NCC Pediatrics Continuity Clinic Curriculum: Medical Professionalism Faculty Guide
Goals & Objectives:
1. Develop categories and identify elements of professional behavior in medicine.
2. Provide an explanation to the statement that “professionalism is a set of skills thatdevelops over the course of time in medical practice.”
Pre-Meeting Preparation:
• Skim the AAP technical report "Professionalism in Pediatrics" (2007)
• Review some physician disciplinary actions to review. Click on the link: VA, DC,CA (start at page 35), WV
• Form categories of the types of unprofessional behavior cited.
• Prepare to discuss an incident in which you were challenged with a decision thatinvolved professionalism in the care of patients.
Conference Agenda:
• Have the most junior participant write their categories of professional behavior onthe white-board. Using the real-life examples of citations, expand or modify thecategories.
• Have each participant discuss a situation in which their professionalism waschallenged.
Extra-Credit: • Teaching and Assessing Professionalism (APPD, 2008)
• Professionalism in Pediatrics, our square pegs, their round holes (AAP News, Oct 2011)
• Opting in to Online Professionalism: Social Media and Pediatrics (Pediatrics, Oct 2013)
• Tattoos, Beer, and Bow Ties The Limits of Professionalism in Medicine (JAMA Peds, June 2016)
Professionalism in PediatricsMary E. Fallat, MD, Jacqueline Glover, PhD, and the Committee on Bioethics
ABSTRACTThe purpose of this report is to provide a concrete overview of the ideal standardsof behavior and professional practice to which pediatricians should aspire and bywhich students and residents can be evaluated. Recognizing that the ideal is notalways achievable in the practical sense, this document details the key componentsof professionalism in pediatric practice with an emphasis on core professionalvalues for which pediatricians should strive and that will serve as a moral compassneeded to provide quality care for children and their families.
INTRODUCTIONProfessionalism has been a central and defining feature in medicine since Hip-pocrates.1 The concept of professionalism is now receiving renewed attentionbecause of advances in technology, managed care and other business arrange-ments in health care, and a growing sense of the erosion of public trust in themedical profession.2
Pediatricians have a special status in society as privileged and trusted advocatesfor the well-being of children. Pediatricians have a responsibility to use theirknowledge, skills, and influence to advocate for children and their interests in alldomains of society, not just in health care. A child’s health is broadly understoodto include emotional, social, educational, psychological, and spiritual well-being.
As the pediatrician-child/family relationship has been threatened over timewith the imposition of a business model, it has become more important than everto adopt a standard of professionalism for pediatricians. The ability to promoteprofessionalism across the continuum of medical education, from medical schoolcurricula through continuing medical education for practicing pediatricians, de-pends on the ability to define and assess professionalism in the context of pediat-rics.3,4 Various professional groups have supported the need for a normativedefinition of professionalism, and there is considerable overlap in the definitionsthat they have formulated.5–8 The American College of Physicians astutely noted inits recent iteration of their ethics manual that written guidelines are not a substi-tute for the experience and integrity of individual physicians but may serve as areminder of the shared duties and obligations of the medical profession.9 Allowingthat the ideal may not be fully achievable in the practical sense, the purpose of thisdocument is to provide a background on professionalism in pediatrics that servesa dual role: (1) to provide a concrete overview of the ideals for which pediatriciansshould strive and (2) to describe standards of professional behavior by whichpracticing pediatricians and trainees can be evaluated. This document begins witha general discussion of statements concerning professionalism in pediatrics andproceeds to the application of these statements in the central relationships in
www.pediatrics.org/cgi/doi/10.1542/peds.2007-2230
doi:10.1542/peds.2007-2230
All technical reports from the AmericanAcademy of Pediatrics automatically expire5 years after publication unless reaffirmed,revised, or retired at or before that time.
The guidance in this report does notindicate an exclusive course of treatmentor serve as a standard of medical care.Variations, taking into account individualcircumstances, may be appropriate.
KeyWordsprofessionalism, pediatricians, physician-patient relations, medical student, resident
AbbreviationsABP—American Board of PediatricsAAP—American Academy of PediatricsAMA—American Medical AssociationHIPAA—Health Insurance Portability andAccountability Act
PEDIATRICS Volume 120, Number 4, October 2007 e1123 by guest on April 9, 2020www.aappublications.org/newsDownloaded from
pediatric practice—to patients and families, to studentsand residents, to other health professionals, to the pro-fession, and to society in general.
STATEMENTS OF PROFESSIONALISM IN PEDIATRICSThe American Board of Pediatrics (ABP) began its dis-cussion of professionalism when it defined the optimalattitudes, knowledge, clinical judgment, technical skills,and interpersonal skills that applicants should possess inits 1974 publication Foundations for Evaluating the Compe-tency of Pediatricians.10 Since 1976, residency programdirectors have been asked to evaluate interpersonalskills, work habits, and personal qualities of residents,and beginning in 1982, the ABP requested that programdirectors also evaluate and attest to applicants’ ethicaland moral behavior as it affects their professional per-formance.
The ABP continued its pediatric-specific efforts toclarify ethics and professionalism issues in practice withthe pioneering 1987 publication “Teaching and Evalua-tion of Interpersonal Skills and Ethical Decision Makingin Pediatrics.”11 Admittedly, the content area in ethics isnot straightforward. To assist residents and pediatriciansin practice with difficult ethical decisions, the AmericanAcademy of Pediatrics (AAP) Committee on Bioethicshas been publishing guidelines on key ethical issuessince 1983 (available at http://aappolicy.aappublications.org). Most recently, the ABP added more specific guide-lines for the teaching and evaluation of professionalismas part of the core curriculum for residency training inpediatrics. The following 8 components of professional-ism have been endorsed by the ABP as the most appro-priate for teaching and evaluation12:
● Honesty and integrity—embody the principles of fair-ness, the ability to meet commitments and keep one’sword, and the duty to be intellectually honest andstraightforward in interactions with patients and peersand in all professional communication.
● Reliability and responsibility—represent accountabil-ity to children, families, other physicians, medicalstaff, community, and ultimately society. They requireacceptance of responsibility for errors made, includingthe willingness to acknowledge and discuss errors,consequences, and alternatives with the family andwith peers.
● Respect for others—involves treating all persons withrespect and regard for individual worth and dignity,including sensitivity to gender, race, and cultural dif-ferences as well as maintenance of patient confidenti-ality when appropriate.
● Compassion/empathy—the ability to understand chil-dren’s and family members’ reactions to pain, discom-fort, and anxiety from their point of view, not that ofthe physician.
● Self-improvement—involves a commitment to life-long learning and education.
● Self-awareness/knowledge of limits—the maturity torecognize when a problem involves knowledge ortechnical skills beyond the experience of the providerand to ask for consultation or assistance in those sit-uations.
● Communication and collaboration—involve the rec-ognition that patients’ families and the health careteam must work cooperatively with each other andcommunicate effectively to provide the best patientcare and social activism.
● Altruism and advocacy—refer to the unselfish regardor devotion to the welfare of others. Patient well-being should be the primary motivating factor in pa-tient care, ahead of physicians’ own interests andneeds.
PEDIATRICIANS’ RESPONSIBILITIES TO PATIENTS, FAMILIES,AND COMMUNITIESThe connotation of “good doctor” historically brings tomind a physician who embodies both the art and scienceof medicine. The concept is epitomized in the pediatri-cian who can give advice without being patronizing,who is concerned about how an illness and its conse-quences (financial, emotional, psychological) will affectthe family, and who strives to help the child and/orparent understand a disease process and its natural his-tory (compassion/empathy). This doctor is thorough andtechnically skillful and continually incorporates newknowledge into his or her practice (self-improvement).13
To other physicians, a “good pediatrician” is a colleaguewith whom they would entrust the care of their ownchild.14
To be effective, the relationship between a pediatri-cian, his or her patient, other medical professionals, andthe parent or surrogate (hereafter, “parent”) of that childmust be collaborative. The role of the parents is to takean interest in and responsibility for their child’s healthcare, seek attention for medical problems in a timelymanner, and communicate and work effectively withtheir child’s pediatrician to create an acceptable treat-ment plan. In return, the pediatrician’s obligation is toprovide appropriate information regarding the child’shealth care, including the benefits, risks, and costs of allreasonable treatment alternatives (communication andcollaboration). Parents should have their questions an-swered, feel free to seek second opinions, and be advisedof the pediatrician’s potential conflicts of interest (hon-esty and integrity). Pediatricians should communicate toparents any errors in patient care, including any conse-quences that have resulted or may result because of theerror (honesty and integrity; reliability and responsibil-ity).
Children, as patients, should be afforded continuous
e1124 AMERICAN ACADEMY OF PEDIATRICS by guest on April 9, 2020www.aappublications.org/newsDownloaded from
access to care. On-call pediatricians should be responsivein a timely manner, coverage should be available duringabsences, and notice of closing a practice or changingparticipation in insurance plans is expected (curtailingaccess). Except in cases of emergency or in which statelaw allows otherwise, the permission of a parent will benecessary before a pediatrician can offer medical treat-ment to a child. Parents may accept or refuse a recom-mended medical treatment on behalf of their child. Pe-diatricians and pediatric medical subspecialists have aduty to respect the wishes of the child and family whenthese wishes are intended to do good (beneficence) andavoid harm (nonmaleficence). A child’s parent usually isthe most appropriate person to determine what actionswill be in the best interest of the child (communicationand collaboration; altruism and advocacy). Children andadolescents who desire to participate should be includedin the decision-making process (patient assent) whentheir neurologic status, development, and level of ma-turity allow, although state laws that affect the minor’sability to consent to (provide legally binding authoriza-tion for) medical care are complex.15
Resolving Conflicting Goals of CareConflicts may occur when the parent, child, and physi-cian fail to agree on what would be optimal care undera given set of circumstances. When pediatricians andparents disagree, the pediatrician should explain the ba-sis for the disagreement, educate the parent, and attemptto meet the child’s needs within the constraints thatexist. In these cases, the physician must seek to under-stand the reason for the disagreement and determine ifthe child would be put at significant risk of serious harmby following the wishes of the child and/or parent. Incases in which serious harm to a child is likely if theparent’s wishes are followed, the pediatrician must get asecond opinion and act to protect the best interests of thechild. Institutional ethics committees should be con-sulted for guidance, education, and advice regardingunusual or complicated ethical problems that involvethe care and treatment of children.16
If a physician or other health care professional isunwilling to honor a family’s refusal of intervention in asituation in which the family has chosen an establishedalternative, he or she should withdraw from the caseand must provide reasonable assistance to the parent inmaking alternative arrangements for care. A physicianmay not discontinue care of a child as long as additionaltreatment is medically indicated or until another physi-cian has assumed care.
Nondiscrimination, Societal Obligations, and Continuity ofCareThe AAP believes that the medical care of infants, chil-dren, and adolescents should be delivered or directed bywell-trained pediatricians who provide primary care and
help to manage and facilitate essentially all aspects ofpediatric care.17 A pediatrician has broad authority toenter into or decline a medical relationship with a familyexcept in emergency situations. Once a relationship isestablished, however, the pediatrician should assumeresponsibility for the medical care of the child and alsorecognize when the child needs to be referred to a pe-diatric medical subspecialist, pediatric surgical specialist,or other physician or qualified clinician for diagnosis ortreatment of a condition or symptom complex outside ofthe physician’s scope of practice (self-awareness/knowl-edge of limits).18
Pediatricians or pediatric subspecialists who offertheir services to the public should not refuse to acceptchildren into their practice because of race, color, reli-gion, national origin, disability, sexual orientation, orany other basis that would constitute discrimination (re-spect for others). Pediatricians should not refuse to carefor acutely ill children on the basis of the ability of thefamily to pay for services rendered. However, practiceoverhead expenses preclude the provision of compre-hensive health services for every child whose familyrequests routine or preventive health services unlessthere is some means of compensation. The AAP believesthat the medical care of infants, children, and adoles-cents should be accessible, continuous, comprehensive,family centered, coordinated, compassionate, culturallyeffective, and provided according to the medical homeconcept.17 Pediatricians have a special obligation to worktogether to help secure access to health care for allchildren, including those who are uninsured or under-insured.19
Pediatricians have an obligation to refrain from pro-viding nonbeneficial interventions and should also begood stewards of health care resources by using the mostefficient means to diagnose a condition, using resourcesof optimal quality wisely, and helping to ensure thatresources are available equitably.5 A pediatrician maynot refuse to treat a child whose condition is within thephysician’s current realm of competence solely becausethe child has a communicable disease. A pediatricianshould honor requests for second opinions and shouldbe available to provide guidance to the parents and childafter they have obtained opinions from other physicians.Pediatricians and subspecialists to whom they refer theirpatients should make every effort to communicate effec-tively and in a timely manner with each other abouttheir assessments of the patient and coordinate theirtreatment plans (reliability and responsibility).
Boundaries in Patient CareCompassionate and empathetic care for the child histor-ically has been balanced with the need to remain objec-tive and avoid becoming overinvolved. Boundary viola-tions can pose a serious threat to professionaljudgment.20 An increase in trust and change in bound-
PEDIATRICS Volume 120, Number 4, October 2007 e1125 by guest on April 9, 2020www.aappublications.org/newsDownloaded from
aries is likely to occur as a child/family-pediatrician re-lationship evolves. Boundary transgressions might in-clude abusive behaviors, sexual behavior between thephysician and the patient or members of the patient’sfamily, a physician who treats family members, andgift-giving between a family and the physician.21–23 Thedevelopment of strong empathetic and nonromantic,nonsexual feelings of affection for a patient or family donot constitute boundary violations and are deeply val-ued by patients and families, and it provides an oppor-tunity for personal growth for the pediatrician.
The pediatrician may wish to continue providing carefor a patient who is an adolescent or a young adult (eg,during high school and college matriculation or for olderchildren with special health care needs) to minimizefragmentation of care. The pediatrician, the family, andthe patient should discuss whether, for any reason, thepatient might instead wish to change physicians. Maturepatients should be encouraged to take increasing respon-sibility for their personal health care by communicatingdirectly with the pediatrician and making their ownappointments while informing parents of these appoint-ments. As the new patient-physician relationshipevolves, it may be appropriate to develop an optionunder which the adolescent can obtain confidential careif needed.24,25
One of the most common and difficult boundary is-sues occurs when a pediatrician treats his or her ownfamily members. Because the close relationship carries apotential for the pediatrician to lose objectivity or fail toexplore sensitive issues and areas with the patient, fam-ily members should be encouraged to seek another pe-diatrician. Exceptions include underserved areas inwhich there may be only 1 pediatrician, which wouldmake this impractical, or in the case of an emergency.Regarding nonurgent care rendered to minor patients,the American Medical Association (AMA) has stated, “Inparticular, minor children will generally not feel free torefuse care from their parents.”19 This same concern maycarry over to medical care that is provided to minors byother relatives.
Occasionally, a pediatrician may receive a gift from apatient or the parents of a patient. Small gifts given ingratitude may sometimes be accepted if they do notaffect professional clinical judgment. Repeated attemptsat gift-giving or the offer of expensive gifts may repre-sent an attempt by the family to consciously or uncon-sciously control the patient-physician interaction. Largeror more expensive gifts are clear and serious boundarytransgressions unless they are given as a charitable do-nation to a nonprofit institution.26 There is also a poten-tial conflict of interest when patients who make largecontributions to medical institutions receive preferentialtreatment (eg, they are seen immediately, moved to thetop of the operating room schedule, etc).
Privacy and Access to Health InformationRespecting the privacy of patients and their families,including protecting the confidentiality of patient infor-mation, is a central feature of professionalism in pediat-ric practice. The importance of privacy has been under-scored by federal regulation, known as the Privacy Rule,issued pursuant to the Health Insurance Portability andAccountability Act (HIPAA).27,28 HIPAA was intended tocreate national standards to protect individual personalhealth information and give patients or their surrogatesincreased access to their medical charts.
Under the HIPAA Privacy Rule, parents have newrights to control and have access to the health informa-tion about their minor children, with limited exceptions.When a minor has the right to consent to care or aparent has agreed that the minor may receive confiden-tial care, the minor may exercise his or her own rights toaccess and control protected health information. How-ever, state or other applicable law governs if it has ex-plicitly addressed disclosure of a minor’s health informa-tion or medical charts to a parent. If state or other lawdoes not define the parent’s ability to access the child’shealth information, a licensed health care professional isallowed to exercise discretion to grant or deny suchaccess.
The HIPAA Privacy Rule also dictates the need forprivacy regarding patient identification that extends toinpatient rounds, patient charts, and telephone and ca-sual conversations that formerly might have been con-ducted in public places such as elevators and hall corri-dors. Teaching conferences, computerized presentations,and radiographic exhibits all must avoid the use of pa-tient identifiers and preferentially take place in areaswhere strict confidentiality can be preserved. Physiciansare expected to take a leadership role in safeguarding thepatient’s privacy in contracts and organizational policiesand procedures.27
AdvocacyAt the very heart of professionalism is the pediatrician’scommitment to put the interests of children and theirfamilies above his or her own. Altruism may be thedefining feature of professionalism and the one that ismost at risk with the corporate transformation of Amer-ican health care. In particular, managed care arrange-ments can intensify the inherent conflict between thehealth care interests of children and the pediatricians’financial interests.29
Financial incentives to reduce or limit access to careare viewed by many as particularly problematic29,30 andare a source of growing distrust of both pediatricians andmanaged care organizations. Pediatricians must not al-low financial considerations to affect clinical judgmentabout a child’s health and welfare. Managed care, withits emphasis on primary and preventive care, has thepotential to increase access to a full range of pediatric
e1126 AMERICAN ACADEMY OF PEDIATRICS by guest on April 9, 2020www.aappublications.org/newsDownloaded from
clinicians and services but can also result in underutili-zation of appropriate services.30
Pediatricians must be advocates for their patients.They should facilitate access to appropriate and effectivepediatric services and challenge treatment-authorizationpolicies that delay or deny needed treatments, includingmental health services, social work services, develop-mental evaluations, occupational and physical therapy,child life interventions, dental services, and vision, hear-ing, and speech and language services. It is permissibleand even desirable for pediatricians to discuss their con-cerns about specific insurance policies with parents andto ask parents to help by bringing these concerns to theattention of their insurance companies to effect a reso-lution.
Pediatricians should exercise due diligence in con-tracting with payers to avoid assuming legal or financialobligations that would put them in conflict with thehealth and well-being of their patients.31 Physicians arelegally responsible for the claims submitted for theirprofessional services and for the accuracy and complete-ness of information in the medical chart. Pediatriciansshould ensure that coding and billing appropriately re-flect the level of services provided to the patient.32 To doso, some pediatricians choose to implement complianceprograms in accordance with the guidance from theOffice of Inspector General.33,34 If an insurance companyis perceived to be conducting business unethically, itshould be reported to the relevant state board of insur-ance.
As advocates, pediatricians play a necessary role inquality assurance. This may include the need to providefeedback to referring physicians. A pediatrician shouldmake every effort to determine all of the facts in aspecific case before making a judgment about the qualityof care that was rendered by another physician, partic-ularly if opinions are being sought by the parents. Gen-erally, feedback can and should ultimately be providedin an educational and noncritical manner to both pro-vider and parent. The pediatrician receiving feedbackshould recognize this is an opportunity for learning.Qualifying feedback as a source of continuing educationrather than criticism will help pediatricians care for fu-ture patients. Pediatricians, pediatric medical subspecial-ists, and pediatric surgical specialists should all respectone another as critical partners in the optimal delivery ofcare.
Information and EducationPediatricians should inform and educate patients andparents and help them understand clinical recommen-dations and make informed choices among all reason-able care options and referrals. “Gag orders” or insurancepolicy clauses that prohibit the primary care physicianfrom full disclosure of medical options and/or specialtyreferrals are never appropriate. Pediatricians are obli-
gated to disclose the full range of medically, scientifi-cally, legally, ethically, and practically acceptable treat-ment options, even those that are not included in thefamily’s insurance coverage and those with which thepediatrician may philosophically disagree. Health plansmust disclose all relevant information about benefits,including any restrictions in coverage and financial in-centives that might negatively affect a child’s access tocare.35,36 Descriptions should be clear, simply written,and easy for any family to understand. It remains theobligation of parents to understand their children’s in-surance benefits. Pediatricians cannot and should not beexpected to counsel parents on the details of their insur-ance plans. Parents bear the ultimate responsibility tounderstand who and what is covered or not covered. Inthe inpatient setting, social workers and case managersoften can assist with these issues.
Appeals ProcessesPatients and families should have access to fair appealsprocesses, and pediatricians should be child advocateswithin that system. However, health plans are not obli-gated to pay for treatments that are not justifiable onclinical or scientific grounds even if some patients mightdesire them. Pediatricians should take an active role inthe development of practice guidelines and familiarizethemselves with the attributes/recommendations thatwill enable them to distinguish medical managementguidelines that are based solely on cost/utilization datafrom those that are based on scientific evidence.37
MEDICAL SCHOOL TEACHING FACULTY RESPONSIBILITIES TORESIDENTS AND STUDENTSThe obligations of medical school academic and clinicalfaculty to residents and students should include:
● Instructional development of academic competency—adequate, up-to-date academic preparation of resi-dents and students to be competent and ethically re-sponsible pediatricians.
● Modeling appropriate behaviors—using systems orstandards that nurture professionalism, interdiscipli-nary collaboration, respect, and partnership with childand family, including a humane working environ-ment.
● A caring and compassionate environment for learn-ing—active involvement in bedside teaching, with fos-tering of an appropriate learning environment, includ-ing faculty treatment of residents and students.
● Fair assessment processes—fair assessment of profes-sionalism, including remedial education, and one-on-one direct oversight with interim evaluations if thereare problems.
PEDIATRICS Volume 120, Number 4, October 2007 e1127 by guest on April 9, 2020www.aappublications.org/newsDownloaded from
CommunicationPediatric training should focus on providing a core foun-dation of knowledge, attributes, skills, and competenciesto all pediatric residents regardless of their future careerpaths. Communication is a key element of medical prac-tice. Clinicians should be capable of effective, respectful,and compassionate 2-way communication with patients,parents, and other members of the health care team.Health care communication must be formally taught,learned, and evaluated. Students and residents should betaught the principles of cultural effectiveness to enhancetheir understanding of the child and family in the con-text of the medical home.
Modeling Appropriate BehaviorWithin pediatric training programs, residency programdirectors and pediatric faculty members must model theprofessional behavior they seek to instill in their train-ees. Recently, both informal and formal residency cur-ricula have become more challenging as a consequenceof the 80-hour workweek limitation on house officers.Opportunities to model behavior can occur in the clinic,at the bedside, on the telephone, or in the patient’schart. Being able to communicate clearly in the medicalchart and document medical care concisely and correctlyare equally important as verbal communication withfamilies, patients, physicians, and other health care pro-fessionals. Medical liability risk managers have describedthis as an area of professionalism that is in need ofimprovement and recommend use of the acronym OL-FACTORY to help physicians improve their documenta-tion skills: O � original, L � legible, F � factual, A �accurate, C � consistent, T � timely, O � objective, R �rational, and Y � yours.38
Clinical teachers must teach by example and be ca-pable of demonstrating how to manage difficulties thatoccur in relationships with patients, medical staff, orcolleagues; effectively and compassionately communi-cate with patients, families, colleagues, and members ofthe interdisciplinary team; gracefully and honestly ac-knowledge errors; confront poor practice in a colleagueor trainee; and explain to children and parents whenthings have “gone wrong.” Mentors of pediatric houseofficers and medical students should be aware of theprocess of socialization that exists and the various waysthat trainees learn and internalize professional and hu-manistic values, attitudes, and behaviors. Students andresidents may be more influenced by what is known asthe “hidden curriculum” (what is taught by observingthe daily behavior of health care professionals, bothgood and bad) than by formal training in ethics, al-though formal curricula in both ethics and professional-ism are still valuable.39 When pediatricians behave inways that are contrary to ethical standards taught informal courses, they reinforce the view that medicine isa profession that lacks integrity.40 Perhaps more impor-
tantly, when pediatricians keep silent in the face ofinappropriate behavior, the implication is that the statusquo is acceptable, and the opportunity to discuss theprofessional behavior in the clinical context is lost. Cur-rently, unprofessional and unethical physician behavioris often tolerated when it should not be. Students andresidents should be encouraged and advised to evaluatefaculty members as teachers of ethics, knowledge, andattitude, and faculty members should be encouraged toevaluate each other on the basis of professionalism aswell as academic productivity.
Caring and CompassionCaring and compassion are central to the effective prac-tice of pediatrics. Students and residents must be taughtto attend to the emotional, spiritual, and practical real-ities of illness and its effects on children and families aswell as themselves.41 Historically, medicine has definedits mission in terms of “curing” disease while overlook-ing illness (ie, the patient’s experience of disease). Pa-tients and families require a caring physician who isempathetic and strives to understand the illness experi-ence of each child and affected family. How does oneteach or remediate sensitivity and caring? Personal re-flection, small-group discussions,42,43 participation infamily conferences, and longitudinal experiences withfamilies who are living with chronic illness44 are allexamples of key strategies that may be used in nurturingprofessionalism among trainees. More focused methodsinclude role modeling, one-on-one discussion, closer su-pervision, observation of resident interactions with fam-ilies under stressful situations, and feedback sessions inwhich the resident specifically asks for guidance abouthow they could or should have handled difficult inter-actions with parents or patients.45 Exposure to parentpanels, former patients, and siblings of patients throughsmall-group discussion; support group attendance;grand-rounds formats; use of standardized patients inteaching venues; and supervised role-playing are otherways.46
Because students and residents develop their profes-sional identities over time, professionalism should beviewed as a developmental process across all stages of amedical career.47,48 More emphasis on stress manage-ment is essential, and incoming residents might benefitfrom improved orientation regarding the demands ofresidency and ways of coping. In addition to learninghow to care for others, young physicians also must learnto care for themselves.49 Those who have their personalneeds met are, in turn, more supportive of their patients’and families’ needs,50 and this self-nurturing will pro-mote the ability to show compassion and empathy forothers.45 Those who create pediatric training programsneed to be mindful of the ways that students and resi-dents are treated. It is more likely that pediatricians intraining will become caring and compassionate toward
e1128 AMERICAN ACADEMY OF PEDIATRICS by guest on April 9, 2020www.aappublications.org/newsDownloaded from
their patients if they feel that they are treated in a caringand compassionate manner.
Fair Assessment ProcessesStudents and residents are expected to treat patients,families, medical staff, and colleagues fairly. In return,they must be treated fairly in the educational system.This will require developing clear expectations for per-formance, providing adequate opportunities to learn ex-pected competencies and receive clear and frequentfeedback, and providing remediation when neces-sary.3,51–53 There should be a safe mechanism for studentsand residents to appeal evaluations with which theydisagree, including those related to professionalism.
Documentation of deficiencies, mentoring, and per-sonal counseling sessions are critical in the process. Theprinciples and practice of professionalism that are beingtaught must be in place continually during the process ofcounseling and remediation. It is inappropriate for train-ing directors and medical school faculty members toallow residents who have failed to develop appropriateprofessional skills despite counseling and remediation tocomplete the training program and qualify for the ABPexamination process.
PEDIATRICIANS’ RESPONSIBILITIES TO OTHER HEALTH CAREPROFESSIONALS: TEAM RESPECT AND COMMUNICATIONPediatricians must treat each other and all other healthcare professionals with integrity, honesty, and respect intheir daily interactions, because effective patient caredepends on effective team functioning.54 All health careprofessionals share a primary bond in their mutual eth-ical concern for patients. Respectful treatment includesbeing truthful and responsible, following through oncommitments, honoring the expertise of other healthcare professionals, being open to learn from others, andbeing collaborative in patient care. Pediatricians shouldraise concerns about trainees, colleagues, and individualhealth care professionals directly with the relevant par-ties instead of verbalizing issues in front of patients,families, and/or staff. There should be no tolerance ofverbal or physical abuse on the part of either physicianor staff members, because it undermines credibility andeffectiveness with patients and other health care profes-sionals.
Pediatricians also have obligations to provide appro-priate supervision and referral. The AAP acknowledgesthe crucial role that nonphysician health care profes-sionals play in pediatric care and stresses the importanceof working collaboratively with nurses, social workers,chaplains, nurse practitioners, physician assistants, andothers.55,56 Pediatricians should respect the contributionsof other health care professionals but also acknowledgethe appropriate limitations and roles of these profession-als. The AAP states that the relationship among pediatricprofessionals is one of interdependence.56 Incorporation
of the input of these colleagues into the plan of careinstead of treating it as separate and unrelated ensureseffective, coordinated care.
Sexual harassment in the workplace and in educa-tional settings creates an environment that demeanspeople and has a negative effect on individual perfor-mance and effectiveness as well as organizational pro-ductivity and unit morale. It is incumbent on employers,organizations, and institutions to represent all their con-stituents, male and female, and provide education andguidance that discourages this destructive behavior. Inparticular, medical schools and training programs mustbe aware of the prevalence of the problem and haveaction plans available.57
PEDIATRICIANS’ RESPONSIBILITIES TO THE PROFESSION
Peer ReviewProfessional self-regulation is a privilege, not a right, andhas to be earned continuously to sustain public confi-dence in the profession.58 Work toward a system ofmedical regulation that combines professional, organiza-tional, and patients’ perspectives should be aimed atmaking the medical profession accountable for its per-formance.
The use of explicit standards (such as clinical practiceguidelines that are based on evidence evaluation), theadoption of collective and personal responsibility forobserving standards of practice, effective local medicalregulation that is based on quality reviews, a systematicprocess for ensuring continuing medical education, andswift and effective strategies for dealing with physicianmisconduct are integral to maintaining a professionalpractice.
Ironically, science and technology have provided themedical profession with powerful tools that empowerand enable physicians to extend and improve quality oflife while exposing patients to the potential for iatro-genic harm.13 Although members of the public appreci-ate what medical technology can achieve, they also haveheightened awareness of the risk of medical errors59 andthe historic reluctance of the medical profession to admitto these errors. Professionalism demands that eachhealth care professional know and accept his or her ownlimits. It is our responsibility to be open about risks andvariations in performance, to communicate effectively,to act promptly to protect pediatric patients from poorpractice, and to admit to the errors that are an expectedand everyday occurrence in judgment-based clinical de-cision-making.13,60
There is a general reluctance of doctors to reportcolleagues whose performance falls below a minimumstandard because of a lack of absolute clinical guidelines,the question of what constitutes an acceptable degree ofvariation in practice and outcome, the influence of casemix on outcomes, and other variables. Poor performance
PEDIATRICS Volume 120, Number 4, October 2007 e1129 by guest on April 9, 2020www.aappublications.org/newsDownloaded from
or substandard performance can have protean causesincluding stress, burnout, the effects of physical or men-tal illness, death of a loved one, chronic fatigue, com-munication or systems-of-care failure, and others. Ex-amples include lack of attention to detail, failure toreturn telephone calls or pages in a timely fashion whenon call, or failure to follow-up with families regardingtest results when promised. Addressing these issues re-quires active intervention tempered by concern, com-passion, and understanding, because the primary profes-sional obligation of patient safety is at stake.
Clear evidence of what constitutes poor or unsafepractice is more certain and widely recognized. Exam-ples include practicing medicine under the influence ofdrugs or alcohol or with untreated mental health disor-ders, falsifying medical information, or intellectual dis-honesty with colleagues or patients.19 Physicians have anethical obligation to report such behavior in accordancewith the legal requirements in each state, and the pro-fession should show its determination to confront poorpractice. Alcohol or drug impairment should be reportedto the hospital’s in-house impairment program, the chiefof pediatrics, or the chief of the hospital staff. Somemedical societies or state licensing boards have externalimpaired-physician programs to which individuals canbe referred. Issues of incompetence and remediationshould be addressed by the appropriate clinical author-ity. The hospital peer-review body should be notifiedwhen appropriate, and sentinel events should be dis-cussed thoroughly and reported to the Joint Commis-sion. A sentinel event is defined by the Joint Commis-sion as an unexpected occurrence that involves death orserious physical or psychological injury or the riskthereof. Serious injury specifically includes loss of limbor function. The phrase “or the risk thereof” includesany process variation for which a recurrence wouldcarry a significant chance of a serious adverse outcome.Incompetence that poses an immediate threat to thehealth of children should be reported directly to the statelicensing board. Physicians who are under investigationor have been charged should be protected from destruc-tive gossip and rumors, and communication should begoverned by the rules of confidentiality until suchcharges are proven or the physician is exonerated.
We are in the midst of a professional evolution inwhich the language of professional quality review andimprovement is replacing professional solidarity. Medi-cal societies’ ethics committees, hospital credentials andutilization committees, morbidity and mortality reviews,and other forms of peer review have long been estab-lished by organized medicine to scrutinize physicians’professional conduct. Pediatricians in both academic andprivate practice should welcome and support thesemethods of ensuring good medical practice. They bal-ance the pediatricians’ right to exercise medical judg-ment freely with the obligation to do so wisely, compas-
sionately, objectively, and temperately.19 They alsodemand acceptance of the tenet that mistakes happen,can affect any system and, thus, involve any doctor,have to be discussed openly, and provide critical oppor-tunities for learning and creating systematic improve-ment. In states where peer review is considered “discov-erable” by state law, which allows physicians who areengaged in good-faith peer-review activities to be suedafter case review, the peer-review process is underminedby the lack of confidentiality, and the effectiveness ofpeer review is limited.
Medical TestimonyPediatricians are often called to court to testify on behalfof children in cases of suspected abuse and/or neglect.Whether as expert witnesses or witnesses of fact, pedi-atricians have ethical obligations to give honest, objec-tive, and accurate information and should not accept acommitment as an expert witness outside their definedarea of expertise. When medical malpractice is an issue,an expert witness is key to ensuring a fair hearing for thephysician in question as well as for the patient andfamily. The AAP has articulated recommendations forpediatricians who provide expert witness testimony inmedical malpractice cases.61 It is unethical for expertwitnesses to base their fees for testifying contingent onthe outcome of the case.62,63 Reliable, objective, and ac-curate expert witness testimony and a truthful analysisof the standard of care are extremely important in pedi-atric cases in which juries can be manipulated out ofcompassion for injured children and their families.61
A witness of fact who, in the case of medical malprac-tice, is the treating physician, whether as the defendantor the previous or subsequent treating physician, has anethical obligation to be adequately prepared and to tes-tify honestly and truthfully to the best of his or hermedical knowledge. A witness of fact is not to be anadvocate or a partisan in the legal proceeding.
PHARMACEUTICAL ANDOTHER INDUSTRIES AND POTENTIALCONFLICTS OF INTERESTIssues of professionalism and the integrity of the profes-sion as a whole are raised when pediatricians are therecipients of special marketing incentives such as giftsand other perquisites from representatives of the healthcare industry. Such behavior challenges the physician’sclinical objectivity64,65 and poses a conflict of interestbetween the patient’s welfare and the physician’s finan-cial interests. Also, issues of justice are raised as theincreased costs of marketing are passed on to childrenand their families. Despite these concerns, the AMAacknowledges the fact that gift-giving has been a cus-tomary practice in medicine with a beneficial educa-tional and service function to physicians and patients.The AMA recently launched an initiative to educatephysicians and members of the health care industry
e1130 AMERICAN ACADEMY OF PEDIATRICS by guest on April 9, 2020www.aappublications.org/newsDownloaded from
about the AMA guidelines on appropriate gifts fromindustry. The AAP has endorsed the AMA guidelinesregarding gifts to physicians from industry. The AMAguidelines do not prohibit gifts outright but offer 7 basicguidelines for their appropriateness66:
● Any gifts should primarily entail a benefit to patients(eg, education to improve patient care) and should notbe of substantial value.
● Individual gifts of minimal value should be related tothe physician’s work (eg, pens, notepads).
● Meetings should be primarily dedicated, in both timeand effort, to promoting scientific and educationalactivities and discourse.
● Subsidies for meetings should be accepted by the con-ference’s sponsor, not individual participants.
● Subsidies should not be accepted directly or indirectlyto pay for the costs of travel, lodging, or other personalexpenses of physicians attending conferences, includ-ing compensation for the physician’s time.
● Scholarship funds are permissible as long as the selec-tion of students is made by the academic or traininginstitution.
● No gifts should be accepted if there are “stringsattached.”
The American College of Physicians took a slightlydifferent approach in its ethics manual,50 and stronglydiscouraged the acceptance of all types of individualgifts, hospitality, trips, and subsidies from the health careindustry. The American Medical Student Associationtook the toughest policy stand on gifts from the healthcare industry and advocated for outright prohibition.Their recently initiated PharmFree Campaign urgesmedical students to take a pledge to accept no money,gifts, or hospitality from the pharmaceutical industry; toseek unbiased sources of information; and to avoid con-flicts of interest in their medical education and practice.67
The Compliance Program for Pharmaceutical Manu-facturers of the Office of Inspector General provides clearexamples of the expectations regarding the manufactur-ers’ conduct and relationships with purchasers, researchfunding for educational programs, and potential conflictsof interest.68 It is advisable for physicians to heed thisguidance as it pertains to the professional relationshipbetween physicians and representatives of pharmaceu-tical manufacturers.
SUMMARYThe provision of health care in contemporary society isincreasingly complex. Pediatricians are being asked tocare for more patients with more complicated medicaland social histories, using more technology, and oftenwith less time and compensation for the care of eachpatient. The degree of bureaucratic oversight is growing
exponentially. In the practical sense, this leaves pedia-tricians at risk of losing sight of what called them into thehealth profession in the first place—a desire to care forchildren and their families. This report outlines the keycomponents of professionalism in pediatric practice inthe belief that an emphasis on core professional valueswill serve as a moral compass in these turbulent timesand will invigorate pediatric practitioners with the en-thusiasm to strive to provide the quality care to whichthey committed and for which they trained and sacri-ficed when they began their medical careers.
COMMITTEE ON BIOETHICS, 2003–2004
Jeffrey R. Botkin, MD, MPH, ChairpersonDouglas S. Diekema, MD, MPHG. Kevin Donovan, MD, MLAMary E. Fallat, MDEric D. Kodish, MDSteven R. Leuthner, MD, MAMarcia Levetown, MD
LIAISONS
Christine E. Harrison, MDCanadian Paediatric Society
Alessandra Kazura, MDAmerican Academy of Child and AdolescentPsychiatry
Ernest F. Krug, III, MDiv, MDAmerican Board of Pediatrics
Michael K. Lindsay, MDAmerican College of Obstetricians and Gynecologists
CONSULTANT
Dena S. Davis, JD, PhD
CONTRIBUTOR
Jacqueline Glover, PhD
STAFF
Alison Baker, MS
REFERENCES1. Orr RD, Pang N, Pellegrino ED, Siegler M. Use of the Hippo-
cratic oath: a review of twentieth century practice and a con-tent analysis of oaths administered in medical schools in theU.S. and Canada in 1993. J Clin Ethics. 1997;8:377–388
2. Swick HM. Academic medicine must deal with the clash ofbusiness and professional values. Acad Med. 1998;73:751–755
3. Arnold L. Assessing professional behavior: yesterday, today,and tomorrow. Acad Med. 2002;77:502–515
4. National Board of Medical Examiners. Embedding Professional-ism in Medical Education: Assessment as a Tool for Implementation.Philadelphia, PA: National Board of Medical Examiners; 2003
5. ABIM Foundation. American Board of Internal Medicine; ACP-ASIM Foundation. American College of Physicians-AmericanSociety of Internal Medicine; European Federation of InternalMedicine. Medical professionalism in the new millennium: aphysician charter. Ann Intern Med. 2002;136:243–246
6. Medical School Objectives Writing Group. Learning objectivesfor medical student education: guidelines for medical schools—
PEDIATRICS Volume 120, Number 4, October 2007 e1131 by guest on April 9, 2020www.aappublications.org/newsDownloaded from
report I of the Medical School Objectives Project. Acad Med.1999;74:13–18
7. Accreditation Council for Graduate Medical Education. ACGMEOutcome Project: Enhancing Residency Education Through OutcomesAssessment—General Competencies. Version 1.3. Chicago, IL: Ac-creditation Council for Graduate Medical Education; 1999.Available at: www.acgme.org/outcome/comp/compFull.asp.Accessed August 30, 2004
8. American Board of Internal Medicine. Project Professionalism.Philadelphia, PA: American Board of Internal Medicine; 1994
9. Snyder L, Leffler C; Ethics and Human Rights Committee,American College of Physicians. Ethics manual: fifth edition.Ann Intern Med. 2005;142:560–582
10. American Board of Pediatrics. Foundations for Evaluating theCompetency of Pediatricians. Chapel Hill, NC: American Board ofPediatrics; 1974
11. American Board of Pediatrics, Medical Ethics Subcommittee.Teaching and evaluation of interpersonal skills and ethicaldecision making in pediatrics. Pediatrics. 1987;79:829–834
12. American Board of Pediatrics. Appendix F: professionalism. In:Program Director’s Guide to the ABP: Resident Evaluation, Tracking& Certification. Chapel Hill, NC: American Board of Pediatrics;2003
13. Irvine D. The performance of doctors: the new professionalism.Lancet. 1999;353:1174–1177
14. Petersdorf RG. Defining the good doctor [published correctionappears in JAMA. 1993;269:2370]. JAMA. 1993;269:1681–1682
15. English A, Kenney KE. State Minor Consent Laws: A Summary.2nd ed. Chapel Hill, NC: Center for Adolescent Health and theLaw; 2003
16. American Academy of Pediatrics, Committee on Bioethics. In-stitutional ethics committees. Pediatrics. 2001;107:205–209
17. American Academy of Pediatrics, Medical Home Initiatives forChildren With Special Needs Project Advisory Committee. Themedical home. Pediatrics. 2002;110:184–186
18. American Academy of Pediatrics, Committee on PediatricWorkforce. Scope of practice issues in the delivery of pediatrichealth care. Pediatrics. 2003;111:426–435
19. American Medical Association. Code of Medical Ethics: CurrentOpinions With Annotations. Chicago, IL: American MedicalAssociation; 2000
20. Lazarus AA. Boundaries in the physician-patient relationship.JAMA. 1995;274:1346
21. American Academy of Pediatrics, Committee on Practice andAmbulatory Medicine. The use of chaperones during the phys-ical examination of the pediatric patient. Pediatrics. 1996;98:1202
22. American Academy of Pediatrics, Committee on Bioethics. Ap-propriate boundaries in the pediatrician-family-patient rela-tionship. Pediatrics. 1999;104:334–336
23. Novack DH, Suchman AL, Clark W, Epstein RM, Najberg E,Kaplan C. Calibrating the physician: personal awareness andeffective patient care. JAMA. 1997;278:502–509
24. Sawyer SM, Bowes G. Adolescence on the health agenda.Lancet. 1999;354(suppl 2):SII31–SII34
25. Hofmann AD. Managing adolescents and their parents: avoid-ing pitfalls and traps. Adolesc Med. 1992;3:1–12
27. Standards for Privacy of Individually Identifiable HealthInformation; Final Rule. 67 Federal Register 53181–53273(2002) (codified at 45 CFR §160, 164)
28. Health Insurance Portability and Accountability Act. Pub L No.104–191 (1996)
30. Povar G, Moreno J. Hippocrates and the health maintenanceorganization: a discussion of ethical issues. Ann Intern Med.1988;109:419–424
31. Morreim EH. Gaming the system: dodging the rules, ruling thedodgers. Arch Intern Med. 1991;151:443–447
32. American Academy of Pediatrics. Coding for Pediatrics. 12th ed.Elk Grove Village, IL: American Academy of Pediatrics; 2007
33. US Department of Health and Human Services, Office of In-spector General. Compliance Program Guidance for Individualand Small Group Physician Practices. 65 Federal Register59434–59452 (2000)
34. US Department of Health and Human Services, Office of In-spector General. Publication of the OIG Compliance ProgramGuidance for Hospitals. 63 Federal Register 8987–8998 (1998)
35. Hall MA, Berenson RA. Ethical practice in managed care: adose of realism. Ann Intern Med. 1998;128:395–402
36. American Academy of Pediatrics, Committee on Child HealthFinancing. A Pediatrician’s Guide to Managed Care. Berman S,Gross RD, Lewak N, eds. 2nd ed. Elk Grove Village, IL: Amer-ican Academy of Pediatrics; 2001
37. American Academy of Pediatrics, Task Force on Medical Man-agement Guidelines. Guiding principles, attributes, and processto review medical management guidelines. Pediatrics. 2001;108:1378–1382
38. American Academy of Pediatrics. Medical Liability for Pediatri-cians. Berger JE, Dietschel CH Jr, eds. 6th ed. Elk Grove Village,IL: American Academy of Pediatrics; 2004
39. Hafferty FW, Franks R. The hidden curriculum, ethics teach-ing, and the structure of medical education. Acad Med. 1994;69:861–871
40. Inui TS. A Flag in the Wind: Educating for Professionalism inMedicine. Washington, DC: Association of American MedicalColleges; 2003
41. Goleman D. Emotional Intelligence. New York, NY: BantamBooks; 1997
42. Kjeldmand D, Holmstrom I, Rosenqvist U. How patient-centred am I? A new method to measure physicians’ patient-centredness. Patient Educ Couns. 2006;62:31–37
43. Amiel GE, Ungar L, Alperin M, Baharier Z, Cohen R, Reis S.Ability of primary care physician’s to break bad news: a per-formance based assessment of an educational intervention.Patient Educ Couns. 2006;60:10–15
44. Gaver A, Borkon JM, Weingarter MA. Illness in context andfamilies as teachers: a year-long project for medical students.Acad Med. 2005;80:448–451
45. Werner ER, Adler R, Robinson R, Korsch BM. Attitudes andinterpersonal skills during pediatric internship. Pediatrics. 1979;63:491–499
46. Greenberg LW, Ochsenschlager D, O’Donnell R, Mastruserio J,Cohen GJ. Communicating bad news: a pediatric department’sevaluation of a simulated intervention. Pediatrics. 1999;103:1210–1217
47. Testerman JK, Morton KR, Loo LK, Worthley JS, LambertonHH. The natural history of cynicism in physicians. Acad Med.1996;71(10 suppl):S43–S45
48. Ginsburg S, Regehr G, Stern D, Lingard L. The anatomy of theprofessional lapse: bridging the gap between traditional frame-works and students’ perceptions. Acad Med. 2002;77:516–522
49. Branch WT Jr. The ethics of caring and medical education. AcadMed. 2000;75:127–132
50. Markakis KM, Beckman HB, Suchman AL, Frankel RM. Thepath to professionalism: cultivating humanistic values and at-titudes in residency training. Acad Med. 2000;75:141–150
51. Papadakis MA, Osborn EH, Cooke M, Healy K. A strategy forthe detection and evaluation of unprofessional behavior inmedical students. University of California, San Francisco
e1132 AMERICAN ACADEMY OF PEDIATRICS by guest on April 9, 2020www.aappublications.org/newsDownloaded from
School of Medicine Clerkships Operation Committee. AcadMed. 1999;74:980–990
52. Association of American Medical Colleges, Group on Educa-tional Affairs. Assessment of Professionalism Project. Washington,DC: Association of American Medical Colleges; 2002. Availableat: www.aamc.org/members/gea/professionalism.pdf. Ac-cessed July 30, 2007
53. Ginsburg S, Regehr G, Hatala R, et al. Context, conflict, andresolution: a new conceptual framework for evaluating profes-sionalism. Acad Med. 2000;75(10 suppl):S6–S11
54. American College of Physicians. Ethics manual: fourth edition.Ann Intern Med. 1998;128:576–594
55. American Academy of Pediatrics, Committee on Fetus andNewborn. Advanced practice in neonatal nursing. Pediatrics.2003;111:1453–1454
56. American Academy of Pediatrics, Committee on Hospital Care.The role of the nurse practitioner and physician assistant in thecare of hospitalized children. Pediatrics. 1999;103:1050–1052
57. American Academy of Pediatrics, Committee on PediatricWorkforce, Subcommittee on Women in Pediatrics. Preventionof sexual harassment in the workplace and educational set-tings. Pediatrics. 2000;106:1498–1499
58. Irvine D. The performance of doctors. I: professionalism andself regulation in a changing world. BMJ. 1997;314:1540–1542
59. Institute of Medicine, Committee on Quality of Health Care inAmerica. To Err Is Human: Building a Safer Health System. Kohn
61. American Academy of Pediatrics, Committee on Medical Lia-bility. Guidelines for expert witness testimony in medical mal-practice litigation [published correction appears in Pediatrics.2002;110:651]. Pediatrics. 2002;109:974–979
62. American College of Physicians. Guidelines for the physicianexpert witness. Ann Intern Med. 1990;113:789
63. American Board of Internal Medicine, Subcommittee on Eval-uation of Humanistic Qualities in the Internist. Evaluation ofhumanistic qualities in the internist. Ann Intern Med. 1983;99:720–724
64. Wazana A. Physicians and the pharmaceutical industry: is a giftever just a gift? JAMA. 2000;283:373–380
65. Lexchin J. Interactions between physicians and the pharma-ceutical industry: what does the literature say? CMAJ. 1993;149:1401–1407
66. American Medical Association. Ethical guidelines for gifts tophysicians from industry. Available at: www.ama-assn.org/ama/pub/category/5689.html. Accessed April 26, 2007
67. Rothman DJ. Medical professionalism: focusing on the realissues. N Engl J Med. 2000;342:1283–1286
68. Department of Health and Human Services, Office of InspectorGeneral. OIG Compliance Program for Pharmaceutical Manu-facturers. 68 Federal Register 23731–23743 (2003)
PEDIATRICS Volume 120, Number 4, October 2007 e1133 by guest on April 9, 2020www.aappublications.org/newsDownloaded from
Outline categories of professional behavior here. As an example, this outline of categories of a wholly unrelated topic is provided.
Use the space below to make your outline.
ACGME Professionalism Milestones:
• Humanism• Professionalization• Professional Conduct• Awareness of Limitations• Trustworthy• Accept Ambiguity
Notes for Faculty
There are no right answers but often residents will not recognize aspects of professional behavior based on their experience to date. Also, residents may not recognize commonalities between specific behaviors. Prompt the residents to consider other categories using an example or one of your own experiences.
As a guideline, you can use the ACGME Professionalism Milestones or the elements of professionalism from the 2002 Physician Charter to help residents expand their own list once they’ve committed to it.
Point out that some aspects of professionalism are manifested at early stages in one’s career (e.g. being on time) and others may manifest later in a career (research integrity, financial conflicts of interest).
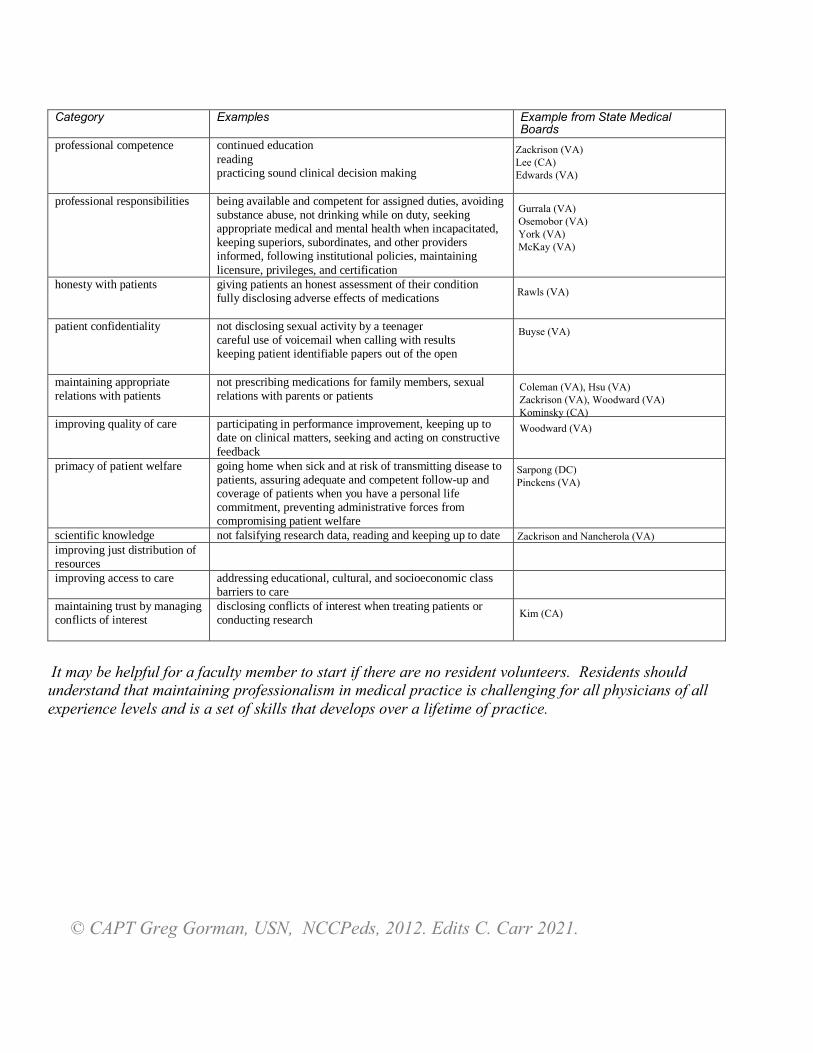
Category Examples Example from State Medical Boards
professional competence continued education reading practicing sound clinical decision making
professional responsibilities being available and competent for assigned duties, avoiding substance abuse, not drinking while on duty, seeking appropriate medical and mental health when incapacitated, keeping superiors, subordinates, and other providers informed, following institutional policies, maintaining licensure, privileges, and certification
honesty with patients giving patients an honest assessment of their condition fully disclosing adverse effects of medications
patient confidentiality not disclosing sexual activity by a teenager careful use of voicemail when calling with results keeping patient identifiable papers out of the open
maintaining appropriate relations with patients
not prescribing medications for family members, sexual relations with parents or patients
improving quality of care participating in performance improvement, keeping up to date on clinical matters, seeking and acting on constructive feedback
primacy of patient welfare going home when sick and at risk of transmitting disease to patients, assuring adequate and competent follow-up and coverage of patients when you have a personal life commitment, preventing administrative forces from compromising patient welfare
scientific knowledge not falsifying research data, reading and keeping up to date improving just distribution of resources improving access to care addressing educational, cultural, and socioeconomic class
barriers to care maintaining trust by managing conflicts of interest
disclosing conflicts of interest when treating patients or conducting research
It may be helpful for a faculty member to start if there are no resident volunteers. Residents should understand that maintaining professionalism in medical practice is challenging for all physicians of all experience levels and is a set of skills that develops over a lifetime of practice.