Clinical note Nerve resection, crush and re-location relieve complex regional pain syndrome type II: A case report C. Peter N. Watson a,⇑ , Susan E. Mackinnon b , Jonathan O. Dostrovsky a , Gary J. Bennett c , R. Peter Farran d , Torie Carlson d a Department of Medicine, University of Toronto, Toronto, Ontario, Canada b Department of Surgery, Washington University School of Medicine, St. Louis, MO, USA c Anesthesia Research Unit, McGill University, Montreal, Quebec, Canada d Department of Anesthesia, University of Calgary, Alberta, Canada Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article. article info Article history: Received 29 October 2013 Received in revised form 13 January 2014 Accepted 28 January 2014 Available online xxxx Keywords: Complex regional pain syndrome Causalgia Surgical treatment abstract This case report describes the remarkable recovery of a patient with very long-standing, medically intrac- table and disabling, lower-limb, complex regional pain syndrome type II following the resection, crush- ing, and relocation of sensory nerves. Ó 2014 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved. 1. Introduction Chronic neuropathic pain due to nerve trauma (complex regional pain syndrome [CRPS] type II, or causalgia) is usually not treated by peripheral nerve section, grafting, or relocation surgery by chronic noncancer pain specialists. This appears to be due to a perception of lack of efficacy and fear of pain exacerbation or of the expectation of the inevitable return of pain. The experience of peripheral nerve surgeons is to the contrary [19]. It is time for a re-evaluation of sur- gical treatment in light of advances and experience in reconstructive plastic surgery and hence, the need for the publication of reports of successful surgery of this type. We selectively searched pain jour- nals, books, and book chapters on CRPS to determine the evidence base for chronic noncancer pain specialists regarding the surgical treatment of causalgia. A few reports were found in the pain litera- ture of the relief of upper-limb nerve causalgia by nerve section and grafting [14,27] and a report of infraorbital nerve causalgia re- lieved by nerve section, grafting, and relocation [37]. Here we report the remarkable case of severe, very long-standing, and intractable lower-limb causalgia with immediate and long-term relief following peripheral nerve surgery. 2. Methods Assessment tools used in this case report were the visual ana- logue scale (pain, depression), numerical rating scale (pain), cate- gory scale (pain), the Hospital Anxiety and Depression scale (HADS) [40], the Pain Disability Index (PDI) (function) [6,28], the Brief Pain Inventory Interference scale (BPI-I) (function) [7], and the Short Form Health Survey (SF12v2) [36] for health-related quality of life. Figs. 1 and 2 and Supplemental Figs. 1–4 show clin- ical and functional impairment before surgery. We have used, in part, a qualitative narrative approach in order to capture the un- ique perspective of the patient and her mother. This is in the article but also online. The patient and her mother provided written per- mission to print unedited photographs including their faces in print and online. 3. Case report 3.1. History and examination A 19-year-old woman from Alberta, Canada was seen by one of the authors (P.W.) in October 2010. At this time the patient pre- sented with a 13-year history of continuous, severe, burning pain, allodynia, edema, erythema, and hair coarsening of the left lower leg following a severe inversion ankle sprain without fracture at http://dx.doi.org/10.1016/j.pain.2014.01.025 0304-3959/Ó 2014 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved. ⇑ Corresponding author. Address: Department of Medicine, University of Toronto, Toronto, ON M9A 1T8, Canada. Tel.: +1 416 239 3494; fax: +1 416 239 6365. E-mail address: [email protected](C. P. N. Watson). PAIN Ò xxx (2014) xxx–xxx www.elsevier.com/locate/pain Please cite this article in press as: Watson CPN et al. Nerve resection, crush and re-location relieve complex regional pain syndrome type II: A case report. PAIN Ò (2014), http://dx.doi.org/10.1016/j.pain.2014.01.025
Transcript
PAIN�
xxx (2014) xxx–xxx
w w w . e l s e v i e r . c o m / l o c a t e / p a i n
Clinical note
Nerve resection, crush and re-location relieve complex regionalpain syndrome type II: A case report
http://dx.doi.org/10.1016/j.pain.2014.01.0250304-3959/� 2014 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
⇑ Corresponding author. Address: Department of Medicine, University of Toronto,Toronto, ON M9A 1T8, Canada. Tel.: +1 416 239 3494; fax: +1 416 239 6365.
Please cite this article in press as: Watson CPN et al. Nerve resection, crush and re-location relieve complex regional pain syndrome type II: A casePAIN
C. Peter N. Watson a,⇑, Susan E. Mackinnon b, Jonathan O. Dostrovsky a, Gary J. Bennett c, R. Peter Farran d,Torie Carlson d
a Department of Medicine, University of Toronto, Toronto, Ontario, Canadab Department of Surgery, Washington University School of Medicine, St. Louis, MO, USAc Anesthesia Research Unit, McGill University, Montreal, Quebec, Canadad Department of Anesthesia, University of Calgary, Alberta, Canada
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
a r t i c l e i n f o
Article history:Received 29 October 2013Received in revised form 13 January 2014Accepted 28 January 2014Available online xxxx
This case report describes the remarkable recovery of a patient with very long-standing, medically intrac-table and disabling, lower-limb, complex regional pain syndrome type II following the resection, crush-ing, and relocation of sensory nerves.
� 2014 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
1. Introduction 2. Methods
Chronic neuropathic pain due to nerve trauma (complex regionalpain syndrome [CRPS] type II, or causalgia) is usually not treated byperipheral nerve section, grafting, or relocation surgery by chronicnoncancer pain specialists. This appears to be due to a perceptionof lack of efficacy and fear of pain exacerbation or of the expectationof the inevitable return of pain. The experience of peripheral nervesurgeons is to the contrary [19]. It is time for a re-evaluation of sur-gical treatment in light of advances and experience in reconstructiveplastic surgery and hence, the need for the publication of reports ofsuccessful surgery of this type. We selectively searched pain jour-nals, books, and book chapters on CRPS to determine the evidencebase for chronic noncancer pain specialists regarding the surgicaltreatment of causalgia. A few reports were found in the pain litera-ture of the relief of upper-limb nerve causalgia by nerve sectionand grafting [14,27] and a report of infraorbital nerve causalgia re-lieved by nerve section, grafting, and relocation [37]. Here we reportthe remarkable case of severe, very long-standing, and intractablelower-limb causalgia with immediate and long-term relief followingperipheral nerve surgery.
Assessment tools used in this case report were the visual ana-logue scale (pain, depression), numerical rating scale (pain), cate-gory scale (pain), the Hospital Anxiety and Depression scale(HADS) [40], the Pain Disability Index (PDI) (function) [6,28], theBrief Pain Inventory Interference scale (BPI-I) (function) [7], andthe Short Form Health Survey (SF12v2) [36] for health-relatedquality of life. Figs. 1 and 2 and Supplemental Figs. 1–4 show clin-ical and functional impairment before surgery. We have used, inpart, a qualitative narrative approach in order to capture the un-ique perspective of the patient and her mother. This is in the articlebut also online. The patient and her mother provided written per-mission to print unedited photographs including their faces inprint and online.
3. Case report
3.1. History and examination
A 19-year-old woman from Alberta, Canada was seen by one ofthe authors (P.W.) in October 2010. At this time the patient pre-sented with a 13-year history of continuous, severe, burning pain,allodynia, edema, erythema, and hair coarsening of the left lowerleg following a severe inversion ankle sprain without fracture at
Fig. 1. Interrupted line: area of ‘‘all pain’’ (dotted line, white arrow), area of ‘‘’’deeppain’’ (open circles, white double-headed arrow), area of dynamic and punctateallodynia to touch and hyperalgesia to pin (interrupted line, black arrow), scar fromfirst operations in 2004 and 2005 (marked with x).
2 C. P. N. Watson et al. / PAIN�
xxx (2014) xxx–xxx
the age of 6 years after a fall from a playground climber. Prior to2010 she had been treated with an ankle foot arthrosis brace forone month and had many nonsurgical treatments (SupplementaryTable 1) in a pediatric pain clinic. At this stage, the pain wasthought to be due to CRPS Type II. The sensory findings were con-sistently localized to the superficial peroneal nerve, and about2 years after injury the pain was completely and repeatedlyblocked by local anesthetic injections at the fibular head, per-formed by one of the authors (P.F.). More details of these localanesthetic and also phenol blocks are appended to SupplementaryTable 1. The phenol block provided partial relief, but the residualpain was severe enough to warrant referral to Neurology.
At age 13 years (December 2004, 7 years after the initial trau-ma), the patient had an ‘‘arthroscopic debridement of the left an-kle, lateral ligament repair and reconstruction of the joints usinga screw in the left ankle’’ (case notes). Shortly after this operationshe developed frequent severe electric shock-like neuropathic painin the allodynic area of the left lateral ankle.
In June 2005 the screw was removed and a neuroma (casenotes) was resected, but with no improvement. The patient partic-ipated in a multidisciplinary pain management program beginningin 2006. The treatments included physiotherapy with a pediatricpain physiotherapist, and group and individual cognitive-behav-ioural therapy for pain management, pain education, relaxationtraining, biofeedback, and supportive counseling with a pediatricpain psychologist (T.C.). At this time, she was assessed for socialand emotional functioning and was described as having difficultieswith pain-related anxiety. Over the next 2 years, with continueddecline in her physical functioning, the patient’s social and emo-tional functioning also declined. At age 18 years (2009) she wastransferred to an adult pain service and participated in privatelyfunded psychological pain management with one of the authors
Please cite this article in press as: Watson CPN et al. Nerve resection, crush andPAIN
(T.C.). Her pain continued unabated and in the severe (7–10/10)range for all components despite the variety of medications andprocedures listed in Supplementary Table 1.
During the period of 2009–2010, the patient gained 80 pounds(probably related to antidepressants and gabapentinoids), acquiredbenign intracranial hypertension (headaches and papilledema)attributed to the birth control pill, and acquired idiopathic throm-bocytopenic purpura attributed to diclofenac. The latter 2 compli-cations responded to treatment.
An electromyogram and nerve conduction study 18 months be-fore the surgery described below identified absence of conductionof the left superficial peroneal nerve. Sural nerve conduction waspresent and symmetrical. The diagnosis by the physiatrist/electro-physiologist was CRPS type II involving one nerve (the superficialperoneal) based on this test and the clinical findings. A consulta-tion with a neurosurgeon specializing in peripheral nerve surgeryat this time concluded that there was also possible involvementof the sural nerve (due to the extent of sensory disturbance [13]).
When examined in October 2010 (P.W.), the patient reported asteady burning pain, frequent electric shocks, and extreme sensi-tivity of the left lower lateral leg with touch-evoked pain in thesame area, all rated as severe and between 7 and 10 on a 0–10 scale(Fig. 1). She slept with her leg exposed (Fig. 2) and slept poorly be-cause of the pain evoked by contact with the bed linens. She re-mained severely restricted in activities, getting about in awheelchair for short distances at home. She moved about on herhands and knees to avoid tactile contact with the lower left leg(Supplementary Fig. 1). She could not wear shoes, socks, or longpants (wearing shorts instead) because of the aggravation of theskin sensitivity and steady, burning pain (Supplementary Fig. 2).She wrapped her leg in ice before a shower (SupplementaryFig. 3A, B) and could not submerge the leg in a bath. An ankle footarthrosis brace failed to provide protection (Supplementary Fig. 4).She was taking long-acting oxycodone 120 mg every 12 hours,transdermal fentanyl 25 lg/hour every 3 days, pregabalin 150 mgtwice a day, amitriptyline 150 mg at night, and oral ketamine25 mg twice daily. The area of ‘‘all pain’’ was over a wide area ofthe left lower lateral leg (Fig. 1) with an area of ‘‘deep’’ pain overthe anterolateral ankle. She had exquisite allodynia to touch, bothpunctate and dynamic, and hyperalgesia to pin and cold on the leftlateral lower leg (Fig. 1). Here the skin was equally dry and of thesame temperature as the corresponding area on the right leg. Therewas no weakness of the ankle or in the limb proximally, and thereflexes were present and equal. There were no trophic changesin skin, hair or nails, or swelling. There was pain-limited restrictionof left ankle movements. The diagnosis was CRPS II based in part onthe previous observations of others of lower-limb erythema, ede-ma, hair coarsening, and allodynia. The lesion was thought to liein either the superficial peroneal plus sural nerves [13], or in thesuperficial peroneal nerve alone, with centrally mediated extrater-ritorial pain [29] extending into the territory of the sural nerve.
Consultation with 3 experienced and highly respected pain neu-rosurgeons in different North American centers counseled againstnerve resection. The patient was then referred to a plastic surgeonin St. Louis, Missouri, USA (S.M.) based on previous success with asimilar case [37].
Pain descriptors (see Dr. Mackinnon’s rating scale online) cho-sen just prior to surgery in St. Louis were of ‘‘throbbing,’’ ‘‘smart-ing,’’ ‘‘aching,’’ ‘‘shooting,’’ ‘‘stabbing,’’ ‘‘tingling,’’ and‘‘hypersensitive.’’ Pain severity in the left leg ‘‘now,’’ ‘‘over the pastmonth,’’ and ‘‘past week’’ was severe and 10/10 on a 0–10 ratingscale where 10 means worst possible pain. A quality-of-life visualanalogue scale was 10/10 and also ‘‘100% affected.’’ A visual ana-logue scale for depression was 7/10, for stress 7/10, and coping5/10. Pain was reported to be increased by activity and by hotand windy weather. Difficulty falling asleep and remaining asleep
re-location relieve complex regional pain syndrome type II: A case report.
Fig. 2. Before surgery: sleeping position with lower lateral left leg having no contact with bedclothes.
C. P. N. Watson et al. / PAIN�
xxx (2014) xxx–xxx 3
were identified. Intimate personal relations were described as af-fected, as well as frequent suicidal rumination and inability towork and do household chores. Three wishes expressed were: 1)‘‘to be normal and have no pain, be on no meds, and no side effectsand to want my brain back,’’ 2) ‘‘to go to school to study psychol-ogy and acupuncture,’’ and 3) ‘‘be able to have normal relation-ships and to learn who I really am without meds.’’
3.2. Surgical procedure (Sept 28, 2011, full details online;Supplementary Figs. 5A–C, 6A & B), further details of surgical rationaleand technique: http://nervesurgery.wustl.edu and references[3,4,10,19,32]
Surgery entailed resecting and cauterizing the superficialperoneal and sural nerves near the ankle, relocating the proximalnerve stumps into deep muscle around the gastrocnemius/soleusinterface, and crushing both nerves [3] near the fibular head, for30 seconds with a hemostat about 35 cm proximal to the ankle.See online description for further details.
3.3. Postoperative course
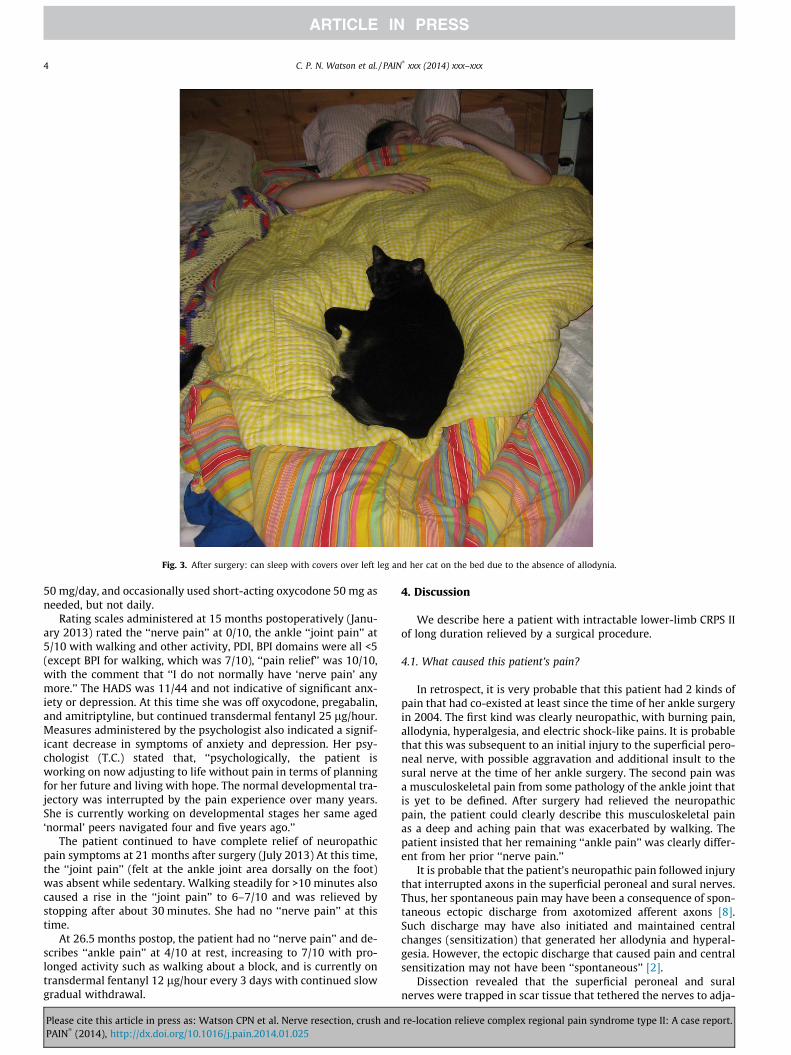
Immediately and at 12 days postoperatively, there was anabsence of all neuropathic pain components (steady burning,shocks, and skin sensitivity [allodynia]), and strikingly, the patientwas immediately able to wear socks and tolerate clothing and bed-clothes on the lower left leg due to relief of the allodynia (Fig. 3)(Supplementary Fig. 7). She said, ‘‘It is the first time in 7 years thatI have been without pain.’’ The severe, constant, nontriggered‘‘nerve pain’’ in the allodynic area was also much diminished.The predominant steady pain after surgery she described as ‘‘jointpain’’ slowly diminished.
Please cite this article in press as: Watson CPN et al. Nerve resection, crush andPAIN
At 5 months after surgery the patient was re-assessed in Toron-to (P.W.). She said that since immediately after the surgery, theskin sensitivity had been gone and she had been able to wear socks,shoes, and pants. Her previous pain was replaced by a differentpostoperative ‘‘pressure-pain’’ clearly distinct from the preopera-tive ‘‘nerve pain’’ and rated at 2/10 and ‘‘mild’’ without medication.This pain was ‘‘0.5/10’’ with medication consisting of pregabalin50 mg twice daily, amitriptyline 50 mg at bedtime, long-actingoxycodone 80 mg every 8 hours, transdermal fentanyl 100 lg/hourevery 3 days, and oxycodone 50 mg every 4 hours as needed (thiswas used infrequently). There was a problem with withdrawalsymptoms due to opioid dose reduction, and an increased opioiddose may also relate to the reduction in amitriptyline and pregab-alin because of weight gain and the discontinuation of ketamine atthis time. Her HADS score was 5 (no significant depression or anx-iety), all BPI interference scales and PDI scales were 0–4 at most or‘‘moderate,’’ and the SF12v2 indicated a good health-related qual-ity of life. There was a problem with insomnia but this was not be-lieved to be pain-related. She was driving, going out socially, andwalking 50 feet, but stopped at this distance by ankle soreness,which she felt as an ache that was unlike her previous ‘‘nervepain.’’ Examination revealed healed scars. There was a large areaof reduced sensation to touch, pin, and cold over the lateral leftleg, conforming to the superficial peroneal and sural nerve territo-ries (Supplementary Figs. 6A & B and 8). There was no allodynia,hyperesthesia, or hyperalgesia. The skin, hair, and nails of the leftleg appeared normal. A plan for gradual medication reductionwas developed.
At 1 year postoperatively, the patient continued as before andcould walk for 30 minutes. She remained on 10 mg long-actingoxycodone every 8 hours, celecoxib, transdermal fentanyl 100 lg/hour every 3 days, pregabalin 150 mg/day, and amitriptyline
re-location relieve complex regional pain syndrome type II: A case report.
Fig. 3. After surgery: can sleep with covers over left leg and her cat on the bed due to the absence of allodynia.
4 C. P. N. Watson et al. / PAIN�
xxx (2014) xxx–xxx
50 mg/day, and occasionally used short-acting oxycodone 50 mg asneeded, but not daily.
Rating scales administered at 15 months postoperatively (Janu-ary 2013) rated the ‘‘nerve pain’’ at 0/10, the ankle ‘‘joint pain’’ at5/10 with walking and other activity, PDI, BPI domains were all <5(except BPI for walking, which was 7/10), ‘‘pain relief’’ was 10/10,with the comment that ‘‘I do not normally have ‘nerve pain’ anymore.’’ The HADS was 11/44 and not indicative of significant anx-iety or depression. At this time she was off oxycodone, pregabalin,and amitriptyline, but continued transdermal fentanyl 25 lg/hour.Measures administered by the psychologist also indicated a signif-icant decrease in symptoms of anxiety and depression. Her psy-chologist (T.C.) stated that, ‘‘psychologically, the patient isworking on now adjusting to life without pain in terms of planningfor her future and living with hope. The normal developmental tra-jectory was interrupted by the pain experience over many years.She is currently working on developmental stages her same aged‘normal’ peers navigated four and five years ago.’’
The patient continued to have complete relief of neuropathicpain symptoms at 21 months after surgery (July 2013) At this time,the ‘‘joint pain’’ (felt at the ankle joint area dorsally on the foot)was absent while sedentary. Walking steadily for >10 minutes alsocaused a rise in the ‘‘joint pain’’ to 6–7/10 and was relieved bystopping after about 30 minutes. She had no ‘‘nerve pain’’ at thistime.
At 26.5 months postop, the patient had no ‘‘nerve pain’’ and de-scribes ‘‘ankle pain’’ at 4/10 at rest, increasing to 7/10 with pro-longed activity such as walking about a block, and is currently ontransdermal fentanyl 12 lg/hour every 3 days with continued slowgradual withdrawal.
Please cite this article in press as: Watson CPN et al. Nerve resection, crush andPAIN
We describe here a patient with intractable lower-limb CRPS IIof long duration relieved by a surgical procedure.
4.1. What caused this patient’s pain?
In retrospect, it is very probable that this patient had 2 kinds ofpain that had co-existed at least since the time of her ankle surgeryin 2004. The first kind was clearly neuropathic, with burning pain,allodynia, hyperalgesia, and electric shock-like pains. It is probablethat this was subsequent to an initial injury to the superficial pero-neal nerve, with possible aggravation and additional insult to thesural nerve at the time of her ankle surgery. The second pain wasa musculoskeletal pain from some pathology of the ankle joint thatis yet to be defined. After surgery had relieved the neuropathicpain, the patient could clearly describe this musculoskeletal painas a deep and aching pain that was exacerbated by walking. Thepatient insisted that her remaining ‘‘ankle pain’’ was clearly differ-ent from her prior ‘‘nerve pain.’’
It is probable that the patient’s neuropathic pain followed injurythat interrupted axons in the superficial peroneal and sural nerves.Thus, her spontaneous pain may have been a consequence of spon-taneous ectopic discharge from axotomized afferent axons [8].Such discharge may have also initiated and maintained centralchanges (sensitization) that generated her allodynia and hyperal-gesia. However, the ectopic discharge that caused pain and centralsensitization may not have been ‘‘spontaneous’’ [2].
Dissection revealed that the superficial peroneal and suralnerves were trapped in scar tissue that tethered the nerves to adja-
re-location relieve complex regional pain syndrome type II: A case report.
cent structures and possibly to each other. Stump neuromas andneuromas-in-continuity are often surrounded by scar tissue thattethers them to adjacent structures. Normal axons are relativelyinsensitive to mechanical distortion, but axonal sprouts ending ina neuroma may acquire exquisite mechanosensitivity [5,38]. Thereis evidence for this in both animals [5,11,17,30,38] and man[23,24]. For example, in the chronic constriction injury model inthe rat, the mid-thigh neuroma-in-continuity becomes tetheredto both dorsal and ventral thigh muscle in a large mass of scar tis-sue. Taping the neuromatous mass or stretching it by flexing thelimb causes discharge that excites nociceptive neurons in thespinal cord dorsal horn [18]. In the patient described here, the loca-tion of neuromatous scars and intraoperative observations suggestthat any movement of the foot, even movement of the toes, mighthave caused discharge in sensory axons ending in the neuroma; alikely cause of pain. The presence of electric shock-like pain isespecially suggestive of mechanical distortion of a neuroma, as thiswould lead to the simultaneous discharge of large numbers ofabnormally mechanosensitive afferent endings in the neuroma[1]. Pain evoked by mechanical stress on a neuroma is anotherexample of stimulus-evoked pains related to activities of daily liv-ing that may be confused with ‘‘spontaneous pain’’ [2].
It is noteworthy that the patient experienced immediate andcomplete relief of her neuropathic pain symptoms (steady burningpain, allodynia, hyperalgesia, and electric shock-like pain). Thissuggests that the entire neuropathic pain syndrome was depen-dent on neural activity originating distal to the resections. This isconsistent with the observation that neuropathic pain can be tem-porarily eliminated by local anesthesia of a neuroma [12]. Our pa-tient experienced immediate relief of severe neuropathic pain of13 years duration. Such a result challenges the concept that centralneuroplastic changes always become permanent and independentof a peripheral afferent drive. It is well known from many recentstudies [26] that various different types of peripheral nerve injuryin animal models of neuropathic pain lead to a constellation ofchanges not only in the affected nerves including their dorsal rootganglia but also in the dorsal horn, thalamus, and descending mod-ulatory pathways. These central changes can include activation ofglia, alterations in chloride homeostasis, changes in gene expres-sion, up- or downregulation of various neurotransmitters andreceptors, and can lead to reduced inhibition and sensitization ofspinal cord dorsal horn nociceptive neurons [15,25,26,31,33,39].There is also much evidence that in many cases these centralchanges, which result in mechanical allodynia and hyperalgesiaand nociceptive behavior, depend on afferent activity from the in-jured nerve [9].
The fact that this patient’s neuropathic pain did not return afterthe operation (also the case for the infraorbital nerve resection pa-tient we have described previously [37]) may be explained in 2ways. First, it may be that spontaneous ectopic discharge wasnever a factor in this patient, with ectopic discharge due to abnor-mal mechanosensitivity the only pain generator. Animal data sup-port the idea that axotomized axons may acquire abnormalmechanosensitivity without demonstrating spontaneous discharge[5,11,17,30,38]. Second, it may be that spontaneous discharge froma neuroma does not recur when a new neuroma forms.
4.2. Why the reluctance to operate?
In our experience, there is a general view in the community ofphysicians and surgeons specializing in chronic pain that surgeryaimed at further denervation does not generally help neuropathicpain such as CRPS II. The belief seems to be that nerve transectionruns the risk of aggravating a central sensitization component andexacerbating pain, and in the best of cases offers no more thantemporary relief.
Please cite this article in press as: Watson CPN et al. Nerve resection, crush andPAIN
The following discussion is based on a search of books and arti-cles in the pain literature likely to form the evidence base of painspecialists. In Mitchell’s 1872 description of causalgia, a term hecoined for nerve trauma pain (now CRPS II) in Civil War soldiers[21], there is an account of median nerve resection that moderatedpain in the distribution of the resected nerve. Noordenbos andWall’s (1981) report [22] of surgical outcomes in 7 cases of painfrom nerve trauma (3 upper and 4 lower limbs) emphasized thelack of satisfactory relief by nerve resection. They concluded that,‘‘This operation should not be done in patients with this condition.Reasons are given to suggest that peripheral nerve damage induceschanges in the central nervous system which are not reversed bytreatment directed at the area of the original injury.’’ This articleby 2 eminent pioneers in the pain field may have contributed toa negative view. However, details given of these 7 patients did re-veal that 3/7 had some evidence of improvement.
The results of experimental studies of the consequences ofnerve injury in rats probably also contributed to a reluctance tooperate on CRPS II patients. First, it was shown that transected pri-mary afferent sensory fibers ending in a stump neuroma acquired aspontaneous discharge that originated at both the end of the tran-sected axon and in the axon’s cell body in the dorsal root ganglion[11,16,34,35]. Insertion of microelectrodes into human stump neu-romas confirmed that these phenomena occurred in man and thatthey were present even many years after the nerve injury [23,24].Spontaneous discharge offered a ready explanation for the pres-ence of spontaneous pain and dysesthesiae. It was known thatexcising a neuroma is followed by the growth of a new neuroma.This may have suggested to some that one could hope for no morethan partial and temporary cessation of pain-evoking spontaneousafferent discharge. It should be noted that the experimental evi-dence is not as clear-cut as it might seem. The appearance of spon-taneous discharge in sensory axons after nerve transection is notalways seen [20], and to the best of our knowledge, no one has everdemonstrated the return of spontaneous discharge after neuromaresection.
Although there are many articles in a general search, and partic-ularly of articles found in plastic surgery journals, only a few re-ports of surgery for CRPS II have appeared in the pain literaturein the last 2 decades. Inada et al. (2005) [14] reported 2 cases of re-lief of digital nerve injury pain in the hand by nerve sectioning andthe use of an artificial nerve guide tube. Two of the current authors(P.W. and J.D.) and their colleagues reported (2007) the case of ayouth with intractable infraorbital nerve injury pain due to orbitalfracture who had gradual (unlike this patient), but eventually com-plete, relief (now at 9 years) after nerve resection proximal to theinjury with grafting and nerve relocation [37]. Stovkis et al.(2010) [27] reported on 34 patients operated on for upper-limb‘‘neuroma pain’’ by nerve resection with either restoration of nervecontinuity or burying of the proximal stump in bone or muscle.Nineteen of 34 (56%) reported satisfaction with the result at amean of 22 months and with functional improvement. However,none of the 34 patients had complete resolution of ‘‘spontaneous’’pain.
4.3. Conclusions
The option of peripheral nerve surgery, with or without a graftor nerve reconstitution, for patients with CRPS II needs to be morewidely recognized. A surgeon skilled in nerve reconstruction andfamiliar with the techniques described here is essential. More de-tails of this type of surgery are available in the additions to thisarticle online, at http://[email protected], and in reference[19]. Crushing the nerve proximal to the neuroma excision maybe essential for a positive outcome [3,19] (see also online surgerydescription re: Schwann cell senescence). A search for Tinel sign(s)
re-location relieve complex regional pain syndrome type II: A case report.
before surgery may help in patient selection. It may be possible toidentify a positive Tinel response even when the skin is allodynicbecause the localized response (electric shock-like pain) ought tobe distinct from the pain of dynamically touching an allodynicarea. Consideration of the involvement of more than one nervemay be important, as a wide area of allodynic skin may not neces-sarily be due to central sensitization. It may be critical to search fortethering by neuromatous adhesions. Involvement of a nerve(s)with a significant motor component may be a contraindication.The risk that this type of surgery may fail or even exacerbate painis unknown, and the true outcomes of this procedure can only beknown from careful, quantitative follow-up of many other cases.
Conflict of interest statement
The authors have no conflicts of interest.
Acknowledgements
The authors would like to acknowledge the substantial contri-butions to this article of Dawn and Heather Gilchrist, Judy Watt-Watson, and Anna Mann.
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at http://dx.doi.org/10.1016/j.pain.2014.01.025.
[2] Bennett GJ. What is spontaneous pain and who has it? J Pain 2012;13:921–9.[3] Bridge PM, Ball DJ, Mackinnon SE, Nakao Y, Brandt K, Hunter DA, Hertl C. Nerve
crush injuries—a model for axonotmesis. Exp Neurol 1994;127:284–90.[4] Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron
2006;52:77–92.[5] Chen Y, Devor M. Ectopic mechanosensitivity in injured sensory axons arises
from the site of spontaneous electrogenesis. Eur J Pain 1998;2:165–78.[6] Chibnall JT, Tait RC. The Pain Disability Index: factor structure and normative
data. Arch Phys Med Rehabil 1994;75:1082–6.[7] Daut IE, Cleeland CS, Flanery RC. Development of the Wisconsin Brief Pain
Questionnaire to assess pain in cancer and other diseases. PAIN�
1983;17:197–210.[8] Devor M. The pathophysiology of damaged peripheral nerves. In: Wall PD,
[9] Devor D. Ectopic discharge in Ab afferents as a source of neuropathic pain. ExpBrain Res 2009;196:115–28.
[10] Diamond J, Gloster A, Kitchener P. Regulation of the sensory innervation ofskin: trophic control of collateral sprouting. In: Scott SA, editor. Sensoryneurons: diversity, development, and plasticity. New York: Oxford UniversityPress; 1992. p. 309–32.
[11] Govrin-Lippmann R, Devor M. Ongoing activity in severed nerves: source andvariation with time. Brain Res 1978;159:406–10.
[12] Gracely RH, Lynch SA, Bennett GJ. Painful neuropathy: altered centralprocessing maintained dynamically by peripheral input. PAIN�
1992;51:175–94.[13] Haymaker W, Woodhall B. Peripheral nerve injuries: principles of diagnosis. St.
Louis, MO: WB Saunders; 1953.
Please cite this article in press as: Watson CPN et al. Nerve resection, crush andPAIN
[14] Inada Y, Morimoto S, Moroi K. Surgical relief of causalgia with an artificialnerve tube graft: successful surgical treatment of causalgia by in situ tissueengineering with a polyglycolic acid-collagen tube. PAIN� 2005;117:251–8.
[15] Iwata K, Tsuboi Y, Shima A, Harada T, Ren K, Kanda K, Kitagawa J. Centralneuronal changes after nerve injury: neuroplastic influences of injury andaging. J Orofac Pain 2004;18:293–8.
[16] Kajander KC, Wakisaka S, Bennett GJ. Spontaneous discharge originates in thedorsal root ganglion at the onset of a painful peripheral neuropathy in the rat.Neurosci Lett 1992;138:225–8.
[18] Laird JM, Bennett GJ. An electrophysiological study of dorsal horn neurons inthe spinal cord of rats with an experimental peripheral neuropathy. JNeurophysiol 1993;69:2072–85.
[19] Mackinnon SE, editor. Peripheral nerve surgery. New York: Thieme; 2014.[20] Michaelis M, Liu X, Jänig W. Axotomized and intact muscle afferents but no
[21] Mitchell SW. Injuries to nerves and their consequences. Philadelphia: JBLippincott; 1872.
[22] Noordenbos W, Wall PD. Implications of the failure of nerve resection andgraft to cure chronic pain produced by nerve lesions. J Neurol NeurosurgPsychiatry 1981;44:1068–73.
[23] Nordin M, Nyström B, Wallin U, Hagbarth K-E. Ectopic sensory discharges andparesthesiae in patients with disorders of peripheral nerves, dorsal roots anddorsal columns. PAIN� 1984;20:231–45.
[24] Nyström B, Hagbarth KE. Microelectrode recordings from transected nerves inamputees with phantom limb pain. Neurosci Lett 1981;27:211–6.
[25] Ossipov MH, Dussor GO, Porreca F. Central modulation of pain. J Clin Invest2010;120:3779–87.
[26] Sorkin LS, Yaksh TL. Behavioral models of pain states evoked by physical injuryto the peripheral nerve. Neurotherapeutics 2009;6:609–19.
[27] Stovkis A, van der Avoort DJ, Van Neck JW, Hovius SE, Coert JH. Surgicalmanagement of neuroma pain: a prospective follow-up study. PAIN�
2010;151:862–9.[28] Tait RC, Chibnall JT, Krause S. The Pain Disability Index: psychometric
properties. PAIN� 1990;40:171–82.[29] Tal M, Bennett GJ. Extra-territorial pain in rats with a peripheral
mononeuropathy: mechano-hyperalgesia and mechano-allodynia in theterritory of an uninjured nerve. PAIN� 1994;57:375–82.
[30] Tal M, Wall PD, Devor M. Myelinated afferent fiber types that becomespontaneously active and mechanosensitive following nerve transection in therat. Brain Res 1999;824:218–23.
[31] Tsuda M, Beggs S, Salter MW, Inoue K. Microglia and intractable chronic pain.Glia 2013;61:55–61.
[32] Upton AR, McComas AJ. The double crush in nerve entrapment syndromes.Lancet 1973;2:359–62.
[33] von Hehn CA, Baron R, Woolf CJ. Deconstructing the neuropathic painphenotype to reveal neural mechanisms. Neuron 2012;73:638–52.
[34] Wall PD, Devor M. Sensory afferent impulses originate from dorsal root gangliaas well as from the periphery in normal and nerve injured rats. PAIN�
1983;17:321–39.[35] Wall PF, Gutnik M. Ongoing activity in peripheral nerve: the physiology and
pharmacology of impulses originating from a neuroma. Exp Neurol1974;43:580–93.
[36] Ware JE, Kosinski M, Keller SD. A 12 Item Short-Form Health survey:construction of scales and preliminary tests of reliability and validity. MedCare 1996;34:220–33.
[37] Watson CPN, Stinson JN, Dostrovsky JO, Hawkins C, Rutka J, Forrest C. Nerveresection and re-location may relieve causalgia: a case report. PAIN�
2007;132:211–7.[38] Welk E, Leah JD, Zimmerman M. Characteristics of A- and C-fibers ending in a
sensory nerve neuroma in the rat. J Neurophysiol 1990;63:759–66.[39] Woolf CJ, Salter MW. Neuronal plasticity: increasing the gain in pain. Science
2000;288:1765–9.[40] Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta
Psychiatr Scand 1983;67:361–70.
re-location relieve complex regional pain syndrome type II: A case report.