JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1975, p. 486-497 Copyright X 1975 American Society for Microbiology Vol. 2, No. 6 Printed in U.SA. Nationwide Epidemic of Septicemia Caused by Contaminated Intravenous Products: Mechanisms of Intrinsic Contamination DONALD C. MACKEL,* DENNIS G. MAKI, ROGER L. ANDERSON, FRANK S. RHAME, AND JOHN V. BENNETT Hospital Infections Branch, Bureau of Epidemiology, Center for Disease Control, Atlanta, Georgia 30333 Received for publication 25 August 1975 Between 1 July 1970 and April 1971, in many hospitals in this country, there were outbreaks of nosocomial septicemia caused by Enterobacter cloacae or E. agglomerans (formerly Erwinia, herbicola-lathyri). All of these hospitals used infusion products manufactured by one company, Abbott Laboratories, and all affected patients had onset of septicemia while receiving the company's infusion products. Septicemia was epidemiologically and microbiologically traced to intrinsic contamination of the company's screw-cap closure for infusion bottles which was sealed with a newly introduced elastomer liner. Epidemic organisms were isolated from these closures. Investigations both in the laboratory and in the manufacturing plant into the mechanism of contamination of these products revealed the following. (i) Epidemic strains were present in numerous areas throughout the manufacturing plants. (ii) Viable microorganisms gained access to the interior of screw-cap closures after the autoclave step of production. (iii) Cooling closures actively drew moisture through the thread interstices into the inner-most depths of the closure. (iv) Transfer of contaminants from closures to fluid was easily effected by simple manipulations duplicating normal in-hospital use. (v) The red-rubber liner used in the company's screw-cap closures before the introduction of elastomer contained a broad-spectrum antimicrobial inhibitor. The findings from this epidemic and the associated studies show that the screw- cap closure as it is now designed cannot be considered secure for products that must remain sterile. Between 1 July 1970 and April 1971, many hospitals in this country that routinely used infusion products made by one manufacturer, Abbott Laboratories, experienced outbreaks of septicemia with Enterobacter cloacae or Entero- bacter agglomerans (formerly called Erwinia, herbicola-lathyri group [10]) (3-5; D. G. Maki, F. S. Rhame, D. C. Mackel, and J. V. Bennett, Am. J. Med., in press). Epidemiological and microbiological investigations showed that the epidemic was caused by intrinsic microbial contamination of a newly introduced screw-cap closure with an elastomer liner (Maki et al., Am. J. Med., in press). The new elastomer- lined cap replaced caps incorporating shel- lacked paper (Gilsonite) and red rubber liners beginning in March 1970 (Fig. 1). Studies were undertaken in late February 1971 to determine the mechanisms by which the product became contaminated during manufac- ture. Investigations were conducted at both of Abbott's two manufacturing plants in March 1971 at the invitation and with the cooperation of the company. The studies reported here are based only on investigations at the Rocky Mount, N.C., plant. Screw-cap closures with elastomer liners were in use on all intravenous fluids produced by this plant at the time of these investigations. Additional experiments to determine the means by which closures and fluids became contaminated were conducted at the Center for Disease Control, Atlanta, Ga. MATERIALS AND METHODS The manufacturing process. The steps in produc- tion of infusion fluids in Abbott's Rocky Mount plant during the epidemic are depicted in Fig. 2. Bottles, after being inspected and washed, moved through the various production steps on a stainless steel conveyer belt. Caps were machine assembled from individual components within the plant each day, but assembled caps were routinely stored for several months before being used on bottles. Bottles were filled, loaded onto autoclave racks, autoclaved, unloaded to the conveyer belt, and rinsed, all by machine. They were then hand inspected, labeled and oversealed by machine, and the metal strap 486 Downloaded from https://journals.asm.org/journal/jcm on 06 February 2022 by 191.53.237.52.
Transcript
JOURNAL OF CLINICAL MICROBIOLOGY, Dec. 1975, p. 486-497Copyright X 1975 American Society for Microbiology
Vol. 2, No. 6Printed in U.SA.
Nationwide Epidemic of Septicemia Caused by ContaminatedIntravenous Products: Mechanisms of
Intrinsic ContaminationDONALD C. MACKEL,* DENNIS G. MAKI, ROGER L. ANDERSON, FRANK S. RHAME,
AND JOHN V. BENNETT
Hospital Infections Branch, Bureau of Epidemiology, Center for Disease Control, Atlanta, Georgia 30333
Received for publication 25 August 1975
Between 1 July 1970 and April 1971, in many hospitals in this country, therewere outbreaks of nosocomial septicemia caused by Enterobacter cloacae or E.agglomerans (formerly Erwinia, herbicola-lathyri). All of these hospitals usedinfusion products manufactured by one company, Abbott Laboratories, and allaffected patients had onset of septicemia while receiving the company's infusionproducts. Septicemia was epidemiologically and microbiologically traced tointrinsic contamination of the company's screw-cap closure for infusion bottleswhich was sealed with a newly introduced elastomer liner. Epidemic organismswere isolated from these closures. Investigations both in the laboratory and inthe manufacturing plant into the mechanism of contamination of these productsrevealed the following. (i) Epidemic strains were present in numerous areasthroughout the manufacturing plants. (ii) Viable microorganisms gained accessto the interior of screw-cap closures after the autoclave step of production. (iii)Cooling closures actively drew moisture through the thread interstices into theinner-most depths of the closure. (iv) Transfer of contaminants from closures tofluid was easily effected by simple manipulations duplicating normal in-hospitaluse. (v) The red-rubber liner used in the company's screw-cap closures before theintroduction of elastomer contained a broad-spectrum antimicrobial inhibitor.The findings from this epidemic and the associated studies show that the screw-cap closure as it is now designed cannot be considered secure for products thatmust remain sterile.
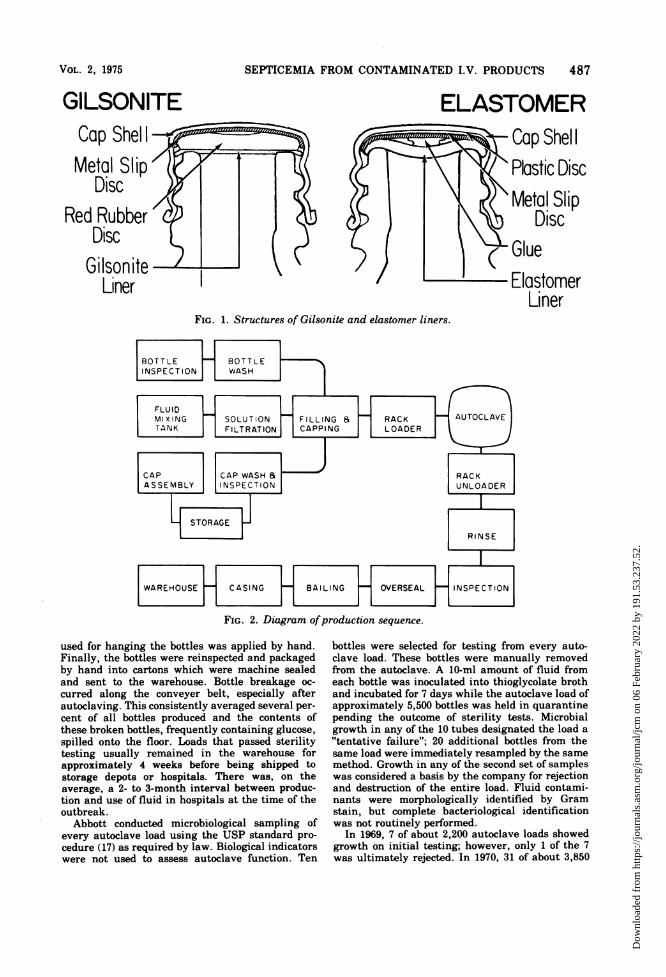
Between 1 July 1970 and April 1971, manyhospitals in this country that routinely usedinfusion products made by one manufacturer,Abbott Laboratories, experienced outbreaks ofsepticemia with Enterobacter cloacae or Entero-bacter agglomerans (formerly called Erwinia,herbicola-lathyri group [10]) (3-5; D. G. Maki,F. S. Rhame, D. C. Mackel, and J. V. Bennett,Am. J. Med., in press). Epidemiological andmicrobiological investigations showed that theepidemic was caused by intrinsic microbialcontamination of a newly introduced screw-capclosure with an elastomer liner (Maki et al.,Am. J. Med., in press). The new elastomer-lined cap replaced caps incorporating shel-lacked paper (Gilsonite) and red rubber linersbeginning in March 1970 (Fig. 1).
Studies were undertaken in late February1971 to determine the mechanisms by which theproduct became contaminated during manufac-ture. Investigations were conducted at both ofAbbott's two manufacturing plants in March1971 at the invitation and with the cooperation
of the company. The studies reported here arebased only on investigations at the RockyMount, N.C., plant. Screw-cap closures withelastomer liners were in use on all intravenousfluids produced by this plant at the time ofthese investigations. Additional experiments todetermine the means by which closures andfluids became contaminated were conducted atthe Center for Disease Control, Atlanta, Ga.
MATERIALS AND METHODSThe manufacturing process. The steps in produc-
tion of infusion fluids in Abbott's Rocky Mountplant during the epidemic are depicted in Fig. 2.Bottles, after being inspected and washed, movedthrough the various production steps on a stainlesssteel conveyer belt. Caps were machine assembledfrom individual components within the plant eachday, but assembled caps were routinely stored forseveral months before being used on bottles. Bottleswere filled, loaded onto autoclave racks, autoclaved,unloaded to the conveyer belt, and rinsed, all bymachine. They were then hand inspected, labeledand oversealed by machine, and the metal strap
486
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
SEPTICEMIA FROM CONTAMINATED I.V. PRODUCTS 487
GILSONITECap ShelIXMetal Slip
DiscRed Rubber 4&
Liner
ELASTOMER~Cap ShellI
Plastic DiscMetal Slip
Disc~Glue
ElastomerLiner
FIG. 1. Structures of Gilsonite and elastomer liners.
FIG. 2. Diagram ofproduction sequence.
used for hanging the bottles was applied by hand.Finally, the bottles were reinspected and packagedby hand into cartons which were machine sealedand sent to the warehouse. Bottle breakage oc-curred along the conveyer belt, especially afterautoclaving. This consistently averaged several per-cent of all bottles produced and the contents ofthese broken bottles, frequently containing glucose,spilled onto the floor. Loads that passed sterilitytesting usually remained in the warehouse forapproximately 4 weeks before being shipped tostorage depots or hospitals. There was, on theaverage, a 2- to 3-month interval between produc-tion and use of fluid in hospitals at the time of theoutbreak.
Abbott conducted microbiological sampling ofevery autoclave load using the USP standard pro-cedure (17) as required by law. Biological indicatorswere not used to assess autoclave function. Ten
bottles were selected for testing from every auto-clave load. These bottles were manually removedfrom the autoclave. A 10-ml amount of fluid fromeach bottle was inoculated into thioglycolate brothand incubated for 7 days while the autoclave load ofapproximately 5,500 bottles was held in quarantinepending the outcome of sterility tests. Microbialgrowth in any of the 10 tubes designated the load a"tentative failure"; 20 additional bottles from thesame load were immediately resampled by the samemethod. Growth in any of the second set of sampleswas considered a basis by the company for rejectionand destruction of the entire load. Fluid contami-nants were morphologically identified by Gramstain, but complete bacteriological identificationwas not routinely performed.
In 1969, 7 of about 2,200 autoclave loads showedgrowth on initial testing; however, only 1 of the 7was ultimately rejected. In 1970, 31 of about 3,850
VOL. 2, 1975
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
488 MACKEL ET AL.
autoclave loads showed initial growth and 10 were
ultimately rejected; 28 of these 31 autoclave loadsoccurred during the 9-month period from Aprilthrough November 1970. This marked rise in posi-tivity during 1970 coincided temporally with theintroduction and progressive increase in use ofelastomer-lined closures at the plant, which beganin March 1970. Increased rates of lots failing theinitial sterility test occurred during this time withautoclave loads of Gilsonite and elastomer, whencompared with baseline 1969 rates (solely Gil-sonite).
Besides the required microbiological quality con-
trol sampling of every autoclave load, Abbott car-
ried out an environmental contamination surveil-lance program. Multiple water samples from theproduction line at various stages of the manufac-turing process, especially from the autoclave, were
sampled daily. The plant received potable munici-pal water from the town of Rocky Mount, which was
6 miles (about 9.6 km) away. Chlorine residuals inthis water were consistently less than 0.1 part per
million (ppm), and bacteriological testing hadshown frequent contamination in the past. During1970, high bacterial counts were occasionally re-
corded in water samples from the autoclave duringthe cooling cycle; however, organisms had not beenmicrobiologically identified. Each autoclave loadwas monitored by thermo-couple testing. Because ofthe relatively low chlorine residuals in city waterreceived in the plant, water used in the autoclavecooling cycle was either selectively chlorinated or
passed through an ultraviolet decontaminator.After the sterilization step of the autoclave cycle,the load was slowly cooled by the autoclave conden-sate and chlorinated, or ultraviolet-treated waterwas progressively introduced. The autoclave coolanttemperature immediately prior to removal of theload was approximately 25 C, and the temperatureof the bottles at this point was about 40 C.
Microbiological methods. The enrichment brothused in all studies, both for field investigations andlaboratory studies, was brain heart infusion brothenriched with 0.5% beef extract (EBHIB). Variousamounts and concentrations of broth were useddepending upon the final dilution resulting from thesamples and sampling procedures used.
Intravenous fluid was cultured by the addition ofconcentrated EBHIB directly into the bottle (Makiet al., Am. J. Med., in press). Studies on 107one-liter bottles of fluid had compared this tech-nique to membrane filtration under strict asepticconditions in a laminar flow hood. One-half of eachbottle was passed through a bacteriological mem-
brane filtration system (0.45 ,um pore size, MilliporeCorp.). The filter was then placed onto Trypticasesoy agar containing 5% sheep blood with its surfacepremoistened with 0.2 ml of EBHIB. Samples were
incubated for 48 h at 35 to 37 C and then at room
temperature for 5 days. The remaining 500 ml ineach bottle was cultured by adding an equal volumeof double-strength EBHIB. These were incubated at35 to 37 C and discarded at 7 days if no growthappeared. Contaminants in the fluid, including theepidemic strains, were isolated in a substantially
higher frequency from fluid that was sampled by thedirect addition of concentrated broth (Table 1).
Unless stated otherwise, all cultures were incu-bated at 35 to 37 C for 18 to 24 h and then examinedfor growth. All cultures having no growth were
incubated at room temperature for at least 5 more
days and reexamined daily. All broth culturesshowing growth were streaked to Trypticase soyagar containing 5.0% sheep blood (TSAB) and toMacConkey agar. Representatives of all distinctmicrobial colonies were picked and inoculated totriple sugar iron agar unless colonial morphologyand Gram stain suggested the use of a differentmedium.
Standard procedures were used for the definitiveidentification of isolated organisms. Susceptibilityof isolates to antibiotics was determined by a stan-dardized disk testing technique (1).
RESULTS
A. Environmental studies at the productionfacility. The environmental studies at the pro-duction facility were designed to determine ifthe epidemic strains were present in theinanimate environment of the plant and, if so,where and in what numbers.Samples were collected during normal pro-
duction. Surface samples were taken withcotton swabs premoistened in EBHIB; thesewere rubbed over the sampling area andbroken off into a tube containing 6 ml ofbroth. Samples of water and liquid quaternaryammonium compound (used as a conveyer beltlubrication) were filtered through a 0.45-,tmmembrane filter. Membrane filters used forsampling belt lubricants were washed with an
equal volume of EBHIB-containing neutral-izers, 0.5% Tween 80, and 0.07% lecithin. Inaddition, portions of belt lubricant were inocu-lated directly into neutralizing broth for cul-ture. Air sampling was performed by 10-minexposures of open petri dishes containingTSAB.Of the 96 environmental samples, 16 (17%)
TABLE 1. Comparative microbiological results fromdirect addition of broth and membrane filtration
techniques
No. of bottles with:
Any or- Epidemicganisms organisms
Positive only by broth tech- 17 5nique
Positive only by membrane fil- 0 0tration techniques
Positive by both methods 25 0Negative by both techniques 65 102
J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
SEPTICEMIA FROM CONTAMINATED I.V. PRODUCTS 489
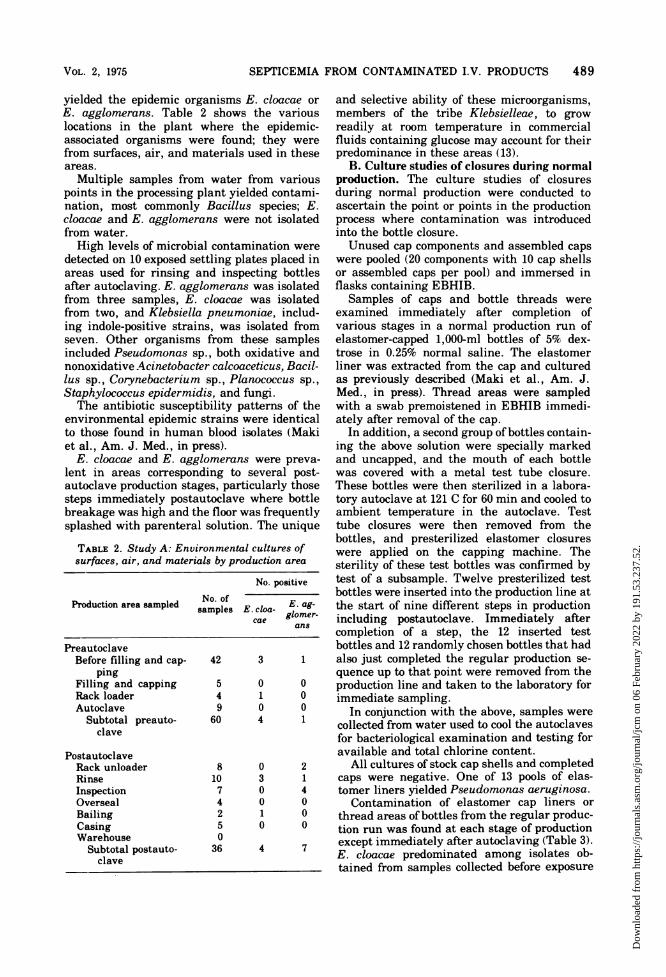
yielded the epidemic organisms E. cloacae orE. agglomerans. Table 2 shows the variouslocations in the plant where the epidemic-associated organisms were found; they werefrom surfaces, air, and materials used in theseareas.
Multiple samples from water from variouspoints in the processing plant yielded contami-nation, most commonly Bacillus species; E.cloacae and E. agglomerans were not isolatedfrom water.High levels of microbial contamination were
detected on 10 exposed settling plates placed inareas used for rinsing and inspecting bottlesafter autoclaving. E. agglomerans was isolatedfrom three samples, E. cloacae was isolatedfrom two, and Klebsiella pneumoniae, includ-ing indole-positive strains, was isolated fromseven. Other organisms from these samplesincluded Pseudomonas sp., both oxidative andnonoxidative Acinetobacter calcoaceticus, Bacil-lus sp., Corynebacterium sp., Planococcus sp.,Staphylococcus epidermidis, and fungi.The antibiotic susceptibility patterns of the
environmental epidemic strains were identicalto those found in human blood isolates (Makiet al., Am. J. Med., in press).
E. cloacae and E. agglomerans were preva-lent in areas corresponding to several post-autoclave production stages, particularly thosesteps immediately postautoclave where bottlebreakage was high and the floor was frequentlysplashed with parenteral solution. The unique
TABLE 2. Study A: Environmental cultures ofsurfaces, air, and materials by production area
No. positive
Production area sampled No. ofglomsamples E. cloa-Eagloe-cae gomr
and selective ability of these microorganisms,members of the tribe Klebsielleae, to growreadily at room temperature in commercialfluids containing glucose may account for theirpredominance in these areas (13).
B. Culture studies of closures during normalproduction. The culture studies of closuresduring normal production were conducted toascertain the point or points in the productionprocess where contamination was introducedinto the bottle closure.Unused cap components and assembled caps
were pooled (20 components with 10 cap shellsor assembled caps per pool) and immersed inflasks containing EBHIB.
Samples of caps and bottle threads wereexamined immediately after completion ofvarious stages in a normal production run ofelastomer-capped 1,000-ml bottles of 5% dex-trose in 0.25% normal saline. The elastomerliner was extracted from the cap and culturedas previously described (Maki et al., Am. J.Med., in press). Thread areas were sampledwith a swab premoistened in EBHIB immedi-ately after removal of the cap.
In addition, a second group of bottles contain-ing the above solution were specially markedand uncapped, and the mouth of each bottlewas covered with a metal test tube closure.These bottles were then sterilized in a labora-tory autoclave at 121 C for 60 min and cooled toambient temperature in the autoclave. Testtube closures were then removed from thebottles, and presterilized elastomer closureswere applied on the capping machine. Thesterility of these test bottles was confirmed bytest of a subsample. Twelve presterilized testbottles were inserted into the production line atthe start of nine different steps in productionincluding postautoclave. Immediately aftercompletion of a step, the 12 inserted testbottles and 12 randomly chosen bottles that hadalso just completed the regular production se-quence up to that point were removed from theproduction line and taken to the laboratory forimmediate sampling.
In conjunction with the above, samples werecollected from water used to cool the autoclavesfor bacteriological examination and testing foravailable and total chlorine content.
All cultures of stock cap shells and completedcaps were negative. One of 13 pools of elas-tomer liners yielded Pseudomonas aeruginosa.
Contamination of elastomer cap liners orthread areas of bottles from the regular produc-tion run was found at each stage of productionexcept immediately after autoclaving (Table 3).E. cloacae predominated among isolates ob-tained from samples collected before exposure
VOL. 2, 1975
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
490 MACKEL ET AL.
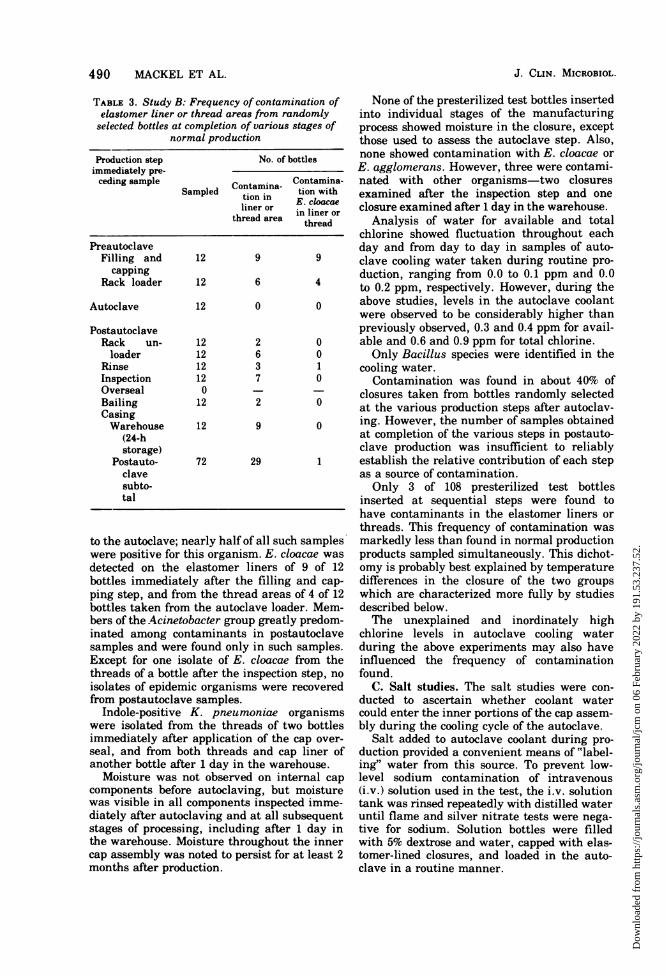
TABLE 3. Study B: Frequency of contamination ofelastomer liner or thread areas from randomlyselected bottles at completion of various stages of
normal production
Production step No. of bottlesimmediately pre-ceding sample Contamina- Contamina-
to the autoclave; nearly half of all such sampleswere positive for this organism. E. cloacae was
detected on the elastomer liners of 9 of 12bottles immediately after the filling and cap-ping step, and from the thread areas of 4 of 12bottles taken from the autoclave loader. Mem-bers of the Acinetobacter group greatly predom-inated among contaminants in postautoclavesamples and were found only in such samples.Except for one isolate of E. cloacae from thethreads of a bottle after the inspection step, no
isolates of epidemic organisms were recoveredfrom postautoclave samples.
Indole-positive K. pneumoniae organismswere isolated from the threads of two bottlesimmediately after application of the cap over-
seal, and from both threads and cap liner ofanother bottle after 1 day in the warehouse.
Moisture was not observed on internal cap
components before autoclaving, but moisturewas visible in all components inspected imme-diately after autoclaving and at all subsequentstages of processing, including after 1 day inthe warehouse. Moisture throughout the innercap assembly was noted to persist for at least 2months after production.
None of the presterilized test bottles insertedinto individual stages of the manufacturingprocess showed moisture in the closure, exceptthose used to assess the autoclave step. Also,none showed contamination with E. cloacae orE. agglomerans. However, three were contami-nated with other organisms-two closuresexamined after the inspection step and oneclosure examined after 1 day in the warehouse.
Analysis of water for available and totalchlorine showed fluctuation throughout eachday and from day to day in samples of auto-clave cooling water taken during routine pro-duction, ranging from 0.0 to 0.1 ppm and 0.0to 0.2 ppm, respectively. However, during theabove studies, levels in the autoclave coolantwere observed to be considerably higher thanpreviously observed, 0.3 and 0.4 ppm for avail-able and 0.6 and 0.9 ppm for total chlorine.Only Bacillus species were identified in the
cooling water.Contamination was found in about 40% of
closures taken from bottles randomly selectedat the various production steps after autoclav-ing. However, the number of samples obtainedat completion of the various steps in postauto-clave production was insufficient to reliablyestablish the relative contribution of each stepas a source of contamination.Only 3 of 108 presterilized test bottles
inserted at sequential steps were found tohave contaminants in the elastomer liners orthreads. This frequency of contamination wasmarkedly less than found in normal productionproducts sampled simultaneously. This dichot-omy is probably best explained by temperaturedifferences in the closure of the two groupswhich are characterized more fully by studiesdescribed below.The unexplained and inordinately high
chlorine levels in autoclave cooling waterduring the above experiments may also haveinfluenced the frequency of contaminationfound.
C. Salt studies. The salt studies were con-ducted to ascertain whether coolant watercould enter the inner portions of the cap assem-bly during the cooling cycle of the autoclave.
Salt added to autoclave coolant during pro-duction provided a convenient means of "label-ing" water from this source. To prevent low-level sodium contamination of intravenous(i.v.) solution used in the test, the i.v. solutiontank was rinsed repeatedly with distilled wateruntil flame and silver nitrate tests were nega-tive for sodium. Solution bottles were filledwith 5% dextrose and water, capped with elas-tomer-lined closures, and loaded in the auto-clave in a routine manner.
J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
SEPTICEMIA FROM CONTAMINATED I.V. PRODUCTS 491
A control group of 20 bottles was not auto-claved and not exposed to salt-laden coolant.
In addition, a rubber finger cot was placedover the entire closure of a second control groupof 20 production bottles which were positionedthroughout the autoclave load in a randomfashion.The bottles in the autoclave were then steri-
lized in routine production fashion. As the tem-perature approached 100 C during the coolingcycle, approximately 700 lb (about 318 kg) ofcommercial bulk salt was rapidly introducedinto the cooling water line at the autoclavepump. In the second test, the entire experimentwas repeated, except salt was introduced whenthe temperature reached 60 C. In both testsclosures were exposed for 10 to 20 min tocoolant containing salt.At the end of the cooling cycle, bottles were
removed from the autoclave and immediatelytaken to the laboratory for analysis of sodiumin the inner cap assembly components. The topof the cap was carefully removed with a sharpknife without altering the relationship of thecap to the bottle thread area. The technologisttested for sodium chloride by adding minutedroplets of 0.1% silver nitrate to the variousareas and looking for formation of white silverchloride precipitate. The presence of sodiumwithin the intrinsic moisture found in variousportions of the cap assembly was also tested forby probing with a clean platinum wire loopwhich was then flamed.The salt concentration of the cooling water in
the two experiments was 1.0 and 0.6%, respec-tively. In both experiments, whether salt wasadded at the beginning or the middle of thecooling cycle, sodium chloride was repeatedlydetected in the interstices of the thread areasall the way to the elastomer disk of every clo-sure tested (Fig. 1). Salt was also found in thespace between the metal slip disk and theelastomer liner. No sodium chloride was de-tected on the inner surface of the elastomerdisk that faces fluid or within the fluid itself.No sodium chloride was detected in the 40
caps covered with rubber finger cots during thetwo experiments or in the control bottle capsfrom nonautoclaved bottles.The above observations indicated that auto-
clave cooling water, if contaminated withmicroorganisms, could have served as a vehicleby which the inner cap assembly became con-taminated. The absence of fluid in closureswith an impervious rubber "overseal" sug-gested a way to prevent access of contaminatedfluid to the closure during production.
D. Fluorescein dye studies of cap assem-blies. Fluorescein dye was utilized as a marker
to study factors influencing migration of envi-ronmental moisture into the closure.Twelve commercially obtained 1-liter bottles
of D5/W with elastomer-lined caps were stud-ied. Approximately 0.25 lb (about 113 g) ofwater-soluble uranine (sodium fluorescein) wasdissolved in tap water in deep stainless steelpans at room temperature. Upright bottleswere then exposed to the dye in three differentways.
In experiment D-1, four bottles, totallyimmersed in the dye solution, were heated to100 C, atmospheric pressure, for 40 min. Thebottles were then allowed to cool in the dyesolution to approximately 65 to 70 C beforeremoval and examination.
Experiment D-2 was similar to experimentD-1 except that four bottles were immersed inthe dye solution only up to a line approximately1 cm below the lower lip of the cap, i.e., at thelowermost thread of the neck.
In experiment D-3, four bottles were placedin a pan containing sufficient water withoutdye to create a fluid level at the middle of theupright bottles. The bottles were then heated to100 C in an autoclave and allowed to cool to atemperature of approximately 75 to 80 C; at thistime warmed dye solution (65 to 70 C) waspoured from above onto the tops of the caps.
Four control bottles were handled exactly asthe respective test bottles in each experimentexcept they were not heated.Each bottle was thoroughly wiped dry with a
clean Cel-Fiber paper towel immediately uponremoval from the dye solution. When the bottlereached room temperature, the top of the capwas removed with a clean knife immediatelyabove the plastic slip disk. Each inner compo-nent of the cap assembly was then carefullyremoved with clean hemostats and placed inseparate petri dishes. The presence of dye oneach individual component was tested usingwhite and long- and short-wave ultravioletlight.The control (nonheated) bottles showed no
fluorescence beyond the threaded area in anyof the experiments. In contrast, bottles whichhad been heated and allowed to cool had dyewithin the innermost portions ofthe closure, forexample, between the slip disk and liner, in allthree experiments.
Similar results were obtained when an equalnumber of bottles capped with Gilsonite-linedclosures were subjected to identical experimen-tal conditions.
This laboratory experiment confirmed theearlier studies (study B) which showed thatmovement of moisture into the closure de-pended upon a falling cap temperature. This
VOL. 2, 1975
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
492 MACKEL ET AL.
was not the sole mechanism of cap contami-nation, however, because control bottles atambient temperature in study B also mani-fested contamination, although in a greatlyreduced frequency.
E. Matched study comparing elastomer andGilsonite closures. As previously noted (Makiet al., Am. J. Med., in press), no cases of sep-ticemia were traced to Gilsonite-capped fluidsduring the nationwide outbreak. To determinethe relative frequency and nature of con-
tamination of closures and fluid, elastomer-and Gilsonite-capped fluids were processed inthe same production load under comparableconditions of manufacture.
Approximately 1,400 bottles of D5/1/4 normalsaline capped with Gilsonite closures were pro-duced in the middle of a 20,000-bottle elas-tomer-capped production run. Both productionautoclaves were employed to assess the differ-ential risk of contamination between the twoautoclaves in the plant. Immediately uponreaching the warehouse, random cases ofbottles with each type of closure were selectedand sent to the Center for Disease Control formicrobiological testing of caps and fluid.High-frequency contamination of both types
of closures was observed (Table 4). However,Gilsonite liners were significantly less fre-quently contaminated (26.9%) than elastomerliners (85.0%) (X2 = 85.6, P < 0.005). Further-more, E. cloacae and E. agglomerans wereisolated from 8.3% of closures lined with elas-tomer but from none of those lined with Gilson-ite (P = 0.001, Fisher's exact test). Of 120fluids from bottles with each type of closure,64.1% of the elastomer-lined closures and 23.3%of the Gilsonite-lined closures were contami-nated. Epidemic organisms were found in eightelastomer fluids, but in no fluids from Gil-sonite-capped bottles. Both Gilsonite and elas-tomer closures sampled within 2 weeks ofmanufacture were uniformly noted to containvisible moisture at the time they were openedfor culture.
Cultures from elastomer caps yielded ninedifferent microorganisms, including the two
epidemic species, whereas only three specieswere recovered from Gilsonite caps (Table 5),all of which were also isolated from elastomerliners. No fermentative organisms were iso-lated from Gilsonite closures.No significant differences were noted be-
tween the two autoclaves in contaminationrates of cap liners or fluids.The extraordinarily high frequency of con-
tamination ofelastomer closures compared withcultures of these closures from stock supplies(Maki et al., Am. J. Med., in press) or studyB may have been related to a lower free chlo-rine content of autoclave cooling water duringthe matched study (0.1 ppm, compared with0.3 to 0.4 ppm in study B). Also, the lowerfrequency of contamination of stock suppliescompared with the present study may havebeen related to the freshness of contamina-tion; virtually all stock supplies were culturedafter being stored for 1 or more months in theAbbott warehouse and the hospital which pro-vided time for the cap interior to dry.The lower frequency of overall contamina-
tion of Gilsonite compared with elastomer didnot seem to be explained by a lesser vulner-ability of the former to ingress of contaminated
TABLE 5. Study E: Microorganisms isolated fromcap enclosures
TABLE 4. Study E: Comparative study ofelastomer and Gilsonite closure and subsequent fluid contaminationduring production-matched study
Type of closure FluidDetermination
Elastomer Gilsonite Elastomer Gilsonite
No. sampled 120 115 120 120No. contaminated 102 (85.0%) 31 (26.9%) 77 (64.1%) 28 (23.3%)No. contaminated with 10 (8.3%) 0 (0.0%) 8 (6.6%) 0 (0.0%)E. cloacae or E. ag-glomerans
J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
SEPTICEMIA FROM CONTAMINATED I.V. PRODUCTS 493
moisture, since closures of both types uniformlydemonstrated moisture and behaved similarlyin study D with fluorescein dye. Therefore, thelower frequency of overall contamination andthe absence of the epidemic strains in Gilsonitecaps suggested the possibility of a microbialinhibitor in this closure.
F. Inhibitory properties of cap components.The following studies were undertaken toinvestigate the possibility of an inhibitor in theGilsonite closure.Agar and broth diffusion studies were per-
formed to detect possible inhibitory substancesfrom the components of Gilsonite and elas-tomer closures. Agar plate studies utilizedinocula identical to those used in standardizedantimicrobial disk susceptibility tests (1) andMueller-Hinton agar. Broth studies employedEBHIB and inocula of either 103 or 106 testorganisms. Organisms used for these studieswere isolated from either elastomer or Gilsoniteclosures except for the ATCC 25923 Staphylo-coccus aureus strain and a urinary isolate ofSerratia marcescens. Other organisms testedincluded two strains of E. cloacae, both aero-genic and anaerogenic E. agglomerans, onestrain each of indole-positive and indole-negative K. pneumoniae, and one strain eachof oxidative and nonoxidative A4. calcoaceticus,Bacillus sp., P. maltophilia, nonfermenter Ve,and a yeast species.Components were removed from assembled
closures furnished by the company and fromclosures of bottles from the matched studydescribed above; they were autoclave-sterilizedbefore use in the following tests.Agar plate diffusion studies showed that the
red rubber disk from the Gilsonite closureinhibited surface growth of E. cloacae and E.agglomerans. Zones of inhibition of 2 to 4 mmwere noted around the disk, and no growthoccurred under the disk. No inhibition occurredaround or under Gilsonite paper, elastomerliners, or other components of either cap.One thousand organisms of both epidemic
strains inoculated into 6 ml of broth containinga single red rubber liner showed no growthafter 48 h of incubation at 35 to 37 C. Inocu-lated broth alone as well as broth containingGilsonite paper or elastomer disks consistentlydemonstrated expected turbidity within 24 h.Epidemic strains were consistently inhibited inmore than 40 experiments using different redrubber liners. Using an inoculum of 10" orga-nisms, minimal growth of the epidemic strainsoccurred after overnight incubation, but tur-bidity was slight compared with growth in con-trol tubes (1+ compared to 4+ on a 0 to 4+scale).
Similar experiments were conducted on othertest strains using an inoculum of 10 in 6 ml ofbroth to which a single liner had been added.Again, the red rubber liner completely inhib-ited the test strains of Serratia, Klebsiella,Staphylococcus, Acinetobacter, Bacillus, andyeast, but only for 24 h; of all tested organisms,only P. aeruginosa was not inhibited.These experiments were repeated with red
rubber liners from Gilsonite closures takenfrom bottles that had been stored in a ware-house for at least 2 years after production; nodemonstrable inhibitory activity remained atthis time. However, red rubber liners fromclosures frozen at -10 C for 2 years retainedfull inhibitory activity.The above experiments indicated the pres-
ence of an antimicrobial inhibitor with broad-spectrum activity in the red rubber liner of theGilsonite closure; activity appeared to diminishwith time at room temperature. This propertyprobably best explains the significantly lowerfrequency of contamination of Gilsonite clo-sures and the failure to identify clinical infec-tions traced to these products. Epidemic strainswere more sensitive to the inhibitor than othertested organisms.
G. Contamination transfer from closures tofluid. When frequent contamination with epi-demic organisms of the elastomer closures ofstock products was recognized (Maki et al.,Am. J. Med., in press), studies were conductedto determine if microorganisms in cap linerscould be transferred to fluid.A number of serial manipulations were per-
formed on bottles with elastomer closures fromvarious 1-liter lots of solutions containing dex-trose. Several of the experimental manipula-tions were specifically designed to simulate asclosely as possible normal in-hospital practicesin infusion therapy.Only the elastomer liners in the caps were
cultured; these and fluids were sampled bymethods previously described (Maki et al., Am.J. Med., in press).
All sampling procedures were performed inlaminar flow hoods by technologists wearingsterile gloves and clean laboratory overgar-ments. Open petri dishes containing TSABwere exposed in the hoods to monitor the sterileair environment.
In experiment G-1, the side of the cap of 59bottles was struck gently on a bench edge, afterwhich the cap was carefully unscrewed andlifted just above the bottle lip. The cap wasthen immediately replaced and tightened andeach bottle was briefly shaken. (These actionssimulated the removal of a tight cap and theaddition to and mixing of an additive into the
VOL. 2, 1975
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
494 MACKEL ET AL.
solution.) All bottles were left at room tempera-ture for 48 h before both closures and fluidswere cultured. The 59 bottles were from fivedifferent lots.
In experiment G-2, the closure on each of 18test bottles was immediately replaced afterremoval without prior striking. Each bottlewas briefly shaken and then kept at roomtemperature for 48 h before caps and fluidswere cultured. As controls, 18 bottles from thesame lot were directly sampled without anymanipulation, i.e., the cap was removed andthe fluid was sampled immediately.
Exposed TSAB plates used for monitoring airin the laminar flow hoods were consistentlynegative for microbial growth.
Cultures of cap liners in experiment G-1showed microorganisms in 33 (57%) of 59samples, and microorganisms were detected in28 of 59 (48%) solutions examined (Table 6).Fluid within the bottle contained the sameorganism as found on its cap liner in 17instances (Table 7). A total of five fluids werefound contaminated with two microorganisms.In only three bottles in which the fluids werecontaminated were the caps sterile. The re-maining 25 positive fluids occurred among 33bottles with contaminated caps.
TABLE 6. Study G: Transfer of contaminants fromcap to fluid by bottle manipulating
..No. of % ContaminatedExpt Conditions bottles.oluidbtls Caps Fluid
G-la Hit on 59 56.9 47.5bench,open andclose,shake
G-2b Open and 18 61.1 72.2close,shake
Unmanipu- 18 77.8 5.6lated
a Bottles were derived from five different lots.b All bottles were from the same lot.
In experiment G-2, contamination was foundin 11 of the 18 examined caps, and in 13 of the18 fluids (Table 6). In six instances, the same
contaminants were found in caps and fluids(Table 7). One of these matched samplesyielded both E. cloacae and E. agglomerans.Fluids were contaminated, but caps were
sterile in four bottles. The remaining ninepositive fluids had caps that were contami-nated.The frequency of cap contamination in con-
trols (unmanipulated bottles) of experiment G-2(78%) did not differ significantly from thatobtained for caps from the manipulated bottlesin experiments G-1 and G-2. However, thefrequency of fluid contamination in the controlbottles (1 of 18) was statistically significantlyless than the manipulated test bottles (P =
0.00004 and P = 0.00008, respectively, byFisher's test).The frequency with which systems with con-
taminated caps had matching isolates fromfluid (Table 7) was significantly greater inmanipulated bottles of experiment G-1 and G-2than controls (P = 0.0038 and P = 0.014, re-
spectively, by Fisher's test). The likelihood offinding a fluid contaminated with organismsisolated from a contaminated cap was more
than seven times greater after manipulation ofthe cap and bottle than when systems were
sampled directly.Table 7 also gives the frequency with which
matching organisms were present in the cap forall positive fluid cultures. The number of obser-vations on controls (one match of one positivefluid) is insufficient to permit reliable compari-sons of these frequencies.These experiments clearly showed that ma-
nipulations of the cap and bottle simulatingthose commonly observed during normal hos-pital use significantly increased the rate offluid contamination with organisms present incontaminated caps.The presence of contaminated fluid in bottles
with sterile caps does not eliminate other cap
components as sources of the organisms influid. Only the elastomer liner was extractedand cultured, but other cap components and
TABLE 7. Study G: Transfer of contaminants from cap to fluid by bottle manipulating
Matching organisms in fluid All contaminated fluidsExpt Total contami-
nated caps No. of caps nated caps (%) Total Matching orga-natedcapsM ~~~nisms in cap (%)
thread areas may have been important sitesfrom which organisms could be transferred.
DISCUSSIONBacterial species similar to those associated
with epidemic cases were frequently isolatedfrom the manufacturing plant environment.These strains possessed characteristic biochemi-cal activities and had multiply-sensitive anti-microbial susceptibility patterns identical tothose isolated from cultures of stock infusionproducts, in-use i.v. fluid, and blood culturesfrom epidemic cases (3-5; Maki et al., Am.J. Med., in press). Early in the investigation,the in vitro susceptibility of these strains tomost tested antimicrobials suggested an extra-hospital, inanimate source of these organisms,unexposed to antibiotics or high concentrationof other gram-negative bacteria capable oftransferring episomal resistance.
Environmental specimens frequently yieldedorganisms of genera Klebsiella, Enterobacter,or Serratia (members of the tribe Klebsielleae).It is probable that the glucose-rich environ-ment of infusion product manufacturing plantsprovide members of this tribe with selectivegrowth advantages. We found that 50 of 51tested strains, all members of this tribe,proliferated luxuriously in commercial D5/Wat 25 C, attaining a mean concentration of morethan 105 organisms per ml in 24 h, whereas 48of 49 tested randomly selected bacterial strainsthat were not members of tribe Klebsielleaeeither remained static or died (13). In five ofthe six outbreaks of epidemic septicemia linkedto contaminated infusion fluid (3-9, 12, 14, 15;Maki et al., Am. J. Med., in press), membersof tribe Klebsielleae have predominated; thisis almost certainly related to the selectivegrowth properties of these organisms in glu-cose-containing fluids.
Large-scale microbiological studies of ware-house- and hospital-stored Abbott stock showedthat a high percentage of cap liners, particu-larly the newly introduced elastomer (about40%) were contaminated (Maki et al., Am. J.Med., in press). Cultures of unassembled capcomponents (study B) indicated that the mate-rials were not contaminated with the epidemicstrains prior to introduction on the productionline; contamination, specifically with the epi-demic organisms E. cloacae and E. agglo-merans, occurred after capping, both before andto a lesser extent after autoclaving (Table 2).The autoclave cycle (112 C, 22 min) appeared
to be adequate to destroy frequent preauto-clave contamination, and the finding of no con-tamination immediately after autoclaving sug-
gests that contamination of autoclave coolantor survival of organisms present from preauto-clave stages of production did not play a majorrole in post-sterilization contamination at thetime of our study. Most importantly, study Bshowed that contaminants were readily intro-duced at multiple stages of postautoclave pro-cessing; very frequent contamination (9 of 12samples of warehouse stock) suggested thecumulative nature of manufacturing contami-nation. The number of production-line samplesobtained in study B was insufficient to permitvalid statistical evaluation of the relative riskof contamination of each postautoclave produc-tion stage.
It could be assumed that some micro-organisms, if present in autoclave coolingwater, could be introduced into closures, sincestudy B demonstrated conclusively that auto-clave coolant infiltrated all aspects of the innercap assembly. Gilsonite-lined closures wereconsiderably less frequently contaminated thanelastomer-lined ones in surveys of hospital andof warehouse stock (40% versus 8% ([Maki etal., Am. J. Med., in press]) and in study Ecomparing fresh, simultaneously manufac-tured products. Most interestingly, althoughthe epidemic strains were frequently isolatedfrom elastomer-lined closures, Gilsonite-linedclosures did not yield these organisms. In vitrostudies revealed a diffusible antibacterial sub-stance in the red rubber liner of the Gilsoniteclosure which exhibited substantial activityagainst most tested bacteria, including theepidemic strains (study F). Findings of thisstudy may explain the far-reaching conse-quences of Abbott's seemingly innocuousswitch from the use of Gilsonite to elastomer inits bottle closures in March 1970 and theapparent absence of clinical problems with theGilsonite screw-cap closure for over 35 years.The absence of contamination of presterilized
controls (study B) which were inserted into theproduction line at room temperature, ratherthan the usual 40 C, and study D using fluo-rescein dye strongly suggested the impor-tance of a falling cap temperature in promotingingress of environmental contaminants intothe closure. A cooling closure actively drewambient moisture, with any contained micro-organisms, through the thread interstices andup into the innermost parts of the cap. Thisapparently was not the sole mechanism of capcontamination, however, because control bot-tles at ambient temperature in study Balso manifested contamination although in agreatly reduced frequency (Table 2). Thisphenomenon presumably explains why the
VOL. 2, 1975
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
496 MACKEL ET AL.
closures of test bottles at room temperaturefailed to become contaminated after insertionat various stages of production despite heavycontamination of bottles which were taken con-currently from the production line and whichwere falling in temperature.The frequency of contamination of both Gil-
sonite and elastomer closures and fluids fromproduction line stock was extremely high inthese plant studies, much higher than culturestudies of warehouse or hospital stock (Makiet al., Am. J. Med., in press), possibly re-flecting the freshness of samples. Visible mois-ture was present throughout the closuresof these freshly manufactured bottles, and itis possible, but unproven, that storage condi-tions lead to drying, which secondarily leadsto a substantial reduction in the frequencyof detectable contamination, especially withgram-negative bacilli.The chemical constituents of red rubber are
numerous and highly complex. Information onthe composition of the red rubber and theelastomer liners could not be obtained from themanufacturers. Natural rubber contains about95% hydrocarbon, 3% protein, 2% resins andfatty acids, and very little mineral matter.During vulcanization and molding, variousminerals and chemicals are added, includingsulfur, zinc-dimethyldithiocarbonate, and zincoxide. Depending on the desired final product,other chemicals may also be used, e.g., aro-matic chlorinated hydrocarbons, ketones, zincchloride, mevalonic acid, and isopentenyl pyro-phosphate (2). Investigators in Australia iden-tified various chemicals in infusion fluids, suchas zinc oxide, traceable to the rubber closures.Unidentified chemicals were believed to beaccelerators and "chemicals comprising thesecret formulary of the rubber manufacturer"(11). Many of these compounds are known tohave antiseptic, astringent, and fungicidalproperties (2, 16).
Migration of bacterial contamination fromcaps to fluid was easily accomplished, in vitro,by simple manipulations simulating normal in-hospital use (study G). These procedures pro-duced fluid contamination in more than 50% ofbottles with contaminated caps. Although fluidwithin unopened bottles may have rarely beencontaminated, causing almost immediate sepsisat the inception of i.v. therapy (Maki et al.,Am. J. Med., in press), most septicemiasprobably arose from the transfer of microorga-nisms present in the closure to fluid duringtherapy, effected by routine and expected ma-nipulations of the type simulated experi-mentally.
U.S.P. microbiological quality-control re-quirements followed by the company wouldpermit 99.3% of autoclave loads with an in-trinsic contamination frequency of 6/1,000, theactual value in samples of Abbott products, tobe released for consumer use (Maki et al., Am.J. Med., in press). In addition, U.S.P. didnot require the history of previous quality con-trol positives to be taken into account in judg-ing the likely sterility of subsequent autoclaveloads. The substantial increase in autoclaveloads failing both initial sterility test and re-test in 1970 involved both elastomer- andGilsonite-capped products. Since bottles selectedfor quality control were sampled immediatelyafter autoclaving, the most likely source of or-ganisms in these bottles was autoclave coolingwater. Contamination of the products with theepidemic strains and other organisms was ob-served to occur at postautoclave stage of pro-duction; thus, contaminated autoclave coolingwater, if involved, was not the only source ofthe contamination. Since organisms in positivequality control specimens were not identified,the contribution of autoclave cooling water mustnecessarily remain speculative. Sequential sam-pling schemes requiring the cumulative num-ber of positive samples to be plotted against thetotal number of samples is capable of detectingdepartures from expected experience. Theformal adoption of such sampling plans shouldbe seriously considered by industry and regula-tory agencies. Sequential sampling will detectongoing production problems resulting in sys-tematic, low-level contamination of products.Quality control sampling is not a practical wayto reliably detect low-frequency contaminationof individual autoclave loads; biological indica-tors to monitor autoclave function and adher-ence to good manufacturing practices are addi-tional ways of assuring that infusion productsare microbiologically safe.Our findings show that, in addition to se-
quential sampling, other improvements inquality control are needed. (i) Finished pro-ducts should be selected for sampling fromnewly produced stock when they reach thewarehouse, rather than immediately afterautoclaving. (ii) The total volume of fluid withinbottles should be sampled, rather than frac-tions. (iii) The direct addition of concentratedbroth to the container appears to be a simplerand more sensitive culture technique thanmembrane filtration. (iv) Culture medium suchas enriched brain heart infusion broth is pre-ferred to thioglycolate media. (v) Gram-negativeisolates from positive quality-control specimensshould be identified through genus and species;
J. CLIN. MICROBIOL.
Dow
nloa
ded
from
http
s://j
ourn
als.
asm
.org
/jour
nal/j
cm o
n 06
Feb
ruar
y 20
22 b
y 19
1.53
.237
.52.
SEPTICEMIA FROM CONTAMINATED I.V. PRODUCTS 497
other isolates should be identified throughgenus.The identification of gram-negative isolates
in positive quality-control samples serves bothscientific and public health objectives. Knowingthe identity of such organisms helps the assess-ment of potential clinical seriousness of con-tamination, permits correlation to be made be-tween product and i.v.-associated human casesif they occur, and provides the manufacturerwith information of great value in detectingimportant inplant sources of contamination.Further characterization of such isolates byantibiotic susceptibility and application ofother typing systems would enhance the objec-tives.These studies raise the question of whether
a screw-cap closure in its conventional form canbe made totally safe from contamination. Atpresent this type of closure cannot be recom-mended for use with infusion products or othermedications that must remain sterile.
Within individual hospitals the outbreakswere terminated by discontinuing use of infu-sion products from Abbott Laboratories andnationwide by total product recall (3-5; Maki etal., Am. J. Med., in press). These epidemio-logical and laboratory investigations werebrought to a successful conclusion because eachdiscipline complemented the other. Hypothesesgenerated by epidemiological observation weresubjected to microbiological testing. The resultsof such tests led to new epidemiological hy-potheses and studies that ultimately providedclear insight into the genesis of a complex prob-lem.
LITERATURE CITED1. Bauer, A. W., W. M. M. Kirby, J. C. Sherris, and
M. Turk. 1966. Antibiotic susceptibility testing by astandardized single disc method. Am. J. Clin. Pathol.45:493-496.
2. Bourne, H. C., Y. T. Yee, and S. Seferian. 1968. The
toxicity of rubber additives. Arch. Environ. Health16:700-705.
3. Center for Disease Control. 1971. Nosocomial bactere-mias associated with intravenous fluid therapy-U.S.A. Morbid. Mortal. Weekly Rep. 20(suppl. 9).
4. Center for Disease Control. 1971. Follow-up on septi-cemias associated with contaminated Abbott intra-venous soluition- United States. Morbid. Mortal.Weekly Rep. 20:91-92.
5. Center for Disease Control. 1971. Follow-up on septi-cemia associated with contaminated Abbott intra-venous fluid from Abbott Laboratories. Morbid.Mortal. Weekly Rep. 10:110.
6. Center for Disease Control. 1973. Septicemias associ-ated with contaminated intravenous fluids. Morbid.Mortal. Weekly Rep. 22:99.
7. Center for Disease Control. 1973. Follow-up on septi-cemias associated with contaminated intravenousfluids. Morbid. Mortal. Weekly Rep. 22:115.
8. Center for Disease Control. 1973. Follow-up on septi-cemias associated with contaminated intravenousfluids. Morbid. Mortal. Weekly Rep. 22:124.
9. Duma, R. J., J. F. Warner, and H. P. Dalton. 1971.Septicemia from intravenous infusions. N. Engl. J.Med. 284:257-260.
10. Ewing, W. H., and M. A. Fife. 1971. Enterobacteragglomerans, the herbicola-lathyri bacteria. Centerfor Disease Control, Atlanta, Ga.
11. Garvon, J. M., and B. W. Gunner. 1964. The harmfuleffects of particles in intravenous fluids. Med. J.Aust. 2:1-6.
12. Her Majesty's Stationery Office. 1972. Report of thecommittee appointed to inquire into the circum-stances, including the production, which led to theuse of contaminated infusion fluids in the Deven-port Section of Plymouth General Hospital, London.
13. Maki, D. G., and W. T. Martin. 1975. Nationwideepidemic of septicemia caused by contaminated in-fusion products. IV. Growth of microbial pathogensin fluids for intravenous infusion. J. Infect. Dis.131:267-272.
14. Phillips, I., S. Eykyn, and M. Laker. 1972. Outbreakof hospital infection caused by contaminated auto-claved fluids. Lancet 1:1258-1260.
15. Sack, R. A. 1970. Epidemic of gram-negative organismsepticemia subsequent to elective operation. Am. J.Obstet. Gynecol. 107:394-399.
16. Stecher, Paul G. (ed.). 1968. Merck index, 8th ed.Merck & Co., Inc., Rahway, N.J.
17. The United States Pharmacopeia XVIII. 1970. p. 851-856. Mack Publishing Co., Easton, Pa.