Neonatal Renal Review Carol A. Botwinski, EdD, ARNP, NNP-BC Associate Professor of Nursing University of Florida, Tampa, FL The speaker has signed a disclosure form and indicated she has no significant financial interest or relationship with the companies or the manufacturer(s) of any commercial product and/or service that will be discussed as part of this presentation. Session Summary Homeostasis of the newborn is dependent upon a functioning renal system. The immature renal system of the newborn responds slowly and erratically to physiologic changes and demands that are placed on it. Knowledge of renal physiology and embryological development is essential in caring for these newborns, as renal disease, specifically renal failure, is common in ill neonates. Acute renal failure (ARF) in the neonatal period has been recognized with increasing frequency and may occur in as many as 8% of infants in neonatal intensive care units. This lecture presents a practical overview of ARF in the newborn, reviewing practical considerations regarding diagnosis, recognition, and management of the infant with acute renal failure to help prepare the participant for certification exams. Session Objectives Upon completion of this presentation, the participant will be able to: differentiate between pre-renal, intrinsic, and post-renal causes of renal injury in the newborn; discuss the differences in neonatal vs. adult renal function; indicate the practical laboratory/radiology tests used to evaluate renal injury; discuss the evaluation and management of the newborn with renal injury. Test Questions 1. Nephrogenesis is complete by _______ weeks EGA. a. 30 b. 32 c. 34 d. 36 2. Prostaglandins produced by the kidneys have (a) ____________ effect on renal vascular system. a. vasoconstrictor b. vasodilation c. synergistic d. no B15 FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW B15: NEONATAL RENAL REVIEW Page 1 of 13
Transcript
Neonatal Renal Review Carol A. Botwinski, EdD, ARNP, NNP-BC Associate Professor of Nursing University of Florida, Tampa, FL
The speaker has signed a disclosure form and indicated she has no significant financial interest or relationship with the companies or the manufacturer(s) of any commercial product and/or service that will be discussed as part of this presentation.
Session Summary
Homeostasis of the newborn is dependent upon a functioning renal system. The immature renal system of the newborn responds slowly and erratically to physiologic changes and demands that are placed on it. Knowledge of renal physiology and embryological development is essential in caring for these newborns, as renal disease, specifically renal failure, is common in ill neonates. Acute renal failure (ARF) in the neonatal period has been recognized with increasing frequency and may occur in as many as 8% of infants in neonatal intensive care units. This lecture presents a practical overview of ARF in the newborn, reviewing practical considerations regarding diagnosis, recognition, and management of the infant with acute renal failure to help prepare the participant for certification exams.
Session Objectives
Upon completion of this presentation, the participant will be able to:
differentiate between pre-renal, intrinsic, and post-renal causes of renal injury in the newborn;
discuss the differences in neonatal vs. adult renal function;
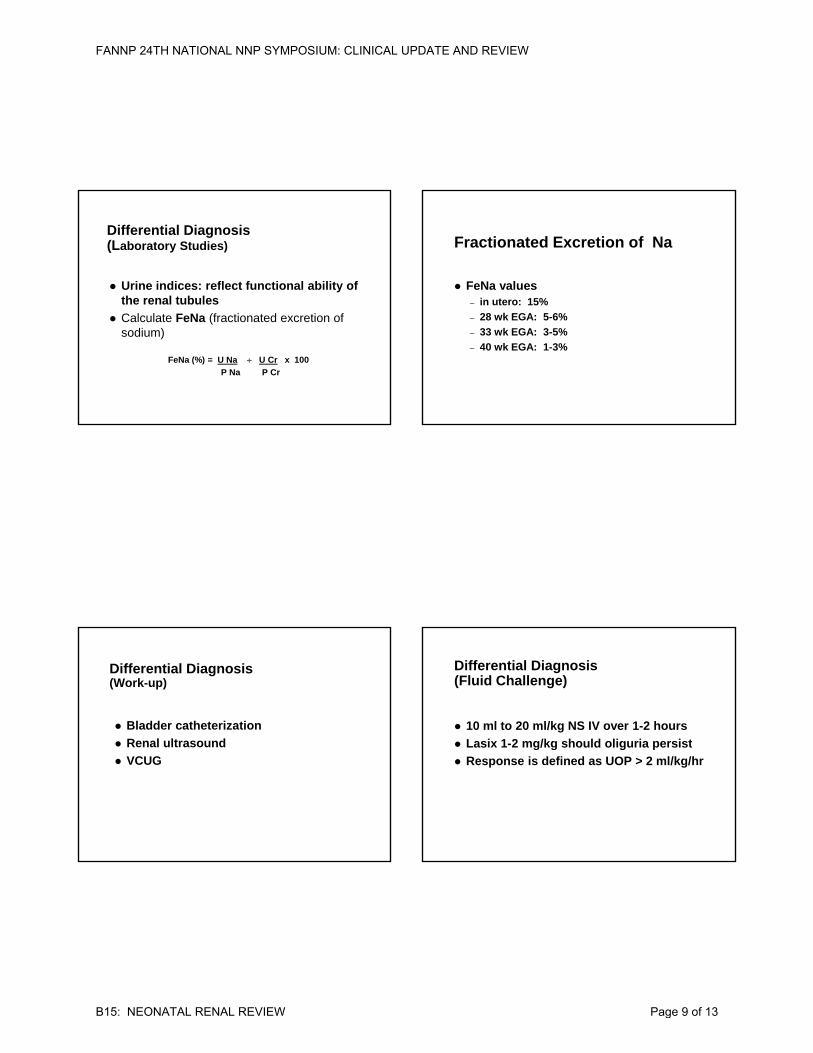
indicate the practical laboratory/radiology tests used to evaluate renal injury;
discuss the evaluation and management of the newborn with renal injury.
Test Questions
1. Nephrogenesis is complete by _______ weeks EGA.
a. 30 b. 32 c. 34 d. 36
2. Prostaglandins produced by the kidneys have (a) ____________ effect on renal vascular system.
a. vasoconstrictor b. vasodilation c. synergistic d. no
B15 FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
B15: NEONATAL RENAL REVIEW Page 1 of 13
3. Newborns with spina bifidia are at risk for _________:
a. intrinsic renal failure b. post-renal failure c. pre-renal failure d. transcellular failure
4. The most common risk factor for renal failure in the newborn period is:
a. placental abruption b. Apgar c. prematurity d. neonatal sepsis
References
Abitbol, C., Bauer, C., Montane, B., et al. (2003). Long-term follow-up of extremely low birth weight infants with neonatal renal failure. Pediatric Nephrology, 18: 887-893.
Cataldi, L., Leone, R., DeMitri, B., et al. (2005). Potential risk factors for the development of acute renal failure in preterm newborn infants: A case-control study. Archives of Disease in Childhood, Fetal and Neonatal Edition, 90: 514-519.
Chua, A. & Sarwal, M. (2005). Acute renal failure and management in the neonate. NeoReviews, 6: e369-376.
Cuzzolin, L., Fanos, V., Pinna, B., et al. (2006). Postnatal renal function in preterm newborns: A role of diseases, drugs and therapeutic interventions. Pediatric Nephrology, 21: 931-938.
Gouyon, J. & Guignard, J. (2000). Management of acute renal failure in newborns. Pediatric Nephrology, 14: 1037-1044.
Kelly, L. & Seri, I. (2005). Renal developmental physiology: Relevance to clinical care. NeoReviews, 9(4): e150-e161.
Lee, M., Chua, A. & Yorgin, P. (2005). Neonatal peritoneal dialysis. NeoReviews, 6: e384-e391.
Lunn, A., Shaheen, I. & Watson, A. (2006). Acute renal insufficiency in the neonatal intensive care unit. Archives of Disease in Childhood, Fetal and Neonatal Edition, 91: F388-F390.
Marks, S., Masscotte, P., Steele, B., et al. (2005). Neonatal renal venous thrombosis: Clinical outcomes and prevalence of prothrombotic disorders. Journal of Pediatrics, 146: 811-816.
Seri, I., Evans, J. & Tulassay, T. (1998). Renal insufficiency and acute renal failure. In H.W. Taeusch, R. Ballard (Eds.), Avery’s diseases of the newborn (8th ed., pp. 1158-1170). Philadelphia, PA: WB Saunders Co.
Swinford, R., Bonilla-Felix, M., Cerda, R. & Portman, R. (2006). Neonatal nephrology. In G.B. Merenstein & S.L. Gardner (Eds.), Handbook of neonatal intensive care (6th ed., pp. 736-772). St. Louis, MO: Mosby Elsevier.
Thayyil, S., Sheik, S., Kempley, S. & Sinha, A. (2008). A gestation and postnatal age-based reference chart for assessing renal function in extremely premature infants. Journal of Perinatology, 28(3): 226-229.
Vogt, B.A., MacRae Dell, K. & Davis, I.D. (2006). The kidney and urinary tract. In R.J. Martin, A. A. Fanaroff & M. C. Walsh (Eds.), Neonatal-perinatal medicine: Diseases of the fetus and infant (8th ed., vol. 2, pp. 1659-1685). St Louis, MO: Mosby Elsevier.
Session Outline
See presentation handout on the following pages.
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW
B15: NEONATAL RENAL REVIEW Page 12 of 13
What Do You Think?
Baby B is a FT delivered by C/S for severe fetal distress associated with placenta abruption. Apgars were 2 & 4. Vigorous resuscitation, including intubation, ventilation and volume expansion for hypotension. At 24 hours of age, she is severely oliguric, edematous, & urine is grossly bloody
Post renal disease Prerenal renal disease Intrinsic renal disease
FANNP 24TH NATIONAL NNP SYMPOSIUM: CLINICAL UPDATE AND REVIEW