50
NEONATAL SEPSIS
| Date post: | 16-Jul-2015 |
| Category: |
Documents |
| Upload: | airamsherlyn-natinga |
| View: | 416 times |
| Download: | 4 times |
NEONATAL SEPSIS
Airamsherlyn P. Natinga, MD
DefinitionDefinition
Neonatal sepsisNeonatal sepsis is a clinical syndrome is a clinical syndrome of systemic illness accompanied by of systemic illness accompanied by bacteremia occurring in the first month bacteremia occurring in the first month of life.of life.
IncidenceIncidence
primary sepsis is 1 - 8 per 1000 live primary sepsis is 1 - 8 per 1000 live births births
as high as 13-27 per 1000 for infants as high as 13-27 per 1000 for infants weighing <1500 gweighing <1500 g
mortality rate is high (13-25%)mortality rate is high (13-25%) higher rates are seen in premature higher rates are seen in premature
infants and in those with early fulminant infants and in those with early fulminant disease disease
PathophysiologyPathophysiology
3 Clinical Situations :3 Clinical Situations :
A.A. Early- Onset DiseaseEarly- Onset Disease
B.B. Late - Onset DiseaseLate - Onset Disease
C.C. Nosocomial Sepsis Nosocomial Sepsis
PathophysiologyPathophysiology
A. Early-Onset DiseaseA. Early-Onset Disease first 5 – 7 days of lifefirst 5 – 7 days of life is usually a multi-system fulminant illness is usually a multi-system fulminant illness
with prominent respiratory symptomswith prominent respiratory symptoms Typically, the infant has acquired the Typically, the infant has acquired the
organism during the intrapartum period from organism during the intrapartum period from the maternal genital tract…the maternal genital tract…
PathophysiologyPathophysiology
In this situation, the infant is colonized with the In this situation, the infant is colonized with the pathogens in the perinatal period..pathogens in the perinatal period..
Several infectious agents….Several infectious agents….TreponemesTreponemesVirusesViruses ListeriaListeria CandidaCandida can be acquired transplacentally via can be acquired transplacentally via
hematogenous routes hematogenous routes
PathophysiologyPathophysiology
acquisition of other organisms is associated acquisition of other organisms is associated with the birth process. with the birth process.
with rupture of membranes, vaginal flora or with rupture of membranes, vaginal flora or various bacterial pathogens may ascend to various bacterial pathogens may ascend to reach the amniotic fluid and the fetus reach the amniotic fluid and the fetus ChorioamnionitisChorioamnionitis develops, leading to fetal develops, leading to fetal colonization and infection.colonization and infection.
aspiration of infected amniotic fluid by the fetus aspiration of infected amniotic fluid by the fetus or neonate may play a role in resultant or neonate may play a role in resultant respiratory symptoms. respiratory symptoms.
PathophysiologyPathophysiology
presence of vernix or meconium impairs the presence of vernix or meconium impairs the natural bacteriostatic properties of amniotic natural bacteriostatic properties of amniotic fluid. fluid.
Finally, the infant may be exposed to vaginal Finally, the infant may be exposed to vaginal flora as it passes through the birth canal. flora as it passes through the birth canal.
PRIMARY SITES of colonization :PRIMARY SITES of colonization :1.1. nasopharynxnasopharynx2.2. oropharynxoropharynx3.3. conjuctivaconjuctiva4.4. umbilical cordumbilical cord
PathophysiologyPathophysiology
Trauma to these mucosal surfaces Trauma to these mucosal surfaces infection infection
Early-onset disease is characterized by a Early-onset disease is characterized by a sudden sudden onset and fulminant course that can onset and fulminant course that can progress rapidly to septic shock with a high progress rapidly to septic shock with a high mortality rate.mortality rate.
PathophysiologyPathophysiology
2. Late - Onset Disease2. Late - Onset Disease as early as 5 days of age but common as early as 5 days of age but common 1st 1st
week of life week of life although these infants may have a history of although these infants may have a history of
obstetric complications obstetric complications less frequent than less frequent than early-onset disease early-onset disease
infants usually have an identifiable focus, most infants usually have an identifiable focus, most often meningitis in addition to sepsisoften meningitis in addition to sepsis
PathophysiologyPathophysiology
bacteria responsible for late-onset sepsis bacteria responsible for late-onset sepsis and meningitis include those : and meningitis include those :
1. acquired after birth from the maternal 1. acquired after birth from the maternal genital tract genital tract
2. acquired after birth from human contact 2. acquired after birth from human contact or from contaminated equipmentor from contaminated equipment
PathophysiologyPathophysiology
The reasons for The reasons for delay in development in clinical delay in development in clinical illness, the predilection for central nervous illness, the predilection for central nervous system (CNS) disease, and the less severe system (CNS) disease, and the less severe systemic and cardiorespiratory symptomssystemic and cardiorespiratory symptoms are are unclear. unclear.
PathophysiologyPathophysiology
C. Nosocomial SepsisC. Nosocomial Sepsis occurs in high-risk newborn infants occurs in high-risk newborn infants
They are related to :They are related to :
1.1. to the underlying illness and debilitation of the to the underlying illness and debilitation of the infantinfant
2.2. the flora in the NICU environment the flora in the NICU environment
3.3. invasive monitoring and other techniques used invasive monitoring and other techniques used in neonatal intensive care in neonatal intensive care
PathophysiologyPathophysiology
Breaks in the natural barrier function of the Breaks in the natural barrier function of the skin and intestine allow this opportunistic skin and intestine allow this opportunistic organism to overwhelm the neonate organism to overwhelm the neonate
Infants, especially premature infants, have an Infants, especially premature infants, have an increased susceptibility to infection increased susceptibility to infection underlying illnesses and immature defenses underlying illnesses and immature defenses that are less efficient at localizing and clearing that are less efficient at localizing and clearing bacterial invasion.bacterial invasion.
Causative OrganismsCausative Organisms
Agents associated with primary sepsis are usually from the Agents associated with primary sepsis are usually from the vaginal flora :vaginal flora :
1.1. group B streptococci (GBS)group B streptococci (GBS) most common most common 2.2. Gram-negative enteric organisms especially E. Gram-negative enteric organisms especially E.
colicoli3.3. Listeria monocytogenesListeria monocytogenes4.4. StaphylococcusStaphylococcus 5.5. other streptococci (including the enterococci)other streptococci (including the enterococci)6.6. anaerobesanaerobes7.7. HHaemophilus influenzaeaemophilus influenzae
Causative OrganismsCausative Organisms
The flora causing nosocomial sepsis vary in The flora causing nosocomial sepsis vary in each nursery…each nursery…
The Agents are :The Agents are :
1.1. Staphylococci (especially SStaphylococci (especially Staph. taph. epidermidisepidermidis))
2.2. gram-negative rods (including gram-negative rods (including PPseudomonas, Klebsiella, Serratia,seudomonas, Klebsiella, Serratia, and and PProteusroteus and fungal organisms predominate and fungal organisms predominate
Clinical PresentationClinical Presentation
initial diagnosis of sepsis is, by necessity, a initial diagnosis of sepsis is, by necessity, a clinical one because it is imperative to begin clinical one because it is imperative to begin treatment before the results of culture are treatment before the results of culture are available available
Clinical S/Sx of sepsis are nonspecific, and the Clinical S/Sx of sepsis are nonspecific, and the
differential diagnosis is broad differential diagnosis is broad
Clinical PresentationClinical Presentation
1.1. Temperature irregularityTemperature irregularity.. Hypo- or Hypo- or hyperthermia (greater heat output required by hyperthermia (greater heat output required by the incubator or radiant warmer to maintain a the incubator or radiant warmer to maintain a neutral thermal environment or frequent neutral thermal environment or frequent adjustments of the infant servo control probe).adjustments of the infant servo control probe).
2.2. Change in behaviorChange in behavior.. Lethargy, irritability, or Lethargy, irritability, or change in tone.change in tone.
3.3. SkinSkin.. Poor peripheral perfusion, cyanosis, Poor peripheral perfusion, cyanosis, mottling, pallor, petechiae, rashes, sclerema, mottling, pallor, petechiae, rashes, sclerema, or jaundice.or jaundice.
Clinical PresentationClinical Presentation
4.4. Feeding problemsFeeding problems. . Feeding intolerance, Feeding intolerance, vomiting, diarrhea (watery loose stool), or vomiting, diarrhea (watery loose stool), or abdominal distention with or without visible abdominal distention with or without visible bowel loops.bowel loops.
5.5. CardiopulmonaryCardiopulmonary.. Tachypnea, respiratory Tachypnea, respiratory distress (grunting, flaring, and retractions), distress (grunting, flaring, and retractions), apnea within the first 24 h of birth or of new apnea within the first 24 h of birth or of new onset (especially after 1 week of age), onset (especially after 1 week of age), tachycardia, or hypotension, which tends to be tachycardia, or hypotension, which tends to be late sign.late sign.
6.6. MetabolicMetabolic.. Hypo- or hyperglycemia or Hypo- or hyperglycemia or metabolic acidosis.metabolic acidosis.
Risk Factors :Risk Factors :
1.1. Prematurity and low birth weightPrematurity and low birth weight
2.2. Rupture of membranesRupture of membranes.. Premature or Premature or prolonged (>18 h) rupture of membranesprolonged (>18 h) rupture of membranes
3.3. Maternal peripartum feverMaternal peripartum fever (≥38 ˚C/100.4 (≥38 ˚C/100.4 ˚F) or infection. Chorioamnionitis, urinary ˚F) or infection. Chorioamnionitis, urinary tract infection (UTI), vaginal colonization tract infection (UTI), vaginal colonization with with E..coli. E..coli. and other obstetric and other obstetric complications.complications.
4.4. Amniotic fluid problemsAmniotic fluid problems.. Meconium- Meconium-stained or foul-smelling, cloudy amniotic stained or foul-smelling, cloudy amniotic fluid.fluid.
Risk Factors :Risk Factors :
5.5. Resuscitation at birthResuscitation at birth.. Infants who had Infants who had fetal distress, were born by traumatic fetal distress, were born by traumatic delivery or were severely depressed at birth delivery or were severely depressed at birth and required intubation and resuscitation.and required intubation and resuscitation.
6.6. Multiple gestationMultiple gestation..7.7. Invasive proceduresInvasive procedures. . Invasive monitoring Invasive monitoring
and respiratory or metabolic support.and respiratory or metabolic support.8.8. Infants with galactosemiaInfants with galactosemia (predisposition (predisposition
to to E. coli E. coli sepsis), immune defects, or sepsis), immune defects, or asplenia.asplenia.
Risk factorsRisk factors9.9. Iron therapyIron therapy (iron added to serum in vitro (iron added to serum in vitro
enhances the growth of many organisms).enhances the growth of many organisms).
10.10. Other factors.Other factors. males are 4 times more affected than females males are 4 times more affected than females more common in black than in white infantsmore common in black than in white infants Variations in immune function may play a roleVariations in immune function may play a role NICU staff and family members are often NICU staff and family members are often
vectors for the spread of microorganisms, vectors for the spread of microorganisms, primarily as a result of improper hand primarily as a result of improper hand washing.washing.
DiagnosisDiagnosis
A . Laboratory StudiesA . Laboratory Studies
1. Cultures1. Cultures Blood and other normally sterile body fluids Blood and other normally sterile body fluids
should be obtained for culture.. *Positive should be obtained for culture.. *Positive bacterial cultures will confirm the diagnosis of bacterial cultures will confirm the diagnosis of sepsis sepsis
Computer-assisted, automated blood culture Computer-assisted, automated blood culture systems systems shown to identify up to 94% of all shown to identify up to 94% of all microorganisms by 48 hr of incubation microorganisms by 48 hr of incubation
DiagnosisDiagnosis
CulturesCultures … … Results may vary because of a number of Results may vary because of a number of
factors, including maternal antibiotics factors, including maternal antibiotics administered before birth, organisms that are administered before birth, organisms that are difficult to grow and isolate (ie., anaerobes), and difficult to grow and isolate (ie., anaerobes), and sampling error with small sample volumes (the sampling error with small sample volumes (the optimal amount is 1-2 mL/sample). optimal amount is 1-2 mL/sample).
Therefore, in many clinical situations, infants are Therefore, in many clinical situations, infants are treated for “presumed” sepsis despite negative treated for “presumed” sepsis despite negative cultures, with apparent clinical benefit. cultures, with apparent clinical benefit.
DiagnosisDiagnosis
2. Gram's stain of various fluids2. Gram's stain of various fluids helpful for the study of CSF helpful for the study of CSF Gram-stained smears and cultures of amniotic Gram-stained smears and cultures of amniotic
fluid or of material obtained by gastric fluid or of material obtained by gastric aspiration aspiration
Adjunctive laboratory testsAdjunctive laboratory testsA.A. WBC count with differentialWBC count with differential Neutropenia may be a significant finding with Neutropenia may be a significant finding with
an ominous prognosis when associated with an ominous prognosis when associated with sepsis sepsis
Serial white blood cell counts several hours Serial white blood cell counts several hours apart may be helpful in establishing a trend.apart may be helpful in establishing a trend.
DiagnosisDiagnosis
B.B. Platelet countPlatelet count decreased platelet count is usually a decreased platelet count is usually a
late*sign and is very nonspecific late*sign and is very nonspecific
B.B. Acute-phase reactantsAcute-phase reactants complex multifunctional group comprising complex multifunctional group comprising
complement components, coagulation complement components, coagulation proteins, protease inhibitors, C-reactive proteins, protease inhibitors, C-reactive protein (CRP), and others that rise in protein (CRP), and others that rise in concentration in the serum in response to concentration in the serum in response to tissue injury. tissue injury.
DiagnosisDiagnosis
remain elevated with ongoing remain elevated with ongoing inflammation, but with resolution they inflammation, but with resolution they decline rapidly due to a short half-life of 4decline rapidly due to a short half-life of 4—7 h —7 h
CRP demonstrates high sensitivity and CRP demonstrates high sensitivity and negative predictive value negative predictive value
II.II. The standard ESRThe standard ESR may be elevated but usually not until may be elevated but usually not until
well into the illness well into the illness
DiagnosisDiagnosis
I.I. C R P C R P increases the most in the presence of increases the most in the presence of
inflammation caused by infection or tissue inflammation caused by infection or tissue injury injury
highest concentrations in patients with highest concentrations in patients with bacterial infections, whereas moderate bacterial infections, whereas moderate elevations chronic inflammatory conditions elevations chronic inflammatory conditions
onset of inflammation, CRP synthesis onset of inflammation, CRP synthesis increases within 4—6 h, doubling everyincreases within 4—6 h, doubling every 8 8 h, and peaks at about 36—50 hh, and peaks at about 36—50 h
DiagnosisDiagnosis
III.III. Cytokines IL-1ß, IL-6, IL-8, and TNFCytokines IL-1ß, IL-6, IL-8, and TNF major mediators of the systemic response major mediators of the systemic response
to infection to infection Studies have shown that combined use of Studies have shown that combined use of
IL-8 and CRP as part of the workup for IL-8 and CRP as part of the workup for bacterial infection reduces unnecessary bacterial infection reduces unnecessary antibiotic treatment antibiotic treatment
III.III. Surface neutrophil Surface neutrophil CD11CD11 has been shown to be an has been shown to be an
excellent marker of early infection that excellent marker of early infection that correlates well with CRP but peaks earlier. correlates well with CRP but peaks earlier.
DiagnosisDiagnosis
IV.IV. Miscellaneous tests. Miscellaneous tests. Abnormal values for bilirubin, Abnormal values for bilirubin,
glucose, and sodium may, in the proper glucose, and sodium may, in the proper clinical situation, provide supportive clinical situation, provide supportive evidence for sepsis.evidence for sepsis.
DiagnosisDiagnosis
Radiologic StudiesRadiologic Studies
1.1. Chest X-ray filmChest X-ray film in case with respiratory in case with respiratory symptoms symptoms
2.2. Urinary Tract Imaging. Imaging with renal Urinary Tract Imaging. Imaging with renal ultrasound examination, renal scan, or ultrasound examination, renal scan, or voiding cystourethrographyvoiding cystourethrography - should be part - should be part of the evaluation when UTI accompanies of the evaluation when UTI accompanies sepsis. Sterile urine for culture must be sepsis. Sterile urine for culture must be obtained by either a suprapubic or catheterized obtained by either a suprapubic or catheterized specimen specimen
DiagnosisDiagnosis
3.3. Other studies.Other studies. Examination of the Examination of the placenta and fetal membranes may placenta and fetal membranes may disclose evidence of chorioamnionitis disclose evidence of chorioamnionitis and thus an increased potential for and thus an increased potential for neonatal infection neonatal infection
Differential Diagnosis Differential Diagnosis
1.1. Respiratory distress syndrome (RDS)Respiratory distress syndrome (RDS)
2.2. Metabolic diseasesMetabolic diseases
3.3. Hematologic diseaseHematologic disease
4.4. CNS diseaseCNS disease
5.5. Cardiac diseaseCardiac disease
6.6. other infectious processes (ie. TORCH other infectious processes (ie. TORCH infections)infections)
ManagementManagement
1.1. GBS prophylaxisGBS prophylaxis major pathogen in the late 1960s and currently major pathogen in the late 1960s and currently
remains the most common cause of early-remains the most common cause of early-onset sepsis onset sepsis
10 to 30% of pregnant women are colonized 10 to 30% of pregnant women are colonized with GBS in the vaginal or rectal area with GBS in the vaginal or rectal area
incidence of infection has been estimated at incidence of infection has been estimated at 0.8—5.5/1000 live births (unchanged for the 0.8—5.5/1000 live births (unchanged for the past three decades). past three decades).
Case fatality rate ranges from 5—15% Case fatality rate ranges from 5—15%
ManagementManagementConsensus guidelines regarding Consensus guidelines regarding management of GBS were published by management of GBS were published by CDC in 1996 and were supported by CDC in 1996 and were supported by American Association of Pediatrics and American Association of Pediatrics and American College of Obstetricians and American College of Obstetricians and Gynecologists. The guidelines Gynecologists. The guidelines recommended one of two approaches: recommended one of two approaches:
a)a) the prenatal screening approach the prenatal screening approach (screening all pregnant women for GBS (screening all pregnant women for GBS infection at 35—37 weeks gestation and infection at 35—37 weeks gestation and treatment of those women with positive treatment of those women with positive culturescultures) )
ManagementManagement
b)b) identifying women who present with risk identifying women who present with risk factors treating them during laborfactors treating them during labor
To ensure appropriate treatment for neonates To ensure appropriate treatment for neonates born to mothers who receive antibiotics for born to mothers who receive antibiotics for fever and presumed choriomanionitis, as well fever and presumed choriomanionitis, as well as for those born to mothers who receive as for those born to mothers who receive intrapartum antibiotic prophylaxis (IAP) intrapartum antibiotic prophylaxis (IAP) because of GBS colonization, they are because of GBS colonization, they are clinically using an algorithm in their hospital clinically using an algorithm in their hospital based on AAP guidelines, with some based on AAP guidelines, with some alterations based on clinical experiences.alterations based on clinical experiences.
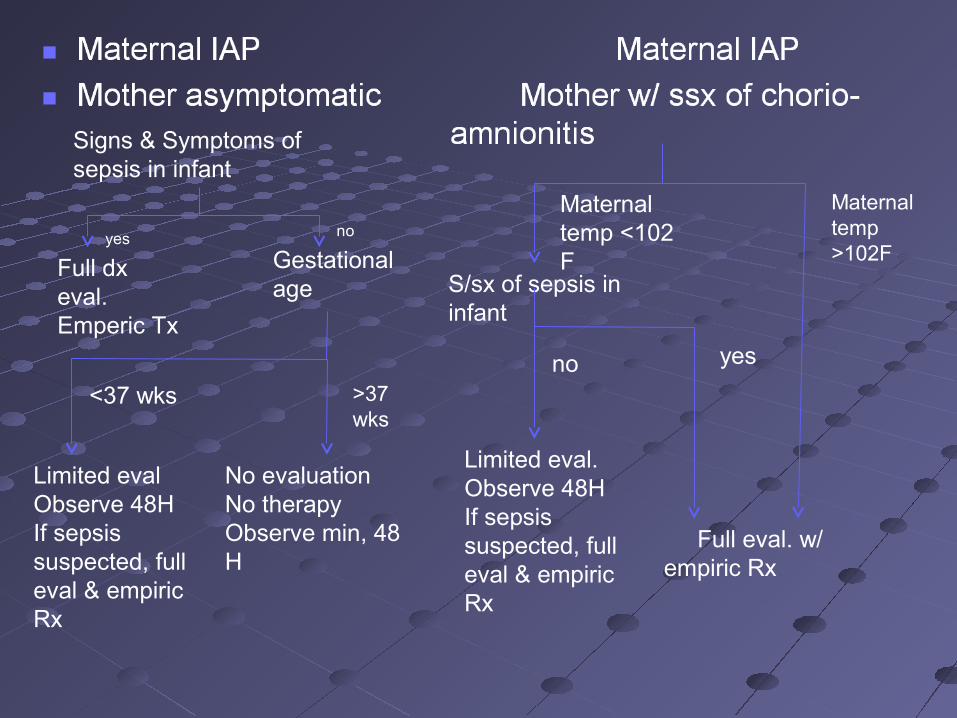
Signs & Symptoms of sepsis in infant
yes no
Full dx eval.Emperic Tx
Gestational age
<37 wks
Maternal temp <102 F
S/sx of sepsis in infant
Maternal temp >102F
no yes
Full eval. w/ empiric Rx
Limited eval.Observe 48HIf sepsis suspected, full eval & empiric Rx
>37 wks
Limited evalObserve 48HIf sepsis suspected, full eval & empiric Rx
No evaluationNo therapyObserve min, 48 H
ManagementManagement
2.2. Standard precautionsStandard precautions have been mandated by the U.S. have been mandated by the U.S.
Occupational Safety and Health Occupational Safety and Health Administration (OSHA) and apply to Administration (OSHA) and apply to blood, semen, vaginal secretions, wound blood, semen, vaginal secretions, wound exudate and CSF and amniotic fluids exudate and CSF and amniotic fluids
caution to prevent injuries when using or caution to prevent injuries when using or disposing of needles or other sharp disposing of needles or other sharp instruments instruments
ManagementManagement
3.3. Initial therapyInitial therapy Treatment is most often begun before a Treatment is most often begun before a
definite causative agent is identified. definite causative agent is identified. Penicillin, Penicillin, usually usually Ampicillin,Ampicillin, plus an plus an
AminoglycosideAminoglycoside such as Gentamicin. such as Gentamicin.
In nosocomial sepsis In nosocomial sepsis flora of the NICU flora of the NICU must be considered: however, generally, must be considered: however, generally, staphylococcal coverage withstaphylococcal coverage with
Vancomycin plus either an Aminoglycoside Vancomycin plus either an Aminoglycoside or a 3or a 3rdrd Gen. ephalosporin Gen. ephalosporin
ManagementManagement
3.3. Continuing therapy Continuing therapy is based on culture is based on culture and sensitivity results, clinical course, and sensitivity results, clinical course, and other serial lab studies (eg., CRP). and other serial lab studies (eg., CRP).
Monitoring for antibiotic toxicity is Monitoring for antibiotic toxicity is important as well as monitoring levels of important as well as monitoring levels of aminoglycosides and vancomycin. aminoglycosides and vancomycin.
ManagementManagement
When GBS is documented as the When GBS is documented as the causative agent causative agent PenicillinPenicillin is the DOC is the DOC AminoglycosideAminoglycoside is often given as well is often given as well because of documented synergismbecause of documented synergism
Complications and Supportive Complications and Supportive TherapyTherapy
1.1. RESPIRATORYRESPIRATORY Ensure adequate oxygenation with blood Ensure adequate oxygenation with blood
gas monitoring and initiate O2 therapy or gas monitoring and initiate O2 therapy or ventilator support if needed ventilator support if needed
2.2. CARDIOVASCULARCARDIOVASCULAR Support BP and perfusion to prevent Support BP and perfusion to prevent
shock. Use volume expanders, 10-20 mL/kg shock. Use volume expanders, 10-20 mL/kg (normal saline, albumin, and blood), and (normal saline, albumin, and blood), and monitor the intake of fluids and output of urine. monitor the intake of fluids and output of urine.
Pressor agents such as dopamine or Pressor agents such as dopamine or dobutamine may be needed.dobutamine may be needed.
Complications and Supportive Complications and Supportive TherapyTherapy
3.3. HematologicHematologic
a.a. DICDIC one may observe generalized bleeding at one may observe generalized bleeding at
puncture sites, the gastrointestinal tract, or puncture sites, the gastrointestinal tract, or CNS sites. In the skin, large vessel CNS sites. In the skin, large vessel thrombosis thrombosis gangrene. gangrene.
Lab. parameters consistent with DIC include : Lab. parameters consistent with DIC include : thrombocytopenia, inc. PT, and inc. Partial thrombocytopenia, inc. PT, and inc. Partial Thromboplastin TimeThromboplastin Time
Complications and Supportive Complications and Supportive TherapyTherapy
Measures include treating the underlying Measures include treating the underlying disease; fresh-frozen plasma, 10 mL/kg; disease; fresh-frozen plasma, 10 mL/kg; vitamin K; platelet infusion; and possible vitamin K; platelet infusion; and possible exchange transfusion.exchange transfusion.
Complications and Supportive Complications and Supportive TherapyTherapy
b)b) NeutropeniaNeutropenia Multiple factors contribute to the increased Multiple factors contribute to the increased
susceptibility of neonates to infection, including susceptibility of neonates to infection, including developmental quantitative and qualitative developmental quantitative and qualitative neutrophil defects. neutrophil defects.
Studies suggest Studies suggest use of recombinant human use of recombinant human granulocyte colony-stimulating factor (rhG-granulocyte colony-stimulating factor (rhG-CSF) or recombinant human granulocyte-CSF) or recombinant human granulocyte-macrophage colony-stimulating factor (rhGM-macrophage colony-stimulating factor (rhGM-CSF) can partially counterbalance these CSF) can partially counterbalance these defects and reduce morbidity and mortality. defects and reduce morbidity and mortality.
Complications and Supportive Complications and Supportive TherapyTherapy
4.4. CNSCNS Implement seizure control measures Implement seizure control measures
Phenobarbital,Phenobarbital, 20 mg/kg loading dose 20 mg/kg loading dose monitor for the syndrome of inappropriate monitor for the syndrome of inappropriate
antidiuretic hormone (SIADH) :antidiuretic hormone (SIADH) :
i.i. decreased urine output, decreased urine output,
ii.ii. hyponatremia, hyponatremia,
iii.iii. decreased serum osmolarity, anddecreased serum osmolarity, and
iv.iv. increased urine specific gravity and osmolarity increased urine specific gravity and osmolarity
Complications and Supportive Complications and Supportive TherapyTherapy
4.4. METABOLICMETABOLIC Monitor for and treat hypo- or Monitor for and treat hypo- or
hyperglycemia. hyperglycemia. Metabolic acidosis Metabolic acidosis may accompany sepsis and is treated may accompany sepsis and is treated with bicarbonate and fluid replacement.with bicarbonate and fluid replacement.
Future Developments Future Developments
Immunotherapy progress continues in the Immunotherapy progress continues in the development of various hyperimmune development of various hyperimmune globulins, monoclonal antibodies to the specific globulins, monoclonal antibodies to the specific pathogens causing neonatal sepsis pathogens causing neonatal sepsis
They may prove to be significant adjuvants to They may prove to be significant adjuvants to the routine use of antibiotics for the treatment the routine use of antibiotics for the treatment of sepsisof sepsis
Research is also ongoing into blocking some Research is also ongoing into blocking some of the body's own inflammatory mediators that of the body's own inflammatory mediators that result in significant tissue injury, including result in significant tissue injury, including endotoxin inhibitors, cytokine inhibitors, nitric endotoxin inhibitors, cytokine inhibitors, nitric oxide synthetase inhibitors, and neutrophil oxide synthetase inhibitors, and neutrophil adhesion inhibitors. adhesion inhibitors.

………………Thank youThank you………………
Early-onset disease is characterized by a sudden onset and fulminant course that can progress rapidly to septic shock with a high mortality rate.












![Sepsis neonatal [autoguardado]](https://static.documents.pub/doc/80x56/58e75b911a28ab4a278b506b/sepsis-neonatal-autoguardado.jpg)




