Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live NCCN Guidelines: Gastric Cancer 1 PRACTICE AID Unresectable locally advanced, locally recurrent, or metastatic disease Karnofsky PS ≥60% or ECOG PS ≤2 Karnofsky PS <60% or ECOG PS ≥3 Perform HER2, PD-L1, MSI by PCR/MMR by ICH testing (if not done previously) if metastatic adenocarcinoma is documented or suspected Best supportive care HER2 All Others Trastuzumab • Add to first-line chemotherapy for HER2 overexpressing metastatic adenocarcinoma • Combination with fluoropyrimidine and platinum agents • Not recommended for use with anthracyclines First·Line Therapy • Two-drug cytotoxic regimens are preferred because of lower toxicity • Three-drug cytotoxic regimens should be reserved for medically fit patients with good PS and access to frequent toxicity evaluation • Oxaliplatin is generally preferred over cisplatin because of lower toxicity Preferred Regimens • Fluoropyrimidine (fluorouracil or capecitabine) and oxaliplatin • Fluoropyrimidine (fluorouracil or capecitabine) and cisplatin Performance Status Palliative Management
Transcript
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
Perform HER2, PD-L1, MSI by PCR/MMR by ICH testing (if not done previously) if
metastatic adenocarcinoma is documented or suspected
Bestsupportive
care
HER2 All Others
Trastuzumab• Add to first-line chemotherapy for HER2 overexpressing metastatic adenocarcinoma• Combination with fluoropyrimidine and platinum agents • Not recommended for use with anthracyclines
First·Line Therapy
• Two-drug cytotoxic regimens are preferred because of lower toxicity• Three-drug cytotoxic regimens should be reserved for medically fit patients with good PS and access to frequent toxicity evaluation• Oxaliplatin is generally preferred over cisplatin because of lower toxicity
Preferred Regimens• Fluoropyrimidine (fluorouracil or capecitabine) and oxaliplatin • Fluoropyrimidine (fluorouracil or capecitabine) and cisplatin
Performance Status
Palli
ativ
e M
anag
emen
t
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
NCCN Guidelines: Gastric Cancer1PRACTICE AID
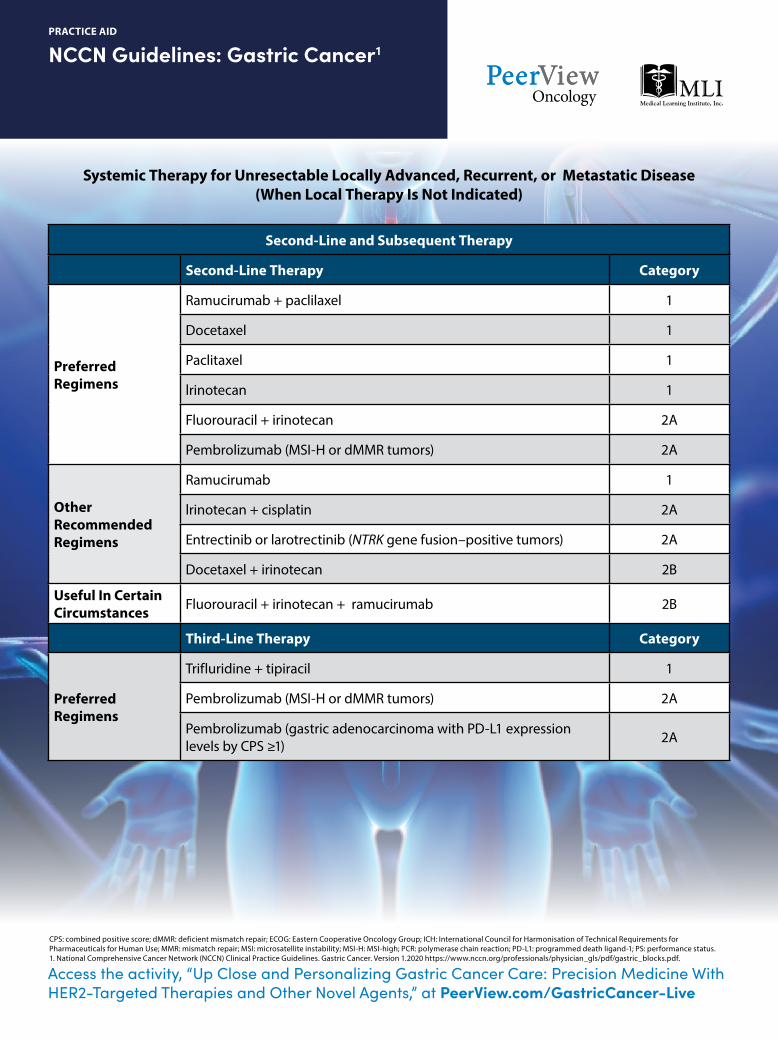
CPS: combined positive score; dMMR: deficient mismatch repair; ECOG: Eastern Cooperative Oncology Group; ICH: International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use; MMR: mismatch repair; MSI: microsatellite instability; MSI-H: MSI-high; PCR: polymerase chain reaction; PD-L1: programmed death ligand-1; PS: performance status.1. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines. Gastric Cancer. Version 1.2020 https://www.nccn.org/professionals/physician_gls/pdf/gastric_blocks.pdf.
Systemic Therapy for Unresectable Locally Advanced, Recurrent, or Metastatic Disease (When Local Therapy Is Not Indicated)
Second-Line and Subsequent Therapy
Second-Line Therapy Category
Preferred Regimens
Ramucirumab + paclilaxel 1
Docetaxel 1
Paclitaxel 1
lrinotecan 1
Fluorouracil + irinotecan 2A
Pembrolizumab (MSI-H or dMMR tumors) 2A
Other Recommended Regimens
Ramucirumab 1
lrinotecan + cisplatin 2A
Entrectinib or larotrectinib (NTRK gene fusion–positive tumors) 2A
Docetaxel + irinotecan 2B
Useful In Certain Circumstances Fluorouracil + irinotecan + ramucirumab 2B
Third-Line Therapy Category
Preferred Regimens
Trifluridine + tipiracil 1
Pembrolizumab (MSI-H or dMMR tumors) 2A
Pembrolizumab (gastric adenocarcinoma with PD-L1 expression levels by CPS ≥1) 2A
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
NCCN’s Principles of Pathologic Review and Biomarker Testing1
PRACTICE AID
lmmunohistochemical Criteria for Scoring HER2 Expression in Gastric Cancer
Surgical Specimen Expression Pattern,
lmmunohistochemistry
Biopsy Specimen Expression Pattern,
lmmunohistochemistry
HER2 Overexpression Assessment
0No reactivity or membranous
reactivity in <10%of cancer cells
No reactivity or no membranous reactivity
in any cancer cell Negative
1+
Faint or barely perceptible membranous reactivity in
≥10% of cancer cells; cells are reactive only in part
of their membrane
Cluster of five or more cancer cells with a faint
or barely perceptible membranous reactivity
irrespective of percentage of cancer cells positive
Negative
2+
Weak to moderate complete, basolateral, or lateral
membranous reactivity in ≥10% of cancer cells
Cluster of five or more cancer cells with a weak to moderate complete,
basolateral, or lateral membranous reactivity
irrespective of percentage of cancer cells positive
Equivocal
3+
Strong complete, basolateral, or lateral
membranous reactivity in ≥10% of cancer cells
Cluster of five or more cancer cells with a strong
complete, basolateral, or lateral membranous reactivity irrespective
of percentage of cancer cells positive
Positive
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
NCCN’s Principles of Pathologic Review and Biomarker Testing1
PRACTICE AID
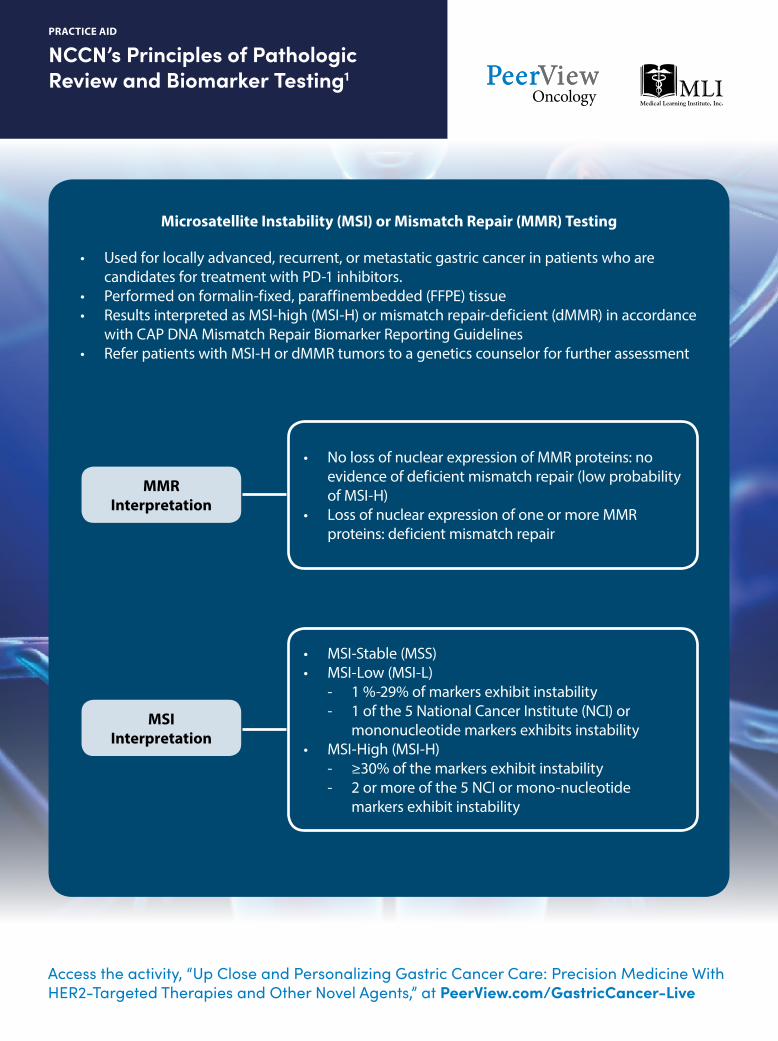
• Used for locally advanced, recurrent, or metastatic gastric cancer in patients who are candidates for treatment with PD-1 inhibitors.
• Performed on formalin-fixed, paraffin embedded (FFPE) tissue • Results interpreted as MSl-high (MSI-H) or mismatch repair-deficient (dMMR) in accordance
with CAP DNA Mismatch Repair Biomarker Reporting Guidelines• Refer patients with MSI-H or dMMR tumors to a genetics counselor for further assessment
• No loss of nuclear expression of MMR proteins: no evidence of deficient mismatch repair (low probability of MSI-H)
• Loss of nuclear expression of one or more MMR proteins: deficient mismatch repair
• MSI-Stable (MSS)• MSI-Low (MSI-L) - 1 %-29% of markers exhibit instability - 1 of the 5 National Cancer Institute (NCI) or mononucleotide markers exhibits instability• MSI-High (MSI-H) - ≥30% of the markers exhibit instability - 2 or more of the 5 NCI or mono-nucleotide markers exhibit instability
Microsatellite Instability (MSI) or Mismatch Repair (MMR) Testing
MMR Interpretation
MSI Interpretation
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
NCCN’s Principles of Pathologic Review and Biomarker Testing1
PRACTICE AID
CAP: College of American Pathologists; NCCN: National Comprehensive Cancer Network; PD-1: programmed cell death protein 1; PD-L1: programmed death-ligand 1. 1. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines. Gastric Cancer. Version 1.2020 https://www.nccn.org/professionals/physician_gls/pdf/gastric_blocks.pdf.
• Used for locally advanced, recurrent, or metastatic gastric carcinomas in patients who are candidates for treatment with PD-1 inhibitors
• An FDA-approved companion diagnostic test for use on FFPE tissue is available as an aid in identifying patients for treatment with PD-1 inhibitors
• Should be performed only in CLIA-approved laboratories
• This is a qualitative immuno-histochemical assay using anti–PD-L1 antibodies for the detection of PD-L1 protein in FFPE tissues from gastric adenocarcinoma
• A minimum of 100 tumor cells must be present in the PD-L1–stained slide for the specimen to be considered adequate for PD-L1 evaluation
• A specimen is considered to have PD-L1 expression if the Combined Positive Score (CPS) ≥1
- CPS is the number of PD-L1 staining cells (ie, tumor cells, lymphocytes, macrophages) divided by the total number of viable tumor cells, multiplied by 100.
PD-L1 Testing
Assessment of PD-L1 Protein
Expression in Gastric Cancers
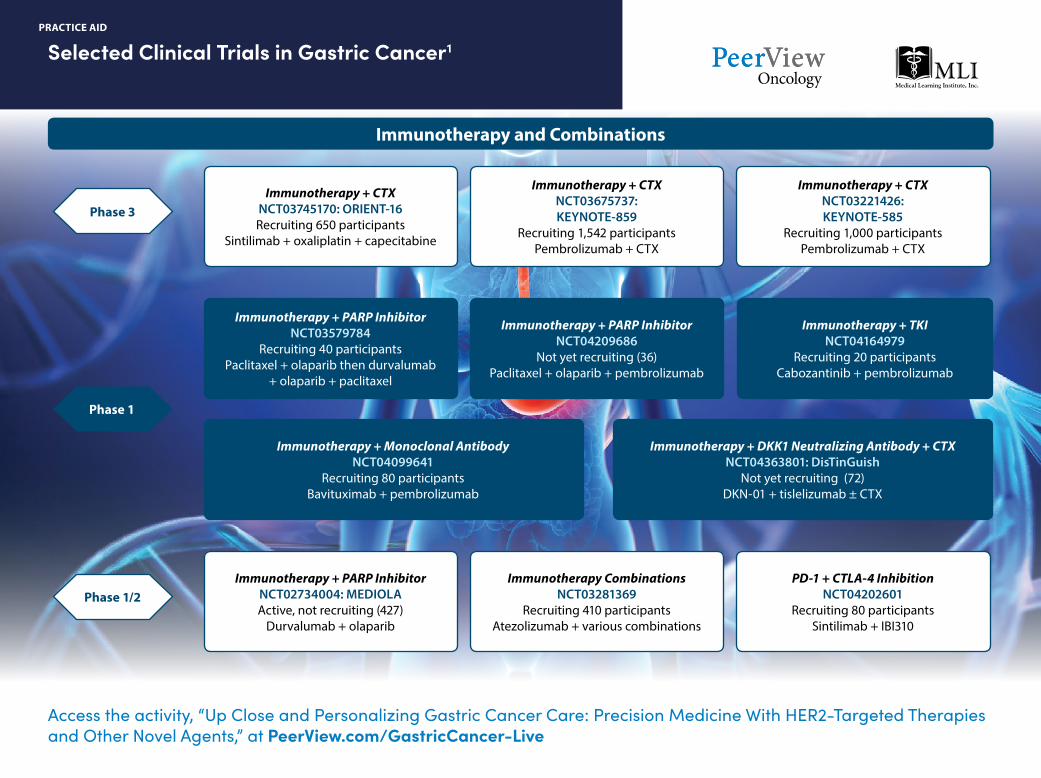
Selected Clinical Trials in Gastric Cancer1
PRACTICE AID
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
Not yet recruiting (220)Trastuzumab deruxtecan monotherapy
and combinations with CTX or durvalumab
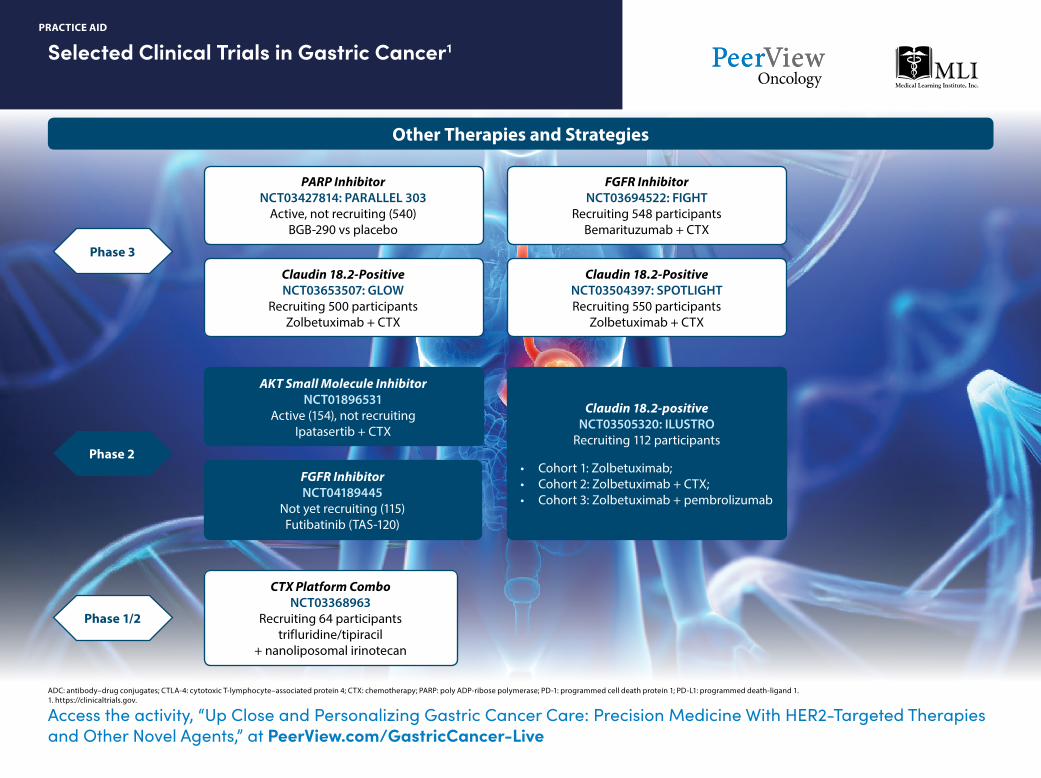
Phase 3
Phase 2
Phase 1b/2
Phase 2/3
Phase 1
Selected Clinical Trials in Gastric Cancer1
PRACTICE AID
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
ADC: antibody–drug conjugates; CTLA-4: cytotoxic T-lymphocyte–associated protein 4; CTX: chemotherapy; PARP: poly ADP-ribose polymerase; PD-1: programmed cell death protein 1; PD-L1: programmed death-ligand 1. 1. https://clinicaltrials.gov.
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
ASCO Guidance on Allocation of ScarceResources During COVID-19 Pandemic1,2
PRACTICE AID
What special training is necessary to prepare my staff for a local outbreak of COVID-19?
Train staff on:• Symptom recognition• Screening procedures• Use of Standard Precautions and personal protective equipment (PPE)• Obtaining SARS-COV2 testing for patients according to current testing guidelines• Protocols for triaging and assessing patients quickly• Identifying and referring patients, families, and
coworkers to telephone-based mental health services
What patient scheduling changes should be made while pandemic restrictions exist?
• Because of reduced waiting areas, the number of appointments may have to be decreased or the time between appointments may have to be increased
• Postpone routine follow-up visits of patients not on active cancer treatment, including 6-month and 12-month survivorship visits
• Schedule brief, remote check-ins with patients on maintenance therapies to ensure that they have sufficient drug supplies; provide instructions on when they should call their provider
• Institute direct telecommunication for survivorship check-ins; create a timeline over the next months to schedule calls
• Communicate COVID-19 information and the rationale for changes in appointments via direct telecommunication, websites, and patient portals
• Consider home collection of routine lab samples instead of patient visits into the clinic; results can be communicated via telephone
• For areas not yet affected by widespread, local transmission, postpone nonurgent visits so urgent visits can be scheduled more immediately
• Use telemedicine for patients not requiring a physical exam, treatment, or in-office diagnostics
• Ask patients to use telephone triage, patient portals, online assessment tools, or to call and speak with a staff member
• Conduct remote check-ins to monitor high-risk patients’ symptoms
What workplace changes should be made to prepare for a local outbreak of COVID-19?
• If necessary, obtain additional PPE for staff members who do not usually use it
• Limit facility access to one point of entry, if possible; vendors, minimal ancillary services, most or all visitors, and people younger than age 18 years should be denied access
• Consider remote or virtual support services• Establish outside triage stations with social distancing
of 6 feet apart to screen patients and visitors for COVID-19 symptoms and fever before appointments
• Install barriers or social distancing mechanisms at front desks if screening is not conducted outside of the facility
• Convert waiting areas to allow for distancing of at least 6 feet (eg, move chairs, cordon off every other chair)
• Convert open infusion suites to semi-private spaces with at least 6 feet distance between patients and/or use available curtains as a barrier between patients
• Suspend (or move to a virtual platform) all onsite group and patient activities (eg, yoga, education seminars, support groups)
How should clinical trial investigators respond to the COVID-19 pandemic?
• ASCO acknowledges that conducting clinical trials will be particularly challenging during this time
• The FDA has issued guidance on management of clinical trial patients during the coronavirus pandemic
– Go to: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/fda-guidance-conduct-clinical-trials-medical-products-during-covid-19-public-health-emergency
• The National Cancer Institute has issued guidance on the NCI Central Institutional Review Board
Access the activity, “Up Close and Personalizing Gastric Cancer Care: Precision Medicine With HER2-Targeted Therapies and Other Novel Agents,” at PeerView.com/GastricCancer-Live
ASCO: American Society of Clinical Oncology; HCC: hepatocellular carcinoma.1. https://www.sirweb.org/practice-resources/toolkits/covid-19-toolkit/covid-19-planning. 2. https://www.asco.org/asco-coronavirus-information/provider-practice-preparedness-covid-19.
ASCO Guidance on Allocation of ScarceResources During COVID-19 Pandemic1,2
PRACTICE AID
What screening and infection prevention and control practices should my workplace undertake?
• To address asymptomatic or presymptomatic transmission, everyone should put on a face mask or other face covering—regardless of symptoms—before entering the facility
• When scheduling appointments, ask patients to call ahead and discuss the need to reschedule their appointments if they develop symptoms of a respiratory infection (eg, cough, sore throat, fever) on the day they are scheduled to be seen
• Contact the patient the day before the appointment and screen for symptoms of cough, sore throat, fever, or other flu-like symptoms
– If symptoms are present, use triage protocols to determine if an appointment is necessary or if the patient can be managed from home – If the patient can be managed from home, the patient should be rescheduled until such time when he or she is determined to be no longer infectious
What screening and infection prevention and control practices should my workplace undertake upon patient arrival or during the visit?
• Allow only essential visitors who are not displaying symptoms of a respiratory or other infection; if essential, limit the number to one visitor per patient for all provider visits
• Visitors should not enter communal treatment areas—ask them to wait in vehicles or return after treatment• Encourage use of alternative mechanisms for patient and visitor interactions, such as video-calls on cell phones or tablets• Healthcare personnel should wear facemasks at all times while they are in the healthcare facility; when available,
facemasks are preferred over cloth face coverings, because they protect the wearer from exposure to infectious material from others
• Healthcare personnel screening patients and visitors at arrival should wear PPE (including masks) and have access to waste bins and cleaning/disinfecting agents
• Ask patients and visitors if they have symptoms of cough, sore throat, or fever; if they’ve been out of the country in the past 14 days; or if they’ve been exposed to anyone with respiratory symptoms or known COVID-19; when available, use an infrared thermometer to take temperatures during screening
• Provide signage with COVID-19 screening questions and visualization of symptoms for all patient/visitors, as well as patient education materials and illustrations of proper hygiene for infection prevention and symptoms to report
• Patients with suspected infection should receive a facemask and be rapidly isolated until more thorough screening or testing can be conducted. Isolation should take place in an exam room or other private area with the door closed
• All staff entering the room of a patient with known or suspected COVID-19 should adhere to Standard Precautions and use a N95 respirator or facemask, gown, gloves, and eye protection; cloth face coverings are not proven effective PPE and should not be worn for the care of patients with known or suspected COVID-19 or other situations where a respirator or facemask is warranted
• Establish a plan of action for patients who present with respiratory symptoms (eg, resource for testing, schedule patient with primary care or local/health department)