6/9/14 1 + Neonatal Fever Benjamin B. Constance, MD, FAWM + Objectives Define who is at risk for SBI Clarify risk stratification Provide treatment guidelines Bust some myths + Based on… + Case – what do you want to know? 20 day old male temp 38°C + History Birth history Past medical history Symptom development Immunization status Nutrition source Sick exposures Medications used Maternal HIV / HSV Physical Exam Rectal temperature Full vital signs Hydration status Head to toe exam Complete skin exam Repeat exams Observe behavior Observe feeding + Case 20 day old male temp 38°C X39 week NSVD GBS and HSV negative mother Feeding 3oz q4h, wet diapers Normal physical exam
n Perinatally acquired: GBS, E coli, S pneumoniae, S aureus, L monocytogenes, HSV
n Sepsis Evaluation: CBC, BCx, UA, UCx, CSF cell count, glucose, protein and culture, +/- CXR, stool cell count
+ CAUTION!!!
n SBI can present with hypothermia (<36°C)
n Difficulty with thermoregulation
n Don’t miss low core temperature!
n Consider this same as fever
+ Identifying Sick Patients n Somnolent
n Tachycardia
n Hypotension
n Capillary refill >3 seconds
n Pale, cool skin
n Diaphoresis
n Respiratory distress
n Decreased urine output
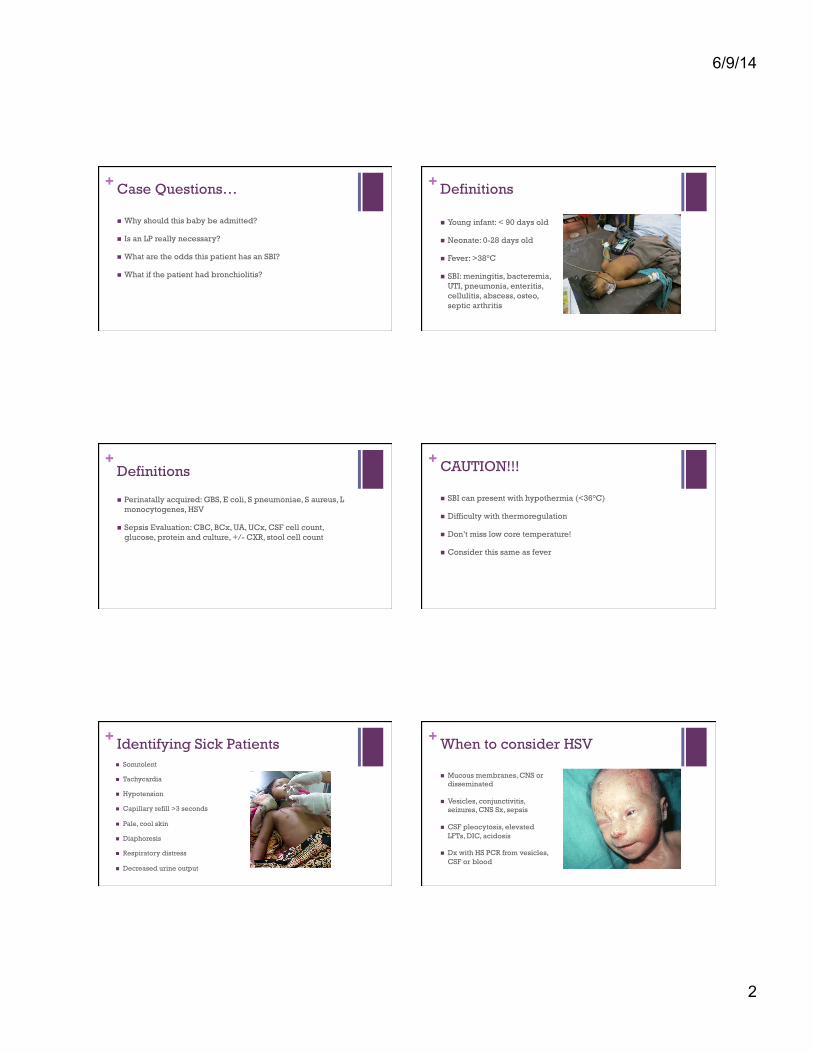
+ When to consider HSV
n Mucous membranes, CNS or disseminated
n Vesicles, conjunctivitis, seizures, CNS Sx, sepsis
n CSF pleocytosis, elevated LFTs, DIC, acidosis
n Dx with HS PCR from vesicles, CSF or blood
6/9/14
3
+ Neonatal HSV and Status Pediatric Immunity
n Little innate immunity n Protection from maternal breast milk n Unable to compartmentalize infections n Present with vague symptoms n Rapidly deteriorate into septic shock
0 - 28 days 29 - 56 days 57-89 days
Pediatric Immunity
n First primary immunizations at 2 months n Regain weight post birth n Protection from maternal breast milk n More resilient n Still difficulty compartmentalizing infections
0 - 28 days 29 - 56 days 57-89 days
Pediatric Immunity
n First primary immunizations at 2 months n Protection from maternal breast milk n More resilient n Starting to develop innate immunity
0 - 28 days 29 - 56 days 57-89 days
+ General Resuscitation n Assess airway, breathing,
circulation
n IV / IO access
n IV fluids 20-30 ml/kg
n Fever control
n Oxygen
n Monitor (if available)
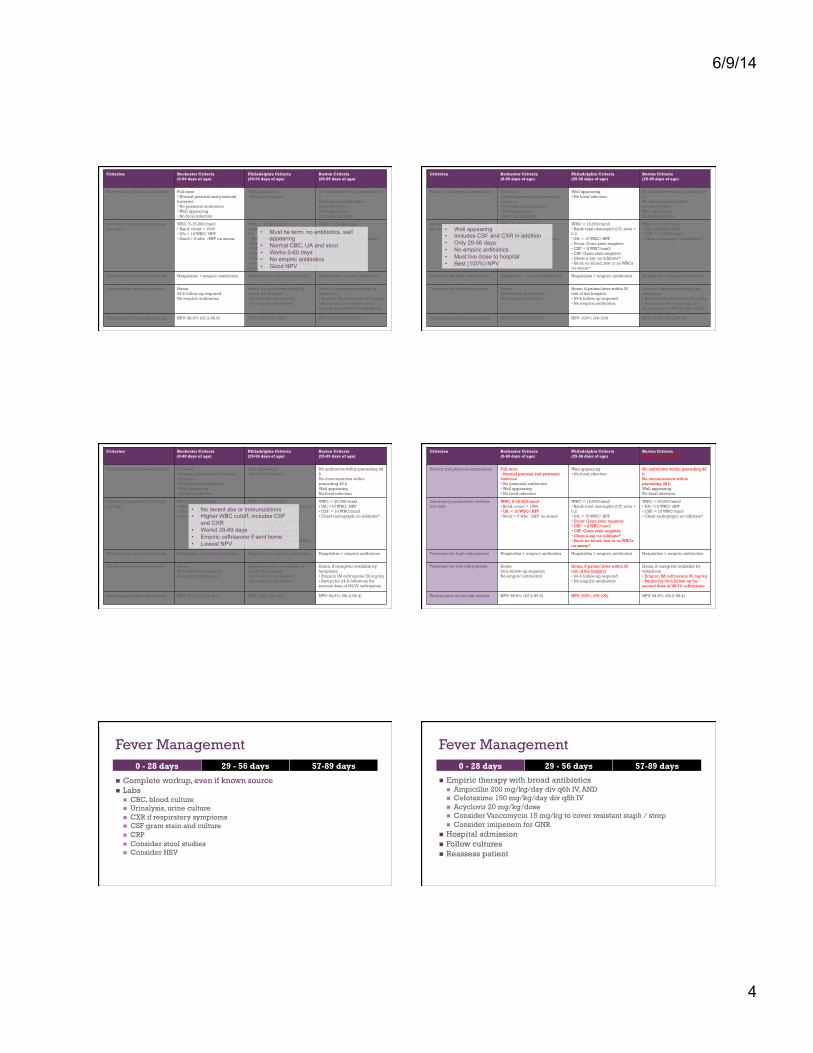
Criterion
Rochester Criteria (0-60 days of age)
Philadelphia Criteria (29-56 days of age)
Boston Criteria8 (28-89 days of age)
History and physical examination
Full-term • Normal prenatal and postnatal histories • No postnatal antibiotics • Well appearing • No focal infection
Well appearing • No focal infection
No antibiotics within preceding 48 h No immunizations within preceding 48 h Well appearing No focal infection
n CBC, blood culture n Urinalysis, urine culture n CXR if respiratory symptoms n CSF gram stain and culture n CRP n Consider stool studies n Consider HSV
0 - 28 days 29 - 56 days 57-89 days
Fever Management
n Empiric therapy with broad antibiotics n Ampicillin 200 mg/kg/day div q6h IV, AND n Cefotaxime 150 mg/kg/day div q8h IV n Acyclovir 20 mg/kg/dose n Consider Vancomycin 15 mg/kg to cover resistant staph / strep n Consider imipenem for GNR
n Hospital admission n Follow cultures n Reassess patient
0 - 28 days 29 - 56 days 57-89 days
6/9/14
5
Fever Management
n Complete workup, even if known source n Labs
n CBC, blood culture n Urinalysis, urine culture n CXR if respiratory symptoms n CSF gram stain and culture n CRP n Consider HSV
0 - 28 days 29 - 56 days 57-89 days
Fever Management 0 - 28 days 29 - 56 days 57-89 days
All Tests Normal
Yes
No
§ Follow-up in 24 hours § Consider ceftriaxone if LP done § Admit for poor social situation § Only discharge if well appearing
§ Perform LP if not already § Ceftriaxone 50 mg/kg § Consider acyclovir § Consider vancomycin § Admit to hospital
Fever Management
n Well appearing is low risk n Typically 1 dose PCV (ê sepsis risk) n Routine urine testing n Consider blood and CSF (Boston) n Discharge with 24h follow up if well appearing
0 - 28 days 29 - 56 days 57-89 days
Fever Management
n Evaluate for source, or occult infection n UTI à UA n Bacteremia à CBC, blood cultures n Pneumonia à chest x-ray n Meningitis à consider CSF if elevated serum WBC
n Treat specific sources of infection n If normal workup, reassess in 48 hours n Bronchiolitis? à still check UA and culture n Ill appearing à admit + full sepsis workup + ceftriaxone
0 - 28 days 29 - 56 days 57-89 days
+Testing
n Enterovirus PCR in summer months (dec hosp stay and antibiotic use)
n CXR only if having resp sx <12wks (Crain et al 2 of 148 abnormal cxr)
n Sool studies only based on Sx, not routinely helpful
+What about RSV?
n Stud: <56 days 1,248 infants, 269 RSV pos
n SBI in RSV+ 7% vs RSV- 12.5% (still large amount) [Lavine et al]
n Given high risk of SBI in <28 days, full workup should be done despite flu or RSV
6/9/14
6
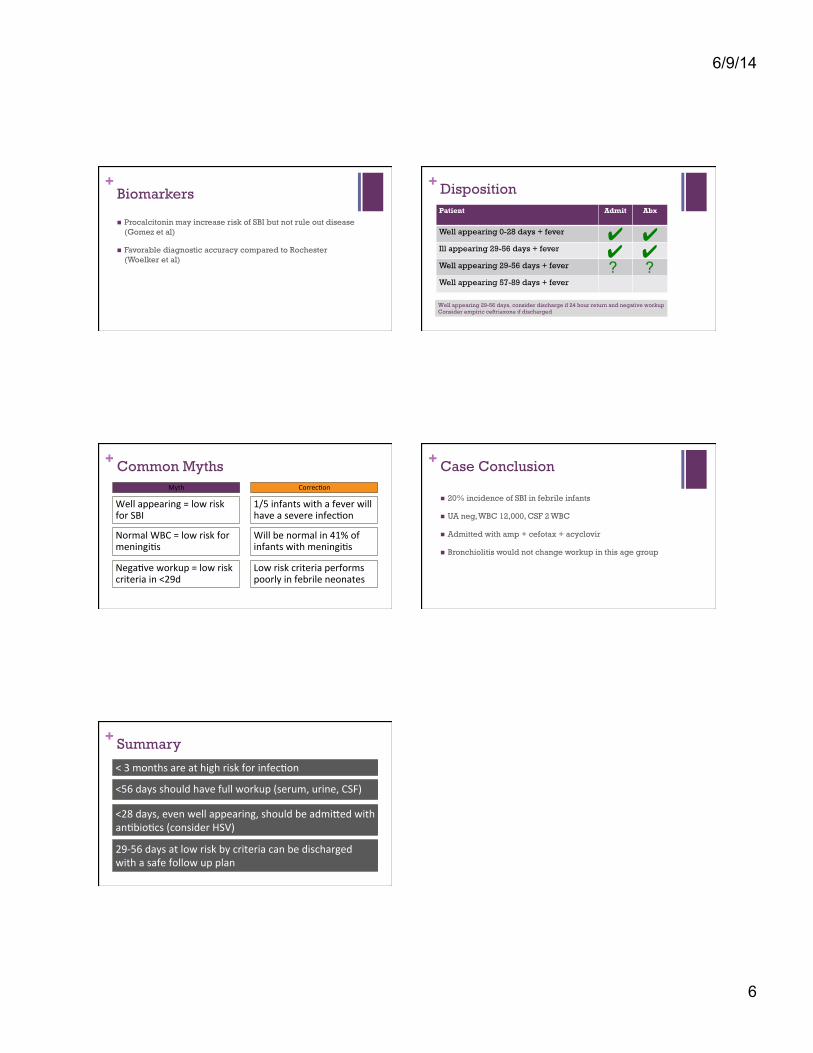
+Biomarkers
n Procalcitonin may increase risk of SBI but not rule out disease (Gomez et al)
n Favorable diagnostic accuracy compared to Rochester (Woelker et al)
+ Disposition Patient Admit Abx
Well appearing 0-28 days + fever
Ill appearing 29-56 days + fever
Well appearing 29-56 days + fever
Well appearing 57-89 days + fever
✔ ✔ ?
✔ ✔ ?
Well appearing 29-56 days, consider discharge if 24 hour return and negative workup Consider empiric ceftriaxone if discharged
+ Common Myths
Well appearing = low risk for SBI
1/5 infants with a fever will have a severe infec;on
Normal WBC = low risk for meningi;s
Will be normal in 41% of infants with meningi;s
Nega;ve workup = low risk criteria in <29d
Low risk criteria performs poorly in febrile neonates
Myth Correc;on
+ Case Conclusion
n 20% incidence of SBI in febrile infants
n UA neg, WBC 12,000, CSF 2 WBC
n Admitted with amp + cefotax + acyclovir
n Bronchiolitis would not change workup in this age group
+ Summary
< 3 months are at high risk for infec;on
<56 days should have full workup (serum, urine, CSF)
<28 days, even well appearing, should be admiQed with an;bio;cs (consider HSV)
29-‐56 days at low risk by criteria can be discharged with a safe follow up plan