaluation project, 2010-11 implementation [C1 response]; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.258 Based on information provided by the Department of Health and Ageing 2011.
244KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
the Engaging Divisions of General Practice to Improve Indigenous Access to Mainstream Primary Care (C3) measures. The first year of the measure involved identifying the workforce needs to inform the design of the orientation packages. Orientation packages were designed by NACCHO affiliates in response to the needs analysis prepared by the Aboriginal and Torres Strait Islander Health Registered Training Organisation National Network in 2009, and informed by stakeholder consultations. Although national guidelines have not been provided for the contents of orientation packages, they generally consist of a number of modules that provide the ATSIOW workforce with background information on the Australian health workforce, relevant information about working in the health system, and an understanding of the ATSIOW service delivery role. Participating in orientation is mandatory for ATSIOWs, and is expected to be undertaken within six months of commencement in the position, in order to prepare them for undertaking and shaping this new role. Despite ATSIOW orientation being mandatory, at the community site visits there appeared to be some confusion amongst IHS and mainstream funded organisations about what ‘ATSIOW orientation’ was. Some organisations thought that participating in internal organisational orientation negated the need for employees to participate in the jurisdictional ATSIOW orientation provided on behalf of the department. One national stakeholder suggested that orientation should be the responsibility of the funded organisations rather than being delivered at a jurisdiction-wide level. Consultations with stakeholders during the evaluation’s community site visits also suggest there has been inconsistency in ATSIOW participation in orientation. These stakeholders reported that whether ATSIOWs participate in orientation depends on: the timing of their recruitment and whether orientation was scheduled in
the early stages of their employment; and the geographical area in which the ATSIOWs are based, and whether
orientation is easily accessible – ATSIOWs in regional and remote areas raised as barriers the costs associated with travelling to main centres for orientation, and having to take time off work around orientation. The ATSIOW based in the Australian Capital Territory completed orientation in Victoria through VACCHO.
Overall, providers and participants both considered the orientation to be relevant to ATSIOW roles, but there were challenges with delays between recruitment to the role and delivery of orientation in some jurisdictions; and in tailoring the content appropriately to a wide range of backgrounds, experiences and qualifications.
245KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Available reports259 from some of the NACCHO affiliates which delivered ATSIOW orientation in 2010-11 indicate a range of ways in which the learning from orientation is embedded. Some providers reported undertaking a training needs analysis and/or stakeholder consultation to develop the orientation workshops260; others developed supporting material such as student manuals.261 One provider reported visiting participants in the workplace after the training to elicit how the learning was being applied on the job.262 Another suggested the content could be adapted to provide an introductory program for high school students interested in health care careers.263 Most reported that participant evaluation surveys showed they found the content relevant to their role.Eleven ATSIOWs were consulted during site visits for this report. The vast majority (10) were based in mainstream organisations. Those who had participated in ICDP-specific orientation generally found it valuable. These ATSIOWs reported that a key benefit from the orientation (and other joint training) was being able to meet other ATSIOWs to share information and experiences. A number of ATSIOWs said such networking opportunities helped them to understand the scope of the role, which is considered by many ATSIOWs and their managers to be loosely defined. Other opportunities for networking were provided by SBOs, and these were considered valuable for the same reason. Some ATSIOWs commented that the orientation was valuable but, if it had been completed in the absence of any other training, would have been inadequate to support them to fulfil the requirements of their role. These ATSIOWs came from a human services (but not health) background. The quality of the ATSIOW orientation was considered poor by some national stakeholders who also suggested that, alone, it was not adequate to support people in entry-level positions.ATSIOW national workshop
A national workshop for ATSIOWs was coordinated and facilitated by the NACCHO on 21-22 June 2011 in Sydney.
259 Aboriginal Health and Medical Research Council n.d., Aboriginal Outreach Worker (AOW) orientation workshop, Final report, AHMRC, Sydney.260 Victorian Aboriginal Community Controlled Health Organisation 2011, Victorian Aboriginal Outreach Worker orientation program, Final report, VACCHO, Melbourne.261 Aboriginal Health Council of South Australia 2011, Aboriginal and Torres Strait Islander Outreach Worker (ATSIOW) orientation development and training, Final report, AHCSA, Adelaide.262 Aboriginal Health Council of Western Australia 2011, Orientation training for ATSIOWs, Final report, AHCWA, Perth.263 ibid.
246KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The national workshop attracted 121 participants, including 87 ATSIOWs, 14 IHPOs funded under the ICDP C2 and C3 measures and other staff affiliated with relevant organisations. The majority (71 per cent) of participants were based in mainstream primary health care organisations (Divisions of General Practice or SBOs), with the remainder (29 per cent) located in the Aboriginal community controlled sector (Aboriginal Community Controlled Health Services or NACCHO affiliates).264 ATSIOW training
Funding of ATSIOW training (that is, training other than orientation and the national workshop) commenced in 2010-11. In order to receive training, an ATSIOW’s training needs are first identified through discussions between the employer and the ATSIOW. When that has been agreed and an appropriate training provider has been identified, the employer contacts the NACCHO affiliate or SBO of the relevant DoGP. Proposals for training are then forwarded to the department by the NACCHO affiliate or SBO. The department provides funds directly to the NACCHO affiliate or SBO, who coordinate the payment of funds to the identified registered training organisation. The assessed need for training for different ATSIOWs is seen to be dependent on their existing skills and backgrounds (as per their own perceptions and those of their managers). The experiences and skills of ATSIOWs engaged with during the site visits varied significantly, with some having clinical and health backgrounds and others having relationships with the community but no experience in health. Although the ATSIOW role is non-clinical, many ATSIOWs had or planned to undertake clinical training, and were taking on some clinical duties such as simple care coordination (such as making referrals).Not all ATSIOWs may need or desire training as despite the role being an entry level position, approximately 80 per cent of ATSIOWs already have qualifications of Certificate III and above, with 40 per cent holding qualifications at above Certificate III level.265 The majority of the 11 ATSIOWs consulted during site visits had participated in numerous training courses, including basic training such as first aid and occupational health and safety, and health and public health focused training such as sexual health, Smoke Check and Quality Use of Medicines (QUM). Two ATSIOWs in regional areas said it was hard to access training due to limited funding.Access to Certificate III and some Certificate IV training in health-related disciplines was considered invaluable by the majority of ATSIOWs and
264 National Aboriginal Community Controlled Health Organisation n.d., Aboriginal and Torres Strait Islander Outreach Workers National Workshop Report, June 21-22nd 2011, NACCHO, Canberra.265 Internal email from Measure Manager to ICDP Evaluation Unit (28 Oct 2011), Follow up to Mondays meeting with KPMG re: ICDP Evaluation.
247KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
managers consulted through the site visits, as this training is seen to directly relate to the role requirements of the ATSIOWs and thus to support them to perform their role. Although a significant proportion of ATSIOWs already have Certificate qualifications, ATSIOWs may be supported through this measure to pursue a higher level of qualification to the level of Certificate III266 and/or new qualifications (i.e., different in focus to their existing qualifications). Therefore, even for those with existing qualifications, the training can be seen as relevant. Two of the ATSIOWs consulted had completed a Certificate III (one in Health, one in Aboriginal Health) and will be completing Certificate IV.267 They reported that this had been supported by their workplaces, in terms of encouragement and in providing financial support for incidental costs associated with training, which some organisations charge. Preliminary findings suggest that the ability to participate in training is considered attractive by many ATSIOWs. Some ATSIOWs and managers consulted made the link between being able to develop their skills and the sustainability of their position, i.e., they would be more likely to stay in the role if there were adequate professional development opportunities. However, many also raised the issue of the positions being time-limited contracts, and linked this to negative impacts on sustainability (i.e., they considered that the short-term nature of the contracts would lead to people being less inclined to continue working in their role). A couple of stakeholders considered that, compared with existing health worker positions, there was no established career path for ATSIOWs.A few stakeholders reported difficulties with ATSIOWs accessing training. Mainstream organisations reported that some Tasmanian ATSIOWs cannot access health worker training provided by the TAC, so have an agreement in place to receive development support from Victoria. Others attended training in Sydney. In New South Wales, one stakeholder based outside the capital city reported difficulties in finding adequate funding for flights and accommodation to participate in training in Sydney. However, it is understood that ICDP funding for this activity has included travel costs. The issue was not raised by other stakeholders consulted on this measure. It may be that there is a lack of clarity or understanding about the existing provisions for training in isolated cases.Two organisations in regional areas, two SBOs and some national stakeholders considered ATSIOW funding to be inadequate for the costs of both salaries and training. It is understood that funding for salaries and training is provided under separate ICDP measures, and it is not clear to what extent stakeholders 266 Only some modules in the Certificate IV are considered relevant to the ATSIOW role. This measure supports the attainment of qualifications up to a Certificate III; other funding must be sought for support to attain a Certificate IV or higher.267 Australian Government, State and Territory Governments 2012, Training.gov.au (website), viewed 3 December 2012.
248KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
are amalgamating funding. Stakeholders reported that training costs largely fell on employers. In some cases, a few ATSIOWs reported that training was restricted due to costs (direct and indirect, such as travel to training locations and days off). At many Regional Forums, participants thought there were opportunities to improve the training available for staff through the ICDP. Participants reported that the training is currently poorly coordinated, and varies in its accessibility. They suggested conducting coordinated needs analyses to understand what training is required across locations and providing more targeted, accessible training. Many Regional Forum participants said that the ICDP workforce values networking opportunities and suggested that a strategic approach to promote networking for all workforce components may be warranted. The strategy could consider options to provide more networking opportunities, ways of sharing local innovations that could have relevance for other regions and options for integrating ICDP workforce groups into the broader Aboriginal and Torres Strait Islander workforce.1.67 GP registrar training postsThe evaluation found that there has been considerable uptake of the GP registrar training posts in IHSs in 2010-11, but low awareness amongst stakeholders about the availability of these posts. The training posts may also be impacted by the limited number of qualified GPs available to supervise them. These findings are based on data on GP registrar training post placements provided by the department, consultation with the department, and consultation with NACCHO, NACCHO affiliates, SBOs and IHSs. On 1 January 2010, funding for 38 GP registrar placements was added to the pre-existing Aboriginal and Torres Strait Islander Health Training Posts program. Because the Workforce Support, Education and Training measure funding added to an existing program, GP placements began immediately. In the 2010 calendar year, 46 placements were made (above the 2008 baseline), indicating subscription beyond the expected levels. In 2010-11, $2.014 million was spent on the GP registrar training posts, with the placement of GP registrars in 38 additional training posts.Placement results indicate good subscription to the placement program, but stakeholders indicated that capacity constraints in IHSs limit the number of qualified GPs available to supervise GP registrars in the training posts, which may impact on the quality or value of the training posts. None of the stakeholders consulted through community site visits were aware of the GP registrar training posts. This could be due to limited promotion of this scheme and/or the fact that these posts existed prior to ICDP and are thus not seen as an ICDP initiative.
249KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.68 Nursing and midwifery scholarships The evaluation found that nursing and midwifery scholarships were under-subscribed in 2010-11, and awareness of the scholarships was low amongst stakeholders consulted. These findings are based on data provided by and consultations with the department and the fund holder (the Royal College of Nursing Australia), NACCHO and affiliates, SBOs and IHSs.The first round of nursing and midwifery scholarships occurred in the 2010-11 year, with the initial application period occurring from August to October 2010. These are postgraduate scholarships for registered and enrolled nurses or midwives working in an IHS to undertake professional development at an Australian university or RTO; 268 and clinical placement scholarships to support students enrolled in an approved undergraduate or entry level nursing or midwifery course to undertake a clinical placement in an IHS.269
The department has provided funding for 50 professional development scholarships and 50 clinical placement scholarships annually. However, these were not fully subscribed in 2010 or 2011.Table 63 below identifies the number of scholarships that were provided in 2010 and 2011 by jurisdiction. Note that these are tracked per calendar year.Table 63: Number of nursing and midwifery professional development and clinical placement scholarships provided, 2010 and 2011 calendar years, by state or territory.270
Jurisdiction
Professional development scholarships
2010
Professional development scholarships
2011
Clinical placement
scholarships 2010
Clinical placement
scholarships 2011
NSW 4 9 16 10QLD 4 6 5 3
268 Described as “Postgraduate Scholarships for nurses working in an Aboriginal Medical Service” in: Royal College of Nursing Australia 2011, Nursing and Allied Health Scholarship Support Scheme Progress Report For the period of 1 July 2010 – 31 December 2010, RCNA, Australia, p. 3. 269 Described as “Clinical Placement Scholarship undertaking in an Aboriginal Medical Service” in Royal College of Nursing Australia 2011, Nursing and Allied Health Scholarship Support Scheme Progress Report For the period of 1 July 2010 – 31 December 2010,RCNA, Australia, p. 3. 270 Royal College of Nursing Australia 2011, Nursing and Allied Health Scholarship Support Scheme Progress Report For the period of 1 July 2010 – 31 December 2010, RCNA, Australia; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
250KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Jurisdiction
Professional development scholarships
2010
Professional development scholarships
2011
Clinical placement
scholarships 2010
Clinical placement
scholarships 2011
WA 5 6 4 6NT 6 13 1 0VIC 1 5 7 1SA 1 3 3 2TAS 0 1 1 0ACT 0 0 1 0Totals 21 43 38 22
As Table 63 shows, the total number of clinical placement scholarships decreased from 38 to 22 between 2010 and 2011, whereas the total number of professional development scholarships increased from 21 to 43 over the same period. At this stage, the reason for these changes is unclear. The demand for either scholarship did not reach the target number; therefore, all eligible applicants received a scholarship. Almost 10 ineligible applications were received for each scholarship type in 2010-11.As for the GP registrar training posts, few of the stakeholders consulted (both through site visits and other consultations) were aware of the nursing and midwifery professional development and clinical placement scholarships. Lack of adequate promotion was suggested as a reason for this by national stakeholders and health services engaged through the site visits. There also appeared to be some confusion amongst health workers engaged through the site visits between these scholarships and the Puggy Hunter Scholarship Scheme, a scholarship scheme for Aboriginal and Torres Strait Islander people studying health related disciplines271, which seemed better known.1.69 Facilitators and barriers The following barriers and facilitators to the implementation and operation of the Workforce Support, Education and Training measure have been identified by the evaluation to date.Facilitators: Existing GP registrar training posts and nursing and midwifery scholarships.
The GP registrar training posts in IHSs, and the AMS professional
271 Eligible health areas include: Aboriginal health worker; Allied health (excluding pharmacy); Dentistry/oral health (excluding dental assistants); Medicine; Midwifery; and Nursing.
251KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
development and clinical placement nursing and midwifery scholarships, were added to existing national programs for training posts and scholarships already administered by the fund holders, GPET and the RCNA. This enabled both components to be implemented relatively quickly, and to take advantage of existing infrastructure. However, this may also contribute to the low level of awareness of both components amongst stakeholders, since they were not new or clearly distinguished from existing offerings.
Barriers: ATSIOW participation in orientation. While the department contractually
expected ATSIOWs to receive orientation within six months of the commencement of their employment, this standard has not generally been met. Departmental staff consider contributing factors to include the lengthy consultation process undertaken to develop orientation packages, delays in ATSIOW recruitment that meant people were recruited after the orientation session had been run, the desire to assemble a ‘critical mass’ of participants for each orientation session, and the turnover of ATSIOWs.272 As discussed previously, accessibility of training (including orientation) can be an issue in some locations.
Recruitment challenges. Community site visit consultations highlighted common challenges across the ICDP measures in attracting staff to work in Aboriginal and Torres Strait Islander health, including to ATSIOW positions. A number of national stakeholders pointed out that there is no ICDP workforce plan to address this and related issues such as recruiting to different ICDP measures from a limited pool of workers. This issue is discussed in more detail in the following chapters.
Support for GP Registrar Training Posts. An issue raised during the national stakeholder consultations is the inadequate numbers of qualified GPs in IHSs available to supervise registrars. This is a broader systemic issue in the IHSs sector.
Brand and identity of nursing and midwifery scholarships. As noted above, the nursing and midwifery scholarships offered under the Workforce Support, Education and Training measure are not yet well known or distinguished from pre-existing scholarships which also support learning and working in Aboriginal and Torres Strait Islander health.
1.70 OpportunitiesOpportunities to strengthen the Workforce Support, Education and Training measure in the future include:
272 Internal email from Measure Manager to ICDP Evaluation Unit (28 October 2011), Follow up to Mondays meeting with KPMG re: ICDP Evaluation.
252KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Coordinated ICDP workforce training strategy. Some Regional Forum participants and national stakeholders consulted stated that a comprehensive needs analysis and strategy for ongoing training across the ICDP for new roles including ATSIOWs, IHPOS and Care Coordinators, is required. Such an analysis could identify common needs by position, sectors and/or geographic location, leverage synergies between ICDP measures, support networking and sharing of learning across the ICDP workforce, and identify options for integrating ICDP workforce groups into the broader Aboriginal and Torres Strait Islander workforce. It could also inform the development of a clear career pathway to support ATSIOWs to develop their skills and competencies while being retained in the Indigenous health sector.
Promotion of ATSIOW individualised training component. The evidence suggests that there is scope to improve the awareness and understanding of the ATSIOW individualised training component of the measure amongst SBOs, employing organisations and ATSIOWs. This should include the items which training support covers (i.e., travel and training), eligibility and relevant training providers (e.g., a list of available registered training organisations offering relevant training within their jurisdiction on the ICDP website).
Improved promotion of available scholarships and training opportunities through the Workforce Support, Education and Training measure for GPs, nurses and midwives. This may include promotion to students and to existing workers within the Aboriginal and Torres Strait Islander health sector. Potential promotional avenues include through peak organisations and other organisations with a membership base, and direct promotion to primary health care services such as pamphlets and fact sheets. This should include clear branding of both the training posts and scholarships in a way which distinguishes them from pre-existing programs and emphasises their focus on Indigenous chronic disease.
253KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expanding the Outreach and Service Capacity of Indigenous Health Organisations (C2)This chapter describes the progress of the Expanding the Outreach and Service Capacity of Indigenous Health Organisations (C2) measure in 2010-11. In this chapter, we discuss the measure’s achievements, activities, facilitators, barriers, signs of progress towards desired outcomes and opportunities for the future. Expanding the Outreach and Service Capacity of Indigenous Health Organisations at a glanceActivities in 2010-11 were predominantly focused on recruitment, which proceeded generally as planned. In total, 70.4 FTE ATSIOWs, practice managers and other health workers were recruited under this measure up to the end of 2010-11. Workforce allocation and recruitment were on track in 2010-11, however, there is no data to inform an understanding of how quickly positions were filled (or how long left vacant) or retention of this workforce. Consultations with workers, organisation and national level stakeholders suggest that recruitment has been slow in some locations, and turnover, particularly of ATSIOWs, has been significant. Some barriers to recruitment and retention have been suggested to the evaluation, including job uncertainty associated with contract-based positions, and a limited pool of potential recruits. The true nature and extent of these barriers is unknown at this stage. There is some limited emerging evidence to suggest that ATSIOW positions can increase Aboriginal and Torres Strait Islander people’s awareness of available health services, due to promotion activities undertaken by ATSIOWs of ICDP and non-ICDP services, programs and initiatives. There is also some limited emerging evidence of increased access to health care within IHSs by Aboriginal and Torres Strait Islander people due to ATSIOWs linking patients to services they require.At this stage, no information is available about the impact of practice managers or other health workers. The total expenditure for this measure was $13.508 million in 2010-11.1.71 Potential effects based on implementation findingsFigure 22 below is the causal pathway for the Expanding the Outreach and Service Capacity of Indigenous Health Organisations measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
254KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expanding the Outreach and
Service Capacity of Indigenous Health
Organisations
Increase in IHSs’ capacity to provide outreach support to
Aboriginal and Torres Strait
Islander patients
Aboriginal and Torres Strait
Islander people increase their utilisation of
primary health care services
Increase in IHSs’ capacity to deliver primary health care
services
Increase in IHSs’ capacity to manage
non-clinical functions
Improvements in IHSs’ infrastructure to accommodate staff and deliver
services
Practice Managers are effective in
reducing non-clinical duties of clinical health
staff
ATSIOWs are effective in facilitating
Aboriginal and Torres Strait
Islander people’s access to primary
health care services
Recruitment and retention of ATSIOWs, Practice
Managers and additional health
professional positions
Figure 22: Expanding the Outreach and Service Capacity of Indigenous Health Organisations causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect273 and the observed impacts.274 Both the plausibility and observed
273 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.
255KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. Table 64 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the measure and it was largely implemented according to plan in 2010-11, therefore, the plausibility of effect is not affected. Information is available for some of the key dependencies and suggests that staff turnover may limit the impact of this measure and its sustainability. The main factor influencing the implementation of this measure observed in the reporting period is the recruitment challenges in filling additional positions funded under the measure. The capacity of Indigenous health services (IHSs) to absorb, support and make best use of the workforce enhancements and capital infrastructure provided is also likely to be an external factor impacting on the implementation of the measure.
274 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
256KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 64: Assessment of key dependencies of the C2 measure.
Key dependencies
Findings Evidence
Recruitment and retention of ATSIOWs, Practice Managers and additional health professional positions
Recruitment proceeded as planned although it appears that recruitment has taken longer than expected and turnover, particularly of ATSIOWs, has been significant in some locations.
This is based on data provided by and consultations with the department, stakeholder feedback at Regional Forums and consultations with a small number of workers, organisations and national stakeholders
ATSIOWs are effective in facilitating Aboriginal and Torres Strait Islander people’s access to primary health care services
Some indications that ATSIOW positions have increased Aboriginal and Torres Strait Islander people’s awareness of available health services; and some indication of increased access to health care due to ATSIOWs linking patients to services they require.
This is based on community focus groups and consultations with a very small number of workers and organisations
Practice Managers are effective in reducing non-clinical duties of clinical health staff
Data is not available for the First Monitoring Report.
Not applicable
257KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Contextual considerations
Geographical accessibility is one of a number of factors influencing recruitment. For example, lifestyle preferences, reduced opportunities for professional development and accommodation constraints are barriers to recruiting workers in rural and remote locations, which are frequently identified as a recruitment issues in the literature. The organisational capacity and leadership support available within IHSs may vary significantly, and is likely to be less in smaller organisations. This may impact on the effectiveness of ATSIOWS, and issues such as retention of staff in some locations.
Literature review
below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). The evaluation found that the measure contributed to an increase in IHS capacity to provide outreach and primary health care services, and improved IHS infrastructure to accommodate staff and deliver services. Delays in recruitment, turnover of staff and substitution of existing roles could limit these effects. Contextual factors influencing the operation of the measure are recruitment challenges and variable capacity of IHSs to absorb and make best use of the additional workforce funded under this measure.
258KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 65: Assessment of expected and observed impacts of the C2 measure based on implementation progress.
Expected Observed impacts EvidenceIncrease in IHS capacity to provide outreach support to Aboriginal and Torres Strait Islander patients
Recruitment of staff in IHSs is likely to have increased capacity. Delays in recruitment, turnover of staff and substitution of existing roles could all limit this effect.
This is based on data provided by the department, and qualitative information from consultation with community members through a focus group
Increase in IHS capacity to managed non-clinical functions
Data is not available for the First Monitoring Report.
Not applicable
Improvements in IHS infrastructure to accommodate staff and deliver services
Capital work programs on track to increase relevant infrastructure.
This is based on data provided by the department
Increase in IHS capacity to delivery primary health care services
Increase in staff likely to result in increased capacity.
This is based on consultations with a small number of IHSs
Aboriginal and Torres Strait Islander people increase their utilisation of primary health care services
Empirical information not available for the First Monitoring Report, although some indications that the new workforce has resulted in individual patients reconnecting with their primary health care service.
This is based on consultations with a small number of IHSs
259KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected Observed impacts EvidenceContextual considerations
The factors influencing recruitment highlighted previously as being experienced by IHSs are the key contextual consideration observed in the reporting period; consultations suggest that many IHSs have experienced delays in recruiting this workforce.The apparently variable capacity of IHSs to absorb and make best use of the additional workforce funded under this measure is also likely to impact on the implementation of the measure.
This is based on consultations with a small number of IHSs
260KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.72 Measure overviewThe Expanding the Outreach and Service Capacity of Indigenous Health Organisations (C2) measure is predominantly a workforce measure providing for the recruitment of ATSIOWs, practice managers and other health workers (including GPs, nurses and AHWs) to IHSs (collectively referred to hereafter within this report as the C2 workforce). It includes some investment in; infrastructure to support the health workforce, such as staff housing in remote communities; and to the meeting costs of the National Aboriginal and Torres Strait Islander Health Equality Council (NATSIHEC). NATSIHEC is an advisory body to the Minister of Indigenous Health which provides advice on the implementation of the ICDP overall. The measure closely links to the Engaging Divisions of General Practice to Improve Indigenous Access to Mainstream Primary Care (C3) measure which provides a similar workforce within Divisions of General Practice. The 2010-11 total expenditure was $13.507 million for this measure. 1.73 Workforce enhancement While there was considerable progress with the recruitment to funded positions, consultations suggest that staff turnover may have had a negative impact on the overall workforce numbers. Funding for the first phase of the C2 workforce was provided in February 2010. Forty-seven IHSs received funding in 2010-11 to employ ATSIOWs, practice managers and other health workers (this total includes IHSs which also received funding in 2009-10). below provides a profile of recruitment, with comparison of allocated positions with actual recruitment. Note that these figures represent cumulative totals from February 2010 to 30 June 2011. The following points need to be noted when interpreting this data: differences between allocation and recruitment may be due to late
allocation of positions in the financial year; and recruitment numbers may be low due to turnover of staff.
261KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 66: Number of C2 workforce FTE, allocated (A) and actual recruitment (R), to 30 June 2011, by jurisdiction.275
Jurisdiction
ATSIOW (A)
ATSIOW (R)
Practice Managers (A)
Practice Managers (R)
Other health workforce (A)
Other health workforce (R)
Totals (A)
Totals (R)
NSW 8 8 6 6 1.1 1.1 15.1
15.1
QLD 9 9 5.6 5 2.4 2.4 17.0
16.4
WA 9 7 2.7 2.7 2.7 2.7 14.4
12.4
NT 6 6 2.4 2.4 4.8 4.8 13.2
13.2
VIC 5 4 1.3 1.3 0.8 0.8 7.1 6.1SA 2 1 1.1 1.1 2 2 5.1 4.1TAS 1 1 1 1 0 0 2 2ACT 1 1 0 0 0 0 1 1Totals 41 37 20.1 19.5 13.8 13.8 74 7
0.4
As the data in above shows, the majority of IHSs that received funding in 2010-11 were able to recruit to the funded positions. It is important to note, however, that the data presented in is cumulative and does not show the timing of recruitment, nor turnover. Therefore, it cannot provide information about the time between allocation of funding to an organisation and recruitment or the retention of recruited positions.Tasmania became a signatory to the National Partnership Agreement on Closing the Gap in Indigenous Health Outcomes in 2010-11, and became eligible for workforce under the ICDP thereafter. In March 2010 an additional 1.5 FTE ATSIOW positions were created in Tasmania and funded in 2010-11.In 2010-11, the department commenced planning for the 2011-12 workforce through consultation with Indigenous Health Partnership Forums in each jurisdiction. As only six staff (ATSIOWs, practice managers and their line managers) working at three IHSs were consulted during the data collection phase for this report, the qualitative evidence is somewhat limited. The majority of ATSIOWs 275 Based on information provided by the Department of Health and Ageing 2011; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
262KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
consulted in this phase were employed within the mainstream sector (in Divisions of General Practice) under the Engaging Divisions of General Practice to Improve Indigenous Access to Mainstream Primary Care (C3) measure. Further, few IHSs visited engaged during the evaluation had recruited practice managers or other health workers, and the practice managers consulted were very new to the role and therefore could not provide much information about their role or activities. Information gathered through community site visits and Regional Forums suggests that recruitment may have taken longer than expected in some IHSs, and in particular there were difficulties recruiting male ATSIOWs. There was also some suggestion of high turnover within ATSIOW positions (across both the mainstream and IHSs); some workers consulted during the evaluation were the second or third person to fill the position. One organisation reported that low numbers of potential candidates (Aboriginal and Torres Strait Islander or people with strong community connections) for the positions contributed to recruitment difficulties. Reasons identified for retention challenges included worker burn out, and workers leaving ATSIOW positions to take up other opportunities. Due to high demand for services from their target populations, the IHSs consulted during the community site visits valued having additional staff (chiefly ATSIOWs) to support them in meeting client demand. Activities of the C2 workforce
The activities undertaken by the C2 workforce vary according to role and in part local context with the priority focus being on engaging communities and promoting local health services and other aspect of ICDP. One ATSIOW and one ATSIOW manager (in different IHSs) engaged through the site visits reported that the ATSIOW had promoted ICDP initiatives to patients such as the Practice Incentives Program (PIP) Indigenous Health Incentive and the PBS Co-payment measures. These findings are complemented by the findings of Regional Forums, which several ATSIOWs attended. The ATSIOWs commented that they had used opportunistic mechanisms to promote the ICDP and access to health care more generally, for example through talking with patients when they come in for appointments. The ATSIOWs also engaged with and supported clinical staff, for example, in delivering smoking cessation programs. These limited consultations with ATSIOWs and their managers suggest that Aboriginal and Torres Strait Islander community members may have increased awareness of available health services within the site visit locations. Both ATSIOWs and other staff attributed this to the work that ATSIOWs had done in promoting services and linking people in with services. For example, IHS staff in one location reported increased attendance by community members at diabetes management sessions, a program which the ATSIOW (in conjunction with other IHS staff) had promoted.
263KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Two national stakeholders consulted for this report reported that ATSIOWs were undertaking community engagement and some clinical tasks, although the latter are not part of the ATSIOW position description. Examples include care coordination, such as making referrals to internal and external health programs and services. There was a perception from these stakeholders that this was occurring because some ATSIOW positions were being filled by people with AHW level skills. These stakeholders identified a risk that AHWs who do not continue providing clinical tasks (i.e., in roles such as ATSIOW roles) will lose their skills over time, unless they continue to perform clinical duties.Of the two newly recruited practice managers consulted for the evaluation, only one was funded by the ICDP. This practice manager indicated s/he intended to promote the role of chronic disease management, the uptake of Medicare items and the ICDP more broadly.Practice managers also planned to link in with other components of the ICDP, such as by supporting Care Coordinators and working with ATSIOWs in undertaking health promotion tasks. However, at the time the site visits were conducted, these practice managers were yet to commence these tasks. There is very limited data to inform a view around patient engagement. In one focus group, community members who accessed the local IHS reported that the ATSIOW (identified by name) had encouraged them to access the various health services provided by that IHS, including health checks and healthy lifestyle and smoking cessation activities. One IHS reported that the majority of their patients were registered for the PIP Indigenous Health Incentive, which the ATSIOW had been actively promoting within the community. Another reported increased utilisation of healthy lifestyle programs that the ATSIOW was involved with, such as anti-smoking programs run out of one IHS. 1.74 Capital worksThe 2010-11 year saw the continuation of capital works projects originally funded in 2009-10. Table 67 below lists the selected projects funded under the Expanding the Outreach and Service Capacity of Indigenous Health Organisations measure.
264KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 67: Capital works projects funded by the Expanding the Outreach and Service Capacity of Indigenous Health Organisations measure, by jurisdiction, to 30 June 2011.276
Jurisdiction
Location Description of project Project status 2010-11
NSW Grafton New health administration facility
Property purchased
NSW Tamworth Refurbishment of property for use as medical facility
Mid-construction
QLD Bamaga Three new staff houses Construction to commence in 2011-12
WA Wiluna New clinic and staff housing Construction commencedWA Kiwirrkurr
aNew clinic and staff house Mid construction
NT Galiwinku New staff house Completed 3 May 2011VIC Mooroopn
aClinic extension Mid construction
SA - - -TAS - - -ACT - - -
1.75 Facilitators and barriers The following facilitators to the implementation and operation of the Expanding the Outreach and Service Capacity of Indigenous Health Organisations measure have been identified by the evaluation to date:The site visits highlighted what may be common critical success factors for the C2 workforce – and specifically for ATSIOWs. These include key design features of the ATSIOW role - being well connected within the community and/or being Aboriginal or Torres Strait Islander, and being located within the IHS, were considered to be appropriate and to support the aims of the measure. Stakeholders reported that there are many non-ICDP positions that are similar to the role of the ATSIOW within IHSs, meaning there are opportunities to create linkages and leverage off existing programs. One potential risk with the placement of ATSIOWs in organisations which already have similar positions is duplication of effort.
276 Based on information provided by the Department of Health and Ageing 2011; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.
265KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Other facilitators identified for ATSIOWs included: Taking time to build trust with individuals and groups. Where ATSIOWs
initially focused on building good relationships with the community members they were working with, they were reportedly more successful in engaging them.
Working closely with other staff in the service, with other services and within the local community. This is seen to support the ATSIOW to build on pre-existing relationships they have with services, and allow each to contribute a range of complementary skills to a patient’s care.
The following barriers relevant to this measure have been identified by the evaluation: Difficulties recruiting due to time limited positions. The available workforce
data does not capture how long positions were vacant before being filled or how long people stay in their role. IHSs engaged through the site visits, which were located in both urban and outer regional locations, reported having some difficulties in recruiting ATSIOWs, particularly male workers. The recruitment of practice managers may also have been challenging, given that the practice managers interviewed were all were new at the time of consultations. According to some national stakeholders and IHS staff, the fact that positions are time limited (IHSs were reportedly using contracts of between one and three years in length) is a constraint on recruitment, as non-permanent positions are seen as less attractive to potential employees.
Broad scope of the ATSIOW role. Stakeholders noted that the ATSIOW role is broad in scope. This has reportedly led to confusion about the focus, boundaries and responsibilities of the role. However, the breadth of the ATSIOW position description was considered to be positive in other ways, as it enables ATSIOWs to tailor the role to their skills and experiences and the needs of their target population. National stakeholders and those at Regional Forums commented that positions were funded on the assumption that one person can serve an entire region, which is unrealistic, particularly in large regional or remote areas. This is not necessarily a valid criticism of this measure; ATSIOWs are placed within established organisations which are likely to have other, complementary mechanisms to engage people across their catchment area.
Impact of ATSIOW recruitment on the broader Aboriginal and Torres Strait Islander health workforce. There have been anecdotal reports (made both directly to the department and to evaluation) that recruitment of the ATSIOW positions (in both mainstream and IHSs) is depleting the ranks of the existing Aboriginal and Torres Strait Islander health workforce, and AHWs specifically.
266KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
A small number of national stakeholders raised concerns that ATSIOW positions (which are supposed to be entry level) were being advertised by some organisations with higher salaries than AHW positions (which require specific qualifications and skills). The disparity in pay may encourage people to leave AHW positions for ATSIOW positions. This would undermine the aim of the ICDP to enhance the workforce overall, and could result in workers be de-skilled over time. It was reported to the evaluation that at least one IHS had deliberately targeted AHWs for ATSIOW positions because they had experience and skills which could be applied in the ATSIOW role. It is difficult to determine the nature and extent of this issue based on the information available to inform this report. However, it should be noted that the department does not specify a salary for ATSIOWs, but rather provides organisations with a set funding amount from which they draw the salary. The department reported that their intelligence indicates that these are isolated instances rather than representative of a systematic issue.277
Lack of an overarching workforce strategy. As discussed in relation to the Workforce Support, Education and Training (C1) measure, stakeholders engaged in Regional Forums and through community site visits said the absence of an overarching ICDP workforce strategy led to difficulties for each of the measures which fund new workforce positions (such as ATSIOWs, IHPOs and Care Coordinators).
1.76 Opportunities Potential opportunities to strengthen the Expanding the Outreach and Service Capacity of Indigenous Health Organisations measure in the future include: Providing further networking opportunities for ATSIOWs. To address
confusion about the scope of the ATSIOW role, to support ATSIOWs with a view to sustaining the workforce, and to help gain traction quickly, additional and more frequent networking opportunities could be provided which allow the department to clarify expectations and offer other relevant support and professional development.
Improved collection of data. Current administrative data held by the department does not provide information on the length of time it takes to recruit to C2 workforce positions in IHSs, nor on the length of time that incumbents stay in the role (i.e., retention). An opportunity exists to improve the understanding of the operation of this measure through collecting this data.
277 KPMG consultation with measure manager (November 2011). 267
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Improving Indigenous Access to Mainstream Primary Care Program (C3)This chapter describes the progress of the Improving Indigenous Access to Mainstream Primary Care Program. In this chapter we discuss the implementation of the measure in 2010-11, the second year of the ICDP, including achievements, activities, facilitators, barriers, signs of progress towards desired outcomes, and opportunities for the future. Improving Indigenous Access to Mainstream Primary Care at a GlanceThe evaluation found that the Improving Indigenous Access to Mainstream Primary Care measure was ‘on track’ in 2010-11 in terms of workforce and program support components. The data available on recruitment of Aboriginal and Torres Strait Islander Outreach Workers (ATSIOWs) and Indigenous Health Project Officers (IHPOs) suggests recruitment was strong and exceeded departmental expectations. The extent of staff retention is unknown. The activities being undertaken by ATSIOWs and IHPOs align with guidelines and position descriptions, and, while the roles are distinct, many examples were provided of these two positions working together to support improvements to Aboriginal and Torres Strait Islander self identification, cultural competency of mainstream primary health care providers, and increased access to health care services by Aboriginal and Torres Strait Islander people. There is emerging evidence to suggest that teams of IHPOs and ATSIOWs have supported increased access to primary health care services for some Aboriginal and Torres Strait Islander people. The measure appears to be supporting increased collaboration between the IHS and mainstream primary health care sectors and collaboration at the jurisdictional level around the ICDP, however, in some locations barriers exist including perceived competition for funding and positions, and reluctance from some stakeholders to engage across the sectors.During 2010-11 a number of program supports were successfully implemented for IHPOs and ATSIOWs including resources, and opportunities for networking. 1.77 Potential effects based on implementation findingsFigure 23 below is the causal pathway for the Improving Indigenous Access to Mainstream Primary Care measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
268KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Mainstream primary health care practices change their
practices in order to provide culturally
sensitive care
Aboriginal and Torres Strait
Islander patients engage with mainstream
primary health care practices
ATSIOWs are effective in facilitating
Aboriginal and Torres Strait
Islander people’s access to
mainstream primary health care practices
Recruitment and retention of
ATSIOWs and IHPOs
IHPOs are effective in
implementing initiatives that address access barriers and
promote culturally
sensitive care
Improving Indigenous Access
to Mainstream Primary Care
Increase in capacity to provide support to Aboriginal and
Torres Strait Islander patients
Aboriginal and Torres Strait
Islander people increase their utilisation of mainstream
primary health care services
Increase in capacity of mainstream
primary health care practices to deliver culturally sensitive primary health care
services
Reduced barriers to culturally sensitive
care
Figure 23: Improving Indigenous Access to Mainstream Primary Care causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility
269KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
of effect278 and the observed impacts.279 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. Table 68 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). There have been no significant changes to the design of the measure. It was implemented according to plan in 2010-11; therefore, the plausibility of effect is not affected. Information is available for some of the key dependencies which suggests that staff turnover may limit the impact of this measure and its sustainability. The main factors that could influence this measure are the capacity and capability of the workforce to address community need, the organisational readiness and cultural safety of DoGPs to host and support the C3 positions and organisational links between DoGPs and general practices. The transition to Medicare Locals, which required time and focus from DoGPs, may have diverted attention from the implementation of this measure. Table 68: Assessment of key dependencies of the C3 measure.
Key dependencies
Findings Evidence
Recruitment and retention of ATSIOWs and IHPOs
Recruitment is on target. The growth in recruitment was particularly significant in 2010-11, with over 50 FTE recruited in this fiscal year. The level of retention is unclear as relevant data is unavailable. However, several DoGPs reported difficulties in the recruitment and retention of ATSIOWs.
This is based on program documentation, recruitment data provided by the department, and qualitative information from consultations with DoGPs, IHPOs and ATSIOWs
278 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.279 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
270KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
ATSIOWs are effective in facilitating Aboriginal and Torres Strait Islander people’s access to mainstream primary health care practices
ATSIOWs have the required skills to fulfil their roles. There are indications that ATSIOWs have supported increased access to mainstream primary health care services for some Aboriginal and Torres Strait Islander people.
This is based on qualitative information from consultations with national stakeholders (relevant peak and representative organisations), ATSIOWs, IHPOs and primary health care providers, and community focus groups
IHPOs are effective in implementing initiatives that address access barriers and promote culturally sensitive care
IHPOs have the required skills to fulfil their roles. There are indications that IHPOs have supported increased access to mainstream primary health care services for some Aboriginal and Torres Strait Islander people.
This is based on qualitative information from consultations with national stakeholders (relevant peak and representative organisations), ATSIOWs, IHPOs and primary health care providers, and community focus groups
271KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Mainstream primary health care practices change their practices in order to provide culturally sensitive care
Many practices are making changes to their processes and procedures including: now consistently asking patients
about their Aboriginal and Torres Strait Islander status;
implementing recall and reminder systems for Aboriginal and Torres Strait Islander patients;
proactively signing up patients to the PIP Indigenous Health Incentive and the PBS co-payment measure; and
undertaking cultural awareness training.
There are indications that these practice changes are not universal across practices.
This is based on analysis of a non-representative sample of 20 fund holder reports from a variety of jurisdictions, and qualitative information from consultations with ATSIOWs, IHPOs and primary health care providers
Aboriginal and Torres Strait Islander patients engage with mainstream primary health care practices
There are indications that IHPOs and ATSIOWs have supported increased access to primary health care services for some Aboriginal and Torres Strait Islander people.
This is based on a review of the literature (empirical), qualitative information from consultations with national stakeholders (relevant peak and representative organisations), ATSIOWs, IHPOs and primary health care providers, and community focus groups
Contextual considerations
Geography influences recruitment. For example, lifestyle preferences, reduced opportunities for professional development and accommodation constraints are barriers to recruiting workers in rural locations, which are frequently identified as a recruitment issue in the literature.
Literature review
272KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
273KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). There is evidence of increased practice capacity to provide culturally sensitive care and support to Aboriginal and Torres Strait Islander patients, in line with the requirements of registration for the PIP Indigenous Health Incentive (B3a measure). There are also indications of increased utilisation of mainstream primary health care services, but insufficient data to link this to the activities of this measure. Contextual factors influencing the operation of this measure are the organisational readiness and cultural safety of Divisions of General Practice which employ this new workforce.Table 69: Assessment of expected and observed impacts of the C3 measure based on implementation progress.
Expected Observed impacts EvidenceReduced barriers to culturally sensitive care
There are indications of increased capacity in terms of culturally sensitive care, and that there is still scope for this to be further enhanced across the system. Main indications of increase capacity relate to the criteria for PIP Indigenous Health Incentive registration: practices asking patients about
their Aboriginal and Torres Strait Islander status;
improved recall and reminder systems for Aboriginal and Torres Strait Islander patients;
signing up patients to the PIP Indigenous Health Incentive and the PBS co-payment measure; and
cultural competency.
This is based on analysis of a non-representative sample of 20 fund holder reports from a variety of jurisdictions, and qualitative information from consultations with ATSIOWs, IHPOs and primary health care providers
Increase in capacity of mainstream primary health care practices to deliver culturally sensitive primary health care services
As above. As above.
274KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected Observed impacts EvidenceIncrease in capacity to provide support to Aboriginal and Torres Strait Islander patients
As above. As above.
Aboriginal and Torres Strait Islander people increase their utilisation of mainstream primary health care services
Information related directly to the activities of this measure’s workforce is not available, but there are indications of an overall increase in the use of mainstream primary health care services (refer chapter ).
Refer chapter
Contextual considerations
The organisational readiness and cultural safety of DoGPs to host and support these workers was identified as a key external factor impacting on the implementation of the measure. Consultations showed variations in both readiness and cultural safety amongst host organisations.
Fund holder reports, SSE, and qualitative information gathered from a small group of relevant stakeholders
1.78 Measure overviewThis measure aims to improve access to culturally sensitive mainstream primary care services for Aboriginal and Torres Strait Islander peoples. It primarily involves workforce enhancement through the recruitment of ATSIOWs and IHPOs to Divisions of General Practice, and relevant program supports at the local, state and national levels. The 2010-11 total expenditure was $18.73 million for this measure. 1.79 Workforce enhancement In 2010-11 recruitment to ATSIOW and IHPO positions was strong and, where targets existed, aligned with these specified targets. However, there were challenges reported in recruiting ATSIOWs. This finding has been informed by analysis of a (non-representative) sample of 20 fund holder reports, data on recruitment provided by the department, and consultations with ATSIOWs, IHPOs and their managers, and national stakeholders (relevant peak and representative organisations) during 2010-11. Ninety Divisions of General Practice (DoGPs) and six SBOs had funding in 2010-11 to employ ATSIOWs and IHPOs under this measure. Note that these figures represent cumulative totals from February 2010 to 30 June 2011.
275KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
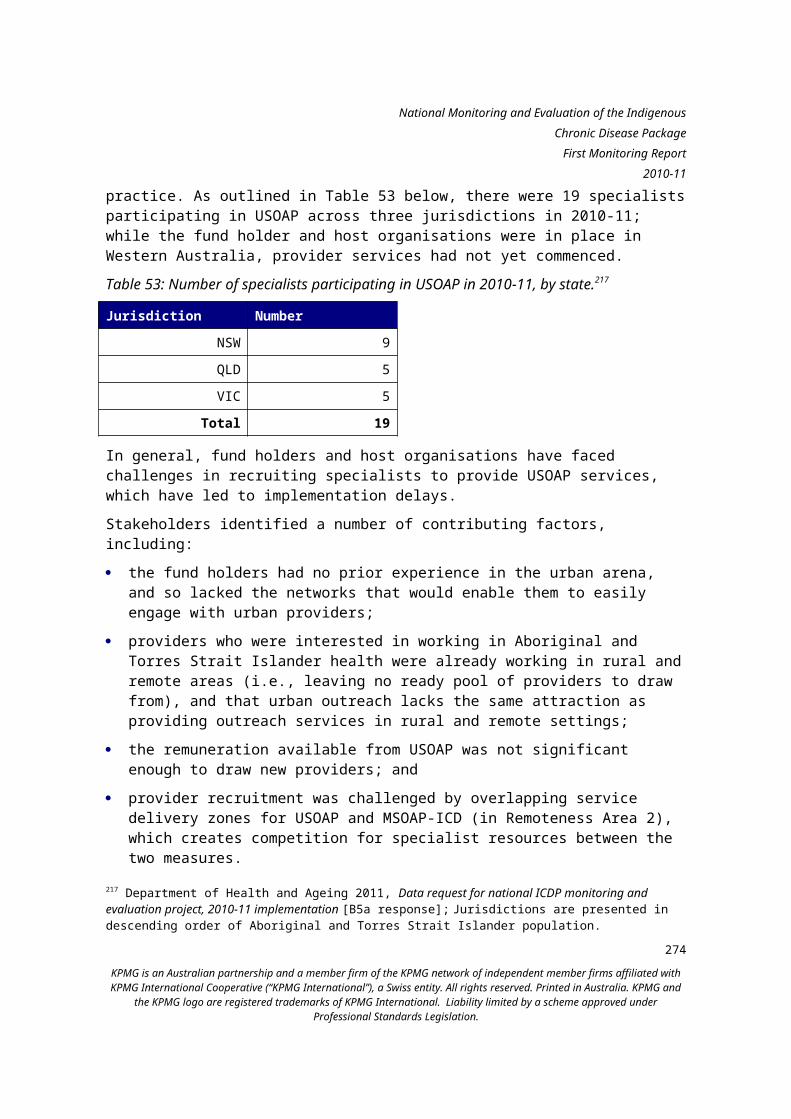
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Workforce recruitment in 2010-11 built on the substantial recruitment activity that had occurred in 2009-10. As in the previous year, Indigenous Health Partnership Forums assisted the department in selecting locations for the placement of ATSIOWs within mainstream settings (in DoGPs). below sets out the ATSIOW and IHPO positions that had been recruited by the end of 2010-11 by jurisdictions. A further nine FTE IHPO positions were funded to be based in NACCHO and the eight affiliates. The following points need to be noted when interpreting this data: differences between allocation and recruitment may be due to late
allocation of positions in the financial year; and recruitment numbers may be low due to turnover of staff.
276KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 70: ATSIOWs and IHPOs in Divisions and SBOs to 30 June 2011, by jurisdiction.280
JurisdictionATSIOW Allocated
ATSIOW Recruited
IHPO Allocated
IHPO Recruited
NSW 26.0 26.0 27.0 27.0QLD 23.0 21.4 17.8 16.8WA 13.0 11.4 12.5 12.2NT 3.0 2.0 2.0 2.0VIC 8.0 7.1 13.9 13.7SA 9.0 9.0 7.4 7.4TAS 3.0 3.0 4.0 4.0ACT 1.0 1.0 1.0 1.0Totals 86.0 80.9 85.5 83.9
The overall target for recruitment of ATSIOWs over the four years of the ICDP was 80 FTE281, and during 2009-10 and 2010-11, 80.9 FTE ATSIOWs were recruited282, exceeding the target. The growth in ATSIOW recruitment was significant in 2010-11 with an increase of over 50 FTE recruited in this fiscal year.However, the level of retention is unclear at this stage; therefore, it is possible that, while recruitment targets are met, turnover is high or the actual size of the workforce employed at any one time is lower than the target. This is also true of IHPOs, which had the same target of 80 FTE positions across the life of the ICDP. During the eight community site visits, all mainstream organisations discussed the recruitment and retention of IHPOs and ATSIOWs. Some strategies described to support successful recruitment included targeted advertising (such as in Aboriginal or Torres Strait Islander media) and making use of existing professional networks to encourage people to apply for the positions. Several DoGPs reported difficulties in the recruitment and retention of ATSIOWs. A number of factors may contribute to this, including the
280 Based on information provided by the Department of Health and Ageing 2011; Jurisdictions are presented in descending order of Aboriginal and Torres Strait Islander population size.281 Urbis 2010, Indigenous Chronic Disease Package Monitoring and Evaluation Framework. Department of Health and Ageing. Canberra, viewed 14 August 2012.282 This information was extracted by KPMG from the workforce location data provided by the department.
277KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
requirement that ATSIOWs be of Aboriginal and/or Torres Strait Islander descent.283 This limits the potential recruitment pool. Another factor seen to contribute to challenges recruiting ATSIOWs is a perceived disconnect between some of the expectations of the role (particularly those around community engagement) and the description of the role as primarily an entry-level position.Supporting the workforce
An important aspect of the design of this measure is the employment of IHPOs and ATSIOWs in teams, where more senior workers (IHPOs) can support entry-level workers (ATSIOWS). Consultations indicated that this strategy was effective in providing professional and personal support for workers. This team-based structure may be of particular importance in the mainstream setting, where ATSIOWs may be the first and/or only Aboriginal and Torres Strait Islander people in their new workplace.During consultations, examples of work being done by DoGPs to improve the cultural safety of the workplace were provided, which is an important factor in both the recruitment and retention of Aboriginal and Torres Strait Islander employees; however, these examples are location-specific. It does not appear that a systemic approach was taken by SBOs or DoGPs to review the cultural safety of their network workplaces ahead of recruiting funded ATSIOW and IHPO positions. Many fund holders in the sample reports reviewed recounted providing assistance to GP practices to undertake cultural awareness training, but only one Division reported including their practice staff in such training. During the site visit consultations, IHPO and ATSIOW workers were asked to reflect on their capability in relation to their role, access to orientation, training and ongoing professional development. Overall, IHPOs and ATSIOWs in the mainstream setting reported that they felt they had the required skills to fulfil their roles. Access to organisational orientation was consistently reported to be sufficient and helpful in the mainstream setting; however, reports about access to role-specific orientation were less consistent. In several cases IHPOs reported that they had been employed for some time before they had had access to role-specific orientation. All fund holders consulted for this measure were aware of the guidelines, and were able to provide commentary on the position descriptions for ATSIOWs and IHPOs.
283 Department of Health and Ageing 2010, Closing the Gap: Improving Indigenous Access to Mainstream Primary Care – Indigenous Health Project Officers and Aboriginal and Torres Strait Islander Outreach Workers Program Guidelines, Canberra, viewed 27 November 2012.
278KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
ATSIOW and IHPO roles and key activitiesThe evaluation found that in 2010-11 there appeared to be significant variation in how the ATSIOW role is being interpreted; however, this largely appeared to be consistent with the guidelines, since they allow for variation in response to local needs. The IHPO role, on the other hand, was considered by IHPOs, managers and national stakeholders to be better defined by the guidelines, and the consultations suggested that common tasks were being undertaken in line with the position descriptions given by the guidelines.These findings have been informed by analysis of holder reports, and consultations with ATSIOWs, IHPOs and DoGP staff during community site visits. ATSIOWs
The community site visits conducted in 2010-11 suggest that, although there was significant variation in the specific tasks undertaken by ATSIOWs, the five ATSIOWs engaged through these site visits were commonly performing tasks in line with the following to broad functions: Support for individual patients – in some cases this was similar to low-level
care coordination, involving activities such as providing transport, assisting with enquiries and educating patients about chronic disease self management.
Community liaison – performing tasks such as community needs analyses, ICDP education and promotion of available programs and services in the community.
The majority of ATSIOWs engaged in these visits were also providing transport, although this varied depending on factors such as: overall workload; vehicle availability; regulations within their organisation – some organisations do not allow
ATSIOWs to provide transport for safety reasons; and existing transport options within the community. While some ATSIOWs felt that it was not appropriate or useful for them to provide transport, others reported that informal interactions during transport facilitate good community engagement, and that patients place a high value on transport (this is consistent with community member consultations undertaken to date).
279KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
There was also some evidence of ATSIOWs undertaking clinical duties, where the ATSIOW possessed relevant skills. For example one ATSIOW consulted during the site visits was a nurse, and was working collaboratively with AHWs to complete the initial part of Health Assessments prior to the patient being seen by a GP. Another was in the process of completing AHW training and was doing basic health checks with their clients.Generally, ATSIOWs brought strong community links to the role, which allowed them to engage successfully with the community relatively quickly. During consultations, it was also noted that in many cases ATSIOWs had service-based links in the local area, such as to an IHS or NACCHO affiliate, through their previous employment or personal relationships. These types of links were considered by workers and employers to be very valuable. Working with local service providers was considered by ATSIOWs and service providers to be mutually beneficial: service providers (e.g., AHWs, GPs, nurses) reported improved
understanding of the rationale for ICDP measures and how to work in more culturally appropriate ways;
ATSIOWs and IHPOs reportedly improved their understanding of the issues and challenges facing mainstream providers, and some had increased their clinical knowledge, assisting them to understand the health issues Aboriginal and Torres Strait Islander people are facing; and
analysis of six month reports from program fund holders (see below) showed that, to support awareness about the role of the ATSIOW within the community, most DoGPs developed referral pathways as a way for practices to refer clients to ATSIOWs. In addition to referral tools, most of the ATSIOWs engaged (often together with an IHPO) visited practices to promote their services. ATSIOWs and IHPOs engaged during the evaluation’s site visits reported similar activities, and highlighted the importance of ‘getting out to the community’ so people are aware of the services available.
IHPOsThe role of the IHPO appeared to be more uniform across localities where they were employed, when compared to the diversity of the role of ATSIOWs. The eight IHPOs engaged through the evaluation’s site visits were reportedly performing a mixture of the tasks outlined below.Generally IHPOs were recruited before ATSIOWs and therefore undertook initial tasks alone, such as: building relationships with members of the community;
280KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
building an understanding of services available within the community; and undertaking initial needs analyses.Many of the tasks undertaken were provided in an ongoing way (in collaboration with ATSIOWs and/or Care Coordinators), for example: working with General Practices to improve the cultural appropriateness of
their service, such as collecting Aboriginal and Torres Strait Islander status of patients, updating information systems to support Aboriginal and Torres Strait Islander identification, providing cultural awareness training, implementing recall and reminder systems;
developing referral pathways between local services, including Aboriginal and Torres Strait Islander and mainstream services;
community awareness raising about the Aboriginal and Torres Strait Islander and mainstream services that are available within the community;
community education (i.e., through community events) about healthy lifestyles; and
promotion of the ICDP to the community as well as to local health providers such as GPs, pharmacists and nurses, and local services.
At the majority of sites visited to date, IHPOs reported working together with ATSIOWs to promote the ICDP. Promotion had targeted both the community, through mechanisms such as stalls at community events, posters and flyers; conversations with known community members to ‘spread the word’; and engaging with local services (e.g., pharmacists, GPs), through mechanisms such as ATSIOWs/IHPOs giving talks at local forums, and talking to General Practice staff at scheduled visits. The analysis of six monthly fund holder reports shows that similar activity was occurring within host DoGPs across Australia (i.e., no differences for urban, regional and remote). Some strategies used by IHPOs reported by Divisions include: running workshops and education sessions to professionals about the
Closing The Gap measures, and publishing articles in Divisional and regional newsletters;
establishing specific Closing The Gap newsletters; developing a PIP Indigenous Health Incentive calculator for practices to
estimate their financial benefits from registering; becoming more involved, or continuing their involvement, in a wide
selection of committees, groups and meetings with community, Indigenous and health organisations; and
running health checks and preliminary screening at some public events.
281KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Identification of Aboriginal and/or Torres Strait Islander status
The evaluation found emerging evidence that in 2010-11, IHPOs and ATSIOWs were undertaking successful work to improve Aboriginal and Torres Strait Islander identification with health services. This finding has been informed by analysis of fund holder reports, and consultations with ATSIOWs, IHPOs, DoGP staff and primary health care providers, through community site visits. Promoting identification of Aboriginal and Torres Strait Islander people is a key role for IHPOs, and this supports work also being done within general practices to increase self-identification through the PIP Indigenous Health Incentive program (B3a measure). Based on the IHPOs and ATSIOWs consulted during site visits, it appears these workers have frequently worked with PIP Indigenous Health Incentive practices to provide education and support to increase identification processes at the organisational level, and have also provided education to the community about why it is important to self-identify, the benefits of self-identification, and how the information is used. Consistent with this, the fund holder reports reviewed, showed that both IHPOs and ATSIOWs were involved in engaging with practices to encourage identification. One report stated that the IHPO was responsible for designing related campaigns and posters. In other reports, ATSIOWs had helped practices to track the Aboriginal and Torres Strait Islander patients identified, developed systems for them to use, and disseminated posters. In one DoGP, it was reported that the ATSIOW and IHPO attended Indigenous community forums and Aboriginal health clinics to inform community members and individuals about their rights in relation to self-identification. An IHPO from another Division was reported to have offered practices training on Aboriginal and Torres Strait Islander identification, including role modelling, but this was not taken up. During consultations it was clear that access to the PBS Co-payment (B2 measure) was seen as a tangible benefit for the patient to encourage self-identification. Engaging with mainstream practices
The evaluation found emerging evidence that in 2010-11, IHPOs and ATSIOWs were engaging with mainstream practices to support cultural awareness/competency. This finding has been informed by analysis of fund holder reports, and consultations with ATSIOWs, IHPOs, DoGP staff and primary health care providers, through community site visits. The ATSIOWs and IHPOs engaged during the site visits report successes in working with GPs who were initially reluctant to engage with them about the
282KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
ICDP. As a result of the work they have done with local primary health care services (described above), ATSIOWs and IHPOs consulted consistently reported outcomes such as general practices: now consistently asking patients about their Aboriginal and Torres Strait
Islander status; implementing recall and reminder systems for Aboriginal and Torres Strait
Islander patients; and proactively signing up patients to the PIP Indigenous Health Incentive and
the PBS Co-payment measure (B2 measure). The fund holder reports also highlight these outcomes. Encouraging practices to ask patients to self-identify is discussed above. The fund holder reports reviewed showed that most Divisions with IHPOs reported registering patients for the PIP Indigenous Health Incentive and PBS co-payment measure; and a small number of ATSIOWs were reported to be involved in patient registration. Although not discussed in the reports reviewed as an outcome achieved, the Divisions consulted during site visits did note that where practices do not have recall and reminder systems for Aboriginal and Torres Strait Islander patients, this is a barrier to their efforts on closing the gap.Despite examples of positive outcomes, there still appear to be some limitations to mainstream services providing culturally appropriate care. IHPOs, ATSIOWs and their managers consulted provided examples such as GPs not seeing it as necessary or relevant to their patients, being apprehensive about asking people about their Aboriginal and Torres Strait Islander status, and (despite not asking patients to self-identify) believing they do not have any Aboriginal and Torres Strait Islander patients. ATSIOWs and IHPOs engaged during the evaluation’s site visits reported providing support to local service providers in order for them to develop their own understanding of community needs and culture. A number of the ATSIOWs and IHPOs had been involved in providing education or cultural awareness training to local GPs and, less frequently, to other health workers such as nurses and pharmacists. ATSIOWs and IHPOs reported they have also included cultural education in promoting the ICDP (for example, the PIP Indigenous Health Incentive). The analysis of a sample of fund holder six month reports supported this data, showing that the majority of IHPOs within DoGPs had provided cultural awareness training to primary health care services to increase their cultural competence. Other methods used by IHPOs included providing practices with a tool to assess the cultural appropriateness of their service, providing practices with promotional materials such as welcome signs, and awarding plaques to practices delivering culturally sensitive services.
283KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
ATSIOWs, IHPOs and other primary health care staff in some locations reported an increased uptake of MBS items specific to Aboriginal and Torres Strait Islander people, specifically Aboriginal and Torres Strait Islander health assessment items. For assessment of utilisation of MBS items please see chapter . Engaging with Aboriginal and Torres Strait Islander communities
The evaluation found emerging evidence that ATSIOW and IHPO promotion of the ICDP in the community may be leading to a better understanding of health services and ICDP-specific measures amongst community members, and some improvements in access to these services. This finding has been informed by consultations with ATSIOWs, IHPOs and primary health care providers, and community focus groups. As noted above, some of the IHPOs engaged (five in total) reported that they (and in some cases in conjunction with an ATSIOW) had promoted the PIP Indigenous Health Incentive to local GPs and/or community members. The community focus groups suggest that this information may have flowed through to community members both directly and indirectly. Community members at four focus groups reported knowing about the PIP Indigenous Health Incentive initiative due to engagement with staff from Medicare Locals and IHSs in their region, their local GP, or through word of mouth. Community members at one focus group also said that the ATSIOWs had improved their awareness of how to live a healthy lifestyle and how this can be supported by attending programs and accessing services. In the sample of six month reports reviewed, all Divisions reported an increase in registrations for PIP Indigenous Health Incentive and the PBS Co-payment as a result of their promotion of the ICDP. National stakeholders also reported emerging evidence of increased access to health care services due to the presence of ATSIOWs and IHPOs (particularly when they are Aboriginal and Torres Strait Islander) within mainstream services. While just over half the fund holder reports identified a difficulty in quantifying improvements in access to mainstream services, given the early stage in the project and sometimes lack of ATSIOW or IHPO in place, it was acknowledged by the vast majority of stakeholders engaged through the 2010-11 site visits and consultations, that there are significant barriers to increasing the utilisation of mainstream services by Aboriginal and Torres Strait Islander people. The analysis of fund holder reports shows that a range of approaches were used by IHPOs and ATSIOWs within Divisions of General Practice to address
284KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
these barriers. Many Divisions undertook a survey of general practices to help identify barriers. Some Divisions also surveyed or held focus groups with patients and members of the Aboriginal and Torres Strait Islander community. Other strategies included undertaking site visits to practices, producing and/or distributing promotional resources, placing information and artwork in practice waiting rooms to create a welcoming environment, and developing directories of registered PIP Indigenous Health Incentive practice and PBS co-payment services. Many Divisions sought endorsement of resources by local Elders and incorporated local artwork in materials and waiting rooms to recognise and reflect the Aboriginal and Torres Strait Islander community of the area. Relationship building was another common approach. Key stakeholders included local Elders, Traditional Owners, Aboriginal Medical Services, Aboriginal and Torres Strait Islander community organisations, health organisations, and other community organisations. One Division sought to link practices with local Aboriginal and Torres Strait Islander organisations. Another was exploring exchanging staff between mainstream services and IHSs. Information collected at the evaluation site visits suggests that ATSIOWs, and less frequently IHPOs, supported increased utilisation of primary health care services by directly linking people with these services. For example ATSIOWs and IHPOs reported: making appointments for patients; encouraging them to attend appointments; organising access to community transport or providing transport directly;
and telling local people which pharmacies know about the PBS Co-payment
measure (CtG scripts) so they feel comfortable going there (i.e., they know they will not have to explain the initiative to the pharmacist).
In some locations, ATSIOWs provided a critical link between the community and mainstream services. For example, in one location the ATSIOW’s core role was as community liaison for a local mainstream mobile clinic. The ATSIOW greeted patients and took initial information from them before they went on to see the GP or nurse. The ATSIOW also chatted to patients while they were waiting to make sure they stayed until they were called into their appointment. In this case service access was supported because community members felt comfortable engaging with an Aboriginal person, and this reportedly took away some of the fear about engaging with this mainstream service. Information collected through site visits suggested that some community members perceive that the work of ATSIOWs and IHPOs in improving the cultural safety of mainstream practices is providing them with an enhanced
285KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
choice about how and where they can access primary health care services. For example, some people reported that while they like to attend their local IHS for some services, they also value having the option of accessing a mainstream service for convenience or privacy reasons. IHPOs and ATSIOWs have also been reported to have encouraged and supported recruitment of nurses to local health services, they have sought out specialists who will provide free services to Aboriginal people, and worked to attract specialists providing visiting services, in some cases through outreach services provided through ICDP (the USOAP B5a and MSOAP-ICD B5b measures). One-fifth of the fund holder reports reviewed discussed engaging nurses and specialists, including in developing processes and brochures. The same number also reported having outreach services in place, one of which was through the MSOAP-ICD program.Supporting coordination within the service system
The evaluation found emerging evidence that the work undertaken by IHPOs in 2010-11 may have contributed to improved coordination within the service system around the ICDP.This finding has been informed by consultations conducted through community site visits, review of documentation provided by the department, and consultations with state and territory and national stakeholders.
Jurisdictional level coordination
Data collected at the site visits shows that IHPOs within state-based organisations have undertaken a range of tasks to support improved collaboration between ICDP stakeholders. For example, in Western Australia one IHPO was working with the members of their organisation (ACCHOs) and local DoGPs to promote the ICDP and support improved engagement between the IHS and mainstream sector through joint training and information sharing. In Queensland, the IHPO within the SBO had encouraged the coordinated rollout of the ICDP across DoGPs and IHSs. In New South Wales and South Australia the SBOs have brought together regional ICDP stakeholders for joint meetings and networking events. Participation in the Indigenous Health Partnership Forums by IHPOs sitting within SBOs and peak organisations was varied, with some participating fully, and others sitting on sub-committees. It is acknowledged that this variation is largely dependent on the arrangements within the jurisdiction. This is one mechanism through which IHPOs are engaging with ICDP stakeholders.
286KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Local level coordination
The analysis of a sample of fund holder six month reports shows that IHPOs within DoGPs were proactive in supporting collaboration across the IHS and mainstream sectors. Collaboration with local Aboriginal and Torres Strait Islander services and groups was achieved by building personal relationships, developing formal partnerships (including Memoranda of Understanding), and appointing representatives to Divisions’ Closing the Gap advisory committees. Many Divisions were in the process of jointly establishing steering committees with local Aboriginal and Torres Strait Islander organisations. Two Divisions reported challenges engaging local Indigenous organisations, with one attempt leading to a breakdown in the relationship. Other approaches to improved shared planning and priority setting included the mapping of services in the area that are supportive of Aboriginal and Torres Strait Islander people, working with local schools to deliver information about preventative health information and the availability of health screening, and supporting Aboriginal Medical Services and other local services in funding submissions and joint projects. Most fund holders in the sample reported that relationships had strengthened by the end of the reporting period. Four of the mainstream primary health care organisations consulted through the site visits have formed strong partnerships with local IHSs and these are reportedly working well due to the combined efforts of staff, including IHPOs and ATSIOWs in some cases. For example, one ATSIOW engaged who was employed by a Medicare Local reported that they had an existing relationship with staff in a local IHS, and this had allowed them to act as a key point of contact between the IHS and the Medicare Local, and encourage information sharing. Other examples of collaborative arrangements include working together to implement programs, and sharing ICDP funding across the two organisations. Consultations with jurisdictional level organisations, such as health councils and general practice peak organisations, suggest that there are mixed views on the contribution of this measure to improved collaboration. Some stakeholders are supportive of the ICDP’s aims to facilitate better engagement between the IHS and mainstream sectors, such as by placing ATSIOWs within both IHSs and Divisions of General Practice. Other stakeholders identify this as problematic, believing that such a move fosters competitiveness for funding and is ‘forced’ collaboration. 1.80 Program supportsThe evaluation found that in 2010-11 a number of supports were implemented for IHPOs and ATSIOWs including resources, and opportunities for networking.
287KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
This finding has been informed by consultations with national stakeholders involved in the implementation of these resources, consultations with ATSIOWs and IHPOs through the community site visits, and review of program documentation. In 2010-2011, DoGPs that received workforce positions through the Improving Indigenous Access to Mainstream Services Program received the GP Resource Kit284 from the department to inform practices about the ICDP measures and related processes, and encourage them to participate. The GP Resource Kit comprises a folder of documents that includes 10 laminated ‘practice detail cards’ on the following topics, plus a GP booklet providing more detailed information: information for General Practitioners on the ICDP; patient identification; PIP Indigenous Health Incentive; Aboriginal and Torres Strait Islander health assessment items; MBS items overview; chronic disease follow-up services; allied health follow up services; Practice Nurses/registered AHW follow up services; Pharmaceutical Benefit Scheme co-payment measure; and CCSS Program.The majority of ATSIOWs and IHPOs engaged through the evaluation’s site visits knew about the resource kit and reported providing them to GPs and pharmacists. Some ATSIOWs and IHPOs reported that they had requested additional copies of the resource kit to assist them with their promotion of the ICDP and their roles.In April 2011, the AGPN initiated the IHPO Workforce Support Project,285 a six month project run with contracted support from the Australian Mentoring Centre to provide support to IHPOs who may otherwise feel isolated in their mainstream placements.286 The need for this type of workforce support was identified at the April 2010 IHPO national orientation workshop hosted by
284 The Department developed the GP Resource Kit for staff working in mainstream primary health care practices and Indigenous Health Services, and has been distributed to all practices who have received ICDP workforce positions. 285 Australian General Practice Network 2011, Workforce Support (webpage), viewed 5 December 2011. 286 KPMG consultation with Measure Manager (2 November 2011).
288KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
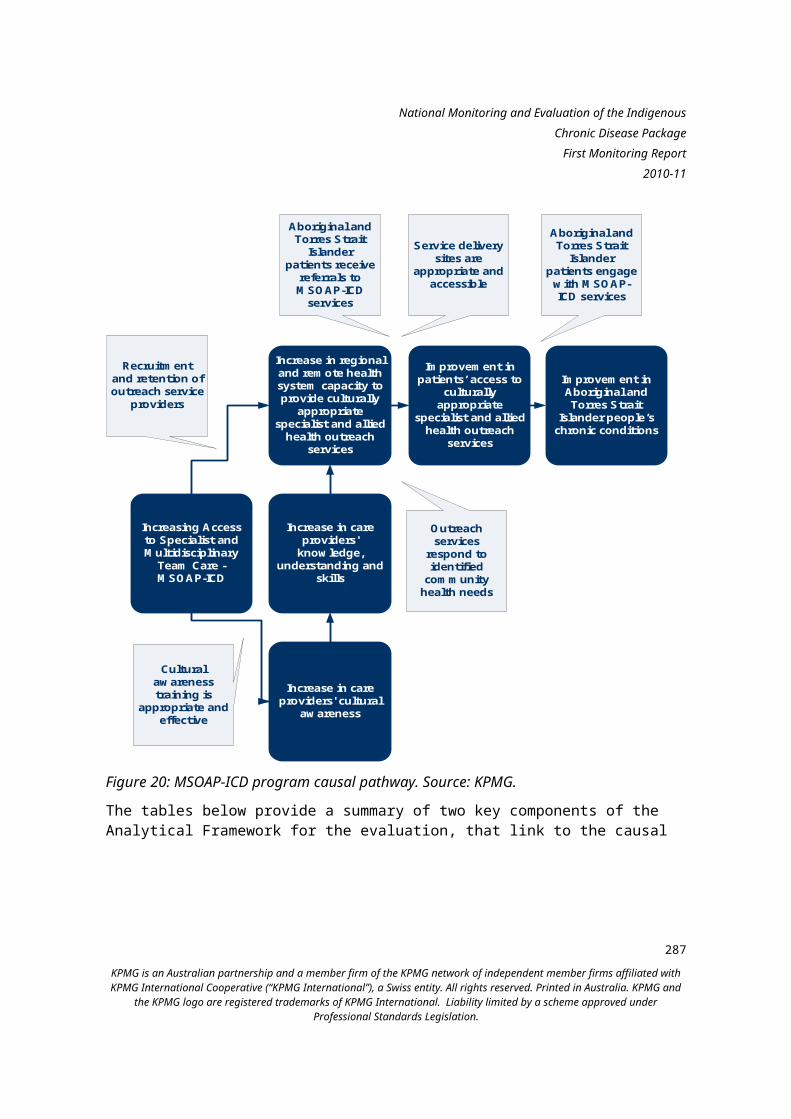
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
AGPN. The IHPO Workforce Support Project was intended to complement other support being offered by SBOs, Divisions and IHPOs themselves. The project was overseen by a reference group involving AGPN and a number of IHPOs and involved the following activities: Developing a standard, national approach to IHPO orientation,
commencement and support. With the assistance of SBOs and Divisions, the key steps and resources needed to successfully orientate, commence and support an IHPO were identified and then shared through the AGPN Website resource library.
Developing a peer mentoring approach, including by connecting peer mentors in the SBOs with mentees in the Divisions, and providing an online webinar for SBOs on developing peer mentoring relationships and frameworks.
Producing five editions of the IHPO Workforce Connections e-Newsletter to share good practice, ideas, resources, tips and contacts within the workforce.287
Creating an online resource library on the AGPN website,288 including content such as: a ‘day in the life’ IHPO survey; fact sheets; good practices; peer mentoring and links to other resources.
In 2010-11, some states undertook their own jurisdictional workshops or events which included ATSIOWs and IHPOs. In February 2011, VACCHO and General Practice Victoria (GPV) co-hosted the Victorian Outreach Worker Forum, where the purpose was to network, provide feedback on program implementation; and identify ongoing needs, such as regarding the orientation package. Eight IHS and mainstream ATSIOWs participated in this event.289
In Queensland, General Practice Queensland (GPQ) held a three-day workshop in March 2011 for ATSIOWs and IHPOs. The workshop included mural building, discussion of monitoring and reporting on performance indicators, identifying learning and development needs and how to meet these needs.
287 Australian General Practice Network 2011, Workforce Support (webpage), viewed 5 December 2011.288 Australian General Practice Network 2011, Workforce Support (webpage), viewed 5 December 2011.289 Department of Health and Ageing 2011, Commonwealth’s Indigenous Chronic Disease Package Update 17th edition, Department of Health and Ageing, Canberra.
289KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
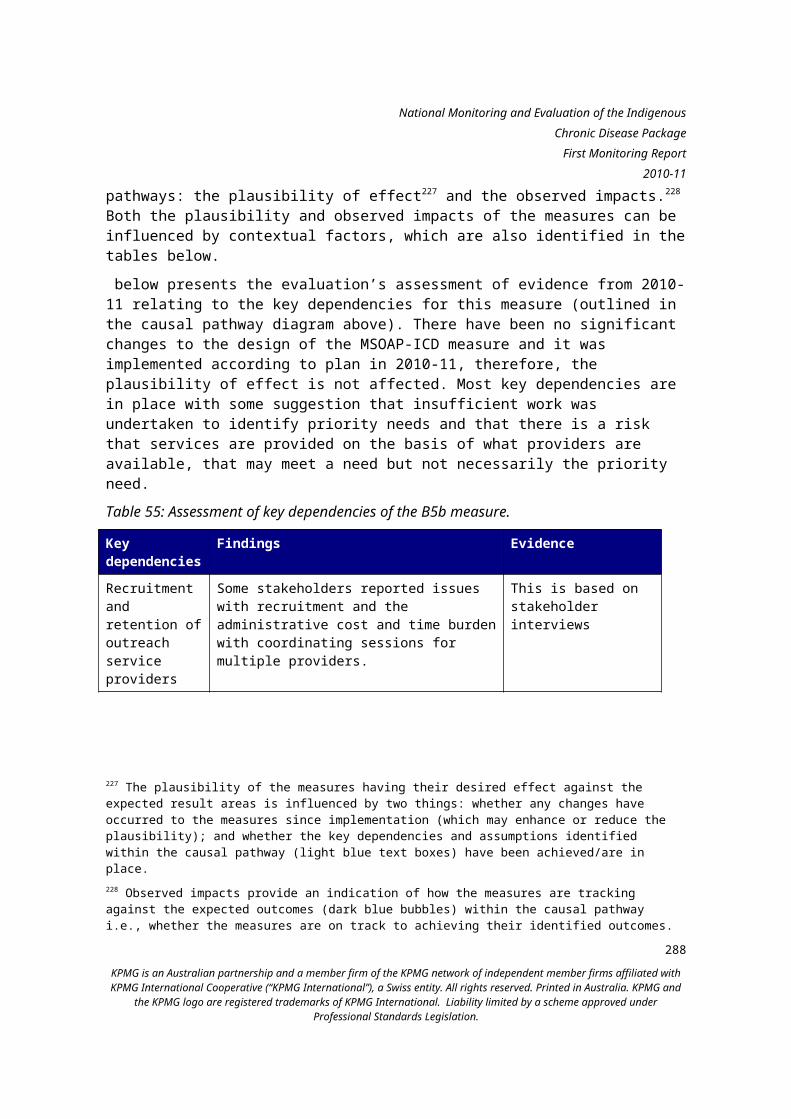
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.81 Facilitators and barriers The key facilitators and barriers to the implementation of the Improving Indigenous Access to Mainstream Primary Care Program are set out below. These predominantly consist of structural or organisational supports for the IHPO and ATSIOW roles. Facilitators: Broad role definitions. While in some cases this was reported to have
caused confusion and anxiety in the early stages of implementation, overall the inherent flexibility of the program guidelines regarding the IHPO and ATSIOW roles appears to be facilitating the establishment of local tailored approaches which build on the strengths of individuals and teams.
Community links. In most areas there has been a strong focus on recruiting people with strong existing community links to both IHPO and ATSIOW roles. This was consistently identified by stakeholders as a critical success factor to facilitate community trust and to help establish service level linkages.
Team based structure. The IHPO/ATSIOW team structure, and the inclusion of Care Coordinators in those teams where possible, is seen to provide the structure and support necessary for individuals to operate effectively in their roles. This is true for both IHPOs (who may benefit from the community insight which ATSIOWs provide) and ATSIOWs (who typically report that the support provided by their IHPO colleague is invaluable).
Vehicle access. Several workers consulted identified vehicle access as important to their ability to be able to reach community members and facilitate their access to mainstream primary care. In the sample of fund holder reports reviewed, many Divisions identified lack of a vehicle as a barrier to providing services and taking patients to clinics (all of these except one were in urban and inner regional locations). A few Divisions reported that they were looking to overcome this barrier through leasing a vehicle to be shared between the ATSIOW, IHPO and Care Coordinator positions. Two Divisions which had the use of a vehicle reported this to be a facilitator for progressing access to mainstream healthcare, and that transport has become a large proportion of the services which they provide.
Barriers: Recruitment and retention. Organisations have to recruit from a limited
local pool of staff which can make recruitment challenging. Analysis of fund holder reports shows that many Divisions were still in the process of recruiting ATSIOWs in 2011, or had only recently filled the position. As noted above and in the previous chapter, factors such as annual/short-term contracts and movement of staff to other positions may also have an
290KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
impact on retention. Additionally, there have been some negative perceptions reported by ATSIOWs, IHPOs and their managers about the likely sustainability of the program, i.e., that it may not be funded beyond the current funding period.
National health reform. The Sentinel Site Evaluation Report suggested that DoGP management may in some cases be distracted by the establishment of Medicare Locals, and therefore less engaged with supporting the ICDP workforce.290
Perceived competition between sectors. Perceived competition for funding to recruit staff between IHSs (under the ICDP C2 measure) and mainstream organisations (under this measure) may have a negative impact on the relationships between IHS and mainstream sectors.
1.82 OpportunitiesThe following opportunities were identified for the future operation of the Improving Indigenous Access to Mainstream Primary Care Program: Networking opportunities for ATSIOWs and IHPOs: Ongoing and regular
networking opportunities between ATSIOWs and IHPOs in different organisations and across the IHS and mainstream health sectors are likely to support understanding and confidence, and act as a mechanism to share experiences and good practice. This type of professional development can be particularly useful for newly created and evolving roles such as the IHPO and ATSIOW roles.
Support for team-based arrangements: Stakeholder consultations suggested that ATSIOWs and IHPOs who work as part of a team are more effective in addressing patient needs. There may be opportunities to ensure that the benefits of the team-based approach are maximised, for example, providing training in working as a team, or developing case studies about ‘what works well in team work’ for dissemination to ATSIOWs and IHPOs.
290 Menzies School of Health Research 2011, Sentinel Sites Evaluation Report June 2011, Department of Health and Ageing, Canberra.
291KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Attracting More People to Work in Indigenous Health (C4)This chapter describes the progress of the Attracting More People to Work in Indigenous Health measure against relevant activities and outputs (as described in the Evaluation Framework). It discusses findings against expected results and barriers, facilitators and opportunities identified to date. Attracting More People to Work in Indigenous Health at a glanceThe key achievement in the 2010-11 financial year was the development, testing and refining of the Health Heroes and Do Something Real campaigns, using a strong evidence base.Delays in the campaign development tendering process, and limited awareness of both campaigns (which is likely to have been influenced by a number of factors including the relative infancy of the campaigns and limited promotion of the measure) have limited their impacts to date. There are indications that the Health Heroes campaign promotional materials may be effective in engaging Aboriginal and Torres Strait Islander secondary school students.Potential effects based on implementation findingsFigure 24 below is the causal pathway for the Attracting More People to Work in Indigenous Health measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
292KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Campaigns are effective, evidence based and achieve desired exposure
Improvements in knowledge of and
attitudes towards jobs in health/Aboriginal and Torres Strait Islander
health
Health professional are more likely to seek
employment in IHS sector
More Aboriginal and Torres Strait Islander
students pursue further education and
employment in the health care sector
More Aboriginal and Torres Strait Islander people become health
professionals
Increase in health system capacity and capability to deliver primary health care services to Aboriginal and
Torres Strait Islander people
Individuals and communities are receptive to the
messages
Attracting More People to Work in Indigenous Health
Students are motivated and
supported
Students are supported and provided with opportunities
to complete training and gain employment
Changes in knowledge and attitudes lead to changes in behaviour
IHSs are able to employ additional
health professionals
Figure 24: Attracting More People to Work in Indigenous Health causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect291 and the observed impacts.292 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. Table 71 below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal
291 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.292 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
293KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
pathway diagram above). There have been no significant changes to the design of the measure and it was largely on track with some delays in tendering of specific components of the campaigns. The plausibility of effect is unlikely to be affected. Information is available for some of the key dependencies and demonstrates that the campaigns are evidenced based. The main contextual factors that could influence how receptive individuals are to the measure are community norms regarding employment and whether there are employment opportunities in the locality where individuals live.Table 71: Assessment of key dependencies of the C4 measure.
Key dependencies
Findings Evidence
Campaigns are effective, evidence based and achieve desired exposure
The two campaigns were developed utilising developmental research and input from experts in Aboriginal and Torres Strait Islander communication.
This is based on review of measure/campaign documentation, and qualitative information gathered through consultations with relevant stakeholders involved in the measure implementation.
Individuals and communities are receptive to the message
No data is currently available.There appeared to be limited awareness of both campaigns amongst consulted stakeholders while noting that the evaluation did not engage the intended target audience for the campaigns.
This is based on review of measure/campaign documentation, and qualitative information gathered through consultations with primary health care providers, Aboriginal and Torres Strait Islander community members and the measure manager
Health Heroes:Students are motivated and supported
Data is not available for the First Monitoring Report.
Not applicable
294KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Health Heroes:Students are supported and provided with opportunities to complete training and gain employment
Data is not available for the First Monitoring Report.
Not applicable
Do Something Real:Changes in knowledge and attitudes lead to changes in behaviour
Data is not available for the First Monitoring Report.
Not applicable
Do Something Real:IHSs are able to employ additional health professionals
Data is not available for the First Monitoring Report.
Not applicable
295KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Key dependencies
Findings Evidence
Contextual considerations
It is likely that receptiveness to the messages within the campaigns, and the eventual impact of these messages will vary between individuals and communities.: Community norms and patterns of
employment are likely to vary between individuals and across communities. For instance, a paper by the Centre for Aboriginal Economic Policy Research notes that in urban areas, employment may have become more of a norm.293
The availability of employment opportunities within communities is likely to vary, for example there are usually fewer employment opportunities in remote areas compared to non-remote areas.294
Literature review
Table 72 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). There are indications that the Health Heroes campaign promotional materials may be effective in engaging Aboriginal and Torres Strait Islander secondary school students. Data is not available to assess any other expected impacts and no contextual factors have been identified.
293 Gray M & Hunter B 2011, Change in Indigenous Labour Force Status: Establishing Employment as a Social Norm? , Centre for Aboriginal Economic Policy Research, Canberra. 294 Gray M, Hunter B & Lohoar S 2011, Increasing Indigenous employment rates. Issues Paper no. 3. Produced for the Closing the Gap Clearinghouse, Australian Institute of Health and Welfare, Melbourne & Institute of Family Studies, Canberra.
296KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 72: Assessment of expected and observed impacts of the C4 measure based on implementation progress.
Expected Observed impacts EvidenceDo Something Real:Improvements in knowledge of and attitudes towards jobs in health / Aboriginal and Torres Strait Islander health
There are indications that the Health Heroes campaign promotional materials may be effective in engaging Aboriginal and Torres Strait Islander secondary school students.
Qualitative information gathered through consultations with primary health care providers, Aboriginal and Torres Strait Islander community members and the measure manager
Health Heroes:More Aboriginal and Torres Strait Islander students pursue further education and employment in the health care sector
Data is not available for the First Monitoring Report.
Not applicable
Health Heroes:More Aboriginal and Torres Strait Islander people become health professionals
Data is not available for the First Monitoring Report.
Not applicable
297KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Expected Observed impacts EvidenceDo Something Real:Health professionals are more likely to seek employment in the IHS sector
Data is not available for the First Monitoring Report.
Not applicable
Do Something Real:Increase in health system capacity to deliver primary health care services to Aboriginal and Torres Strait Islander people
Data is not available for the First Monitoring Report.
Not applicable
Contextual considerations
None identified. Not applicable
1.83 Measure overviewThe Attracting More People to Work in Indigenous Health measure consists of two promotional campaigns aiming to promote careers in the health workforce to Aboriginal and Torres Strait Islander people: Health Heroes, targeted to Aboriginal and Torres Strait Islander secondary students and their key influencers; and Do Something Real, targeted to practicing and training health care professionals from both Aboriginal and Torres Strait Islander backgrounds and across the broader community. The measure aims to increase Aboriginal and Torres Strait Islander participation in the health workforce. In 2010-11 the actual expenditure was $2.1 million.295.
295 Email communication received sent from Measure Manager to ICDP Evaluation Unit (1 December 2011). Re: Fw: C4 RE: Data request for ICDP National Evaluation _ Monitoring Report 1.
298KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
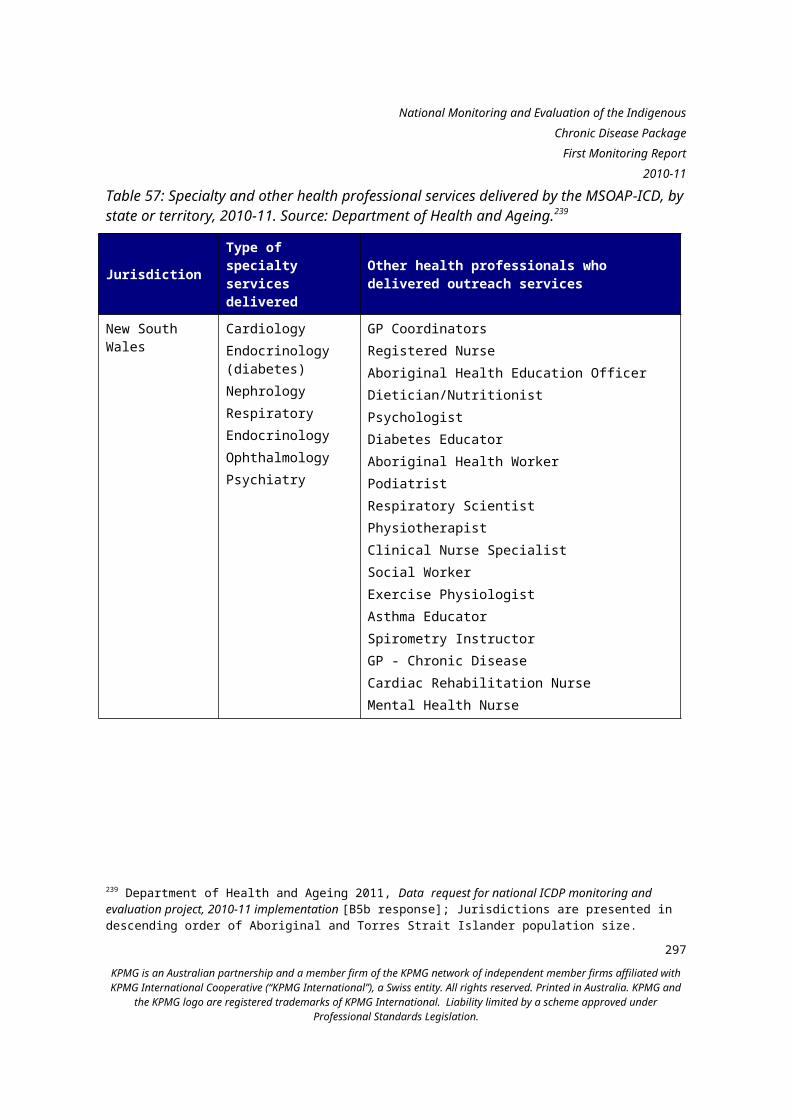
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
1.84 ResearchDevelopmental research conducted for the Attracting More People to Work in Indigenous Health measure in 2010-11 focused on the Health Heroes campaign component, and included collection of benchmarking data to inform the rollout of the campaign. This finding was informed by consultations with the department, and analysis of documentation provided by the department and that was publicly available. Health Heroes campaign
In May 2011 the department contracted Orima Research to conduct benchmarking research296 to obtain measures of pre-campaign knowledge, attitudes and intentions of the Health Heroes target audience (Aboriginal and Torres Strait Islander secondary students and their key influencers) with respect to pursuing a job in the health sector. The benchmarking research involved the conduct of a national, self-completion, paper-based survey targeting Aboriginal and Torres Strait Islander secondary school students from years 7-12. These students were enrolled in randomly selected schools with at least 20 Aboriginal and Torres Strait Islander students. Focus areas for the survey included post-school education and work plans, current training and career information seeking behaviours and relevant media consumption. The survey was administered in schools by teachers or other school staff who could assist students to complete the survey. Three hundred and ninety eight (398) surveys were completed by respondents to produce estimates for all enrolled Aboriginal and Torres Strait Islander students across Australia.A report on the findings from the benchmarking research was provided to the department on 30 June 2011. Conclusions of the benchmarking study were297: the target population (Aboriginal and Torres Strait Islander secondary
students) has limited awareness of the range of health jobs available and the education and training pathways into the health workforce;
there was limited understanding of the key benefits of working in the health care sector;
only a small number of the respondents indicated that they intend to work upon completion of study; and
respondents’ key sources of information about working in the health care sector are school, family and television.
296 This research resulted in: Orima Research 2011, Careers in Indigenous health quantitative benchmarking study, Final report, Department of Health and Ageing, Canberra. 297 Orima Research 2011, Careers in Indigenous health quantitative benchmarking study, Final report, Department of Health and Ageing, Canberra.
299KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Formal evaluation of the mass media element of the campaign was not undertaken due to the limited budget of the campaign.As at June 2011 there was evidence that formative research had informed the design of the Health Heroes campaign, as discussed in the following section. 1.85 Promotional campaignsCampaign development
In 2010-11, the two campaigns that define this measure, Health Heroes and Do Something Real, were developed utilising the developmental research and input from experts in Aboriginal and Torres Strait Islander communication.This finding was informed by consultations with the department and national stakeholders, and review of documentation provided by the department.
Health Heroes campaign
A Campaign Reference Group (CRG) was convened in 2010-11 to provide expert advice for development of the Health Heroes campaign communication strategy, including validating the concepts and sentiments used in the campaign, and sourcing the ‘Heroes’ to be featured in the campaign. Membership of the CRG comprising both mainstream and Aboriginal and Torres Strait Islander health and education sector representatives, including:
General Practice Victoria Australian General Practice Network National Aboriginal Community Controlled Health Organisation Australian Medical Association Australian Indigenous Doctors Association Department of Education, Employment and Workplace Relations Royal Australian College of General Practitioners Community Services and Health Industry Skills Council
The CRG considered the Orima research report298 that was commissioned to inform the design of the measure in the development of the Health Heroes communication strategy. The communication strategy was completed in October 2010.In 2010-11, the department contracted the creative agency BCM to develop the advertising concept for the Health Heroes campaign, and Orima Research
298 Orima Research 2010, A report on developmental research to inform communications activities designed to attract more Aboriginal & Torres Strait Islander secondary school students to work in health, Department of Health and Ageing, Canberra.
300KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
to undertake concept testing of Health Heroes communications materials developed by BCM with the campaign target group (Aboriginal and Torres Strait Islander secondary school students (years 7-12) and their key influencers). The purpose of concept testing was to further develop and refine the creative materials based on feedback from the intended audience. Four rounds of concept testing occurred from November 2010 to June 2011, reflecting the time needed to recruit participants across different geographies. Concept testing was conducted in Adelaide, South Australia and Alice Springs, Northern Territory in early April 2011. The advertising concept was refined and again tested in Redfern, New South Wales and Mildura, Victoria in late April 2011. The revised Health Heroes advertising material was presented to the Independent Communications Committee299 on 17 May 2011.The production shoot for the Health Heroes campaign occurred during 19-31 May 2011, in Sydney, Brisbane, Noosa, Palm Island, Alice Springs and Broome. Final advertising materials were tested with the target audience and key influencers (i.e., parents) in Melbourne, Mt Druitt, Alice Springs and Coober Pedy from 14-17 June 2011. The Health Heroes campaign was launched in early 2011-12.A number of public relations activities were also undertaken to support the campaign including community engagement sessions in secondary schools, provision of resource kits to 1,300 schools, and online communications activities.
Do Something Real campaign
In March 2011, the department appointed the public relations agency Boxing Clever to lead the development of the Do Something Real campaign. This included undertaking the public relations and community engagement activity for the campaign. Under Boxing Clever’s guidance, the development of the campaign was informed by input provided through interviews with representatives from a broad range of stakeholder groups, across the mainstream and Aboriginal and Torres Strait Islander health and education sectors, incuding:
Australian General Practice Network Australian Indigenous Doctors Association
299 The Independent Communications Committee (ICC) provides advice to Financial Management and Accountability Act 1997 agencies in relation to proposed advertising campaigns valued at more than $250,000. Advertising campaigns with expenditure in excess of $250,000 are considered by the ICC which provides a report to the responsible agency Chief Executive on compliance with key aspects of the Guidelines on Information and Advertising Campaigns by Australian Government Departments and Agencies (March 2010). The ICC is supported by a Secretariat within the Department of Finance and Deregulation.
301KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
National Aboriginal Community Controlled Health Organisation Department of Education, Employment and Workplace Relations Australian Medical Association Department of Families, Housing, Community Services and Indigenous
Affaires Department of Health and Ageing Royal College of Nursing Indigenous Allied Health Australia Australian Healthcare and Hospitals Association Services for Australian Rural and Remote Allied Health National Rural Health Alliance General Practice Victoria Leadership in Indigenous Medical Education NSW Department of Health Aboriginal Health and Medical Research Council Royal Flying Doctor Service Royal Australian College of General Practitioners NT Department of Health and Families WA Department of Education Aboriginal Health Council of Western Australia School of Medicine and Public Health, University of Newcastle Remote Area Health Corps Rural Health Workforce Australia Congress of Aboriginal and Torres Strait Islander Nurses Community Services and Health Industry Skills Council WA Department of Health, Aboriginal Health Improvement Unit.
Awareness and impact
The ability of the evaluation to comment on awareness and impact of the two campaigns for 2010-11 is limited for the following reasons: the campaigns were in the developmental/early implementation stages
during this reporting period and thus significant progress against identified 302
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
results cannot be expected to have been achieved at this early stage. Note, the evaluation does provide some commentary on the awareness of stakeholders of these campaigns as the evaluation activities were undertaken during the early months after the launch of the two campaigns; and
the evaluation had not engaged the key target audience of Aboriginal and Torres Strait Islander secondary school students.
Based on information available, the evaluation has found that in 2010-11 there was limited awareness of the campaigns amongst those Aboriginal and Torres Strait Islander community members consulted by the evaluators.This finding has been informed by consultations with community members and service providers through site visits, and with national stakeholders.
Health Heroes campaign
A number of health service stakeholders engaged during the community site visits were aware of the Health Heroes website, however, their awareness was only at a high level, i.e., they had heard the name and knew the site was focused on workforce. The majority of these health service stakeholders had not accessed the website. Further, no community members engaged in focus groups had heard of the Health Heroes campaign. Although these stakeholders were all over 18 years of age (i.e., not secondary school students) the campaign also targets key influencers including parents and carers of secondary school students, who may have been present during these consultations. One national stakeholder interviewed had received the Health Heroes promotional materials, and was using them to promote the campaign at student career expos. The promotional materials were sent to key stakeholder to encourage them to use and promote the resources. This stakeholder reported that the pamphlets and DVDs were reportedly the most popular materials. This stakeholder, from a peak organisation, had also sent the promotional materials to members. This suggests there is awareness about the campaign amongst appropriate stakeholders (in at least one case), and that the campaign may be reaching the intended target audience through the distribution of these materials.
Do Something Real campaign
Only a small number of health service stakeholders consulted through site visits had heard of the Do Something Real website, and none attributed the website as having an impact on their decision to take up roles in Aboriginal and Torres Strait Islander health. Again, no community members engaged through focus groups had heard of Do Something Real. Practicing health
303KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
workers and other community members are the key target audience of the Do Something Real Campaign. One stakeholder engaged through the site visits speculated that a lack of promotion of this measure may have led to limited awareness of the campaigns. At the time of writing this report, there was no quantitative information available relating to the campaign communication activities (i.e., development and dissemination of resources), access (i.e., to the websites) and impacts on educational attainment (e.g., education participation rates for Aboriginal and Torres Strait Islander students). 1.86 Facilitators and barriersThe following facilitators and barriers were identified for 2010-11: Strong evidence base for the measure: the first two years of
implementation of the measure were used to undertake developmental research and to develop and test campaign materials. This significant period of development underscores that this type of campaign is a new area of work for the department, which invested in knowledge generation and consultation to inform the social marketing approach. While being a ‘new area of work’ could be considered a barrier to efficient implementation, the developmental research is seen to have contributed to a strong evidence base for the measure, which may be a facilitator for future programs or for ongoing rollout, or both.
Limited Aboriginal and Torres Strait Islander specific social marketing capacity: based on the response to the tendering process, the department also learned that social marketing tailored to the context and audience of Aboriginal and Torres Strait Islander Australians is a new area for the market. This limited capacity is considered to have been a barrier to the efficient implementation of the measure.
Delays in contracting: the department received limited responses to two tenders released in December 2010 for the development of advertising material and conduct of public relations and community engagement for both campaigns due to the lack of specific social marketing capacity outlined above. The second round of tendering in January 2011 was more successful, with relevant providers being contracted in May 2011. However, the requirement to go to tender twice led to delays in commencing campaign development.
1.87 OpportunitiesThe lack of awareness of the Health Heroes and Do Something Real websites in the community indicates that ongoing and targeted promotion is critical. The development and testing of the Health Heroes promotional materials provides the opportunity to progress to broader promotion to the target
304KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
audience. Promotion to students, for example, through career days and schools has been considered useful by some stakeholders to date.
305KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Clinical Practice and Decision Support Resources (C5)This chapter describes the progress of the Clinical Practice and Decision Support Resources measure against relevant activities and outputs (as described in the Evaluation Framework); it discusses findings against expected results identified within the Evaluation Framework and barriers, facilitators and opportunities identified to date. Clinical Practice and Decision Support Resources at a glanceA number of key resources were developed in 2010-11, including the development of the first iteration of the web-based primary health care resource and the National Guide to Preventative Health Assessment for Aboriginal and Torres Strait Islander people. The implementation of the measure however, has been slower than expected.Specifically, issues experienced during the pilot testing stage led to difficulties in recruiting participants to the pilot that limited the testing of components of the web-based resource. This resulted in the resource not being progressed beyond the piloting stage. As the resources were still at pilot testing stage during 2010-11, there is no evidence of outcomes at this date. Potential effects based on implementation findingsFigure 25 below is the causal pathway for the Clinical Practice and Decision Support Resources measure. The causal pathway illustrates the expected outcomes that should occur as a result of the activities of the measure.
306KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Clinical Practice and Decision Support
Guidelines
Increase in care providers' knowledge, understanding
and skills
Increase in better practice management of chronic
disease
Increase in health system capacity and capability to deliver primary health care services to Aboriginal and
Torres Strait Islander people
Providers utilise the resources
appropriately
Providers access and
engage with the resources
Providers know how to
access the resources
Resources are fit for purpose
Figure 25: Clinical Practice and Decision Support Resources causal pathway. Source: KPMG. The tables below provide a summary of two key components of the Analytical Framework for the evaluation, that link to the causal pathways: the plausibility of effect300 and the observed impacts.301 Both the plausibility and observed impacts of the measures can be influenced by contextual factors, which are also identified in the tables below. below presents the evaluation’s assessment of evidence from 2010-11 relating to the key dependencies for this measure (outlined in the causal pathway diagram above). The focus and thus the design of the measure was changed from adapting existing chronic disease management resources to increasing the access to existing resources through a website. The decision to change the measure was based on advice from a technical reference group. To the extent that the advice of the Technical Reference Group was appropriate (i.e., that the lack of ready access to existing resources was the more significant issue), then the redesign of this measure is likely to enhance its effectiveness. 300 The plausibility of the measures having their desired effect against the expected result areas is influenced by two things: whether any changes have occurred to the measures since implementation (which may enhance or reduce the plausibility); and whether the key dependencies and assumptions identified within the causal pathway (light blue text boxes) have been achieved/are in place.301 Observed impacts provide an indication of how the measures are tracking against the expected outcomes (dark blue bubbles) within the causal pathway i.e., whether the measures are on track to achieving their identified outcomes.
307KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
The measure was further modified in 2010-11 to include the development of the second edition of the National Guide to Preventative Health Assessment for Aboriginal and Torres Strait Islander People. No information is available about the impact of this most recent modification on plausibility, as the complementarity of this Guide to the resource cannot be assessed, nor can its value.There has been some delay with the final rollout of the website and thus the evaluation is not able to comment on its effectiveness. There are several contextual factors that could impact on the measure’s effectiveness that relate mainly to access to the website; whether access can be integrated into the usual care activities of health workers; and the specificity of the content of the website.
308KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 73: Assessment of key dependencies of the C5 measure.
Key dependencies FindingsProviders access and engage with the resources
The resources were still at pilot testing stage during 2010-11. Data was therefore not available for the First Monitoring Report.
Providers know how to access the resources
Data not available for the First Monitoring Report.
Providers utilise the resources appropriately
Data not available for the First Monitoring Report.
Resources are fit for purpose
Data not available for the First Monitoring Report.
Contextual considerations
The contextual considerations relating to the plausibility of this measure are: The location of health care providers is likely to
influence factors that may in turn influence the uptake of the web-based resource. For example, there may be issues with access to the internet in remote areas, which may inhibit the use of web-based resources.
The characteristics and location of Aboriginal and Torres Strait Islander people (patients) is also likely to influence whether health care providers use particular resources, as patients have specific needs for chronic disease care and management due to a range of factors including their geographical remoteness and the requirement for culturally appropriate care.302 These variations amongst patients are more likely to influence the types of resources accessed rather than the uptake overall.
302 Steering Committee for the Review of Indigenous Service Provision 2007, Overcoming Indigenous Disadvantage Key Indicators 2007, Report, Commonwealth of Australia, Canberra.
309KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.
National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Table 74 below presents the evaluation’s findings with respect to the expected impacts for this measure (outlined in the causal pathway diagram above). There has been some delay with the final rollout of the website and thus the evaluation is not able to comment on its impacts. A number of key resources were developed in 2010-11, including the first iteration of the web-based primary health care resource and the National Guide to Preventative Health Assessment for Aboriginal and Torres Strait Islander people. The implementation of the measure however, was slower than expected, and the resources were still at pilot testing stage during 2010-11. Accordingly, data is not available for any of the expected impacts in 2010-11, and no contextual considerations were identified.Table 74: Assessment of likely effects of the C5 measure based on implementation progress.
Expected Observed impacts EvidenceIncrease in care providers’ understanding and skills
Data not available for the First Monitoring Report.
Not applicable
Increase in better practice management of chronic disease
Data not available for the First Monitoring Report.
Not applicable
Increase in health system capacity and capability to deliver primary health care services to Aboriginal and Torres Strait Islander people
Data not available for the First Monitoring Report.
Not applicable
Contextual considerations
None identified. Not applicable
1.88 Measure overviewThe Clinical Practice and Decision Support Resources measure involves development of a web-based resource to provide primary health care
310KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
providers with increased access to chronic disease clinical care information that is relevant to Aboriginal and Torres Strait Islander people. In 2010-11, the measure was expanded to include the development of the second edition of the National Guide to Preventative Health Assessment for Aboriginal and Torres Strait Islander people. In 2010-11 the actual expenditure was $1.301 million. 1.89 Web-based primary health care resourceThe main focus of the 2010-11 year was the development and pilot testing of the web based primary health care resource. The evaluation found that delays in pilot testing led to slower than expected progress of the Clinical Practice and Decision Support Resources measure.This finding has been informed by consultations with the department and national stakeholders involved with the measure, documentation review and Regional Forums. Hewlett Packard was engaged by the department in June 2010 to develop and pilot a web-based primary health care resource by the end of the calendar year. The pilot version of the web based primary health care resource went ‘live’ on the internet in October 2010.303 The first pilot test of the web based primary health care resource took place over two weeks in late November and early December 2010 with three participating Indigenous Health Services: Nunkuwarrin Yunti Inc. (South Australia), Gilles Plains Aboriginal Outreach Health Services (South Australia) and the Santa Teresa Health Clinic (Northern Territory). The department experienced difficulty in securing participants for the pilot project, due to a number of factors. The main reason was the difficulty around diverting primary health professionals from ordinary duties, as the testing process required intensive participation over a short period of time. The requirement to only use participants who used the Medical Director or Best Practice information systems in order to test the InfoButton feature also created a challenge (note: none of the three pilot sites had the InfoButton feature).304
The first pilot testing report305 developed by Hewlett Packard identified the following issues: short time frame for testing;
303 Available here 304 Hewlett Packard 2010, Department for Health and Ageing – Web based primary health care resource, Final report, Version 1.0, Department of Health and Ageing, Canberra. 305 ibid.
311KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
small number of participating sites; lack of participation from mainstream primary health care practices; and the InfoButton was not tested. Notwithstanding the testing constraints, the pilot did lead to some changes to the application, namely, some resource items were reclassified, a new classification of resource was added (‘patient education’), additional material was added on ICDP measures (e.g., information on PIP Indigenous Health Incentive; PBS co-payment), and the graphic user interface was updated. The department decided to run a second round of pilot testing to overcome the limitations of the initial pilot testing, and on 28 March 2011, contracted the Improvement Foundation Australia to assist with recruitment of practices. The Improvement Foundation also experienced difficulties with participant recruitment.306 The second pilot was conducted in the 2011-12 fiscal year, and the results of this pilot will be reported on in the next Monitoring Report which covers this fiscal period.While the resource has been publicly accessible since completion of the first round of pilot testing, there had been no public promotion of the site as at the end of 2010-11, as it was not generally intended to be used by the general public. Note that the pilot testing involved this preliminary version of the product, while the full production version will be developed following another tendering process in 2011-12. The measure was expanded to include the development of the second edition of the National Guide to Preventative Health Assessment for Aboriginal and Torres Strait Islander people. The RACGP, in conjunction with NACCHO, was funded to produce and distribute this guide due for completion in 2011-12. This was not part of the original measure plan but was incorporated based on advice from professional groups and was able to be funded because of unexpended funds in other parts of the ICDP.There was little knowledge of this measure amongst stakeholders consulted during the evaluation. Only one national stakeholder said they had heard the guidelines were being developed, and no other stakeholders (including health workers in the community) were aware of the measure. Additionally, as the website is yet to be launched, there is no data available on website use. 1.90 Facilitators and barriersBarriers identified for 2010-11 concern the implementation of the measure throughout the pilot phase:
306 KPMG consultation with Measure Manager (October 2011). 312
KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and
the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under Professional Standards Legislation.

National Monitoring and Evaluation of the Indigenous Chronic Disease Package
First Monitoring Report2010-11
Short pilot testing timeframes: the first pilot testing phase had very short timelines and there was insufficient participation to undertake robust pilot testing.
Lack of an ongoing role for the Technical Reference Group: this issue was discussed by stakeholders at the Regional Forums and in national stakeholder consultations; with stakeholders noting that the last meeting of the Technical Reference Group (TRG) was held in August 2010, prior to the development and testing of the pilot resource, and that the TRG was not involved in assessing the pilot product, nor the results of the first pilot testing.
1.91 OpportunitiesThe challenges experienced in the early stages of the Clinical Practice and Decision Support Guidelines measure present learnings about the conduct of future projects involving web-based resources. Specifically, there are opportunities to modify the pilot process so that more organisations might choose to be involved in pilot testing, and opportunities to better promote the resource to increase awareness. There is also considerable opportunity to promote this resource within the ICDP and specifically for use by various ICDP workforce elements. There was little knowledge of this measure amongst Regional Forum participants with one participant stating that they were about to embark on some research to identify chronic disease resource materials for use within the health service. Finally, there may be a need for additional expert input to ensure recommended resources are of sufficient quality to warrant inclusion, and for ensuring that the resource list is current.
313KPMG is an Australian partnership and a member firm of the KPMG network of independent member firms affiliated with
KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Printed in Australia. KPMG and the KPMG logo are registered trademarks of KPMG International. Liability limited by a scheme approved under
Professional Standards Legislation.

















