63
ALYSSA BRZENSKI Neonatal Emergencies
| Date post: | 01-Jan-2016 |
| Category: |
Documents |
| Upload: | rigel-cervantes |
| View: | 53 times |
| Download: | 3 times |

ALYSSA BRZENSKI
Neonatal Emergencies

Overview
Tracheoesphageal FistulasCongenital Diaphragmatic HerniasOmphaloceles and GastroschisisNecrotizing EnterocolitisMyelomeningocele

TEF

Background
TEF/EA associated with 1:2,500-4,000 live births 30% of the neonate are premature Few cases diagnosed prenatally May present after birth with inability to pass an OGT

Background

Co-morbidities


Waterson Classification

Spitz Classification

Pre-repair Bronchoscopy

The Evidence behind the pre-repair Bronch
May change the operative management (changed operative approach in 57% with 31% being crucial changes)
Bronchoscopy can Define the fistula location Determine unusual characteristics of the
fistula(double fistula or trifurcation) Determine presence of tracheobronchitis (surgery
contraindicated) Locate the aortic arch Influence anesthetic management

Thorascopic vs. Open Repair
Reduces Musculocutaneous sequelae 32% of patients have significant musculocutaeous
sequelae 24% with winged scapula 20% asymmetry of chest wall 2/2 atrophic serratus
anterior 18% developed thoracic scoliosis
Better visualizationReduced Pain Post-operatively

Anesthesia for Thorascopic
Rarely need lung isolation as operative lung compressed by CO2 insufflation (5mmHg)
Can be associated with mild desaturation requiring 100% O2 or mild hand ventilation.
Some centers using HFOV for these repairs to minimize the movement of the operative side (MAP 14-24, Hz=10-14, delta P=20-27, FiO2 adjusted to Sat of 92%)
EtCO2 will be falsely low due to compression of the lung and CO2 insufflation.

Patient Position

Anesthetic Considerations
Routine ASA monitors +/- A-lineMaintence of spontaneous ventilation during
induction Classic teaching that paralysis can be given after
fistula ligatedBalanced anesthetic +/- epidural for post-op
pain managementMay have difficulty with hypercapnia or
difficulty ventilating
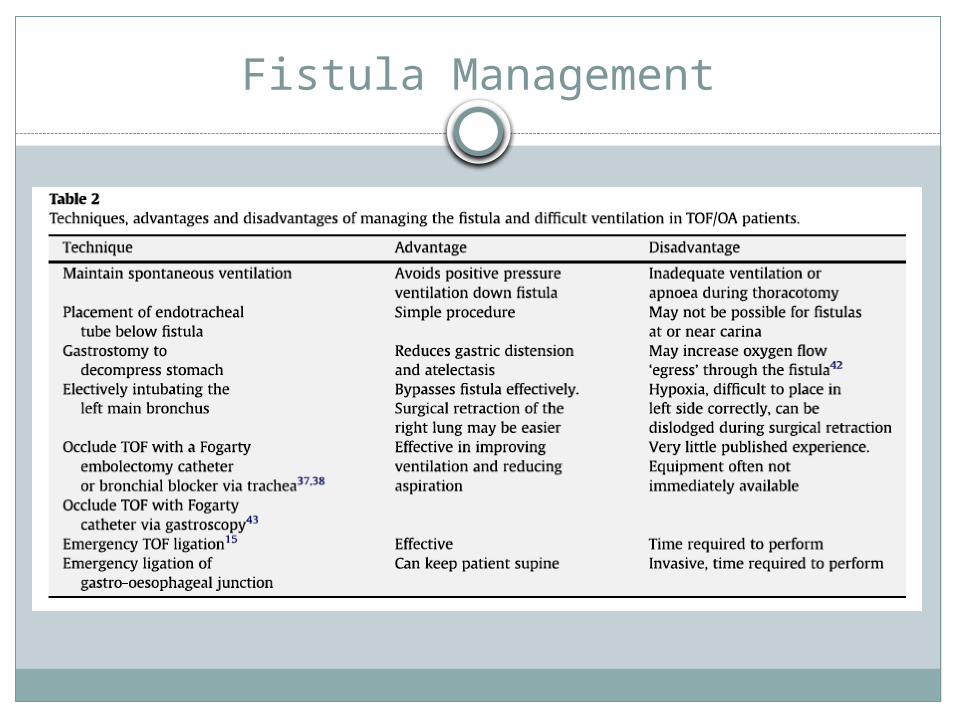
Fistula Management

Extubate or Not?
Must consider pre-op lung disease and other comorbidities
Spontaneous ventilation decreases the stress placed on the suture line
Risk of injury to the repaired fistula with re-intubation

Congenital Diaphragmatic Hernia

Background
1 in 2,500 birthsLocation of the defect
80% left sided 20% right sided 1-2% bilateral
Etiology unknown50-70% post-natal
survival

Co-morbidities

Co-morbidities
Trisomy 13, 18, 21Goldenhar syndromeBeckwith-Wiedemann syndrome
Survival in patients with co-morbidities 15%
Diagnosis
Prenatal diagnosis Ultrasound can detect 50-60% Fetal MRI can further delineate
Postnatal diagnosis Respiratory distress Scaphoid abdomen Distended Chest NGT coiled in the chest

Pathophysiology
Impaired lung development bilaterally with hypoplastic ipsilateral lung Decreased bronchial branches and alveoli Increased muscularization into the intraacinar alveoli Decreased type II pneumocytes
Pulmonary Hypertension and persistent fetal circulation
Hypoxemia, Hypercapnea, and Acidosis

Prenatal ManagementBalloon Tracheal Occlusion

Postnatal Management
Not a surgical emergency!!!!Definitive airway control
Minimize airway pressures to avoid pneumothoraxNGT to decompress the stomachCardiac Echocardiogram to assess pulmonary
HTN

Postnatal Ventilatory Strategy
Gentle ventilation- PIP less than 25cm H20pH> 7.25paCO2<65Preductal Sat>90%
Rescue Ventilatory Strategies iNO HFOV ECMO

When can we operate?
Delay surgery for Physiologic stabilization Improvement in pHTN Hemodynamically stable Minimal vent support
Exact criteria is insitution-dependentSurgery can occur on the HFOV or on ECMO

Anesthesia for CDH Repiars
Standard ASA monitors and A-lineHave adequate access, blood, iNO and
inotropes availableMinimize peak inspiratory pressuresAvoid nitrous oxidePeak airway pressures may increase from
increased abdominal pressure following repair
DO NOT try to expand the contralateral lung after the repair

Intraoperative Complications
Exacerbation of Pulmonary HTNPTX on contralateral lungHemorrhageHypothermia
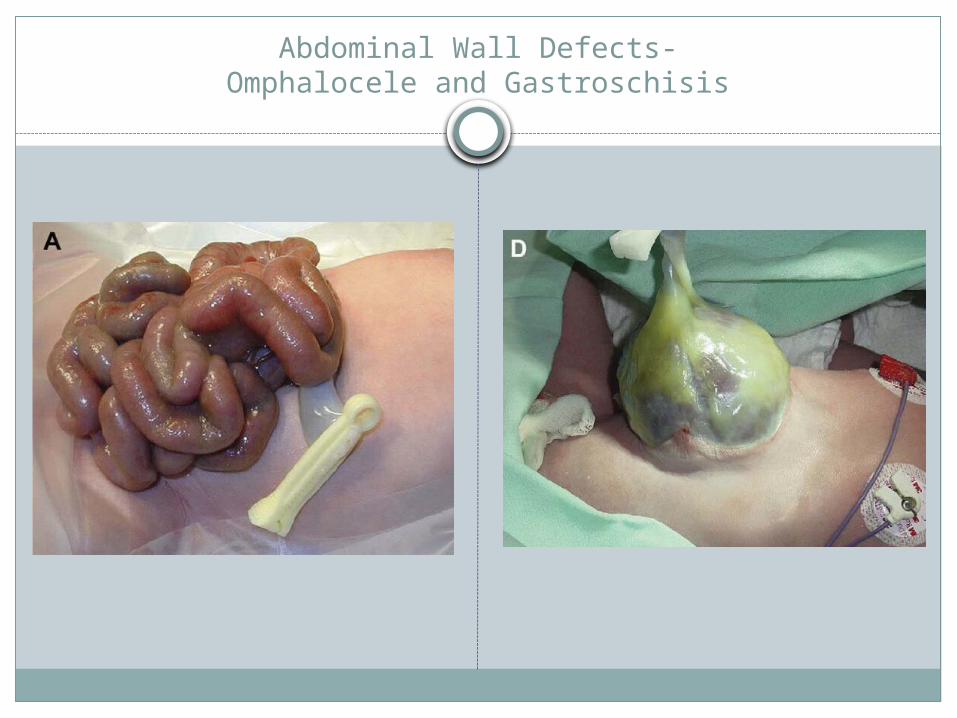
Abdominal Wall Defects-Omphalocele and Gastroschisis
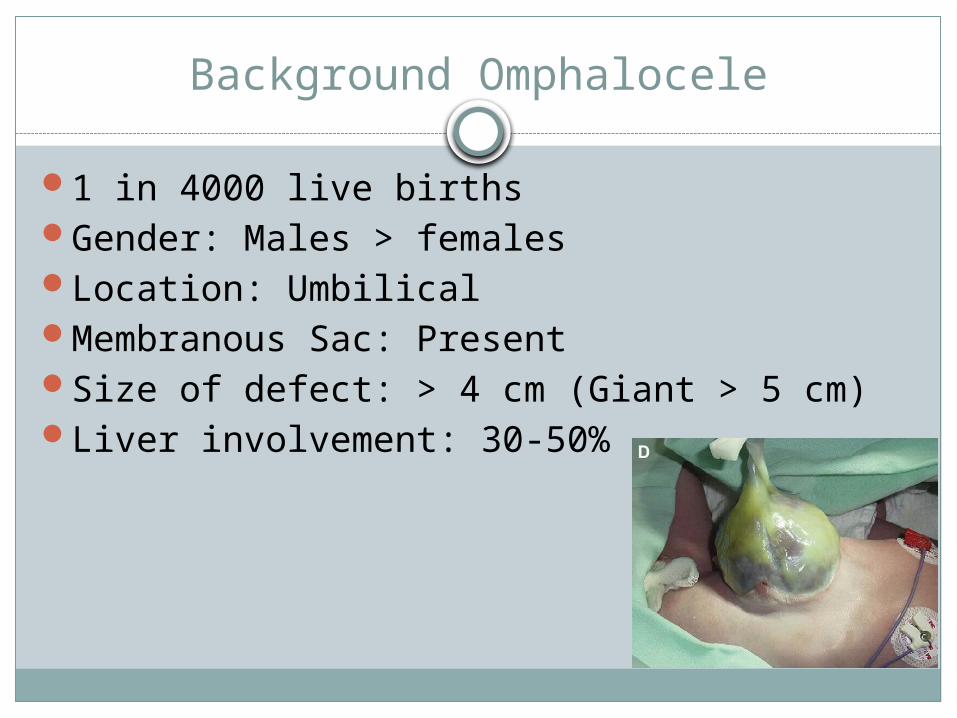
Background Omphalocele
1 in 4000 live birthsGender: Males > femalesLocation: UmbilicalMembranous Sac: PresentSize of defect: > 4 cm (Giant > 5 cm)Liver involvement: 30-50%

Co-morbidities- Omphalocele
50-75% of patients will have other anomalies Cardiovascular (30-50%)- tetralogy of fallot Gastrointestinal(25%)- Genitourinary (25%)- cloacal extrophy Beckwith-Wiedemann syndrome (10%) Chromosomal abnormalities- Trisomy 13, 18, 21
Multiple anomalies more common in minor omphaloceles

Background- Gastroschisis
1 in 4000 birthsGenders: Male = FemaleLocation: Right of the umbilicusMembranous Sac: AbsentSize of defect: 2-5 cmLiver involvement: Rare

Co-morbidities-- Gastroschisis
Low association with other anomalies (10-20%) Gastrointestinal– bowel atresia Genitourinary– cyrptorchidism Chromosomal anomalies: Rare Prematurity common

Prenatal Care
All children with omphalocele or gastroschisis should be born at a hospital with a NICU
Vaginal or C-Section are both acceptable birth plans

Surgical Closure
Omphalocele has a membranous covering– emergent surgery not necessary Unless the membranous covering is ruptured
Gastroschisis does not have a membranous covering- Primary Closure vs Staged Closure

Staged Closure– Spring Loaded Silo

Preoperative Considerations
Optimize the fluid status– Correct hypoglycemiaMaintain euthermiaCover mucosal surfaces with plastic wrapNGT decompressionLabsType and Cross+/- ECHO

Anesthetic Considerations
Standard ASA monitorsAdequate IV accessAvoid nitrous oxideBalanced anesthetic technique– most babies
will remain intubatedFluid, fluid, fluid

Abdominal Compartment Syndrome
Impaired ventilationDecreased preload and hypotensionLower limb venous congestionArterial compression
Decreased renal perfusion and oliguria Decreased perfusion to the lower extremities and
bowelsMonitor the peak airway pressures during
closure of the fascia!!!!

Necrotizing Entercolitis

Background
Occurs in 1-5 of every 1000 live birthsMost common in premature and ELBW
neonates 11.5% of neonates weighing 401-750g will develop
High mortality (15-30%)

Term babies
Unusual in term neonatesFirst 1-3 days of lifeOccurs before feedings beginAssociations
Perinatal asphyxia Congenital Heart Disease Respiratory Distress

Risk Factors
PrematurityEnteral FeedsHyperosmolar formulaBacterial infectionsUmbilical arterial catheters

Pathophysiology
Reduced Mesenteric Blood Flow
Mucosal Ischemia
Intestinal Mucosal Injury

Pathophysiology

What else is affected?
Cardiovascular Hypotension
Metabolic Hyperglycemia Metabolic Acidosis
Hematologic Thrombocytopenia Coagulopathy Anemia
Renal


Treatment
Prevention Feed with breast milk
Medical management Stop feeds Optimize hemodynamics and treat with antibiotics
Peritoneal drainSurgical exploration

Intraoperative Management
Standard ASA monitors plus A-line Adequate IV accessNarcotic based anestheticLarge volume fluid resuscitation Have pRBC, FFP and Platelets availableGlucose sourceKeep the baby warm

Myelomeningocele
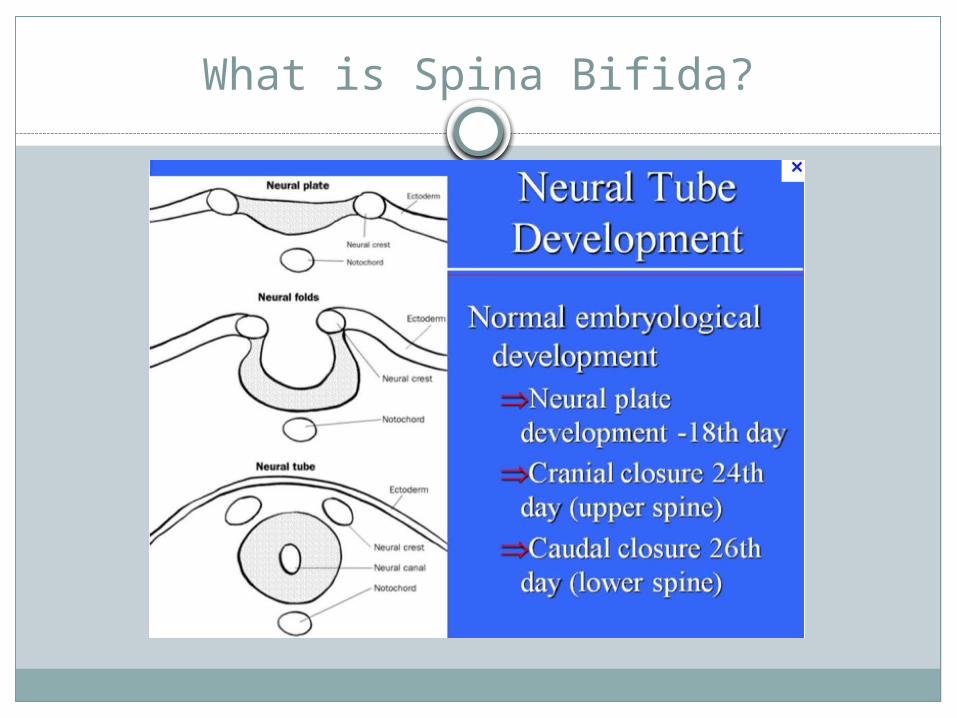
What is Spina Bifida?

Varying Neural Tube Defects

Spina Bifida

Basics of MMC
3.4:10,000 birthsRelated to low folate levels, anticonvulsants
(carbamazepine, valproic acid)Previous child with same partner is a risk
factor
Co-morbidities
Sensory motor deficitsBowel and Bladder IncontinenceArnold Chiari Type II
Caudal displacement of cerebellar vermis, fourth ventricle, and lower brainstem
HydrocephalusCognitive delay
Lower risk if no VP Shunt needed

Co-morbidities

Latex Allergies
All patients with MMC are labeled as latex allergic
High rates due to recurrent procedures including urinary catheterization
Cross reaction to avocados, banana, passion fruit, kiwi, tomato

Management of Myelomeningocele Study


Post-natal MMC Repair
Infants repaired early after birthMust be cautious to not injury the neural
tissue during moving or intubationRoutine ASA monitorsProne position for repairMay or may not receive VP Shunt at the same
timeTypically remain intubated as infant should
not lie supine for the first day

VP Shunts have Complications

















