37
NCOA – Physiological Assessment – Part II Chapter 14 (4 th ed.) Pati Cox, RN, BSN, M.Ed.
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | winter-marsh |
| View: | 20 times |
| Download: | 0 times |
NCOA – Physiological Assessment – Part II
Chapter 14 (4th ed.)
Pati Cox, RN, BSN, M.Ed.
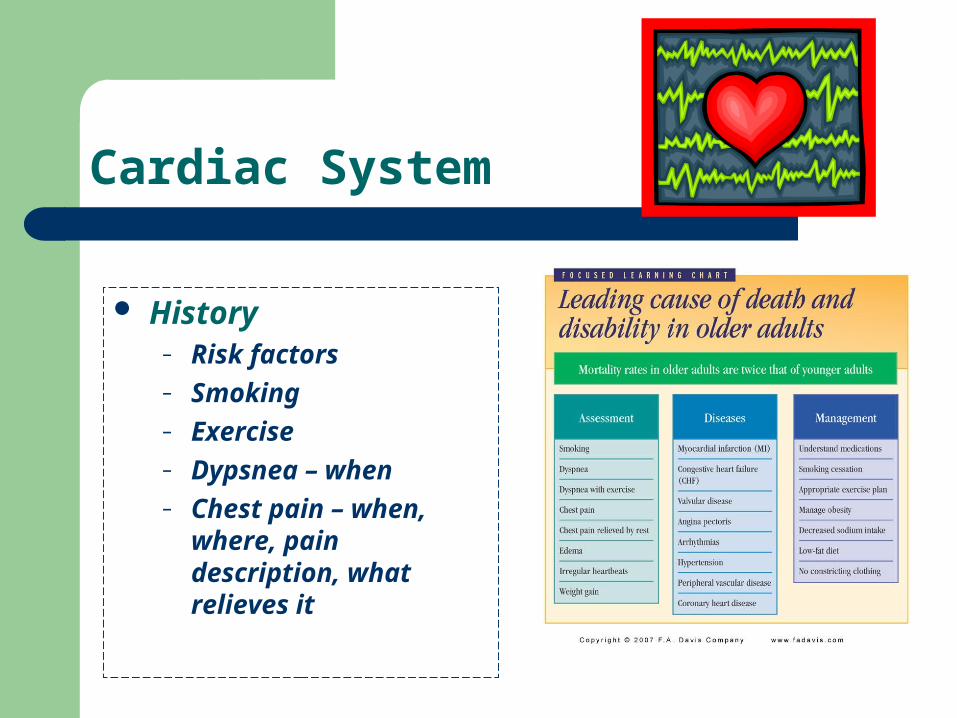
Cardiac System
History– Risk factors– Smoking – Exercise– Dypsnea – when– Chest pain – when,
where, pain description, what relieves it
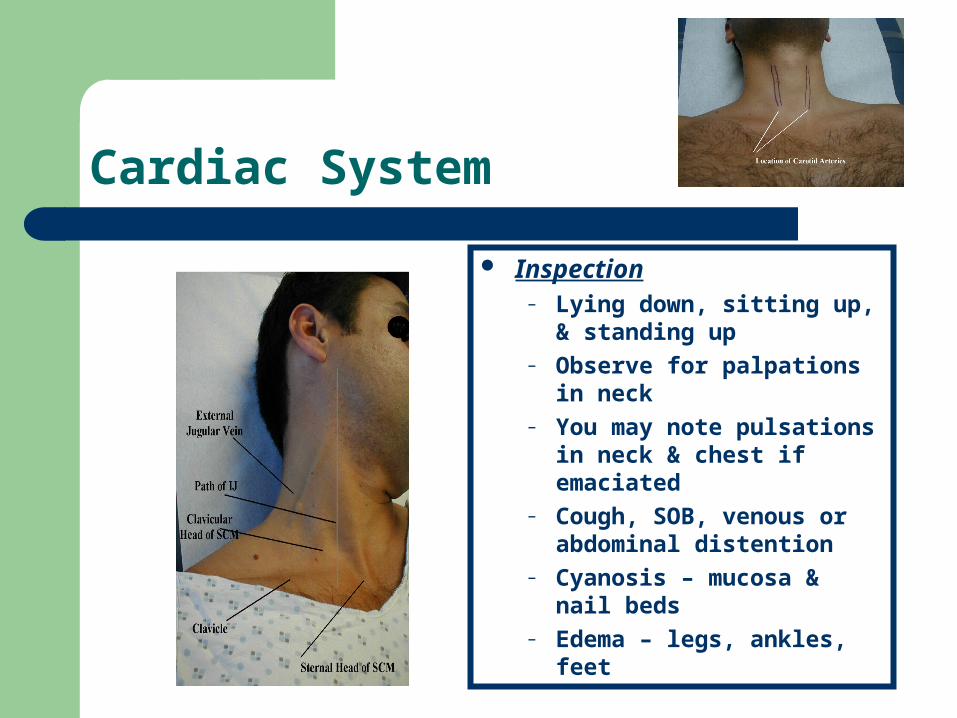
Cardiac System
Inspection– Lying down, sitting up, &
standing up– Observe for palpations in
neck– You may note pulsations in
neck & chest if emaciated– Cough, SOB, venous or
abdominal distention– Cyanosis – mucosa & nail
beds– Edema – legs, ankles, feet
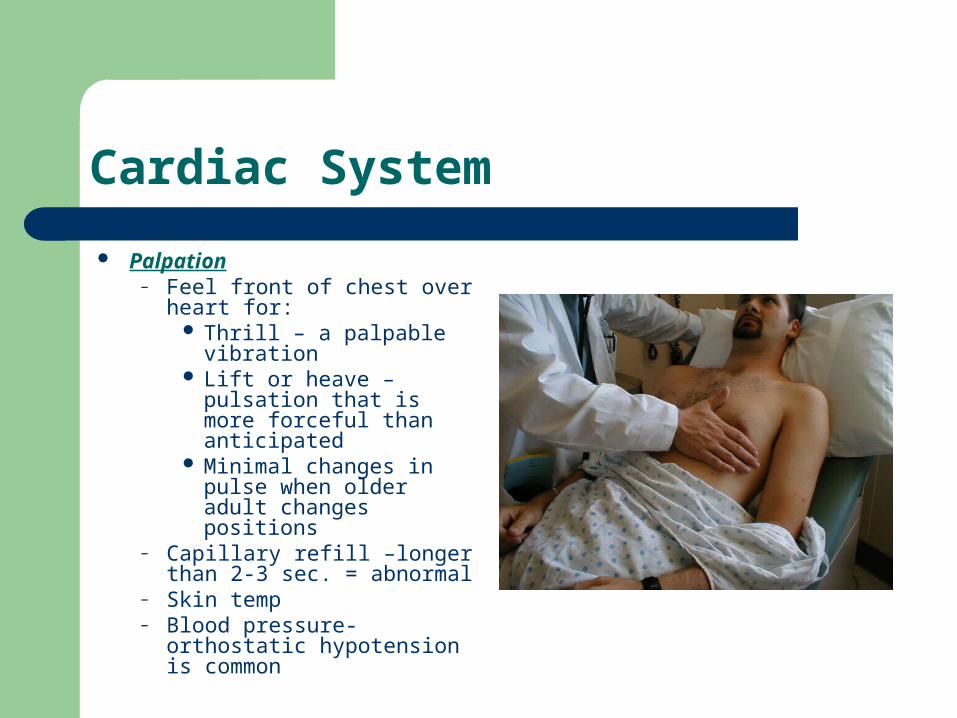
Cardiac System
Palpation– Feel front of chest over
heart for: Thrill – a palpable
vibration Lift or heave – pulsation
that is more forceful than anticipated
Minimal changes in pulse when older adult changes positions
– Capillary refill –longer than 2-3 sec. = abnormal
– Skin temp– Blood pressure-orthostatic
hypotension is common
Cardiac System
Auscultation Assess heart rate
– Typical faster heart rate– Less detectable or distinct– Atrial Fibrillation common– Note irregularities, intensity,
rhythm – REPORT– Lay on Left side if difficult
hearing– Murmur – clicking or humming
sound - REPORT
Respiratory System
History– Dypsnea, Activity or rest? – Cough, dry or productive, color &
consistency– Lung Disease, pneumonia, CHF, anemia– O2 use
Environmental concerns:
Air pollutionTB, TB Skin TestChest x-rayPneumovaxInfluenza Vaccine
Respiratory System
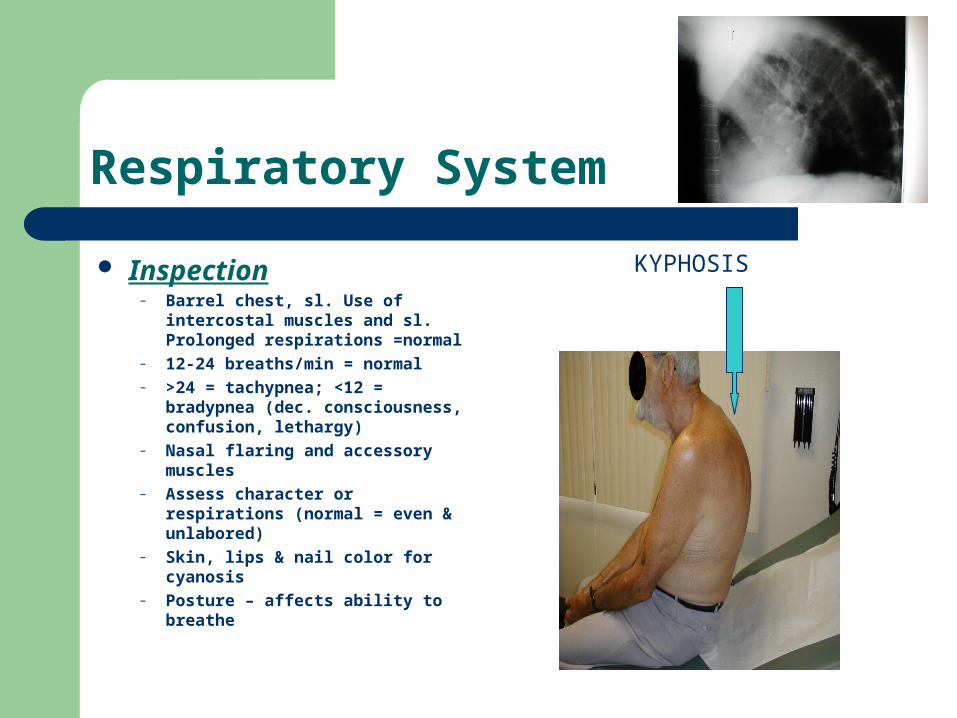
Inspection– Barrel chest, sl. Use of intercostal
muscles and sl. Prolonged respirations =normal
– 12-24 breaths/min = normal– >24 = tachypnea; <12 = bradypnea
(dec. consciousness, confusion, lethargy)
– Nasal flaring and accessory muscles
– Assess character or respirations (normal = even & unlabored)
– Skin, lips & nail color for cyanosis– Posture – affects ability to breathe
KYPHOSIS
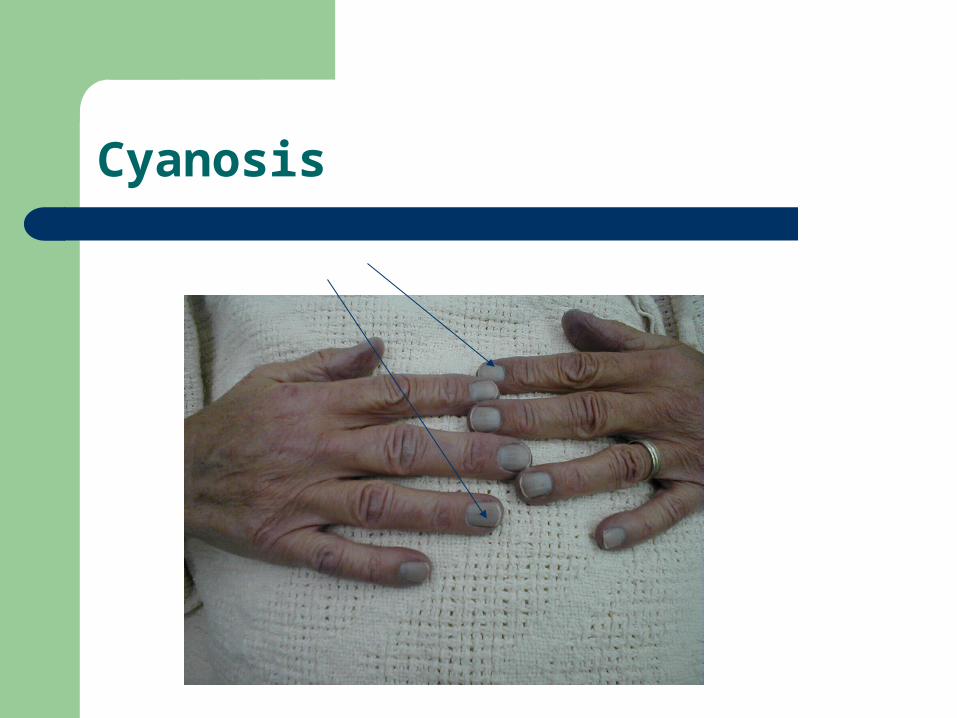
Cyanosis
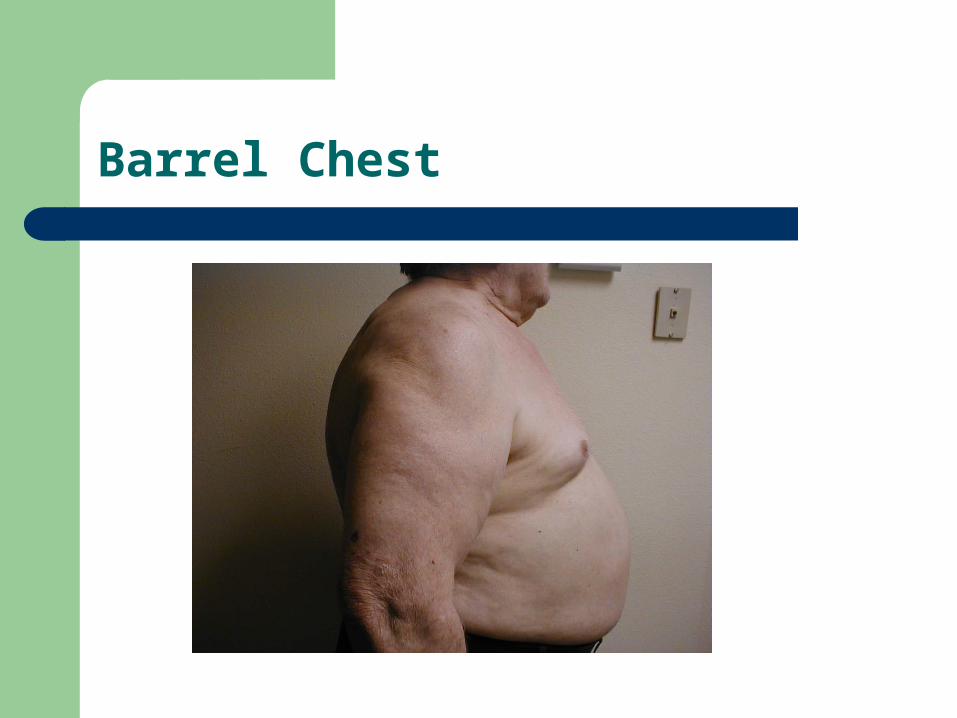
Barrel Chest
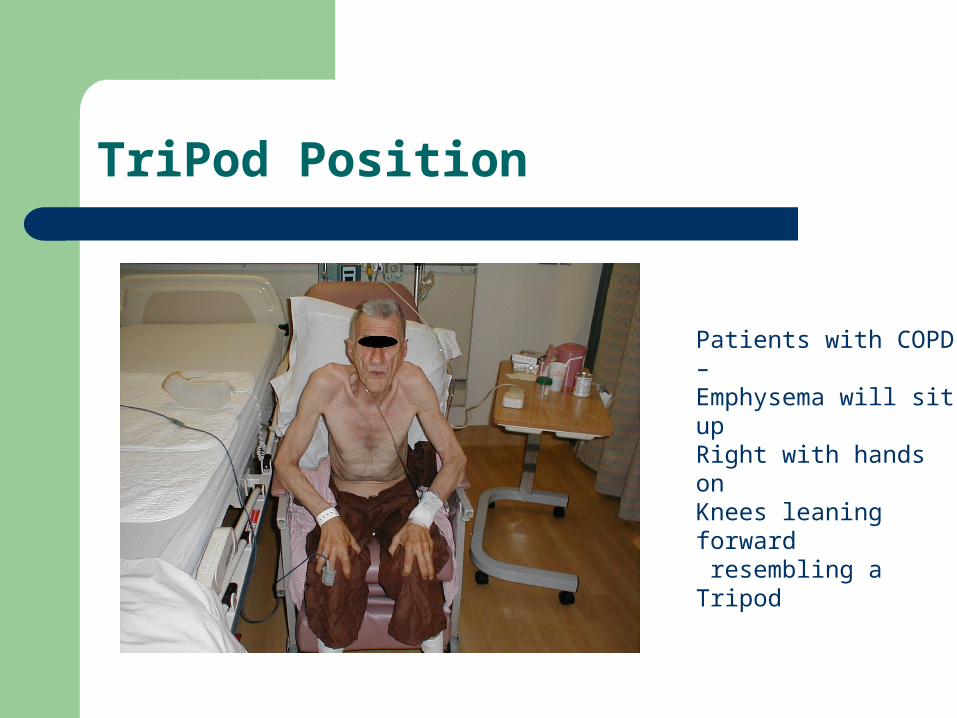
TriPod Position
Patients with COPD –Emphysema will sit upRight with hands onKnees leaning forward resembling aTripod
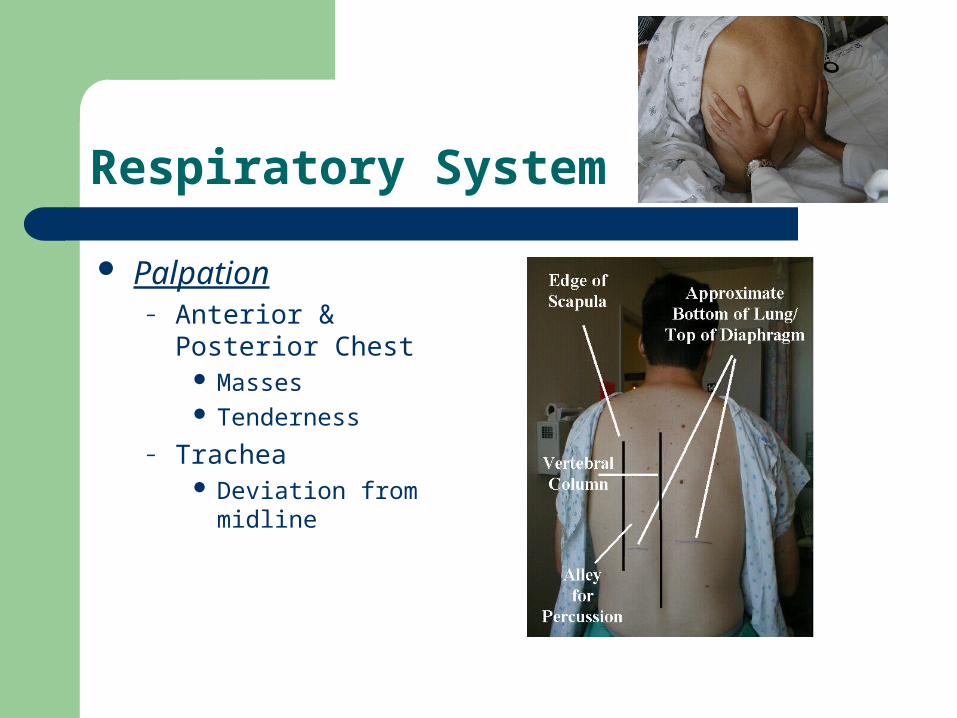
Respiratory System
Palpation– Anterior & Posterior
Chest Masses Tenderness
– Trachea Deviation from midline
Respiratory System
Auscultation– Rem to avoid
hyperventilation; ask to breathe normal in between deep breaths – dizziness
– Should hear softer sounds and diminished sounds in lower bases
– Listen for adventitious sounds
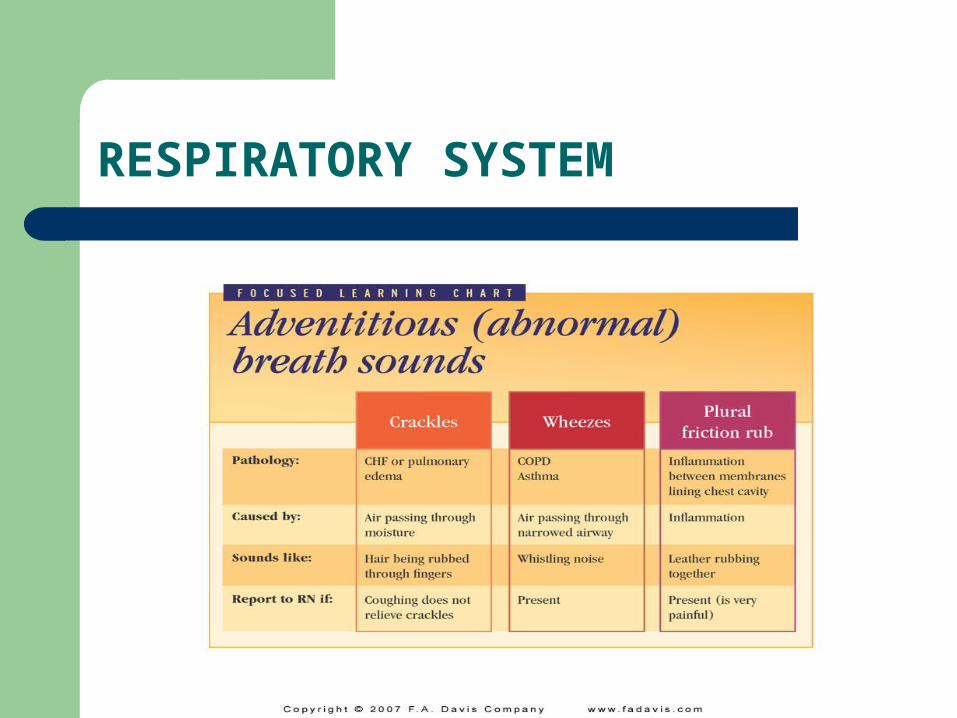
RESPIRATORY SYSTEM
Gastrointestinal System
History– Focus = Nutritional Status, bowel habits, & medications– 24 hour recall of diet– Fluids? (2000-3000 mL per day)– Tolerate diet, fluids?– Fiber intake– Sensations when eating, difficulty swallowing– Injury, infection– Laxative use– Pain – location
RLQ – Appendicitis LLQ – Diverticulosis Tenderness @ base of Xiphoid process – stomach pain, hiatal
hernia, or referred pain from aorta
Gastrointestinal The order of physical examination is:
– Inspection– Auscultation
Need to listen to bowel sounds first before palpation Palpation may elicit pain or a change in bowel sounds – want
older adult relaxed
– Palpation

Gastrointestinal
Gastrointestinal
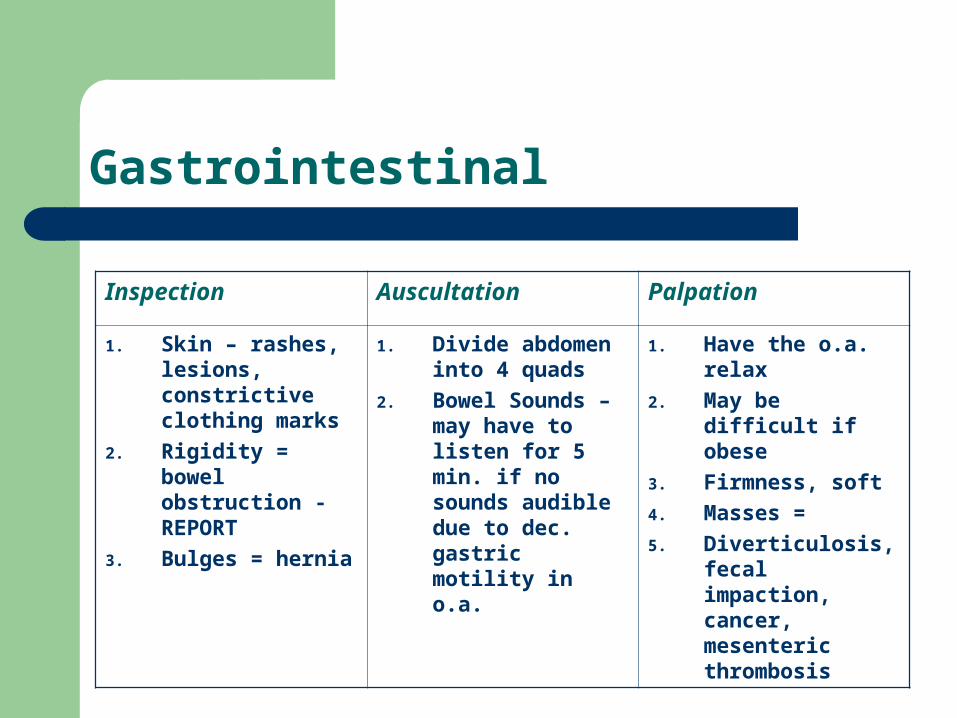
Inspection Auscultation Palpation
1. Skin – rashes, lesions, constrictive clothing marks
2. Rigidity = bowel obstruction - REPORT
3. Bulges = hernia
1. Divide abdomen into 4 quads
2. Bowel Sounds – may have to listen for 5 min. if no sounds audible due to dec. gastric motility in o.a.
1. Have the o.a. relax
2. May be difficult if obese
3. Firmness, soft
4. Masses =
5. Diverticulosis, fecal impaction, cancer, mesenteric thrombosis
Gastrointestinal - Auscultation

Gastrointestinal - Ascites

Gastrointestinal - Hepatomegaly

Gastrointestinal - Gallbladder

Gastrointestinal – Umbilical Hernia
Integumentary System
History– Most important aspect of assessment– Most common complaints
Pruritus Pain Parasthesia Dermatitis
– Sun exposure, environmental allergens, infectious diseases
– Skin care regimen, medications – allergic reactions, soaps, etc
Integumentary System
Inspection Complete in well lit room
– Scalp, skin folds, behind ears, – Fingernails, toenails, genitalia,
buttocks and face– Skin color, odor– Uniformity
Petechiae Ecchymosis Pallor Cyanosis, dusky, gray Jaundice
– Pressure points over bony prominences
– Braden Scale Skin lesions- see text
Palpate– Skin turgor – forehead or
anterior chest– Skin texture– Skin temperature – with back
of hand
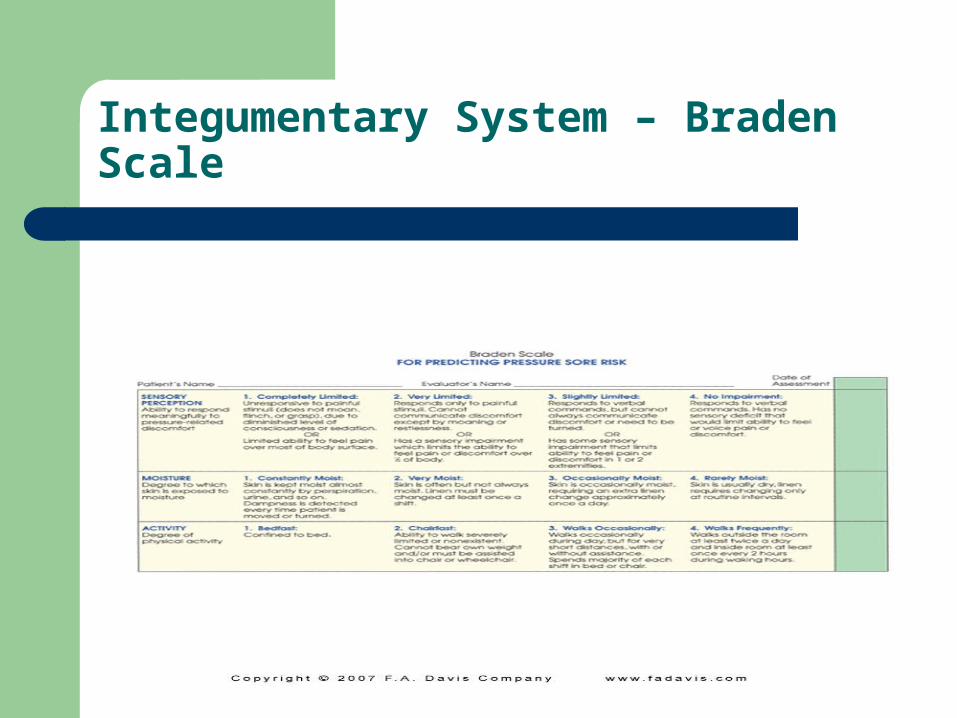
Integumentary System – Braden Scale
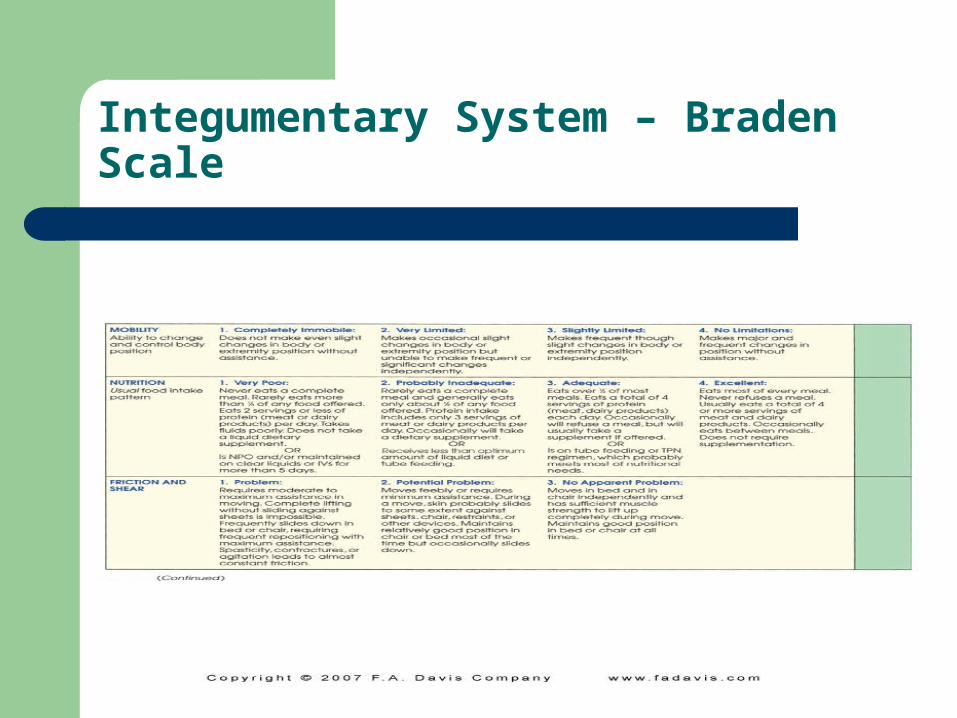
Integumentary System – Braden Scale
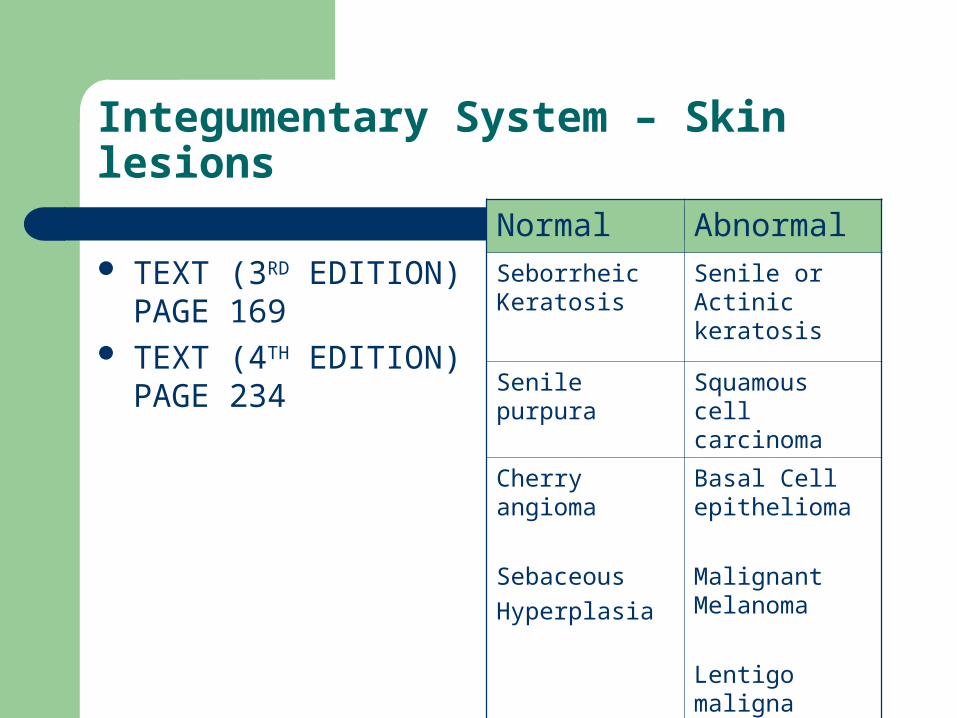
Integumentary System – Skin lesions
TEXT (3RD EDITION) PAGE 169
TEXT (4TH EDITION) PAGE 234
Normal Abnormal
Seborrheic Keratosis
Senile or Actinic keratosis
Senile purpura Squamous cell carcinoma
Cherry angioma
Sebaceous
Hyperplasia
Basal Cell epithelioma
Malignant Melanoma
Lentigo maligna
melanoma
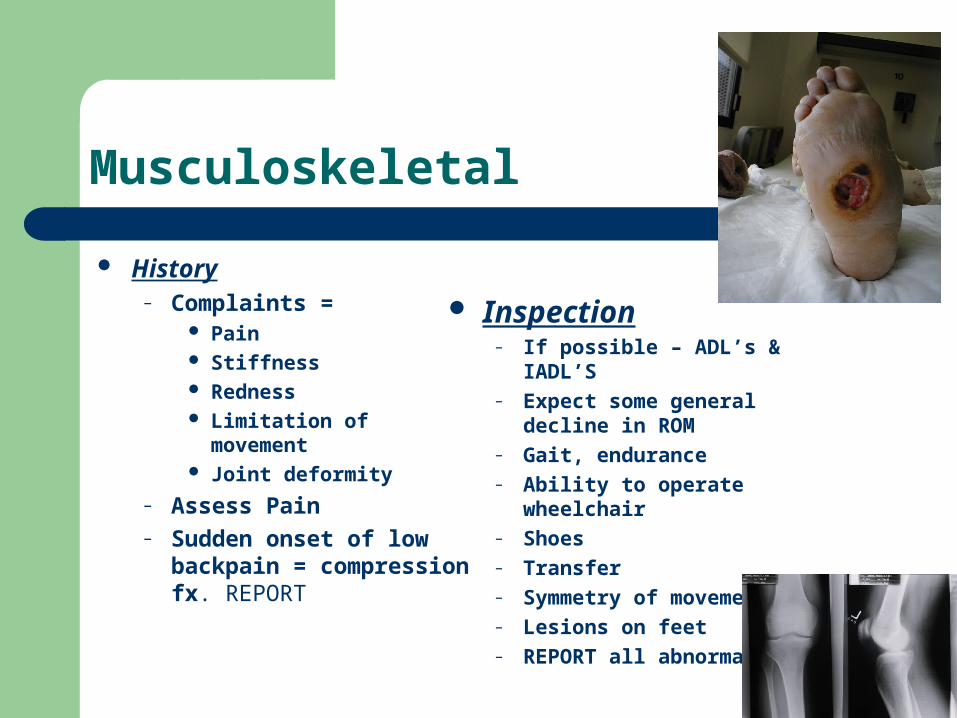
Musculoskeletal
History– Complaints =
Pain Stiffness Redness Limitation of movement Joint deformity
– Assess Pain– Sudden onset of low
backpain = compression fx. REPORT
Inspection– If possible – ADL’s & IADL’S– Expect some general decline
in ROM– Gait, endurance– Ability to operate wheelchair– Shoes– Transfer– Symmetry of movement– Lesions on feet– REPORT all abnormalities
Reproductive - Woman
History– Sexual function– Self breast exam– Breast cancer - Hx– Nipple discharge, pain,
lumps, skin discoloration, change in breast shape
– HRT or other meds such as Digitalis, Thyroid or Antihypertensives
– Pap smears– Vaginal dryness, bleeding
Inspection– External genitalia– Skin or mucous membranes
– lesions,
rashes, discoloration,
hair loss– Inflammation, discharge– Asymmetry
Reproductive - Male
History– BPH (Benign Prostatic
Hypertrophy or Hyperplasia)
– Change in urine stream– Nocturia– Medications
Diuretics, Antihypertensives make BPH worse
– Breast exam
Inspection– External Genitalia– Skin, mucous membranes– Lesions– Rashes– Discoloration– Hair loss– Inflammation– Discharge – Asymmetry– Circumcision
Urinary System
History– Question chief complaint– Most common c/o =
Urgency to void Leakage upon position changes Frequency of urination Voiding small amounts Incontinence – embarrassed
– UTI – most common cause of fever and disorientation in the elderly– Pressure Ulcer formation– Normal urinary & bowel habits– Medical History – children, surgeries, diabetes– Medications – diuretics, antiparkinsonian– Immobility– Dehydration
Urinary System
Inspection– Assess Ua. Amount– Color– Sediment– Incontinence– Pressure ulcers
Palpation– Distention– Masses– Pelvic Discomfort
Functional Assessment
Holistic approach to evaluating the older adult
– Physical– Cognitive– Social
As important as physiological assessment
What the O.A. can (strength) and cannot do (deficit)
Assists in setting realistic goals to maximize functional strengths, compensate for deficits and maintain optimal independence
Functional Assessment
Physical– Individuals current health status– How well he/she performs ADL’s & IADL’s
Cognitive– Individuals memory, judgment, thinking
abilities Social
– Psychosocial approach to determine how the individual interacts with the environment and others
Functional Assessment
Cure is not a goal – focus is to set realistic goals– Maximize functional strengths – Compensate for functional deficits– Achieve and maintain optimal independence in function
Older adult has to many chronic illnesses that are irreversible
Nurses– Monitor for changes– Utilize resources– Validate– Communicate with team members
Functional Assessment
ADL’s– Performed while taking
care of oneself– Bathing– Dressing– Toileting– Feeding– Ambulating & transferring– Continence
Katz Scale –tool utilized to determine overall ability of person
– Page 172 (3RD ED)– Page 238 (4th ED)
IADL’s (Instrumental ADL)– Activities that support
independent living– Telephone– Cook– Shop– Laundry– Manage finances– Take meds– Prepare meals
Lawton’s Scale – tool utilized to determine ability
– Page 173 (3rd ED)– Page 239 (4th ED)
Functional Assessment
Social Function– How older adult interacts with self, environment, &
others– How person functions as a member of the
community– Must consider: culture, socioeconomic status– Self Concept – affects older adult’s ability to
perform self-care activities; psychological intervention may be necessary to improve self concept

















