44
NATIVE AMERICAN SCHOOLS HEALTH & WELFARE TRUST
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | pranav-pettijohn |
| View: | 217 times |
| Download: | 0 times |

NATIVE AMERICAN SCHOOLS HEALTH & WELFARE
TRUST

SELF FUNDING OVERVIEWELIGIBILITYENROLLMENT EFFECTIVE DATE TERMINIATIONBILLING ADJUSTMENTSAPPROVED LEAVE

How does How does Self-Funding Work?Self-Funding Work?
ContributionsContributions AdministrationAdministration
Claim
sC
laims
EmployerEmployer’’s s General AssetsGeneral Assets
Employee Benefit PlanEmployee Benefit Plan
Fixed CostsFixed Costs
Actual ClaimsActual Claims
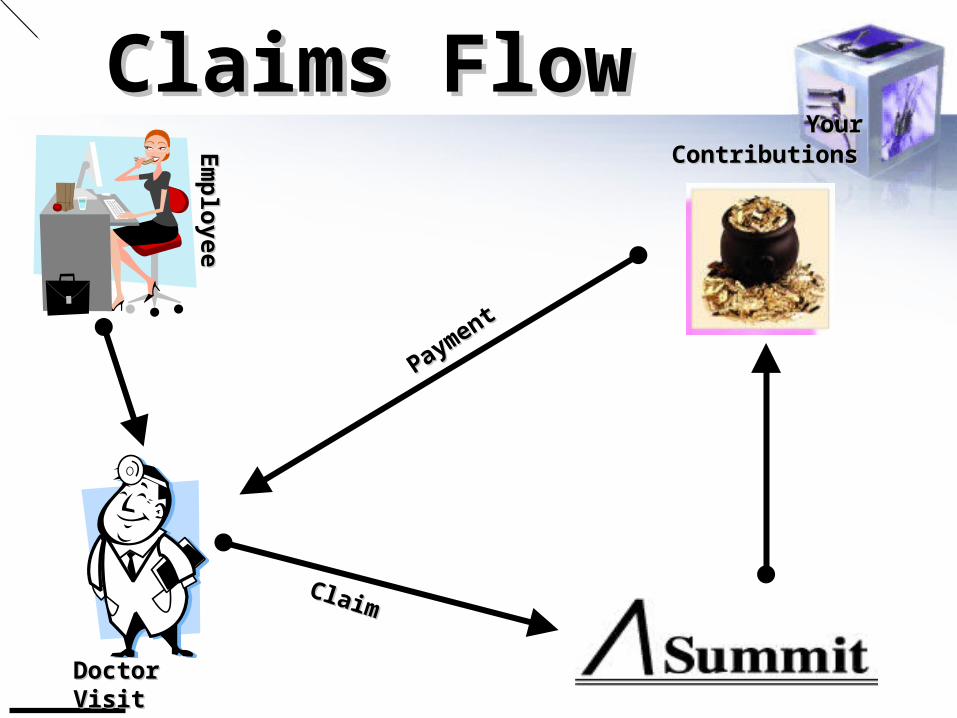
Claims FlowClaims Flow
Em
plo
yeeE
mp
loyee
Doctor VisitDoctor Visit
Payment
Payment
ClaimClaim
Your Your ContributionsContributions

Native American Schools Health Plan©
/\Summit

Stop Loss Specific Deductible
Member 1 Member 2 Member 3 Member 4 Member 5 Member 6
12 Month Policy Year
SpecificReimbursements
Member Claims
SpecificSpecific DeductibleDeductible

/\Summit
Eligibility Criteria - Employee
Generally employees must work 20 hours or more per workweek.
Understand that this does not apply to summer or scheduled breaks during school.

/\Summit
Eligibility Criteria – DependentSpouse
1. Legal Spouse (State Law)
2. Common Law Spouse provided it meets legal requirements of Navajo Nation.

/\Summit
Eligibility Criteria – DependentChild
1. Employee’s child to age 26:
a. Natural child,
b. Step child,
c. Legally adopted child,
d. Foster Child,
e. Guardian:
a) Not Power of Attorney
b) Legal guardianship through courts
- Emancipation at age 18
- To age 26, court document
must decree
2 Qualified Medical Child Support Order (QMCSO)
3. Disabled child over age 26—must provide proof every 2 years.

Eligibility Criteria – DependentChild
PRIOR TO PPACA, PLAN REQUIREMENTS FOR DEPENDENT CHILD
a) Lives with the employee
b) Unmarried;
c) To age 19;
d) If Full-time student, then to age 24
NO LONGER IN EFFECT
/\Summit

/\Summit
Eligibility Criteria – Dependent
Dependent child does NOT include:
1. grandchildren
2. niece or nephew
Unless legal guardian

/\Summit
Enrollment Timeline Employee—
a. New employee: within 31 days
b. annual “Open Enrollment”
Dependent—
a. at the time of employee enrollment, or
b. within 31 days of dependent acquisition
c. annual “Open Enrollment”
APPLIES UNTIL NEXT OPEN ENROLLMENT

/\Summit
Open Enrollment– Employee not previously enrolled to enroll
for coverage
– Dependents not previously enrolled to enroll for coverage
– Enrolled dependents to be dropped from coverage
– Enrollment elections apply until next open enrollment

/\Summit
HIPAA Special Enrollment
HIPAA Special Enrollment Period.
i. Other coverage
ii. Dependent acquisition
iii.Enroll within 31 days of the event
iv. CHIPS—60 day enrollment

/\Summit
Special EnrollmentHIPAA Special Enrollment Period –
- Other Coverage
i. Termination of the other coverage, including COBRA.
ii. Cessation of employer contributions toward the other coverage.
iii. Legal separation or divorce.
iv. Termination of other employment or reduction in hours.
v. Death of the covered person.
Enroll within 31 days of the event

/\Summit
Special EnrollmentHIPAA Special Enrollment Period
- Dependent Acquisition
i. Marriage
ii. Birth of a dependent child.
iii. Adoption of a child
Enroll within 31 days of the event

SPECIAL ENROLLMENTHIPAA Special Enrollment Period
• CHIP– Termination of Medicaid or CHIP Coverage
– Eligibility For Premium Assistance Under Medicaid or CHIP
– Enroll within 60 days
/\Summit

/\Summit
Enrollment Form to Summit• Options:
– Fax: 480.505.0406– Email: [email protected]– On-line enrollment: www.summit-inc.net– Snail Mail: P. O. Box 25160, Scottsdale, AZ
85255
• Retain enrollment form in Personnel file– Compare to next billing ensuring employee
is enrolled in the Plan
• Issue ID card to employee

Life Insurance Enrollment
• Life Insurance Enrollment is done on-line with Lincoln National
• Summit DOES NOT do Life Insurance enrollments
/\Summit

/\Summit
Effective Date of Coverage
• Employee—1st of month following date of hire.
• Dependents, provided enrolled timely:– Date employee coverage is effective– Date dependent is acquired– Date adopted child is “placed for adoption”– Newborn
• Employee has family coverage = birth• Employee has single coverage = birth, provided
enrollment form is submitted within 31 days of birth

/\Summit
Termination of Coverage
Employee:
The last day of the month in which the employee CEASES TO MEET THE ELIGIBILITY CRITERIA.
Note: this does not necessarily mean the employee terminates EMPLOYMENT.

/\Summit
Certified & Contracted Employees:
Termination of Coverage
Certified or contracted employeeCertified or contracted employee
Signed the contract for next school year Signed the contract for next school year
SchoolSchool’’s Health Plan provides coverage s Health Plan provides coverage through the summer months. through the summer months.
The school continues to pay for employee The school continues to pay for employee coverage.coverage.

Termination of CoverageCertified & Contracted Employees
/\Summit
DonDon’’t terminate teachers that are returning t terminate teachers that are returning next school year! next school year!
Keep them on the Health Plan. Keep them on the Health Plan.
Contributions for dependentContributions for dependent’’s coverage s coverage through the summer needs to be addressed through the summer needs to be addressed through payroll.through payroll.

/\Summit
Termination of Coverage Dependents:
- The date an employee’s coverage terminates.
- The date the person ceases to meet the eligibility criteria.1. Spouse: Divorce or legal separation.2. Child: Reaches the maximum age limit.

/\Summit
Termination Notice to Summit
• Options:– Pull original enrollment form & note bottom
with termination information• Date of termination• Reason for termination (necessary for COBRA)
– On-line access: www.summit-inc.net– Notation on corrected census noting
termination date

/\Summit
Termination Notice to Summit
Under Federal law, COBRA:
• Employer: 30 days to notify Summit– Notify Summit if due to “Gross Misconduct”
• Summit: 14 days to provide COBRA election
• Failure to provide timely notice:– could result in litigation and/or penalties– potential claims payments

/\Summit
BILLING ADJUSTMENTSNew Enrollment/Billing
• If new employee is not on the billing:– Refax enrollment with notation “2nd
submission”
– Be aware of the “window”• Date of billing census vs. date enrollment sent
– Adjust the count on the bill to include employee

/\Summit
BILLING ADJUSTMENTS Termination Notice/Billing
Compare the termination notice(s) sent to Summit to next billing
If term’d employee is still on the bill:– Be aware of the “window”– Make the # count adjustment on the bill– Provide documentation to Summit for the
adjustment with the check.– Resubmit term notice with “2nd submission

/\Summit
BILLING ADJUSTMENTS Dependent Enrollment Audit
October billing/census will include all dependents covered by the employee
Verify against your records
Coordinate with Summit for corrections

/\Summit
Leave of Absence Provisions
Conditions that allow continued coverage under the Plan after loss of eligibility:
a. Administrative Leave
b. Family Medical Leave Act (FMLA)
c. Leave of Absence (LOA)

/\Summit
Administrative Leave
• Coverage continued for enrolled employee and enrolled dependents
• School pays applicable contributions
• Coverage continues until investigation is closed
• If administrative action is suspension, coverage for 30 days of suspension.

/\Summit
Leave of Absence (FMLA)
Employee must have worked for 1,250 hours in the preceding 12 months to be eligible for Leave of Absence under FMLA.
Employee must request leave under FMLA.

/\Summit
Reason for leave must comply with FMLA criteria.
i. “Serious health condition”
ii. For self
iii. For immediate family members
Leave of Absence (FMLA)

/\Summit
Employee remains covered under the health plan while on FMLA.
Employer pays the employee’s health plan contribution while employee is on FMLA leave.
Leave of Absence (FMLA)
Employee is granted leave of absence

/\Summit
Leave of Absence (FMLA)
Serious Health Condition = 12 weeks
Military Caregiver Leave = 26 weeks
Qualifying Exigency = 12 work weeks
Leave of Absence (FMLA)
/\Summit
Employee returns to work or is terminated from the Plan.
Last day of FMLA is qualifying event for COBRA.

/\Summit
Leave of Absence, Regular
When employee does not qualify for FMLAMay be granted or denied LOAGenerally, employee pays the cost of health plan coverage
After 90 days of leave, the employee returns to work or is terminated from the Plan.
/\Summit
The 90 days coverage under the Plan while on Regular Leave of Absence, applies to the maximum allowable coverage duration under COBRA.
Leave of Absence, Regular
If an employee is terminated from the Plan,
COBRA is offered.

/\Summit
Employee was on leave for 90 days (3 months).
Employee elects COBRA.
Due to termination of employment, COBRA is offered for 18 months.
Three months have already been used, leaving 15 months of COBRA continuation of coverage.
Leave of Absence, Regular
ExampleExample

/\Summit
Coordinating Paid Time Off with FMLA or Regular Leave
Each employer establishes the guidelines.
Variables include:
Requirement for employees to use up all available Paid Time Off before going on either FMLA or LOA
Allow an employee to use PTO concurrently with FMLA/LOA

Claims FlowClaims Flow
Em
plo
yeeE
mp
loyee
Doctor VisitDoctor Visit
Payment
Payment
ClaimClaim
Your Your ContributionsContributions

Native American Schools Health Plan©
/\Summit

Stop Loss Specific Deductible
Member 1 Member 2 Member 3 Member 4 Member 5 Member 6
12 Month Policy Year
SpecificReimbursements
Member Claims
SpecificSpecific DeductibleDeductible

SELF FUNDING OVERVIEWELIGIBILITYENROLLMENT EFFECTIVE DATE TERMINIATIONBILLING ADJUSTMENTSAPPROVED LEAVE

















