NCD Clinical Management: Focus for 2015 Feisul Idzwan Mustapha MBBS, MPH, AM(M) Public Health Physician, NCD Section, Disease Control Division Ministry of Health, Malaysia Clinical Dietetics Update 2015 23 March 2015 Cheras, Selangor [email protected]Ministry of Health Malaysia Slides #10 till #25 courtesy of Dr Rotina Abu Bakar, Public Health Physician, Disease Control Division, MOH
Transcript
NCD Clinical Management:Focus for 2015
Feisul Idzwan Mustapha MBBS, MPH, AM(M)
Public Health Physician, NCD Section, Disease Control DivisionMinistry of Health, Malaysia
Slides #10 till #25 courtesy of Dr Rotina Abu Bakar,
Public Health Physician, Disease Control Division,
MOH
2
Source of icons: World Heart Federation Champion Advocates Programme
Global NCD
Targets
20%15%
23%15%
HED* <1.2%
35.2%30.0%
8.7 6.0 gm
32.2%24.0%
<15.0%
Targets for Malaysia
* Heavy episodic
drinking
Proportional mortality, Malaysia (% of total deaths, all ages, both sexes)
3
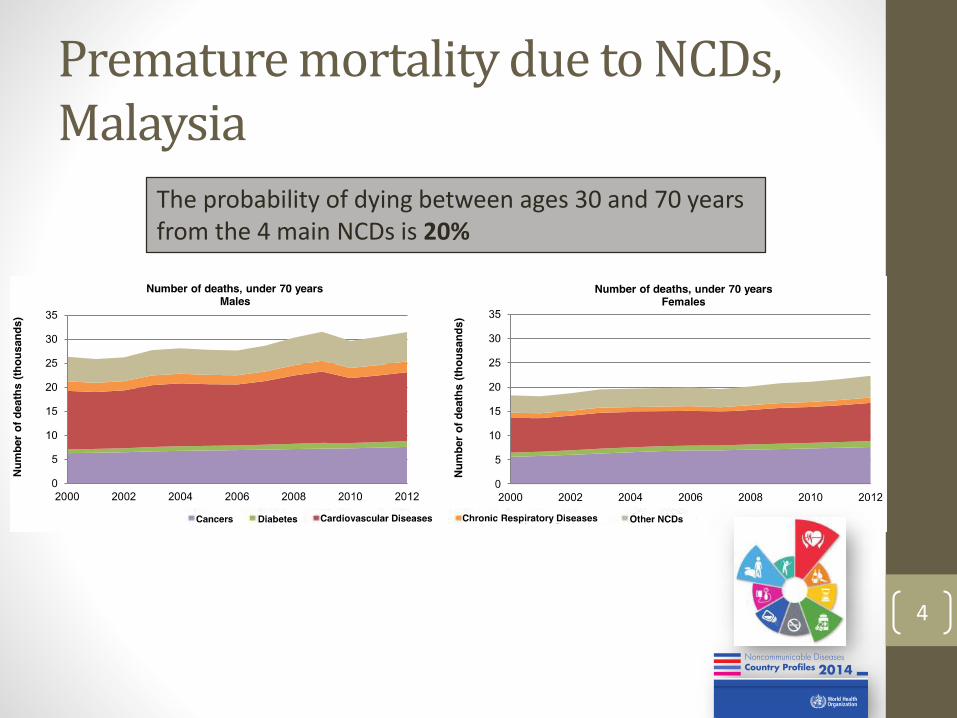
Premature mortality due to NCDs, Malaysia
4
The probability of dying between ages 30 and 70 years from the 4 main NCDs is 20%
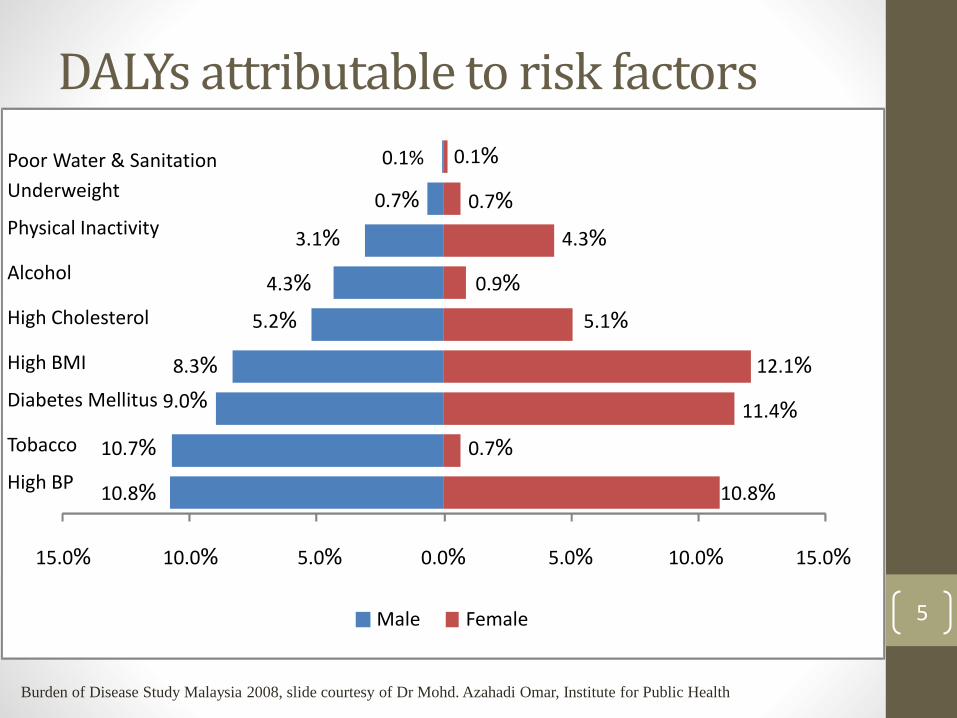
DALYs attributable to risk factors
5
10.8%
10.7%
9.0%
8.3%
5.2%
4.3%
3.1%
0.7%
0.1%
10.8%
0.7%
11.4%
12.1%
5.1%
0.9%
4.3%
0.7%
0.1%
15.0% 10.0% 5.0% 0.0% 5.0% 10.0% 15.0%
High BP
Tobacco
Diabetes Mellitus
High BMI
High Cholesterol
Alcohol
Physical Inactivity
Underweight
Poor Water & Sanitation
Male Female
Burden of Disease Study Malaysia 2008, slide courtesy of Dr Mohd. Azahadi Omar, Institute for Public Health
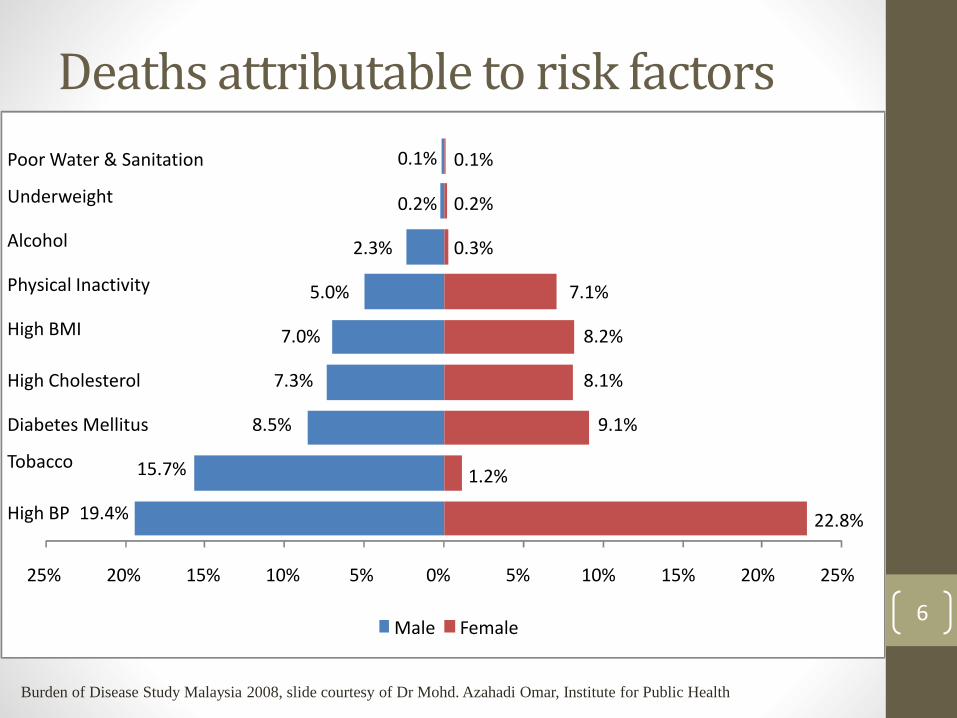
19.4%
15.7%
8.5%
7.3%
7.0%
5.0%
2.3%
0.2%
0.1%
22.8%
1.2%
9.1%
8.1%
8.2%
7.1%
0.3%
0.2%
0.1%
25% 20% 15% 10% 5% 0% 5% 10% 15% 20% 25%
High BP
Tobacco
Diabetes Mellitus
High Cholesterol
High BMI
Physical Inactivity
Alcohol
Underweight
Poor Water & Sanitation
Male Female
Deaths attributable to risk factors
Burden of Disease Study Malaysia 2008, slide courtesy of Dr Mohd. Azahadi Omar, Institute for Public Health
6
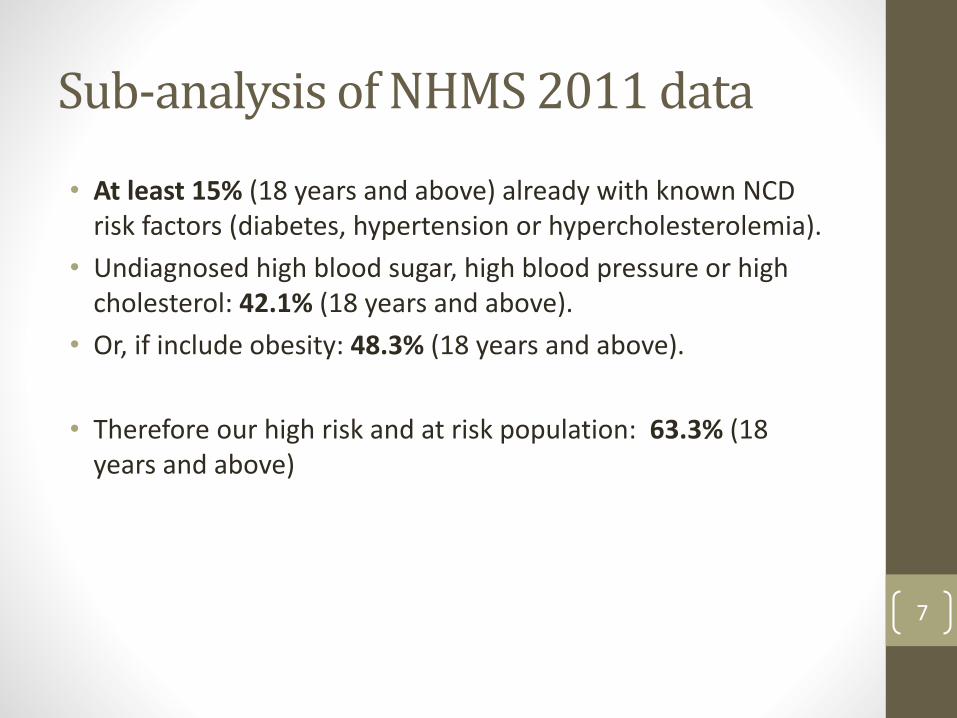
Sub-analysis of NHMS 2011 data
• At least 15% (18 years and above) already with known NCD risk factors (diabetes, hypertension or hypercholesterolemia).
• Undiagnosed high blood sugar, high blood pressure or high cholesterol: 42.1% (18 years and above).
• Or, if include obesity: 48.3% (18 years and above).
• Therefore our high risk and at risk population: 63.3% (18 years and above)
7
8
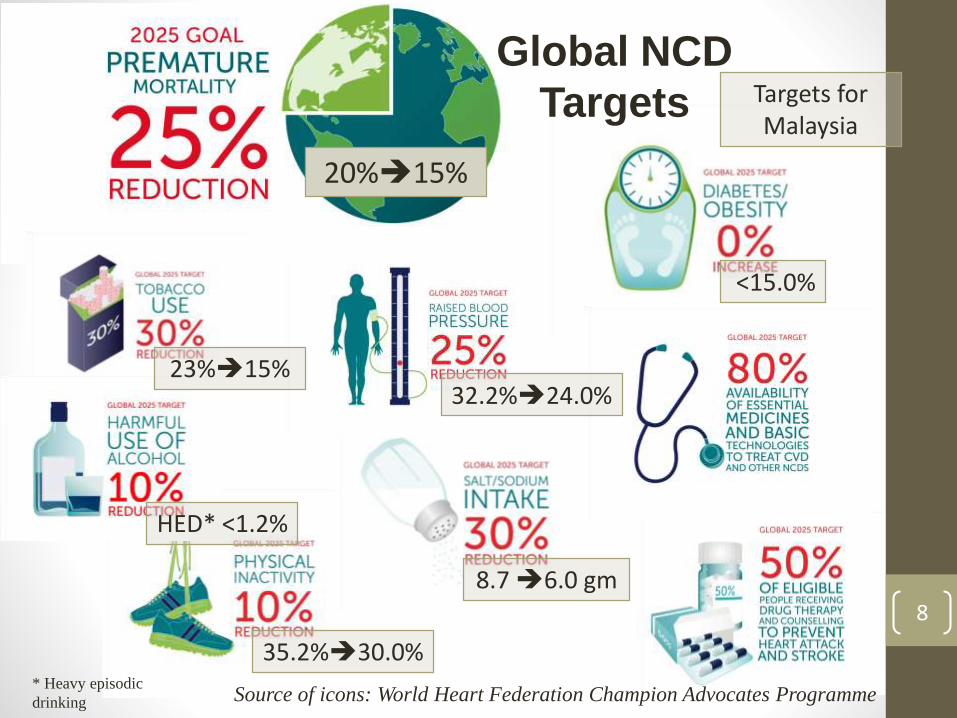
Source of icons: World Heart Federation Champion Advocates Programme
Global NCD
Targets
20%15%
23%15%
HED* <1.2%
35.2%30.0%
8.7 6.0 gm
32.2%24.0%
<15.0%
Targets for Malaysia
* Heavy episodic
drinking
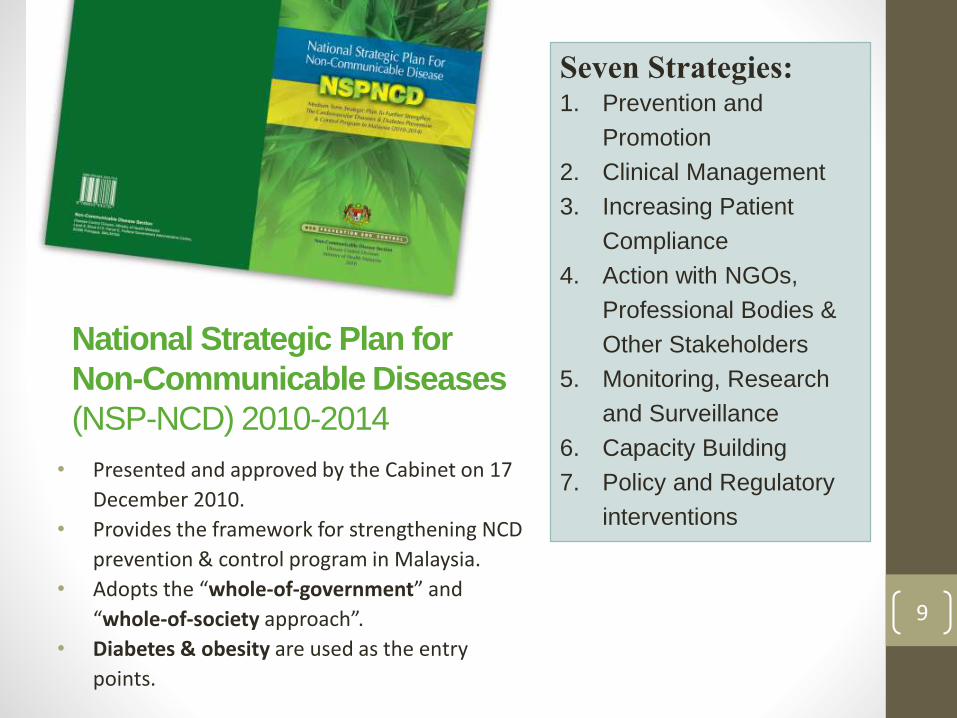
National Strategic Plan for
Non-Communicable Diseases
(NSP-NCD) 2010-2014
• Presented and approved by the Cabinet on 17
December 2010.
• Provides the framework for strengthening NCD
prevention & control program in Malaysia.
• Adopts the “whole-of-government” and
“whole-of-society approach”.
• Diabetes & obesity are used as the entry
points.
Seven Strategies:1. Prevention and
Promotion
2. Clinical Management
3. Increasing Patient
Compliance
4. Action with NGOs,
Professional Bodies &
Other Stakeholders
5. Monitoring, Research
and Surveillance
6. Capacity Building
7. Policy and Regulatory
interventions
9
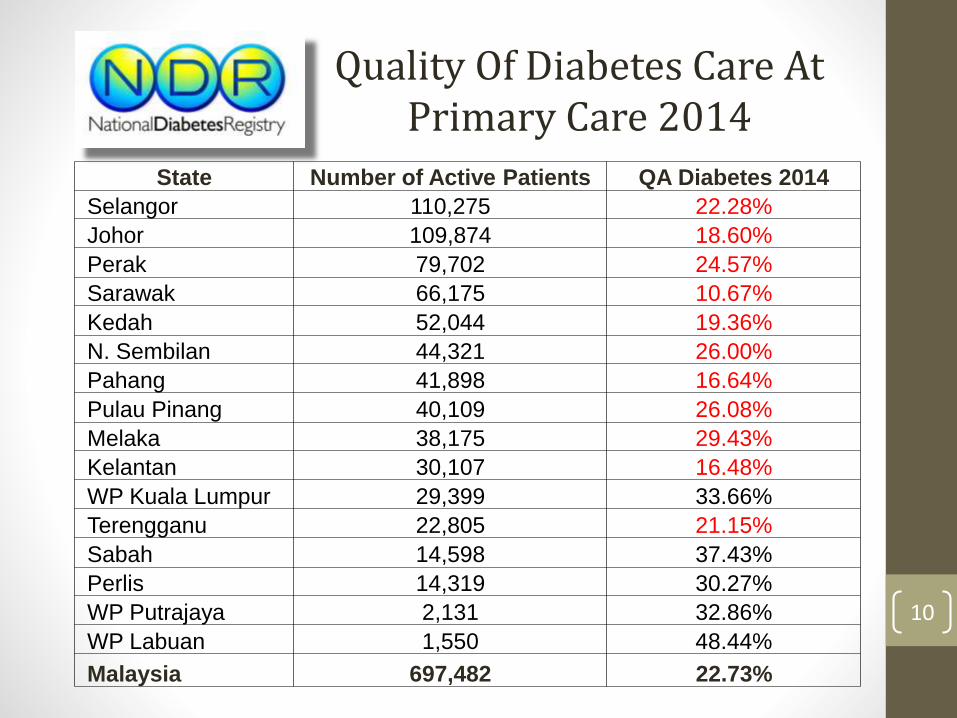
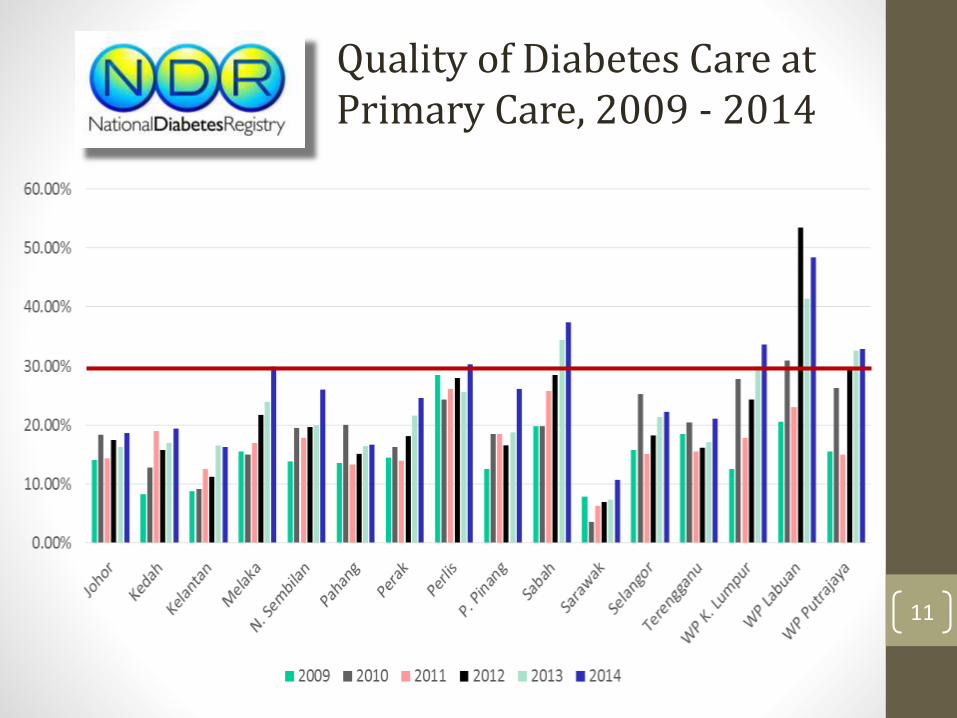
Quality Of Diabetes Care At Primary Care 2014
10
State Number of Active Patients QA Diabetes 2014
Selangor 110,275 22.28%
Johor 109,874 18.60%
Perak 79,702 24.57%
Sarawak 66,175 10.67%
Kedah 52,044 19.36%
N. Sembilan 44,321 26.00%
Pahang 41,898 16.64%
Pulau Pinang 40,109 26.08%
Melaka 38,175 29.43%
Kelantan 30,107 16.48%
WP Kuala Lumpur 29,399 33.66%
Terengganu 22,805 21.15%
Sabah 14,598 37.43%
Perlis 14,319 30.27%
WP Putrajaya 2,131 32.86%
WP Labuan 1,550 48.44%
Malaysia 697,482 22.73%
Quality of Diabetes Care at Primary Care, 2009 - 2014
11
Translating Chronic Care Model into Our Primary Care
Multidisciplinary NCD Team• Doctor• AMO
• Nurse / DE• Dietician
• Pharmacist
Decision support
Community Resources
Efficient Clinical Information System
Informed, Empowered Patient
Coordinated, Continuous and Comprehensive Care
Self-management support
Productive Interactions
12
Focus 2015: Initiatives to Improve Clinical Outcome of NCDs
13
No Strategy Activity
1. Informed,
Empowered Patient
1. Development and implementation of
Peer Support Diabetes Program.
2. Multidisciplinary
NCD Team
2. Development and implementation of
an appraisal system / incentive to
recognize health center with excellent
Diabetes care, based on QA
achievement.
3. Personalized NCD care by Medical
Officer and Diabetes Educator in
health centres.
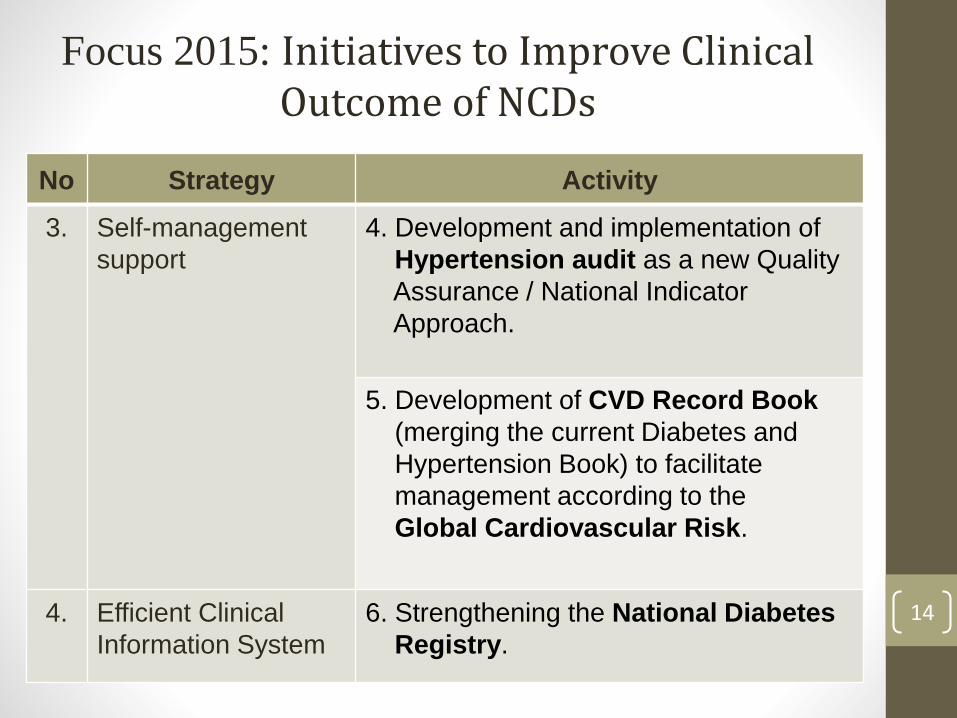
Focus 2015: Initiatives to Improve Clinical Outcome of NCDs
14
No Strategy Activity
3. Self-management
support
4. Development and implementation of
Hypertension audit as a new Quality
Assurance / National Indicator
Approach.
5. Development of CVD Record Book
(merging the current Diabetes and
Hypertension Book) to facilitate
management according to the
Global Cardiovascular Risk.
4. Efficient Clinical
Information System
6. Strengthening the National Diabetes
Registry.
1. Peer Support Diabetes Program
• Rationale:
• Informed, Empowered Patient is one of the crucial component of the Chronic Care Model.
• Patients are more likely to accept advise from their peers or people living with the same condition.
• Successful implementation of a Peer Support Group Program in other countries (e.g. US, Canada) have shown to:
• Help patients understand and in control of their disease better;
• Help patients achieve good disease control; and
• Reduce rates of referral to hospitals due to complications.
• This program has been carried out by few centers using their own template :
• JKN Negeri Sembilan – since 2010, “mentor-mentee system”.
• KK Padang Rengas, Perak & PKD Hulu Langat, Selangor (and Astra Zeneca) – peer as trainers during diabetes education session.
15
1. Peer Support Diabetes Program
• The program module was reviewed twice and now in the final stage of preparation.
• NCD will be responsible for developing the program and training modules, conduct training, implement and monitor the program.
16Program Pembimbing Rakan Diabetes
(PERINTIS) Malaysia
2. Appraisal System for Excellent Diabetes Health Centre • This appraisal system will act as a motivational drive for
healthcare providers to improve quality of Diabetes care at primary care centers in Malaysia.
• A draft proposal has been discussed on 16 December 2014, involving officers from the Family Health Development Division, State Epidemiologist (NCD), Family Medicine Specialists, Medical Officers and Diabetes Educators.
• Will be subjected to the approval of the Deputy Director General of Health (Public Health) for nation-wide implementation.
17
3. Personalised NCD Care
• Definition:
• Personalised care planning empowers individuals (patients with chronic diseases), promotes independence and helps people to be more involved in decisions about their care.
• It centres on listening to individuals, finding out what matters to them and finding out what support they need.
• Rationale:
• Individuals with long term conditions will be at a point be able to take more control over their condition and understand how it affects their lives.
• 70% of individuals with a long term condition say their care has improved as a result of personalised care planning (GP Patient
Survey 2009/10, Department of Health, UK). 18
3. Personalised NCD Care
• The role of the healthcare professional in personalised care planning:
• Supporting patients by taking them through a process of discussion, shared decision making and ongoing support.
• Adopt a different role from the traditional “diagnoser and treater”, to working with people rather than doing to them.
• The current / coming Family Health Team (population-based) and Family Doctor Concept needs to be complemented with empowerment of paramedic esp. Diabetes Educators.
19
3. Personalised NCD Care
• Empowerment of Diabetes Educators (DE):
• There are 328 DEs in the country, 263 of them at the KlinikKesihatan, while 65 are at the hospital.
• Many of them are not able to practice their expertise at the KlinikKesihatan even though they provide NCD services either due to manpower constrain or unavailability of a structured service documents like specific scope of responsibility and Fail Meja to guide them to function as an effective Diabetes Educator.
• Development of Diabetes Educator’s Service Documents:
• First meeting planned for 10 to 11 March 2015.
• Disease Control Division, Family Development Division, State Epidemiologists (NCD), Primary Care Officers, Family Medicine Specialists, Medical Officers and Diabetes Educators. 20
3. Personalised NCD Care
• Menjalankan dan menyelaras aktiviti Pendidikan BersepaduDiabetes secara berstruktur.
• Pengendalian pesakit Diabetes secara individu
• Menyelaras sesi perbincangan penjagaan kes bersepadu (team colaborative care case discussion).
• Menyelaras dan memantau perlaksanaan Program Peer Support for Diabetes.
• Menyelaras dan menjalankan aktiviti intervensi bersepadugangguan toleransi glukosa (IGT)
• Menyelaras aktiviti pendidikan kesihatan umum diabetes.
• Terlibat dalam Program Pencegahan NCD Dalam Komuniti (KOSPEN) 21
4. Hypertension Audit/QA/NIA
• Discussions on developing a Hypertension Audit mechanism as a monitoring tool of quality of Hypertension care at KlinikKesihatan in Malaysia has started since 2013.
• After several meetings between the NCD Sector and Family Health Development Division, it has been agreed that the Hypertension audit will be first piloted at Klinik Kesihatan with Tele-primary Care (TPC) system using TPC data.
• This proposal was approved by the Deputy Director General of Health (Public Health).
• A draft data dictionary and proposed outputs have been provided to TPC Unit of Family Health Development Division.
22
4. Hypertension Audit/QA/NIA
• This initiative has also been considered in the development of TPC-OHCIS (Tele-primary Care - Oral Health Clinical Information System), which will be developed by Syarikat MIMOS Berhad, an agency under MOSTI.
• Few states (Penang, Kelantan) have carried out their own manual Hypertension clinical audit and this needs to be discussed further in view for standardization and pilot audit.
• First meeting planned for 25 to 26 February 2015.
• Disease Control Division, Family Health Development Division, State Epidemiologists (NCD), Primary Care Officers, Family Medicine Specialists, and Medical Officers.
23
5. Cardiovascular Record Book
• There is a need now to start managing Cardiovascular / Diabetes patients holistically using the global cardiovascular risk assessment, instead of by individual risk factor / disease management.
• The current challenge is to develop a suitable CV Risk Calculator for Malaysia.
• Learning trip for officers from the Disease Control Division and Family Health Development Division to the UiTM Primary Care Specialist Clinic on 9 January 2015.
• First meeting held on 19 to 21 January 2015.
• Disease Control Division, Family Development Division, State Epidemiologist (NCD), Primary Care Officers, Family Medicine Specialists, Medical Officers and Diabetes Educators. 24
6. Strengthening the NDR
• The National Diabetes Registry will be improved by reviewing the following documents :
• User Manual, Quality of Diabetes Care at MOH Healthcare Facilities Glycaemic Control 2008.
• SIQ Investigation, Quality of Diabetes Care at MOH Healthcare Facilities Glycaemic Control 2008.
• First meeting was held on 19 to 21 January 2015.
• Disease Control Division, Family Health Development Division, State Epidemiologists (NCD), Primary Care Officers, Family Medicine Specialists, Medical Officers and Diabetes Educators.
25
Other issues…
• Steno Diabetes Centre branch in Malaysia
• MOH focal point: Institut Kesihatan Umum (IKU), under its Director, Dr Tahir Aris
• Komuniti Sihat, Perkasa Negara (KOSPEN) initiative
26
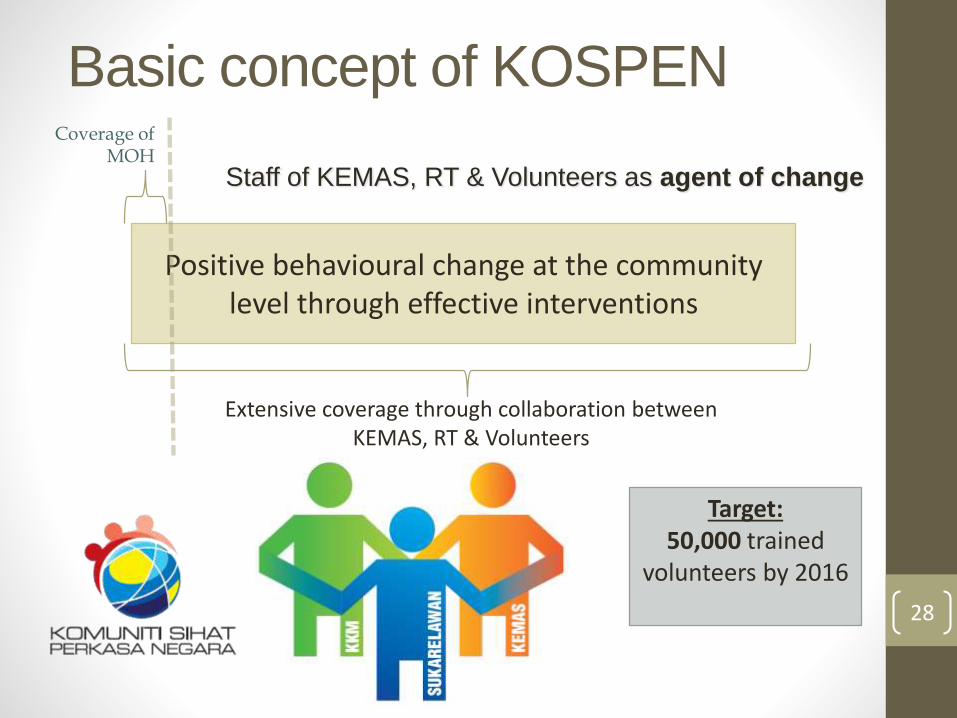
KOmuniti Sihat, PErkasa Negara (KOSPEN): Empowering Communities, Strengthening the Nation
Positive behavioural change at the community level through effective interventions
Coverage of MOH
Extensive coverage through collaboration between KEMAS, RT & Volunteers
Staff of KEMAS, RT & Volunteers as agent of change
Target:50,000 trained
volunteers by 2016
Basic concept of KOSPEN
28
Increasing awareness & knowledge
Health-promoting living environment
Translation of knowledge into sustainable actions
Strategies
1. Healthy eating2. Active living3. Smoke-free4. Weight management5. Early detection of
NCD risk factors
Scope
29
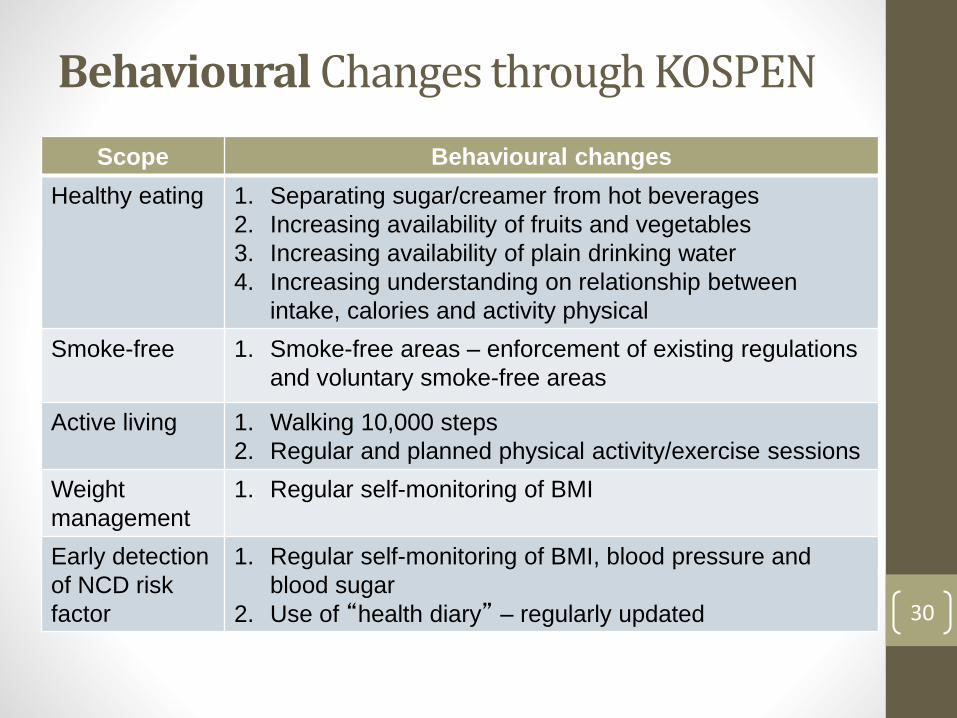
Behavioural Changes through KOSPEN
30
Scope Behavioural changes
Healthy eating 1. Separating sugar/creamer from hot beverages
2. Increasing availability of fruits and vegetables
3. Increasing availability of plain drinking water
4. Increasing understanding on relationship between
intake, calories and activity physical
Smoke-free 1. Smoke-free areas – enforcement of existing regulations
and voluntary smoke-free areas
Active living 1. Walking 10,000 steps
2. Regular and planned physical activity/exercise sessions
Weight
management
1. Regular self-monitoring of BMI
Early detection
of NCD risk
factor
1. Regular self-monitoring of BMI, blood pressure and
blood sugar
2. Use of “health diary” – regularly updated
Environmental Changes through KOSPEN
31
Scope Health-promoting living environment
Healthy eating 1. Community events – separates sugar/creamer from hot
beverages
2. Community events – availability of fruits & vegetables
3. Community events – availability of plain drinking water
4. Healthy stalls or food vendors
Smoke-free 1. Enforcement of smoke-free areas gazetted under
regulations
2. Smoke-free announcement for community events
3. Recognition for voluntary smoke-free homes
Active living 1. Creation of walking tracks with health messages
notices on eating, calories and physical activities
Weight
management
1. Self-monitoring facilities
Early detection
of NCD risk
factor
1. Self-monitoring facilities
32
Challenges for KOSPEN
Lack of perceived priority for health by the community
Health is more of the health sector responsibility
Need more moderation, advocacy, lobbying and sensitisation
Need to motivate health volunteers
Number of active volunteers still needs to be increased
Lack perceived priority for NCD within the health sector.
Large scale implementation
3,300 localities (2014), 6,300 localities (2015) and 10,000 localities (2016)
33
Summary
• In order to achieve the voluntary NCD global targets, we need to prioritise our actions
• NCD prevention
• NCD control / management
• What are the biggest contributors or determinants?
• What factors are within our control? What factors are beyond?